
Abstract
A key goal for successful bone regeneration is to bridge a bone defect using healing procedures that are stable and durable. Adipose-derived stem cells (ASCs) have the potential to differentiate into bone. Meanwhile, platelet-rich plasma (PRP) is an interesting biological means to repair tissue by inducing chemotactic, proliferative, and anabolic cellular responses. This study evaluated bone regeneration using a combination of ASCs and PRP in a rat calvarial defect model. ASCs were isolated from inguinal fat pads of F344 inbred rats, while PRP was prepared from these rats. ASCs were cultured in control medium supplemented with 10% fetal bovine serum or 5% PRP in vitro. After 1 week, levels of growth factors including insulin-like growth factor-1, transforming growth factor-β1, hepatocyte growth factor, and vascular endothelial growth factor in the culture supernatant were measured by enzyme-linked immunosorbent assays. Moreover, the ASC/PRP admixture was transplanted into the rat calvarial defect. Microcomputed tomography, histological, and immunohistochemical (osteopontin and osteocalcin) analyses were performed at 4 and 8 weeks after transplantation. The in vitro study showed that the levels of growth factors secreted by ASCs were significantly increased by the addition of PRP. Transplantation of the ASC/PRP admixture had dramatic effects on bone regeneration overtime in comparison with rats that received other transplants. Furthermore, some ASCs directly differentiated into osteogenic cells in vivo. These findings suggest that the combination of ASCs and PRP has augmentative effects on bone regeneration. The ASC/PRP admixture may be a promising source for the clinical treatment of cranial defects.
Introduction
B
A number of surgical techniques have been developed to reconstruct bony defects, including autografts, 3 allografts, 4 xenografts, 5 and alloplasts.6,7 Transplantation of autogenous bone is the gold standard of filling materials because it directly provides bone-forming cells to the implant site 3 and it is histocompatible and nonimmunogenic, reducing to a minimum the likelihood of immunoreactions and transmission of infections. 8 Nevertheless, autografts also have disadvantages, namely, donor site morbidity and the lack of suitable graft sites and materials. 9 The other methods for bone regeneration, allografts, xenografts, and alloplasts, have been used with variable success, and each method has distinct disadvantages that limit its clinical application. Allografts can be used for large defects, but their use is limited owing to possible immune rejection, disease transmission, and their lower incorporation rate in comparison with autografts. 4 Xenografts are rarely used because they have the same drawbacks as allografts and their physiological structures and functions do not exactly match that of human tissue. 5 Alloplasts were recently used as a means to regenerate bone. However, they typically lack osteoinductivity and may expose patients to risks of foreign body reactions and infections. 7
Stem cells are a functional element for tissue regeneration. Recent developments in the field of bone regeneration suggest that it will eventually be possible to replace or repair damaged tissue.10,11 Mesenchymal stem cells (MSCs) possess adipogenic, osteogenic, chondrogenic, myogenic, and neurogenic potential in vitro.11–13 MSCs have the potential to directly differentiate into osteogenic cells and efficiently regenerate bone tissue.11,14,15 Additionally, MSCs secrete a variety of growth factors and cytokines for bone reconstruction.16–18 Several clinical studies have reported that MSCs have great potential for bone regeneration.19,20 However, bone marrow procurement is painful for donors, often necessitating general anesthesia, and it yields low numbers of MSCs. 21
On the other hand, subcutaneous adipose tissue is a rich source of MSCs. 22 Adipose tissue is available in large quantities and is relatively easy to obtain. The procedures have minimal donor site morbidity and induce limited patient discomfort. 23 Furthermore, recent reports have demonstrated that, under proper conditions, adipose-derived stem cells (ASCs) have the potential to differentiate into an osteogenic lineage as efficiently as MSCs.24,25 An effective approach for bone regeneration with ASCs in vivo was recently reported.26,27 In addition, both paracrine and autocrine responses can be elicited by growth factors secreted by ASCs.28–30 ASCs not only secrete growth factors but also can respond to growth factors, thereby amplifying the biological response of the body to cell therapy.
Platelet-rich plasma (PRP) may be a promising cell carrier. PRP is a platelet fraction concentrated from peripheral blood and contains a cocktail of proteins that collectively stimulate repair and regeneration. PRP contains a variety of growth factors, including platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), transforming growth factor-β1 (TGF-β1), hepatocyte growth factor (HGF), and insulin-like growth factor (IGF).31,32 These growth factors have different functions, and cumulatively accelerate tissue and wound healing. Consequently, after increasing the baseline concentration of platelets, PRP may be a powerful biological autologous cocktail of growth factors that can dramatically enhance tissue recovery. Recently, the application of both MSCs and PRP to critical bone defects was found to promote bone repair. 33
We hypothesized that an admixture of ASCs and PRP may be clinically useful for bone tissue engineering. However, the detailed mechanism underlying bone regeneration remains unclear. In particular, the effects of growth factors secreted from an ASC/PRP admixture on bone regeneration have not been verified. The purpose of this study was to evaluate the ability of bone regeneration in a rat calvarial defect model using a combination of ASCs and PRP.
