
Abstract
Endogenous regeneration through cell homing provides an alternative approach for tissue regeneration, except cell transplantation, especially considering clinical translation. However, tooth root regeneration through cell homing remains a provocative approach in need of intensive study. Both platelet-rich fibrin (PRF) and treated dentin matrix (TDM) are warehouses of various growth factors, which can promote cell homing. We hypothesized that endogenous stem cells are able to sense biological cues from PRF membrane and TDM, and contribute to the regeneration of tooth root, including soft and hard periodontal tissues. Therefore, the biological effects of canine PRF and TDM on periodontal ligament stem cells (PDLSCs) and bone marrow mesenchymal stem cells (BMSCs) were evaluated respectively in vitro. Beagle dogs were used as orthotopic transplantation model. It was found that PRF significantly recruited and stimulated the proliferation of PDLSCs and BMSCs in vitro. Together, PRF and TDM induced cell differentiation by upregulating the mineralization-related gene expression of bone sialoprotein (BSP) and osteopotin (OPN) after 7 days coculture. In vivo, transplantation of autologous PRF and allogeneic TDM into fresh tooth extraction socket achieved successful root regeneration 3 months postsurgery, characterized by the regeneration of cementum and periodontal ligament (PDL)-like tissues with orientated fibers, indicative of functional restoration. The results suggest that tooth root connected to the alveolar bone by cementum–PDL complex can be regenerated through the implantation of PRF and TDM in a tooth socket microenvironment, probably by homing of BMSCs and PDLSCs. Furthermore, bioactive cues and inductive microenvironment are key factors for endogenous regeneration. This approach provides a tangible pathway toward clinical translation.
Introduction
R
It would be more advantageous to apply well-designed biofunctional scaffolds combined with growth factors to achieve in situ tissue regeneration without ex vivo cell culture and delivery. In situ tissue regeneration, also termed endogenous regeneration, aims to stimulate the body's own biologic resources and its reparative capability to repair or regenerate tissues by using a target-specific biomaterial system and/or bioactive cues to recruit endogenous stem cells or tissue-specific progenitor cells to the site of injury, 14 namely cell homing. 15 Cell homing offers an alternative approach to methods of tooth root regeneration/periodontal regeneration using cell transplantation, especially considering clinical translation. Recently, Kim et al. applied this principle to periodontal regeneration practice. 16 Nine weeks postsurgery, regeneration of a putative PDL at the interface between a rat incisor scaffold infused with cell homing factors and native alveolar bone were demonstrated. However, cell homing remains a provocative approach in need of experimental testing, especially in large animal models before clinical translation. Exploration of low price and the extensive source of bioactive factor reservoir and bioscaffolds should be taken into account to simplify and optimize the procedure. Furthermore, there is much further work to be done in elucidating the interaction between cells, bioactive cues, and microenvironment to effectively facilitate endogenous cell migration, differentiation, and regeneration of tissues.
Endogenous tooth root regeneration requires sequential release of multiple factors and a well-designed biofunctional scaffold that can support cell penetration and tissue ingrowth. Bioactive cues, such as growth factors, activate the body's own regenerative capability, induce the mobilization of tissue-specific host stem/progenitor cells and drive proliferation and even differentiation of these recruited cells into the targeted cell types to regenerate functional tissues. 17 Platelet-rich fibrin (PRF), developed by Choukroun et al. in 2001, 18 releases many growth factors such as platelet-derived growth factor, insulin-like growth factors-1, transforming growth factor-β, fibroblast growth factor-1, vascular endothelial growth factor, and epidermal growth factor for at least 1 week19–21 and promotes the recruitment, cell proliferation, and differentiation. The effects of PRF on periodontal regeneration have been proved by animal models 5 and human clinical applications.22,23 Scaffold biomaterials, served as structural substitutes of tooth root, should be designed to mimic, as closely as possible, a natural extracellular environment to influence cell behavior and control cell fate in vivo. Treated dentin matrix (TDM), which is regarded as a natural decellularization matrix scaffold, retains numerous bioactive molecules, including noncollagenous proteins and growth factors 24 that are essential for tooth root periodontal tissue formation. 25 Previous studies found that PDLSCs treated with dentin noncollagenous proteins presented several features of cementoblasts differentiation, and dentin matrix could induce cementogenesis and PDL formation from PDLSCs.25,26 Our previous studies indicated that TDM is a suitable scaffold and inductive microenvironment for tooth root regeneration,27,28 which could induce dental follicle stem cells to develop new cementum–periodontal complex. Furthermore, TDM shares similar structure and mechanical characteristics with dentin, and it is cost effective.
Overall, we hypothesized that endogenous stem cells are able to sense biological cues from PRF membrane and TDM in local microenvironment and contribute to the regeneration of periodontal tissues surrounding tooth root. As a part of our series of studies on tooth root regeneration,27,28 it aims to regenerate the tooth root with tooth–PDL–alveolar interfaces, by the combined use of PRF membrane and TDM through cell homing in canine orthotopic model. This is a requisite exploration, which may provide a tangible pathway toward clinical translation.
