
Abstract
Brain-derived neurotrophic factor (BDNF) exerts therapeutic effects following intracerebral hemorrhage (ICH). However, it is difficult to maintain sufficient concentrations in the hemorrhage hemisphere. We demonstrated previously that BDNF fused to a collagen-binding domain (CBD) could bind to collagen in the ventricular ependyma and stimulate cell proliferation in the subventricular zone (SVZ). In this study, we verified the therapeutic effects of CBD-BDNF in the rat ICH model induced by bacterial collagenase by injecting CBD-BDNF into the lateral ventricle of ICH rats. The results demonstrated that CBD-BDNF was retained at high levels in the hemorrhage hemisphere, where it promoted neural regeneration and angiogenesis, reduced tissue loss, and improved functional recovery.
Introduction
I
Endogenous neurogenesis plays an important role in repairing nerve damage after ICH. The subventricular zone (SVZ) of the lateral ventricle is the main region that generates new neurons in the adult brain. 7 After ICH, these endogenous progenitor cells could be induced to proliferate in the SVZ. Some newly proliferating cells then migrate to the site around the injury sites, where they further differentiate into neurons during the process of neurogenesis. 8 However, this regeneration is not sufficient for repairing, particularly after severe injuries. Brain-derived neurotrophic factor (BDNF) could promote neural regeneration and angiogenesis. The administration of BDNF into the lateral ventricle of adult rat improved neurological deficits by promoting endogenous neurogenesis after ICH. 9 Therefore, enhancing endogenous neurogenesis could be a feasible therapy for ICH.
However in practice, it is difficult to retain BDNF solution in the SVZ due to its rapid diffusion into cerebrospinal fluid. To maintain BDNF concentrations in the brain, multiple injections, a micro-osmotic pump, and the transplant of genetically modified cells or an adenoviral vector overexpressing BDNF have been used in the previous study.10–12 However, the cost, surgical risk, and immunological rejection would all be increased. In addition, excessive amounts of BDNF could cause possible adverse effects. 13
Therefore, the delicate control of dose and localization of BDNF is critical. We demonstrated previously that BDNF fused by a collagen-binding domain (CBD) could bind specifically to collagen. 14 The type I collagen is rich in the ventricular ependyma of the lateral ventricle. 15 CBD-BDNF could bind to the collagen of the ventricular ependyma, and this retained CBD-BDNF would directly stimulate cell proliferation in the SVZ, and exert therapeutic effects for a prolonged period. In this study, the collagen-targeting therapeutic strategy was assessed in a rat ICH model. We evaluated neurogenesis, angiogenesis, and functional recovery after ICH using behavioral testing, multiple molecular imaging, and immunohistochemistry (IHC).
Materials and Methods
Preparation of CBD-BDNF and native BDNF
The preparation of BDNF fused with collagen-binding domain (CBD-BDNF) and BDNF without collagen-binding domain (NAT-BDNF) was performed as described previously. 14 Both CBD-BDNF and NAT-BDNF contained 6× His purification tags to allow them to be distinguished from the endogenous proteins. The ability of BDNF to bind to the collagen matrix was quantified using a modified ELISA, as described previously.14,16
Surgical procedures and application of BDNF
All animal experiments were performed in accordance with the guidelines issued by the Committee on Animal Research of Peking Union Medical College Hospital, and were approved by the Institutional Ethics Committee. The procedure for inducing ICH in rats was described previously. 17 Briefly, adult male Sprague–Dawley rats (n=100, 230−250 g) were anesthetized by intraperitoneal injection of 10% chloral hydrate (400 mg/kg), and then injected with collagenase type IV (0.4 U dissolved in 1 μL saline; Sigma) into the left caudate putamen using stereotactic coordinates (0.2-mm posterior and 3.0-mm lateral of bregma, at a depth 6 mm below the surface of the skull). Collagenase was injected at a rate of 1 μL/min using a microinjector. After injections, the needle was left in place for 5 min prior to withdrawal.
Three days after ICH induction, the hematoma size became stable. 18 Magnetic resonance imaging (MRI) was performed in all rats to evaluate the degree of hematoma, and to measure the lesion volumes. Rats subjected to ICH with lesion sizes ranging from 15 to 20 mm3 were selected, and assigned randomly to three groups (25 rats in each group: 12 rats for collagen-binding assay in vivo, 6 rats for image study, 6 rats for behavioral tests and immunohistochemical analysis, and one flexible); rats received 10 μL (0.5 nmol) NAT-BDNF (the NAT-BDNF group, n=25), 10 μL (0.5 nmol) CBD-BDNF (the CBD-BDNF group, n=25), or 10 μL PBS (the control group, n=25) that was injected slowly for 2 min into the left lateral ventricle using a stereotactic frame (0.8-mm posterior and 1.6-mm lateral of bregma, at a depth 4 mm below the surface of the skull). After injection, the needle was removed, the cranial hole was sealed with bone wax, the wound was sutured, and the rats were placed in a warm box with free access to food and water.
Evaluation of collagen content in the rat hemorrhage hemisphere
Six rats were sacrificed by cervical dislocation. The hemorrhagic hemispheres of three rats were excised rapidly and frozen immediately in liquid nitrogen. Proteins were extracted for western blotting. Antibodies against collagen type I (1:200 dilution; Santa Cruz) were used to assess the collagen content in the rat hemorrhage hemisphere, and recombinant collagen (10 μg; Sigma) was used as the positive control. The remaining three rats per group were perfused intracardially with chilled saline followed by 4% paraformaldehyde in 0.01 M PBS (pH 7.4). The brains were postfixed in paraformaldehyde, and then paraffin embedded. Coronal sections (8 μm) were isolated from a 1.5-mm area surrounding the bregma. The samples were examined by IHC using antibodies against collagen (1:200 dilution; Santa Cruz).
Collagen-binding assay of BDNF in vivo
At 3 and 12 h after injection with NAT-BDNF or CBD-BDNF, 24 rats were sacrificed by cervical dislocation. The hemorrhagic hemispheres were then excised and frozen immediately in liquid nitrogen, and proteins of the ventricular ependyma and choroid plexus of hemorrhage hemispheres were extracted for analysis by western blotting. Antibodies against polyhistidine (1:1000 dilution; Sigma) were used to distinguish exogenous from endogenous proteins.
Behavioral testing
The modified neurological severity score (mNSS) test was performed at 1, 3, 7, 14, and 28 days after ICH by two investigators who were blinded to the experimental groups. The mNSS test is composed of motor, sensory, balance, and reflex tests. 19 Neurological function is graded on a scale of 0−18 (normal score=0; maximal deficit score=18). A single point is awarded for a specific abnormal behavior or the lack of a tested reflex. Thus, the higher the score, the poorer the neurological function was indicated.
Magnetic resonance imaging
MRI includes T2-weighted imaging (T2WI), diffusion-weighted imaging (DWI), and proton magnetic resonance spectroscopy ( 1 H MRS). MRI was performed using the ClinScan 7T system, which combines Bruker hardware interfaced with Siemens software. Rats were anesthetized using 10% chloral hydrate (400 mg/kg) to prevent movement artifacts on the MRI images. A birdcage-type coil with four channels was used as the transmitter, with a quadrature half-volume coil as the receiver.
