
Abstract
Cell-based regenerative therapies offer a new alternative approach to the treatment of chronic disease. Specifically, studies by our laboratory and others have shown that a subpopulation of cells derived from the bone marrow, known as early outgrowth cells (EOCs), are able to attenuate the progression of chronic kidney disease (CKD). In this study we examined the efficacy of a tissue engineering system, in which EOCs were embedded into submillimeter-sized collagen cylinders. These small individual units are referred to as modules and together form a functional microtissue. Due to their resemblance to endothelial cells, late outgrowth cells (LOCs) were used to coat the module surface, hypothesizing that as such they would promote vascularization and enhance engraftment of the encapsulated EOCs. These coated modules were transplanted subcutaneously into the subtotally nephrectomized rat model of CKD. While coated module therapy significantly improved both renal structure and function, noncoated modules with embedded EOCs were unable to reproduce these salutary effects on the kidney. Nevertheless, in both treatments, the embedded EOCs quickly degraded the modular environment and were seen to migrate to the liver, spleen, and bone marrow as early as 6 days after transplantation. With the efflux of EOCs, and unexpectedly no evidence of vascularization, we hypothesized that the LOCs did not enhance EOC engraftment, but rather augmented the renoprotection provided by EOCs by secretion of their own soluble and potent antifibrotic factors. To the best of our knowledge, this is the first study to document an effective subcutaneous approach for renoprotection.
Introduction
T
In contrast to this endocrine hypothesis, current therapeutic approaches to cell therapy are based on the paracrine mechanism of action that requires cells to be administered as close as possible to the site of injury. This invasive approach has been used in the heart where cells have been administered into coronary arteries or into the myocardium.5,6 While complications are relatively infrequent, a number of important concerns may limit the use of such an approach. First, the invasive nature of cell administration requires specialized imaging facilities and carries with it the risk entailed by invasive procedures. Second, administration of highly proliferative, relatively undifferentiated cells also carries a risk of neoplastic transformation.7–15 Indeed, the latter was highlighted in a recent case report 15 in which a patient with kidney disease who had received BMDCs, injected into the kidney parenchyma, subsequently presented with masses at the sites of injection and hematuria. Nephrectomy revealed the masses as angiomyeloproliferative lesions that were derived from the administered cells. To obviate the need for direct injection into the site of injury, we sought to explore modular tissue engineering and subcutaneous delivery as an alternative therapeutic modality.
A recent bottom-up approach to tissue engineering involves the fabrication of small collagen modules that allow for the encapsulation of cells. 16 As a consequence of collagen's strong cell adhesive properties, the surface of collagen modules can be seeded with endothelial cells (ECs) to enhance vascularization. 17 Previous reports in rats17,18 and SCID/bg mice 19 have demonstrated that this EC coverage leads to the formation of vessel-like structures, which can integrate into the host's vascular system. This vasculature is expected not only to ensure the adequate oxygenation of the cells within the tissue construct, but in this context to also facilitate the entry of the EOC-derived antifibrotic factors into the host's circulation.
While EC coating of modules enhances vascularization, their use is limited by the difficulties in preparing primary autologous EC cultures or the requirement for immunosuppressive treatment if allogeneic ECs are used. To provide a feasible alternative, we considered autologous/syngeneic bone marrow-derived endothelial-like cells. These cells are phenotypically and functionally similar to those of mature endothelium, arising after prolonged incubation of the circulating mononuclear cells from which EOCs are derived. After 14–21 days of cell culture, endothelial-like cells emerge as rapidly proliferating colonies 20 that, given their long period of cell culture, are commonly referred to as late outgrowth cells (LOCs). 21
We hypothesized that a collagen module that contained EOCs within and LOCs on its surface would have the advantage of: (1) enabling EOC secretions to easily permeate and enter the systemic circulation, (2) require a minimally invasive procedure of administration that would also permit their easy removal in the event of a rationale to terminate therapy (e.g., neoplastic transformation) and (3) maintain long-term viability as a consequence of LOC-facilitated vascularization. In this study, we investigate the renoprotective effects of EOC-containing modules, with or without LOC coverage, comparing these approaches with the intravenous injection of EOCs.
Materials and Methods
Cell isolation and culture
EOCs were cultured as previously described. 22 Briefly, bone marrow cells were flushed from the femora and tibiae of 3–4-week-old male Fischer 344 (F344) rats with sterile phosphate buffered saline (PBS). The collected cells were plated in differential EC culture medium (EGM-2; Lonza) on human fibronectin-coated tissue culture flasks and incubated at 37°C with 5% CO2 for 10 days to produce EOCs. The culture medium was changed every 2–3 days. To generate LOCs, bone marrow cells were plated at a 1:4 dilution and cultured as described above. After 2 weeks in culture, confluence was reached and the adherent cells were trypsinized and collected by centrifugation at 1400 rpm for 7 min. The supernatant was discarded, and the cell pellet was resuspended in EGM-2 and once again plated at a 1:4 dilution. After an additional 10 days in culture, cells reached confluence and were considered LOCs.