Materials and Methods
Animals model
This study was reviewed and approved by the committee guidelines of Sichuan University. Adult dogs (1–2 year-old males, 12–15 kg, Chengdu Dossy Biological Technology Company) were used in the present study.
Cell culture
Canine PDL was isolated from the extracted premolars. The PDL was minced and digested in a solution of 1% collagenase and 1% dispase (Sigma) for 40 min at 37°C. Both single cells and digested tissues were suspended in 3 mL complete α-MEM culture medium supplemented with 10% fetal bovine serum (FBS; Hyclone), 100 units/mL penicillin and 100 mg/mL streptomycin. They were seeded into a 25 cm2 plastic flask (Corning), and incubated at 37°C in 5% CO2 in a humidified atmosphere.
Canine bone marrow aspirate was collected from the iliac crest under general anesthesia with 3% sodium pentobarbital (1 mL/kg), and gradient centrifugation in Percoll was conducted to separate mononuclear cells, which were later plated in a 25 cm2 plastic flask (Corning). The culture medium consisted of α-MEM, 10% FBS, 100 units/mL penicillin and 100 mg/mL streptomycin. The cells were kept at 37°C with 5% CO2, and after 24 h the nonadherent cells were removed along with the culture medium.
When the cells reached 80–90% confluence, they were detached with 0.25% trypsin/EDTA (Gibco) and replated. PDLSCs and BMSCs of the third passage were used in this study.
Fabrication of canine TDM and PRF membrane
Dental crown, cementum, dental pulp, and predentin were mechanically removed. Then the dentin matrices were treated with 17% ethylene diamine tetraacetic acid (EDTA; Sigma) for 8 min, 10% EDTA for 8 min, 5% EDTA for 12 min. The following procedures were the same as previous protocols.27,29
Blood was taken from the canine lower limb vein and transferred into a 5 mL glass tube without anticoagulation. The tube was immediately centrifuged at 400 g for 10 min. Then PRF membrane was prepared according to a previously reported protocol. 30
PRF conditioned medium
BMSCs and PDLSCs were considered as effective cell sources for cell homing. To test the biological effects of PRF on BMSCs and PDLSCs, PRF-conditioned medium was prepared as described previously 31 with slight modifications. A PRF membrane derived from 5 mL of blood was placed in a tube with 4 mL sterile α-MEM containing penicillin (100 IU/mL) and streptomycin (100 μg/mL) for 24 h in a cell incubator. Then the membrane was transferred into a new tube of 4 mL sterile α-MEM and incubated for another 24 h. The PRF-conditioned medium was centrifuged at 3000 rpm for 5 min to remove the red blood cells when used.
Effect of PRF on cell migration
Twenty four-well plates of Transwell Filter Inserts (Corning) containing polycarbonate membranes with pore sizes of 8 μm were used. The PRF-conditioned medium was added to the lower chamber, and 1×105 cells were seeded into the upper chamber. Cells cultured in α-MEM containing 10% FBS served as positive control, and α-MEM containing 0.1% FBS as negative control. The cells were incubated at 37°C with 5% CO2 for 24 h. 32 After removal of nonmigrated cells on top of the filter, cells that had migrated through the membrane were fixed in 4% paraformaldehyde, stained with Giemsa, and counted randomly in 6 microscope fields at high-power magnification (×400). The experiment was performed three times and each time in triplicate.
Effect of PRF on cell proliferation
The effect of PRF on proliferation of BMSCs and PDLSCs were measured using the cell counting kit-8 (CCK-8; Dojindo). BMSCs and PDLSCs were seeded into 96-well plates at about 2×103 cells per well, respectively, and cultured with the PRF-conditioned medium. At each experimental time, cell culture medium was discarded, and 110 μL fresh culture medium containing 10 μL CCK-8 solution was added to each well. Cells were incubated at 37°C for 2 h, and the absorbance was finally detected at 450 nm using a spectrophotometer (Thermo Varioskan Flash; Thermo). Three parallel replicates were prepared. Cells cultured in α-MEM containing 10% FBS served as positive control, and α-MEM containing 0.1% FBS as negative control. The testing lasted for 6 continuous days.
Effect of PRF/TDM on cell differentiation
Six-well plates of Transwell Filter Inserts (Corning) containing polyester (PET) membranes with pore sizes of 0.4 μm were used. Since the narrow space between the upper and lower chambers cannot accommodate PRF membrane and TDM, we placed one PRF membrane and one TDM fabricated with a canine tooth root together into the upper chamber, and 3×104 cells were seeded into the lower chamber. The cells were incubated at 37°C in air with 5% CO2 for 7 days. Total cellular RNA was extracted by using a reagent (Invitrogen) to evaluate the gene expression of bone sialoprotein (BSP), osteocalcin (OCN), osteopotin (OPN), and collagen III (Col-III) using the quantitative Real-Time Polymerase Chain Reaction Kit (qRT-PCR; Takara). The primer sequences for BSP, OCN, OPN, Col-III, and 18S rRNA (Sango Biotech) are listed in Table 1. Relative gene expression levels were calculated using the 2−ΔΔCT method. 33 The experiment was repeated three times.
