
Abstract
Cell-based treatments are being developed as a novel approach for the treatment of many diseases in an effort to repair injured tissues and regenerate lost tissues. Interest in the potential use of multipotent progenitor or stem cells has grown significantly in recent years, specifically the use of mesenchymal stem cells (MSCs), for tissue engineering in combination with extracellular matrix-based scaffolds. An area that warrants further attention is the local or systemic host responses toward the implanted cell–biomaterial constructs. Such immunological responses could play a major role in determining the clinical efficacy of the therapeutic device or biomaterials used. MSCs, due to their unique immunomodulatory properties, hold great promise in tissue engineering as they not only directly participate in tissue repair and regeneration but also modulate the host foreign body response toward the engineered constructs. The purpose of this review was to summarize the current state of knowledge and applications of MSC–biomaterial constructs as a potential immunoregulatory tool in tissue engineering. Better understanding of the interactions between biomaterials and cells could translate to the development of clinically relevant and novel cell-based therapeutics for tissue reconstruction and regenerative medicine.
Introduction
S
Today, different classes of materials are being investigated, including metals, ceramics, polymers (natural and synthetic), and composites. Metals or metal alloys and ceramics are widely used in bone-based applications due to their stability and relatively low immunogenicity. Polymers, both natural and synthetic, are more suited toward soft tissue reconstruction or augmentation. While many of these materials are used in clinical practice, the extent of defect or underlying pathophysiology is often beyond the scope of application of these materials. Instead, many polymers can be modified for the delivery of cells or inductive proteins to provide a microenvironment suitable for tissue repair.
One of the major mediators of inflammation is macrophages, both resident and circulating, often recruited to the site of tissue damage. Such injuries could be from mechanical trauma or surgery, chronic pathology or disease, or through the introduction of a foreign material or infectious agent. Furthermore, foreign material or pathogens are marked for phagocytosis by the immune system through circulating serum proteins recognizing the “non-self” surfaces. In addition to phagocytosis and degradation, macrophages build the immune repertoire by sending chemotactic signals to other circulating cells. Therefore, there are many aspects of the healing process that may be altered to achieve the most desired clinical outcomes, many of which rely on macrophage activity. These factors must be considered in the decision-making process regarding the use of a cell-based or biomaterial construct. 3 To this end, bio-inspired engineered tissues represent the future of regenerative medicine. There is increasing interest in combining biomaterial scaffolds, such as hydrogel polymers, with adult stem cells to enhance their tissue regeneration or engraftment capabilities. This review will discuss the role of such cell–biomaterial composites in moderating the host immune response for cell delivery.
Inflammation and Foreign Body Reaction
The immune system functions through two main pathways: innate and adaptive immunity. Innate immunity is considered as the first line of defense. Foreign material is nonspecifically recognized by macrophages and thus cleared or destroyed from the host. Adaptive immunity is pathogen specific, and while this has limited contributions in wound healing, the pathways involved in adaptive immunity are largely responsible for material or tissue rejection and chronic inflammation.
Macrophages are key immune cells that have a vital role in innate and adaptive immunity, as well as normal healing and remodeling. Normal healing is a complex, progression of hemostasis and inflammation, leading to tissue regeneration. 4 The steps are similar, despite the myriad insults the body may be faced with. Platelet aggregation initiates clotting almost immediately following injury. The wound bed is then infiltrated with proinflammatory neutrophils and macrophages, followed by pro-remodeling fibroblasts. These processes work in parallel to balance destruction with regeneration or granulation.5,6 Even under optimal conditions, this results in loss of normal tissue architecture, loss of function, fibrosis, or scarring.
