
Abstract
Implantation of ex vivo expanded and osteogenically differentiated mesenchymal stem cells (MSCs) for bone regeneration has drawbacks for clinical applications, such as poor survival of implanted cells and increased treatment expenses. As a new approach for bone regeneration that can circumvent these limitations, we propose dual delivery of substance P (SP) and bone morphogenetic protein-2 (BMP-2) to facilitate endogenous stem cell recruitment to bone defects by SP and subsequent in situ osteogenic differentiation of those cells by BMP-2. A heparin-conjugated fibrin (HCF) gel enabled dual delivery with fast release of SP and slow release of BMP-2, which would be ideal for prompt recruitment of endogenous stem cells in the first stage and time-consuming osteogenic differentiation of the recruited stem cells in the second stage. The HCF gels with SP and/or BMP-2 were implanted into mouse calvarial defects for 8 weeks. Local delivery of SP to the calvarial defects using HCF gel was more effective in recruiting MSCs to the calvarial defects than intraperitoneal or intravenous administration of SP. Many of the cells recruited by SP underwent osteogenic differentiation through local delivery of BMP-2. The efficacy of in vivo bone regeneration was significantly higher in the SP/BMP-2 dual delivery group. The dual delivery of SP and BMP-2 using the HCF gel therefore has potential as an effective bone regeneration strategy.
Introduction
A
Such bone regeneration requires two main events, that is, endogenous stem cell mobilization/homing to a bone defect and subsequent osteogenic differentiation of the recruited stem cells. Therefore, we designed a dual delivery system that can release a stem cell recruiting factor first, followed by an osteogenic differentiation inducer. For the stem cell mobilization/homing step, we used substance P (SP), a small peptide that is known to function as a chemotactic factor for mobilizing MSCs to the circulation. 8 SP has been reported to be effective in tissue regeneration by promoting recruitment of MSCs to damaged tissues,9,10 which makes it an ideal candidate agent for promoting endogenous stem cell mobilization/migration in our system. For the osteogenic differentiation inducer, we used bone morphogenetic protein-2 (BMP-2), which is a well-known growth factor that induces osteogenic differentiation of stem cells. 11 However, the in vivo half-life of BMP-2 is relatively short, 12 and in vitro osteogenic differentiation of stem cells by BMP-2 requires several weeks. 13 To address these issues, we used a heparin-conjugated fibrin (HCF) gel to achieve sustained delivery of BMP-2 for effective bone regeneration. We had previously developed the HCF gel and found it to be effective in achieving sustained release of BMP-2. 14 The sustained release of BMP-2 from the HCF gel appeared to be based on an interaction between the heparin in the HCF gel and the heparin-binding motif of BMP-2. 15 However, because SP is a short peptide that lacks a heparin-binding motif, we expected the release profile of SP from the HCF to be different from that of BMP-2. In this study, we locally delivered SP and BMP-2 to calvarial defects in mice by using the HCF gel to determine whether the dual delivery of the stem cell recruiting factor (SP) and the osteogenic differentiation inducer (BMP-2) would facilitate bone regeneration even without exogenous stem cell transplantation. The bone regeneration efficacy was compared among experimental groups by various analytical methods (Table 2).
HCF, heparin-conjugated fibrin; qRT-PCR, quantitative real-time polymerase chain reaction; SP, substance P.
Materials and Methods
Synthesis of the HCF gel
Heparin (molecular weight, 4000–6000; Sigma, St. Louis, MO) was covalently bonded to bovine fibrinogen (Sigma; F8630) as previously described. 14 Briefly, heparin (100 mg) was dissolved in a buffer (100 mL, pH 6) composed of 0.05 M 2-morpholinoethanesulfonic acid (Sigma). N-hydroxysuccinimide (0.04 mM; Sigma) and 1-ethyl-3-(3-dimethylaminopropyl)-carbodiimide hydrochloride (0.08 mM; Sigma) were added to the solution to activate the carboxylic acid groups of the heparin. After 12 h of reaction at 4°C, the solution was stirred to homogeneity, and the product was precipitated with excess anhydrous acetone and lyophilized. Fibrinogen (100 mg; Sigma) was dissolved in phosphate-buffered saline (PBS, 20 mL, pH 7.4) at 4°C and reacted with activated carboxyl acid groups of the lyophilized heparin (60 mg) under the same conditions for 3 h. The product was precipitated with a large excess of acetone and lyophilized. The resultant white powder was completely dissolved in PBS and dialyzed through a porous membrane bag (molecular weight cutoff, 12,000–14,000 Da; Spectrum Lab, Rancho Dominguez, CA) at 4°C for 24 h to remove residual heparin. Finally, heparin-conjugated fibrinogen was lyophilized for 48 h. The HCF gel was formed by mixing heparin-conjugated fibrinogen (40 mg/mL) and normal fibrinogen (60 mg/mL) with factor XIII (88 U/mL), aprotinin (100 KIU/mL), calcium chloride (6 mg/mL), and thrombin (500 IU/mg). The ratio of heparin-conjugated fibrinogen and normal fibrinogen was 1:1 (v/v), and the final fibrinogen concentration of the HCF gel was 15 mg/mL. To form HCF, normal fibrinogen, in addition to heparin-conjugated fibrinogen, was also added for enhancing mechanical properties of the formed HCF.
Release profiles of SP and BMP-2 from the HCF gel in vitro
The release profiles of SP (Millipore Corp., Billerica, MA) and BMP-2 (Cowell Medi Co., Busan, Korea) from the HCF gel were determined by enzyme-linked immunosorbent assays (ELISA; R&D Systems, Inc., Minneapolis, MN). SP- and BMP-2 were added in the heparin-conjugated fibrinogen solution (2 μg SP and/or 2 μg BMP-2/1 mL of HCF) and mixed with normal fibrinogen (60 mg/mL) with factor XIII (88 U/mL), aprotinin (100 KIU/mL), calcium chloride (6 mg/mL), and thrombin (500 IU/mg). BMP-2 was dissolved in heparin-conjugated fibrinogen solution at 4°C for 2 h and then mixed with thrombin solution for gelation. The final volume of the hydrogels used for in vitro release test was 1 mL. The SP- and BMP-2-loaded HCF gel was immersed in a 2-mL microcentrifuge tube containing 1.5 mL of PBS, and the tubes were incubated at 37°C with continuous agitation to minimize the concentration gradients of the released SP or BMP-2 in the PBS.16,17 At various time points, the supernatant was collected and fresh buffer was added to the microcentrifuge tubes. The concentrations of SP and BMP-2 in the supernatants were determined by ELISA.