BSP, bone sialoprotein; OCN, osteocalcin; OPN, osteopontin; Col-III, collagen III; 18S rRNA, 18S ribosomal RNA.
In situ tooth root regeneration
The schematics for the tooth root regeneration strategy in animal models are shown in Figure 1. Canine bilateral third and fourth mandibular premolars were carefully extracted after anesthesia. The sockets were washed with saline water and the blood clots were removed, although the walls of the sockets were never scraped. Animals were randomly divided into four groups. For group I, allogeneic TDM was wrapped with PRF membrane prepared from autologous vein blood and placed into an alveolar socket. The surgical procedures of the following groups were identical as group I, except for little differences. For group II, TDM were treated with autoclave sterilization. For group III, PRF membranes were not involved. For group IV, the root-shaped implant socket was generated 3 months after tooth extraction. The gingiva was closely sutured after surgery. The animals were maintained on a soft diet for 1 week and antibiotics for 3 days postsurgery.
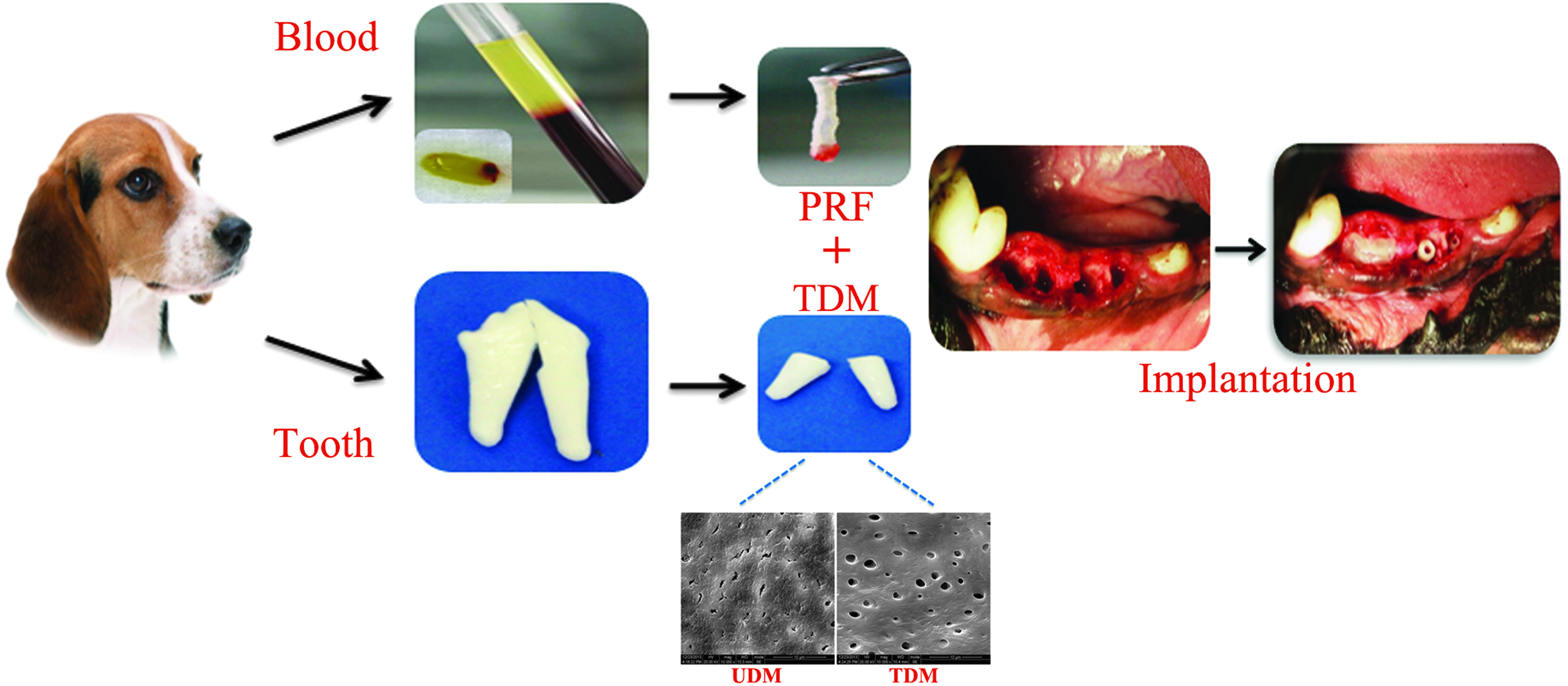
The schematics for tooth root regeneration strategy in animal models. Treated dentin matrix (TDM)/untreated dentin matrix (UDM) with or without platelet-rich fibrin (PRF) were transplanted into fresh premolar alveolar socket after tooth extraction or 3-month after tooth extraction according to different groups to evaluate the regeneration of tooth root regeneration. Scanning electron microscopy (SEM) examination of TDM and UDM showed that the dentinal tubules were exposed sufficiently and fiber bundles of intertubular and peritubular dentin became loose in TDM, but these morphological features were not found in UDM. (Scale bar=10 μm). Color images available online at www.liebertpub.com/tea
Sample harvesting and histological analysis
All dogs were sacrificed 3 months postimplantation. The mandible containing the experimental teeth were sawed and placed in 4% paraformaldehyde at 4°C for 7 days. The micro computed tomography (CT) scanner (Inveon CT, Siemens AG) was used to determine the changes of the TDM and alveolar bone. Then samples were demineralized and embedded in paraffin, followed by the section parallel to the long axis of the teeth at 5 μm for hematoxylin and eosin (H&E) stain, and Masson's trichrome staining was performed on the sections according to the manufacturer's protocol.
