
Abstract
A promising bone graft substitute is porous titanium. Porous titanium, produced by selective laser melting (SLM), can be made as a completely open porous and load-bearing scaffold that facilitates bone regeneration through osteoconduction. In this study, the bone regenerative capacity of porous titanium is improved with a coating of osteostatin, an osteoinductive peptide that consists of the 107–111 domain of the parathyroid hormone (PTH)-related protein (PTHrP), and the effects of this osteostatin coating on bone regeneration were evaluated in vitro and in vivo. SLM-produced porous titanium received an alkali-acid-heat treatment and was coated with osteostatin through soaking in a 100 nM solution for 24 h or left uncoated. Osteostatin-coated scaffolds contained ∼0.1 μg peptide/g titanium, and in vitro 81% was released within 24 h. Human periosteum-derived osteoprogenitor cells cultured on osteostatin-coated scaffolds did not induce significant changes in osteogenic (alkaline phosphatase [ALP], collagen type 1 [Col1], osteocalcin [OCN], runt-related transcription factor 2 [Runx2]), or angiogenic (vascular endothelial growth factor [VEGF]) gene expression; however, it resulted in an upregulation of osteoprotegerin (OPG) gene expression after 24 h and a lower receptor activator of nuclear factor kappa-B ligand (RankL):OPG mRNA ratio. In vivo, osteostatin-coated, porous titanium implants increased bone regeneration in critical-sized cortical bone defects (p=0.005). Bone regeneration proceeded until 12 weeks, and femurs grafted with osteostatin-coated implants and uncoated implants recovered, respectively, 66% and 53% of the original femur torque strength (97±31 and 77±53 N·mm, not significant). In conclusion, the osteostatin coating improved bone regeneration of porous titanium. This effect was initiated after a short burst release and might be related to the observed in vitro upregulation of OPG gene expression by osteostatin in osteoprogenitor cells. Long-term beneficial effects of osteostatin-coated, porous titanium implants on bone regeneration or mechanical strength were not established here and may require optimization of the pace and dose of osteostatin release.
Introduction
B
Today, porous metallic-based implants are not only used in hip12,13 and knee 14 replacement surgery but also in craniomaxillofacial surgery.15,16 During the past decade, the development of porous titanium has greatly benefitted from the introduction of additive manufacturing techniques. These additive manufacturing techniques, such as selective laser melting (SLM), 17 enable the production of fine and precisely controlled porous structures, which can be designed to exactly meet (patient-specific) mechanical properties desired for both trabecular or cortical bone defects. 18 Manufactured porous titanium implants, containing pores ranging between 460 and 670 μm, form a unique, mechanically strong osteoconductive scaffold suitable to graft cortical bone defects.19,20 However, porous titanium may be further improved through addition of osteoinductive properties. One successful method to reinforce porous titanium with osteoinductive properties is to incorporate bioactive gels, 20 but an interesting alternative method might be to make the titanium surface bioactive.
Titanium can be made bioactive through altering the surface chemistry and topography by blasting, etching, or oxidization regimes, 21 or by deposition of an inorganic (e.g., calcium phosphates) or organic (e.g., peptides) surface coating. 22 A recently explored peptide that has potential to equip titanium with osteoinductive properties is osteostatin. Osteostatin is the N-terminal sequence 107–111 of the C-terminal domain of parathyroid hormone (PTH)-related protein (PTHrP). The short length and amino acid composition of this pentapeptide ensures its stability, and osteostatin has been shown to stimulate osteoblast activity and inhibit osteoclast activity.23,24 The exact mechanism of action is not well understood because the putative receptor through which osteostatin acts is still unknown, but ceramic-based scaffolds coated with osteostatin have, nevertheless, been shown to enhance bone regeneration in vivo.25,26 The aim of this study was to determine the potential benefits of osteostatin-coated porous titanium on bone regeneration.
Materials and Methods
Osteostatin-coated porous titanium was evaluated both in vitro and in vivo. In vitro, osteoprogenitor cells were seeded on porous titanium scaffolds with and without osteostatin coating and their proliferation and differentiation were determined. In vivo, porous titanium implants with and without osteostatin were used to graft critical-sized cortical bone defects in rats. Bone regeneration was evaluated with in vivo and ex vivo microcomputed tomography (μCT), histological analysis, and biomechanical torsion testing.