MSC culture
Before cell migration assay, MSCs were cultured in a growth medium consisting of high-glucose Dulbecco's modified Eagle's medium (DMEM; Gibco BRL, Grand Island, NY), 10% (v/v) fetal bovine serum (FBS; Gibco BRL), 100 U/mL of penicillin, and 100 μg/mL of streptomycin.
In vitro cell migration assay
To test the effect of SP on in vitro cell migration, 1×104 human bone marrow-derived mesenchymal stem cells (hBMMSCs; Lonza, Inc., Allendale, NJ, passage number=5) were seeded in the upper chamber of a collagen-coated transwell with a pore size of 3.0 μm (Corning, Inc., New York, NY), and SP (2.0 μg/mL), BMP-2 (2.0 μg/mL), or both was added to the lower chamber. 18 The culture medium was DMEM (Gibco BRL) supplemented with 10% FBS (Gibco BRL) and 1% penicillin/streptomycin. After 3 days of culture, the cells that remained on the top surface of the porous membrane of the upper chamber were removed using a cotton swab, and the migrated cells that moved through the pores of the porous membrane and attached on the bottom surface of the porous membrane were fixed with methanol for 5 min and stained with crystal violet (Sigma) for 30 min. 19 The stained cells were counted at high magnification (×20). Cells were counted in four fields per sample, and the counts were averaged.
Mouse calvarial defect model for evaluating SP-induced MSC migration in vivo
The mouse calvarial defect model was as previously described. 20 Six-week-old Institute of Cancer Research mice (Koatech, Kyunggi-do, Korea) were anesthetized with xylazine (20 mg/kg) and ketamine (100 mg/kg). After the scalp hair was shaved, a longitudinal incision was made in the midline of the cranium from the nasal bone to the posterior nuchal line, and the periosteum was elevated to expose the surface of the parietal bones. Using a surgical trephine burr (Ace Surgical Supply Co., Brockton, MA) and a low-speed micromotor, two circular transosseous defects (diameter, 4 mm) per mouse were produced in the skull. The defect size corresponded to the critical defect size for the mouse calvarial defect model. 20 The drilling site was irrigated with saline, and the bleeding points were electrocauterized. The animals were divided into four groups with five mice per group: no SP, SP (intraperitoneal [i.p.]), SP (intravenous [i.v.]), and SP (HCF, 100 μL). The no SP group received HCF gel implantation only, the SP (i.p) group received i.p. injection of SP (0.2 μg/mouse), the SP (i.v.) group received i.v. injection of SP (0.2 μg/mouse), and the SP (HCF) group received SP (0.2 μg)-loaded HCF gel ([2×0.2 μg/gel]/mouse). The dose of SP was proven to be optimal for MSC recruitment and bone regeneration, respectively. 8 The skin was then closed with resorbable 6-0 Vicryl sutures (Ethicon, Edinburgh, United Kingdom). The animal study was approved by the Institutional Animal Care and Use Committee at Seoul National University (#120305-5).
Flow cytometric analysis
The implanted HCF gel was retrieved 3 days after implantation for analysis of the infiltrated cells. The retrieved HCF gel was digested with 1.25 mg/mL collagenase type I (Worthington Biochemical Corp., Lakewood, NJ) at 37°C for 2 h to isolate the infiltrated cells. After blocking with 3% (w/v) bovine serum albumin (BSA) in PBS at room temperature for 30 min, the cells were treated with FITC-labeled anti-CD29 antibody (1:100 dilution; Abcam, Cambridge, United Kingdom), PE-labeled anti-CD45 antibody (BD Biosciences, San Jose, CA), PE/Cy7-labeled anti-CD44 antibody (Biolegend, San Diego, CA), and APC-labeled anti-CD90 antibody (Biolegend) on an ice bath for 30 min. After washing with 0.1% BSA/PBS, the cells were analyzed with a flow cytometer (FACS Calibur; BD Biosciences) equipped with the ImageQuest software (BD Biosciences).
Western blot analysis
The retrieved tissue samples at 3 days after implantation were lysed using a Dounce homogenizer (50 strokes, 4°C) in ice-cold lysis buffer (15 mM Tris HCl [pH 8.0], 0.25 M sucrose, 15 mM NaCl, 1.5 mM MgCl2, 2.5 mM EDTA, 1 mM EGTA, 1 mM dithiothreitol, 2 mM NaPPi, 1 μg/mL pepstatin A, 2.5 μg/mL aprotinin, 5 μg/mL leupeptin, 0.5 mM phenymethylsulfonyl fluoride, 0.125 mM Na3VO4, 25 mM NaF, and 10 μM lactacystin). Protein concentration was determined using a bicinchoninic acid (BCA) protein assay (Pierce Biotechnology, Rockford, IL). Equal protein concentrations from each sample were mixed with Laemmli sample buffer, loaded, and separated by sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) on a 10% (v/v) resolving gel. Proteins separated by SDS-PAGE were transferred to an Immobilon-P membrane (Millipore Corp.) and then probed with antibodies against CD29 (Abcam), Runx2 (Abcam), osteocalcin (Abcam), PPARγ (Abcam), collagen type II (Abcam), and Ly6G (neutrophils; Abcam) for 1 h at room temperature. The membranes were incubated with horseradish peroxidase-conjugated secondary antibody (Santa Cruz Biotechnology, Santa Cruz, CA) for 1 h at room temperature. The blots were developed using an enhanced chemiluminescence detection system (Amersham Bioscience, Piscataway, NJ). Luminescence was recorded on X-ray film (Fuji super RX; Fujifilm Medical Systems, Tokyo, Japan) and bands were imaged using a densitometer (Model GS-690; BioRad, Hercules, CA).
Quantitative real-time polymerase chain reaction for cells infiltrating into the HCF gel
To characterize the cells that infiltrated into the HCF gel, quantitative real-time polymerase chain reaction (qRT-PCR) was performed. Total RNA extracted from the cells was reverse-transcribed into cDNA. The expression of CD29, CD140b, and CD45 was examined to determine whether the cells had characteristics of MSCs. Since the CD45 is an hematopoietic stem cell marker, we considered that CD29+/CD45− and CD140b+ cells were considered as MSCs.21,22 The expression of osteocalcin (osteogenic differentiation), PPARγ (adipogenic differentiation), and collagen type II (chondrogenic differentiation) was examined to evaluate the multipotency difference of recruited MSCs. qRT-PCR was performed using the Step One Plus RT-PCR system (Applied Biosystems, Foster City, CA) with FAST SYBR Green PCR master mix (Applied Biosystems). The primers used are listed in Table 1.