Statistical analysis
All in vitro data were expressed as the means±standard deviation by t-test. Statistical significance was analyzed using the SPSS 11.5 software (SPSS). A value of p<0.05 was considered statistically significant.
Results
Characteristics of canine TDM and PRF membrane
General observations of TDM and PRF are shown in Figure 1. Scanning electron microscope (SEM) demonstrated that the dentinal tubules were sufficiently exposed after being treated with EDTA. Whereas that of the untreated dentin matrix were slightly exposed. This surface feature of TDM is beneficial for the release of growth factors and dental hard tissue formation.27,29 The structure of PRF has been well demonstrated previously,5,34 therefore, the evaluation was not involved in the present study.
PRF promotes cell migration and proliferation in vitro
After 24 h culture, PRF exerted similar effect on cell migration with the positive control. PRF enhanced cell migration with more than two-fold increase in BMSCs and PDLSCs compared with the negative control (Fig. 2). The difference was statistically significant (p<0.0001). PRF presented similar effect on cell proliferation compared with the positive control over 6 days. Both of the two groups presented significant promotion of cell proliferation compared with the negative control (Fig. 3A).
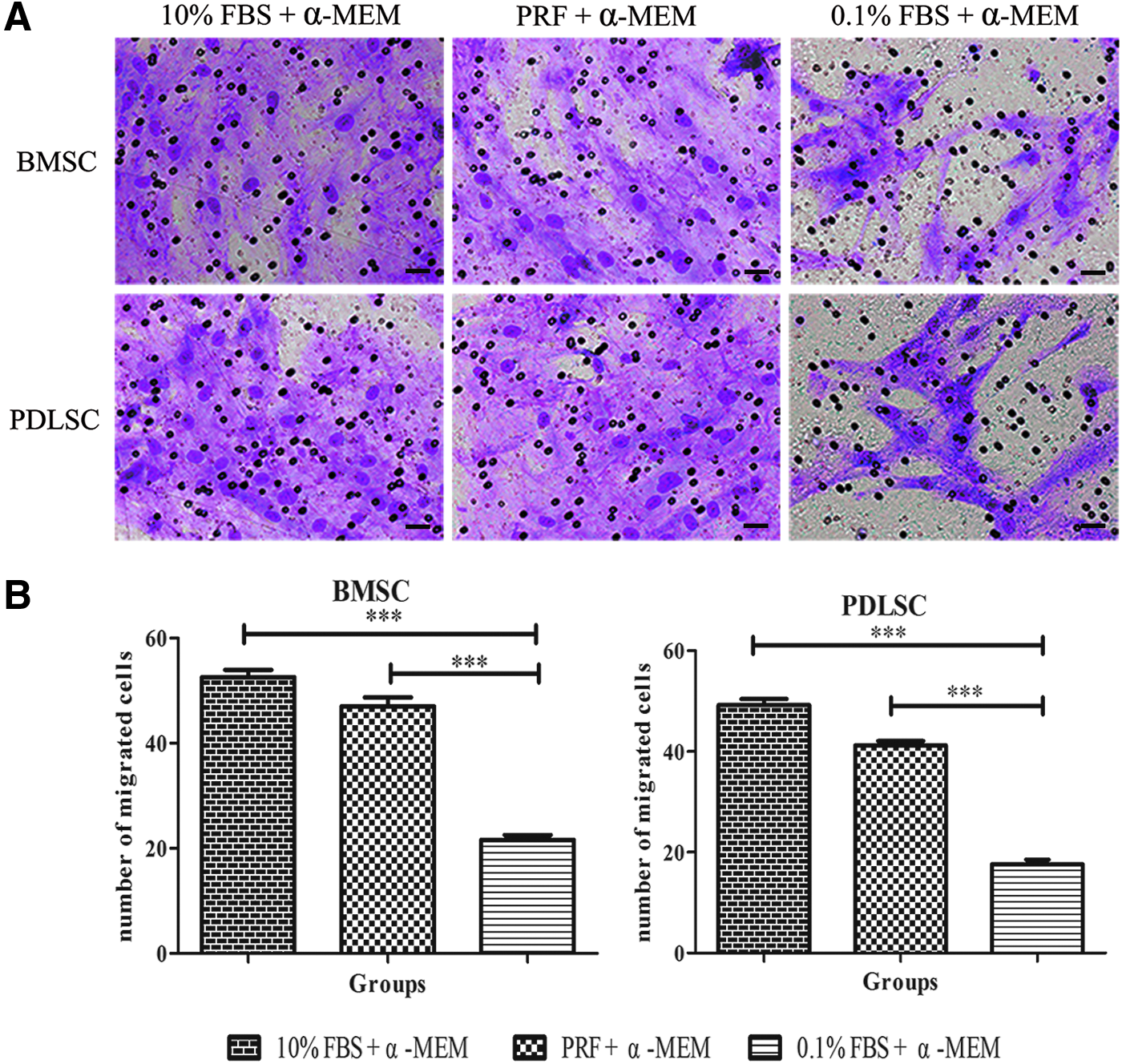
The effects of platelet-rich fibrin (PRF) on migration of bone marrow mesenchymal stem cells (BMSCs) and periodontal ligament stem cells (PDLSCs) were evaluated by Transwell after 24 h of coculture. PRF significantly promoted the migration of both BMSCs and PDLSCs.

PRF and TDM induces cell differentiation in vitro
Compared with the control group, PRF/TDM caused significant increase of the mRNA expressions of mineralization-related genes of BSP and OPN for BMSCs and BSP, OPN, and OCN for PDLSCs after 7-day incubation. The difference was statistically significant (Fig. 3B). There was no significant difference in the expression level of Col-III between the control group and test group.
Cementum–PDL complex can be regenerated through the implantation of PRF and TDM
For group I and group II, micro CT revealed that TDM was kept intact and a clear space was found between the TDM surface and the surrounding alveolar bone (Fig. 4A, B). For group III and group IV, however, TDM integrated with the surrounding alveolar bone and no space was found between them (Fig. 4C, D).

