
Abstract
In this study, the potential of a chitosan-agarose-gelatin (CAG) cryogel scaffold for the repair of subchondral cartilage defects was explored in female New Zealand white rabbits. Custom-made CAG cryogel scaffold was implanted in a surgically created subchondral defect (diameter of 4 mm, depth of 4 mm) in knee joint of rabbit. The repair of the subchondral defect was evaluated at regular time interval by both macroscopic as well as microscopic examinations. The gross evaluation of the scaffold-implanted site showed integration of the scaffold with the surrounding tissue. Scanning electron microscopy and histological staining of the remnants of implanted cryogel scaffold showed infiltration of the host cells. The repair of the subchondral defect along with well-integrated regenerated cartilage was confirmed by the histology analysis of the joint. Results showed significant cartilage regeneration by the fourth week until eighth week after implantation. Immunohistochemical analysis confirmed that regenerated tissue is hyaline cartilage and absence of hypertrophy marker was reported. In addition, the CAG scaffolds did not elicit any adverse immunological rejection as shown by hematological analysis. Enzyme-linked immunosorbent assay did not show any statistically significant change in the concentration of tumor necrosis factor-α in the serum, and remained in a nontoxic range. Rabbits with a surgically created defect but no scaffold did not show any cartilage regeneration throughout the experiment of 8 weeks. These results demonstrate that CAG cryogel scaffolds promote repair of an osteochondral defect at a load-bearing site in rabbits.
Introduction
A
Considering the limitations of the existing methods, tissue engineering has emerged as a potential future approach for the repair of such defects. Different studies on engineered cartilage tissues have effectively mimicked the functional properties of native hyaline cartilage.17–19 Three-dimensional scaffolds constitute an important component of tissue engineering approach. They act as a substrate to promote repair of articular cartilage.20,21 Both natural and synthetic materials have been used for the fabrication of such scaffolds. Most of these constructed scaffolds have focused on the use of a single polymeric material and include collagen, alginate, and so on. Such scaffolds seeded with chondrocytes or MSCs have been widely used in osteochondral defect experiments.21–23 Recent development involves biphasic scaffolds. Such hybrid scaffolds have shown promising results both in in vitro and in vivo studies. Hybrid scaffolds of hyaluronan and calcium phosphate ceramic, loaded with rat bone marrow MSCs, exhibited the formation of fibrocartilagenous tissue in the hyaluronic sponge and bone-like tissue was observed in the ceramic portion after 6 weeks of implantation in a rat model. 24 Double-layered collagen matrices have shown hyaline-like cartilage repair of articular defects when implanted for 6 months in rabbit model. On the other hand, biocomposite cryogels composed of polyvinyl alcohol, alginate, tetraethylorthosilicate, and calcium oxide have proved to be effective in repair of cranial defect in rat model. 25
In vitro studies have already described the potential of chitosan-agarose-gelatin (CAG) cryogel scaffolds for cartilage tissue engineering. These studies have indicated that CAG scaffolds support the growth and proliferation of primary goat chondrocytes together with the synthesis of large amount of extracellular matrix. 26 The results give an initial insight into the utility of CAG cryogel matrices for cartilage tissue engineering. CAG cryogel matrices also support the growth and proliferation of various other types of cells, like COS-7, NIH 3T3 (skin fibroblast cell line), C2C12, and HL-1 (myoblast and cardiomyocyte cell lines, respectively). 27 Thus, they can also be used for general tissue engineering applications. The aim of this study was to explore the efficacy of these scaffolds for the regeneration of subchondral cartilage defects in vivo using mature New Zealand white rabbit as an experimental model. Sterile custom-made cryogel scaffolds were implanted at the defect site developed surgically in the condyle of the left knee of rabbit and repair was monitored over known period of time.
Materials and Methods
Animals
All experimental procedures were conducted in accordance with Institute Animal Ethical Committee (IAEC) of Indian Institute of Toxicological Research (Reference number: ITRC/IAEC/01/2012). Female New Zealand white rabbits weighing ∼2–3 kg were used for the experiments. A total of 36 rabbits were used for the study. Prior to initiation of the study, rabbits were randomized and assigned to six different groups; each group was allotted with six animals. Out of six animals, three were used as control (with defect but no scaffold treatment) and three were used as test (defect treated with scaffold).
Fabrication of CAG scaffolds
CAG cryogel scaffolds, for implantation, were synthesized by following previously reported protocol. 26 Briefly, a polymer solution was prepared by dissolving chitosan (100 mg) in 5 mL of aqueous acetic acid solution (1%). After complete dissolution of chitosan, equal amount of gelatin (100 mg) was added to this solution; polymers were dissolved at room temperature using mechanical stirring. On the other hand, another polymer solution was prepared by dissolving 300 mg of agarose in boiling water (5 mL). This polymeric solution was cooled down to the temperature of around 50–55°C. Thereafter, both the polymeric solutions were mixed together. From 0.2% (v/v) glutaraldehyde stock, 0.5 mL was added to this polymeric mixture and mixed thoroughly. The solution mixture having dissolved polymers and crosslinker was poured into precooled syringes and incubated at −12°C for 16 h, resulting in the formation of an interconnected porous network. The synthesized cryogel scaffolds were thawed and washed using deionized water to remove the unreacted polymers and crosslinker. Scaffolds were further dried and stored for the future use.