Cell characterization
EOCs and LOCs were detached from their flasks using trypsin or Accutase (Stemcell technologies), the latter being used exclusively for those cells immunostained with VE-cadherin. Afterward, 1×106 LOCs and 1×106 EOCs were transferred into individual 15-mL falcon tubes and centrifuged at 1400 rpm for 5 min. Each individual cell pellet was then suspended in 400 μL of BSA/PBS, followed by the addition of a specific antibody at 0.01 μg/μL. For the six cell surface markers assessed in this experiment, the following antibodies were tagged with specific fluorophores: CD34 (APC), VEGFR2 (V450), CD133, and VE-cadherin (PE), CD45 (PE/Cy7), and isolectin (FITC). Each sample was then incubated for 20 min at 4°C and individually subjected to flow cytometry with the MACSQuant analyzer (Miltenyi biotec). The percentage of fluorescently labeled cells was then determined using the MACSQuantify software (Miltenyi biotec).
Module fabrication
Acidified type-1 collagen (3.1 mg collagen/mL; Cohesion technologies) was mixed with 10× MEM (Invitrogen) and neutralized with 0.8 NaHCO3, as previously described. 23 Neutralized type-1 collagen with or without EOCs (Sigma) was then infused through a syringe pump (Razel Scientific Instruments, Inc.) into the side inlet of a custom-designed T-junction device through polysulfone Masterflex Tygon L/S 13 Lab tubing (Cole-Parmer Instrument Co.). 24 At the same time, compressed air (75.8 kPa) was directed into the upper inlet of the T-junction. With this apparatus, the compressed air meets the collagen fraction at the intersection region of the T-junction whereby the pressurized air generates collagen modules of ∼2 mm in length. The thus-formed collagen modules were then propelled from the T-junction's lower outlet into 3 m of gas-sterilized polyethylene tubing (PE60, 0.76 mm ID; Becton Dickinson and Company). The tubing was then removed from the T-junction outlet and placed within a humidified incubator for 1–2 h at 37°C and 5% CO2 to allow the collagen to gel. To recover modules, a 10-mL air-filled syringe was connected to the tubing by an 18G needle (Becton Dickinson) to expel the modules into a nontissue culture-treated dish containing EGM-2. Pseudoendothelialization of the module surface was performed as described previously with ECs. 17 Briefly, EOC-containing modules were incubated with 3–5×106 LOCs in a 15-mL falcon tube containing 5 mL of EGM-2 and gently rocked for 1 h to ensure maximal coverage. After rocking, the module suspension was transferred to a nontissue culture-treated dish and placed in a 37°C, 5% CO2 incubator for 24 h.
Viability assessment of module encapsulated EOCs
After 24 h of incubation, the culture medium was aspirated and modules underwent three washes with PBS until their final suspension in 1 mL of PBS. A Live/Dead kit (Life Technologies) was used to quantify the percentage of viable EOCs within the modules, whereby 1 μL calcein (live cells, excitation/emission: ∼495/∼515) and 2 μL of ethidium bromide (dead cells, excitation/emission: ∼530/∼615) were incubated with the module suspension for 30 min at 20°C. Modules were then washed three times with PBS and imaged using a Zeiss LSM510-META confocal microscope. Fifteen modules were randomly selected and quantified for the presence of both live (green fluorescence) and dead (red fluorescence) EOCs to calculate the proportion that were viable. The LOCs, used in the in vivo studies to facilitate vascularization, were not included in this in vitro component.
3H-proline incorporation
Antifibrotic activity was examined by quantifying the incorporation of [3H]-proline as an index of fibroblast collagen production. Following serum starvation, NRK-49F cells (ATCC), a renal fibroblastic cell line, were incubated with 0.5 mL of conditioned medium for 4 h. Unconditioned serum-free endothelial basal medium (EBM-2) served as a negative control. Fibroblasts were stimulated with transforming growth factor-β1 (TGF-β1) at a concentration of 20 ng/mL, and incubated with [3H]-proline (1 μCi/well, L-[2,3,4,5-3H]-proline; Amersham Biosciences) for 44 h, as an index of collagen production. Fibroblasts were harvested, washed four times with PBS, solubilized in 0.75 mL of 1 M NaOH and then neutralized with 0.5 mL 1 M HCl. The incorporation of exogenous [3H]-proline was measured using a liquid scintillation counter (LS 6000; Beckman Instruments, Inc.). 25
Subtotal nephrectomy animal model
The subtotally nephrectomized or remnant kidney rat provides a well-established model of CKD with close similarities to what is seen in humans. In brief, F344 rats (Charles River) of 12 weeks of age underwent one-step subtotal nephrectomy (SNX, n=49) or sham surgery (n=10), as previously described. 26 Briefly, animals were anesthetized with inhaled 2.5% isoflurane. The right kidney was removed through subcapsular nephrectomy and infarction of ∼2 thirds of the left kidney was achieved through selective ligation of two out of the three or four branches of the renal artery. Sham surgery consisted of laparotomy and manipulation of both kidneys before wound closure. All animal studies were approved by the St. Michael's Hospital Animal Ethics Committee.