In vitro multipotency of the cells infiltrating into the implanted HCF gel
For further analyses, cells infiltrating into the implanted HCF gel were retrieved and cultured as previously reported. 23 The implanted HCF gels were harvested 3 days after implantation and digested in 1.25 mg/mL collagenase type I for 2 h at 37°C to release the cells within the scaffold. The cells were then resuspended in culture medium and plated on tissue culture dishes. One hour later, the medium was changed to obtain adherent semipurified stromal cells. The cells were grown to confluence in 5% CO2 and 95% humidity at 37°C. After securing the cell amount, the differentiation capability of the cells that infiltrated into the implanted HCF gel was evaluated by culturing the cells in three different (adipogenic, osteogenic, and chondrogenic) differentiation media. The optimal seeding densities for differentiating MSCs into three different lineages were based on a previous report. 24 For adipogenic differentiation, the cells (2×105 cells/well) were cultured in DM-2 (Zen-Bio, Inc., Research Triangle Park, NC) medium for 14 days and then stained with oil red O to visualize cellular lipid accumulation. 25 For osteogenic differentiation, the cells (4×104 cells/well) were cultured for 14 days in DMEM-high glucose that was supplemented with 1 μM dexamethasone (Sigma), 0.05 mM ascorbic acid (Sigma), 10 mM β-glycerophosphate (Sigma), and 10% FBS and then subjected to von Kossa staining for detecting mineralization.26,27 For chondrogenic differentiation, the cells (5×105 cells/well) were incubated in chondrogenic medium consisting of low-glucose DMEM (Gibco BRL), 10 ng/mL transforming growth factor-β3 (R&D Systems, Inc.), dexamethasone (100 nM; Sigma), insulin-transferrin-selenium+1 premix (ITS, 1% [v/v]; Sigma), proline (40 mg/mL; Sigma), and ascorbate-2-phosphate (25 mg/mL; Sigma) in 15-mL polystyrene tubes for 4 weeks and stained with Weigert's iron hematoxylin and with safranin O for visualizing proteoglycans. 25
Measurement of proinflammatory factors in blood after delivering SP
The mouse calvarial defects were produced and the animals received SP (0.2 μg/mouse) in three different ways (i.p., i.v., and HCF loading) ([2×0.2 μg/gel]/mouse). The animals that received HCF implantation without SP loading served as untreated control. Three days after SP delivery, animals were sacrificed and blood samples were collected from the heart before euthanized. Blood samples were centrifuged at 1800 g for 20 min, and supernatants (100 μL) were subjected to cytokine array. Among the various cytokines that can be detected by the assay, those showing obvious differences between groups were selected and relative amounts were determined. The amount of proinflammatory factors in the blood was measured using Proteome Profiler Mouse Cytokine Array, Panel A (ARY006; R&D Systems, Inc.) according to the manufacturer's instructions. Western blot analysis for a neutrophils marker (Ly6G) was also performed to confirm the inflammatory status of the i.v. injection of SP.
Mouse calvarial defect model for evaluating bone regeneration
After calvarial defects were created, the animals were treated with SP and/or BMP-2. The animals were divided into eight groups (five mice/group, two calvarial defects/mouse): the control group (HCF gel only [100 μL], no BMP-2, or SP), SP delivery groups with three different modes of delivery, the BMP-2/HCF delivery group, and three groups that received SP in combination with BMP. SP delivery (0.2 μg/mouse) was performed intraperitoneally, intravenously, and via the HCF gel ([2×0.2 μg/gel]/mouse). For all BMP-2 delivery groups, BMP-2 (0.2 μg/100 μL HCF gel) was loaded into the HCF gel before implantation.
Bone formation analysis
Eight weeks after the implantation, the mice were sacrificed and the implants were retrieved and fixed in 4% paraformaldehyde. Bone formation was evaluated using soft X-ray radiography (Softex; Sofron, Tokyo, Japan), microcomputed tomography (micro-CT) scanning (SkyScan-1172; Skyscan, Kontich, Belgium), histological analysis, and immunohistochemical analysis. Radiograms of the implants were obtained using a soft X-ray apparatus. CT images were obtained with a micro-CT system. The CT system was operated at a voltage of 40 kV and a current of 250 mA. After examination with soft X-ray radiography and micro-CT, the HCF implants were retrieved (5 mice/group=10 HCFs/group) and then used for histological analysis (5 HCFs/group) and immunohistochemical analysis and hematoxylin and eosin (H&E) staining (5 HCFs/group). The bone formation volumes were measured by micro-CT analyzer program (Skyscan). The specimens were embedded in paraffin and transversely sectioned to obtain 4-μm-thick sections; the sections were examined after Goldner's trichrome staining. The bone formation area was measured using an image analysis system coupled to a light microscope. The bone formation area was expressed as the percentage of bone area in the total cross-sectional area [(bone area/total area)×100%]. The specimens for immunohistochemical analysis were embedded in optimal cutting temperature compound (Tissue-Tek; Sakura Finetek, Alphen aan den Rijn, Netherlands) at −20°C and transversely sectioned to obtain 10-μm-thick sections. The tissue sections were immunohistochemically stained with antibodies against mouse-specific osteocalcin (Abcam). Immunoreactivity was visualized using a fluorescein isothiocyanate-conjugated secondary antibody (Jackson ImmunoResearch Laboratories, Inc., West Grove, PA). The slides were counterstained with DAPI (Vector Laboratories, Burlingame, CA) to stain the nuclei of cells and photographed using a fluorescence microscope (IX71 inverted microscope; Olympus, Tokyo, Japan).
Statistical analysis
All of the quantitative data are expressed as the mean±standard deviation of at least four independent experiments. For the two-group comparisons, two-sided t-tests were used, whereas one-way ANOVA tests with Bonferroni corrections were performed for the comparison of more than three groups (OriginPro 8 SR4 software, version 8.0951; OriginLab Corporation, Northampton, MA). p<0.05 was considered to be statistically significant.
Results
In vitro release profiles of BMP-2 and SP
The 14 days in vitro release profiles of BMP-2 and SP from the HCF gel were compared. BMP-2 showed sustained release from the HCF gel, compared to SP (Fig. 1). BMP-2 was consistently released from the HCF gel for 14 days. During the first 3 days, most of the SP (89.9%±1.5%) was released from the HCF gel, whereas a relatively small amount of BMP-2 (15.8%±8.3%) was released. After 14 days, SP was almost completely released from the HCF gel, whereas more than 50% (57.8%±5.9%) of the loaded BMP-2 remained in the gel.