Generation of surgical defect model and implantation of custom-made CAG cryogel scaffold at the defect site
Animals were divided in six groups according to the time of sacrifice. The first group was sacrificed after first week, second after third week, third after fourth week, fourth after fifth week, fifth after sixth, and sixth after eighth week of surgery. Rabbits were anesthetized by intramuscular injection of xylazine (8 mg/kg) and ketamine (40 mg/kg). The knee region was shaved and disinfected to avoid any postoperative infections. A medial parapatellar incision was made and the medial femoral condyle was exposed. A defect of ∼4-mm depth and 4-mm diameter (Fig. 1A) was created using surgical blades.5,28,29 In test animals, the defect area was treated by implanting a custom-made sterile cryogel scaffold (Fig. 1B), whereas in control animals, the defect was left untreated. The scaffold was fixed at the defect with the help of surgical glue. After the surgery, the knee joint capsule and skin were closed using resorbable surgical sutures. The rabbits were allowed to move freely postoperatively. To avoid the postoperative infections, antibiotic injections were given on alternate days. Further, to avoid the side effects of antibiotics, rabbits were supplied with vitamin B complex in their drinking water.

Hematological analysis and cytokine estimation in blood serum
To analyze adverse effects of the scaffold on the rabbits, its systemic toxicity was checked. Initially blood was collected before surgery; thereafter, blood was collected at third day after the implantation of scaffold. Final blood collection was done just before sacrifice by puncturing the ear vein of rabbits. Blood collected at different time intervals was analyzed for the cell count using automated blood analyzer. To further confirm any toxic effect of the scaffolds on the host, cytokine tumor necrosis factor-α (TNF-α) concentration in the blood serum was measured by enzyme-linked immunosorbent assay (ELISA) using a kit (Cusabio Biotech Co., Ltd.) as per instructions given by the manufacturer.
Analysis of cytotoxicity on host organs
To analyze any toxic effect of the implanted scaffold on the host vital organs, the rabbits were sacrificed by intracardial injection of thiopentone. After the sacrifice, tissues of all vital organs, like liver, lungs, spleen, and pancreas, were collected. Thereafter, tissues were fixed in 10% formalin saline for 72 h. After fixation, all tissues were processed in an automated tissue processor for dehydration and clearing. Tissues were then embedded in paraffin to form blocks. Sections of 5-μm thickness were cut from the blocks and were mounted on lysine-coated slides. These sections were then stained by hematoxylin and eosin (H&E) for the analysis of any inflammatory response elicited against the scaffold.
Histological evaluation of the defect area
On the day of sacrifice, animals were given an injection of thiopentone. Joints implanted with scaffold were removed from the rabbit with the help of a bone cutter and were further processed for the histological analysis. Joints were fixed by incubating them in 10% formalin saline for 72 h. After fixation, the bony area of the joints was decalcified by incubating them in 8% nitric acid for 20 days; the decalcification solution was changed after every 4 days. The joints were then trimmed to remove the extra bone. These trimmed joints of specific size were then washed in tap water for 7 h. For histological analysis, tissue was then processed in automated tissue processing machine. Tissues were dehydrated in gradient concentrations of ethanol (50%, 70%, and 90%) and finally to ensure the proper dehydration they were then treated with absolute ethanol for two times. The tissue was then cleared by incubating in xylene for two times. Thereafter, the tissues were incubated in paraffin wax for two times. The tissues were then embedded in paraffin and blocks for sectioning were made. Sections of 5-μm thickness were taken on lysine-coated slides. These were stained using H&E, safranin-O/fast green, and toluidine blue for the analysis of cartilage regeneration. Immunohistochemical staining was done using previously reported protocol, with some modification. 30 Antigen retrieval was done by heating sections in 10 mM Tris (pH 10). Thereafter, sections were enzymatically treated with 0.25% trypsin for 20 min. Blocking was done using 5% bovine serum albumin (w/v) dissolved in phosphate buffer saline containing 0.1% triton X-100 for 60 min. The monoclonal anti-collagen, type I antibody was used in dilution of 1:2000 and collagen type II antibody was used at a concentration of 2 μg/mL. The sections were incubated with horseradish peroxidase-labeled anti-mouse secondary antibody at a dilution of 1:250. A peroxidase substrate, 3,3′-diaminobenzidine, was used to develop signal. Histological evaluation was done by using a previously reported scoring system (Table 1). Native osteochondral tissue has a maximum score of 29 points.5,31
Scanning electron microscopy and histological analysis of the implanted scaffolds
Implanted cryogel scaffold remnants were removed from the joints after sacrificing the rabbits. Scaffolds were then fixed in 4% paraformaldehyde solution overnight. Thereafter, scaffolds were dehydrated by using increasing gradient of ethanol concentration 20%, 40%, 60%, 80%, and 100%. To remove any moisture content from the scaffolds, they were placed in a desiccator overnight. Dried scaffolds were then gold coated and were analyzed by scanning electron microscopy (SEM). The implanted scaffolds were histologically analyzed by H&E and 4′,6-diamidino-2-phenylindole staining.