T2WI can provide anatomical information of cerebral lesions. The T2WI sequence parameters were as follows: TR/TE=3380/41 ms, slice thickness=0.7 mm, field of view (FOV)=40×40 mm2, flip angle=90°, acquisition matrix=320×280, voxel resolution=0.16×0.12×0.8, NEX=2, and total acquisition time=3–5 min. T2WI was performed 3 days after surgery to measure the success of the rat ICH model. T2WI was also performed 2 and 4 weeks post-ICH to assess the therapeutic effect of NAT-BDNF and CBD-BDNF on hematoma absorption and brain repair. The total lesion volume was calculated as the sum of the injury area multiplied by the thickness of all the slices (0.7 mm/slice) using the Osirix V.3.9.2 Medical Imaging Software. 20 Brain tissue loss was expressed as the mean percentage of the volume decrease between the lesion and control hemispheres, which was calculated from the central three slices around the hematoma on the T2WI 4 weeks after ICH. Brain tissue loss (%)=(CH − LH)/CH×100% (where LH is the area of the lesion hemisphere, and CH is the area of the contralateral hemisphere), and was calculated using the Osirix V.3.9.2 Medical Imaging Software. 20
DWI is a sensitive and reliable means of evaluating edema. DW images were obtained using a two-dimensional spin-echo–echo-planar imaging sequence (SE-EPI) with TR/TE=4500/35, slice thickness=0.5 mm, and FOV=40 mm×40 mm. Quantitative maps of the apparent diffusion coefficient (ADC) were calculated based on two different b-values (0 and 600 s/mm2). The volume of interest (VOI) was extracted by outlining the regions of either hypointensity or hyperintensity that were clearly different from the surrounding tissue, and the corresponding mirror position of the contralateral hemisphere. Each VOI value was the mean result of three separate measurements on the same sections. The extent of edema was expressed as the ratio obtained from the formula: mean ADC left/mean ADC right.
To evaluate the ICH-induced metabolic variation, 1 H MRS was performed. The 1 H MRS parameters were as follows: TR/TE=1500/135 ms and FOV=15×8×4 mm3. Three-dimensional images were collected. And the extent of the lesion and VOI (located at the surrounding of hematoma) for the 1 H MRS were determined from T2WI. Measurement software supplied with the equipment was employed to obtain the brain metabolite spectra from within the VOI. The values of the metabolites were expressed as ratios of an internal standard, so that metabolite levels over time and between different rats could be compared. We employed Cr as the reference value, and NAA/Cr and CHO/Cr metabolite ratios were examined. The VOI and each VOI value were same, as described previously. The metabolite ratios of NAA=mean (NAA/Cr) left/mean (NAA/Cr) right, whereas the metabolite ratio of CHO=mean (CHO/Cr) left/mean (CHO/Cr) right.
Positron emission tomography
To assess the glucose metabolic activity in the brain lesions, rats were monitored dynamically and investigated longitudinally using 18 F-FDG micro-positron emission tomography (PET) scanning at 3 days, 2 weeks, and 4 weeks post-ICH. Rats were anesthetized as described previously, and 22.2 MBq (0.6 mCi) of 18 F-FDG (produced by the Department of Nuclear Medicine, Peking Union Medical College Hospital, Beijing, China) was injected intravenously. After an uptake period of 40 min, each rat was scanned for 10 min using a micro-PET (Siemens). The PET data were acquired and analyzed using ASI Pro VM software (Concorde Microsystems). Three-dimensional volumetric images were then reconstructed. The VOI in the cerebral hemisphere was drawn on the side without ICH, and the ipsilateral VOI was mirrored on the injured side. Each VOI value was the mean of three separate measurements taken from equally spaced sections through the lesion. The VOI was used to evaluate the extent of hypometabolism. Hypometabolism (%)=the mean radiation intensity left/mean radiation right×100%.
Single-photon emission computed tomography
Single-photon emission computed tomography (SPECT) imaging was performed 4 weeks post-ICH to assess angiogenesis and hemodynamics at the injured site. Rats were anesthetized as described previously. And 2–3 mCi of 68Ga-RGD (Institute of Chinese Atomic Medicine, Beijing, China) was injected intravenously. After an uptake period of 5 min, each rat was scanned for 15–20 min (360° rotation, 120 projections) using a micro-SPECT/CT camera (Bioscan; Nano Spect/CT) with four rotating parallel-hole collimators. CT scans (tube voltage=65 kV, tube current=100 μA, slice thickness=0.6 mm, gapless) were performed subsequently. SPECT data were analyzed semiquantitatively. One day after the 68Ga-RGD scan, 99TCm-ECD-SPECT examinations were performed. Rats were injected intravenously with 74–111 MBq (2–3 mCi) of 99TCm-ECD (Institute of Chinese Atomic Medicine, Beijing, China), and images were captured using the acquisition and reconstruction protocols described earlier.
The VOI in the cerebral hemisphere was drawn on the side contralateral to the lesion on both the 68Ga-RGD and 99TCm-ECD images. The ipsilateral corresponding structure was then mirrored. The mean radioactivity uptake (SUV) in each VOI was the mean of three separate measurements performed on equally spaced sections through the lesion. Hypoperfusion (%)=SUV-99TCm-ECD left/SUV-99TCm-ECD right×100%. Angiogenesis (ratio)=SUV-68Ga-RGD left/SUV-68Ga-RGD right.
Tissue loss measurement by hematoxylin and eosin histology
Hematoxylin and eosin (H&E) histology was performed at 4 weeks after ICH for the tissue loss measurements. The brains were collected and further fixed in 4% paraformaldehyde, and then sliced into 2-mm-thick sections. Each block was embedded in paraffin. Four of the adjacent 6-μm-thick sections were cut from each block and stained with H&E. The percentage of tissue loss in the ipsilateral compared with the contralateral hemisphere of the brain was measured using the Image-pro plus software (Media Cybernetics).
Immunohistochemical assessment
Four weeks after ICH, rats were anesthetized using 10% chloral hydrate (400 mg/kg), and then perfused intracardially with chilled saline followed by 4% paraformaldehyde. The brains were collected and fixed in 4% paraformaldehyde, and then embedded in paraffin. IHC was performed on 20-μm mounted sections using the following antibodies: PCNA (1:500; Abcam), doublecortin (DCX, 1:500; Abcam), glial fibrillary acidic protein (GFAP, 1:200; Sigma), NeuN (1:500; Abcam), CD31 (1:200; Sigma), and vascular endothelial growth factor (VEGF, 1:200; Abcam). Immunoreactive cells were counted based on the evaluation of the mean of three slides (20-μm thick, 200-mm intervals, every 10th slide) per sample using Image-Pro Plus software. The number of PCNA- and DCX-positive cells in the SVZ, and CD31-, VEGF-, GFAP-, and NeuN-positive cells in the peri-hematoma zone were all counted at a magnification of ×200.
Statistical analysis
All the data were expressed as mean±standard deviation (SD). Statistical analysis was performed using SPSS software for Mac (IBM SPSS Statistics Version 20.0). Statistical differences between two groups were analyzed using independent-sample t-tests. One-way ANOVA was used to analyze multiple-comparison procedures. Significant differences were considered as *p<0.05 and **p<0.01.
Results
Collagen-binding assay in vivo
The binding of NAT-BDNF and CBD-BDNF to collagen membranes was tested previously in vitro using a modified ELISA. 21 CBD-BDNF had a markedly lower Kd, which reflected the protein having a higher affinity for collagen. Consistent with this, the quantity of CBD-BDNF retained on collagen membranes was substantially higher than NAT-BDNF. 21 In the present study, we assessed the collagen distribution in the ventricular ependyma and choroid plexus of hemorrhage hemispheres using IHC (Fig. 1A), and identified that the rat hemorrhage hemisphere was rich in collagen using western blotting (Fig. 1B).
