
Abstract
Heart failure due to Myocardial Infarction (MI) remains the leading cause of death worldwide due to the inability of myocardial tissue to regenerate following infarction. Current therapies could only retard the progression of disease, but fails to bring functional improvement and cardiac regeneration. The present study analyzes the potentials of Poly(glycerol sebacate)/Fibrinogen (PGS/Fib) core/shell fibers as a structural support and initial entrapment of cells in an in vivo porcine model using echocardiography, histology, and immunohistochemistry. The echocardiography results showed the increased ejection fraction (EF) in PGS/Fib/VEGF/Cells compared with MI controls. The percentage increase in the End Diastolic Volume (EDV) dimension from post MI period to 4 weeks follow-up was the least in PGS/Fib/VEGF/Cells groups compared with MI and cell control group proving that the PGS/Fib/VEGF/Cells group restored the left ventricle (LV) function after MI, evident from the improvement in EF and prevention of LV enlargement. Further, immunohistochemistry results demonstrated that most of the transplanted mesenchymal stem cells (MSCs) within the PGS/Fib/VEGF scaffolds expressed cardiac marker proteins troponin and actinin and endothelial cell marker protein CD31 indicating differentiation of human bone marrow MSCs into cardiac cells and endothelial cells. The developed nanofibrous cardiac patch PGS/Fib/VEGF/Cells provides both functional and structural integrity to the infarcted myocardium and also serves as a suitable matrix for the entrapment of MSCs in clinical applications for cardiac tissue engineering.
Introduction
M
Cellular cardiomyoplasty is a technique used clinically, wherein cells are suspended in liquid solutions of saline or media and delivered through a catheter to the infarcted myocardium. Regardless of the method used, retention and survival of a considerable amount of cells injected into the ischemic myocardium is vital for any cellular therapy to utilize its full potential for cardiac regeneration. Various factors are responsible for the early loss of cells after transplantation in the ischemic myocardium. Among them and of significant importance is the lack of survival factors in the post MI. We have applied an alternative approach by the encapsulation of cells onto the PGS/Fibrinogen core/shell fibers, which has desirable mechanical and biological properties in a porcine model in vivo for cardiac tissue engineering applications. Studies conducted in the past on large animal models using tissue engineering strategy for cardiovascular constructs are listed in Table 1. Porcine hemodynamics, anatomic characteristics of chest cavity and heart resemble those of human, and hence were employed in the present study to prove the potentiality of PGS/Fibrinogen core/shell fibers for the regeneration of infarcted myocardium.
Adapted from Rashid et al. 30
A, angiography; EC, endothelial cell; H, histology; I, immunohistochemistry; PGA, polyglycolic acid; SMC, smooth muscle cell.
Tissue repair involves a complex cascade of biological events controlled by several growth factors and cytokines that provide local signals at the site of injury; such signals regulate the pathways and mechanisms that are responsible for wound healing and tissue regeneration. The infarcted area is an unfavorable environment for cell survival, homing, and tissue regeneration, and hence in situ injection of growth factors would be useful for endogenous or grafted cells to integrate, proliferate, or differentiate within the infarct area. For these reasons, vascular endothelial growth factor (VEGF) was employed in this study to promote angiogenesis and to overcome the complexity of ischemic environment. VEGF plays a key role in both vasculogenesis and angiogenesis8,9 and also therapies with VEGF for the treatment of ischemic diseases have attracted great attention. VEGF injection can transform the site of infarction into a favorable microenvironment for the recruitment of endogenous myofibroblasts and help to achieve effective revascularization. This engineered vascular niche would further attract new population of cardiomyocyte-like cells to home at the site of injection favoring cardiac regeneration. We have hypothesized that the combination of nanofibrous scaffolds as a cell carrier along with growth factors would provide structural integrity to the developing tissue and prevent loss of cells, favoring enhanced cardiac regeneration.
Materials and Methods
Myocardial infarction
The experimental protocols were approved by the Ethics Committee of the National University of Singapore. Farm pigs (Sus scrofa) (Yorkshire Swine) (30–40 kg) female were used for this study. Before creation of infarction, the animals were premedicated using Atropine sulfate (50 μg/kg, intramuscular [IM]), after which they were anesthetized using IM injection of TKX cocktail solution containing Tiletamine (250 mg), Zolazepam (250 mg), Ketamine (2.5 mL of 100 mg/mL), Xylazine (2.5 mL of 100 mg/mL) at a dosage of 0.05 mL/kg. A laryngoscope and endotracheal tube to intubate the pig and Isoflurane gas (2–3%) was used for maintenance. Medication in the form of antibiotics (Baytril 5% 5 mg/kg, IM) and analgesics (Tramadol 5 mg/kg, IM) was administered to the animal from day 0 before the surgery until 6 days postoperatively. During the creation of infarct, antiarrhythmic drugs (Amiodarone, 150 mg in 500 mL Dextrose 5%, IV) were infused throughout the procedure.
The animal was placed in a right lateral position (left side facing up) and the chest was opened by left thoracotomy through a 2 cm incision over fourth to fifth intercostal space. The pericardium was removed and heart was exposed for the creation of MI. The obtuse marginal (OM) branch of the proximal left circumflex coronary artery (LCX) was ligated using nonabsorbable sutures, to create 1–2 cm infarct at left ventricle (LV). Myocardial ischemia was identified by characteristic ST-segment changes on the ECG and regional myocardial color change. Sixteen pigs were used for the transplantation of fabricated fibrous scaffolds and cells. Three pigs died after the infarct creation, whereas one pig died during the implantation surgery. The dead animals were replaced so as to include three animals per experimental group. After implantation surgery, there was 100% rate of survival among all groups. At Day 0 (pre and postinfarction), week 2, and 4, about 3 mL of blood was collected from the ear vein of the animals and put into EDTA tubes for analysis of biochemical cardiac marker creatine kinase MB (CK MB) in blood to confirm the creation of MI.
The pigs were divided into the following groups–(1) myocardial infarction control (MI control), in which no implant was placed after the creation of infarct, (2) cells control, in which after the creation of MI mesenchymal stem cells (MSCs) at a seeding density of 10×106 cells were injected onto the four corners of the infarcted site of the myocardium, (3) PGS/Fibrinogen core/shell fibers, (4) PGS/Fibrinogen core/shell fibers with VEGF delivered through intramuscular (IM) injection at the four corners; 250 μL each (PGS/Fibrinogen/VEGF) and (5) PGS/Fibrinogen core/shell fibers with the addition of VEGF and MSCs at the same seeding density of 10×106 cells, at the four corners of the scaffold, 250 μL each (PGS/Fibrinogen/VEGF/Cells). Cyclosporin (5 mg/kg/day), was administered 5 days preoperatively and continued upto 4 weeks for the PGS/Fib/VEGF/Cells group and cells control groups. Before implantation, the degradation profile of the scaffolds was tested by immersing them in PBS buffer at a pH 7.4 and analyzing the morphology of the fibers by SEM. SEM analysis, the electrospun nanofibers were dehydrated using a series of ethanol gradients for 15 min each starting from 30%, 50%, 75%, 90%, to 100% ethanol. Hexamethyldisilazane (HMDS; Sigma) (100 μL) was added and allowed to air dry in fume hood overnight. The scaffolds were then sputter coated (JEOL JFC-1200 fine coater) and imaged using SEM (JEOL JSM–5600LV). Supplementary Figure S1a (Supplementary Data are available online at www.liebertpub.com/tea) shows the myocardial infarcted region created after LCX ligation in pigs. LCX artery ligated using a polyester suture and the infarction below the ligated region evident from the myocardial discoloration. Immediately after the creation of infarction, the fibrous cardiac patch was stitched at four corners of the infarct area of the heart. Supplementary Figure S1b shows the implantation of nanofibrous cardiac patch after MI. The muscles and fascia were then closed in a continuous manner using 2/0 and 0 absorbable sutures, respectively. The thoracic cavity was closed in an interrupted manner using 2/0 nonabsorbable sutures. The animals were then allowed to recover and follow up studies were done after second and fourth weeks.