Macrophages exhibit a heterogeneous phenotype and have several important roles in tissue homeostasis. 7 Classically activated macrophages respond to a variety of proinflammatory stimuli to initiate an effective innate immune response (Fig. 1). On the other hand, alternatively activated macrophages are characterized by distinct cell surface markers and are thought to be more anti-inflammatory and, perhaps, reparative. It is now evident that macrophage profiles exist on a spectrum. Microbicidal activity, antigen presentation, and phagocytosis fall under the purview of classically activated macrophages, whereas tissue repair, wound healing, and regulatory or anti-inflammatory activity are associated with alternatively activated macrophages. 8
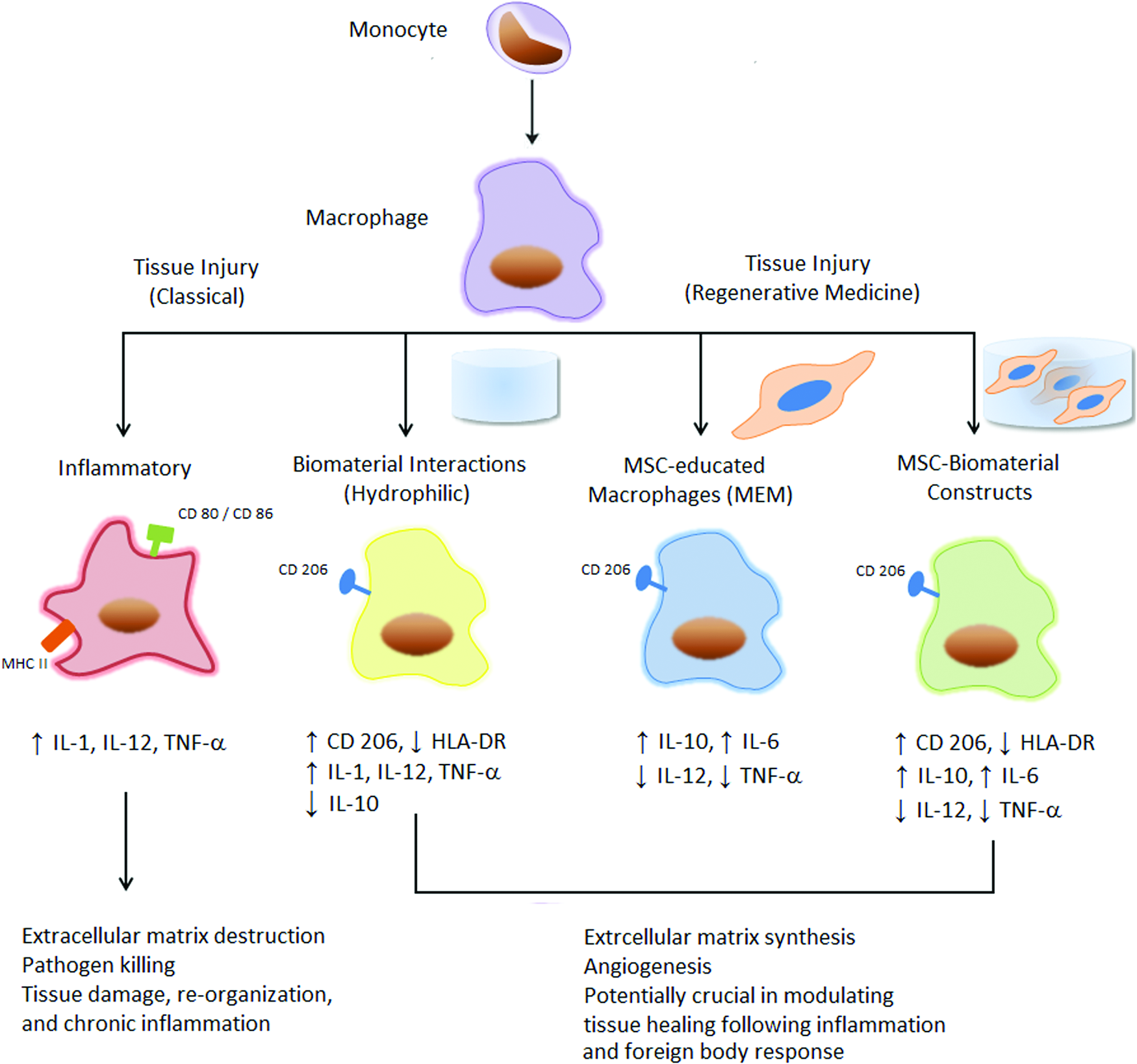
Illustration of the immunomodulatory effects of biomaterials and mesenchymal stem cells (MSCs) on macrophage phenotype and function in vitro. Upon stimulation such as tissue injury, macrophages can acquire a classically activated phenotype, which is associated with proinflammatory cytokines (i.e., IL-1, IL-12, tumor necrosis factor-α [TNF-α]), debris removal, continued inflammation, and tissue injury. These “M1” macrophages bear surface markers such as CD80, CD86, and MHC class II molecules. Alternatively, there is evidence to support an alternatively activated anti-inflammatory immunophenotype, which can be acquired when monocytes are cultured on biomaterials with specific surface chemistry (i.e., hydrophilic) or cocultured with MSCs, with or without a biomaterial scaffold. These alternatively activated macrophages “M2” display surface markers such as CD206 and are associated with an increase in anti-inflammatory cytokines (i.e., IL-10, IL-6, TGF-β), extracellular matrix production, and tissue remodeling. Modified with permission from Hematti and Hanson. 11 IL, interleukin; TGF-β, transforming growth factor β. Color images available online at www.liebertpub.com/tea