Mirco computed tomography (CT) evaluation of implanted tooth roots. Micro CT revealed that TDM kept intact in the alveolar socket and a clear space was found between the TDM surface and the surrounding alveolar bone in groups I
Three months after transplantation, the experiment design discrepancies between the four distinct groups led to different morphological patterns of tissue healing (Fig. 5). In group I and group II, hard tissues were deposited on the TDM surface. Putative PDL with parallel oriented fibers formed, connecting the hard tissue to the alveolar bone (Fig. 6A–D). In group III and group IV, the potential PDL space disappeared and TDM integrated with the surrounding bone. Active replacement resorption with deep and large resorption cavities and bone deposition upon the TDM surface were observed (Fig. 6E–H). The soft–hard tissue interface was not restored.

Panoramic images of HE staining showed representative healing patterns in different groups. Hard tissues were deposited and soft connective tissues formed in group I
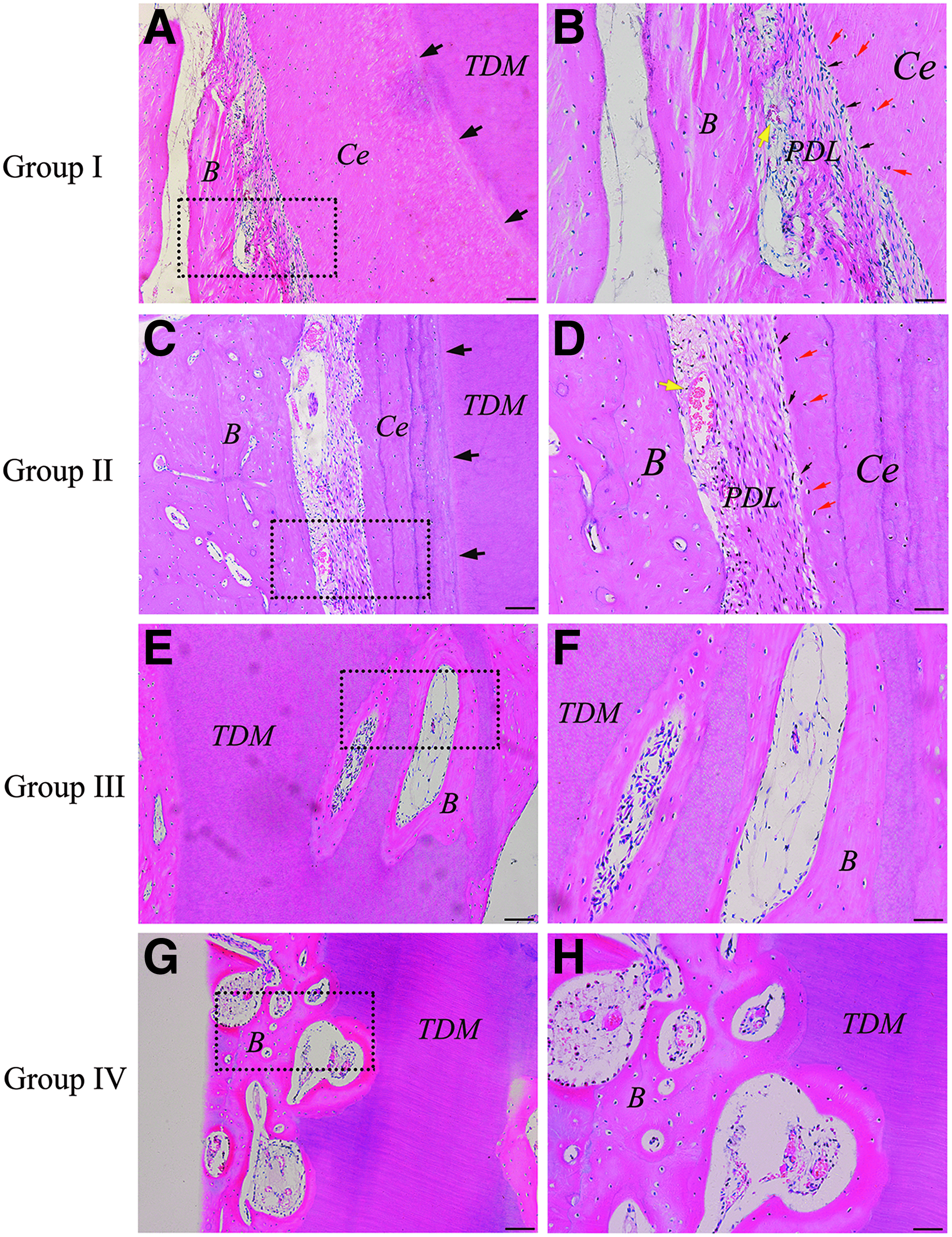
Representative images of HE staining for periodontal tissue healing in different groups. Cementum-like tissue was found covering the TDM surface
In group I and II, the hard tissue deposited on the TDM surface was defined as new cementum-like tissue, with a clear reversal line delineating it from the TDM (Figs. 5A, B and 6A, C, black arrow). Cementoblast-like cells were present near the surface of the cementum-like tissue (Fig. 6B, D, black arrow) and cementocyte-like cells were seen embedded in the cementum-like tissue (Fig. 6B, D, red arrow).
Normal functional PDL consists of fiber bundles perpendicularly inserted into the cementum, named Sharpey's fibers. Although soft connective tissues were found in group I and group II, Masson staining revealed striking differences in the orientation of new fibers between the two groups. It was exciting to find that the angulation of regenerated fibers against the cementum-like tissue surface was about 50° in group I (Fig. 7A), which is close to that of naturally mature ligament (mean±SD=47.3±12.0°). 35 Furthermore, cementoblast-like cells (Fig. 8, yellow arrow) were seen residing between functionally putative periodontal fibers (Fig. 8, white arrow). In contrast, in group II the fibers did not originate at the root, rather, almost parallel to the root surface (Fig. 7B). Revascularization was found in both groups (Fig. 6B, D, yellow arrow).

