
Abstract
Lesions in knee joint articular cartilage (AC) have limited repair capacity. Many clinically available treatments induce a fibrous-like cartilage repair instead of hyaline cartilage. To induce hyaline cartilage repair, we hypothesized that type I collagen scaffolds with fibers aligned perpendicular to the AC surface would result in qualitatively better tissue repair due to a guided cellular influx from the subchondral bone. By specific freezing protocols, type I collagen scaffolds with isotropic and anisotropic fiber architectures were produced. Rabbits were operated on bilaterally and two full thickness defects were created in each knee joint. The defects were filled with (1) an isotropic scaffold, (2) an anisotropic scaffold with pores parallel to the cartilage surface, and (3) an anisotropic scaffold with pores perpendicular to the cartilage surface. Empty defects served as controls. After 4 (n=13) and 12 (n=13) weeks, regeneration was scored qualitatively and quantitatively using histological analysis and a modified O'Driscoll score. After 4 weeks, all defects were completely filled with partially differentiated hyaline cartilage tissue. No differences in O'Driscoll scores were measured between empty defects and scaffold types. After 12 weeks, all treatments led to hyaline cartilage repair visualized by increased glycosaminoglycan staining. Total scores were significantly increased for parallel anisotropic and empty defects over time (p<0.05). The results indicate that collagen scaffolds allow the formation of hyaline-like cartilage repair. Fiber architecture had no effect on cartilage repair.
Introduction
A
Focal chondral and osteochondral defects are common injuries with a great impact on the patient's life. Most defects are located on the medial femoral condyle with a mean defect size of ∼2 cm2. 3 Repair of these AC defects is limited due to the low mitotic activity levels of chondrocytes and their dense extracellular matrix surrounding, limiting chondrocyte migration from adjacent healthy AC to the defect site. 4 In addition, AC lacks vascularization, limiting repair from nonchondrocytic cells. The general concept in the orthopedic community is that if injuries to the AC remain untreated, these injuries may progress into more generalized osteoarthritis, although this process of maturation of new cartilage might be age dependent 5 and clinical studies to the natural history of local AC defects are lacking.
Frequently used repair techniques for localized defects in the knee joint are osteochondral grafting or mosaicplasty (MO), the use of biphasic osteochondral synthetic plugs (e.g., TruFit™ system), autologous cell transplantation (ACI), or microfracturing (MF). However, the efficacy of MF, MO, and ACI techniques are still a matter of debate. 6 MF is frequently used particularly for the smaller AC defects. 7 With this technique, small drill holes are made in the subchondral bone, which creates a route for stem cells from the subchondral bone to enter into the defect site. These cells can subsequently differentiate and produce a fibrocartilage or hyaline-like cartilage tissue type. This technique is cheap, simple and can be applied by all surgeons. However, studies with midterm follow-up periods showed that the repair tissue after MF is of a fibrous instead of a hyaline tissue type.8–10 From animal studies it is known that this fibrous tissue is mechanically inferior to native hyaline cartilage. 11 Moreover, it might result in poor physical and chemical bonding to the adjacent healthy AC. Both might result in progressive failure at longer follow-up periods. 4 Therefore, better repair strategies are urgently needed.
The quality of repair tissue might be improved with tissue engineering and/or regenerative medicine applications. A minimally invasive, cost-effective optimization could be to fill defects with smart scaffolds. 12 In this approach, the subchondral bone should be penetrated as in MF, and thereafter, defects could be filled with a scaffold optimized to attract, guide, stimulate, and differentiate bone marrow-derived stem cells originating from the subchondral bone. In this way, defects could be filled more rapidly with a higher quality repair tissue compared to MF.13,14 Previously, scaffolds, based on type I or II collagen, have been described that guide cell migration from the bone marrow into the defect and stimulate cartilage matrix production. 15 Buma et al. showed that attachment of chondroitin sulfate to isotropic type I- and II-based collagen scaffolds could facilitate cartilage repair when implanted in the knee joint of rabbits. However, tissue migration was limited, particularly in the type II scaffolds, and did not reach the full defect thickness even after 12 weeks. 16 Since it has been shown that tissue formation is guided by the orientation of collagen fibers of the scaffold,17,18 we speculated that by filling defects with anisotropic scaffolds, the defects would be filled more rapidly. Moreover, if collagen is produced along the pore orientation of these anisotropic scaffolds, the quality of the articular repair tissue could be improved.
The aim of this study was to investigate the effect of anisotropic type I collagen scaffolds on AC repair. We hypothesized that anisotropic scaffolds implanted with the fiber orientation perpendicular to the surface of the cartilage would result in a more native-like cartilage repair compared to random, isotropic, collagen scaffolds in a full thickness AC defect in rabbits.
Materials and Methods
Scaffold production
A suspension of 0.8% insoluble bovine type I collagen fibrils in 0.25 M acetic acid was swollen overnight at 4 °C and homogenized using a Potter-Elvehjem system (Louwers Glass and Ceramic Technologies) with an intervening space of 0.35 mm for generally 10 strokes. Air bubbles in the suspension were removed by centrifugation at 750 rpm for 30 min at 4°C (Beckmann Coulter, Allegra 6KR centrifuge).