Labeling of cells
Bone marrow-derived MSCs of human origin purchased from Lonza were cultured in low glucose Dulbecco's modified Eagle's medium (DMEM) supplemented with 10% FBS (GIBCO Invitrogen) and 1% antibiotic and antimycotic solutions (Sigma) in a 75-cm2 cell culture flask. Cells were incubated in CO2 incubator at 37°C at 5% CO2 and expanded till passage 3 to achieve more number of cells. Before implantation, MSCs were labeled with the fluorescent probe PKH26 Red Fluorescent Cell Linker (Sigma), following the supplier's protocols. PKH26 dye has an excitation maximum at 551 nm and emission maximum at 567 nm, which was used to detect the dye under fluorescent microscopy. After implantation of the nanofibrous scaffolds, VEGF and cells were injected at four corners of the nanofibrous patch using a 1-mL syringe, so that the cells get trapped within the nanofibers as indicated in the Supplementary Figure S1c.
Echocardiography
Transthoracic echocardiography (TTE) was performed on all animal models and care was ensured to avoid too much pressure on the thoracic cavity, which might trigger bradycardia. Two-dimensional (2D) images were captured with a 3S (1.5–3.6 MHz) phased array transducer using a Vivid 7 ultrasound (GE Vingmed). The standard parasternal long and short-axis views at different levels (basal, mid, apical) were observed and recorded. M-mode tracing was recorded at the mid level of the left ventricular short-axis view where LV regional wall thickness and diameter were measured. All images were captured in three cardiac cycles, stored digitally, and analysis was performed offline using the GE EchoPac (Version 7.0.1). Indexes of LV end systolic and end diastolic volumes (EDV) were calculated using length–area method from 2D images. LV ejection fraction (EF) was calculated as:
An echocardiography technician blinded to the treatment groups acquired the images and performed the data analysis. Echocardiography was performed before the creation of infarct (baseline), after infarction, 2 and 4 weeks after infarction. After 4 weeks, animals were sacrificed using intravenous delivery of Pentobarbital Sodium 300 mg/mL at 100 mg/kg, and the hearts were harvested. Supplementary Figure S1d, observed that the nanofibers are intact on the heart muscle after 4 weeks of implantation, these nanofibers providing mechanical and functional support to the infarcted myocardium. The LV was segmented into portions, and the region of interest alone having the implant was isolated as shown in Supplementary Figure S1e. The implant area was then cut into two portions of which one section was frozen and the other was fixed for further analysis.
Histology and Immunohistochemistry
Histological analysis tissues were fixed in 10% phosphate buffered formalin (Sigma). Sections were cut into 10 μm thickness and studied by Hematoxylin and Eosin (H&E) staining for analyzing the development of tissue and Masson's Trichrome staining for extracellular matrix (ECM) formation. H&E staining, the formalin fixed sections were washed in DI water followed by nuclei staining using alum Hematoxylin. The sections were then rinsed in running tap water for 5–10 min followed by a quick dip in 0.3% acid alcohol. The sections were again rinsed in running tap water followed by eosin staining for 2 min. The sections were then dehydrated and mounted on a mounting medium. Masson's Trichrome staining, the formalin fixed tissues were incubated in Bouin's solution for 1 h followed by rinsing in running tap water for 5–10 min. The sections were then stained in Weigert's iron Hematoxylin working solution for 10 min followed by rinsing in running tap water for 10 min. Then the sections were stained in Biebrich scarlet-acid fuchsin solution for 10–15 min, followed by wash in distilled water. The sections were again treated in phosphomolybdic–phosphotungstic acid solution for 10–15 min and then directly transferred to Aniline Blue solution and stained for 5–10 min. The sections were then placed in 1% acetic acid solution for 2–5 min followed by wash in distilled water, dehydrated using ethanol, cleared in xylene and then mounted in a mounting medium. The collagen stains blue, nuclei black, and muscle and cytoplasm stains red in color. Immunohistochemical analysis, tissue samples were frozen in liquid nitrogen using embedding medium for 20 s and then transferred to −80°C refrigerator to be stored until it was processed on a cryostat. Ten micrometers thick cryostat sections were used for performing immunohistochemistry. Cardiac specific marker proteins α-actinin (Sarcomeric) (1:100; Abcam), troponin T (1:100; Abcam) and anti-inflammatory marker protein CD68 (1:100; Invitrogen), to analyze any inflammatory response triggered by the nanofiber scaffolds and CD31 (1:100; Abcam) to analyze angiogenesis were employed as primary antibodies. The frozen sections were fixed with 100% methanol for 10 min and then incubated in 0.5% Triton–X solution for 5 min to permeabilize the cell membrane. Nonspecific sites were blocked by incubating in 3% BSA (Sigma) for 1 h, following which primary antibodies were added in the dilution 1:100 and incubated for 90 min at room temperature. The samples were then washed thrice with PBS for 15 min each, to remove any excess unbound primary antibodies. This was followed by incubation for 60 min with AlexaFluor 488 secondary antibody (Invitrogen) in the dilution 1:250 at room temperature. The samples were again washed thrice with PBS for 15 min. The cell nuclei were stained using 1:5000 dilution of 4,6-diamidino-2-phenylindole hydrochloride (DAPI; Invitrogen) for 30 min at room temperature. The sections were again washed with PBS thrice to remove any excess staining. H-1000 Vectashield mounting medium (Vector Laboratories) was added to the slides and the edges were sealed using Fluoromount. The glass slides were then viewed using fluorescence microscopy (Olympus FV 1000) using 60x oil lens and the images were formatted using the FV10-ASW 2.0 viewer. Uniform settings of 60x magnification, sampling speed 4 (us/p), laser 1 (DAPI) wavelength 405 nm and transmissivity 2.5%, laser 2 (green) wavelength 473 nm and transmissivity 3.5%, and laser 3 (red) wavelength 559 nm and transmissivity 2.5% were kept constant throughout the imaging study to analyze the expressions of cardiac proteins. Further, the intensity of the marker proteins was calculated using the ImageJ software. Clinical applications, several algorithms are made available as plug-ins in the public domain software ImageJ; one such plug-in allows for calculation of intensity measurements from OIB files obtained from confocal Olympus FV 1000 microscopy. Using ImageJ, for RGB images, the mean is calculated by converting each pixel to gray scale using the formula gray=0.299 red+0.587 green+0.114 blue and the SDs were calculated using the SD of the gray values used to generate the mean gray value. Intensity calculations, 10 cells were randomly selected from each of the images acquired and intensity measurements were computed. Cell marker proteins accompanying PKH26 dye was used to identify injected cells.
Statistical analysis
All the data presented are showed as mean±standard deviation (SD), analyzed using ANOVA variance. Individual subgroups were analyzed using t-test. Differences were regarded statistically significant at p≤0.05.
Results and Discussion
Cardiac patch degradation profile
The degradation profile evaluated for the cardiac nanofibrous patch to degrade in vivo at different time points as shown in Supplementary Figure S2. The results observed that the fibers are stable for 2 weeks as shown in Supplementary Figure S2a, b. The fibers started swelling after week 3 to 4 by absorbing PBS as indicated in Supplementary Figure S2c, d. The fibers begin to disintegrate after fifth week (Supplementary Fig. S2e) and by week 6 more fibers have disintegrated giving an appearance of short broken fibers as evidenced in Supplementary Figure S2f. The fibers disappear completely by week 7 as evidenced in the Supplementary Figure S2g. The percentage loss of mass measured and plotted in Supplementary Figure S2h. The degradation time frame of the cardiac patch material provides sufficient time for the scaffold material to integrate with the tissue in vivo and degrade after the formation of new tissue, thereby providing structural and functional support to the infarcted myocardium.