Production of osteostatin-coated and uncoated porous titanium
Disk-shaped (Ø 8×height 3 mm) porous scaffolds were used for in vitro experiments, while femur-shaped porous scaffolds were used as implants for in vivo experiments (Fig. 1A). Femur-shaped implants were a copy of the femoral bone segment removed during the in vivo experiments and had a height of 6 mm, a maximum outer diameter of 5 mm, and a minimal diameter of 1.3 mm, leaving an open medullary canal. Porous titanium was produced from Ti6Al4V ELI powder (ASTM B348, grade 23) using SLM (Layerwise N.V.). The porous architecture was based on dodecahedron unit cell design with the following dimensions: 120 μm strut size, 500 μm pore size, 88% porosity. Postproduction, all porous titanium scaffolds underwent an alkali-acid-heat treatment consisting of (i) immersion in a 5 M aqueous NaOH solution at 60°C for 24 h; (ii) immersion in water at 40°C for 24 h; (iii) immersion in 0.5 mM HCl at 40°C for 24 h; (iv) heating to 600°C at a rate of 5°C/min in an electric furnace in ambient air pressure, holding the temperature at 600°C for 1 h, and subsequent natural cooling. 21 Osteostatin was coated on the titanium surface by soaking the scaffolds in 1 mL of 100 nM solution of human PTHrP (107–111) (Bachem) in phosphate-buffered saline (PBS) at 4°C in constant rotation for 24 h. Surface uptake and subsequent release of osteostatin were measured for the rat femur-shaped porous titanium implants through the protein concentration by spectrophotometry absorbance at 280 nm, following a standard protocol described elsewhere. 27

Cell attachment and proliferation
A pool of human periosteal-derived cells (hPDCs, six donors, aged 14±2 years, passage 5) was thawed from the liquid nitrogen cell bank, expanded in a T175 flask, and harvested upon confluence. Cell suspension (i.e., 100 μL) containing 50,000 cells was drop-seeded onto osteostatin-coated and uncoated disk-shaped scaffolds and incubated statically for 1 h to allow cell attachment before being transferred onto a 3D rotator (GrantBio) to perform overnight dynamic rotation seeding. 28 For cell attachment analysis, cell-seeding efficiency was calculated by quantifying total DNA content of the cell-seeded scaffolds (n=3) using the Quant-iTTM dsDNA HS assay kit (Invitrogen). For cell proliferation assay, cell-seeded scaffolds were transferred into 24-well plates and cultured with DMEM medium (DMEM-GlutaMax™-1; Gibco) containing 10% fetal bovine serum (Gibco), 1% sodium pyruvate, and 1% antibiotics/antimycotics. Then, metabolic activity (PrestoBlue®; Life Technologies™) and total DNA content were quantified at defined time points (n=3).
Cell viability and growth morphology
Cell viability of hPDCs on osteostatin-coated and uncoated scaffolds was determined at 1, 7, and 21 days. Living cells were stained with calcein AM and dead cells with ethidium homodimer (LIVE/DEAD® cell viability kit; Life Technologies). Furthermore, cell morphology was assessed through scanning electron microscopy (SEM). Scaffolds were fixed with 2.5% glutaldehyde, postfixed with osmium tetroxide, dehydrated in gradually increased alcohol concentrations, and chemically dried with hexamethyldisilane. Then, scaffolds were sputtered with gold–palladium coating, and cell morphology was observed using SEM coupled with energy dispersive X-ray analysis (FEI XL30 FEG) at 1 kV.