Isotropic porous collagenous scaffolds were prepared by pipetting 4.0 mL of the collagen suspension in one six-well suspension plate well, followed by freezing in a −20°C freezer and lyophilizing in a Sublimator 500 II freeze dryer (Zirbus Technology).17,19 After lyophilization, vapor fixation was performed with 38% formaldehyde under vacuum for 30 min. Vapor crosslinking reaction was stopped by quenching remaining aldehydes with 30 mM NaBH4 in a 1 M sodium phosphate buffer pH 6.5 for 1 h at 4°C. Subsequently, scaffolds were crosslinked using 1- ethyl-3-(3-dimethyl aminopropyl) carbodiimide (EDC) (Fluka Chemie) and N-hydroxysuccinimide (NHS) (Fluka Chemie). 20
Anisotropic collagenous scaffolds were prepared by freezing 10 mL of collagen suspension on a 15×45 mm surface using a freezing gradient from liquid nitrogen (−196°C) to ambient temperature. This temperature gradient results in ice crystal formation in the direction of the temperature gradient starting from the liquid nitrogen upward. Frozen suspensions were lyophilized in the Zirbus freeze dryer to sublimate the ice and leave the collagen as an imprint of the ice crystals, thus yielding orientated collagen lamellae.20,21 These scaffolds were also crosslinked using formaldehyde vapor, quenched and EDC/NHS crosslinked as described above. Scaffolds were cut parallel and perpendicular to the orientation of the scaffold lamellae to obtain anisotropic scaffolds with fibers running perpendicular and parallel to the top surface, respectively. Scaffolds were analyzed with scanning electron microscopy to visualize the iso- and anisotropic architectures in collagen scaffolds, and the crosslinking efficiency was measured using 2,4,6-trinitrobenzene sulfonic acid with a glycine calibration curve.22,23
Animal experiment
For the in vivo experiment, 26 skeletal mature female New Zealand white rabbits were used (mean weight 4.1 kg; SEM±0.12). All procedures were approved by the institutional animal ethics committee. Under general anesthesia, a medial skin incision was made over the knee joint. The joint was opened with a medial parapatellar incision, whereafter the patella was dislocated with the leg in full extension. Two cylindrical full thickness defects (4 mm diameter, 3 mm deep) were created in the patellar groove using a high-speed drill with manual physiological salt irrigation. A spacer was placed onto the 4-mm-diameter drill and fixed 3 mm from the end to standardize the defect size. The two defects were separated by 4 mm of cartilage. Each defect was filled with one of the three scaffolds—isotropic, perpendicular anisotropic, and parallel anisotropic. Empty defects were used as controls. Rabbits were bilaterally operated; thereby each rabbit received one scaffold of each experimental group and a control. No sutures were used to fixate the scaffolds in the defects. The positions of the scaffolds were alternated with a random start. After insertion of the scaffolds, the patella was relocated and the knee was bent three times until 90° of flexion, after which the patella was luxated again to check for proper insertion of the scaffolds. After these procedures, all scaffolds remained in the proper position. Finally, the wound was carefully closed in layers and the animals were allowed full weight bearing and normal daily activity in large rooms with saw dust coverage of the floor. After 4 (n=13) and 12 weeks (n=13), the animals were sacrificed by an overdose of pentobarbital.
Histology
After sacrifice of the rabbits, the knees were inspected macroscopically and synovial tissue was visually analyzed for inflammatory changes. Tissue blocks containing the defects and directly surrounding bone, were dissected with an oscillating saw with irrigation of physiological saline to avoid heat production, fixed in 4% phosphate-buffered (pH 7.4) formalin, and after decalcification with EDTA, embedded in paraffin. Serial sections of 7 μm were stained with hematoxylin/eosin, Picrosirius red, and Safranin O/fast green. Representative sections through the center of the defect were scored blindly by three of the authors (Ed.M., G.H., and P.B.). Sections were described qualitatively in which special attention was given to the location of the new cartilage-like tissue, the presence of fissures, and the remodeling of the subchondral bone. Using a modification of the scoring system developed by O'Driscoll et al. a semiquantitative score of the repair was made.16,24
Statistical analysis
All data are expressed as mean±SEM. Statistical analyses were performed with a two-way ANOVA with factor treatment/scaffold and time and a post hoc LSD (SPSS v18). p-Values<0.05 were considered significant.
Results
Collagen scaffold
A total of 27%±4% and 24%±6% of the available amine groups were used in the crosslinking process for anisotropic and isotropic porous scaffolds, respectively. After lyophilization, isotropic scaffolds showed rounded pores surrounded by collagen sheets (Fig. 1A). Anisotropic scaffolds made with the temperature gradient showed alignment of the collagen sheets with smaller crossing fibers (Fig. 1B parallel anisotropic and Fig. 1C perpendicular anisotropic). The orientation of the collagen sheets was parallel to the heat gradient.
