
Abstract
A series of metal stents coated with chitosan/hyaluronic acid (CS/HA) loading antibodies by electrostatic self-assembled method were prepared, and the types of cells captured by antibodies and their differentiation in vascular endothelial cells (ECs) evaluated by molecular biology and scanning electron microscope. The results showed that CD133 stent can selectively capture hematopoietic stem cells (HSC),which directionally differentiate into vascular ECs in peripheral blood by (CS/HA) induction, and simultaneously inhibit migration and proliferation of immune cells and vascular smooth muscle cells (MCs). CD34 stent can capture HSC, hematopoietic progenitor cells that differentiate into vascular ECs and immune cells, promoting smooth MCs growth, leading to thrombosis, inflammation, and rejection. CD133 stent can be implanted into miniature pig heart coronary and can repair vascular damage by capturing own HSC, thus contributing to the rapid natural vascular repair, avoiding inflammation and rejection, thrombosis and restenosis. These studies demonstrated that CD133 stent of HSC capture will be an ideal coated metal stent providing a new therapeutic approach for cardiovascular and cerebrovascular disease.
Introduction
C
The second generation drug-eluting stents might inhibit rejection and intimal hyperplasia by drugs carried in coatings with reducing the rate of in-stent restenosis significantly. In 2002, Sirolimus eluting stent (SES stent) joined the market in Europe and was quickly promoted into the whole world. Sirolimus can inhibit proliferation of smooth MCs and intimal hyperplasia of blood vessels, thus reducing restenosis. In 2004, Paclitaxel stent went public in Europe and America. They also reduce the rate of restenosis by inhibiting the proliferation of vascular smooth MCs. Clinical results show that drug-eluting stents can decrease the rate of in-stent restenosis to within 5–9% and have good therapeutic effect to coronary artery stenosis. Drug-eluting stents had lower definite thrombosis rates compared with bare-metal stents in 2-year follow-ups.1,2 At present, ∼70% of stents implanted are drug-eluting stents with 300 million patients in 2012. However, Sirolimus delay the formation of functional endothelial layers on stent, which interfere the natural repair process of blood vessels, raising the risks of long-term in-stent restenosis and thrombosis formation. Similarly, Paclitaxel possesses strong cytotoxicity and poor selectivity, so it inhibits the proliferation of smooth MCs and hurts normal cells at the same time, which may bring about distal stimulating effect and cause long-term restenosis, explaining the fact of 20% restenosis in 6 months.3–7
In 2005, Aoki J from Toronto University reported that the third generation bioengineered stent captures cells in peripheral blood and accelerates natural repair of blood vessels by loading antibody in the coating. The CD34 stent was developed with CD34 antibody fixed by Teflon on the surface, and it accelerates endothelialization of blood vessels by capturing endothelial progenitor cells (EPCs) in peripheral blood to injured regions. Clinical safety and feasibility of CD34 stent have been confirmed with a lower restenosis rate of 4.4%, and no late stent thrombosis in 1 year. CD34 stent has been certified for clinical use by the European Union and marketed.8–11 In vivo cell seeding with anti-CD34 antibodies successfully accelerates endothelialization, but stimulates intimal hyperplasia in porcine arteriovenous expanded Teflon grafts. In some areas, cells with platelet-like phenotype were observed on top of cellular layer on coated grafts. 12 Migration and proliferation of vascular smooth muscle were stimulated by CD34 Teflon, leading to lumen thickening of CD34 stent which is similar to that of bare stent and narrower than that of the SES stent. Bare-metal stents used as comparison significantly improved endothelialization of the period, but did not improve endometrial thickness in 1–3 month. 13
In 2010, Wendel reported that the competitive cells such as lymphoid progenitor cells (LPCs), myeloid progenitor cells (MPCs), and platelets, that have significantly higher concentrations than EPCs in the blood, can bind with the CD34 antibody on CD34 stent and quickly cover the EPCs captured, thus resulting in failure of this stent. The CD34 stent can not only capture hematopoietic stem cells (HSC), but also EPCs, LPCs, and MPCs to its surface, and simultaneously increase migration and proliferation of vascular smooth MCs, thus increasing the risk of early rejection and late restenosis. 14 Thus, clopidogrel prevention of thrombosis is also needed after implantation. The in-stent late loss of CD34 stent was ∼0.7–0.9 mm, which was unfavorable compared with that of drug-eluting stents. So, it has not passed certification of the FDA and SFDA up to now. 14
To improve the effectiveness of CD34 stent, Gaku Nakazawa and Bo Feng, respectively reported CD34+SES stent with CD34 antibody fixed onto the surface of SES stent.15,16 Sirolimus can inhibit both the proliferation of vascular smooth MCs and immune cells, and the proliferation of EPCs and mature endothelial cells (ECs), thus delaying early endothelialization of CD34 stent, but still needing the administration of anticlotting drugs to effectively inhibit thrombosis. 17 In 2013, Metzner A from the University Hospital Schleswig-Holstein, Germany reported that CD133+ cells are more favorable to tissue engineering of heart valves than EC and smooth MCs. 18
In this article, a series of metal stent coated with chitosan (CH)/hyaluronic acid (HA) loading CD133 (PROML1), CD34, VEGFR-2, and CD271 antibodies by electrostatic self-assembled method were prepared.19,20 The types of captured cells in peripheral blood and their differentiation results were evaluated by molecular biology fluorescence immunoassay and scanning electron microscopy (SEM). CD133 stent was found to be the most excellent, which can selectively capture HSC that directionally differentiate into EPCs by chitosan/hyaluronic acid (CS/HA) induction, thus contributing to the rapid natural vascular repair.
Materials and Methods
Antibody
Anti-human CD133 monoclonal antibody (ANC9C5, also known as PROML1; Santa Cruz), anti-human CD34 monoclonal antibody (QBEnd/10), goat anti-rabbit IgG(H+L)/TRITC second antibody, goat anti-mouse IgG(H+L)/FITC second antibody and goat anti-mouse Mo IgG(H+L)/TRITC (Beijing Zhongshan Golden-bridge Biological Technology), rabbit anti-human vascular endothelial growth factor receptor 2 polyclonal antibody (VEGFR-2; Fuzhou Xin Mai Biological Technology), anti-human CD271 monoclonal antibody (Biolegend), anti-human CD7/FITC, CD20/FITC, and CD61/FITC monoclonal antibody (Biolegend). Anti-human β-actin monoclonal antibody (Sigma-Aldrich).