Statistical analysis
Data from the hematological analysis, cytokine estimation (ELISA), and histological scoring were analyzed by unpaired t-test. All the results are represented as mean±standard deviation.
Results
Hematological analysis and cytokine estimation in blood serum
As is evident from the results (Table 2), there was no statistically significant increase in concentration of the inflammatory cells in the blood after scaffold implantation, in all the test groups (p>0.05). This indicates that the presence of the scaffold does not elicit any noteworthy immune response.
Interval of blood collection: initial indicates cell count before surgery, intermediate indicates cell count at third day after implantation of scaffold, and final indicates cell count just before sacrifice of the rabbit.
Systemic effect of the implanted scaffold was further evaluated by determining the levels of TNF-α in blood serum. The initial level of TNF-α ranges from 25.21 to 32.93 pg/mL within the defined groups (Fig. 2). The TNF-α level increases from 37.23 to 43.40 pg/mL after third day of implantation but was statistically not significant (p>0.05).
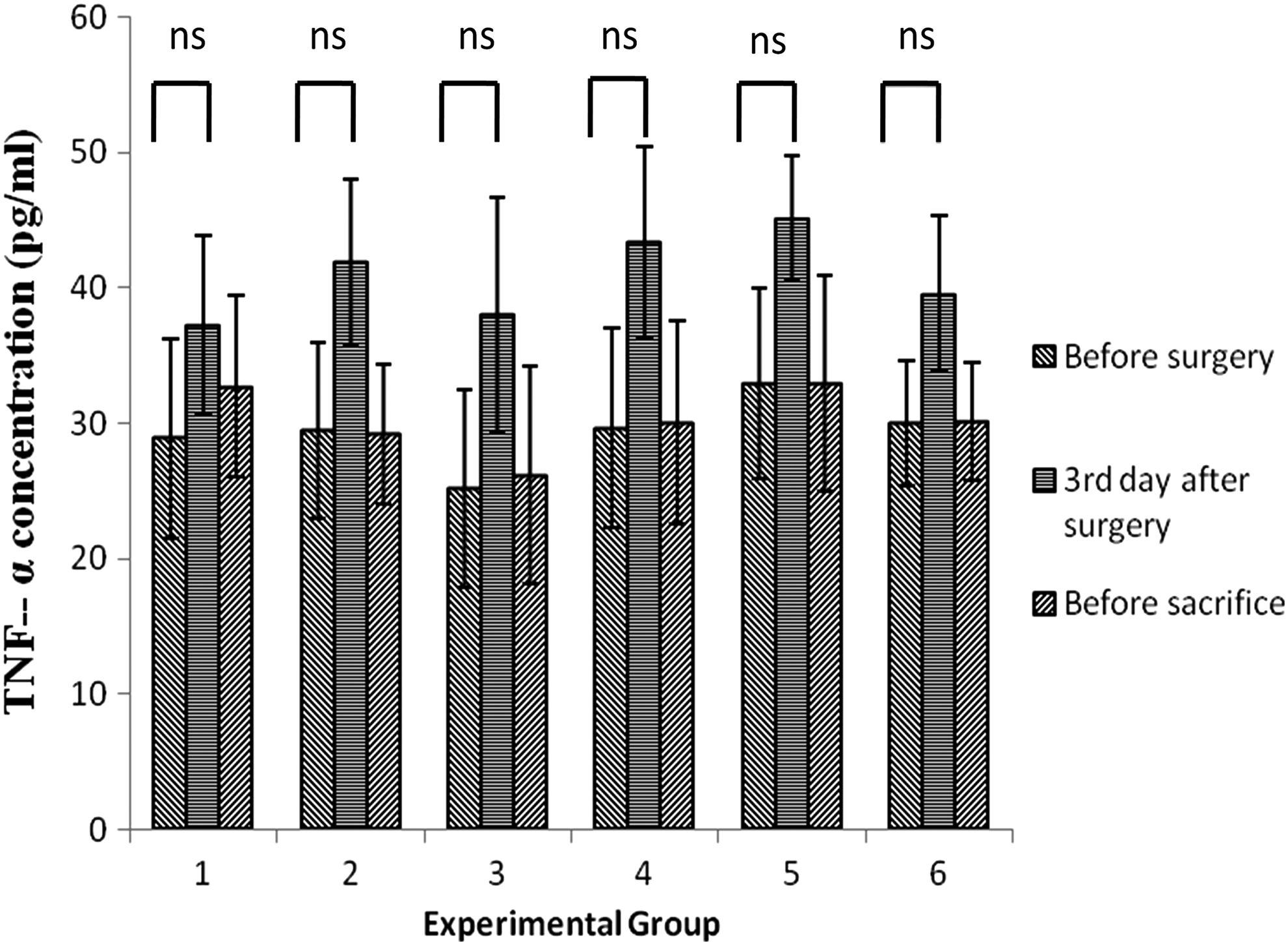
Level of tumor necrosis factor-α (TNF-α) in the blood serum of experimental animals after the implantation of CAG scaffolds at the joint cavity. Level of TNF-α was checked at three different intervals that gives an idea about the biocompatibility of the materials at the joint cavity. Experimental groups 1, 2, 3, 4, 5, and 6 represent rabbits sacrificed after 1, 3, 4, 5, 6, and 8 weeks of scaffold implantation, respectively. ns—not significant.