Materials and Methods
Harvest and primary culture of ASCs
The Animal Care and Use Committee of Juntendo University approved all experiments (approval number: 240194). Adipose tissue obtained from an 11-week-old inbred male F344 rat (Sankyo Labo, Inc., Tokyo, Japan) was processed to isolate the ASC population, as described previously. 34 Briefly, under general anesthesia with 2% isoflurane, the inguinal fat pads of the rat were harvested, washed extensively with phosphate-buffered saline (PBS; Gibco-BRL, Grand Island, NY), minced with fine scissors, and enzymatically digested at 37°C for 40 min with 0.12% collagenase (Wako Pure Chemical Industries, Ltd., Osaka, Japan). An equal volume of control medium (Dulbecco's modified Eagle medium [DMEM; Gibco-BRL] containing 10% fetal bovine serum [FBS; Gibco-BRL] and 1% antibiotic/antimycotic [Gibco-BRL]) was then added to neutralize the collagenase. The cell suspension was centrifuged at 1300 rpm (260 g) for 5 min to obtain a high-density stromal vascular fraction pellet, which was resuspended in control medium. After being counted using trypan blue, the cells were plated at a density of 5×105 cells per 100 mm tissue culture dish (Becton-Dickinson, Franklin Lakes, NJ) and maintained in control medium at 37°C in 5% carbon dioxide. The culture medium was changed every 3 days. Confluent ASC cultures (∼80% confluent) were passaged at a ratio of 1:3 using trypsin/ethylenediaminetetraacetic acid (EDTA; Gibco-BRL).
PRP preparation and activation with/without ASCs
PRP was prepared as described previously. 35 Briefly, 10 mL of whole blood from two 11-week-old inbred male F344 rats was drawn preoperatively via cardiac puncture with an 18-gauge needle (Terumo, Tokyo, Japan) into tubes containing EDTA-2Na. The blood was first centrifuged in a standard laboratory centrifuge machine (Kubota 3740; Kubota Co., Tokyo, Japan) for 10 min at 2400 rpm (450 g). The supernatant plasma was collected along with the buffy coat, which consists of platelets and leukocytes, into a neutral tube with a long cannula. A second centrifugation at 3600 rpm (850 g) was performed for 15 min to concentrate the platelets. The infranatant containing the buffy coat was resuspended in 1.3 mL of the residual plasma to prepare the final PRP product. The final density of platelets in the whole blood and PRP was then analyzed in an automatic counter (Celltacα; Nihon Kohden Co., Tokyo, Japan). After ASCs were expanded to passage 3, a pellet of 1×107 ASCs was mixed with 1 mL of PRP. PRP with or without ASCs was then activated with a 10% calcium chloride solution for transplantation. Similarly, a pellet of 1×107 ASCs was mixed with 1 mL of type I collagen gel (Koken Co., Ltd, Tokyo, Japan) for transplantation.
Enzyme-linked immunosorbent assay
Levels of growth factor in PRP
Levels of TGF-β1, VEGF, IGF-1, HGF, and PDGF-AB in whole blood plasma, preactivated PRP, and postactivated PRP were investigated using an ELISA. PRP gelation was activated with a 10% calcium chloride solution. PRP preparations were made from two rats, and these were used in subsequent experiments in a blinded fashion. The concentrations of the growth factors were measured using a Rat Quantikine ELISA Kit (R&D Systems, Minneapolis, MN) according to the manufacturer's instructions. Briefly, 50 μL of sample was added to 96-well microplates that were coated with a monoclonal antibody against the factor of interest and incubated for 2 h. After washing with washing buffer, a horseradish peroxidase-conjugated cytokine was added to each well, after which the wells were incubated for 1 or 2 h and then washed. The substrate solution was added and incubated for 30 min, and the reaction was terminated by addition of the stop solution. Growth factor concentrations were determined by measuring the optical density at 450 nm using a Microplate Reader (SpectraMax 340PC; Molecular Devices, Inc., Sunnyvale, CA).
Levels of secreted growth factors in ASC culture supernatant
ASCs at passage 3 were plated at a density of 5×105 cells per 100 mm tissue culture dish and maintained in DMEM containing 10% FBS or 5% PRP for 1 week at 37°C in 5% carbon dioxide. Thereafter, levels of TGF-β1, VEGF, IGF-1, HGF, and PDGF-AB in the ASC culture supernatant were measured by ELISA.
Surgical procedures
A calvarial bone defect was created using a modified version of a previously described technique.36,37 In brief, rats were anesthetized by inhalation of 2% isoflurane. In the prone position, xylocaine (0.5 mL of 1%) was intradermally injected in the middle of the calvarium. A midline calvarial incision was made, and cranial skin flaps were elevated. The subcutaneous fascia was divided, and periosteal flaps were reflected bilaterally. A 5 mm bone defect was generated in the left calvarial bone with a dental round bar (ISO standard 005). Animals were randomly assigned to five groups (n=10 per group) as follows: Group 1, transplantation of ASCs/PRP (2×105/20 μL); Group 2, transplantation of ASCs/type I collagen gel (2×105/20 μL); Group 3, transplantation of PRP (20 μL); Group 4, transplantation of type I collagen gel (20 μL); and Group 5, injection of PBS (20 μL). After transplantation, the periosteum and skin were closed with 6-0 nylon sutures (Natsume Co., Tokyo, Japan). All animals survived the entire experiment.
Scanning electron microscopy
For scanning electron microscopy (SEM) analyses, PRP with/without ASCs was immediately immersed after activation in a phosphate-buffered glutaraldehyde fixative for 24 h at 4°C and postfixed in 2% osmium tetroxide for 2 h. Subsequently, samples were dehydrated in a graded series of ethanol, substituted with t-butyl alcohol, and dried at −20°C in a vacuum. Finally, samples were made electrically conductive by mounting on aluminum slabs with a carbon paste, followed by coating in an osmium plasma coater to a thickness of ∼10 nm. Specimens were attached to an acrylic plate with glue tape. Subsequently, half of the plate bottom was cut with a diamond disc and vertically divided into two pieces with a chisel and hammer. The cut face of each specimen was examined with a scanning electron microscope (S4800; Hitachi Co., Tokyo, Japan) at 3 kV.
Tissue preparation and microcomputed tomography analysis
At 4 and 8 weeks after transplantation, rats were euthanized by overdose of pentobarbital sodium via intraperitoneal injection (n=5 per group at each time point). Specimens were harvested and fixed in 4% paraformaldehyde (PFA), after which microcomputed tomography (CT) was performed (LATheta; Hitachi Aloka Co., Tokyo, Japan). The surface area and volume of bone in the defect site were calculated using VGStudio MAX2.0 (Nihon Visual Science Co., Tokyo, Japan).