Module and EOC injection
Four weeks after SNX surgery, urinary protein excretion was examined to ensure similar distributions of proteinuria among each group before the initiation of treatment. Based on these values, animals were randomly allocated into four groups: (1) modules containing 106 EOCs, (2) LOC-coated modules containing 106 EOCs, (3) cell-free modules, and (4) 106 EOCs in sterilized PBS. After 24 h of incubation, each plate of modules was washed three times with sterilized PBS to remove any culture medium residuum and suspended in 0.5 mL of PBS in a 1-mL syringe. Immediately afterward, modules were injected subcutaneously into the right hindquarter using an 18G needle. The intravenous administration of 1×106 EOCs in sterile PBS, prepared as previously described, 2 served as the positive control.
Kidney function
Before surgery and 4 and 8 weeks after it, animals were housed in metabolic cages to collect 24-h urine samples for subsequent determination of urine protein excretion using the benzethonium chloride method. Systolic blood pressure (SBP) was also measured at these time points in conscious rats using an occlusive tail-cuff plethysmograph attached to a pneumatic pulse transducer (Powerlab, ADInstruments) as previously described. 27 Before termination, glomerular filtration rate (GFR) was assessed using a modified FITC-inulin plasma clearance assay. 28 Briefly, 3.74 μL/g body weight of FITC-inulin was injected into the tail vein of each rat. Venous blood was then sampled at 3, 7, 10, 15, 35, and 55 min after receiving FITC-inulin. The concentration of this agent was then assayed by its fluorescence with a Spectramax M5e microplate reader (Molecular Devices) with 485 nm excitation and 527 nm emission settings. GFR was calculated using a two phase exponential decay curve and nonlinear regression method, as previously described 28 in which GFR=I/(A/α +B/β), where I is the amount of FITC-inulin injected, A and B are the y-intercept values for the two decay rates, and α and β are the decay constants for the distribution and elimination phases.
Histochemistry and immunohistochemistry
At the end of the study, 8 weeks postsurgery, animals were terminated. Kidneys were excised as was the subcutaneous tissue containing the modules. Tissues were immersion fixed in 10% neutral buffered formalin, embedded in paraffin or flash frozen in liquid nitrogen and embedded in cryostat matrix (Tissue-Tek; Sakura). Formalin-fixed kidneys were sectioned and stained with Periodic Acid Schiff (PAS) stain or examined immunohistochemically. Subcutaneous tissue containing modules were fixed in formalin, embedded in paraffin, and sectioned before staining with Masson's Trichrome and Hematoxylin and Eosin.
Glomerulosclerosis was assessed on PAS-stained sections using a semiquantitative technique in a masked fashion, as described previously. 26 The degree of of sclerosis was subjectively graded on a scale of 0–4: 0, normal; 1, sclerotic area of <25% (minimal); 2, sclerotic area of 25%–50% (moderately sclerotic); 3, sclerotic area of >50–75% (moderate to severely sclerotic); 4, sclerotic area of >75% (severely sclerotic). A glomerulosclerosis index was calculated for each animal by averaging scores from all the glomeruli in a kidney section, as also previously reported. 26
To visualize ECs in subcutaneous tissue, sections were immunostained with the mouse anti-rat monoclonal antibody CD31 (Abcam) whereas glomerular ECs were immunostained with the mouse anti-rat monoclonal Aminopeptidase P antibody JG-12 (Bender Medsystems). 27 Glomerular capillary density was expressed as the proportional area of JG-12 immunostaining in 30 randomly selected glomeruli from each rat and quantified using computer-assisted image analysis, as previously described. 27 Tubulointerstitial fibrosis was assessed by examining the accumulation of collagen type IV in the renal cortex, detected by immunostaining with a goat anti-rat type IV collagen polyclonal antibody (Southern Biotech), and quantified as the proportional area in 9 nonoverlapping 20× fields for each animal, using computer-assisted image analysis, as previously described. 29 All analyses were performed with prior masking of the identity of the study group from which the sections had been obtained.
CMTMR and CMFDA labeling and tracking
To determine the fate of EOCs and LOCs in vivo, cell tracking studies were performed. EOCs were firstly incubated with a 5 mM solution of 5-(and-6)-4- chloromethyl-benzoyl-amino-tetramethylrhodamine (CMTMR; Invitrogen) for 30 min. Immediately afterward these fluorescently labeled EOCs were encapsulated into collagen modules. LOCs were incubated with a 15 mM solution of 5-Chloromethylfluorescein Diacetate (CMFDA; Invitrogen) for 30 min and then used to coat the surface of the EOC-containing modules. These coated modules were then placed in a 37°C, 5% CO2 incubator for 24 h, and injected subcutaneously into the right hindquarter 4 weeks after surgery. Animals (n=3) were sacrificed 6 days after module injection. The presence of CMTMR and CMFDA-positive cells was determined on a Zeiss LSM510-META confocal microscope by counting their presence in 10 randomly selected fields in a 40 mm frozen section embedded in cryostat matrix. 30 Sections were counterstained with wheat germ agglutinin 488 (WGA 488; Invitrogen) to better visualize tissue architecture.
Statistical analysis
All data are shown as mean±SEM. A minimum number of three independent experiments were performed for all in vitro experiments, and analyzed by a one-way analysis of variance (ANOVA) with a post hoc Tukey's test. Differences between in vivo groups were analyzed by a one-way ANOVA with a post hoc Fischer's least significant difference (LSD) test. Accordingly, for histological experiments, we also used a one-way ANOVA with a post hoc LSD test, with the exception of the glomerulosclerosis index, which was analyzed using a Kruskal–Wallis with a post hoc Dunn's test. All statistics were performed using the GraphPad Prism 6.00 for Mac OS X (GraphPad Software). A change was considered statistically significant when p<0.05.