Analysis of cytotoxicity on host organs
In some cases tissue-engineered scaffolds may degrade and the resulting byproducts may prove to be toxic to the host system. Histological analysis of the vital organs does not show any adverse immune response (data not shown). Thus, it can be concluded that CAG scaffolds do not degrade into any toxic byproducts, and the degraded products formed are metabolized by the host system.
Macroscopic and histological evaluation of the defect area
Macroscopic observation revealed that the joints implanted with scaffold showed improvement in the repair of the defect site over the time period of 8 weeks (Fig. 3). The repaired tissue formed can be seen at the defect site in the rabbits treated with scaffold and was found to be well integrated with the adjacent native cartilage. After 8 weeks, the regenerated tissue at the scaffold-implanted site remodeled to a concave shape (Fig. 3D). In contrast, no sign of repair was evident at defect site in the control rabbit. Unhealed defect was still visible even after 8 weeks of surgery (Fig. 3E).
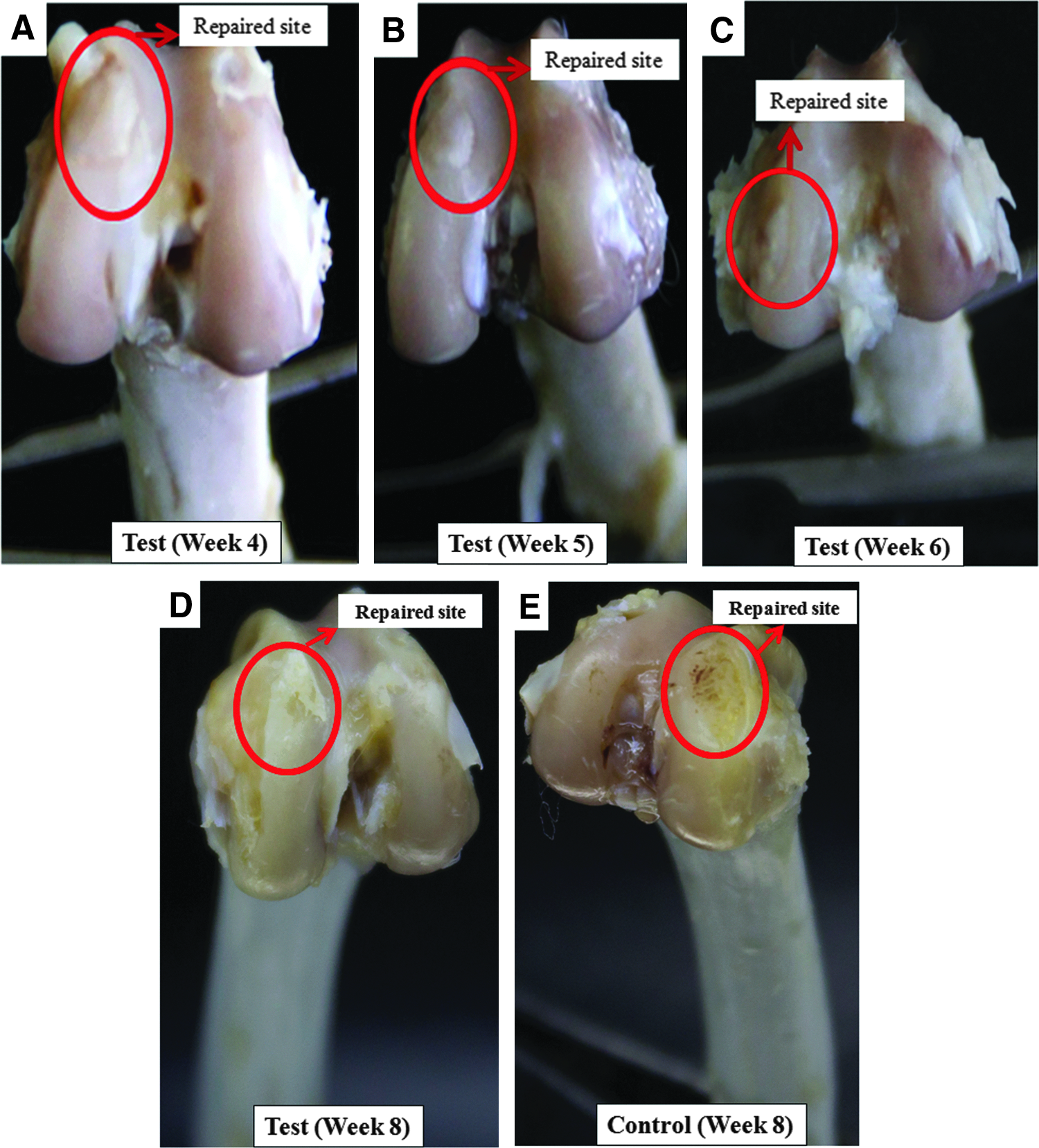
Digital images of samples harvested from rabbits treated with CAG scaffold showing cartilage repair after 4 weeks
The regeneration of cartilage was evaluated using H&E staining. Presence of proteoglycans in the regenerated tissue was displayed by safranin-O/fast green and toluidine blue stains. The histological analysis showed improvement in healing of the joint defect with time (Figs. 4 and 5). The architecture of a healthy cartilage is shown as a positive control (with no defect) in rabbits (Fig. 4A–C). At 1 week postsurgery, both test (defect treated with scaffold) as well as control (defect left untreated) did not show any sign of cartilage regeneration (Figs. 4E and 5B). Further, safranin-O/fast green and toluidine blue staining indicates absence of proteoglycans at the repaired site (Figs. 4D, F and 5A, C). At 3 weeks after surgery, still there was no sign of cartilage regeneration in both scaffold-treated and untreated defects (Figs. 4H and 5E). Presence of proteoglycans was also absent (Figs. 4G, I and 5D, F). Cartilage regeneration was not visible.