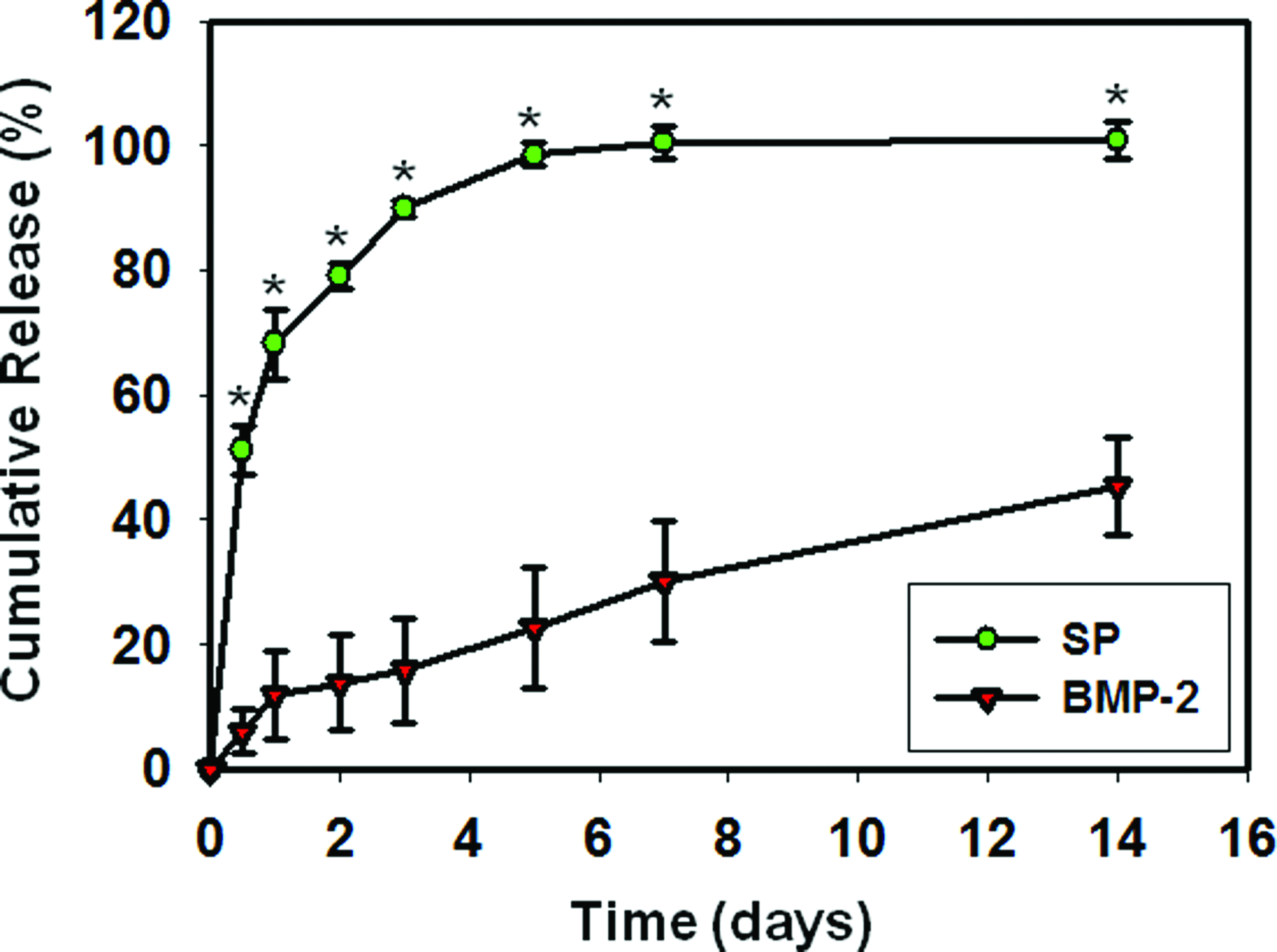
In vitro release profiles of BMP-2 and SP from the HCF gel. The SP- and BMP-2-loaded HCF gel was immersed in phosphate-buffered saline at 37°C with continuous agitation. At various time points, the supernatant was collected and the concentrations of SP and BMP-2 in the supernatants were determined by ELISA. SP and BMP-2 were released relatively quickly and slowly, respectively, which is relevant for stem cell recruitment to the HCF scaffolds and in situ osteogenic differentiation of the recruited stem cells. The percentage was calculated by dividing the measured amounts by the initially loaded amounts. Quantitative data have been provided as the mean±standard deviation values of three independent experiments. *p<0.05 versus BMP-2. BMP-2, bone morphogenetic protein-2; ELISA, enzyme-linked immunosorbent assay; HCF, heparin-conjugated fibrin; SP, substance P. Color images available online at www.liebertpub.com/tea
SP stimulated hBMMSC migration in vitro
The potency of SP for inducing migration of hBMMSCs that are known to be CD29+21 was evaluated. The test scheme is depicted in Figure 2A. BMP-2 treatment was included to determine the possible positive or negative effects of using BMP-2 with SP in terms of cell migration. After 3 days, SP induced obvious cell migration regardless of BMP-2 treatment (Fig. 2B). The number of cells that migrated in the SP-alone treated group (122.8±15.6 cells/field) or the SP/BMP-2 treated group (121.5±12.2 cells/field) was significantly higher than that in the control group (no treatment, 35.9±7.5 cells/field) or the BMP-2-only treated group (54.6±9.7 cells/field) (Fig. 2C).