Materials
A 316L stainless steel stent from MicroPort Medical Shanghai, 316L stainless steel plate was coated by CS/HA loading CD133, CD34, VEGFR-2, or CD271 antibody, respectively. CS/HA/CD133 stent, CS/heparin/CD34 stent, and poly(lactic-co-glycolic acid) (PLGA)/Sirolimus eluting stent (SES stent) implanted within pig's heart coronary artery was coated with CS/HA, CS/Heparin, and PLGA, respectively. The stent and vessel was built up by the MicroPort Medical Shanghai.
Blood
The fresh human peripheral blood with heparin anticoagulant was donated by healthy volunteers. The blood was centrifuged to obtain plasma.
Animals
Miniature Bama pigs were provided and approved by the Animal Care and Use Committee of the Chinese Army General Hospital, Experimental Animal Center. The present study was performed in accordance with the Guidelines for the Care and Use of Laboratory Animals (National Research Council, NIH Publication No. 85-23, revised 1996).
Equipment
Atomic force microscope (Jiangxi Liansheng Technology Co.), X-ray diffraction analyzer (Rigaku D/max2400), SEM (Hitachi-S3400N), fluorescence optical microscope (Nikon 80i), and cell incubator (Nikon).
Hoechst 33342 dyeing
Antibody-coated stents were incubated in fresh human peripheral blood, put in Hoechst 33342 (Sichuan West Asia Reagent) solutions (500 μM/mL), further incubated for 30 min at 37°C, and then fully washed with Tween-80 phosphate buffered saline (PBS) and imaged by a fluorescence optical microscope.
Fluorescence immunohistochemical method
Antibody-coated stents were immerged into fresh human blood, incubated at 37°C for 45 min, washed with Tween-80 PBS and then incubated in CD7/FITC, CD20/FITC, CD61/FITC antibody solution at 37°C for 30 min. The uncombined fluorescence antibody was washed off with Tween-80 PBS and the stents were imaged with fluorescence optical microscope.
Scanning electron microscope
The antibody-coated stents having been incubated in fresh human peripheral blood were fixed in 2.5% glutaraldehyde, staying overnight at 4°C. Then they were dehydrated with ethanol of increasing concentrations, dealcoholized with acetonitrile of increasing concentrations, dried naturally, sprayed with gold, and imaged with SEM.
Coronary stent implantation
Twelve miniature pigs (weighing 30–35 kg), 4 pigs/group, were implanted with stents in the left anterior descending and left or right coronary artery. The method refers to reference.13,14
Statistical analysis
Data were expressed as the mean±SEM from four repeated experiments and evaluated using one-way analysis of variance followed by Student's t-test. Significant differences were established at p<0.05.
Results
HSC include primitive HSC, multipotent HSC, and hemangioblast HSC. Hematopoietic progenitor cells (HPCs) include EPCs, LPCs, and MPCs. They can differentiate into ECs, lymphoid cells, and platelets and vascular smooth MCs.
Chemical and physical characterization of (CS/HA)n/CD133 coating
(CS/HA)n multilayers loading CD133 antibody were coated on 316L steel stents surface by electrostatic self-assembled method,19,21 which is shown in Figure 1. Assay of antibody loading on stent was performed based on the principle of fluorescent antibody immune response, and showed that antibody loading on a stent weighs 50±10 ng by assay of fluorescence immunohistochemical method with Mo IgG(H+L)/TRITC antibody.
(CS/HA)n/CD133 by electrostatic self-assembled. CS/HA, chitosan/hyaluronic acid.
X-ray diffraction analysis showed that thickness of (CH/HA)7 coating on the 316L steel plate is ∼100 nm. The surface of (CH/HA)7 by atomic mechanical three-dimensional (3D) scanning microscope in Figure 2 was uniformly dense island arrangement, which improved the corrosion resistance, antithrombogenicity, and stability of the stent surface.

Atomic force microscope images of surface characterization for CH/HA base coating of (CH/HA)7 (Line roughness Ra 2.528 nm, Rp 3.188, Rmax 16.416, surface roughness Ra 2.556 nm, Rp 3.218, Rmax 53.236). CH, chitosan. Color images available online at www.liebertpub.com/tea
Biocompatibility of CH/HA base coating
Base coating (CH/HA)7 was assembled on stainless steel plates and they were put into fresh human peripheral blood, stirred at 60 rpm, incubated at 37°C for 1 and 24 h, respectively, and then imaged by SEM. The results illustrated in Figure 3 showed that the surface of the base coating was still compact after being incubated in the blood for 1 h and no platelets or other types of cells were found, but part of the surface of the base coating was corroded after being incubated in the blood for 24 h, which was caused by hydrolyzation of HA on the surface. Teflon coating of Genous R stent loading CD34 antibody can hatch adherent fibrin, platelets, and other cell types in the blood to fix on the stent surface. The results indicated that (CH/HA)7 base coating had better biocompatibility than Teflon. 11
SEM images of surface biocompatibility of (CH/HA)7 base coating in fresh human peripheral blood for left panel 1 h and right panel 24 h. SEM, scanning electron microscope.
Release degree and stability of CD133 stent
Release degree of stent loading antibody is an important indicator assuring that the stent can capture cells. CD133 stents were put into different pH solutions, stirred at 60 rpm, incubated at 37°C for 1 h, respectively, and quantified for release degrees by assay of CD133 shown in Figure 4. CD133 stents were put into PBS or heparin plasma, stirred at 60 rpm, incubated at 37°C for 0, 1, 6, 12 h, respectively, and quantified by assay of CD133. The results showed that assay of CD133 were all between 40–60 ng. CD133 stent loading antibody released in acid or base solution rather than in PBS or heparin plasma. CD133 stent has good stability within 3 months at 20–30°C and a year at 5–10°C. The results showed that CD133 stent has good stability, both transport and storage requirements.
Release degree of CD133 stent into different pH solutions for 1 h (n=4).