Analysis of marker protein creatine kinase
Blood testing for the detection of biomarkers of myocardial injury plays a vital role for the evaluation and diagnosis of MI. The criteria for analysis of MI was put forward by the American College of Cardiology (ACC) and the European Society of Cardiology (ESC), which states the following characteristics: (1) typical heart failure symptoms; (2) typical rise and fall pattern of cardiac marker-like creatine kinase, or (3) characteristic electrocardiogram (ECG) pattern involving the development of Q waves. 10 CK enzymes, particularly the more specific isoenzyme CK-MB, is specific and relatively sensitive for detecting acute MI and has long been used for the diagnosis of MI. CK enzyme is present in the skeletal muscle and myocardium and constitutes three isoenzymes: MM, MB, and BB. Among the other isoenzymes CK-MB is present in a relatively high concentration in the myocardium and also used for the diagnosis of MI. Subsequent to myocardial injury, the initial CK-MB begins to increase 2 h after MI and reaches a peak value at 4–6 h, and returns to baseline at 48–72 h. 10 In this study, we have recorded the concentration of CK-MB before infarction, 4–6 h postinfarction, and again during the follow-up period of 2 and 4 weeks. We observed in Figure 1 that the preoperative level of CK-MB was in the normal range (1.0–6.0 μg/L) in all pigs. After infarction the sudden rise in the CK-MB levels was noticed in all the pigs, confirming the creation of MI. The follow-up CK-MB values recorded on weeks 2 and 4 showed that the CK-MB values in all experimental pigs has reached the normal range, except the control MI infarcted pigs, which had values of 11.3±1.6 and 29.8±2.3 on week 2 and 4, respectively, indicating a reinfarction and lack of regeneration. CK-MB has advantages over other cardiac markers in the sense that they remain elevated for longer periods and also can detect the presence of reinfarction in the myocardium.
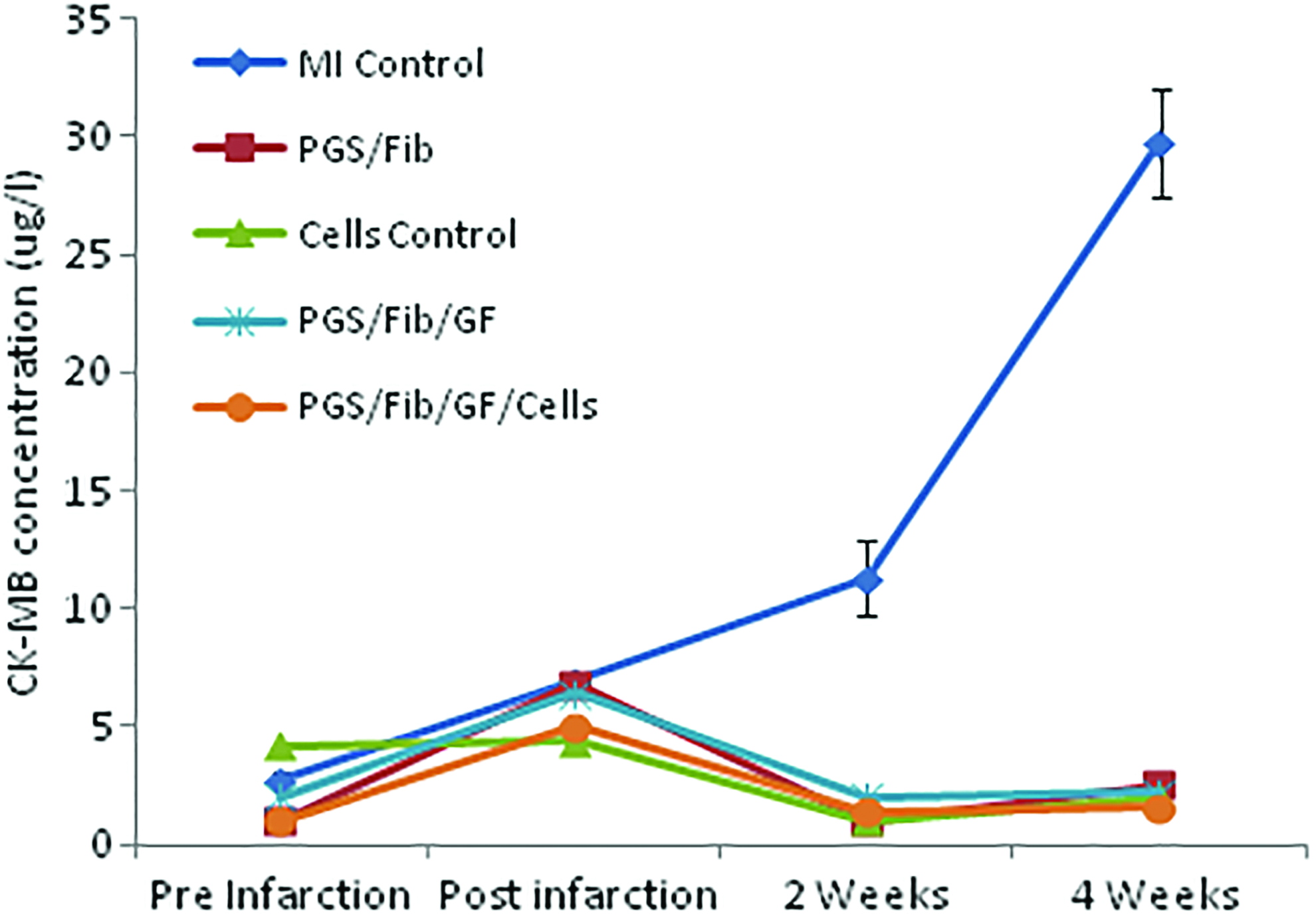
Values of CK-MB in blood before infarction, 4–6 h postinfarction, 2 weeks follow-up and 4 weeks follow-up in myocardial infarction (MI) control, cells control, PGS/Fib, PGS/Fib/VEGF, and PGS/Fib/VEGF/Cells animal models. CK-MB, creatine kinase MB; PGS/Fib, poly(glycerol sebacate/fibrinogen; VEGF, vascular endothelial growth factor. Color images available online at www.liebertpub.com/tea
Echocardiography
EF and fractional shortening
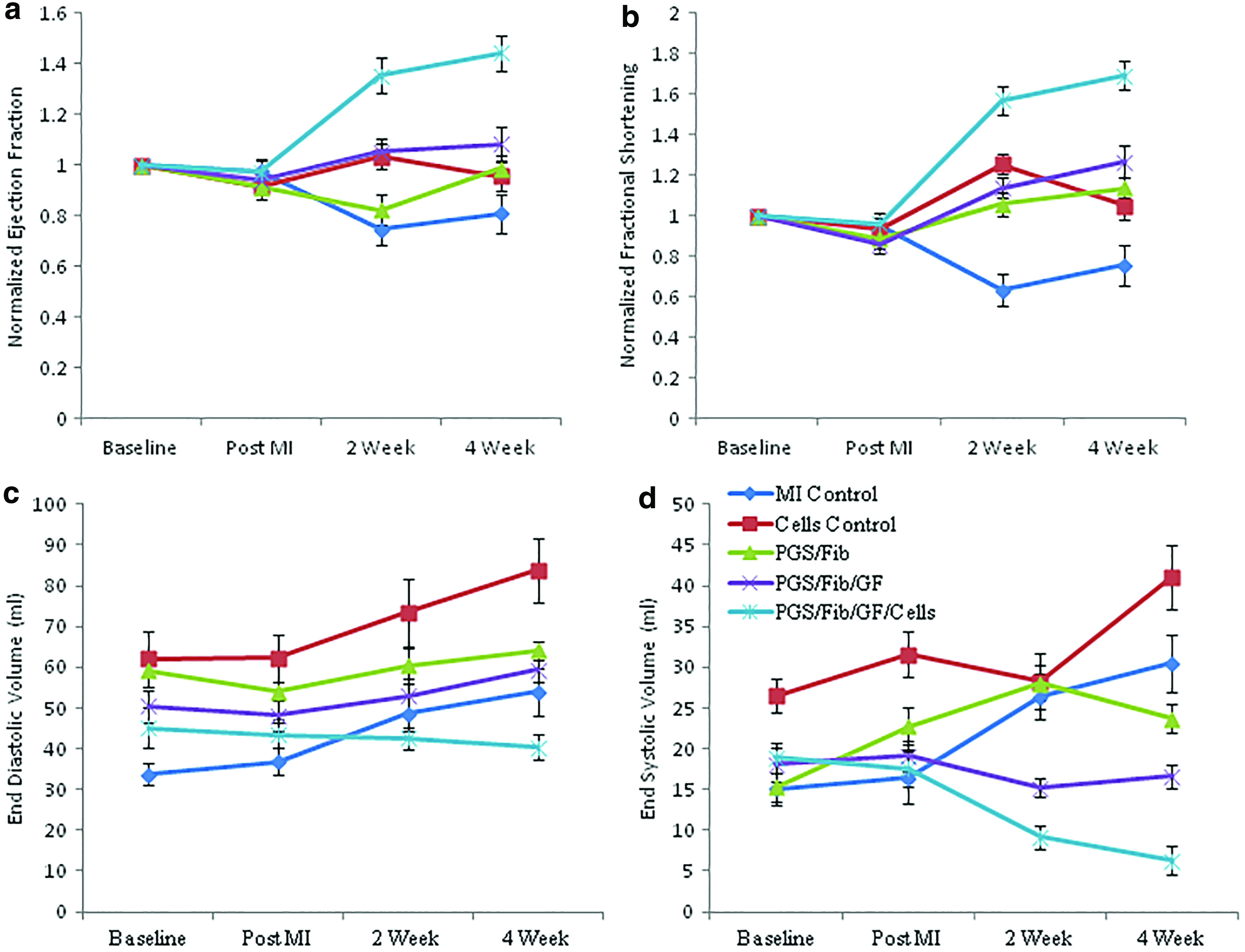
The application of echocardiography in clinical cardiology has increased recently, primarily for the measurement of LVEF and LV volumes. The major predictor for long-term survival and recovery after MI is from the functional status of LV, especially EF. It was noticed in Figure 2a that both MI control and cells control groups had low EF values after 4 week follow-up compared with their cardiac patch counterparts. Low EF is due to poor contractile function of LV owing to the extensive damage of the myocardium or continuing ischemia or left ventricular dilation caused by infarct expansion and stretching of the myocardial scar. In the case of nanofiber implant groups, the EF increased post MI in the follow-up period of 2 and 4 weeks, indicating that the nanofibers provided both structural and mechanical support to the infarcted myocardium preventing LV dilation and subsequent reduction in EF. Echocardiography showed the EF values, after the creation of MI in groups MI control, cells control, PGS/Fib, PGS/Fib/VEGF, and PGS/Fib/VEGF/cells group, was 56.44%±3.9%, 49.87%±2.4%, 60.48%±4.7%, 61.32%±3.2%, and 57.21%±6.2%, respectively. The characteristics of post infarction disease progression, the control animal models demonstrated a deterioration of LV function and infarct wall thinning during the follow-up periods. There was a significant deterioration in EF in the control group after 4 weeks, with values of 46.69%±2.3% and 52%±2.8% on MI control and cells control, respectively. On the contrary, the