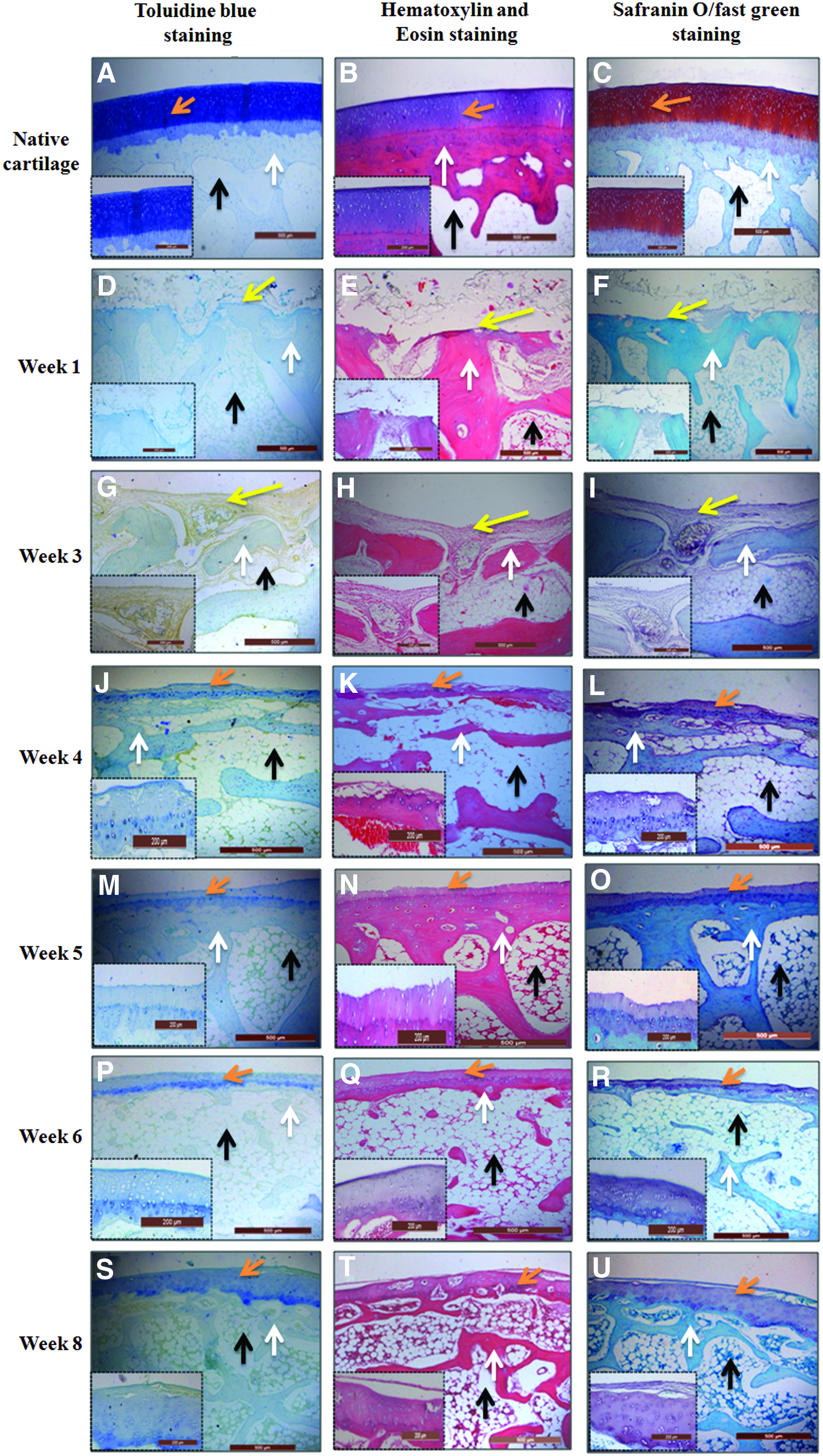
Histological analysis of the joint treated with CAG cryogel scaffold stained using toluidine blue, hematoxylin and eosin (H&E), and safranin O/fast green. Normal joint showing the presence of a completely healthy cartilage
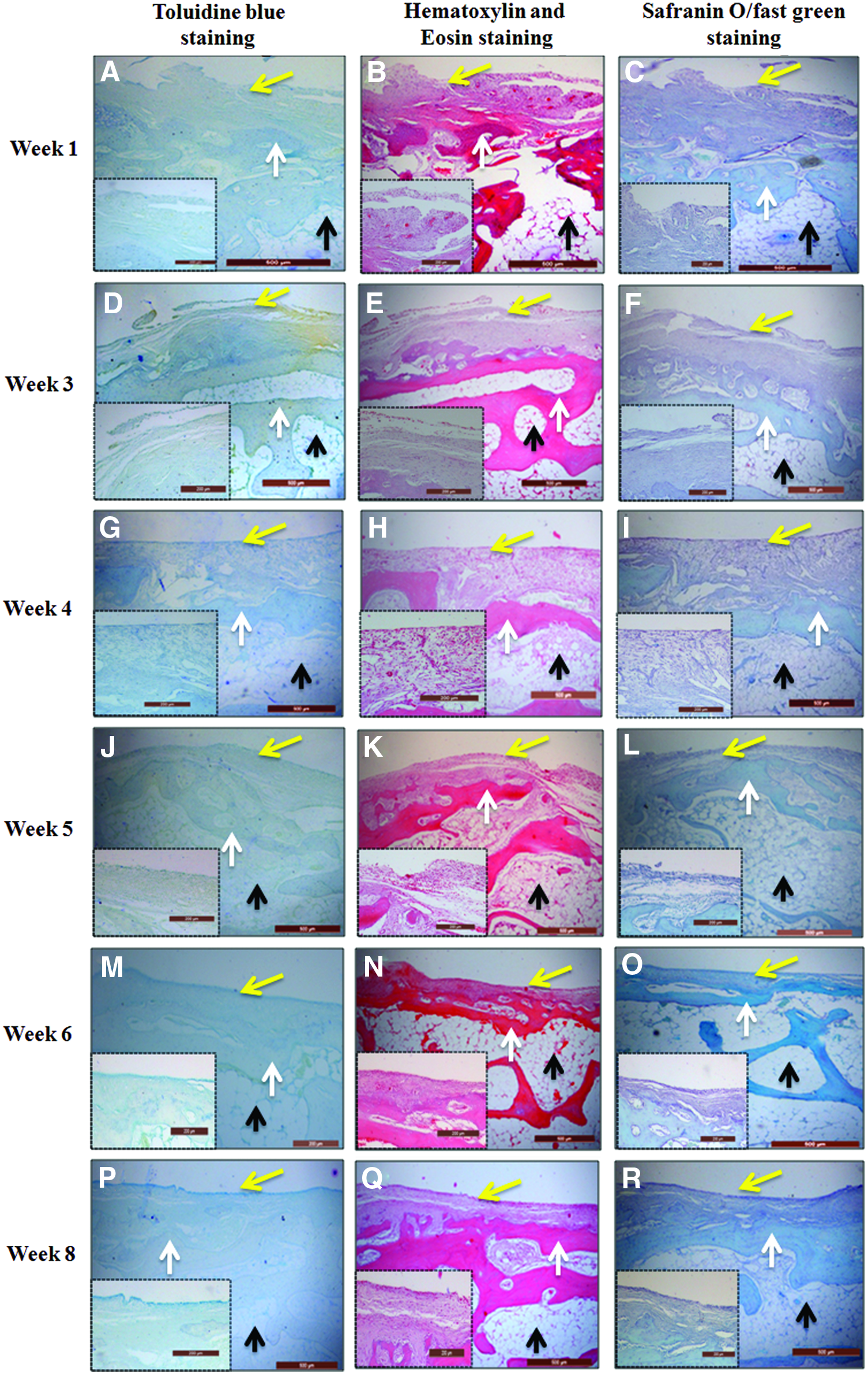
Histological analysis of the control joint left untreated and stained using toluidine blue, H&E, and safranin O/fast green. Repaired site after 1 week
After 4 weeks of surgery, cartilage regeneration was visible over the defect treated with CAG cryogel scaffold (Fig. 4K). Bone below the regenerated cartilage appeared much more organized than of the previous time points. The presence of proteoglycans in the regenerated tissue is indicated by the sections stained with safranin-O/fast green and toluidine blue (Fig. 4J, L). In contrast, in case of the control, where cartilage was subjected to spontaneous regeneration, no signs of cartilage regeneration or presence of proteoglycans were observed (Fig. 5G–I).