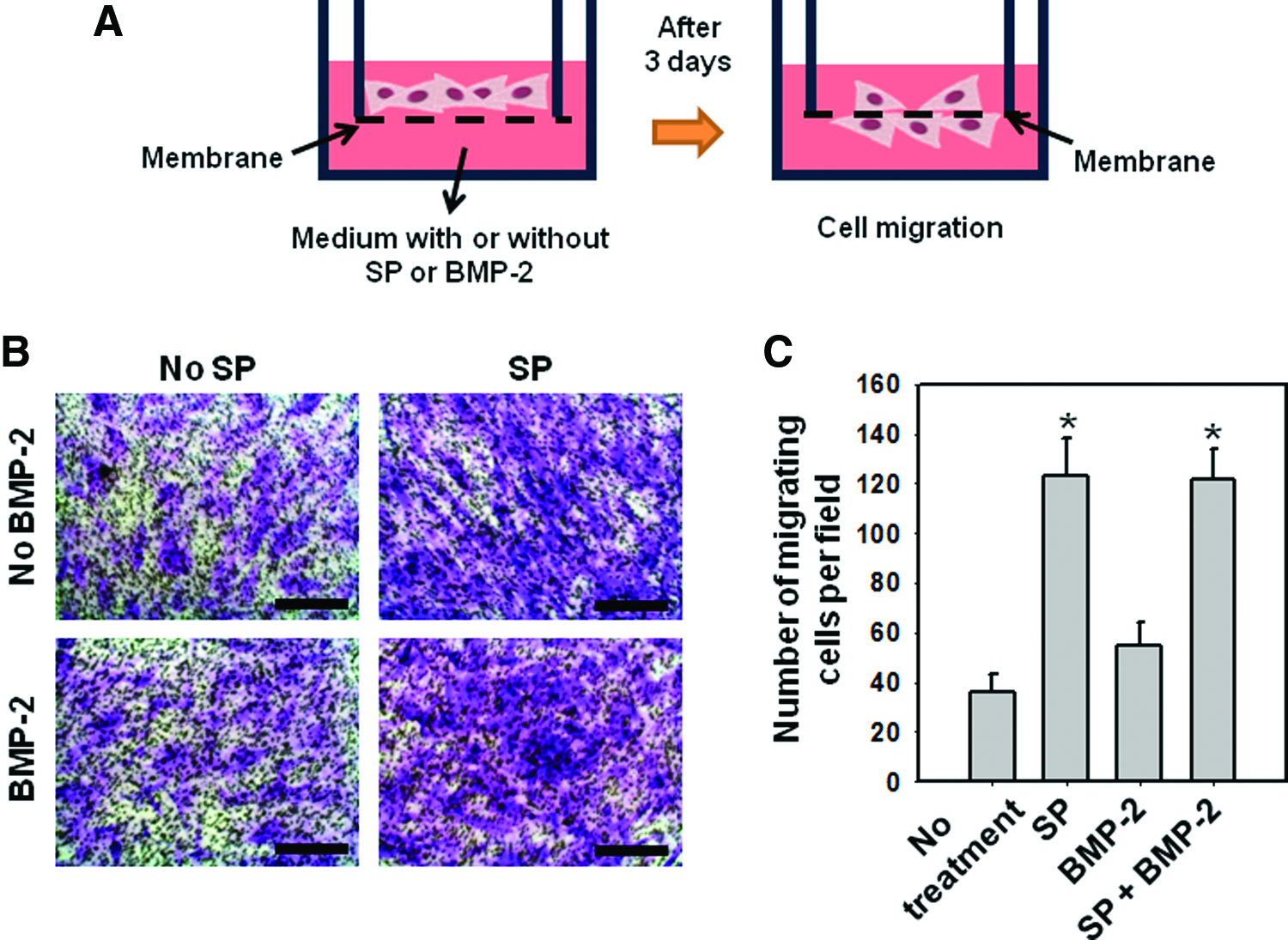
In vitro hBMMSC migration stimulated by SP.
Flow cytometric analysis of cells that infiltrated into HCF scaffolds
To determine whether SP stimulates MSC recruitment, cells retrieved from the HCF gel implanted in mice, treated with SP via three different methods, were analyzed (Fig. 3). FACS analysis of CD29, an MSC marker, and CD45, a hematopoietic stem cell marker, 22 showed that the percentage of CD29+/CD45− cells in the SP (HCF) group (0.96%±0.73%) was significantly higher than that of the other groups [0.04%±0.03%, 0.04%±0.03%, and 0.32%±0.40% for the no-SP, SP (i.p.), and SP (i.v.) groups, respectively] (Fig. 3B). Additionally, most of the CD29+/CD45− cells were also positive for CD90 and CD44, both of which are MSC markers, 28 and the portion of the CD90+/CD44+ cells was considerably higher in the SP (HCF) group (Fig. 3C). Western blot analysis performed at 3 days after implantation confirmed that recruitment of CD29+ cells was enhanced in the SP (HCF) group compared with groups of no SP, SP (i.p.), and SP (i.v.) (Fig. 3D).
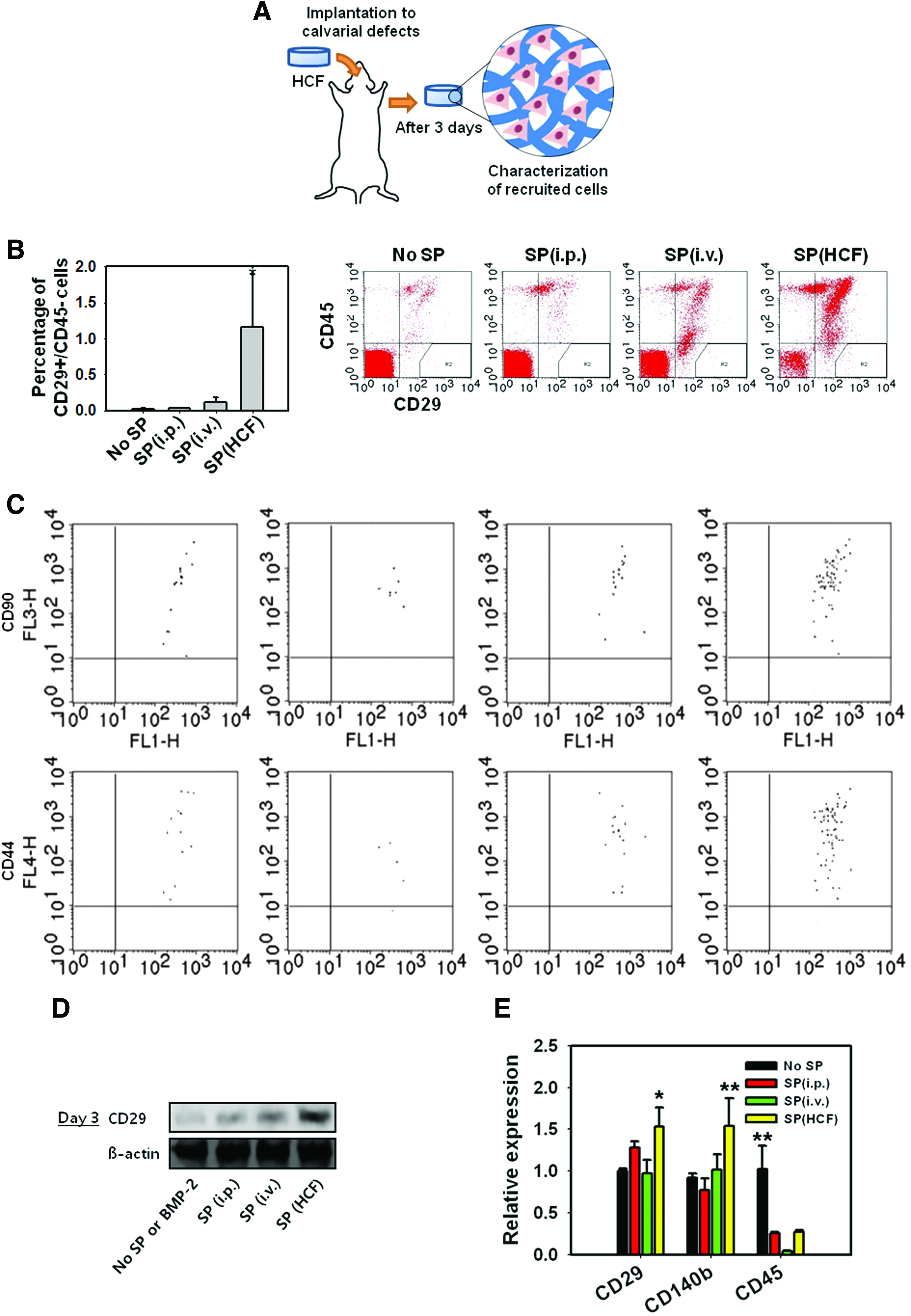
In vivo MSC recruitment stimulated by SP.