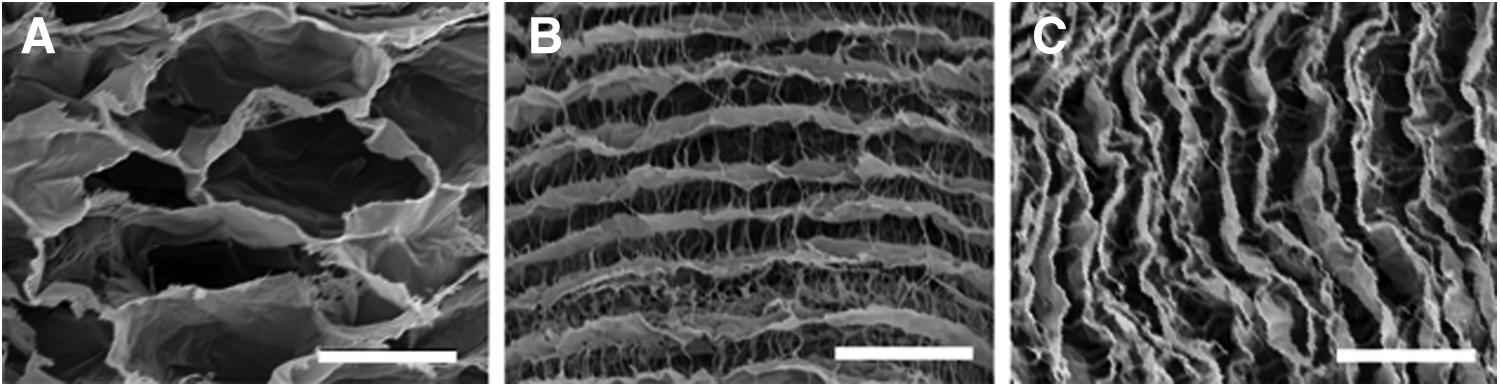
Scanning electron microscopy images of
Macroscopic evaluation
After opening the joints, no significant changes from a normal native appearance were found. In general, the synovial tissue had a normal appearance without signs of inflammation. The synovial fluid was clear and had a normal viscosity and consistency. Both joints of one rabbit of the 4-week group showed severe signs of infection (redness, pus, etc). This animal was excluded from the study. The host cartilage around defect sites showed macroscopically the normal transparent white/bluish color of control cartilage. After a 4-week follow-up, macroscopic inspection showed that all defects, including the controls, could be clearly discerned from the adjacent host cartilage and were all completely filled with material of variable colors, varying from white to transparent red. No difference was observed between the scaffold types (Fig. 2, upper panel). Defects of the 12-week groups were in general whiter and resembled adjacent host cartilage more closely than those of the 4-week group. The surface of the defect site was level with the adjacent host cartilage and had a similar contour (Fig. 2, lower panel). In five perpendicular anisotropic scaffolds, the transition between host and defect was clearly visible. In other cases, this transition was difficult to see macroscopically.