Osteoblastic, osteoclastic, and angiogenic gene expression
Differentiation of hPDCs on osteostatin-coated and uncoated scaffolds was assessed by quantitative real-time polymerase chain reaction. Briefly, at 1, 7, and 21 days, cells were harvested and the total RNA was extracted using an RNA extraction kit (Qiagen) and subsequently converted into cDNA using the cDNA synthesis kit (Fermentas). Expression levels of osteoblastic markers (alkaline phosphatase [ALP], collagen type 1 [Col1], runt-related transcription factor 2 [Runx2], osteocalcin [OCN]), osteoclastic markers (receptor activator of nuclear factor kappa-B ligand [RankL], osteoprotegerin [OPG]), and an angiogenic marker (vascular endothelial growth factor [VEGF]) were quantified using Sybr Green primers (Table 1) in a Rotor-Gene sequence detector at 95°C for 3 min, 40 cycles at 95°C for 3 s, and 60°C for 60 s. Expression levels were calculated based on the 2−ΔCT method by normalizing values to the housekeeping gene, β-Actin.
Cortical femoral bone defects in rats
In 20 male Wistar rats, critical-sized cortical femoral bone defects were grafted with osteostatin-coated or uncoated, porous titanium implants (n=10). The study was approved by the Animal Ethics Committee of the Erasmus University (EMC 2811), and Dutch guidelines for care and use of laboratory animals were followed. Before surgery, rats were administered antibiotics (enrofloxacin, 5 mg/kg body weight) through subcutaneous injection. Surgery was performed aseptically under general anesthesia (1–3.5% isoflurane). First, the right femur was exposed through a lateral skin incision and blunt division of underlying fascia. Then, a 23-mm-long poly ether ether ketone (PEEK) plate was fixated to the anterolateral plane using six titanium screws (Ø 0.8×length 6.5 mm). Periosteum was removed over 8 mm of the mid-diaphyseal region before a 6-mm cortical bone segment was removed with a wire saw and a tailor-made saw guide. Then, an osteostatin-coated or uncoated implant was press-fitted into the defect. Finally, fascia and skin were sutured, and pain medication (buprenorphine, 0.05 mg/kg body weight) was administered through subcutaneous injection twice a day for 3 days. Rats were sacrificed after 12 weeks with an overdose of pentobarbital (200 mg/kg body weight).
Microcomputed tomography evaluation
Bone regeneration was measured using μCT scans (SkyScan 1076; Bruker micro-CT N.V.). In vivo μCT scans were acquired at 4, 8, and 12 weeks using a 35-μm resolution protocol (95 kV, 105 μA current, 1.0 mm Al/0.25 mm Cu filter, and 0.75° rotation step, scan time 14 min). Rats were kept under general anesthesia (1–3.5% isoflurane) during the in vivo μCT scans. Ex vivo μCT scans were acquired after sacrificing the animals using an 18-μm resolution protocol (95 kV, 100 μA current, 1.0 mm Al/0.25 mm Cu filter, and 0.5° rotation step). μCT scan images were reconstructed using volumetric reconstruction software NRecon version 1.6.6 (Bruker micro-CT N.V.).
Bone regeneration was expressed as bone volume (BV), which was measured at four specific regions: (i) total BV: the total volume of bone formed within the 6-mm defect; (ii) outer BV: the bone formed outside the implants; (iii) porous BV: the bone formed inside the porous space of the implants; and (iv) inner BV: the bone formed in the medullary canal of the implants. BV values were measured using CTAnalyzer version 1.13 (Bruker micro-CT N.V.). First, the specific region was selected, then the titanium and its border artifacts were excluded from images using a global threshold and by removal of an extra 35-μm border. Subsequently, bone was captured using a second global threshold. Global thresholds were based on visual inspection and were kept constant for all scans. Bone bridging was determined by measuring the shortest remaining gap size between bone formed at the proximal and distal side of the defect on ex vivo scans with DataViewer 1.4 (Bruker micro-CT N.V.).
Biomechanical evaluation
The mechanical strength of grafted femurs, and hence the biomechanical functionality of the implants, was measured through torsion tests conducted on eight femurs per group. After sorting all 10 grafted femurs according to their total BV after 12 weeks, the 2 middle femurs were retained for histological analysis, leaving the rest for biomechanical testing. Three contralateral intact femurs were included as controls. After harvesting the femurs, soft tissues and PEEK plates were carefully removed. Specimens were kept in 10% neutral buffered formalin solution for 2 days, minimizing the effect of formalin conservation on mechanical properties, 29 and then transferred to PBS. Subsequently, both ends of each femur were embedded in a cold-cured epoxy resin (Technovit 4071; Heraeus Kulzer GmbH). On the upper clamping side, the use of a Cardan joint ensured pure rotation without bending. The lower sides were simply fixed. Torsional strength (maximum torque to failure, N·mm) was determined with a rotation rate of 0.5°s−1 until failure using a static mechanical testing machine (Zwick GmbH).