Results
Cell characterization of EOCs and LOCs
Bone marrow-derived cells exhibited an EOC phenotype after 7–10 days in culture. These EOCs formed colonies with cobblestone appearance at its center whereas cells at its periphery were spindle shaped. When subjected to FACS analysis, EOCs expressed both endothelial and hematopoietic markers (Table 1). After prolonged culture, the cells began to proliferate more rapidly, and achieved a confluent cobblestone appearance that is characteristic of LOCs.31,32 Whereas >90% of LOCs still expressed endothelial surface markers, they were less likely to express either CD133 or CD45 markers when compared with EOCs (Table 1).
EOCs, early outgrowth cells; LOCs, late outgrowth cells.
Cell viability and activity in vitro
Since the plan for in vivo experiments was to subcutaneously implant these modules 24 h after fabrication, we assessed the viability of EOCs in the uncoated module at this crucial time point. Using the Live/Dead assay, the viability of the encapsulated EOCs was >90%. Furthermore, EOCs that fluoresced red were uniformly distributed throughout the module (Fig. 1A), suggesting the absence of any diffusion constraints of either oxygen or nutrients to the core of the module.

In vitro assessment of EOCs embedded in uncoated modules.
We also examined the module's permeability to secreted antifibrotic factors. As previously demonstrated, 2 when treated with conditioned medium from EOCs (EOC-CM) a significant reduction in the extent of 3H-proline incorporation in fibroblasts stimulated with TGF-β was noted. The extent of collagen production was similarly attenuated when fibroblasts were treated with the conditioned medium generated from modules containing EOCs (Fig. 1B), confirming that the modules are, indeed, permeable to the antifibrotic factors produced by EOCs.
EOCs encapsulated in pseudoendothelialized modules preserve renal function