After 5 weeks of implantation, the cartilage regeneration enhanced significantly and the regenerated cartilage was much more organized compared with previous time points (Fig. 4N). The sections stained with safranin-O/fast green and toluidine blue stain were more intense than previous time points, indicating accumulation of proteoglycans in the regenerated tissue (Fig. 4M, O). At higher magnification (100×), the typical lacunae structure of hyaline cartilage can be observed in the regenerated area (Fig. 4M–O). On the other hand, in case of untreated animals, no signs of cartilage regeneration with absence of proteoglycans were observed even after 5 weeks of the surgery (Fig. 5J–L). Further, the results of histological analysis after 6 weeks (Fig. 4P–R) and 8 weeks (Fig. 4S–U) of surgery revealed that the process of repair gets better with time. The regenerated tissue has close resemblance with the native cartilage. The results of H&E staining showed that the tissue regenerated has chondrocytes arranged in lacunae structure as in native cartilage tissue (Fig. 4Q, T). This regenerated cartilage has abundance of cartilage matrix denoted by the more intense staining of safranin-O/fast green and toluidine blue (Fig. 4P, R, S, U). This increase in intensity denotes enhancement in accumulation of cartilage matrix. The matrix in the regenerated tissue is homogenously distributed. New bone formation is also evident at the subchondral defect site. The tissue regenerated is closely integrated with the native cartilage tissue and bone below it. However, defect without scaffold implantation showed no sign of cartilage regeneration even after 6 weeks (Fig. 5M–O) and 8 weeks (Fig. 5P–R) of surgery. These results indicate that CAG scaffolds play a significant role in cartilage repair. Immunohistochemical staining for collagen type II at the repaired site showed abundance of collagen II in the regenerated tissue (Fig. 6A). While, absence of collagen type I in the repaired site was observed (Fig. 6B). Thus, the regenerated tissue is hyaline as native cartilage. These results also corroborate with the results of macroscopic observations.

Immunohistochemical staining images of the repaired tissue after 8 weeks of CAG cryogel implantation. Stained for collagen type II
The histological scoring system was used to evaluate the healing of the defect site, and the score presented (Table 3) showed that at all time points throughout the experiment there was significant difference in the total scores (p<0.05) of the rabbits implanted with scaffold compared with control rabbits.
GAG, chitosan-agarose-gelatin.
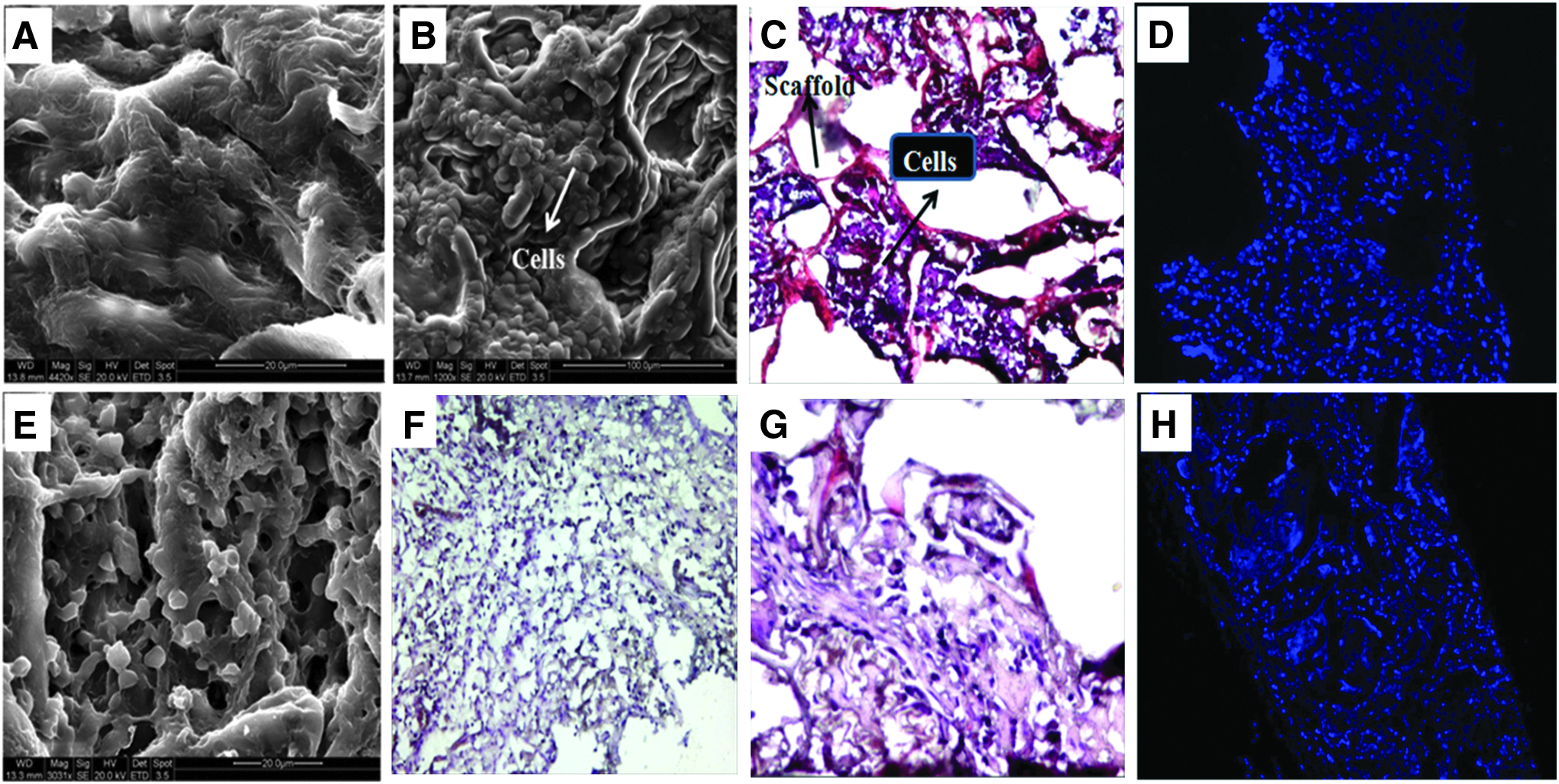
SEM and histological analysis of the implanted scaffold
Both SEM and histological analysis of the implanted scaffold were done after 6 weeks of the surgery (Fig. 7A–D). The results indicate that the implanted CAG scaffold is biocompatible at the implantation site and recruits cells from the surrounding host tissues. Similar results were obtained by the SEM and histological analysis of implanted scaffold 8 weeks postsurgery (Fig. 7E–H). It is assumed that the cells infiltrated into the scaffold were from bone marrow consisting mainly of host reparative cells along with some of the immunogenic cells, red blood cells, and so on. From these results it can further be concluded that CAG scaffolds allow the growth and penetration of the host cells from the surrounding host tissue without eliciting a rejection reaction on the rabbits. These results indicate that CAG scaffolds are biocompatible at the implantation site (joint cavity).