Histological evaluation
Histology was performed on two femurs. Harvested femurs were fixed in 10% neutral buffered formalin solution for 2 days, dehydrated in graded ethanol solution from 70% to 100%, and finally embedded in methyl methacrylate. Sections of ∼20 μm were obtained using a diamond saw (Leica SP1600) and stained with basic fuchsine 0.3% solution to color bone tissue purple and methylene blue 1% solution to color fibrous tissue blue.
Statistical analyses
Statistical analyses were performed using SPSS Statistics 20.0 (SPSS, Inc.). Data are presented as mean±standard deviation (SD). For in vitro experiments, a one-way ANOVA was performed for each time point. For in vivo experiments, a linear mixed model was used to determine the interaction between treatment and time and to determine the overall effect of treatment. Ex vivo measurements (bone regeneration and biomechanical strength) were tested with an unpaired Student's t-test. A power calculation (β-value >0.80, SD ∼25%) was made to find a true difference in bone regeneration or biomechanical strength of at least 35%. Based on this calculation, n=10 was required per experimental group. A p-value<0.05 was considered statistically significant.
Results
Uptake and release profiles of osteostatin-coated porous titanium
SLM, porous titanium scaffolds had an 85% porosity with struts of 163±43 μm and a median pore size of 600 μm (range 460–670 μm) (Fig. 1A). The disk-shaped and femur-shaped scaffolds had a total surface area of, respectively, 561±11 mm2 and 314±47 mm2. The as-produced surface morphology was transferred into nanoscale organized, rod-like TiO2 crystals by the alkali-acid-heat treatment (Fig. 2). 30 After soaking for 24 h, 30% of the osteostatin in the solution was taken up by the femur-shaped scaffolds, equivalent to a 0.02 ng peptide/mm2 scaffold. This was confirmed by measuring 70% of osteostatin in the remaining solution and resulted in a cumulative dose of 4.7±0.7 ng osteostatin per femur-shaped scaffold. These femur-shaped scaffolds released 44.2%±1.5% of the osteostatin within 1 h, 81.3%±0.8% within 24 h, and 98.3%±0.7% within 72 h (Fig. 1B).

Scanning electron microscopy (SEM) images showing the surface morphology of porous titanium.
Cell attachment and proliferation
Cell-seeding efficiency of hPDCs on osteostatin-coated as well as uncoated scaffolds was ∼30% (Fig. 3A). Cell proliferation (Fig. 3B) and cell metabolic activity (Fig. 3C) steadily increased during the 21-day culture period, but on average osteostatin did not lead to significantly more cell activity or proliferation. Only at day 7, total DNA content showed a trend toward more proliferation of hPDCs on osteostatin-coated scaffolds (3008±350 ng vs. 2135±609 ng, p=0.098).

Cell viability and growth morphology
Cells attached to osteostatin-coated and uncoated titanium remained viable during the 21-day culture period (Fig. 4). Cells were already clearly attached after 1 day, but cell morphology changed from a small rounded shape toward a long and elongated shape at 21 days. No clear differences were observed between cells on osteostatin-coated or uncoated surfaces.

Osteoblastic, osteoclastogenic, and angiogenic gene expression
Gene expression of OPG, an osteoclastogenic marker, was significantly altered with osteostatin-coated scaffolds, whereas osteogenic and angiogenic markers did not show a significant difference (Fig. 5). Osteostatin upregulated OPG at day 1 (p<0.05), and RankL was considerably downregulated. As a consequence, the RankL:OPG ratio was significantly lower for osteostatin-coated scaffolds. At day 21, osteostatin downregulated OPG (p<0.05), whereas the expression of the other osteogenic (ALP, Col1, OCN, Runx2) or angiogenic (VEGF) markers measured was not altered through the presence of the osteostatin-coating on the porous titanium implants (Fig. 5).