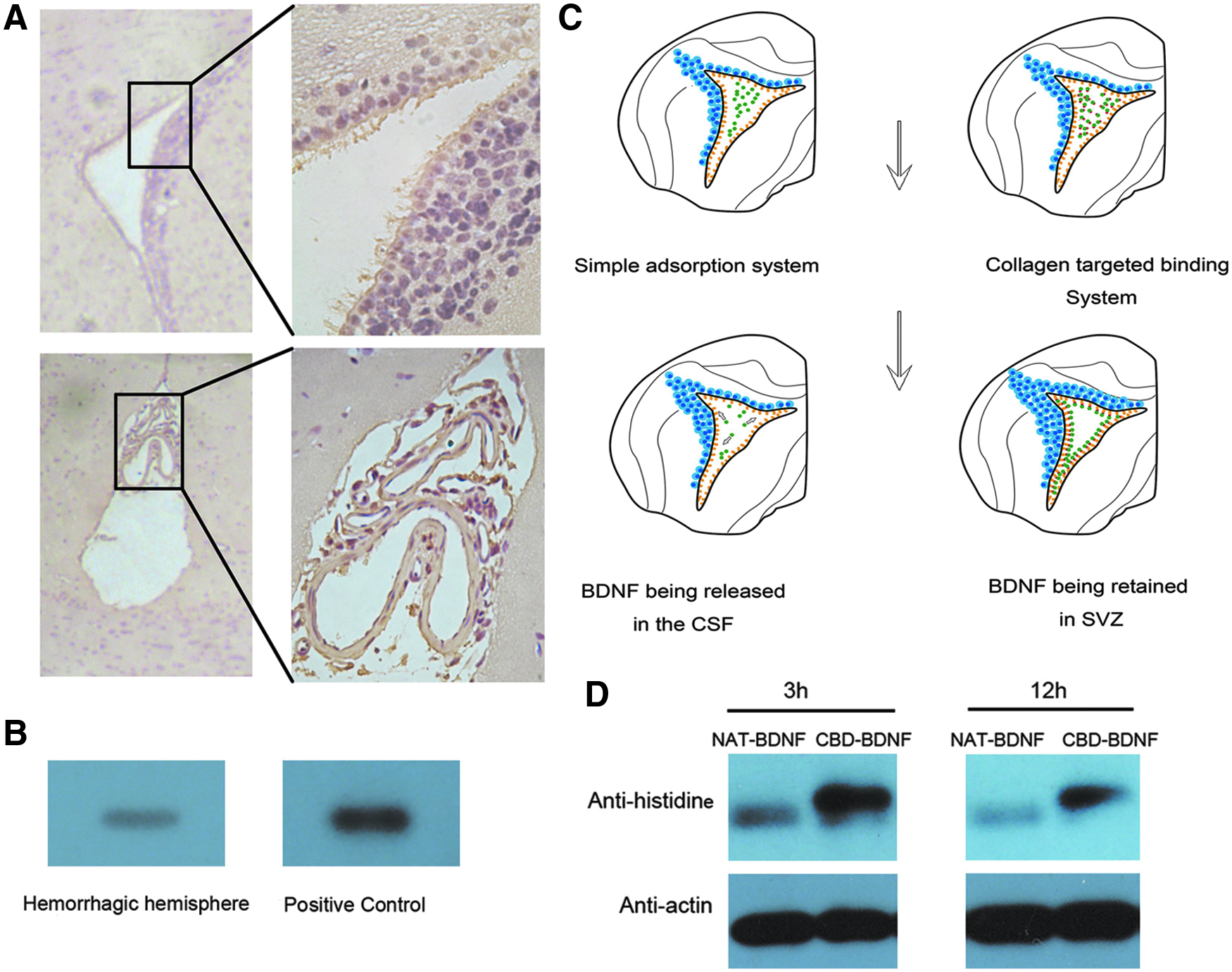
Determination of the collagen content in the brain of rats, and the retention of brain-derived neurotrophic factor (BDNF) without collagen-binding domain (NAT-BDNF) and BDNF fused with collagen-binding domain (CBD-BDNF) in vivo.
We also evaluated whether CBD-BDNF was retained in the hemorrhage hemisphere. Three and 12 h after the injection with NAT-BDNF or CBD-BDNF, proteins were extracted from the hemorrhage hemisphere, and western blotting was used to measure retained BDNF. There was significantly more CBD-BDNF remaining in the hemorrhage hemisphere compared with NAT-BDNF at both time points (Fig. 1C).
Behavioral testing
mNSS was assessed during the recovery of the rats. There was no difference in the scores between groups 1 or 3 days after ICH. However, a significant functional improvement was observed in the CBD-BDNF- and NAT-BDNF-treated groups compared with the control group 1 week after ICH (p<0.05, n=6). Two weeks after ICH injury, the CBD-BDNF treatment group showed significantly better neurological recovery (lower mNSS) than either the control (p<0.01, n=6) or NAT-BDNF groups (p<0.05, n=6). Four weeks after injury, there was still a significant functional improvement (lower mNSS) in the CBD-BDNF group compared with the control group (p<0.01, n=6) and the NAT-BDNF group (p<0.05, n=6; Fig. 2).

The modified neurological severity score (mNSS) test at different time points. *p<0.05, **p<0.01.
Magnetic resonance imaging
MRI T2WI can provide anatomical information regarding the size and position of hematoma in living organisms. 18 Three days after the ICH surgery, the hematoma size tended to be stable. Three days after ICH surgery, all rats received brain MRI T2WI, and only rats with hematoma volumes of 15–20 mm3 were selected for subsequent experiments (Fig. 3A). To assess the therapeutic effects of NAT-BDNF and CBD-BDNF on the reduction of the hematoma, hematoma areas were evaluated on T2WI images, and expressed as a percentage of the contralateral hemispheric area. Two and 4 weeks after injury, the hematoma area in the CBD-BDNF group was significantly smaller than the NAT-BDNF and control groups (p<0.05, n=6). Four weeks after injury, there were no significant differences between the NAT-BDNF and control groups (p>0.05, n=6) (Fig. 3A, B). This suggests that CBD-BDNF reduced the hematoma area effectively at both the early and late stages after ICH.