Untreated SNX animals develop heavy proteinuria, hypertension (SBP), and a substantial reduction in GFR (Supplementary Table S2; Supplementary Data are available online at www.liebertpub.com/tea). In accordance with earlier reports by our laboratory, this progression of kidney injury was diminished by intravascular EOC infusion. Similar preservation of GFR was noted in animals that had received LOC-coated, EOC-containing modules when compared with nontreated controls (Fig. 2), however, not to the same extent as sham-operated animals. Reduction in blood pressure was also evident as was the extent of proteinuria, although the latter fell short of our predefined level of statistical significance (Table 2, Supplementary Table S3). No significant benefit was noted in SNX rats treated with uncoated EOC containing modules with findings that were intermediate between empty and coated modules.
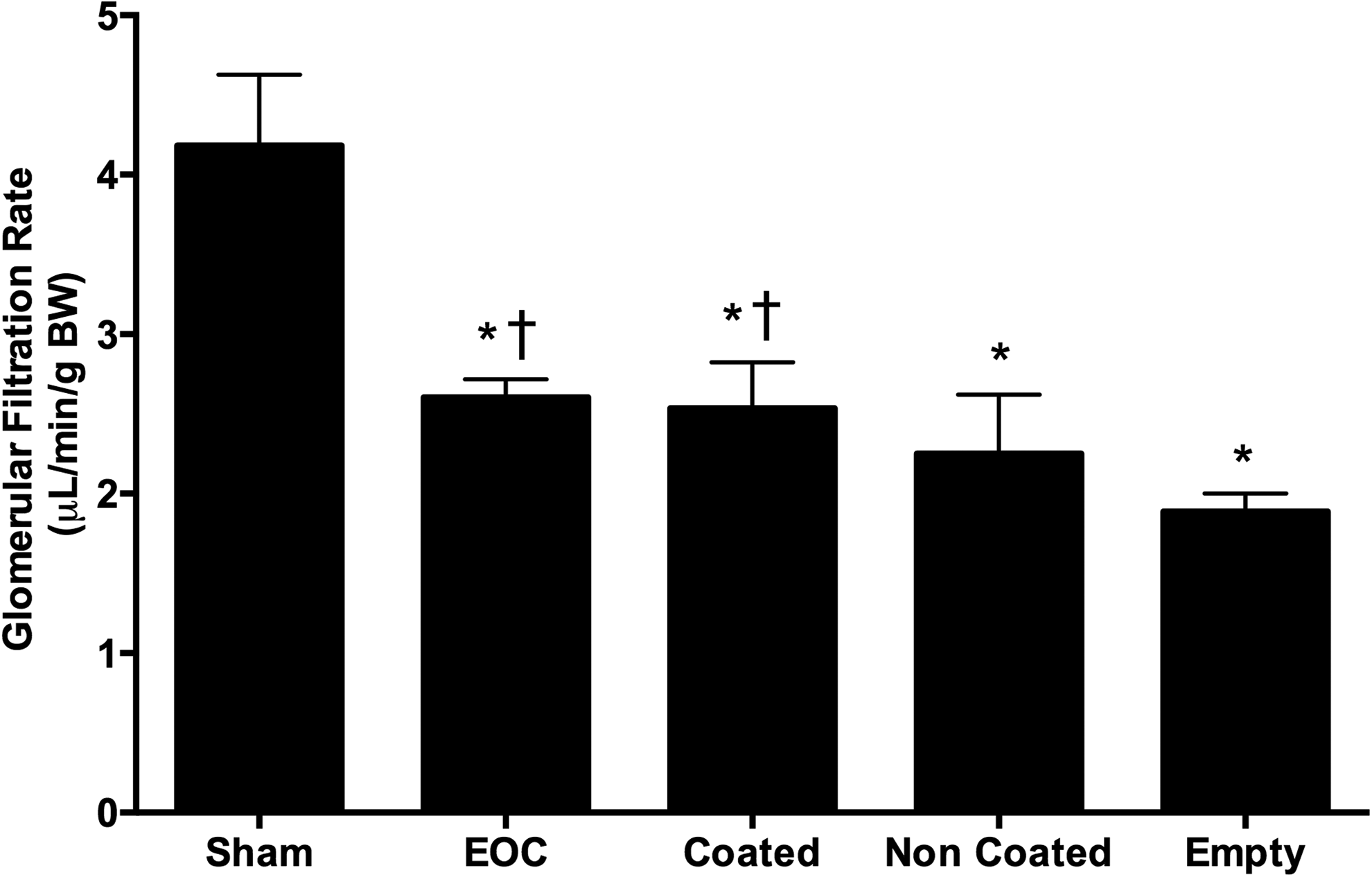
Glomerular filtrate rate in SNX rats at 8 weeks postsurgery. Rats underwent GFR measurement using a modified plasma inulin clearance assay. *p<0.05 versus sham animals, †p<0.05 versus empty module-treated animals. GFR, glomerular filtration rate. SNX, subtotal nephrectomy.
Urine protein excretion is presented as the geographic mean×/÷tolerance factors.
p<0.05 versus empty module-treated animals.
BP, blood pressure.
EOCs encapsulated in coated modules attenuate renal fibrosis and capillary rarefaction
When compared with sham-operated animals, SNX rat kidneys display widespread capillary loss along with extensive fibrosis in both the glomerulus (glomerulosclerosis) and the tubulointerstitium (tubulointerstitial fibrosis). As previously reported, the administration of EOCs attenuates the extent of capillary rarefaction, glomerulosclerosis and tubulointerstitial fibrosis in SNX rats. 2 Coated module therapy was similarly effective in ameliorating both fibrosis (Figs. 3 and 4) and capillary loss (Fig. 5) whereas uncoated EOC-containing modules were not.

Glomerulosclerosis in SNX rats at 8 weeks postsurgery. Kidney sections were stained with PAS to assess the degree of glomerulosclerosis.

Tubulointerstitial fibrosis in SNX rats at 8 weeks postsurgery. Kidney sections were immunolabeled with Collagen IV.
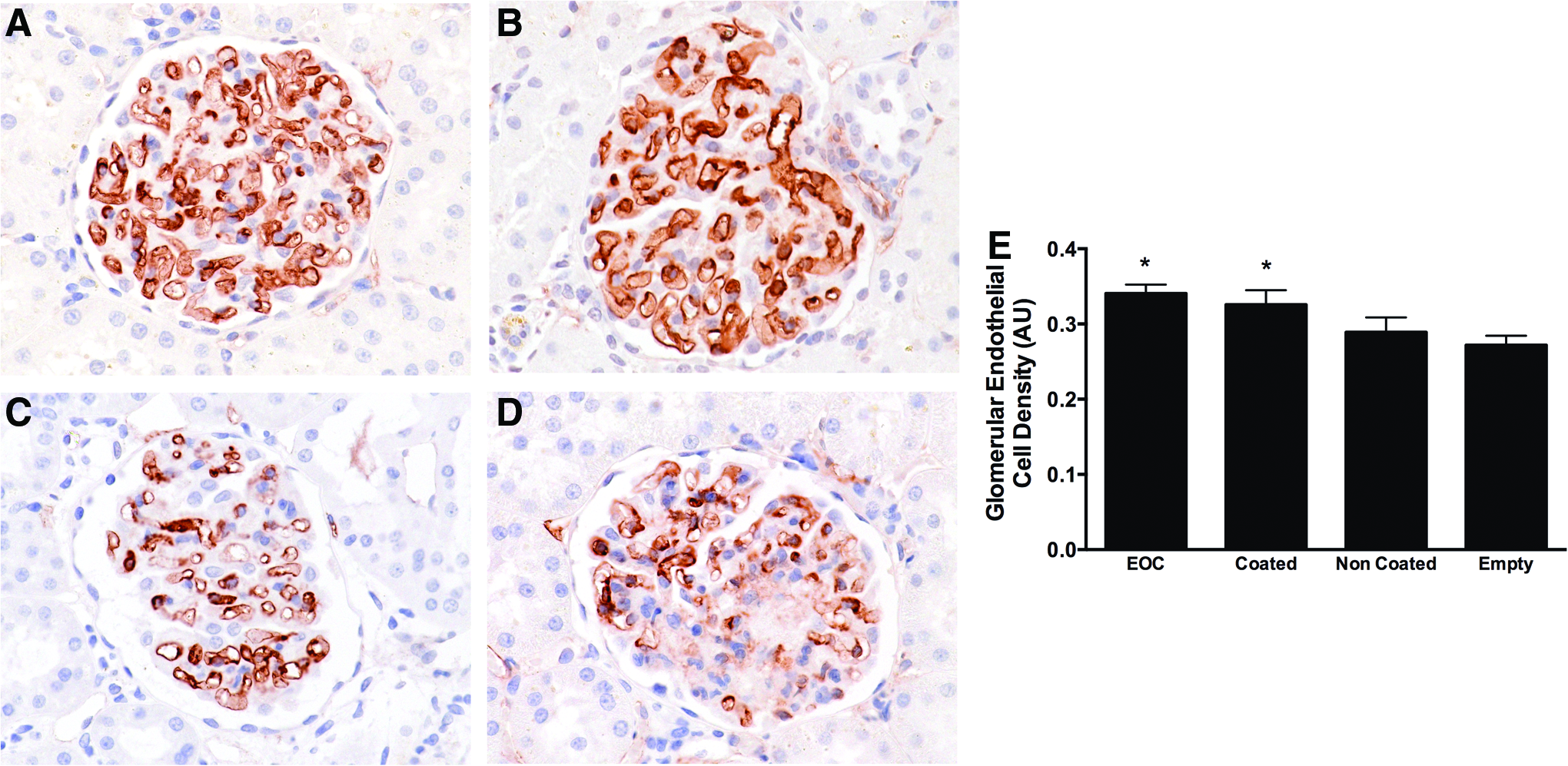
Glomerular capillary density in SNX rats at 8 weeks postsurgery. Kidney sections were immunolabeled with JG-12.