Characterization of HCF-infiltrated cells: qRT-PCR and in vitro multipotency test
Cells isolated from the HCF were cultured for 1 week, and the expression of MSC-related markers was examined. CD140b was used as an MSC marker. 22 The SP (HCF) group showed significantly higher expression of both CD29 and CD140b than the control group, whereas the expression of CD45 was significantly lower in the SP (HCF) group (Fig. 3E). To determine whether the cells that infiltrated into the HCF gel had differentiation potency, differentiation into three different lineages (osteogenic, adipogenic, and chondrogenic) was induced using specific differentiation media (Fig. 4A, B). The degree of differentiation was estimated based on the results of staining for calcium deposition (osteogenic), lipid accumulation (adipogenic), and proteoglycan deposition (chondrogenic). The cells in the control group (no SP) did not differentiate into any of the lineages, and the cells in the SP (i.p.) and SP (i.v.) groups showed relatively low adipogenic, osteogenic, and chondrogenic differentiation potency. The extent of differentiation was highest in the SP (HCF) group in all three cases (Fig 4A, B). Before inducing the differentiation of the recruited cells, the cells did not express the osteogenic, adipogenic, and chondrogenic markers (Fig. 4C).

Multipotency of the cells recruited by SP to the implanted HCF gel. Cells were isolated from the explanted HCF gel at 3 days after implantation into calvarial defects. After in vitro culture of the collected cells, the cells were evaluated for osteogenic (von Kossa staining and osteocalcin), adipogenic (oil red O staining and PPARγ), and chondrogenic (safranin O staining and collagen type II) differentiation by
Effect of different modes of SP delivery on systemic inflammation status
According to our data, i.v. injection of SP resulted in obvious increase of serum proinflammatory factors known to recruit inflammation-related cells and immune cells, compared with other groups (Fig. 5). The proinflammatory factors that showed prominent increase after i.v. injection of SP were chemokine (C-X-C motif) ligand 1 and 9 (CXCL129 and CXCL930), chemokine (C-C motif) ligand 1, 2, and 12 (CCL1, 31 CCL2, 32 and CCL1233), and IL-16. 34 Western blot analysis for a neutrophils marker (Ly6G) confirms the inflammatory status of the i.v. injection of SP (Fig. 5B).

Effect of different modes of SP delivery on systemic inflammation status. The relative amount of proinflammatory factors present in blood.
BMP-2 induced in vivo osteogenic differentiation of cells that infiltrated into the HCF
Eight weeks after implantation, HCF was retrieved and cross sectioned for immunohistochemical analysis. The sections were stained for osteocalcin, an osteogenic marker, and the resulting images were merged with images of DAPI staining (Fig. 6). Without BMP-2 treatment, SP alone did not induce obvious osteocalcin expression regardless of how it was delivered. In contrast, when BMP-2 was used, the expression of osteocalcin increased in all groups, and the SP (HCF gel)/BMP-2 group showed the highest osteocalcin expression relative to the other groups.
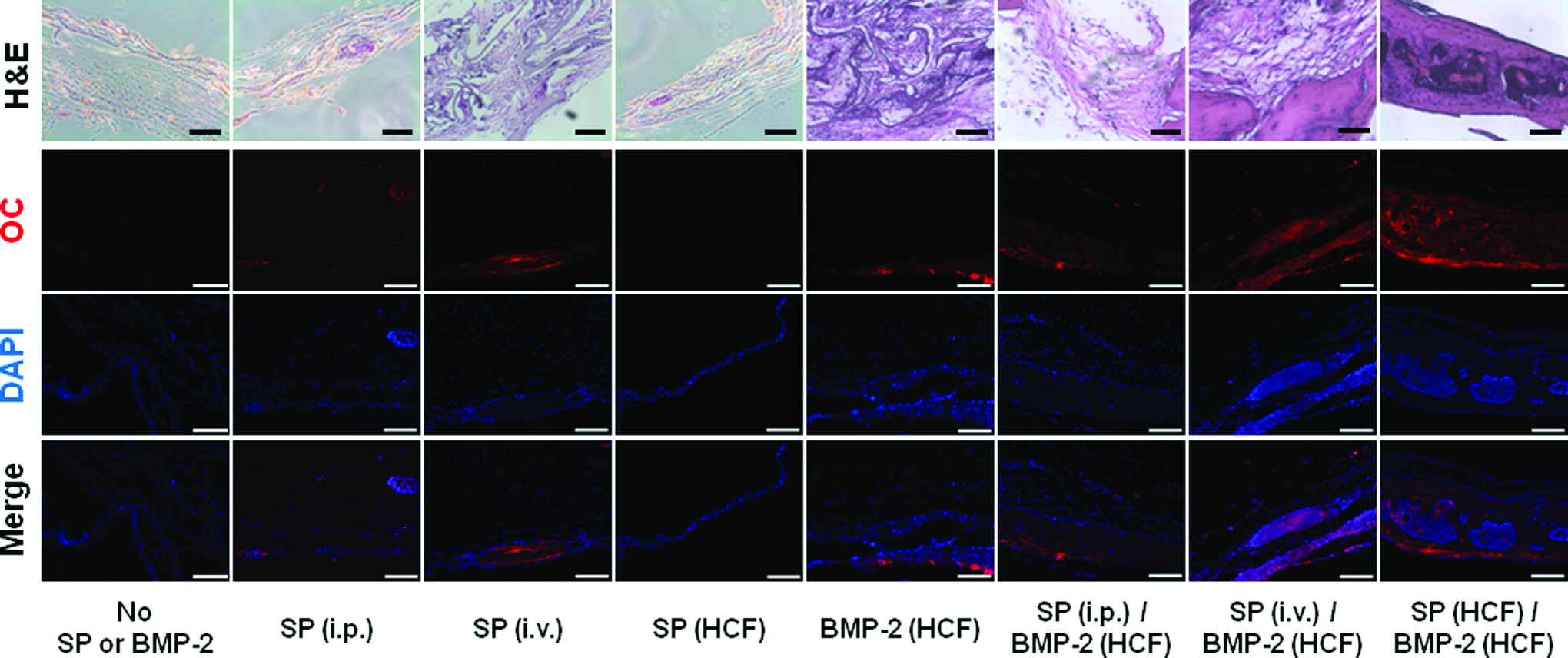
Osteogenic differentiation of cells infiltrating into the HCF gel that was implanted in calvarial defects for 8 weeks. The tissue regenerated in the defects was immunostained for osteocalcin (OC) (red). Cell nuclei were counterstained with DAPI (blue). Dual delivery of SP and BMP-2 induced an apparent increase in osteocalcin expression relative to that for all the other groups. Scale bars=100 μm. Above the fluorescence staining, H&E staining images were added for showing more details about regenerated bone tissue. H&E, hematoxylin and eosin. Color images available online at www.liebertpub.com/tea
In vivo bone regeneration
Eight weeks after implantation, calvarial defects were examined by soft X-ray radiography (Fig. 7A) and micro-CT (Fig. 7B), showing significantly higher bone regeneration in the SP (HCF gel)/BMP-2 treatment group than the other groups. This was further verified by histological analysis using Goldner's trichrome staining (Fig. 7).