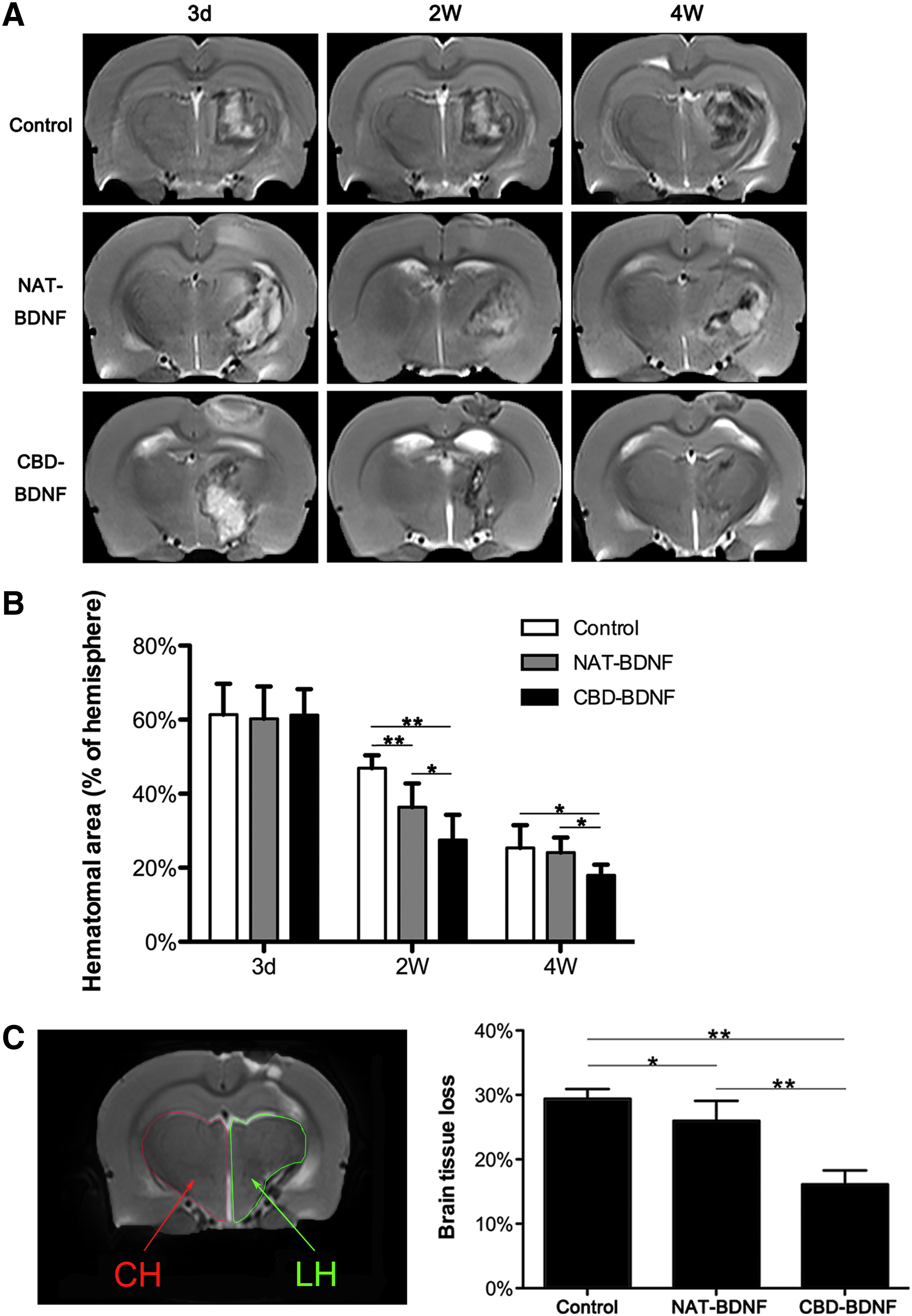
Hematoma area and brain tissue loss, as assessed by magnetic resonance imaging (MRI).
Tissue loss (% area of contralateral hemisphere) was analyzed using the results of T2WI 4 weeks after ICH. Tissue loss in the NAT-BDNF and CBD-BDNF groups was significantly less than in the control group (p<0.01, n=6), and the least tissue loss was observed in the CBD-BDNF group (p<0.01, n=6) (Fig. 3C). Therefore, CBD-BDNF effectively decreased brain tissue loss after ICH.
To determine the therapeutic effect of CBD-BDNF and NAT-BDNF on edema after ICH, the MR technique of DWI was performed to calculate the ADC in the VOI (Fig. 4A). The extent of edema was expressed as the ratio of ADC in the contralateral hemisphere. Two weeks after ICH, the ratio of ADC was increased significantly in the CBD-BDNF treatment group compared with the control group (p<0.01, n=6) (Fig. 4B). These results suggest that CBD-BDNF treatment effectively reduced edema after ICH.

Evaluation of cerebral edema and metabolic changes after intracerebral hemorrhage (ICH) using magnetic resonance imaging (MRI).
1 H MRS allows the noninvasive assessment of metabolic changes during stroke (Fig. 4C). Two and 4 weeks after ICH, there was a significant increase in NAA/Cr, and decrease in Cho/Cr values in the CBD-BDNF treatment group compared with control (p<0.05, n=6) (Fig. 4D). This suggests that CBD-BDNF could effectively repair the impaired neurons and promote nerve regeneration after ICH.
PET imaging of metabolism in the brain
18 F-FDG micro-PET imaging provides accurate, quantitative measurements of regional glucose metabolic variations after ICH injury. In this study, we expressed the extent of metabolic variations as a percentage of the contralateral area. Three days after ICH, all groups had an obvious metabolic defect area (Fig. 5A). However, 2 weeks after ICH injury, both the NAT-BDNF and CBD-BDNF treatment groups exhibited a significantly higher metabolic activity in the affected hemisphere compared with the control group (p<0.05, n=6); there were no significant differences between the NAT-BDNF and CBD-BDNF groups at this time point (p>0.05, n=6). Four weeks after injury, the CBD-BDNF group showed the smallest metabolic asymmetry. Glucose metabolism in the damaged area was highest in the CBD-BDNF group (p<0.01, n=6) (Fig. 5B). These data suggest that CBD-BDNF promoted long-term glucose metabolism and the recovery of neural function after ICH.
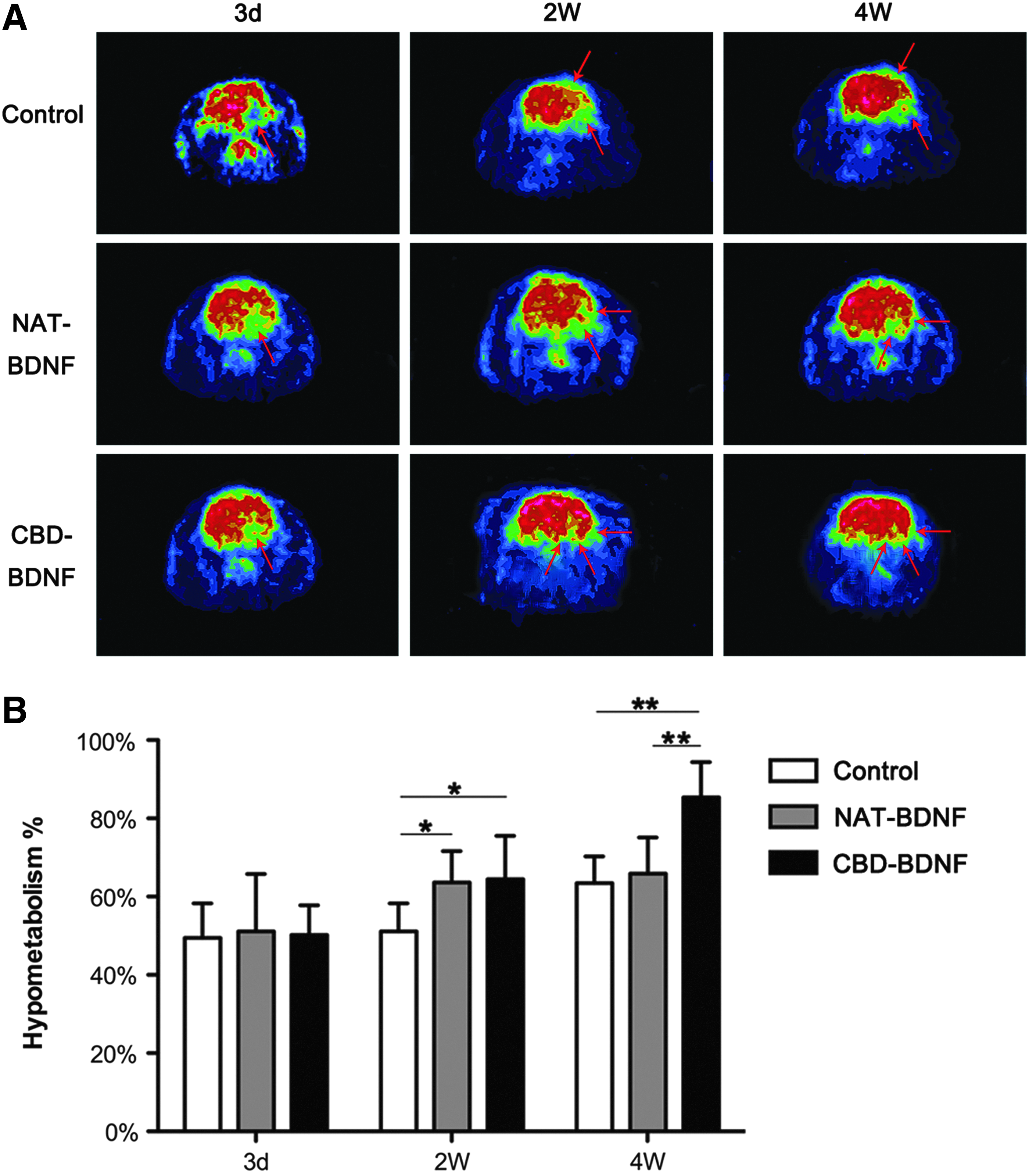
Glucose metabolism in the brain imaged using a micro-positron emission tomography (PET) scanner.