Molecular biology characterization of cells capture
Hoechst 33342 is a kind of DNA-conjugated dye, which can penetrate the membrane of living cells and has low toxicity to cells. Its maximum excitation wave and emission wave are 346 and 460 nm, respectively. It can enter normal cells and fitted into molecules of DNA bases. Blue fluorescence is emitted with the contribution of excitation light. As the membrane permeability of HSC is usually weak that Hoechst 33342 cannot enter into them, it is deemed that HSC resist dyeing by Hoechst 33342, but HPCs do not. CD20/FITC, CD7/FITC, and CD61/FITC were used to represent mainly B-LPCs, T-LPCs, MPCs, and platelets, respectively.
Antibody stents were put into fresh human peripheral blood, incubated at 37°C for 1 h, dyed by Hoechst 33342, and fluorescence imaged. The stents were dyed by CD20/FITC, CD7/FITC, and CD61/FITC antibody, respectively, and fluorescence imaged. The results were illustrated in Figure 5. The results suggested that CD133 stent can capture only HSC that resist dyeing by Hoechst 33342 rather than HPCs or other cells that can be dyed by Hoechst 33342. CD34 stent and VEGFR-2 stent can capture HSC and HPCs (EPCs, MPCs, and LPCs) as they further differentiate into immune cells causing inflammation and rejection and leading to thrombosis and obstruction of blood vessels. CD271 stent can only capture mesenchymal stem cells that resist dyeing by Hoechst 33342 rather than other hematopoietic cells that differentiate into various kinds of histiocytes, which were not involved in the repair of blood vessels. The results suggested that CD133 stent can only capture HSC, which could avoid inflammation and obstruction of blood vessels effectively after stent implantation.
Fluorescence images of captured cells in fresh human peripheral blood on a series of antibody-loaded coated metal stents stained by Hoechst 33342 or CD20/FITC, CD7/FITC, and CD61/FITC. Color images available online at www.liebertpub.com/tea
Morphological characterization of cells capture
Antibody stents were put into fresh human peripheral blood, stirred at 60 rpm, incubated at 37°C for 1 h, and imaged by SEM. The results were illustrated in Figure 6. These showed that CD133 plate can only capture nest-like cells with a diameter of about 6–8 μm, CD34 plate can capture nest-like cells, spindle-like cells, and globule-like cells; VEGFR-2 plate can capture not only nest-like cells, but also spindle-like cells and pebble-like cells with pseudopodium, and CD271 plate can capture more types of cells, especially a lot of mulberry-like cells, stacked sheath-like cells, and dendritic cells. The observation results suggested that CD133 plate can only capture HSC rather than other cells in peripheral blood, which is of good specificity to rapid vascular repair. CD34 plate and VEGFR-2 plate can capture HSC, and also HPCs (EPCs, MPCs, and LPCs) which have no specificity to blood vessel repair. Moreover, MPCs and LPCs might differentiate into various immune cells, leading to early stage inflammation and rejection, and platelets might form pseudomembrane, causing restenosis. The results indicated that CD133 plate can capture only nest-like HSC.
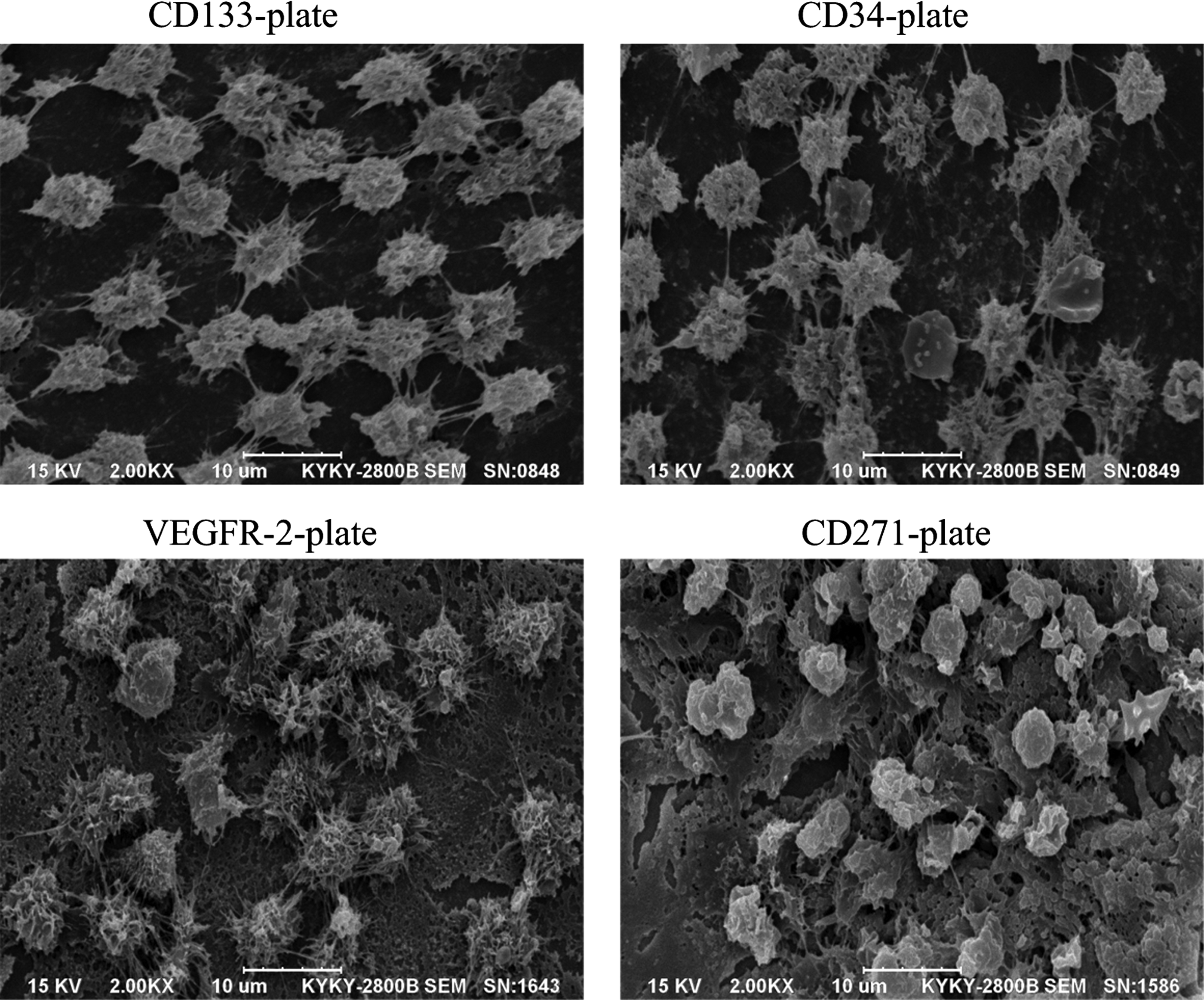
SEM images of captured cells in fresh human peripheral blood on a series of antibody-loaded metal plates at 1 h.