EF in the implant groups improved having values of 68.71%±2.8%, 75.41%±3.2%, and 79.58%±3.6% for PGS/Fib, PGS/Fib/VEGF, and PGS/Fib/VEGF/cells group, respectively. A significant difference in the EF values was noticed after week 4 in the cells control group compared with MI control (p=0.03) and also a significant increase in EF in PGS/Fib group compared with MI control and cells control (p=0.0026). Upon inclusion of VEGF there was no significant increase in the EF compared with PGS/Fib scaffolds. However, PGS/Fib/VEGF/cells group had significantly higher EF compared with the controls and other patch groups (p=0.05). The difference in the increase in EF from creation of MI to 4 weeks follow-up was the maximum in PGS/Fib/VEGF/Cells group followed by PGS/Fib/VEGF group and PGS/Fib group having values of 40.09%±4.9%, 15.45%±1.2%, and 6.56%±0.8%, respectively. Clinical studies have shown that injection of stem cells into 67 patients with MI showed decreased infarct volume compared with the controls, but with little effect observed on EF. 11 Strauer et al., 12 showed that the injection of bone marrow stem cells although brought about an increase in regional functional recovery, there was no effect on EF. BOOST clinical trials also reported no significant difference in EF values compared with the controls after 18 months. 13 Similarly, ASTAMI clinical trials also demonstrated no significant effect on EF values compared with the controls after 6 months. 14 The above-mentioned studies indicate that the injection of MSCs at the region of infarction, has a positive effect on infarct size, even though no significant improvements in EF or LV volumes were observed. This signifies the need for a suitable scaffold material to impart positive effects on the functionality of LV and also degrade after new tissue formation. The degradation profile data, as discussed earlier in Supplementary Figure S2, we are able to evaluate the degradation profile of the patch material under in vivo conditions. Studies have shown that compared with poly (DL-lactide-co-glycolide), PGS degrades by surface erosion, which gives a linear degradation profile of mass and, therefore, its geometry and mechanical properties are retained which is advantageous for cardiac tissue engineering applications. 15 Therefore, our study showed the advantage of employing PGS/Fib/VEGF/Cells as a cardiac patch material having suitable mechanical and biological properties, thereby preventing cardiac remodeling and cell loss in the hostile MI environment which subsequently resulted in improved EF. Improvement in EF also signifies formation of new myocardial tissue within the region of infarction which attenuates the anatomical alterations and improves contractility.
Fractional Shortening (FS) approximates EF, if there is no significant wall motion abnormality. Fractional shortening (FS%) is the percentage change in LV cavity dimensions and is represented as,
Figure 2b observed that the FS values are in correlation with EF values obtained for various samples. For instance, the FS values increased post MI during the follow-up period of 4 weeks in all implanted animals. In the case of MI control and cells control, the FS values decreased during the fourth week follow-up period similar to reduced EF values. This is because low LVEF and low FS is the result of reduced contractile functionality of LV due to continuing ischemia or extensive myocardial damage or a result of LV dilation caused by myocardial scar stretching and infarct expansion. It was noticed that in week 4, even though there was no statistically significant difference between MI control and cells control, upon application of the patch, there was statistical increase in FS in PGS/Fib compared with the controls (p=0.0007). There was no significant increase in FS upon inclusion of VEGF in PGS/Fib/VEGF group compared with PGS/Fib. However, in PGS/Fib/VEGF/Cells group, FS was significantly higher compared with all other animal groups (p=0.003).