Foreign body reactions proceed much like early wound healing, including the response to implanted biomaterials. Circulating proteins and inflammatory cells are recruited to the foreign material, debris is cleared and granulation tissue begins to form. However, instead of proceeding to tissue remodeling, the presence of a foreign material stimulates continued inflammation by tissue macrophages. “Frustrated phagocytosis” occurs when macrophages are unable to engulf the foreign body; rather, these cells fuse to form larger phagocytes and the cycle continues. This chronic inflammatory process takes place in the local tissue of the implanted biomaterial or device and can lead to resorption or failure in addition to further trauma of the local tissue itself.
Interestingly, it has been shown that biologic scaffolds can induce pro- or anti-inflammatory macrophage phenotypes, depending on the composition.9,10 While there is a significant effort in combining different types of cells, such as terminally differentiated chondrocytes, with various biomaterials, incorporating multipotent mesenchymal stromal cells (MSCs) into such cell/biomaterial constructs could be advantageous due to their unique immunomodulatory properties. As illustrated in Figure 1, upon stimulation such as tissue injury or device implantation, macrophages generally become classically activated, characterized by the production of proinflammatory cytokines (i.e., interleukin [IL]-1, IL-12, tumor necrosis factor-α [TNF-α]), debris removal, continued inflammation, and tissue injury. These macrophages demonstrate an increased expression of costimulatory molecules CD80 and 86. Alternatively, when monocytes are cultured on biomaterials with specific surface chemistry (i.e., hydrophilic) or cocultured with MSCs, with or without a biomaterial scaffold, monocytes can acquire an alternative phenotype. These alternatively activated macrophages are identified, in part, by the surface marker CD206 and are characterized by a wound environment with anti-inflammatory cytokines (i.e., IL-10, IL-6, transforming growth factor-β [TGF-β]), extracellular matrix (ECM) production, and tissue remodeling. Undifferentiated MSC-hydrogel constructs may advantageously affect tissue repair in cell-based therapies by directing macrophages along an anti-inflammatory immunophenotype that would traditionally be proinflammatory.