SPECT/CT imaging of hemodynamics and angiogenesis in the brain
SPECT can evaluate variations in angiogenesis and hemodynamics in vivo after ICH. Representative brain short-coronal serial slices from the same animal following in vivo SPECT imaging of 68Ga-PRGD and 99TCm-ECD are presented in Figure 6. In normal rats, there was no 68Ga-RGD uptake, and no cerebral hypoperfusion in the whole brain (Fig. 6A, E). Rats in the control group exhibited decreased 99TCm-ECD uptake, and almost no 68Ga-PRGD uptake (Fig. 5B, F). The CBD-BDNF group showed the smallest hypoperfusion, and localized 68Ga-RGD uptake was also observed (Fig. 5D, H). Moreover, the localization of 68Ga-RGD uptake was matched perfectly at the edge of the lesion, as evidenced by decreased 99TCm-ECD uptake (Fig. 5D, H).
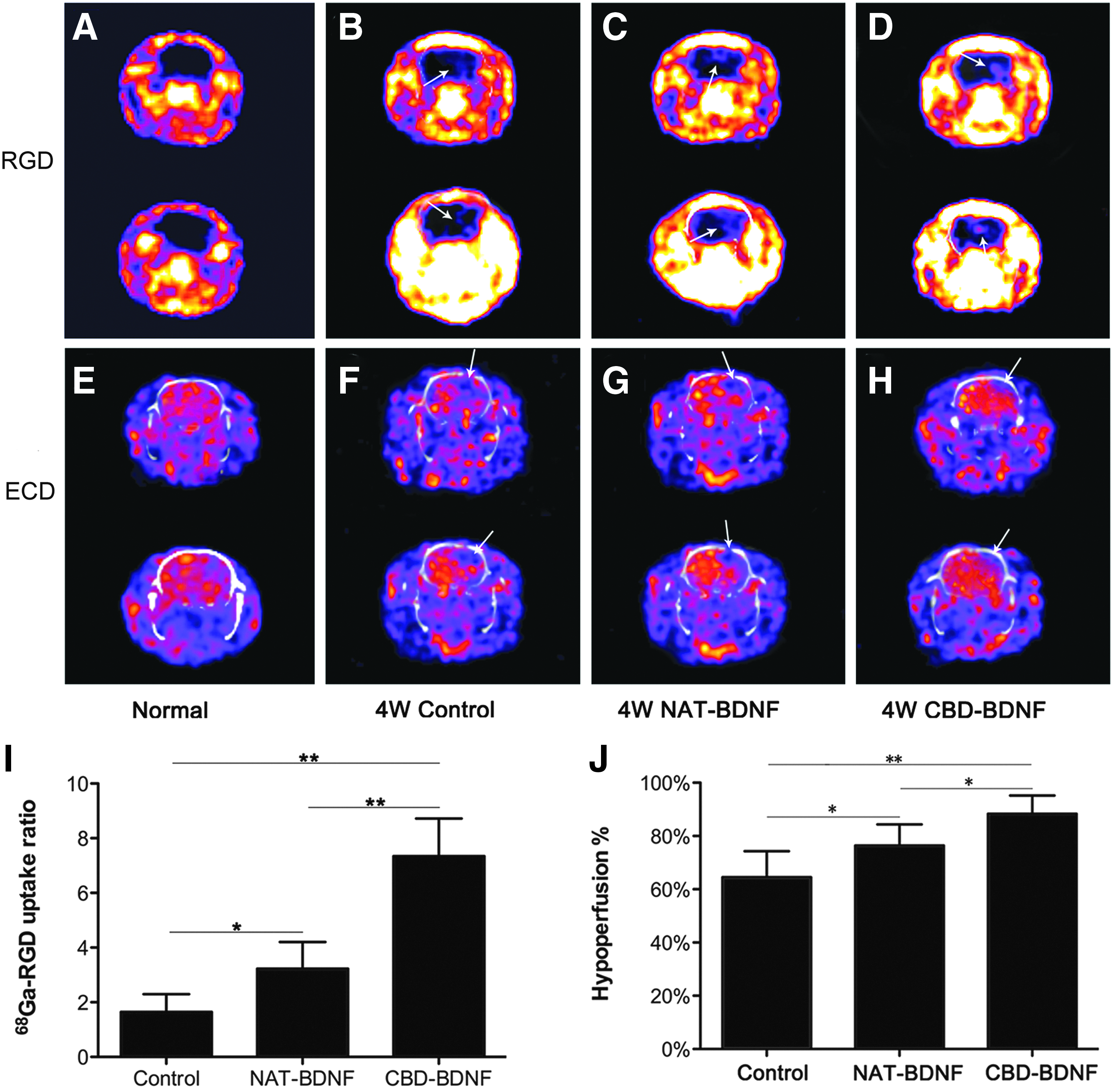
The degree of angiogenesis and blood perfusion after intracerebral hemorrhage (ICH) was assessed by 68Ga-RGD and 99TCm-ECD imaging.
The CBD-BDNF (p<0.01, n=6) and NAT-BDNF groups (p<0.05, n=6) had significantly higher 68Ga-RGD uptake than the control group, and the CBD-BDNF-treated group exhibited the highest 68Ga-RGD accumulation (Fig. 6I). There was a significant reduction in the radial rarefaction and defect areas of the 99TCm-ECD images in the CBD-BDNF (p<0.01, n=6) and NAT-BDNF groups (p<0.05, n=6) compared with the control group. The CBD-BDNF-treated group exhibited the smallest hypoperfusion area (Fig. 6J). These results suggest that CBD-BDNF elevated angiogenesis and hemodynamics after ICH.
Tissue loss analysis by H&E
Tissue loss (% area of contralateral hemisphere) for each group was analyzed from the result of H&E histology at 4 weeks after ICH (Fig. 7A–C). Tissue loss of the NAT-BDNF group and the CBD-BDNF group was significantly smaller than the control (p<0.01, n=6), and the tissue loss of CBD-BDNF was the smallest (p<0.05, n=6) (Fig. 7D). CBD-BDNF effectively decreased tissue loss after ICH.