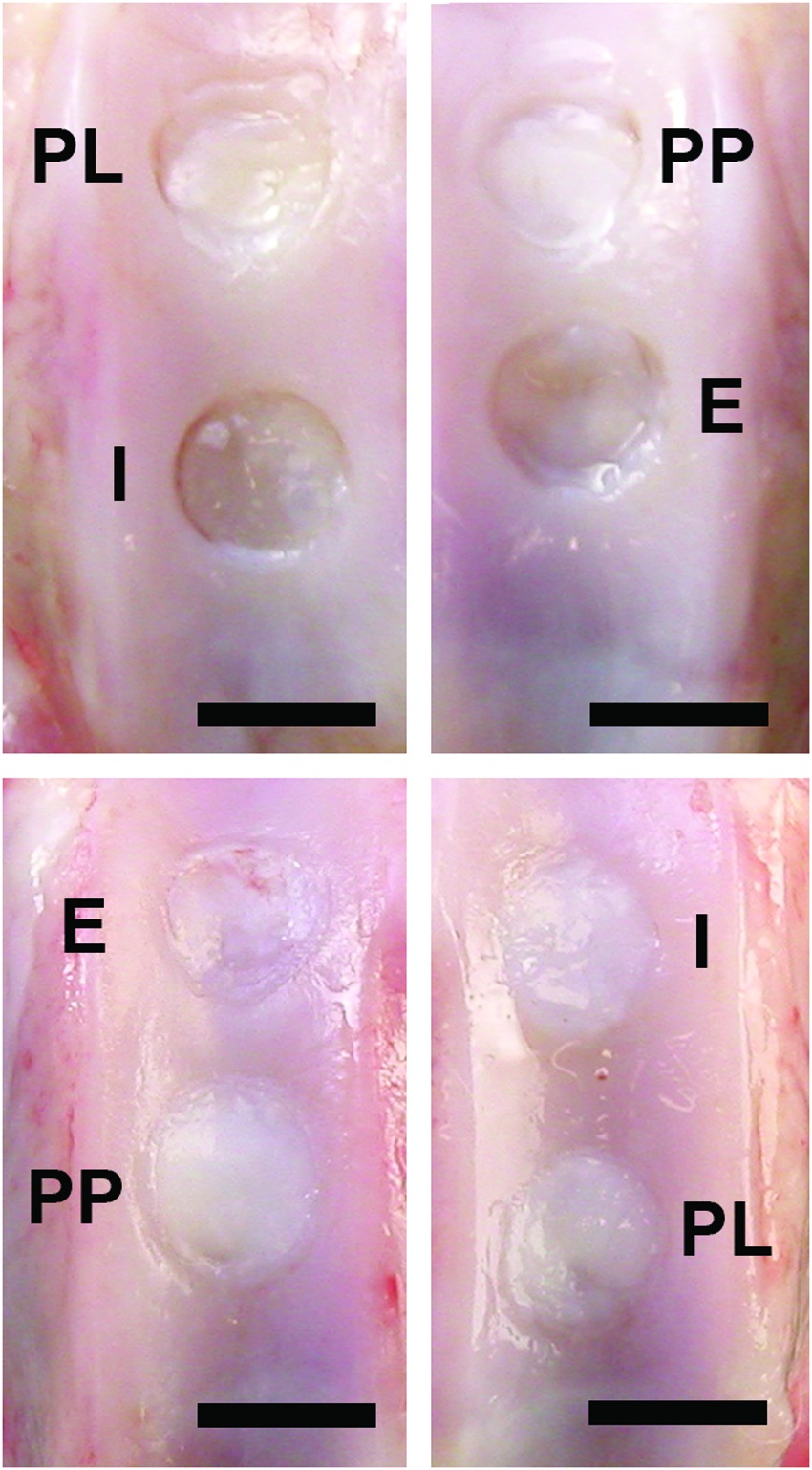
Macroscopic images of defect sites after 4- and 12-week follow-up, upper and lower panel, respectively. PL, parallel anisotropic; PP, perpendicular; I, isotropic; E, empty. Scale bars represent 4 mm. Color images available online at www.liebertpub.com/tea
Histological evaluation
Four weeks
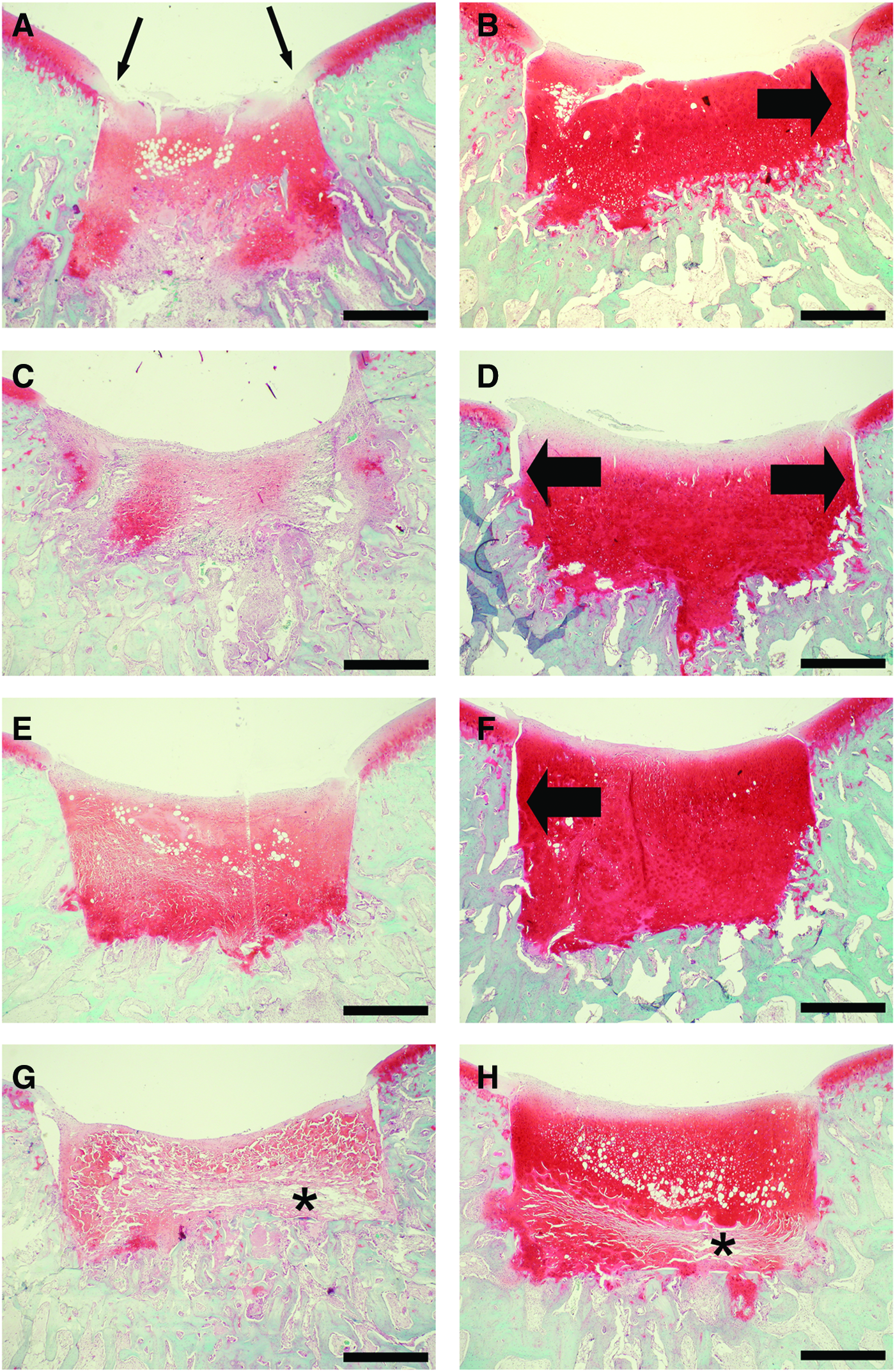
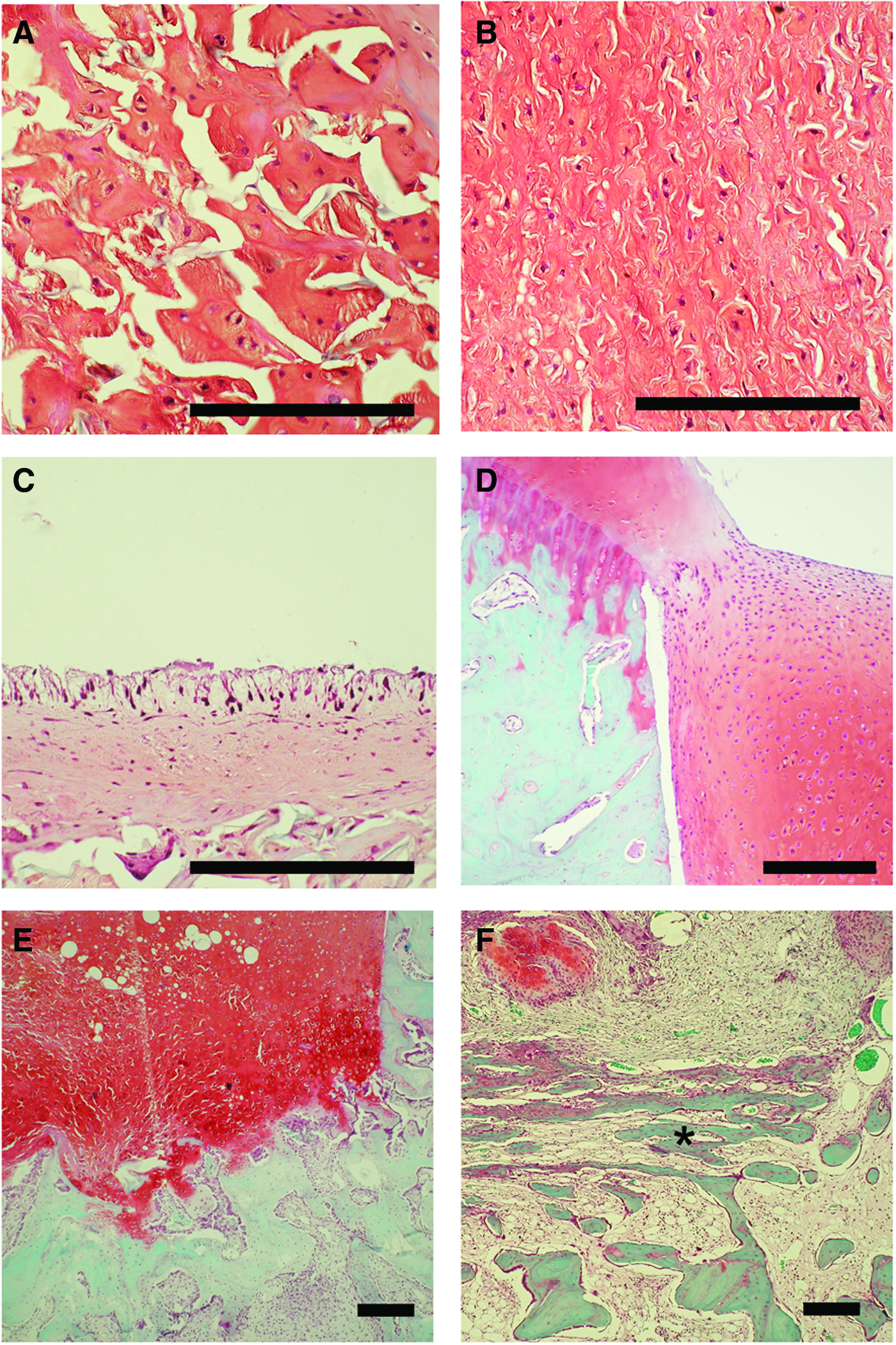
After 4 weeks, the collagen scaffolds could still be seen embedded in newly formed tissues (Figs. 3A, C, E, G and 4A, B). The collagen sheets were thicker in the isotropic scaffolds compared to anisotropic scaffolds (compare the nonstained fibers in the Safranin O) stained sections in Figure 4A. All defects were almost completely filled with partial differentiated cartilage-like tissue as shown by the moderate glycosaminoglycan (GAG) staining with Safranin O (Fig. 3 left panel). Between the different scaffold types or between controls and scaffolds, there was no difference in repair as scored with the modified O'Driscoll method. Total scores ranged between 10.2±1.3 for perpendicular anisotropic and 11.5±1.4 for empty defects (Fig. 5). The contour of the implant surface was similar to that of the native trochlea (Fig. 3 left panel). The surface of the implant site showed occasionally some mild superficial fibrillation (Fig. 4C). The tissue at the surface contained lower cell numbers and was more fibrous compared to the tissues in the deeper parts, which was more chondrogenic. Random scaffolds showed more often areas that were poorly populated with new cells, particularly in areas where the original scaffolds could still be visualized (Fig. 6G). Careful analysis of the Picrosirius red-stained sections showed that the newly formed collagen was less organized as collagen in native AC (Figs. 6A, C, E, G). Integration between implant and host tissue was occasionally observed at the superficial AC side. However, no direct connection was present between the implants and the lateral borders of the subchondral bone (Fig. 4D). A tight tissue connection between subchondral bone and the lower implant side seemed present in all defects (Fig. 4E), but bone remodeling at the bottom of the defect was still very limited or even completely absent after 4 weeks. In three of the defects filled with perpendicular anisotropic scaffolds, a very specific pattern of new bone formation in the bottom of the defects was observed. Trabecular bone was formed with long thin trabeculae orientated parallel to surface of the AC in the direction perpendicular to the anisotropy of the scaffold (Fig. 4F). The new bone seemed to originate from the exposed lateral aspect of the subchondral bone. In defects filled with isotropic scaffolds, locations with less intense staining inside the scaffold were observed (Fig. 3G).