Masson staining showed the orientation of periodontal ligament fibers in group I and II. The angulation of regenerated fibers against the cementum-like tissue surface was about 50° in group I
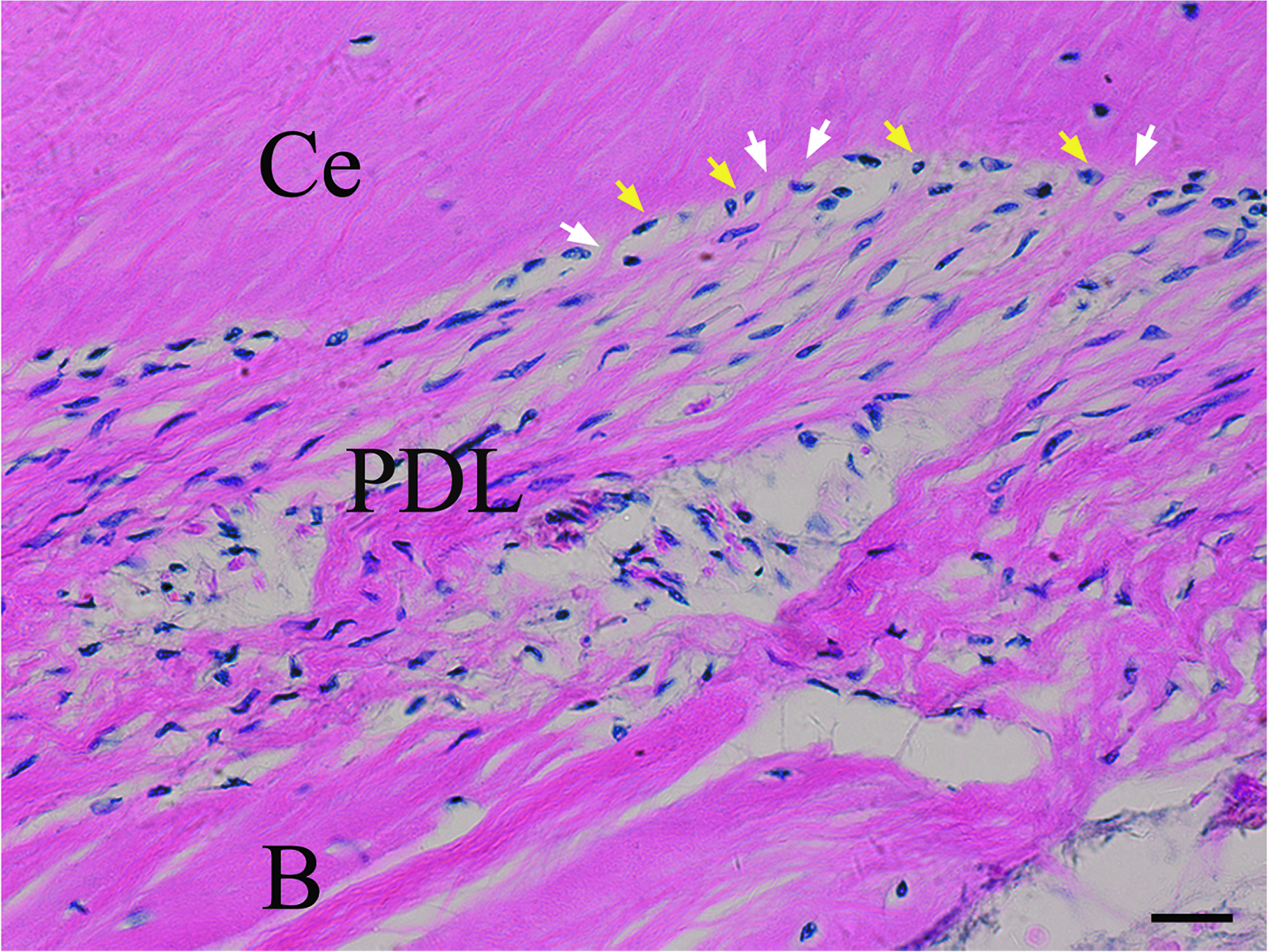
Higher magnification image of PDL–tooth interface. Cementoblast-like cells (yellow arrow) were seen residing between functionally putative periodontal fibers (white arrow). Ce, cementum-like tissue; B, alveolar bone. (Scale bar=20 μm). Color images available online at www.liebertpub.com/tea
Discussion
The tooth–PDL–alveolar interfaces play important roles in tooth function. We combined PRF and TDM together, and transplanted them into the alveolar fossa. It was found that the tooth–PDL–alveolar interfaces could be regenerated, probably through homing of endogenous BMSCs and PDLSCs. This is the first report of in situ regeneration of tooth root possessing the same hard–soft interface structure with natural root.
A key requirement for successful endogenous tissue regeneration is the recruitment of a sufficient number of stem/precursor cells to the injury site. 17 It is proved that after coculture of BMSCs and PDL, BMSCs acquire characteristics of cells in the PDL in vitro. 36 Furthermore, injected BMSCs were capable of homing to periodontium, differentiated into periodontal specific cells and participated in the periodontal defect regeneration after injury. 37 Besides BMSCs homing through bloodstream, PDLSCs residing within neighboring healthy tissue may also be recruited to an injury site for regeneration. In addition, a little PDL tissue still remained in the alveolar socket after tooth extraction, which contains PDLSCs. 