Histological analysis
Following micro-CT scanning, samples were fixed in 4% PFA, decalcified (Kalkitox and 5% sodium sulfate solution; Wako Pure Chemical Industries Ltd.), dehydrated using a graded ethanol series, cleared with xylene, and embedded in paraffin. Coronal sections (5 μm-thick) were stained with hematoxylin and eosin. Moreover, the same specimens were stained with Alcian blue using standard procedures (Alcian blue stain solution; Muto Pure Chemicals, Tokyo, Japan). In representative samples, new bone formation and bone architecture were observed using a light microscope (DP70; Olympus Co., Tokyo, Japan).
Immunohistochemistry
Sections prepared from rats that received the ASC/PRP admixture (Group 1) were used for immunohistochemical staining. Osteocalcin and osteopontin were examined using standard procedures. Briefly, 5 mm tissue sections were deparaffinized in xylene and a graded alcohol series. Endogenous peroxidase activity was blocked with 3% hydrogen peroxide for 10 min, after which sections were rinsed three times with Tris/hydrochloric acid (HCl) buffer for 5 min, blocked with normal goat serum for 30 min, and incubated with an anti-osteocalcin monoclonal antibody (1:500 dilution; Abcam, Inc., Cambridge, United Kingdom) or an anti-osteopontin polyclonal antibody (1:1000 dilution; Abcam, Inc.) overnight at 4°C. After being washed with Tris/HCl buffer, sections were incubated at room temperature for 30 min with a biotin-conjugated anti-mouse or anti-rabbit IgG secondary antibody. Visualization of secondary antibody and counterstaining was performed as described above. Sections were observed with an Olympus DP70 light microscope.
Transplantation of ASCs derived from a green fluorescent protein-transgenic mouse into nude rats
To evaluate the origin of newly formed bone, ASCs were harvested from a 7-week-old inbred male green fluorescent protein (GFP)-transgenic mouse (C57BL/6-Tg [CAG-EGFP]; SLC, Inc., Shizuoka, Japan) and cultured until passage 3. A 5 mm bone defect was generated at the left calvarial bone under general anesthesia by inhalation of 2% isoflurane. The GFP-positive ASC/PRP admixture (2×105/20 μL) was transplanted into the calvarial defect of 11-week-old male nude rats (F344/NJcl-rnu/rnu; CLEA, Inc., Tokyo, Japan).
Samples were collected 4 weeks after transplantation. Fresh-frozen sections of these samples were made according to the Kawamoto method using a Multipurpose Cryosection Preparation Kit. 38 Briefly, Cryofilm type 2C (Section-Lab Co. Ltd., Hiroshima, Japan) was applied to the cutting surface of the completely frozen block, and the block was cut with a tungsten carbide knife at −25°C in a cryostat chamber (Leica CM3050S; Leica Microsystems, Wetzlar, Germany). Sections were fixed with 4% PFA for 3 min and then washed with PBS for 3 min. A mouse monoclonal anti-osteocalcin antibody (1:200 dilution; Abcam, Inc.), a rabbit polyclonal anti-osteocalcin antibody (1:200 dilution; Abcam, Inc.), and a rabbit polyclonal anti-GFP antibody (1:1000 dilution; Abcam, Inc.) were used as the primary antibodies. An Alexa Fluor 488-conjugated goat anti-rabbit IgG (A-11034; Invitrogen, Carlsbad, CA) and an Alexa Fluor 594-conjugated goat anti-mouse IgG (A-11032; Invitrogen) were used as the secondary antibodies. Sections were mounted using mounting medium containing DAPI (H-1200; Vector Laboratories, Inc., Burlingame, CA). After fixation, specimens were observed by fluorescence microscopy (Axioplan 2 imaging microscope and Axiovision software; Zeiss Co., Berlin, Germany).
Statistical analysis
All results were compared using the Kruskal–Wallis test and, if necessary, the Mann–Whitney test. Statistical analyses were performed using GraphPad Prism for Windows (GraphPad Software, La Jolla, CA). A p-value <0.05 was considered to be significant.
Results
Primary culture of ASCs
Digestion of the inguinal fat pads of a F344 rat yielded ∼5×105 nucleated cells, which were used in primary cultures. The cells expanded rapidly in vitro and formed a heterogeneous population that morphologically resembled fibroblast-like cells, as described in previous reports. 35
Platelet counts in PRP
The four whole blood samples contained a mean of 19.1×104/mL platelets, whereas the mean platelet count in the resulting PRP samples was 180.1×104/mL (i.e., the platelet count was ninefold higher in PRP than in whole blood).
Levels of growth factors in PRP
Levels of growth factors (IGF-1, TGF-β1, HGF, VEGF, and PDGF-AB) in whole blood plasma, preactivated PRP, and postactivated PRP were quantified using ELISAs. The concentrations of IGF-1, TGF-β1, HGF, VEGF, and PDGF-AB were 1.3-, 5.3-, 6.5-, 313.3-, and 6.7-fold higher, respectively, in postactivated PRP than in preactivated PRP. Moreover, the concentrations of IGF-1, TGF-β1, HGF, VEGF, and PDGF-AB were 1.6-, 6.1-, 82.7-, 3133.0-, and 13.7-fold higher, respectively, in postactivated PRP than in whole blood plasma (Fig. 1A).

Concentrations of growth factors secreted from postactivated PRP, preactivated PRP, whole blood plasma, and ASCs in specific culture conditions.