Safranin O staining of empty defects
Safranin O stained sections after 4 weeks of implantations. Isotropic implant

Mean total modified O'Driscoll score (±SEM) of isotropic, parallel anisotropic, perpendicular anisotropic, and empty defects (*p<0.05; 4 weeks n=12, and 12 weeks n=13).
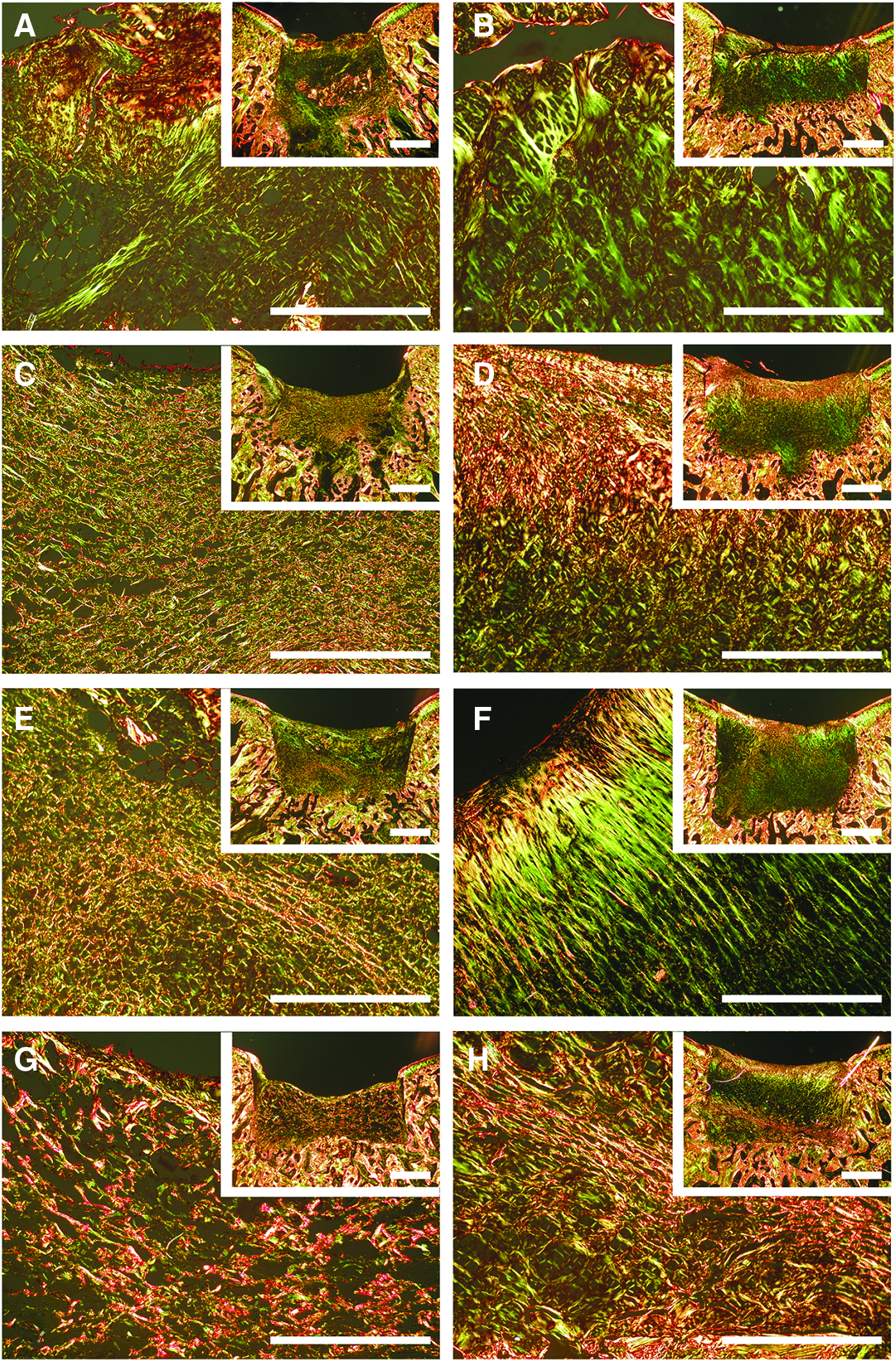
Picrosirius red stained sections after 4
Twelve weeks
All defects were completely filled with cartilage-like tissue (Fig. 3B, D, F, H). The intensity of the GAG staining was increased compared to the 4-week groups (Fig. 3: compare left [4 week] and right [12 week] panel) as visualized by the increased intense red staining in the Safranin O stained sections. Quantitative scores for repair had significantly increased in time for parallel anisotropic and empty defects by 4.1 and 3.9 points, respectively (Fig. 5). For all treatments, the individual O'Driscoll score items showed a time-dependent significant increase for tissue type and thickness (Fig. 7). This significant increase was also measured for degenerative changes, but not significantly for perpendicular anisotropic scaffolds. Cells in the repair tissue were mainly rounded single cells (occasionally in small clusters) surrounded by an intense metachromatically stained extracellular matrix (Fig. 8A). The tissue thus more closely resembled hyaline cartilage-like tissue compared to the 4-week group. The surface of the defect was generally smooth and followed the original contour of the trochlea (Fig. 8B). Occasionally, a small partial thickness fissure was found. This fissure was always located in the central region of the defects and extended into the direction of the subchondral bone (Fig. 8C). In the isotropic scaffolds, we observed more often areas that were poorly populated with new cells (Fig. 3H). Careful analysis of the Picrosirius red stained sections showed that the collagen seemed more organized compared to that in the 4-week defects. Particularly, in the empty defects (Fig. 6B) and in some specimens of the perpendicular anisotropic implants (Fig. 6F), the collagen was more or less orientated perpendicular to the surface of the cartilage. Two defects of the perpendicular anisotropic scaffolds showed new subchondral bone formation up to the original contour of the cartilage with a thin layer of fibrous tissue only on top (Fig. 8D). After 12 weeks, the isotropic scaffolds were still clearly visible in the defects, while the anisotropic scaffolds were not recognizable after 12 weeks (Fig. 3 right panel). Furthermore, isotropic scaffolds did show locations with minor GAG staining (Fig. 3H).