LV volume dimensions
Following infarction, the remaining viable portion of the myocardium undergoes remodeling to compensate for functional loss to maintain adequate cardiac output. Postinfarction LV remodeling initiating the molecular and cellular changes is apparent clinically, as variations in the geometry, size, and functionality of the ventricles, over a span of few weeks. 16 Clinical relevance of LV remodeling, characterized by a decrease in LVEF and an increase in LV volumes after MI was emphasized by White et al. 17 who demonstrated that patients who died during follow-up after MI had significantly lower LVEF and larger LV volumes compared with survivors. Figure 2c, echocardiographic data at 4 weeks after implantation showed continuous improvement in left ventricular EF and prevention of continual increase in left ventricular dimensions in the case of PGS/Fib/VEGF/Cells models. The percentage increase in EDV dimension from post MI period to 4 weeks follow-up was found to be 46.13%±2.8%, 36.61%±3.2%, 18.64%±2.3%, 17.39%±3.9%, and 5.05%±5% for MI control, cells control, PGS/Fib, PGS/Fib/VEGF, and PGS/Fib/VEGF/Cells groups, respectively. A significant difference in the EDV values was noticed after week 4 in the cells control compared with MI control (p=0.004) and also a significant difference in EDV in PGS/Fib compared with controls (p=0.02). Similar to EF and FS, there was no significant difference in PGS/Fib/VEGF compared with PGS/Fib, but PGS/Fib/VEGF/cells group showed significant difference in EDV (p=0.0006) in comparison to all other animal groups. This clearly showed that the PGS/Fib/VEGF/Cells group restored the LV function after MI, evident from the improvement in EF and prevention of LV enlargement. The results also demonstrated that the structural support alone in the form of PGS/Fib nanofibers was not sufficient to prevent post infarction remodeling, demonstrating that the bioactivity due to cellular infiltration into scaffolds are likely to play a key role in the preservation of cardiac functionality as evidenced in the case of PGS/Fib/VEGF/Cells implants. Earlier studies by Hashemi et al., showed that endomyocardial injection of MSCs into female Yorkshire swine resulted in decreased infarct size measured by magnetic resonance imaging, compared with control groups. However, there was no effect on LV volumes or EFs observed. 18 PGS/Fib/VEGF/Cells animals compared with other animal models did not display significant LV dilation, demonstrating that the mechanical and biological support rendered by PGS/Fib/VEGF/Cells implant prevented LV remodeling and restored LV function.
End Systolic Volume (ESV) is the blood volume present in the ventricle at the end of systole, and the beginning of diastole; so it is the lowest volume of blood at any point in the cardiac cycle present in the ventricle, estimating the cardiac output efficiency. Graphically we represented the ESV values obtained for all animal models as shown in Figure 2d. It can be seen that the ESV values were lowest for the implant models compared with controls. A significant difference in the ESV values was noticed after week 4 in cells control compared with MI control (p=0.016) and also significant difference in PGS/Fib compared with the controls (p=0.004), indicating that the patch provides mechanical support to the ventricle to aid in pumping of the blood. Upon incorporation of VEGF, there was a significant difference in ESV in PGS/Fib/VEGF compared with PGS/Fib (p=0.005). PGS/Fib/VEGF/cells group had a significant difference (p=0.001) in ESV value in comparison to all other animal groups. The ESV values at 4 week follow-up were 30.55±3.5 mL, 41.1±3.9 mL, 23.72±1.8 mL, 16.64±1.5 mL, and 7.3±0.8 mL for MI control, cells control, PGS/Fib, PGS/Fib/VEGF, and PGS/Fib/VEGF/Cells groups, respectively. Studies have shown that left ventricular ESV is the main controlling factor for survival after recovery post MI. 17 The study shows that the efficiency of cardiac output, evident from the lowest volume of blood in the systole was in PGS/Fib/VEGF/Cells implant models.
Histological observation of regenerated myocardium
During the initial stage of myocyte necrosis, edema and inflammation are localized to the infarcted region; subsequently leading to a long-term phase of fibroblast proliferation and collagen deposition, known as scar formation. This entire process takes a few weeks to months depending on the type of species. To ensure that the transplanted cells find their suitable niche within the myocardium, a nanofiber-based delivery route was suggested in the present study. Cells are present throughout the whole nanofibrous constructs, represented as purple color, as shown in Figure 3. In the region of infarction, host cardiomyocytes were replaced by fibrillar collagenous scar tissue in the case of MI control and cells control (Fig. 3a, b). During the early stages of MI, matrix metalloproteinase are upregulated, 19 which causes degradation of ECM leading to slippage of myocytes, weakening of the infarct wall, causing LV aneurysm. 20 Administration of PGS/Fibrinogen nanofibrous patch during the preliminary stage of infarction may prevent LV remodeling by increasing the mechanical strength of the infarct before the formation of collagen scar. Furthermore, fibrinogen adheres to cell surface receptors and various substrates, including collagen through mechanical interlocking and hydrogen bonding, covalent and other electrostatic bonding. 21 Hence, it prevents myocytes slippage and resulting aneurysm by binding to the adjacent native myocardium. This was evident from the interaction between the nanofiber surface and myocardium as shown in Figure 3c–e. Moreover, the formation of new blood vessels was also evident in H&E staining of nanofibrous implants indicating neovascularization. There was more neovascularization in the case of PGS/Fib/VEGF and PGS/Fib/VEGF/Cells implants compared with PGS/Fib implants (Fig. 3). This was owing to the injection of VEGF into the ischemic site which promotes neovascularization and angiogenesis. Additionally, in the PGS/Fib/VEGF/Cells implants MSCs transplanted with nanofiber matrix favored the prevention of anoikis by MSCs-PGS/Fibrinogen matrix interactions. We have reported in earlier studies that PGS/Fibrinogen scaffolds prevent anoikis of cardiomyocytes due to enhanced cell–biomaterial interactions. 6 The implantation of PGS/Fib/VEGF/cells scaffolds stimulated the endogenous regenerative capacity of the heart to release cytokines, growth factors, and other paracrine signaling molecules by the transplanted and host cells enhancing angiogenesis and vascularization. 22

Hematoxylin and Eosin staining.
Masson's Trichrome staining of infarcted myocardium, infarcted tissue replaced with fibroblasts and collagen appears blue and viable myocardium appears red (Fig. 4a–e). This staining showed that a larger amount of fibrous tissue, as evidenced by the blue color (Fig. 4a) was present in the MI control animals. In the case of cells control also there was significant amount of scar collagen present in the infarcted myocardium. The presence of MSCs has resulted in the formation of new blood vessels in the scar tissue, as indicated by arrows in Figure 4b. Orlic et al. 23 studied that the bone marrow-derived progenitor cells upon intramyocardial injection led to the regeneration of considerable amount of contracting myocardium, signifying that local injection of bone marrow cells (BMCs) can improve the outcome of MI by generating de novo myocardium. The cardiac patch implant animal models observed new tissues and a smaller amount of fibrous tissues (Fig. 4c–e), the formation of neotissue replaced the scar collagen tissues of the infarcted myocardium. Cardiac repair in the case of nanofibrous implants was identified by a band of newly formed myocardium replacing the infarcted region. Moreover, the scar area was minimal in the case of PGS/Fib/VEGF/Cells compared with PGS/Fib and PGS/Fib/VEGF implants, indicating that PGS/Fib/VEGF/Cells implants provides both mechanical and biological support to the infarcted myocardium. The thickness of the scar area was measured from the bright field images using ImageJ software and it was observed that in MI models the scar tissue extended upto 900±156 μm and in the cells control it was 700±135 μm. The scar tissue extensions in the case of both PGS/Fib and PGS/Fib/VEGF were about 500±143 μm and 462±91 μm, respectively, and in PGS/Fib/VEGF/Cells it was the least spanning less than 200±85 μm. In the absence of nanofibrous patch materials, myocardial replacement was minimally noticed, and healing with the development of scar area was apparent in the repair of infarcted myocardium.