Levels of secreted growth factors in ASC culture supernatant
Levels of growth factors (IGF-1, TGF-β1, HGF, VEGF, and PDGF-AB) in the culture supernatant of ASCs cultured in the presence of 10% FBS or 5% PRP were quantified by ELISAs. PDGF-AB was not detected in either type of cell culture supernatant. The concentrations of the other four growth factors were significantly higher in ASC culture supernatants containing 5% PRP than in those containing 10% FBS. The concentrations of IGF-1, TGF-β1, HGF, and VEGF were 5.7-, 5.2-, 3.6-, and 1.1-fold higher, respectively, in ASC culture supernatants containing 5% PRP than in those containing 10% FBS (Fig. 1B).
SEM observation of activated PRP with/without ASCs
SEM observations of PRP found a high level of densely formed fibrin fibers, a large amount of platelets, and few erythrocytes and leukocytes in the fiber network. The platelets did not exhibit morphologies typical of their resting state. By contrast, the SEM observations of ASC/PRP admixtures revealed that ASCs were encapsulated in a highly condensed fibrin fiber network containing a large amount of platelets (Fig. 2).
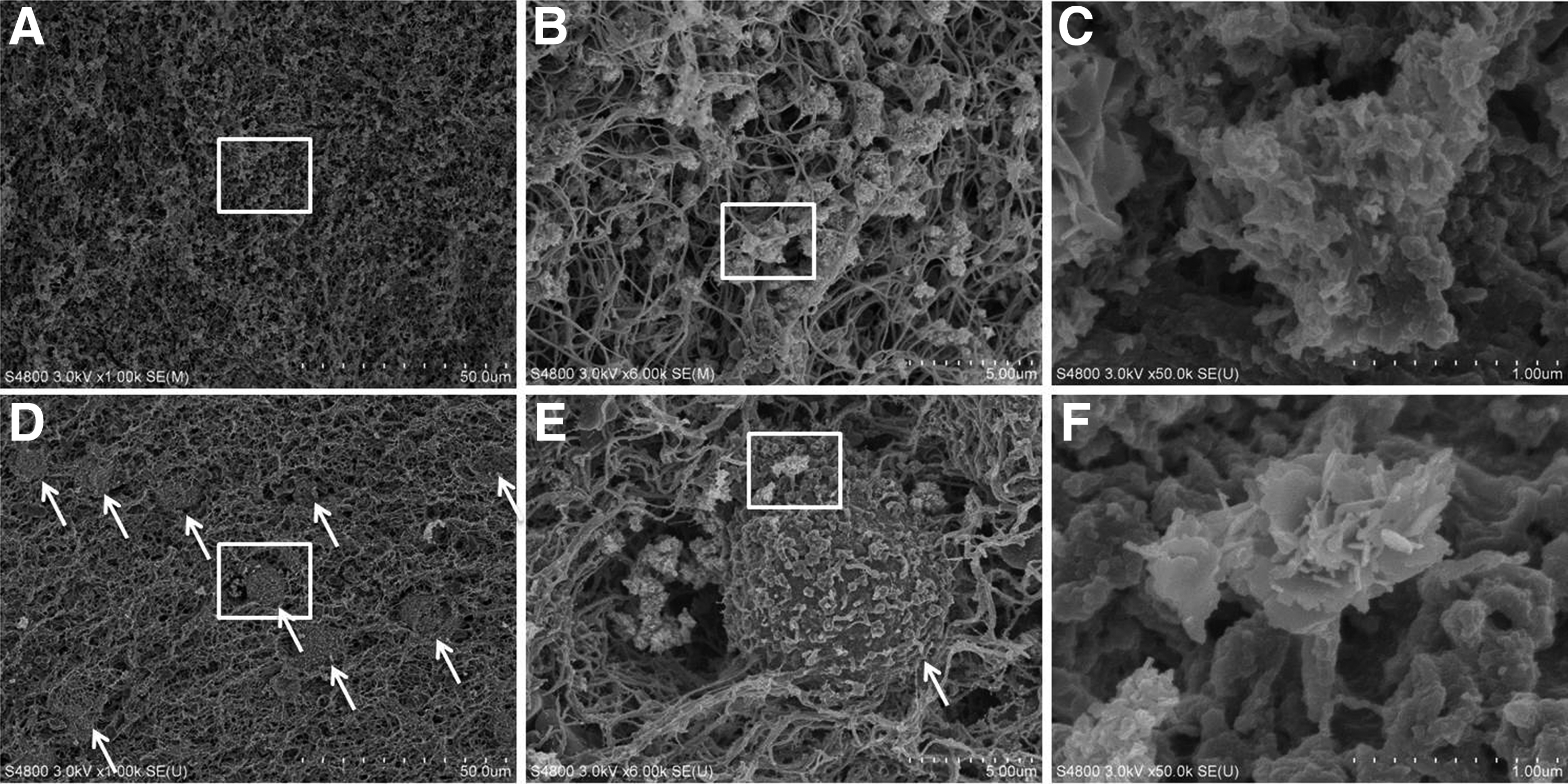
Scanning electron microscopy observations of activated PRP with/without ASCs.
Micro-CT analysis of newly formed bone
Micro-CT analysis demonstrated that both the surface area and three-dimensional volume of newly formed bone were significantly larger in Group 1 than in the other groups. The mean percentage of the surface area of the defect that was covered with newly formed bone at 4 and 8 weeks after transplantation was 94.0% and 95.6% in Group 1, 70.2% and 67.7% in Group 2, 49.8% and 56.4% in Group 3, 44.9% and 52.7% in Group 4, and 23.5% and 35.7% in Group 5, respectively. The mean percentage of the three-dimensional volume of the defect that was filled with newly formed bone at 4 and 8 weeks after transplantation was 48.2% and 66.1% in Group 1, 36.2% and 34.6% in Group 2, 22.9% and 28.5% in Group 3, 17.0% and 24.4% in Group 4, and 10.0% and 14.9% in Group 5, respectively (Fig. 3).