Mesenchymal Stem Cells
MSCs are multipotent progenitor cells with many desirable properties for regenerative medicine.3,11,12 It is now known that MSCs reside within the bone marrow as well as most adult tissues and organs.13–15 These cells are defined by characteristic cell surface markers and multilineage differentiation capabilities. 16 Studies suggest that while isolated from different sources, MSCs possess similar biological, physiological, and functional characteristics.14,17–19 Over the past decade, their ever-growing use in regenerative medicine is based on the evidence that MSCs affect tissue regeneration, inflammation, and vascularization or angiogenesis (Fig. 2) among others, many of them being mediated through paracrine mechanisms.20–25
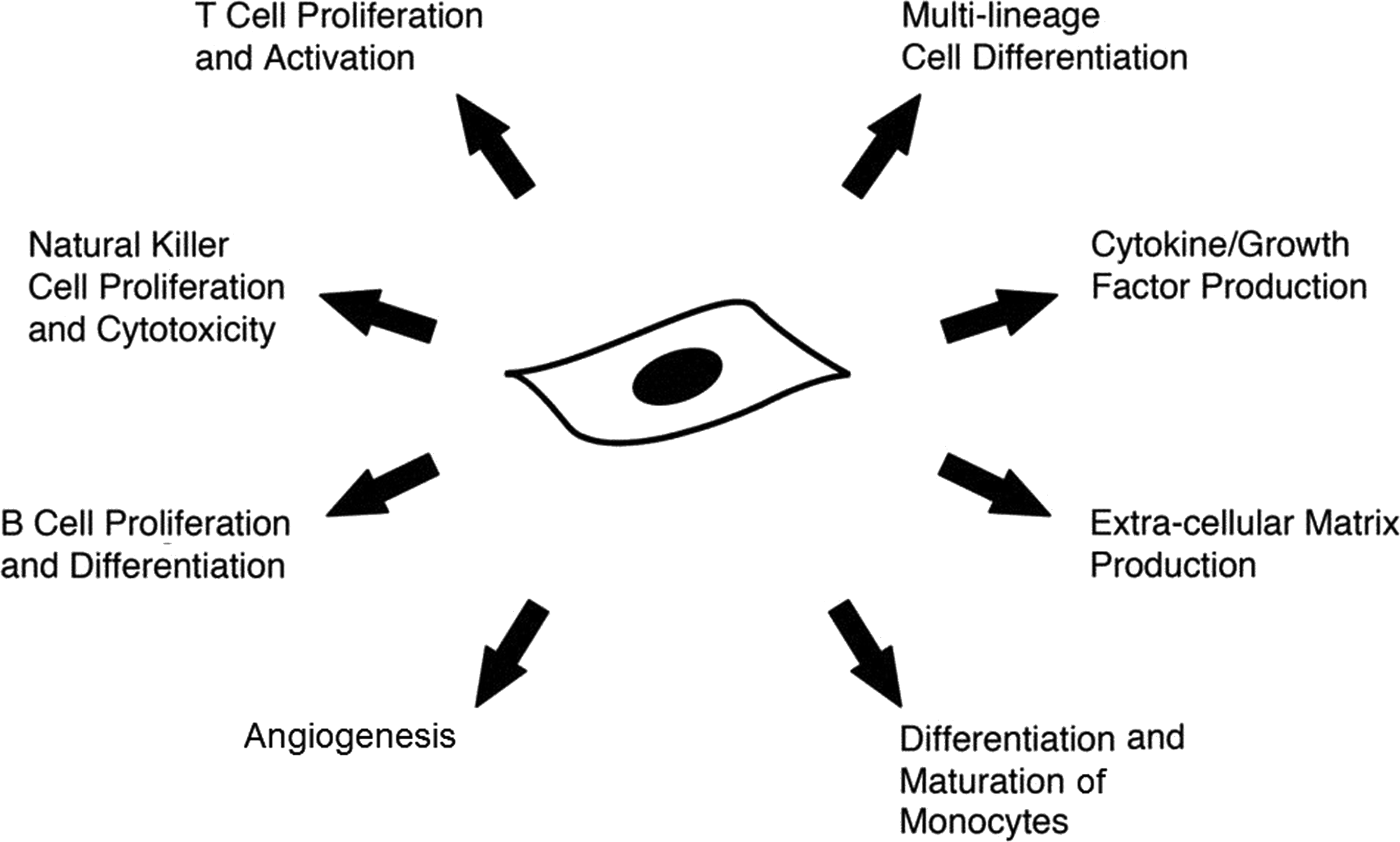
Illustration of the multiple mechanisms through which MSCs modulate tissue healing, inflammation, and regeneration. Modified with permission from Hematti and Hanson. 11
MSCs are shown to hone in on the site of inflammation or injury. Once there, MSCs stimulate resident cells through growth factor secretion and matrix remodeling to promote differentiation of native progenitor cells and the recovery of injured cells. Furthermore, they exert anti-inflammatory effects, making them potential key players in wound healing and in the integration of tissue-engineered constructs. The recent evidence of the effect of MSCs on macrophage phenotype is of great significance.26–29 The immunoprivileged status of MSCs is constantly being challenged as more cross talk between MSCs and components of innate immunity are being discovered. MSCs express low levels of MHC class I and essentially absent levels of MHC class II molecules, largely contributing to their immune protection. However, they are known to express and exert their effect through toll-like receptors and their ligands, 30 which in turn may affect MSCs anti-inflammatory effects. 31 It has been proposed that MSCs may exhibit altering phenotypes in a manner similar to macrophages, demonstrating proinflammatory (MSC1) and anti-inflammatory (MSC2) characteristics. 32
There is ongoing interest in combing MSCs with ECM-based hydrogel scaffolds in tissue engineering strategies. For example, bone marrow-derived MSCs injected locally into chronic wounds, with or without a fibrin-based scaffold, have demonstrated increased reepithelialization and healing. 33 MSC-derived chondrocytes have been used to essentially reconstitute a decellularized cadaveric donor trachea coated with autologous epithelial cells. 34 It is expected that there will be a huge expansion in utilization of these adult stem cells for cellularization of biomaterials for reconstructive and regenerative purposes. Still, clinical utility will be dependent on further elucidating the cross talk between MSCs and the many components of tissue healing and regeneration that we seek to regulate by the addition of cellular constructs based on underlying pathophysiology, medical comorbidities, and concurrent treatments.