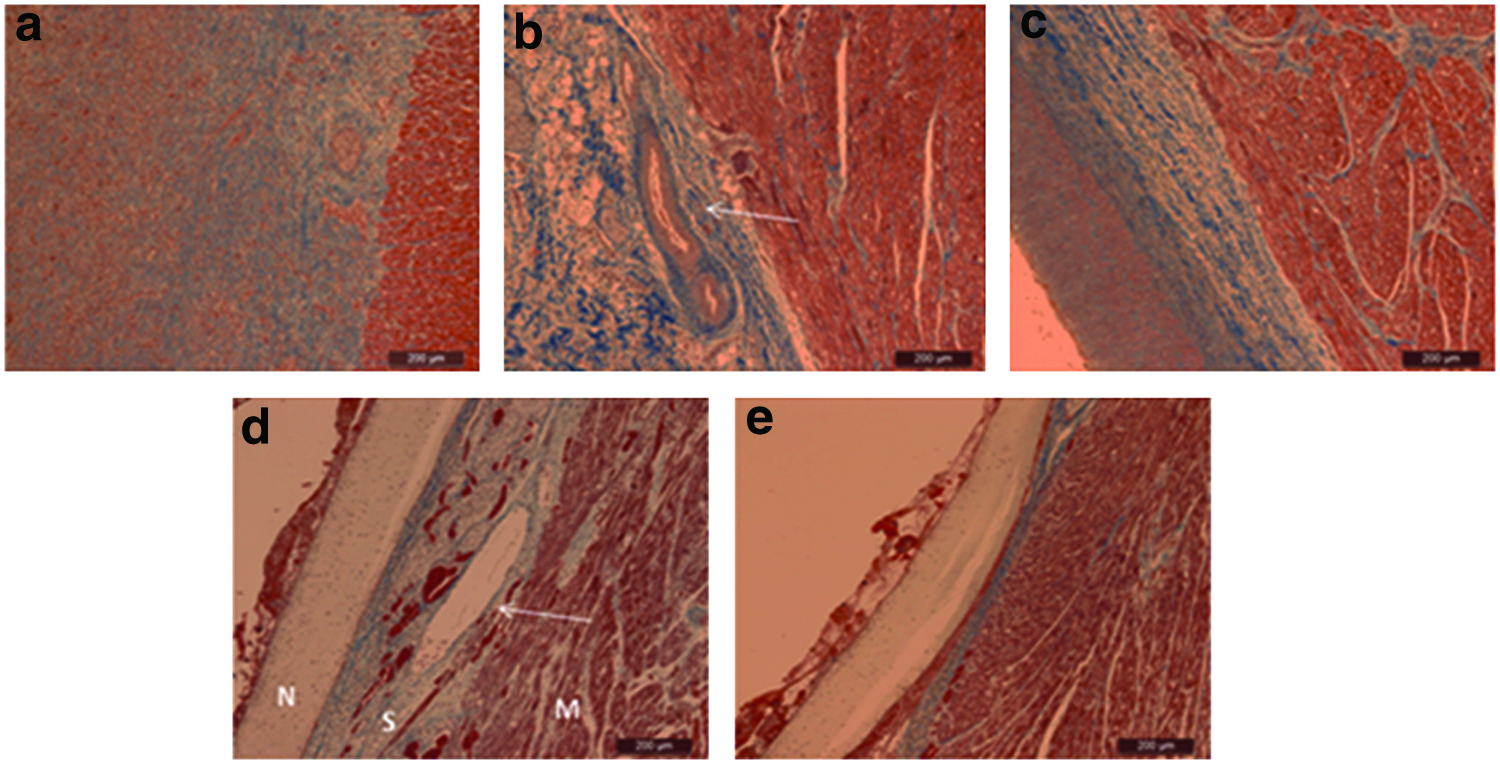
Masson's Trichrome staining.
Immunohistochemistry for the expression of cardiac proteins
Examination with immunofluorescence staining demonstrated that the cells labeled with a fluorescent dye before injection were noticed in the infarcted regions of MI in the groups of MSCs implanted with nanofiber matrix, which suggested that the injected cells survived in the region of infarction after transplantation owing to the presence of PGS/Fib, which serves as a matrix support for cell entrapment. MSCs injected alone in the cells control group were not detected through immunohistochemistry staining, owing to the loss of cells from the site of infarction.
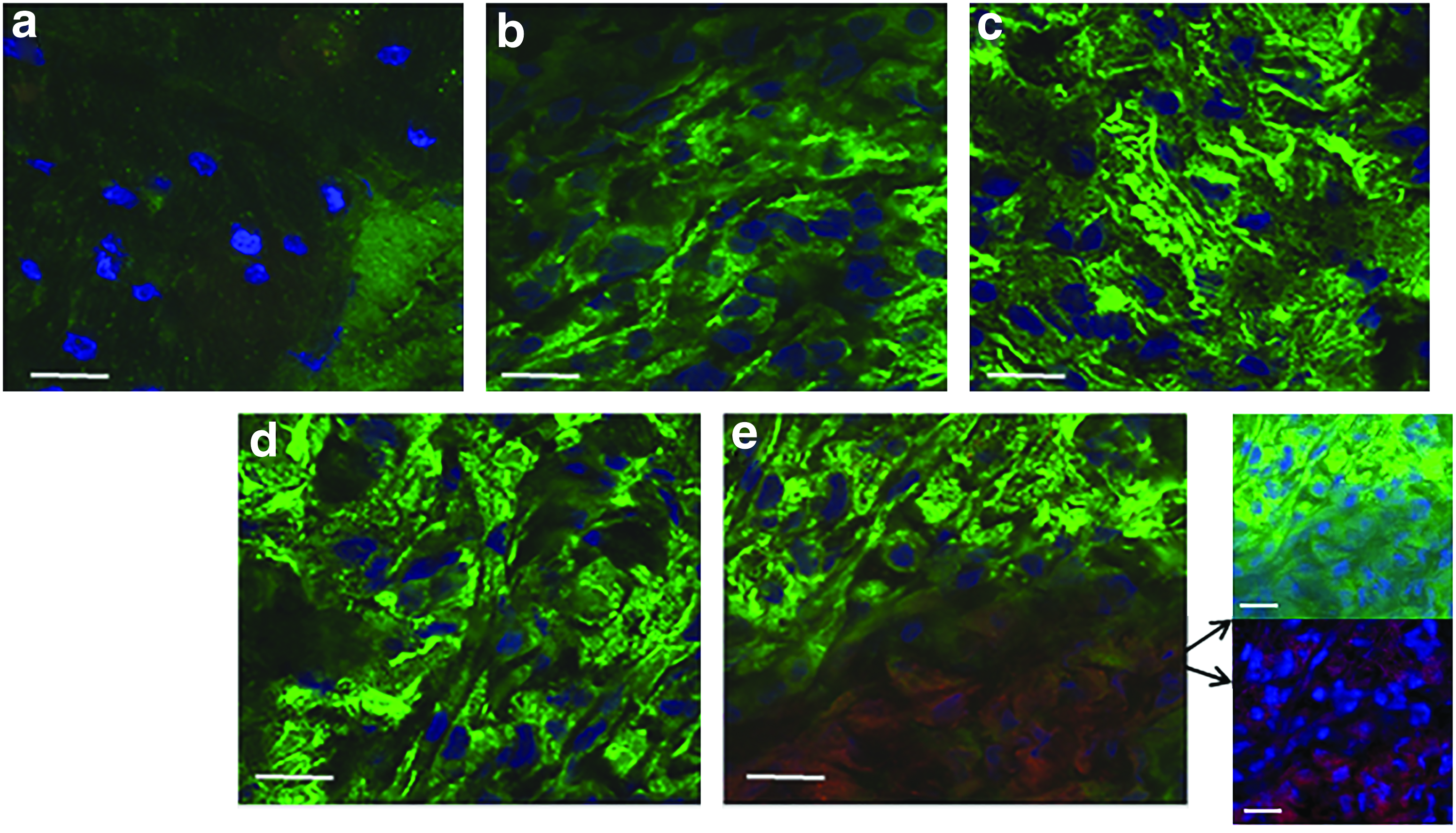
Angiogenesis helps to recover at-risk cardiomyocytes and improves the survival of donor stem cells by enhancing blood circulation in the region of infarction. Angiogenesis in the infarcted myocardium was studied by immunohistochemical staining with anti-CD31 to visualize endothelial cells as indicated in Figure 5a–e. Studies have demonstrated that the BMCs were able to induce angiogenesis, myogenesis, and infarcted myocardium regeneration; this leads to the improvement of cardiac functionality in pigs and mice.23,24 The ultimate objectives of cell therapies are myocardial revascularization and regeneration, thus re-establishing bioelectrical conductivity