Mean of the individual items of the modified O'Driscoll score (±SEM) of isotropic, parallel anisotropic, perpendicular anisotropic, and empty defects (*p<0.05; 4 weeks n=12, and 12 weeks n=13).

Safranin O stained sections after 12 weeks of implantation. Individual round cells embedded in an intense stained extracellular matrix
Discussion
In general, we found no large effects of fiber orientation on cartilage regeneration and that all repair reactions were similar to that of the empty controls. Even though rabbits were skeletally mature, their relative young age could have had a beneficial effect on the self-repair capacity in the empty defects. Wei and Messner found that spontaneous healing of osteochondral defects in the knee joints of nonskeletal mature rabbits resulted in a faster filling and earlier tissue specialization than in adolescent or older skeletal mature animals. 5 However, it was previously described that this model of a full thickness AC defect in the femur of rabbits remains a suitable model to study differences in cartilage repair between similar scaffold types. 16 For implantation, we used collagenous scaffolds that guide the infiltration, proliferation, and differentiation of progenitor cells, and improve the healing response. 16 We chose crosslinked type I collagen scaffolds above type II collagen scaffolds since in our previous studies type II collagen scaffolds only revealed cartilaginous tissue at the superficial zone and at the interface of the matrix with the subchondral bone, leaving large areas of the matrix devoid of new tissue. We speculated that this was induced by rapid differentiation of stem cells into the cartilage phenotype before the defect was filled completely. Therefore, type I collagen scaffolds with an isotropic or anisotropic pore orientation were made and implanted into the defects. We hypothesized that a perpendicular orientation of collagen fibers to the AC surface enables improved guidance of the cells from the subchondral bone for improved complete thickness repair.
A limitation of this study is that the model used does not lead to fibrocartilaginous type of tissue, which is found after MF in patients. Although the tissue after MF is not well documented histologically, 25 the hyaline-like tissue after MF is less prominent and is mainly found in the deeper parts of the defects and not on the surface. This clinical type of tissue also shows more variation and the collagen is less organized than in the rabbit model used in this study (personal experience of PB). It is questionable if animal models can be developed that lead to identical tissue formation as in patients since the rehabilitation conditions are difficult to control in animal models, the defects are always smaller and the load-bearing conditions might be different from the clinical situations. 26
In this study, no blood vessels were found in the area of the original defect. This indicates that indeed cells from the subchondral bone populated the matrix without vascular invasion. The observation that cells can migrate quite easily in such type I collagenous matrices is not completely surprising since this was already demonstrated in a previous study. 16 The cells involved in matrix population are probably mainly derived from the bone marrow. Shapiro et al. demonstrated that chondrocytes from the residual adjacent cartilage did not participate in the repopulation of full thickness AC defects. 4 Repair was completely mediated by the proliferation and differentiation of mesenchymal cells from the marrow. We assume similar repair in this study. The contribution of repair cells from a synovial origin, however, cannot be ruled out. Hunziker et al. performed a study with partial thickness defects in rabbits in which the defects were filled with fibrin. Mesenchymal cells derived from the synovial membrane migrated across the AC surface into the defect, where they repaired the cavity with fibrous connective tissue. 27 With this in mind, we speculate that in our model also some repair along the latter route might have taken place. In all defects, particularly at the surface of the implants, bridges were formed between the new tissue in the defect and the host cartilage. In addition, only the bottom side, not the lateral sides, showed integration with host tissue indicating that the repair cells that fill the defect probably originated from the deeper parts of the subchondral bone directly under the defect site and did not originate from more laterally located subchondral bone.