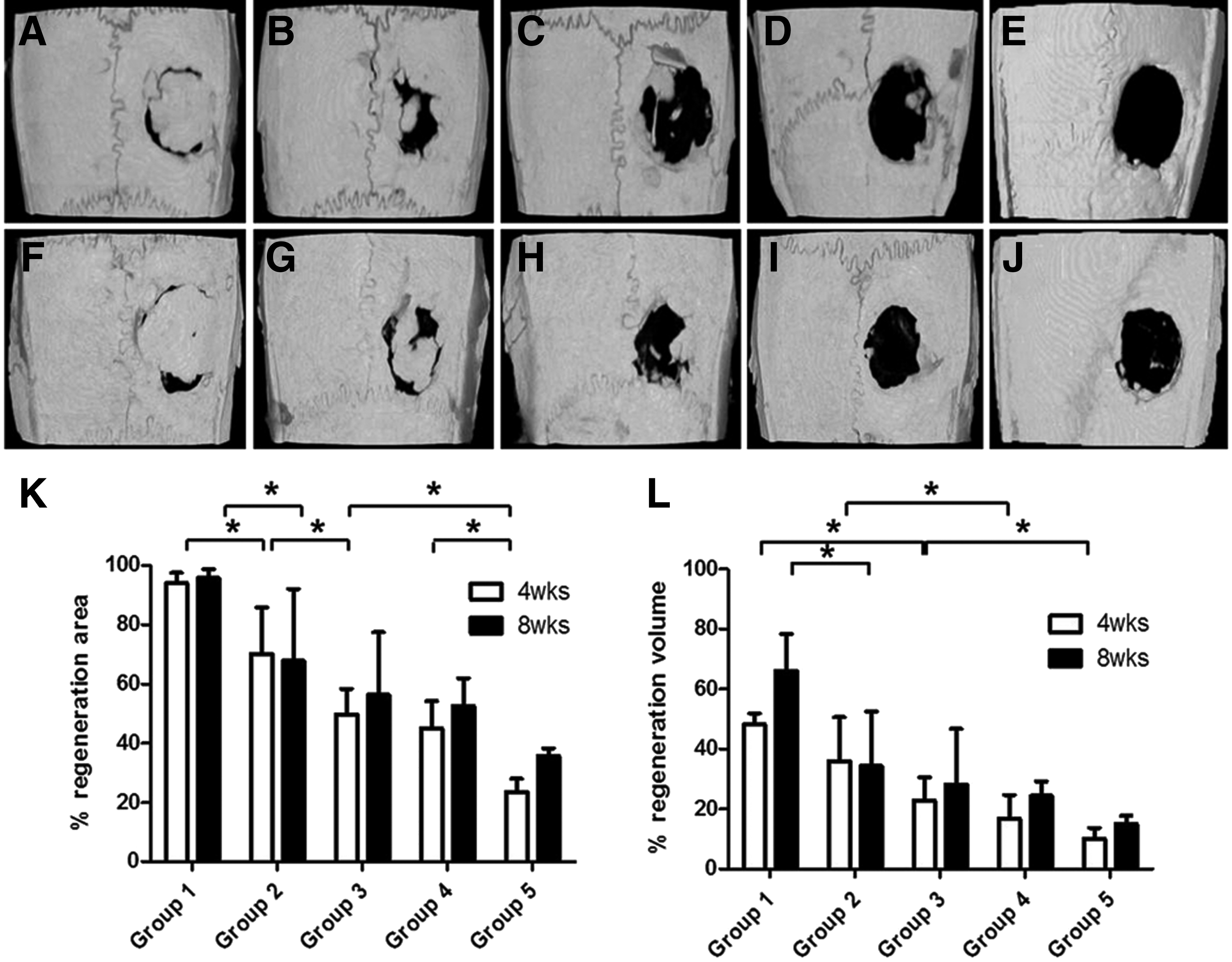
Microcomputed tomography images of bone defects in each group at 4 weeks
Histological analysis
Four weeks after transplantation, fusion of newly formed bone with original bone was observed in Group 1. Furthermore, in this group, newly formed bone with lacunae was observed, which was connected to the original bone. By contrast, in the other groups, fusion of newly formed bone with original bone was not observed at 4 weeks after transplantation. In addition, inflammatory cell infiltration was seen at the bone defect site, a characteristic of inadequate healing processes. Eight weeks after transplantation, the thickness of newly formed bone had increased in Group 1. In Groups 2 and 3, fibrosis and woven bone were observed in the defect site, whereas in Groups 4 and 5, fibrous connective tissue was observed in the defect site (Fig. 4). In samples stained with Alcian blue, mucopolysaccharides were observed in the extracellular matrix of immature newly formed bone in Group 1 at 4 and 8 weeks after transplantation (Fig. 5).