Discussion
By using tissue engineering approach, novel methods can be developed for the treatment of subchondral cartilage injuries. Using polymeric scaffold to deliver cells, like chondrocytes or MSCs, at the defect site is one of the most commonly used techniques for the cartilage treatment defect.5,32 However, studies in past have shown that addition of cells from outside may not be required for the treatment of cartilage defect. The poly(
In case of partial-thickness cartilage defect, the injury does not penetrate the subchondral plate. Thus, there is no access to the reparative cells. However, in the full-thickness cartilage defect, bone marrow reparative cells are easily accessed. These infiltrated bone marrow progenitor cells proliferate within the defect site.38,39 Therefore, scaffold to be used as an implant over these subchondral defect must have suitable physical and chemical properties to enhance the reparative response of these infiltrated progenitor cells. It should allow cells and their products to organize appropriately within the injured site.31,39 Cellular infiltration into the CAG scaffold was observed (Fig. 7). We assume that the supermacroporous cryogel scaffold allows the infiltration, proliferation, and differentiation of the mesenchymal progenitor cells from the bone marrow. Supermacroporous structure of the cryogel scaffold helps in overcoming a major problem of integration with the surrounding tissue.39,40 It facilitates integration with the surrounding native cartilage and subchondral bone tissue. Earlier studies done using scaffold composed of poly(
A material to be used as an implant should be biocompatible to the host and should not cause any damage to the host tissue. The hematological result showed that there was no significant increase in inflammatory cell count and presence of CAG cryogel scaffolds does not elicit any rejection reaction (Table 2). The in vivo biocompatibility of CAG scaffolds has already been proved. 26 The results of TNF-α estimation were similar to the hematological results and its level did not change significantly before and after the scaffold implantation (Fig. 2).
An ideal implant should degrade gradually so that its dissolution allows remodeling of tissue. 31 The CAG cryogel scaffold gets degraded with time. The cryogel scaffold implanted was visible macroscopically during the initial time period but during sectioning of the tissue it got detached, therefore not visible microscopically. The scaffolds may in some of the cases degrade into toxic byproducts that may enter the blood stream causing harmful effect to the other vital organs of the animal. Histological analysis of the vital organs revealed that no harmful inflammatory response was generated in the rabbits.
Histological finding revealed that the cartilage regeneration was observed in the scaffold-treated rabbits by 4 weeks of CAG cryogel scaffold implantation (Fig. 4). The regenerated cartilage that showed low extracellular matrix (ECM) content at the initial time points gets remodeled by the 8th week of implantation and attains maturation. Homogenous distribution of ECM can be seen at the repaired site. Presence of collagen type II in the regenerated cartilage confirmed that the regenerated cartilage is hyaline and not fibrocartilage (Fig. 6A). This was further confirmed by absence of collagen type I in the repaired tissue. The regenerated cartilage did not show expression of hypertrophy marker (Fig. 6B). In contrast, the control group rabbits did not reveal any kind of spontaneous healing. No sign of cartilage regeneration was seen throughout the study of 8 weeks (Fig. 5). Our future work focuses on modifying the scaffold in various ways, like seeding with allogenic chondrocytes or adding bioactive molecules, that can further enhance the repair process.
In conclusion, our previous in vitro studies have shown the potential of CAG cryogel as a scaffold for cartilage tissue engineering due to its improved mechanical strength and porous structure that allow cell infiltration and proliferation. 26 In this study CAG cryogel scaffolds have shown good potential for the treatment of subchondral defect in vivo. The cartilage regenerated had good integration with the subchondral bone and adjacent native cartilage. Additionally, the CAG cryogels were found to be biocompatible.
Footnotes
Acknowledgments
The authors would like to acknowledge Stiftelsen för bistånd åt rörelsehindrade i Skåne, Sweden, and Department of Biotechnology (DBT), Ministry of Science and Technology, Government of India for financial support. A.G. is thankful to IIT Kanpur for providing research fellowship. A.G. is also thankful to CSIR India and IIT Kanpur for providing travel grant to present this work in TERMIS-EU 2013, Istanbul, Turkey, in June 2013. A.K. would like to acknowledge DBT-Tata innovation fellowship award.
Disclosure Statement
No competing financial interests exist.