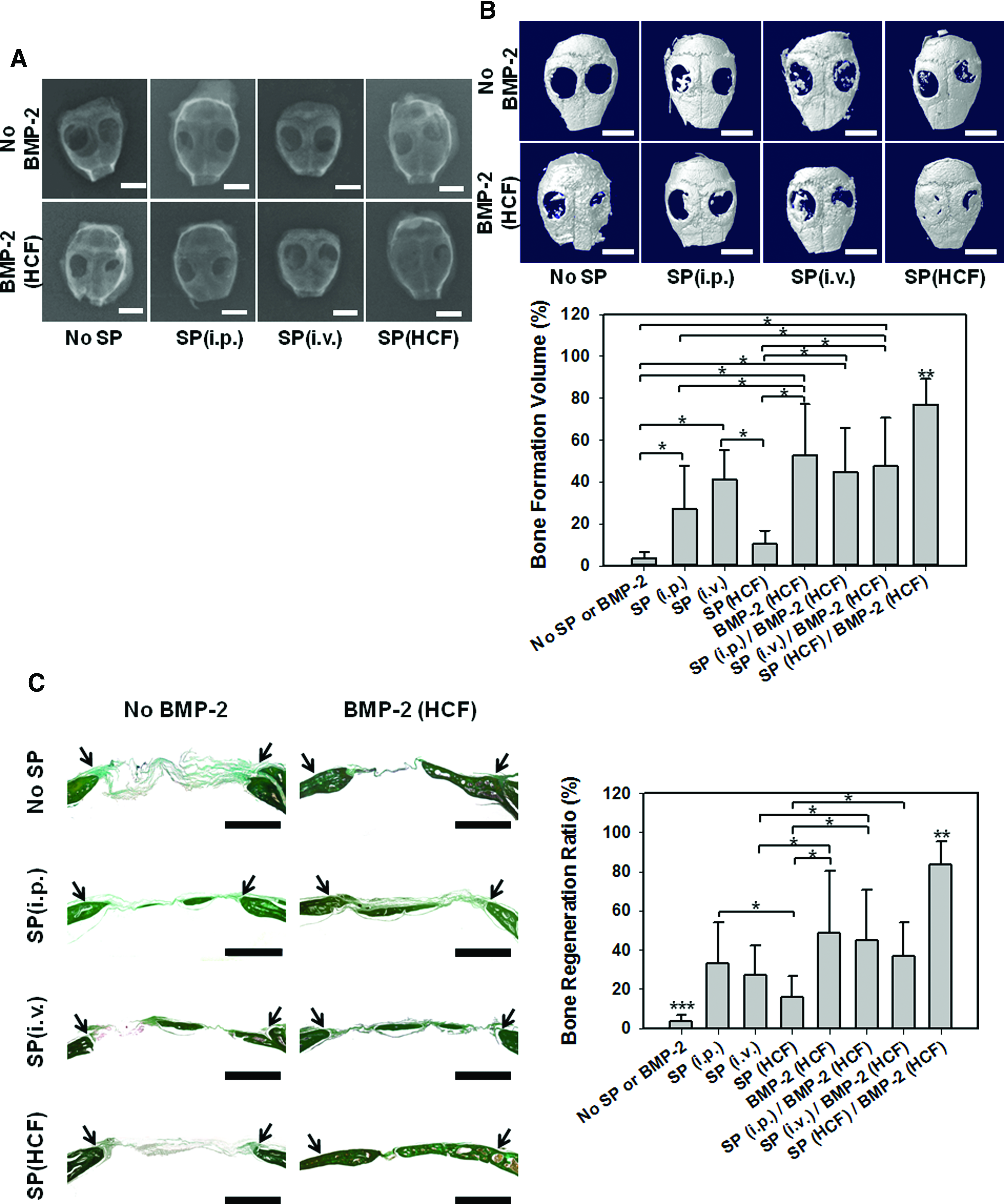
Evaluation of in vivo bone formation following implantation of HCF into mouse calvarial defects for 8 weeks.