38 Therefore, BMSCs and PDLSCs were considered as effective sources for cell homing. However, multiple growth factors released in an optimized ratio and a specific spatiotemporal pattern were involved in the process of tissue regeneration. PRF was defined as an ideal scaffold and a persistent source of multiple growth factors at a natural scale. In this study, it was found that PRF significantly recruited both BMSCs and PDLSCs. This is the first step for endogenous regeneration. Furthermore, PRF was found to stimulate the proliferation of PDLSCs and BMSCs in vitro, which was in accordance with other studies.22,39
The differentiation of recruited cells into the targeted cell types is also vital for regeneration of functional tissues. 17 TDM, which is regarded as a natural decellularization matrix scaffold, is expected to induce regenerative processes not only through specific organomorphic structures, but also by the physiological presentation of different cocktails of regulatory molecules in a mechanically suitable environment. It was proved that TDM is capable of directing the differentiation of the seeded cells.26–29,40 In this study, PRF and TDM were considered as a unit and their effects on cell differentiation were evaluated in vitro. BSP, OPN, and OCN are the common markers found in cementoblasts as well as osteoblasts. 41 The qRT-PCR results demonstrated that after 7 days coculture with PRF and TDM, higher expression of BSP and OPN mRNA were detected in BMSCs, whereas higher expression of BSP, OPN, and OCN were detected in PDLSCs (Fig. 4B). These results indicated that PRF/TDM have the potential to stimulate the differentiation of PDLSCs and BMSCs along the cementoblastic lineage.26,40 This potential is further supported by the results of in situ animal models. However, Zhao et al. 5 found that BSP and OCN mRNA were downregulated in human PDLSCs when cocultured with PRF throughout the experimental period (21 days). This result seemed contrary to our findings, but it may be explained by the presence of TDM, which was not involved in their study. Cementum-like tissue formation was not evident in their study either.