Morphological characterization of cell differentiation
CD133 plates and CD34 plate were put into fresh peripheral blood for 1 h, then in fresh plasma, stirred at 60 rpm, incubated at 37°C, with fresh plasma changed every 6 h. One CD133 plate and one CD34 plate each were taken out after incubation for 6, 12, and 24 h, respectively, and imaged by SEM. SEM images of captured cells and their differentiation in fresh human peripheral blood for CD133 plates and CD34 plates were shown in Figure 7. The results showed that differentiation of nest-like HSC captured by CD133 plate in peripheral blood could not be observed within the first 6 h. After incubation for 12 h, HSC differentiated into spindle-like cells engorged and full. And each cell proliferated into two pebbles-like EPCs with pseudopodium after incubation in vitro for 24 h, but the two cells did not detach fully and linking existed between them. Nest-like HSC, spindle-like cells engorged and full without foot, which had been in differentiation phase were captured by CD34 plate. After incubation in peripheral blood for 6 h, there were globule cells without foot, engorged and full cells on the plate, and all the cells became engorged and full after incubation for 12 h, and compact lymphocytes and platelets were seen on the plate after incubation for 24 h. Cells captured by the plate differentiated into tricholith-like cells, small tricholith-like cells, and pebble-like cells with pseudopodium, and also platelets with pseudopodium and silk-like muscle fibers were observed on the plate. The results indicated that HSC captured by CD133 plate had not been in differentiation phase. High molecular weight HA on the surface of the coating was hydrolyzed into low molecular weight HA, so that CS/HA could induce HSC to directionally differentiate into EPCs. HSC captured were in differentiation phase after incubation for 12 h and completed one generation of proliferation in 24 h. Not only undifferentiated HSCs, but also HPCs which were in the differentiation phase were captured by CD34 plate, and they differentiated into various hemocytes, platelets, and silk-like fibers. The results indicated that the nest-like HSC captured by CD133 plate might directionally differentiate into EPCs by CS/HA induction. But the cells captured by CD34 plate might differentiate into EPCs, MPCs, and LPCs, leading to rejection.
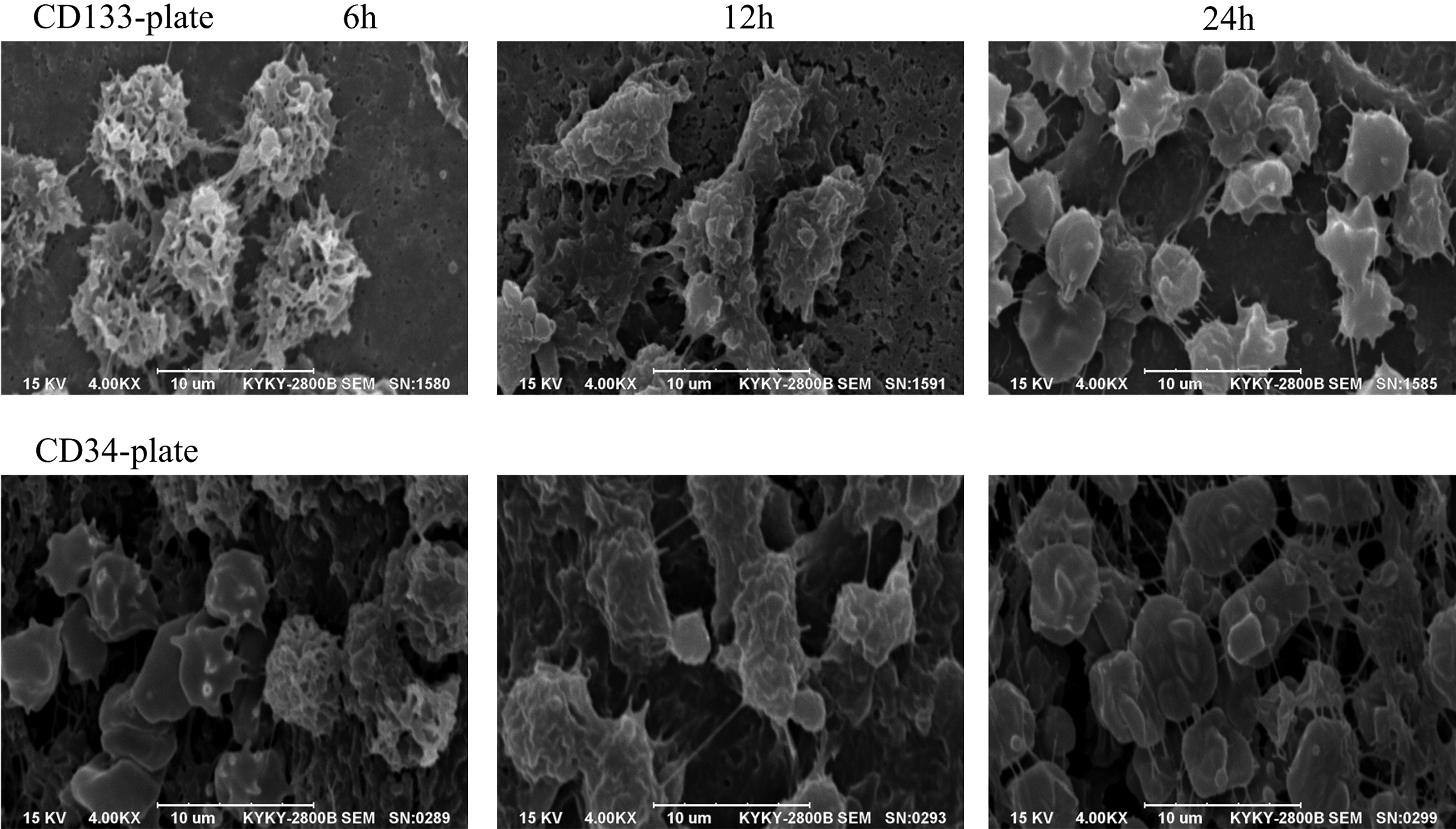
SEM images of captured cell differentiation in fresh human peripheral blood for a series of antibody-loaded metal plates at 6, 12, and 24 h.