EOCs lead to module degradation and cell migration
Coated modular therapy was hypothesized to provide renoprotection by creating a vascularized niche for encapsulated EOCs. However, no augmented vascularization was observable at the site of module implantation. Indeed, neither modules nor the EOCs that they contained on implantation were visible by light microscopy. Instead, only scattered remnants of modules were observed at the sites of implantation (Fig. 6). In this study, the absence of an inflammatory infiltrate in the region where the cell-containing modules had been implanted, suggested that EOC-secreted collagenases may have been responsible for module degradation. 33
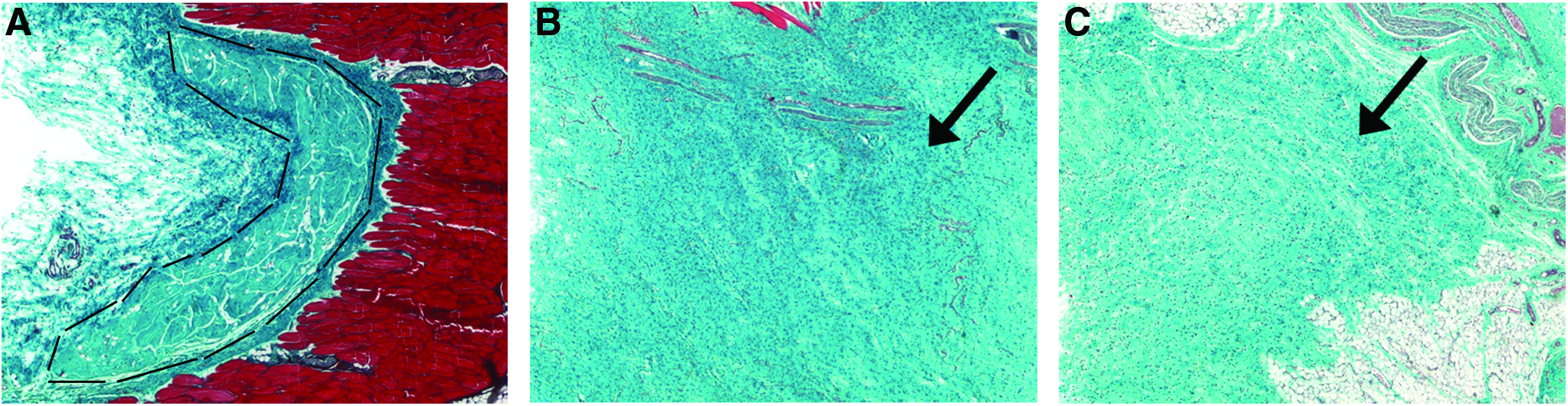
Module implantation site at 28 days post subcutaneous delivery. Module sections were stained with Masson's Trichrome, wherein collagen/connective tissue stains blue and muscle stains red.
Consistent with the degradation of modules, tracking studies revealed the absence of EOCs within the subcutaneous tissues in which the modules had been implanted. In contrast, labeled EOCs were abundantly present in the bone marrow, liver, and spleen, although less so than when the EOCs were injected intravenously (Fig. 7).