Hematoxylin and eosin staining in each group at 4 weeks
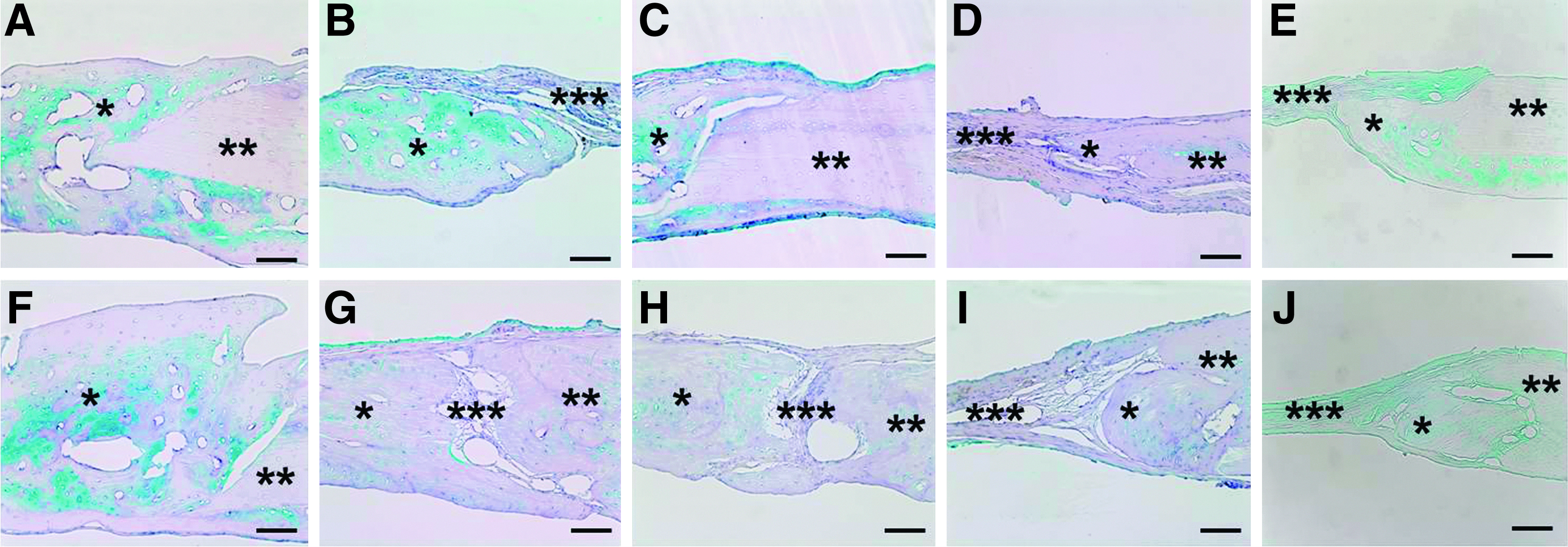
Alcian blue staining of mucopolysaccharides in each group at 4 weeks
Immunohistochemistry
Tissue specimens were analyzed by performing immunohistochemical staining for osteopontin and osteocalcin at 4 and 8 weeks after transplantation. Osteopontin-positive cells were observed at the center of newly formed bone in Group 1. In addition, cells that stained positive for osteocalcin were present throughout the newly formed bone in this group (Fig. 6).
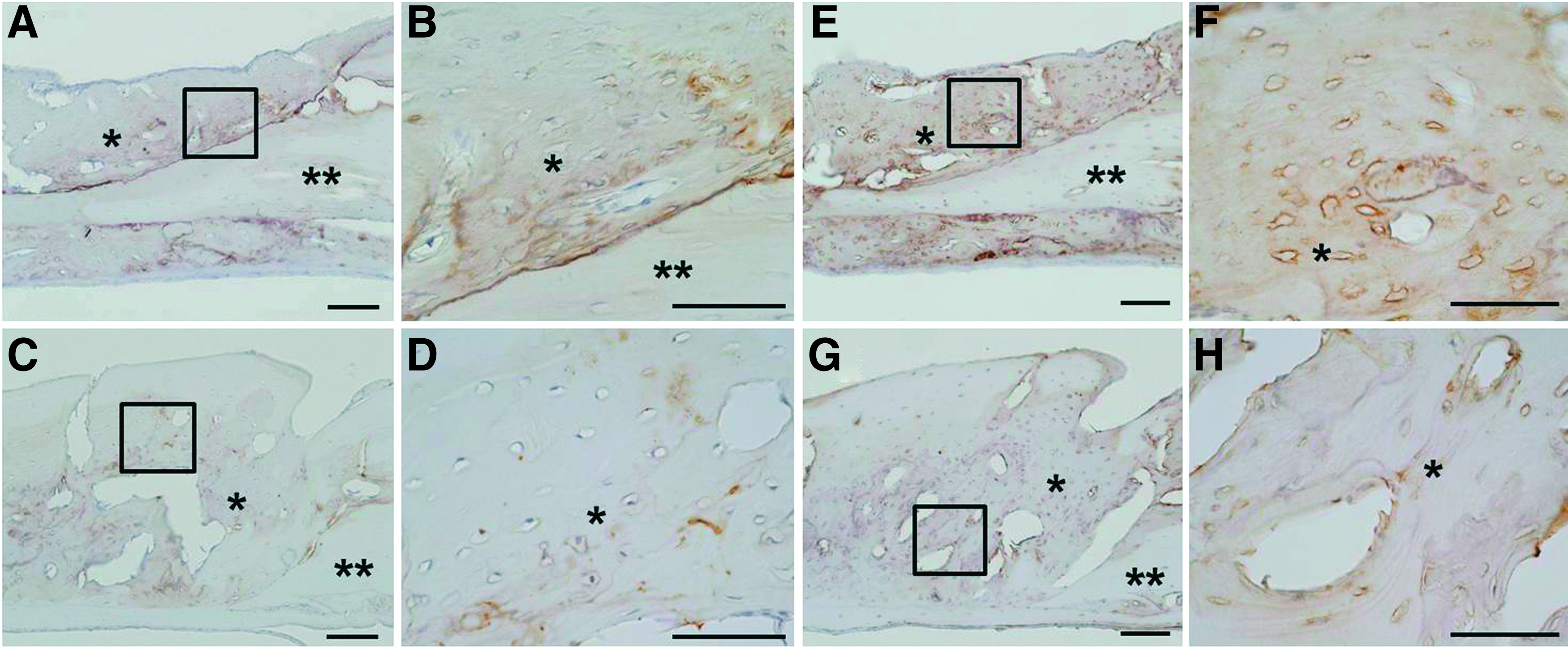
Immunohistological observation of osteopontin
Immunohistochemical evaluation of transplantation of ASCs derived from a GFP-transgenic mouse into nude rats
An admixture of GFP-positive ASCs and PRP was transplanted into the calvarial defect of nude rats to evaluate the origin of newly formed bone. Tissue specimens were analyzed by performing immunohistochemical staining with anti-rat osteocalcin and anti-mouse osteocalcin antibodies. Both rat and mouse osteocalcin-positive cells were observed in newly formed bone (Fig. 7A). High magnification images of the newly formed bone detected lacunae-like structures, which stained positive for mouse osteocalcin (Fig. 7B). To confirm that osteoblastic differentiation of ASCs was induced by the transplanted ASC/PRP admixture in the calvarial bone defect, the mouse cells expressing GFP in the regenerated bone were stained with an anti-mouse osteocalcin antibody and a fluorescence-labeled secondary antibody. Cell nuclei were labeled with DAPI (blue). A number of cells in the newly regenerated bone in the ASC/PRP group displayed both mouse osteocalcin (red) and GFP (green) expression (Fig. 7C–F).