Resistance to erosion and early endothelialization overlay within vascular implanting
Resistance to erosion of stent loading antibody in vascular blood flow is an important indicator assuring that the stent can capture cells. Early endothelialization overlay of CD133 stent and CD34 stent within implanted miniature pig ear artery at 1, 24, 48 h, were imaged by VEGFR-2 and goat anti-rabbit IgG(H+L)/TRITC second antibody which expressed in EPCs. The results were shown in Figure 8. The results showed that CD133 stent and CD34 stent can quickly capture cells expressing VEGFR-2 in 1 h. CD133 stent and CD34 stent can be endothelialized, mostly covered at 24 h and completely covered after 48 h by the differentiation of EPCs expressing VEGFR-2. The results indicated that CD133 stent and CD34 stent can quickly capture cells expressing VEGFR-2 leading to early endothelialization within implanting miniature pig ear artery. HSC captured by CD133 stent might be expressed in primitive HSC (CD133+), multipotent HSC (CD133+/CD34+) and hemangioblast HSC (CD133+/CD34+/VEGFR-2+).22–24 CD133 stent can be completely endothelialized with HSC and directionally differentiate into EPCs by CS/HA induction in 24–48 h. CD34 stent can be about 80% endothelialized. The results indicated that CD133 stent and CD34 stent have good resistance to erosion in vascular blood flow. CD133 stent can be endothelialized more completely than CD34 stent.

Fluorescence images of CD133 stent and CD34 stent capturing cells implanted within miniature pig ear artery by VEGFR-2/TRITC second antibody. Color images available online at www.liebertpub.com/tea
Vascular repair of stents implanted within the heart coronary artery
At 14 day, the newborn intimal vascular repair of CD133 stent, CD34 stent, and SES stent implanted within the small pig heart coronary artery were imaged by HE and SEM at 14 day in Figure 9.13,14 The inflammation score of newborn intimal CD133 stent was 0.10±0.10, significantly less than 1.00±0.21 of SES stent (control) and 1.64±0.38 of CD34 stent by HE staining (p<0.05, n=6). CD133 stent was endothelialized completely with pseudopodium pebble-like EPCs, which expresses no β-actin. CD34 stent was endothelialized mainly with EPCs and parallel bundle vascular smooth MCs, which expresses β-actin. SES stent was pseudomembranous, made of EPCs and filaments expressing no β-actin. The results indicated that the new intimal of CD133 stent showed no inflammation, and was endothelialized completely with pseudopodium pebble-like ECs at 14 day.
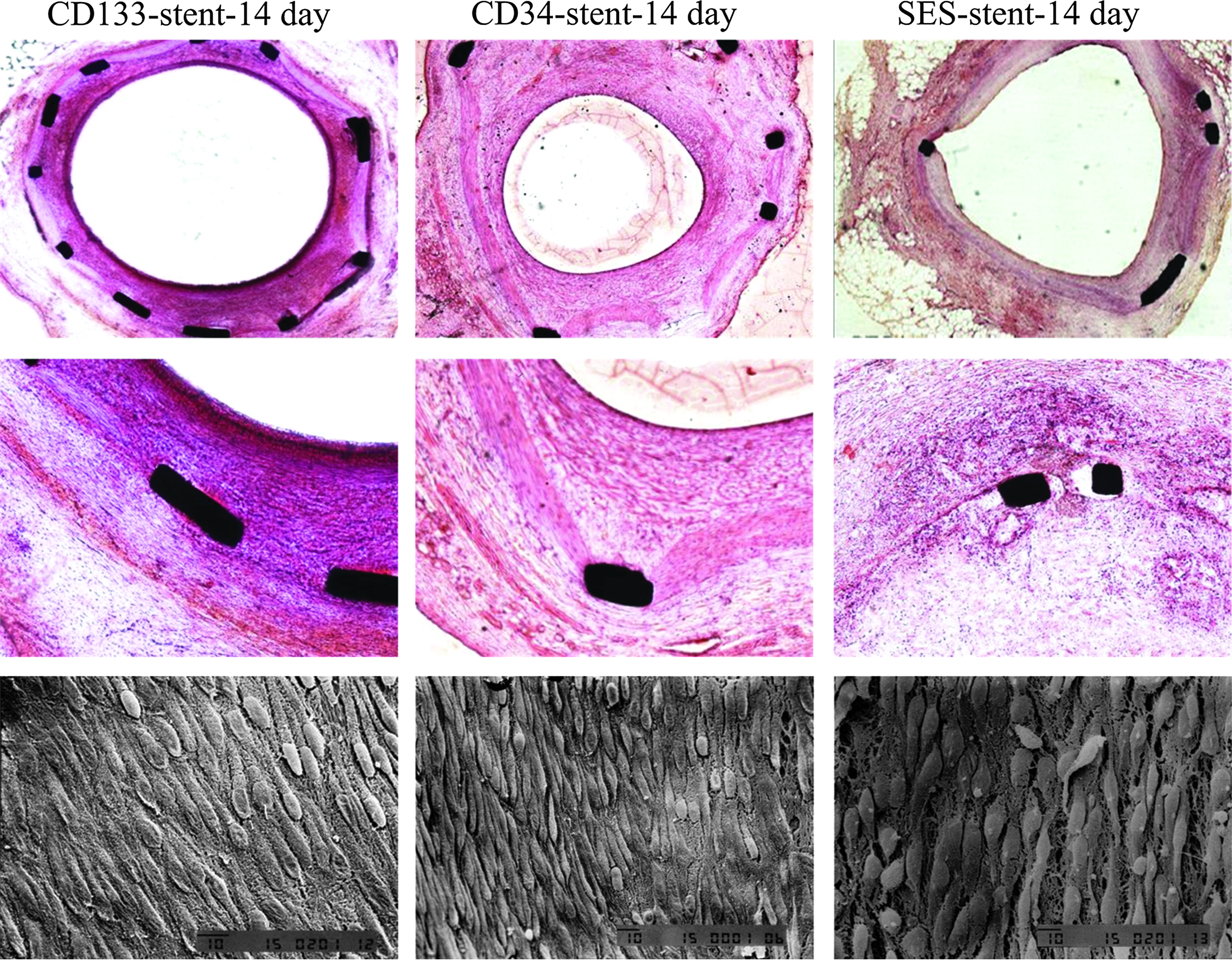