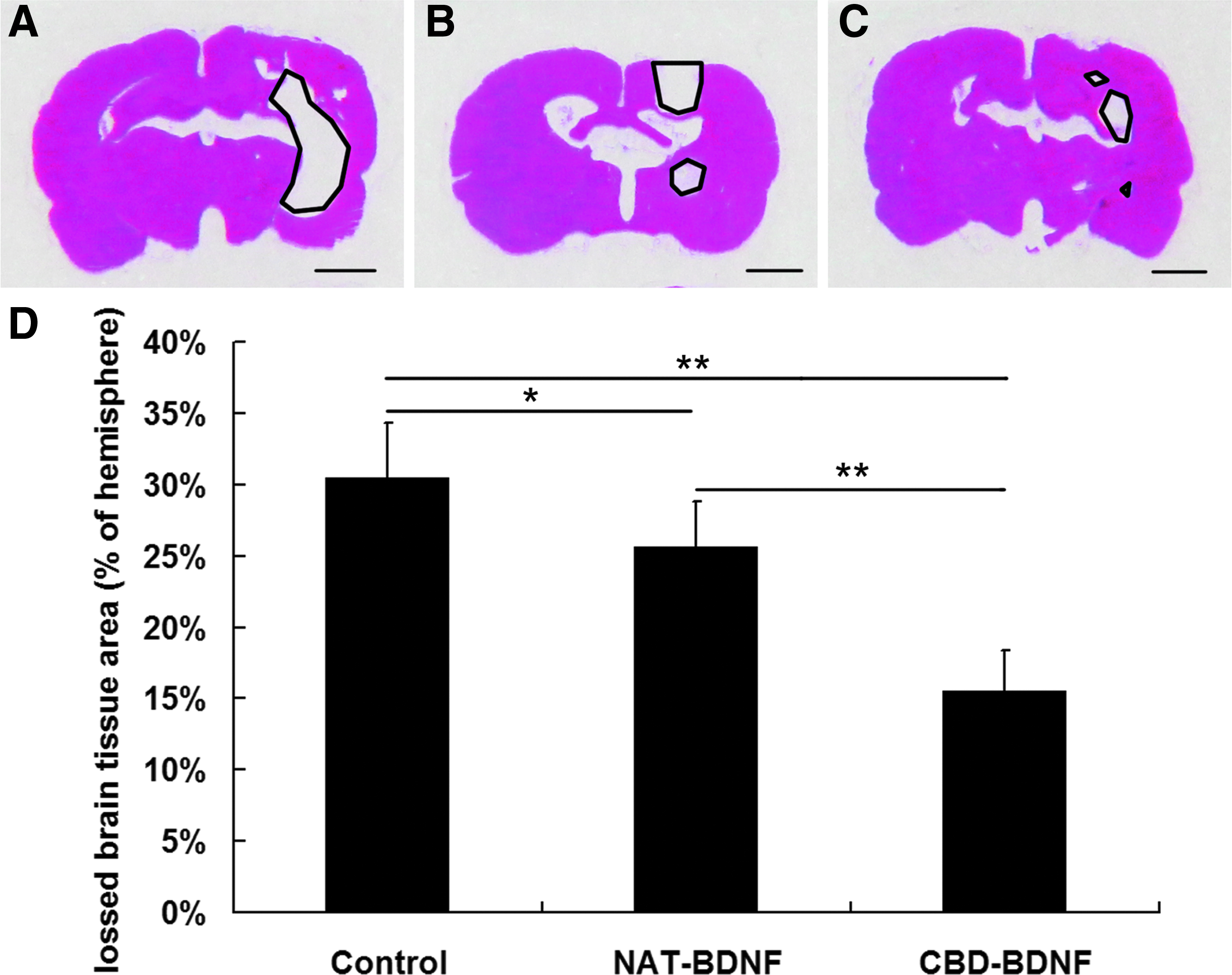
Tissue loss measurements by H&E histology.
Endogenous neurogenesis in SVZ assessed by IHC
Activation of endogenous neurogenesis was observed after ICH, which was accentuated in rats receiving BDNF in SVZ. With its ability to bind to collagen in the ventricular ependyma, CBD-BDNF could enhance the proliferation and differentiation of endogenous cells in the SVZ dramatically. PCNA is a marker that reflects the cell proliferation status of cells. 22 There was a significant increase in the number of PCNA-positive cells in the SVZ of CBD-BDNF group rats compared with the NAT-BDNF (p<0.05, n=6) and control groups (p<0.01, n=6) 4 weeks after ICH (Fig. 8A–D). DCX is a microtubule-associated protein that is expressed by neuronal precursor cells and immature neurons. Because it is expressed almost exclusively in developing neurons, DCX is used increasingly as a marker for neurogenesis. 23 There were more DCX+ cells in the SVZ of CBD-BDNF group than NAT-BDNF (p<0.05, n=6) or control groups (p<0.01, n=6) 4 weeks after ICH (Fig. 8E–H). This suggests that CBD-BDNF actively enhanced the proliferation and differentiation of endogenous cells in the SVZ.
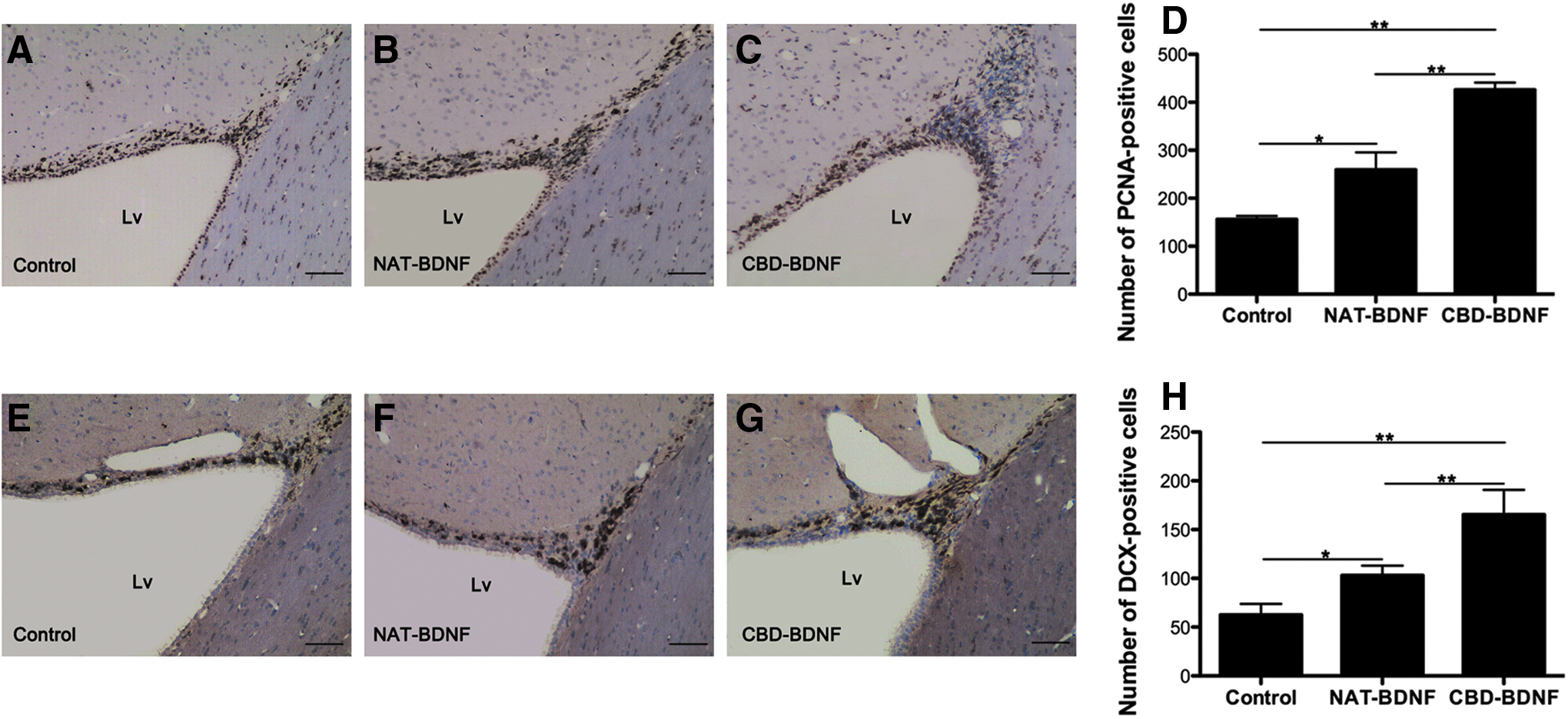
Cell proliferation and differentiation in the subventricular zone (SVZ) of the hemorrhagic hemisphere 2 weeks after intracerebral hemorrhage (ICH).