and synchronous contractility for the achievement of clinical recovery of heart function without causing any adverse effects. Figure 5d, e indicates that the expression of CD31 was more predominant in PGS/Fib/VEGF and PGS/Fib/VEGF/Cells implants, owing to the presence of VEGF, which induces angiogenesis. The intensity of CD31-positive cells were found to be 200.41±56.7, 1146.79±342.76, 1302.86±278.14, 1876.33±446.74, and 2123.54±403.98 in MI control, cells control, PGS/Fib, PGS/Fib/VEGF, and PGS/Fib/VEGF/Cells, respectively. Moreover in PGS/Fib/VEGF/Cells implants, we observed colocalized expression of red and green colors, indicating that some of the MSCs injected have undergone differentiation into endothelial cells and hence showing dual staining. Inset image in Figure 5e shows the individual panels for the merged PGS/Fib/VEGF/Cells groups. In the case of MI control (Fig. 5a) there was no expression of CD31 positive cells, owing to the hostile environment in the ischemic myocardium. Immunofluorescent staining for the nanofibrous implants demonstrated positive expression for endothelial cell marker protein confirming that new blood vessels were formed in the border zone and could provide blood flow to support transplanted and homing stem cells, in correlation with the histological staining results.
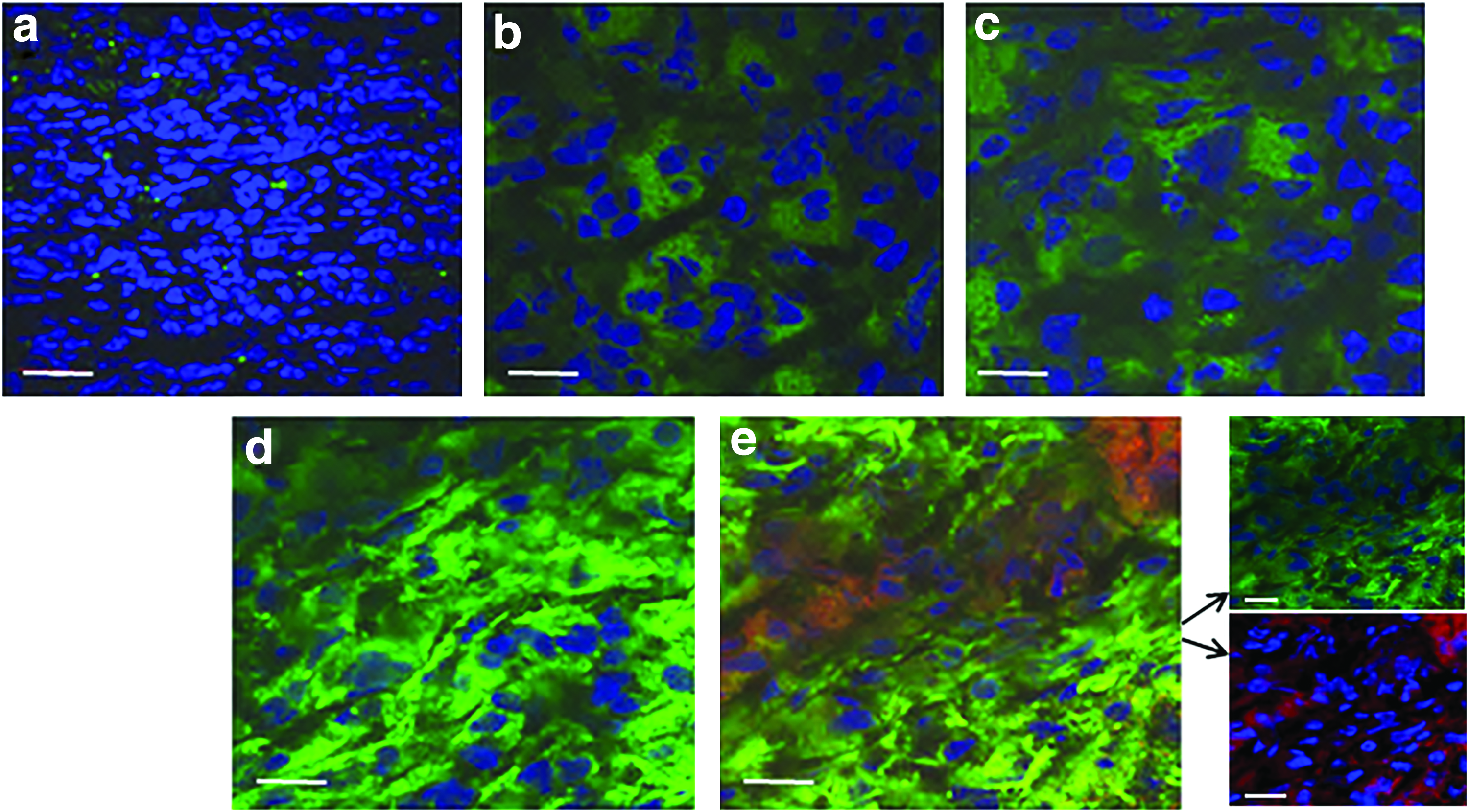
Immunohistochemical staining for CD31.