The new vascular repair of CD133 stent, CD34 stent, and SES implanted within the small pig heart coronary artery was imaged at 14 day by HE and SEM. HE, hematoxylin and eosin; SES, Sirolimus eluting stent. Color images available online at www.liebertpub.com/tea
The neo intimal of CD133 stent, CD34 stent, and SES stent implanted within the small pig heart coronary artery were imaged at 28 day by SEM and anti-human β-actin antibody and goat anti-mouse Mo IgG (H+L)/TRITC which was expressed in vascular smooth MCs, shown in Figure 10. The neo intimal thickness of CD133 stent was 180±30 μM, similar CD34+SES stent of 185±87 μM, significantly less than CD34 stent of 276±108 μM, and more than SES stent of 131±44 μM (p<0.05, n=6). The neo intimal of CD133 stent was made completely of ECs, rather than vascular smooth MCs expressing β-actin, and similar to normal coronary artery. Whereas the neo intimal of CD34 stent was made partly of ECs, some platelets, and vascular smooth MCs expressing β-actin. The neo intimal of SES stent was made completely of ECs and some of fibrin formation of pseudomembrane. The results demonstrated that CD133 stent implanted within small pig heart coronary artery can promote endothelialization, avoid inflammation and formation of pseudomembrane and inhibit smooth MCs proliferation, thus effectively reducing rejection.
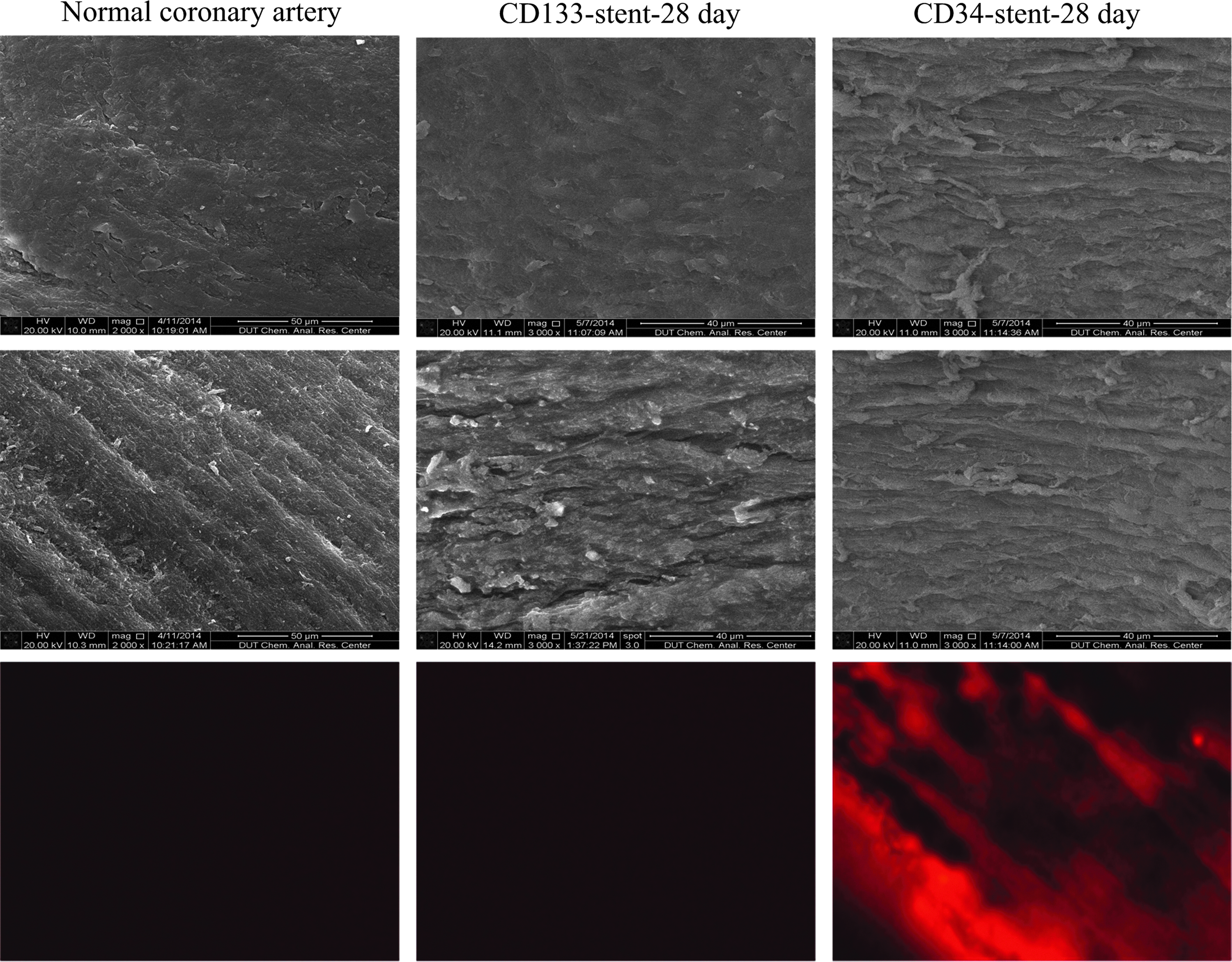
The new vascular repair of CD133 stent and CD34 stent implanted within the small pig coronary artery was imaged at 28 day, compared with normal coronary artery by SEM and β-actin/TRITC. Color images available online at www.liebertpub.com/tea
The neo intimal of CD133 stent compared with those of CD34+SES stent, CD34 stent, and SES stent in Table 1. The early endothelialization of SES stent is significantly delayed, while inflammation and rejection is inhibited, but thrombosis and late vascular restenosis is induced. The early endothelialization of CD34 stent can be rapid, but there is still inflammation and rejection, vascular smooth MCs migration, and excessive proliferation, leading to excessive late endothelialization and late restenosis. The early endothelialization of CD34+SES stent was significantly delayed, and thrombosis inhibited.15,16 The early endothelialization of CD133 stent can be rapid by selective capture of HSC, which directionally differentiates into ECs by CS/HA induction, and meanwhile it inhibits the proliferation and migration of inflammatory cells and smooth MCs, and effectively prevents the formation of inflammation in newborn dummy, effectively inhibits the inflammation rejection, reduces thrombosis and restenosis, thus contributing to the rapid natural vascular repair.