Neurogenesis and angiogenesis in hemorrhagic boundary zone by IHC
VEGF is a potent activator of angiogenesis that promotes endothelial cell proliferation and the formation of new blood vessels, 24 and CD31 is a surface marker of neovascular endothelial cells. 25 VEGF and CD31 IHC was performed 4 weeks after ICH to assess exogenous and endogenous VEGF expression and neovascular endothelial cells in the lesion boundary zone. There were more VEGF-positive endothelial cells and CD31+ cells in the lesion boundary zone in the CBD-BDNF group compared with the NAT-BDNF (p<0.05, n=6) and control groups (p<0.01, n=6) 4 weeks after ICH (Fig. 9A–H).
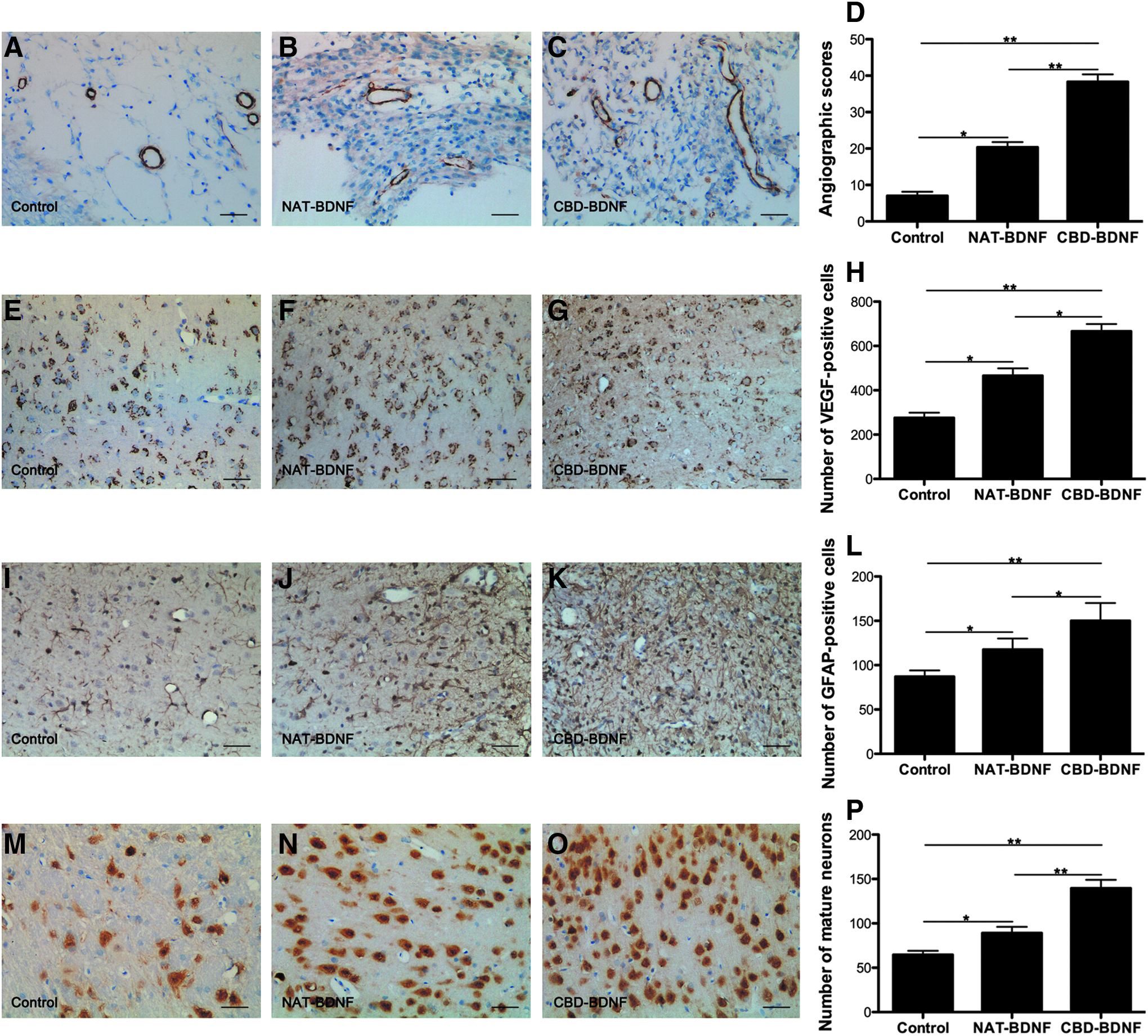
Neurogenesis and angiogenesis in per-hemorrhage by immunohistochemistry 4 weeks after intracerebral hemorrhage (ICH).
CBD-BDNF treatment resulted in more NeuN immunoreactive mature neurons in the lesion boundary zone than the other groups 4 weeks post-ICH (p<0.05, n=6) (Fig. 8I–L). The number of GFAP immunoreactive astrocytes in the lesion boundary zone was also higher in the CBD-BDNF group compared with either the NAT-BDNF (p<0.05, n=6) or control groups (p<0.01, n=6) 4 weeks after injury (Fig. 9M–P). These results suggest that CBD-BDNF may activate endogenous neurogenesis in the SVZ, and promote neurogenesis and angiogenesis in the per-hemorrhage zone after ICH.