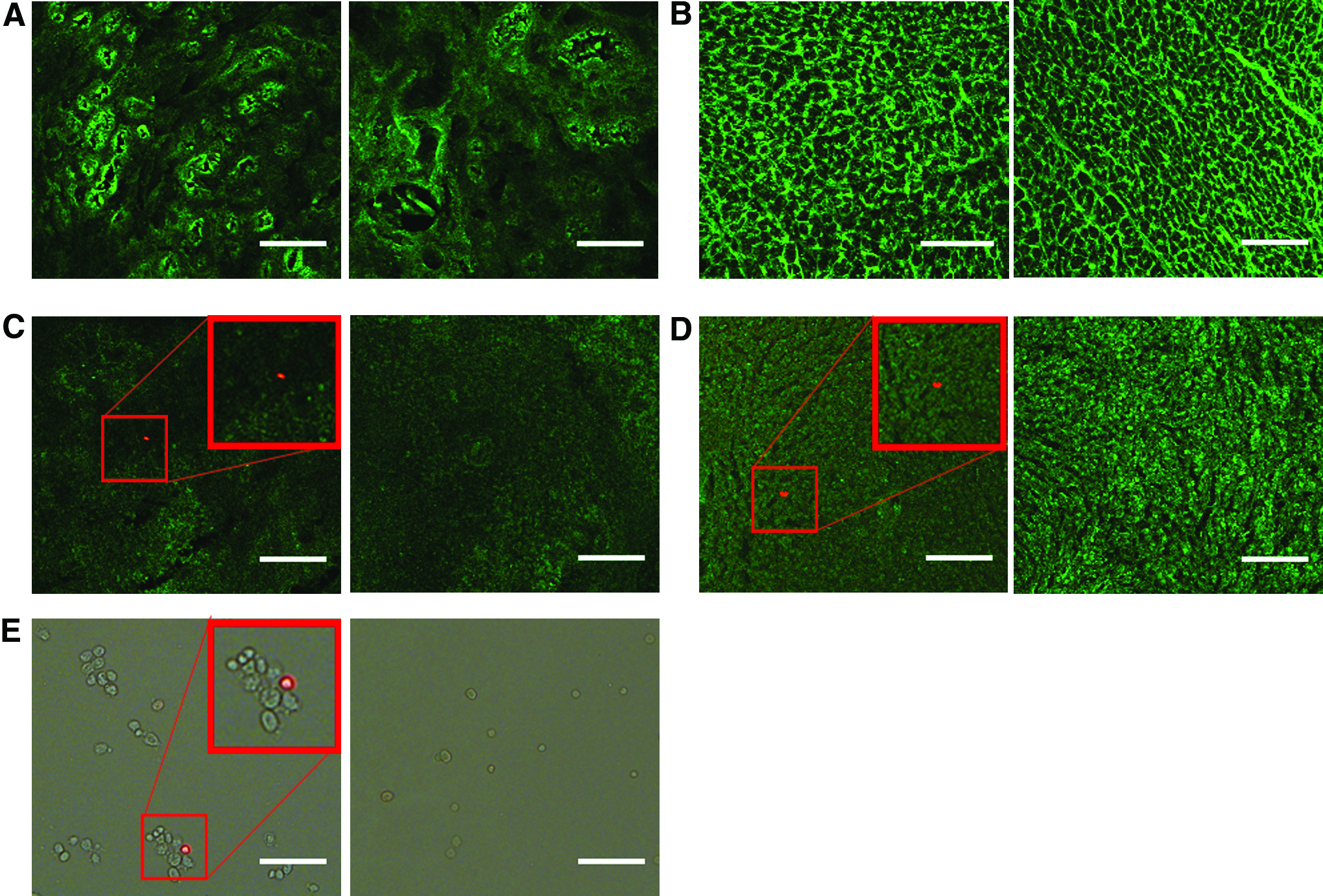
EOC tracking 6 days after subcutaneous module transplantation.
LOCs also demonstrate potent antifibrotic activity
In contrast to EOCs where tracking studies showed that they had vacated the modules, fluorescently labeled LOCs were notably still present on the module surface 6 days after transplantation. Despite the comparatively fewer labeled EOCs in the liver, spleen, and bone marrow of animals that had received coated modules when compared with those treated with intravenous EOCs, both groups showed similar attenuation in fibrosis and preservation of kidney function. Accordingly, we considered that while ostensibly EC-like, LOCs might also exert antifibrotic effects. Indeed, when conditioned medium from LOCs (LOC-CM) was subjected to the 3H-proline assay of fibrogenesis, it was found to be equally potent as EOC-CM in attenuating TGF-β-stimulated 3H-proline incorporation (Fig. 8).

In vitro LOC-CM 3H-proline incorporation assay. LOC-CM was diluted to 1:10,000 and cultured with TGF-β-stimulated fibroblasts. *p<0.001 versus control (no TGF-β, serum-free EBM-2 medium); †p<0.001 versus nontreated fibroblasts (TGF-β, serum-free EBM-2 medium). LOC-CM, conditioned medium from LOCs.
Discussion
In the present study, we explored modular tissue engineering with the aim of developing a clinically feasible approach to treating CKD. We hypothesized that vascularized subcutaneous modules would enable EOCs to remain viable in the long term while secreting their biologically active factors that would ultimately reach the systemic circulation. The present study showed that modular therapy did, indeed, reproduce the benefits seen with intravascular EOC infusion, doing so by subcutaneous delivery. Notably, only modules coated with LOCs were renoprotective, with noncoated modules yielding no significant differences in renal structure and function when compared with empty modules. The enhanced renoprotection seen with coated module therapy was originally hypothesized to be the result of module vascularization, given the similarities between LOCs and mature ECs. As such, they were expected to replicate the previously reported superior efficacy of modules coated with allogeneic ECs,17,18,34 but without the need for concomitant immunosuppression since cells were syngeneic. On histological examination, however, not only was there no evidence of vascularization, but only scattered remnants of the modules remained. Empty modules, on the other hand, remained intact.