ECs, endothelial cells; HPC, hematopoietic progenitor cell; HSC, hematopoietic stem cells; LCs, lymphoid cells; MCs, muscle cells; PLGA, poly(lactic-co-glycolic acid); SES, Sirolimus eluting stent.
Discussion
Endogenous factors, such as chemistry, injury and stress, and extrinsic factors such as cytokines and drugs all can induce marrow stroma cells to cleavage symmetrically and proliferate into bone marrow-derived stem cells and mesenchymal stem cells that have the following features: (1) resist dyeing by Hoechst 33342 (specific binding fluorochrome to DNA of living cells); (2) lack of specific antigen markers of committed progenitor cells; (3) have the potential of self-renewal and multidirectional differentiation. It is these physiological characteristics that are the basis of discerning and identifying bone marrow-derived stem cells. Bone marrow-derived stem cells exhibits self-renewal potential in marrow base, while bone marrow-derived stem cells displaying multidirectional differentiation potency in peripheral blood by induction of various growth factors. Bone marrow-derived stem cells in peripheral blood reside in physiological and pathological positions of tissues and are induced to differentiate into committed HPCs and further into various kinds of functional cells. Bone marrow-derived stem cells in peripheral blood are mainly used for the natural regeneration of blood cells and a variety of naturally repair-damaged tissue. HSC assumes a major role in vascular repair. 25 There are many difficulties for the new biomedical materials of vascular repair: (1) How quickly is the selective capture of HSC without capturing other cells? (2) Is it fixed to the HSC capture site of vascular injury and not washed off by blood flow? (3) Can HSC be induced to differentiate into EPC and ECs rather than to other cells, and avoid rejection, inflammation, and thrombosis? (4) How to inhibit vascular smooth MC migration and proliferation, and avoid restenosis?
CD133 (AC133, ANC9C5, also known as PROML1, DNA encoding 4p15.32) was denominated in 2000 to be a new symbolic antigen of stem cells, which is only expressed on HSC, including HSC (CD133+), multipotent HSC (CD133+/CD34+), and hemangioblast HSC (CD133+/CD34+/VEGFR-2+). CD34 is expressed in 90% CD133+ cells, and CD133 is expressed in 40% CD34+ cells. CD133 is a stem cell marker of earlier stage than CD34 and VEGFR-2. CD133 disappears completely along with the process of HSC differentiating into HPC (Fig. 11).22,23
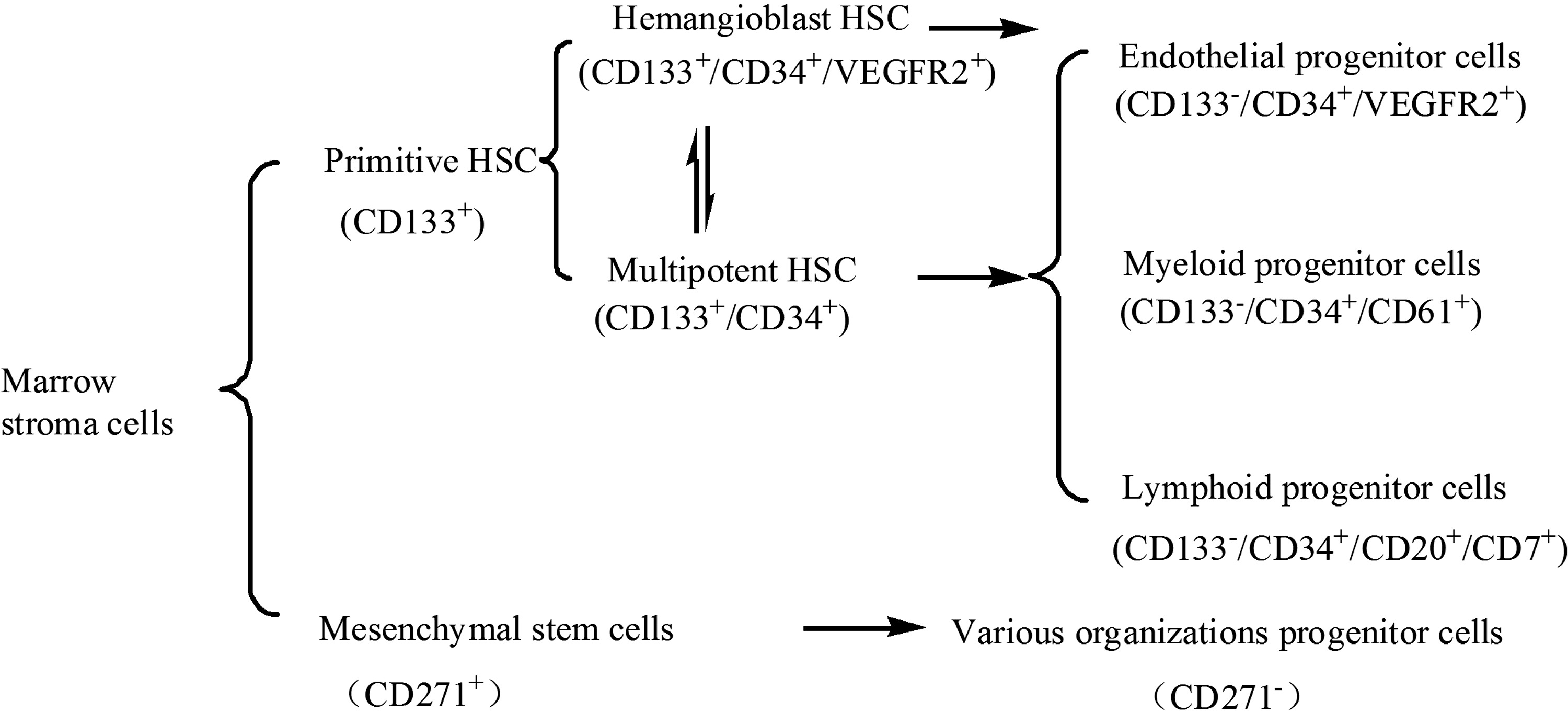
Derived from bone marrow stem cells and their differentiation process in the peripheral blood. HSC, hematopoietic stem cells.