Discussion
ICH accounts for about 10–15% of strokes, and is associated with high mortality and morbidity. To date, there are few effective clinical therapeutic treatments, although surgical decompression for ICH is widely accepted as potentially life-saving. 26 In recent years, some studies have focused on neurogenesis and angiogenesis as potential mechanisms for repair after ICH. 27 Reducing edema and inhibiting the inflammatory response to protect neuronal cells are also current areas of research. 28
Cell therapy, such as using mesenchymal stem cells (MSCs), has shown promise as a restorative strategy. As such MSCs may be able to differentiate into brain parenchymal cells and replace damaged neurons. However, the low survival and differentiation rate of the grafted neurons is a major concern. 29 Neurogenesis via the activation of endogenous neural progenitor cells (NPCs) is another potential treatment strategy for ICH. 27 The SVZ is the main region that generates new neurons in adult rats. Neural stem cells/NPCs can be activated in the SVZ after ICH. However, the number of proliferating cells is insufficient, and brain self-protection is always delayed. 8
BDNF is generally accepted to be a key factor that promotes neurogenesis and angiogenesis. In vitro studies revealed that adult striatal SVZ cells can be induced to differentiate to both neurons and glia after treatment with BDNF. 9 Moreover, BDNF prevents neuronal cell death, and modulates local inflammatory processes.30,31 Although BDNF exerts growth-promoting effects, its application and distribution in vivo are problematic due to its rapid diffusion into the cerebrospinal fluid, and its short half-life. Repeated intraventricular or stereotactic injections are traumatic and expensive, and excessive doses may cause side effects. 10 In a previous study, genetically engineered cells were used to maintain extended delivery of BDNF, but the safety of these strategies and of long-term BDNF expression using gene modification techniques still needs to be determined. 31
Precise control of BDNF dose and localization is critical for achieving a good therapeutic effect, and targeting therapy is a promising approach for BDNF delivery. In this study, we found that collagen-1 is dispersed widely in the ventricular ependyma and choroid plexus of the brain. 15 Collagen-1 in the ventricular ependyma is an ideal target for CBD-BDNF. Because of its CBD, CBD-BDNF can bind to collagen in the ventricular ependyma, and directly stimulate cell proliferation in the SVZ. Meanwhile, CBD-BDNF would be retained at the hemorrhagic ipsilateral ventricle, and exert therapeutic effects for prolonged periods.
In this in vivo study, a single intraventricular administration of CBD-BDNF bound to endogenous collagen in the ventricle and remained stable for much longer than NAT-BDNF. Cell proliferation and differentiation were assessed using staining for PCNA and DCX 4 weeks after ICH. More PCNA-positive neurons in the CBD-BDNF group suggested that CBD-BDNF promoted the proliferation of endogenous cells in the SVZ after ICH. An increased number of DCX-positive neurons existing in the CBD-BDNF group also suggested increased differentiation of the endogenous cells in the SVZ after ICH. These results suggest that the sustained release of CBD-BDNF activates increased proliferation and differentiation of endogenous cells in the SVZ, which helps repair the injury after ICH. This may be due to the short distance to the SVZ and the sustained action of CBD-BDNF bound to the ventricular ependyma.
We assessed many different aspects of the therapeutic effects of CBD-BDNF. Rats in the CBD-BDNF group exhibited the most favorable sensorimotor function recovery, as assessed by mNSS score. The mNSS scores of the CBD-BDNF group were decreased significantly compared with the NAT-BDNF and control groups from the second week after ICH; this difference continued until 4 weeks after treatment.
MRI technology was used extensively in this study. T2WI can provide information of variations in the structure of brain tissue. T2WI was performed 3 days after the surgical procedures to measure the success of the ICH model. Only rats with hematoma volumes of 15–20 mm3 were selected for the subsequent experiments. Because the collagenase-induced rat ICH model causes the disruption of several blood vessels, hematoma volumes are changeful. Therefore, this criterion is much more precise than previous criteria, which used only the mNSS. We also used T2WI to observe the dynamic changes in cerebral hemorrhage volume in vivo. Both 2 and 4 weeks after ICH, the hematoma area in the CBD-BDNF group was smaller than in the other groups. Tissue damage was measured by T2WI, and data revealed that less brain tissue was lost in the CBD-BDNF group than that in the other two groups at 4 weeks. These results suggest that CBD-BDNF reduced hematoma area and tissue loss.
Two MRI technologies (DWI and 1 H MRS) were also applied. DWI is a sensitive and reliable means of evaluating edema. The lower the ADC value, the more serious was edematous brain tissue. 32 DWI of the peri-hematoma zone demonstrated that the ratio of ADC in the CBD-BDNF treatment group was the highest 2 weeks after ICH. This suggests that CBD-BDNF reduced edema. 1 H MRS can assess the metabolic changes after ICH noninvasively. NAA values begin to decline after the destruction of the integrity of neurons. Choline, a marker of membrane phospholipids, is upregulated during myelin breakdown. Cr is used commonly as an internal reference because it is relatively stable in metabolic diseases. 32 The lower NAA/Cr ratios or higher Cho/Cr ratios calculated in this study correspond to a reduced neuronal density and neuronal dysfunction due to injury after ICH. The CBD-BDNF group exhibited the highest NAA/Cr ratio and lowest Cho/Cr ratio in the peri-hematoma zone 2 and 4 weeks after ICH, suggesting that CBD-BDNF helped to improve the survival of neurons and promoted sensorimotor recovery.
Molecular imaging was also used to evaluate the therapeutic effect of CBD-BDNF. PET imaging is a quantitative, accurate method for identifying metabolic variations after ICH. 33 ICH results in metabolic deficits, and eventually cellular apoptosis. Both 2 and 4 weeks after ICH, 18 F-FDG PET imaging revealed that CBD-BDNF increased glucose metabolism in the ICH hemisphere significantly. CBD-BDNF treatment maintained glucose utilization and restrained neuronal apoptosis, promoting the recovery of neurological function. Histological analysis also demonstrated that there were more NeuN immunoreactive mature neurons and GFAP-positive cells in the peri-injured zone of the CBD-BDNF group 4 weeks after ICH.
Sensitive SPECT/CT imaging was used to investigate variations in angiogenesis and perfusion after ICH. To observe neovascularization in the rat ICH model, we applied the novel-labeled SPECT tracer 68Ga-PRGD to visualize and quantify changes in integrin αvβ3 expression, which is enhanced on the vascular endothelium after the activation of angiogenesis and can be imaged using a tripeptide moiety of arginine-glycine-aspartic acid (RGD).34,35 Four weeks after ICH, the CBD-BDNF group exhibited the highest 68Ga-RGD uptake, which was associated with angiogenesis-induced increased integrin αvβ3 expression.
99TCm-ECD perfusion imaging was performed to provide information regarding brain hemodynamics in vivo. 36 Four weeks after ICH, the perfusion of the injured side was improved markedly in the CBD-BDNF treatment group. Interestingly, the localization of 68Ga-RGD uptake perfectly matched the edge of the lesion, as evidenced by decreased 99TCm-ECD uptake, suggesting that angiogenesis occurred right at the edge of the cerebral lesions. Data demonstrated that there were more functional vessels. IHC staining also suggested that there were more CD31- and VEGF-positive endothelial cells in the peri-hematoma region of the CBD-BDNF group 4 weeks after ICH. CBD-BDNF widely improved perfusion and angiogenesis by promoting endothelial cell survival and inducing neoangiogenesis. 37
In this experiment, we verified the therapeutic effect of CBD-BDNF in a rat model of ICH using nerve function defect grades, MRI, molecular imaging, and IHC. The mechanisms by which CBD-BDNF treatment promoted the sensorimotor recovery may be related to enhancing the proliferation and differentiation of endogenous NPCs, promoting angiogenesis, and reducing edema. Taken together, these data suggest that CBD-BDNF could be a promising treatment for the repair of ICH.
Conclusions
In the rat ICH model, CBD-BDNF remained at a higher concentration in the hemorrhage hemisphere, and stimulated the proliferation and differentiation of endogenous NPCs in the SVZ. CBD-BDNF also improved perfusion and angiogenesis, and reduced cell loss and tissue loss, and improved the overall behavioral performance of the rats. As a result, CBD-BDNF could serve as an exciting potential treatment for ICH.
Footnotes
Acknowledgments
This work was supported by National High Technology Research and Development Program (“863” Program) of China (2013AA020106) and National Natural Science Foundation of China (81301061 and 81200916).
Disclosure Statement
No competing financial interests exist.