Irrespective to the origin of the cells, the scaffold architecture might have influenced the penetration speed and distance into the scaffold. Particularly in the random scaffolds, we observed more often areas that were poorly populated with new cells. Careful analysis of the Picrosirius red stained sections showed that particularly in these areas the original scaffold was still present. More causes can account for the paucity of cells in these areas. First, it can be speculated that the available volume for cells might have been limited by remnants of the scaffold, thereby compromising the migration of cells. Second, it could be speculated that the original scaffold negatively influences the survival of cells. We believe, however, that cell survival is not a problem, since cell culture experiments did never show any adverse effect of meniscus fibroblasts or chondrocytes on the matrices (unpublished) and no necrotic cells were found in the HE stained sections. It seems more likely that the specific orientation in combination with the degradation speed determines the cellular density in a certain scaffold type. Brouwer et al. investigate the ingrowth into similar bilayered collagen scaffolds and found more ingrowth in the unidirectional scaffolds. 28 On the other hand, de Mulder et al. showed that after subcutaneous implantation in rat, ingrowth in isotropic polymer scaffolds was more robust than in anisotropic scaffolds. 29 This was explained by the observation that ingrowth in isotropic scaffolds can occur from all directions into the scaffold as a result of the high interconnectivity of the pores, while in anisotropic scaffolds, tissue ingrowth mainly takes place from the open sides of the porous channels.
All defects had hyaline-like cartilage repair tissue after 4 and 12 weeks of implantation although in general the GAG staining was much more intense after 12 weeks. We found no large effects of fiber orientation on cartilage regeneration. All scaffolds induced similar hyaline-like cartilage repair. Surprisingly, it seemed as if the distribution of cells and matrices was more homogeneous in the empty defects and the anisotropic scaffolds compared to the isotropic scaffolds. The influence of pore size, known to influence cell behavior, 30 might have played a role since in this study the morphology of the scaffolds is quite different between the isotropic random and anisotropic scaffolds. Pore sizes of the isotropic scaffolds appeared to be larger and the collagen walls surrounding the pores were also thicker. Potentially, this could have had an effect on the penetration capacity of the cells into the pores of the scaffold. After 12 weeks, the isotropic scaffolds were still clearly visible in the defects, while the anisotropic scaffolds were not recognizable after 12 weeks. Based on the Picrosirius red stained sections, in which we observed that cellular infiltration in the scaffolds was accompanied by a remodeling of the original scaffold into a new matrix around the chondrocytes, we speculate that during invasion by cells, the original scaffold is resorbed. A rapid degradation in anisotropic scaffolds may have resulted in a reduced effect of the collagen fiber alignment. When scaffolds are quickly degraded, they may not have had the time to guide the cells fully. Development of anisotropic scaffolds with thicker collagen walls may result in increased cell guidance and better cartilage formation.
In the present study, the tissue repair was in general better than found in clinical studies, where a more fibrous tissue type was found after MF and ACI.8–10 However, we cannot state that this is an effect of the scaffolds only since the model used was not very discriminative between the different scaffold types and the empty controls. Further optimization of the developed scaffolds could potentially induce an even better tissue repair. Instead of a homogenous architecture, scaffolds can be made with multiple architectures. 31 Such scaffolds, with an isotropic lower part and a parallel anisotropic upper part, have only been tested in vitro with cultured chondrocytes, and resulted in engineered cartilage tissue that mimicked hyaline cartilage.32,33 An interesting observation in the current study was that a limited number of perpendicular anisotropic scaffolds resulted in organized bone formation at 4 and 12 weeks postoperation parallel to the AC surface and perpendicular to the direction of the collagen fibers. This is the first in vivo indication that based on the orientation of collagen, scaffolds could be designed, which induce organized bone in the deeper parts or the defect and cartilage-like tissue in the more superficial areas of the defect. This type of scaffold might offer a new treatment option for deeper osteochondral defects (ICRS grade V defects). These defects are now treated with the sandwich technique in which, first the bone defect is filled with bone graft and sealed from the rest of the defect with a Chondroguide collagen membrane as in the M-ACI technique. 34 A second collagen membrane is then placed over the cartilage defect and can be treated with conventional ACI techniques.
Besides changing the architecture of collagen scaffolds, others have been mixing it with other macromolecules, such as GAGs to direct stem cell differentiation. Buma et al. showed a positive effect on chondrogenic differentiation of chondroitin sulfate. 16 Matsiko et al. showed that addition of hyaluronic acid to collagen increased mesenchymal stem cell infiltration, higher SOX9 expression, and more cartilage matrix production in vitro when compared to collagen and chondroitin sulfate blends. 35 In addition to blending with matrix components, growth factors could be added to stimulate tissue regeneration.36,37
To increase the regenerative capacity of the scaffold, further research could focus on cell-seeded scaffold implantation. Scaffolds could be seeded with a variety of cells such as autologous or allologous chondrocytes, stem cells or cocultures of these two, with cocultures being the most promising. 38 When implanted in osteochondral knee defects in rabbits, cell-less scaffolds showed good repair tissue, however, tissue repair was even better when scaffolds were preseeded with cells. 39 Nonetheless, the cost–effectiveness of these cell-seeding techniques remains unknown until long-term studies are finished. 40
In conclusion, collagen type I scaffolds are able to regenerate AC with hyaline-like cartilage. Differences in collagen scaffold fiber architecture resulted in similar cartilage repair.
Footnotes
Acknowledgments
This study was sponsored by the Netherlands Institute for Regenerative Medicine and the Dutch Arthritis Foundation. Furthermore, the authors would like to thank Elly Versteeg and Anke van Dongen for their help in manufacturing the collagen scaffolds.
Disclosure Statement
No competing financial interests exist.