Biomaterial Constructs
Bioengineered scaffolds provide a microenvironment that allows for biochemical, structural, and cellular support that could promote tissue healing through encapsulated or resident tissue cells. Many of these scaffolds are based on clinically available materials, such as collagen or hyaluronic acid, used without cells for tissue augmentation or repair.35–37 It is only natural that there has been movement in combining these materials with cells for tissue engineering strategies in vivo. Furthermore, whole tissues have been processed to remove antigenic proteins and cells, leaving a complex scaffold for cell seeding or implantation. Alloderm®, Strattice™, and Surgimend® are examples of commercially available, “off the shelf” acellular dermal matrices derived from human, porcine, and bovine tissues, respectively. These are routinely used without cells in reconstructive surgery and soft tissue replacement.38–40
Implantation of a biomaterial construct, with or without encapsulated cells, can stimulate an inflammatory response, both by mechanical and physical injury or by foreign body reaction. Once implanted, the host immune response is initiated by circulating proteins, which quickly cover the biomaterial construct based on the nature of the implanted material. 41 Chemical composition, scaffold geometry, and spatial relationship of a material will affect its functional utility. Protein adsorption and cell differentiation or function have been shown to be influenced by hydrophobicity, the addition of pendant chains, surface topography, porosity, and encapsulated cell concentration.42–44
Currently, polymers are the most clinically relevant biomaterials and are constantly being developed or modified for improved function or tissue integration. The list of such materials is seemingly endless. Synthetic polymers lack biologically functional domains, however, and cannot facilitate cell attachment or migration or direct phenotypic expression, unless modified to do so. Natural polymers, such as collagen, hyaluronic acid, and fibrin, are components of ECM and similar to other physiologically active proteins. This structural similarity allows for progenitor cell attachment, proliferation, and differentiation in vitro. However, naturally occurring polymers are likewise vulnerable to normal physiology, such as hydrolytic degradation, thereby limiting their stability in vivo.
Thus, composite or blend materials are being investigated with nonimmunogenic synthetic polymers that allow for the addition of cell-adhesive peptide sequences and growth factors. 45 The addition of short peptide sequences increases the biocompatibility and functional properties of the scaffold. For instance, the addition of heparin-bound vascular endothelial growth factor to a self-assembling peptide (SAP) solution stimulated more vasculogenesis than the peptide scaffold alone. 46 SAPs are 15–20 amino acid chains that undergo self-assembly, based on the interactions of their repeating or alternating peptide sequence. For example, alternating hydrophobic functional groups with hydrophilic groups allows the protein to fold on itself in the aqueous solution, trapping water and forming a nanofibrous hydrogel. 47 Hydrogel polymers, such as polyethylene glycol diacrylate (PEG-DA), are attractive for use in soft tissue applications because they maintain structure unlike collagen and hyaluronic acid alone. PEG-DA is often used to cross-link ECM-based materials. These materials have high water content to provide an ECM-like environment, 48 supporting cell migration and differentiation but with enhanced structural stability. They are also easily dispensed into areas that are difficult to access. The addition of cells to form three-dimensional tissue constructs shows promise for in situ tissue formation (Fig. 3) with solid implantable or more fluid injectable formulations.