A recent report by Gupta and Sefton 34 demonstrated that islet-encapsulated modules remain intact for at least 60 days after implantation, a considerably longer time than used in our study. Syngeneic islets were used to avoid an immune-mediated inflammatory response that may be harmful to the encapsulated islets or modular device. Specifically for the latter, proinflammatory cytokines, like tumor necrosis factor-α 35 and interleukin-10 36 have been shown to induce the expression of collagenases, which in turn have the potential to degrade these modular constructs. In our study, we also employed a syngeneic approach by isolating BMDCs from healthy, genetically identical donors. Accordingly, as expected, we found no evidence of inflammation at the site of module implantation. In light of these findings, we considered the possibility that rather than an inflammatory infiltrate, the EOCs were responsible for degrading their own modules. Indeed, previous studies have shown that EOCs secrete a range of matrix-degrading enzymes that include the collagenases, matrix metalloproteinases 2, 3, and 19, 33 that likely contributed to the degradation of the modules' collagenous meshwork and for the egress of the cells that they contain.
In light of the extensive module degradation, we speculated that the EOCs would migrate to the liver, spleen, and bone marrow to exert their renoprotective effects. This premise seemed conceivable given the migratory nature of BMDCs and the embryonic sites of extramedullary hematopoiesis within these organs. While the encapsulated EOCs did egress and migrate to the liver, spleen, and bone marrow, we did not observe these cells at nearly the same abundance as seen with intravascular EOC infusion. 2 While the precise mechanisms underlying the relative paucity of module-derived EOCs within these organs is unknown, we speculate that it may be a consequence of apoptosis, necrosis, or migration following the injection of modules into the relatively avascular subcutaneous tissue. As such, the decreased dosage of EOCs provides a plausible explanation for why noncoated module therapy offers intermediate, yet nonsignificant renoprotection. These findings led us to speculate that LOCs might also contribute to the antifibrotic effects of the coated modules.
Since LOCs are derived from the bone marrow-like EOCs, only cultured for longer, it seemed reasonable to hypothesize that LOCs may also secrete soluble antifibrotic factors capable of mediating renoprotection. Akin to the conditioned medium derived from EOCs, LOC-CM also potently reduced proline incorporation in renal fibroblasts. This finding suggests that the presence of LOCs on the surface of the module conferred an additional degree of antifibrotic activity rather than contributing to a vascular network for the modules. However, unlike EOCs that had almost all migrated to the liver, spleen, and bone marrow to exert their antifibrotic effect, LOCs seem more likely to have secreted such factors from within the vicinity of the module.
Unlike previous reports17,18,34 we did not use mature ECs for the endothelialization of the module surface. Instead we used syngeneic marrow-derived LOCs to prevent the need for immunosuppressive treatment. The difference between these LOCs and mature ECs offers a potential explanation for the minimal vascularization seen at site of transplantation. While LOCs strongly expressed endothelial markers, there was also concomitant expression of hematopoietic markers, although at lower levels, suggesting our marrow-derived LOCs are perhaps not fully functional ECs, but rather present a more progenitor-like phenotype. The poor vascularization could also be attributed to the fact that ECs are in constant contact with extracellular matrix proteins in vivo 37 and with the degradation of collagen these LOCs are left without a scaffold and are unable to properly function as endothelium. With its low antigenicity and strong cell adhesion properties, collagen is ideal for tissue engineering. However, its susceptibility to enzymatic degradation, as exemplified in this study suggests that other materials may be more suitable if they are to be used with EOCs. Indeed, alginate, a naturally occurring polysaccharide, might prove superior, after modification to enable LOC/EC attachment, given its previous use in cell encapsulation38,39 where it has been shown not to degrade in the presence of EOCs. 39 Alternative strategies, however, would include the continued use of collagen matrices that had been impregnated with collagenase inhibitors such as marimastat or the use of poloxamine/collagen interpenetrating networks. 40
In summary, this is the first study, to the best of our knowledge, to document an effective subcutaneous approach for renoprotection. Coated module therapy was successful in attenuating the functional and structural manifestations of CKD, with efficacy similar to intravascular EOC infusion.
Footnotes
Acknowledgments
The authors would like to thank Dr. Golam Kabir, Christine Kuliszewski, Jen Switzer, and Deborah Koh for their technical support of the animal studies. The authors would also like to express their gratitude to Chuen Lo and Dean Chamberlain for their technical assistance and guidance throughout the operation of these studies. The authors would like to acknowledge the financial support they received from the Canadian Institute of Health Research (CIHR) and the Heart and Stroke Foundation of Ontario. David Kepecs also acknowledges support from the Queen Elizabeth II/Heart and Stroke Foundation Graduate Scholarship in Science and Technology, as well as an Ontario Graduate Scholarship. Dr. Darren Yuen was previously supported by a KRESCENT postdoctoral fellowship, and currently holds the KRESCENT New Investigator and Canadian Diabetes Association Clinician Scientist Award. Dr. Richard Gilbert is the Canadian Research Chair in Diabetes Complications and this research was supported, in part, by the Canadian Research Chair Program.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.