CD34 is mainly expressed in multipotent HSC, hemangioblast HSC, EPCs (CD133−/CD34+/VEGFR-2+), MPCs (CD133−/CD34+/CD61+), and LPCs (CD133−/CD34+/CD20+/CD7+). VEGFR-2 is mainly expressed in hemangioblast HSC, EPCs, and ECs (CD133−/CD34−/VEGFR-2+). Therefore, CD133 is only expressed in HSC rather than in other cells, but CD34 and VEGFR-2 are expressed not only in HSC, but also in other progenitor cells. By the induction of vascular endothelial growth factors or low molecular weight HA, primitive HSC (CD133+) successively differentiate into multipotent HSC (CD133+/CD34+), hemangioblast HSC (CD133+/CD34+/VEGFR-2+), EPCs (CD133−/CD34+/VEGFR-2+), and ECs (CD133−/CD34−/VEGFR-2+).24,26–28 EPCs are usually in quiescent condition, but can be activated to repair injured blood vessels when the organisms suffer physiological or pathological stimulation. EPCs have the ability of sustained proliferation and differentiation into ECs under special conditions. Early formation of functional endothelial layers after injury can assist preventing intimal hyperplasia and thrombosis. CD271 is mainly expressed in mesenchymal stem cells rather than other hematopoietic cells. CD20 is mainly expressed in LPCs, and pre-B lymphocytes. CD7 is mainly expressed in LPCs, pre-T lymphocytes, and most of mature T lymphocytes, NK cells, and the like. CD61 is mainly expressed in MPCs, platelets, megakaryocytes, osteoclasts, fibroblasts, and macrophages. As a result, CD133 is only expressed in HSC compared with CD34, VEGFR-2, and CD271. By the induction of hematopoietic growth factors, MPCs (CD133−/CD34+/CD61+) can differentiate into rhodocytes, granulocytes, megacaryocytes, and platelets. LPCs (CD133−/CD34+/CD20+/CD7+) can differentiate into B lymphocytes, T lymphocytes, and NK cells. Therefore, CD133 antibody selected to capture HSC has better selectivity.
CS is an alkaline glycosaminoglycan with linear straight chain mucopolysaccharides by the alkaline hydrolysis product of natural β-1, 4 chitin glucosamine. CS has good biocompatibility, biodegradability, and antibacterial properties with inhibiting smooth MCs proliferation and promoting ECs growth. 21 CS has been approved by FDA as an absorbable surgical suture material used for the body. HA is an acid glycosaminoglycan without only acid sulfate with linear straight chain mucopolysaccharides widely present in the extracellular matrix of the human body with a high moisture resistance, viscoelasticity, lubrication, and anticoagulant biodegradable. HA exhibits high affinity for the damaged tissue, and inhibits the wound migration to immune cells, inhibiting inflammation, cell adhesion, and proliferation of fibroblasts. HA with low molecular weight plays an important role in promoting angiogenesis. HA might induce HSC to differentiate into ECs by inhibiting smooth MCs proliferation in peripheral blood, thus immobilizing HA, representing an attractive strategy for improving the thrombin resistance of endovascular devices.29–31 CH/HA base coating is good extracellular matrix environment for proliferation and differentiation of EPCs, which is similar to the real environment. 20 HSC can differentiate for 17–19 generations with the rate of one generation a day and the outermost layer of cells eventually become ECs that no longer functionally differentiates. 32 The volume of each EC cell is ∼10×20 μM, so the total theoretical value of the thickness of the 17–19 neonatal ECs is about 170–190 μM, which is consistent with the thickness of neonatal endothelial of CH/HA/CD133 stent, 180±30 μM, we have measured. Therefore, CH/HA/CD133 stent will be an ideal coated metal stent providing a new therapeutic approach for cardiovascular and cerebrovascular disease.
Conclusions
Ideal coated metal stent should have good biocompatibility and flexibility, and be suitable for surface microstructure directional differentiation of ECs with maintenance functions. It should also have nontoxicity, nonfat inflammation, and no harm to other cells and tissues. 18 We observed that CD133 stent has better resistance to blood flow erosion within the implanted artery. CD133 stent can quickly capture HSC only rather than other cells in vascular blood. HSC can differentiate directionally into ECs by CS/HA induction in the coating, and simultaneously inhibit migration and proliferation of immune cells and vascular smooth MCs, thus contributing to rapid natural vascular repair, avoiding inflammation and rejection, thrombosis, and restenosis. In comparison, CD34 stent can capture HSC and HPCs that differentiate into vascular ECs and immune cells, promoting smooth MCs growth, leading to thrombosis, inflammation and rejection. Therefore, CD133 stent will be an ideal HSC capture stent, with no administration of antirejection drugs and antithrombotic drugs within the intravascularly implanted, and can rapidly repair natural vascular and avoid inflammation and rejection. These studies demonstrated that CD133 stent of HSC capture will be an ideal coated metal stent providing a new therapeutic approach for cardiovascular and cerebrovascular disease.
Author Contributions
Bo Feng and Feng Yang partially designed and performed experiments of coronary stent implantation. Jinghan Sui, Debin Shang, and Qingyu Fan partially performed experiments of loading antibody coatings and analyzing molecular biology characterization of cells captured. Hong Zhao partially designed and performed experiments of atomic mechanical 3D scanning microscope. Fan Zhang processed images and the article syntax changes. Shixuan Zhang initiated the project, led the project team, designed and performed experiments, analyzed results, and wrote the article with input from all authors.
Footnotes
Acknowledgments
This research in experiments of coronary stent implantation was supported by the Natural Science Foundation of China (No. 30770631).
Disclosure Statement
No competing financial interests exist.