Macroscopic photos of explants from in vivo adipogenesis proof of concept experiment combining a polyethylene glycol diacrylate-based hydrogel with adipose-derived MSCs
An example of this is shown in Figure 3. In this proof-of-concept experiment, we demonstrate neoadipogenesis and neovascularization of a construct comprising culture-expanded human adipose-derived MSCs encapsulated in a modified PED-DA hydrogel sphere (Fig. 3A). The constructs were implanted on the flanks of nude mice with an acellular control (Fig. 3B). At 4 weeks, the constructs show viable adipose tissue with new vessel ingrowth along the surface and minimal fibrous capsule formation. Lipid accumulation was confirmed macroscopically with Oil Red O staining. This work illustrates important findings and limitations of current state of tissue-engineered constructs for regeneration. De novo tissue formation can be directed by the material used as a scaffold, and further modifications may steer complex structures, drug delivery, and perhaps even functional tissues. Size of the tissue construct will be limited by vascularity and many of the other limitations of current reconstructive options. The engraftment of a tissue will be dependent on not only blood supply but also limited foreign body reaction or inflammatory response.
Extensive work is focused on the interaction between macrophages and a variety of biomaterials with the goal of further directing the inflammatory response to implantable materials in a favorable manner (Fig. 1). 41 Hydrophobic polymers, in particular, have been shown to enhance monocyte adhesion and foreign body giant cell formation with associated local immune response at the site of implantation in vivo.49,50 Hydrophilic surfaces on the other hand induce apoptosis of adherent macrophages 51 and are associated with variable cytokine expression, including increased interleukin (IL)-10 (anti-inflammatory) and decreased IL-8 (pro-inflammatory) 52 indicating an alternatively activated anti-inflammatory phenotype. While chemically cross-linking ECM-based materials have been shown to increase stability and prolong degradation, it may result in a macrophage phenotypic switch in vitro. Both surface topography and chemistry influence monocyte adhesion, with the introduction of micron-scale architecture reducing adhesion and cell fusion. Likewise, serum coating the construct reduces adhesion of both cells and circulating protein in animal models. Chronic inflammation and fibrosis or capsule formation have also shown variations in response to biomaterial size, surface chemistry, and topography,53,54 although these outcomes have yet to be fully elucidated with the introduction of cellularized constructs. In vitro characterization studies have demonstrated increased concentrations of IL-1β, tumor necrosis factor-α (TNF-α), interferon-γ, and IL-10 when MSC PEG-hyaluronic acid hydrogels were cocultured with differentiating macrophages.27,28 Phenotypic expression indicated an alternative or anti-inflammatory activation. The combination of functional cells encapsulated within a biomaterial construct offers yet another layer of complexity in the foreign body or inflammatory response calling to question cell viability, directed or spontaneous differentiation, or further self-renewal. Nevertheless, in vitro and animal studies show promise and clinical trials are not far off.33,55,56
Conclusions
The future of nanoengineered constructs holds promise in all aspects of medicine from preclinical high-throughput screening to targeted diagnostic–therapeutic modalities to complex tissue replacement. However, the road from bench research to translational studies that provide proof-of-principles for clinical utilization for engineering constructs is challenging. In vivo tissue healing is an orchestrated process dependent on the interactions of many different cells. The end result is affected by a wide range of factors and is not always perfect. For this reason, the combination of biomaterials with stem cells, especially MSCs, is a promising avenue to direct optimal tissue regeneration. This can be achieved by potentially harnessing the anti-inflammatory response to implantable constructs. Advanced understanding of the biology of MSCs during development of homeostasis and in the response to injury is critical. Such knowledge can be applied to studies designed to modulate interactions between biomaterials and host immune cells such that optimal structure and function can be regained and the best clinical outcomes achieved.
Footnotes
Disclosure Statement
The authors have no financial disclosures or conflicts of interest.