Discussion
In this study, dual delivery of SP and BMP-2 using the HCF gel significantly enhanced bone regeneration in a mouse calvarial model. Although stem cell implantation can be used to induce bone regeneration, laborious ex vivo cell manipulation and culture processes make it costly and inconvenient for clinical use. The in situ tissue regeneration we envisioned in this study involves endogenous stem cell mobilization/homing and subsequent differentiation into appropriate lineages for the regeneration or replacement of damaged tissues. Thus, the first requirement for in situ tissue regeneration is to provide an appropriate stimulus for recruitment of endogenous stem/progenitor cells into the target area for tissue regeneration.35,36 SP has been reported as a systemically acting injury-inducible wound messenger that can accelerate wound healing. 8 A previous study reported that SP recruits CD29+ stromal-like cells from the periphery to the site of injury, resulting in accelerated wound healing. 8 In this study, SP, which is known to recruit MSCs from bone marrow to circulation, 37 was used as a chemotactic agent. Granulocyte colony stimulating factor (G-CSF) and granulocyte macrophage colony stimulating factor (GM-CSF) are representative factors that can recruit endogenous cells such as stromal-like cells in vivo. However, the use of G-CSF and GM-CSF is discouraged due to their association with toxicity (i.e., thrombocytopenia). 38 Unlike G-CSF and GM-CSF, SP has been shown to elicit lower toxicity within a dose range that shows similar effectiveness at recruiting progenitors. 39 A previous report has shown that tissue regeneration efficacy is dependent on the SP dose. 8 Therefore, in our study, we used the identical dose of SP that was previously optimized for tissue regeneration. 8 Additionally, BMP-2, which has been reported to induce osteogenic differentiation of stem cells, was used to induce osteogenic differentiation of endogenous stem cells recruited by SP to the bone defects. We have previously reported that local delivery of BMP-2 to a site transplanted with peripheral blood mononuclear cells (PBMNCs), which are known to contain osteogenic progenitors, 40 induced in situ osteogenic differentiation of the transplanted PBMNCs. 41 For the sufficient osteogenic differentiation of MSC, the release period of BMP-2 is important. 9 BMP-2 should be released at a sufficiently high level for a long period to ensure osteoprogenitor migration to the defect site and osteogenic differentiation.3,42 Additionally, higher dose of BMP-2 showed higher amount of in vivo bone formation, however, side effects of BMP-2 also increased. 12 The high dose of BMP-2 contributes to several side effects including bone formation with spinal cord impingement, bone resorption, cervical swelling, and cyst-like bone void formation. 43 Therefore, optimal dose and BMP-2 delivery system are required.
Our data showed that SP treatment significantly increased hBMMSC migration in vitro (Fig. 2) and that local delivery of SP in vivo using the HCF gel significantly increased the number of MSCs that infiltrated into the implanted HCF gel, relative to other SP delivery groups (Fig. 3). These data indicate that if the same amount of SP is used, local delivery of SP to the target area is advantageous over systemic delivery in inducing endogenous stem cell recruitment. There may be a threshold concentration of SP for inducing stem cell homing that may be reached at the target area through systemic delivery of SP. However, systemic delivery of SP would require a relatively higher amount of SP to reach the same local concentration, which may produce a serious inflammatory response. 20 In fact, i.v. injection of SP resulted in obvious increase of the blood proinflammatory factor level compared with other groups that received same amount of SP by either i.p. injection of HCF loading (Fig. 3). Since these increased factors are known to recruit various types of cells involved in inflammatory process and immune response, including, but not limited to, neutrophils, monocytes, T cells, and lymphocytes,29–34 these data support our speculation and local delivery appears to be a logical choice for delivering SP for tissue regeneration.
Because the recruitment and in situ osteogenic differentiation of endogenous stem cells should occur in sequence in the system we designed, we chose the HCF gel as a carrier for both SP and BMP-2. For fast bone regeneration, SP should be released quickly from the HCF gel after implantation to attract endogenous stem cells to the HCF implanted in bone defects. In contrast, BMP-2 should be released in a slow sustained manner for weeks because long-term delivery of BMP-2 promotes efficient osteogenic differentiation of stem cells. 20 We had previously reported that the HCF gel utilizes the interaction between heparin and BMP-2 to provide sustained release of BMP-2 over several weeks. 14 A previous report has shown that the degradation period of HCF was appropriate for bone regeneration. 44 The volume of HCF gel was maintained more than 9 days after in vivo implantation. 44 Sustained release of BMP-2 from HCF can be explained by two main reasons. One is that BMP-2 is released mechanically through degradation of HCF gel. 20 The other is that the interaction between heparin and protein. Two contiguously identical amino acid sequences present in heparin-binding proteins, that is, XBBXBX and XBBBXXBX (B is a basic amino acid and X is a hydropathic amino acid), 15 induce folding of the proteins to spatially place the basic amino acids for binding with heparin. 45 Because SP, which is composed of 11 amino acids (Arg Pro Lys Pro Gln Gln Phe Phe Gly Leu Met), 46 does not fulfill the condition, we expected the release profile of SP from HCF to be different from that of BMP-2. The different release profiles of SP and BMP-2 from HCF (Fig. 1) demonstrate that HCF is an optimal carrier for achieving dual differentiated release of SP and BMP-2 for bone regeneration as we intended. Additionally, the gel-type nature of HCF makes it possible to fill irregularly shaped bone defects. Other BMP-2 delivery carriers for calvarial defect regeneration include PLGA scaffold, chitosan-poly(ethylene oxide) hydrogel, 47 and poly(ethylene glycol)-based hydrogel. 48 These carriers showed faster release of BMP-2 than HCF or need further modification to control the BMP-2 release. Compared to the previous carriers, our HCF showed significantly enhanced bone formation volume (∼70% and 63% vs. 80%). To improve the low mechanical properties of the HCF gels, compared with the other BMP-2 delivery carriers, such as β-tricalcium phosphate or ceramics, HCF gels would have to be further modified for bone defects that are subjected to high mechanical stresses.
The efficacy of SP/BMP-2 dual delivery using the HCF gel in bone regeneration was higher than that of conventional BMP-2 treatment (Fig. 7), probably because the osteogenic effect of BMP-2 applied without a stem cell recruiting agent was not sufficient for inducing full-scale bone regeneration when the size of the bone defect is critical. Consequently, the endogenous stem cell recruitment/in situ differentiation approach can be a powerful alternative, not only to exogenous stem cell implantation but also to conventional BMP-2 treatment. The dual delivery of SP and BMP-2 was effective for bone formation in critical-sized bone defects in this study. SP promotes MSC migration (Fig. 2) to tissue regeneration site. 8 BMP-2 has an osteoinductive potential for inducing MSCs to differentiate into osteoblast lineage. 49 MSCs recruited to the bone defect sites by SP would be induced to regenerate bone by BMP-2. The delivery of BMP-2 only resulted in less bone formation than the dual delivery (Fig. 7). This could be due to limitation in osteoblast migration from the defect margin, which was induced by BMP-2, in critical-sized defects in the BMP-2 (HCF) group. MSC migration to the bone defect site by SP would be necessary for bone regeneration.
Conclusions
We propose dual delivery of SP and BMP-2 to enhance endogenous stem cell recruitment to bone defects by SP and subsequent in situ osteogenic differentiation of those cells by BMP-2. The bone regeneration efficacy was significantly enhanced by SP/BMP-2 dual delivery. The dual delivery of SP and BMP-2 using the HCF gel therefore has potential as an effective bone regeneration strategy.
Footnotes
Acknowledgments
This work was supported by a grant (HI12C0199) from the Ministry of Health, Welfare, and Family Affairs, the Republic of Korea, and a grant (2010-0020352) from the National Research Foundation of Korea.
Disclosure Statement
No competing financial interests exist.