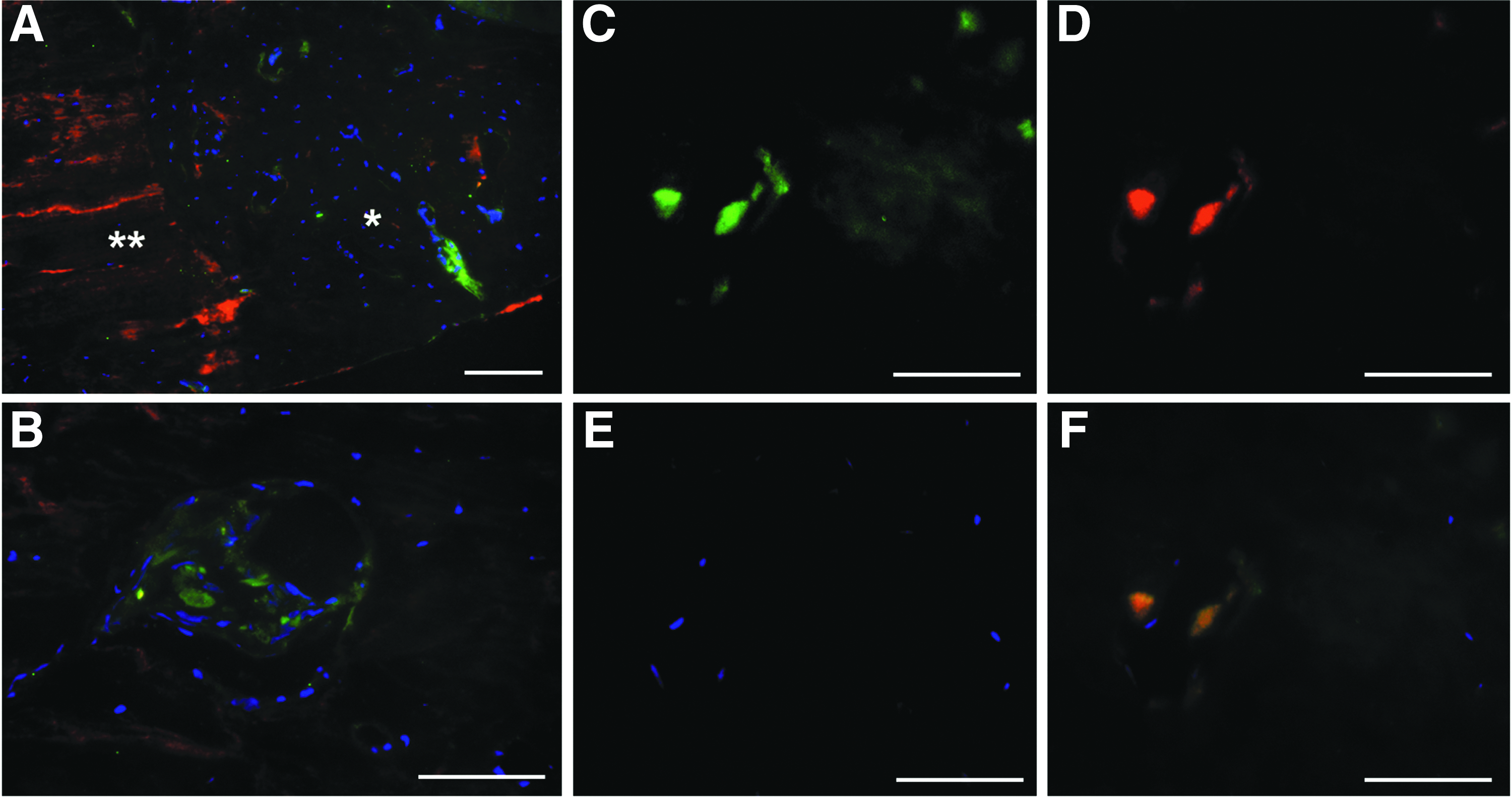
Fluorescence immunohistochemical staining using anti-rat osteocalcin and anti-mouse osteocalcin antibodies
Discussion
In this study, an ASC/PRP admixture had dramatic effects on bone regeneration in a rat calvarial defect model. The following strands of evidence suggest that the combination of ASCs and PRP is effective for bone regeneration: (1) the concentrations of growth factors (IGF-1, TGF-β1, HGF, and VEGF) secreted by ASCs were significantly increased by the addition of PRP, (2) some ASCs directly differentiated into osteoblasts in vivo, and (3) the ASC/PRP admixture contributed to regenerate suitably thick bone with lacunae, which was connected to the original bone.