Myocardial viability is evidenced by the presence of α-sarcomeric actinin-positive and troponin-positive cardiomyocytes. Troponin T is necessary for effective cardiomyocytes, which contain contractile proteins as it regulates the force and velocity of myocardial contraction and actinin is an important constituent of the contractile apparatus. Supplementary Figure S3a–e shows the expression of actinin by various animal models. It can be noticed that in the case of all nanofibrous implants (Supplementary Fig. S3c–e), cardiomyocytes in the infarcted myocardium expressed actinin with characteristic striations, indicating that the functional activity of cardiomyocytes was restored in these animals. Moreover in the PGS/Fib/VEGF/Cells implants, presence of injected MSCs was noticed at the site of infarction. In the case of cells control samples (Supplementary Fig. S3b) few cells expressing actinin was noticed whereas in the case of MI control (Supplementary Fig. S3a) the striations characteristic of functional cardiomyocytes was absent, indicating loss of functional cardiomyocytes in the infarcted myocardium. Similarly immunofluorescent staining for the expression of troponin was also performed in the regenerated myocardium as evidenced in Figure 6a–e. Similar to actinin expression, troponin expression was also meager in the control MI (Fig. 6a), indicating loss of functional myocardium. The intensity of troponin-positive cells were found to be 410.75±89.1, 1364.06±212.98, 1783.46±415.26, 1865.78±489.17, and 2097.34±512.64 in MI control, cells control, PGS/Fib, PGS/Fib/VEGF, and PGS/Fib/VEGF/Cells, respectively. Moreover, in the case of PGS/Fib/VEGF/Cells animals, cardiogenic differentiation of MSCs was noticed, characterized by dual staining of the injected cells. Figure 6e inset shows the individual panels for the merged PGS/Fib/VEGF/Cells scaffolds. Our earlier studies have demonstrated the capability of MSCs to undergo cardiogenic differentiation in certain milieu capable of inducing cardiogenic differentiation of MSCs.5,25
Immunohistochemical staining for troponin was observed in
Anti-CD68 antibody was used to analyze the presence of macrophages after 4 weeks of implantation to detect whether the biopolymer would induce any undesirable inflammatory response as shown in Figure 7a–e. No significant immune and inflammatory reaction was noticed in the infarcted regions in the nanofibers implant groups (Figure 7c–e). CD68 cells clustering in the MI control and cells control (Figure 7a, b) show that inflammation might exist chronically in the infarction site. In prolonged or extensive inflammation cases, the damaged tissue is replaced by fibrotic scars. The magnitude of this inflammatory reaction differs, but the persistence of even a slight degree of inflammation may be considered harmful for the heart patient. There were very few macrophages scattered in the vicinity of PGS/Fib implants, but none on the PGS/Fib/VEGF and PGS/Fib/VEGF/Cells groups. The lack of inflammatory response on these scaffolds after 4 weeks follow-up confirms that the implanted scaffolds at the end of 4 weeks did not trigger any unnecessary immune response in the host body.
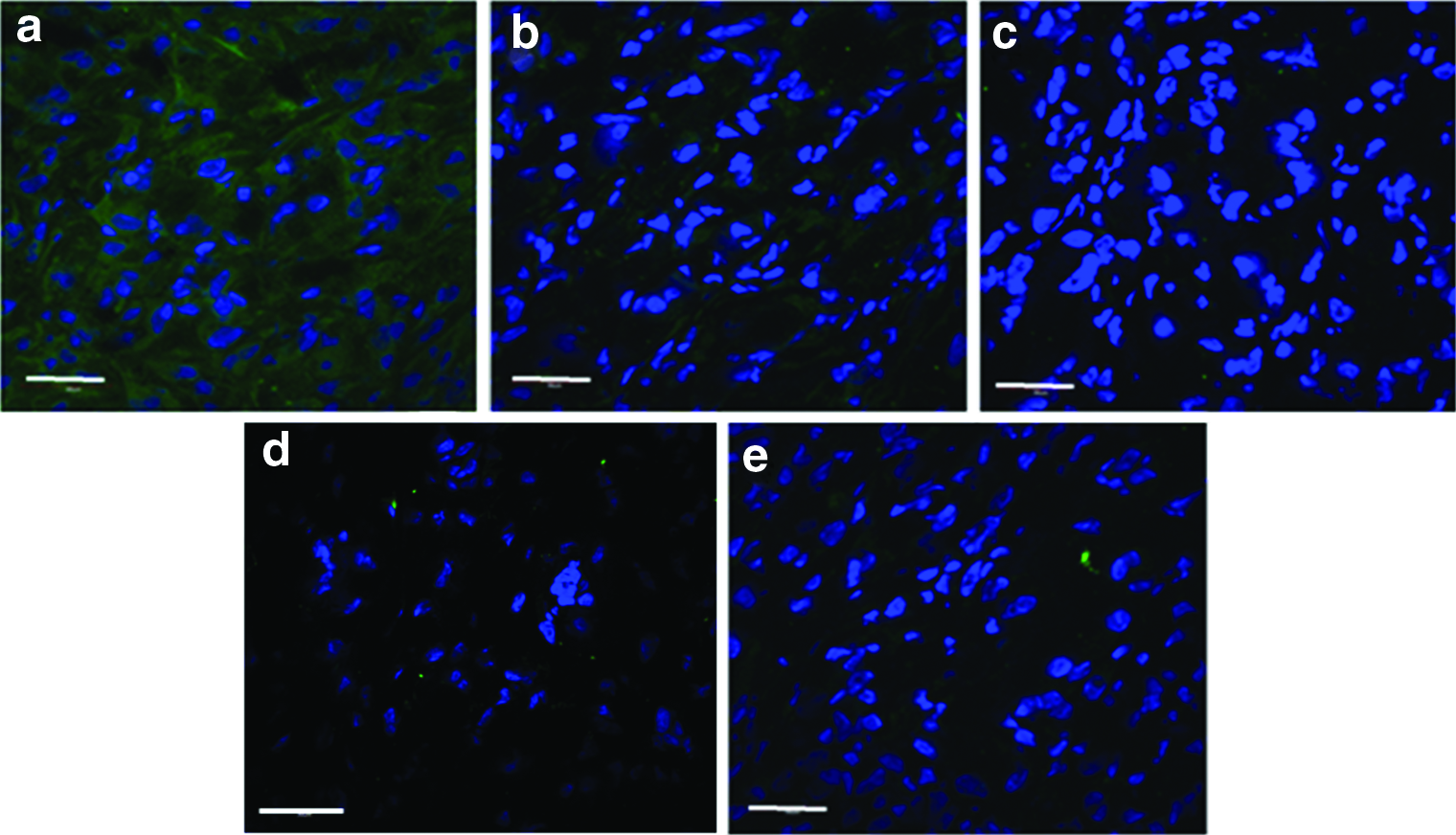
Immunohistochemical staining for CD 68 was observed in
Currently therapies for MI involving biomaterials, gene therapy, stem cells, or revascularization strategies in animal studies and clinical trials, although have shown promise, more precise targeting of therapeutics to the infarct border zone could dramatically enhance infarcted myocardium regeneration. Stem cell therapies that replace loss of myocytes post MI have shown partial functional improvements in in vivo models23,26 and clinical trials,27,28 but cell retention was poor 29 and functional improvement was limited mainly due to the lack of ischemic tissues to support cell engraftment and survival. Cardiac MI, both cardiomyocytes and the ECM are altered pathologically. Hence, it is necessary to correlate a procedure aiming at sustenance of both the ECM and myocardial cells for the regeneration of infarcted myocardium.
Conclusion
The transplanted MSCs along with biodegradable PGS/Fibrinogen core/shell fibers offer structural support within the body, and ultimately degrade allowing the neotissue to take over the mechanical load; in this manner the matrix seems to help to normalize the heart wall stress in the damaged myocardium. Besides chemical properties, the PGS/Fib/VEGF/Cells nanofibers also prevent negative ventricular remodeling of the myocardium by offering structural support to the LV wall. Improved angiogenesis and higher levels of myofibroblast infiltration were possible contributors to the salutatory effects of post MI seen with PGS/Fib/VEGF/Cells animals. In this study, most of transplanted MSCs within the PGS/Fib/VEGF scaffolds expressed cardiac marker proteins of troponin and actinin and endothelial cell marker protein CD31 indicating differentiation of MSCs into cardiac cells and endothelial cells. Echocardiography results showed functional improvement in the form of improved EF and reduction in LV volume dimensions in PGS/Fib/VEGF/Cells scaffolds. PGS/Fib/VEGF/Cells scaffolds which provides both functional and structural integrity to the infarcted myocardium and also serves as a suitable matrix for the entrapment of MSCs has prospective clinical applications for cardiac tissue engineering.
Footnotes
Acknowledgments
This study was supported by the NRF-Technion (R-398-001-065-592), Ministry of Education (R-265-000-318-112), and NUSNNI, National University of Singapore, Singapore.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.