In vitro results indicated that it was possible to use PRF and TDM to regenerate tooth root by cell homing. Therefore, we verified this idea in beagle dog as an orthotopic transplantation animal model. Bioactive cues and inductive microenvironment are key factors for endogenous regeneration. Tooth root/periodontal regeneration require the restoration of both hard and soft tissues to their original functional architecture. In particular, PDL fibers must insert perpendicularly to the cementum. In group I and group II, cementum-like tissue was deposited on the TDM surface with a clear reversal line indicating it was newly formed. Strikingly, the data demonstrated that bioactive molecules released from TDM played a significant role in regenerating a more functional PDL (about 50° to the root surface) in group I, whereas using autoclave-treated TDM in group II, we mainly observed the collagen fibers were parallel with the root surface. Recently, studies have also demonstrated that the PRF membrane promotes periodontal regeneration and enhances alveolar bone augmentation.5,22,23 Kim et al. 16 found newly formed bone and regeneration of a putative PDLin their study, but without cementum regeneration. In addition, the newly formed PDL-like tissues were unfavorable, without well-oriented fibers and the connection to tooth root. This may be because of the absence of inductive scaffold. Although TDMs in group III were implanted into fresh extraction socket, there were no newly formed cementum and PDL-like tissues observed. These distinct differences should be caused by PRF. The healing process after TDM implantation resembles that of tooth replantation in some respects. After tooth replantation, the key requirement for successful periodontal healing is that sufficient PDL cells occupy tooth surface rather than osteoblasts or epithelial cells. As mentioned above, PRF stimulates in vitro proliferation and differentiation of human PDL fibroblasts and promotes periodontal regeneration.5,22,23 Zhao et al. 5 found that when tooth root was replanted with PRF, root resorption was significantly inhibited compared with replantation of the root only. However, without PRF in group III, this key requirement is difficult to meet. We also transplanted PRF and TDM into tooth extraction site 3 months after tooth extraction as delayed implantation in group IV. The results showed that TDM directly integrated with the surrounding bone and became part of the alveolar bone. In fact, it is demonstrated that both dentin and PRF are effective in bone regeneration. 42 After the healing of the tooth extraction socket, the periodontal regeneration microenvironment was replaced by osteogenic microenvironment. Therefore, PRF and TDM promoted bone formation in this osteogenic microenvironment. In summary, PRF serving as bioactive cues, TDM serving as inductive scaffold, as well as tooth socket microenvironment are indispensable for the achievement of endogenous tooth root regeneration in our study.
For the promotion of cell homing to regenerate periodontal tissue defect, even the lost tooth root is expected to ameliorate the translational difficulties in relation to the use of exogenous stem cells. This is the first report of in situ root regeneration by cell homing in a larger animal model. The successful approach applied in this study might accelerate the clinical translation, although mechanical properties of the roots were not analyzed. Are they capable of supporting the porcelain crown and perform normal functions? An important extension study will be done in the future.
Footnotes
Acknowledgments
This study was supported by the National Basic Research Program of China (2010CB944800), National High Technology Research and Development Program of China (2011AA030107), Nature Science Foundation of China (81271095, 81271119, 81200792 and 81300848), International Cooperation Program of China (China, 2013DFG32770 and 2011DFA51970), Doctoral Foundation of Ministry of Education of China (20110181120067, 20110181110089 and 20120181120013), Key Technology R&D Program of Sichuan Province (2012SZ0013, 12ZC0493, 13ZC0971, 2013GZX0158, 2013SZ0015 and 13ZC0979), and Basic Research Program of Sichuan Province (2011JY0125, 12JC0212, 2012JY0077 and 2013JY0019).
Disclosure Statement
The authors declare no competing financial interests.