Some studies have investigated the secretion profiles of ASCs.39,40 ASCs were found to secrete angiogenic cytokines (VEGF and HGF) both in vitro and in vivo, which increases neovascularization and enhances wound healing in injured tissues.41,42 Moreover, Luo et al. reported that ASCs are protected from apoptosis in nerve regeneration by the TGF-β1-dependent reduction in inflammation and promotion of VEGF-dependent angiogenesis. 43 Many factors that are secreted by ASCs function in mechanisms that mediate protection against cell death or, alternatively, induce cell migration and proliferation. 44 However, it was reported that ASCs only release a small amount of PDGF, one of the most important growth factors for bone formation.40,45 Therefore, since the transplantation of ASCs by themselves is not advantageous for bone tissue engineering, the ASCs/PRP admixture may be a useful combination. Furthermore, our results suggest that concentrations of TGF-β1, VEGF, IGF-1, and HGF were significantly higher in ASC culture supernatants containing 5% PRP than in those containing 10% FBS. This indicates that PRP induces the release of growth factors from ASCs. Moreover, a statistically significant increase in VEGF (1.1-fold) was observed when ASCs were cultured in the presence of 5% PRP versus 10% FBS. Several studies have reported that VEGF promotes neovascularization during bone formation and remodeling.46,47 Furthermore, VEGF protects MSCs from culture-induced cellular stress and improves MSC viability. 48 Therefore, although the concentration of VEGF in ASCs increased by only 1.1-fold, this result might be functionally significant and contribute to bone regeneration. Ng et al. reported that the TGF-β, PDGF, and FGF signaling pathways are key for the differentiation of MSCs into adipogenic, chondrogenic, and osteogenic lineages. 49 The differentiation of MSCs into these lineages is affected when these pathways are perturbed by inhibitors of cell surface receptor function. Therefore, the massive release of growth factors from ASCs might contribute to the osteogenic differentiation of transplanted ASCs.
Meanwhile, our study also revealed that postactivated PRP (treated with 10% calcium chloride solution) contained higher concentrations of some growth factors than preactivated PRP. PRP contains several growth factors (e.g., PDGF, TGF, IGF, VEGF, and HGF) and these are released through degranulation, which stimulates the healing of bone and soft tissue. 50 These growth factors are mitogenic for osteoblasts and stimulate the migration of mesenchymal progenitor cells. 51 Growth factors in PRP affect cellular proliferation and differentiation during bone repair. 52 The fibrin matrix itself may also contribute to healing by providing a conductive scaffold for new matrix formation. PDGF reportedly plays an important role in bone regeneration. 53 The most important activities of PDGF include mitogenesis, angiogenesis, macrophage activation, and activation of paracrine signaling. In this study, pre/postactivated PRP contained PDGF-AB, which was not released from ASCs. PRP supports bone reconstruction by reducing the time required for bone regeneration. 53 Additionally, platelets reportedly release growth factors slowly over a 7-day period upon PRP activation without thrombin. 54 Furthermore, many studies have reported that PRP supports bone regeneration with stem cells.14,53,55 These reports and the results of this study suggest that PRP is extremely useful for stem cell therapies.
Our results showed that an admixture of ASCs and PRP induced formation of newly formed bone. Moreover, some mouse-derived ASCs directly differentiated into osteoblasts in the calvarial bone defect of a nude rat. This is of significance to regeneration therapy using stem cell transplantation.
In this study, in rats that received the ASC/PRP admixture, cells that positively stained with Alcian blue and anti-osteopontin and anti-osteocalcin antibodies were formed in newly regenerated bone up to 8 weeks after transplantation. In addition, in this group of rats, the area positively stained with Alcian blue and the anti-osteopontin antibodies coincided at 4 and 8 weeks after transplantation. These observations indicate that transplantation of the ASC/PRP admixture resulted in continuous generation of immature bone, which was connected with the original bone and was suitably thick. The primary focus of this study was to evaluate the new-formed bone structure. We did not perform any mechanical testing in this particular experiment since we used calvarial bone, which is less amenable to mechanical stress than the long bone of the extremities; however, an important purpose of bone tissue engineering research is to regenerate bone that maintains mechanical strength, so studies are planned in a large animal model to allow mechanical testing.
In conclusion, the ASC/PRP admixture contributes to bone repair, not only through the osteogenic potential of ASCs, but also through the release of cytokines by platelets in PRP, which, in turn, support ASCs. These results pave the way for future clinical trials using admixtures of ASCs and PRP. However, some issues remain to be resolved regarding the bone-healing effects of ASCs, including their abilities to induce osteogenesis and regeneration in large bone defect models.56–58 Further analyses are required to investigate the biological interaction of ASCs and PRP for bone regeneration.
Footnotes
Acknowledgments
We would like to thank Ryuji Tsukada and Toyoko Hidano (Division of Experimental Surgery and Biomedical Resources, Juntendo University Graduate School of Medicine) for their expert assistance with animal experiments, Takako Ikegami and Tomomi Ikeda (Laboratory of Molecular and Biochemical Research, Research Support Center, Juntendo University Graduate School of Medicine) for technical assistance, Noriyoshi Sueyoshi, Shinji Nakamura, Yuko Kojima, Yasuko Toi, and Katsumi Miyahara (Laboratory of Biomedical Imaging Research, Biomedical Research Center, Juntendo University Graduate School of Medicine) for their expert assistance with histological analyses, and Junichi Nakamoto (Laboratory of Ultrastructural Research, Juntendo University Graduate School of Medicine) for his expert assistance with SEM analyses.
Authors' Contributions
Each author's contributions to this article; Satoshi Tajima: conception and design, collection and/or assembly of data, data analysis and interpretation, and article writing; Morikuni Tobita: conception and design, data analysis and interpretation; Hakan Orbay: collection and/or assembly of data; Hiko Hyakusoku: data analysis and interpretation; Hiroshi Mizuno: conception and design, financial support, data analysis and interpretation, and final approval of article.
Disclosure Statement
No competing financial interests exist.