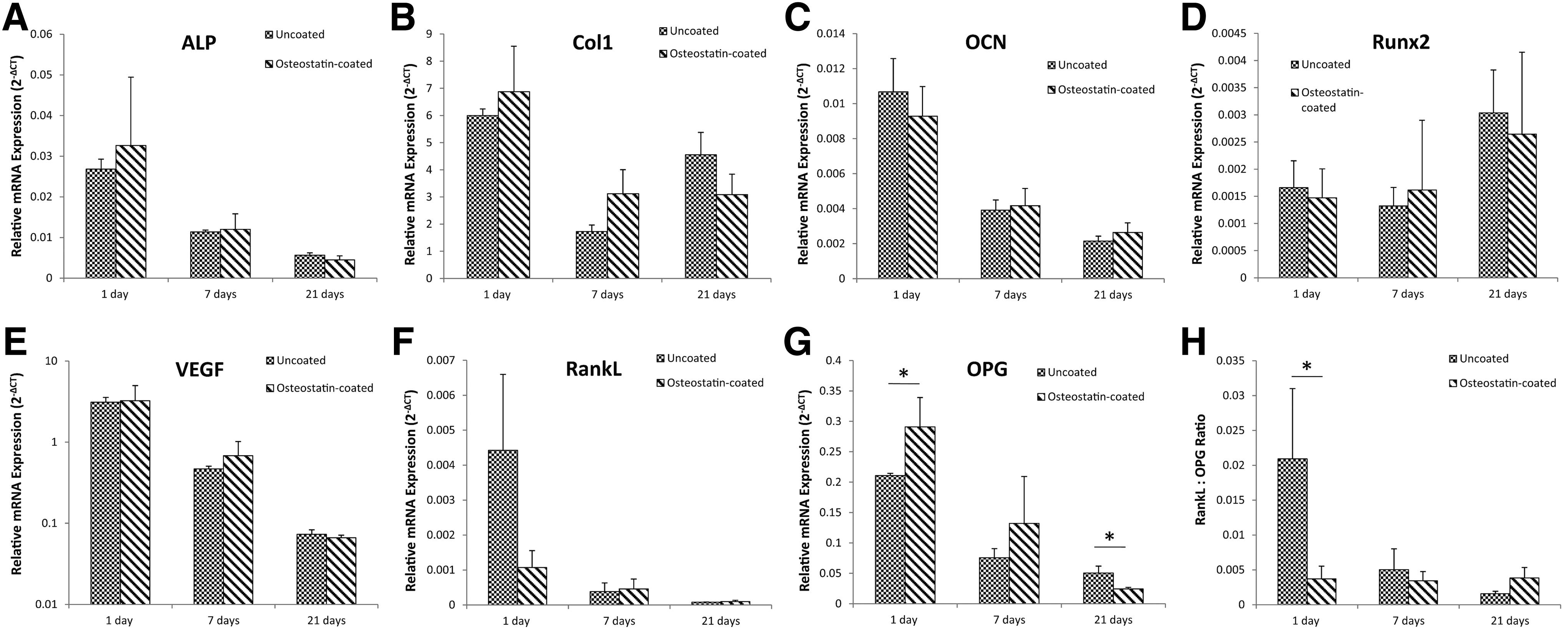
Effects of osteostatin-coated and uncoated scaffolds on expression of osteogenic markers:
Cortical femoral bone defects in rats
Rats were able to tolerate load-bearing immediately after grafting the defects, and all surgical sites healed uneventfully. One rat that received an osteostatin-coated implant was found dead after 10 weeks, the cause of death could not be determined and this rat was excluded from further analysis.
Microcomputed tomography evaluation
Grafting femur defects with osteostatin-coated, porous titanium implants led to more bone regeneration. Although the interaction between time and treatment was not significant (p=0.09), running the linear mixed model without the interaction term showed that the main effect of both treatment and time was highly significant (p=0.005, p<0.001, respectively). After 4 weeks, total BV of osteostatin-coated implants was 18.5±8.0 mm3 compared with 10.4±3.5 mm3 of uncoated implants (Fig. 6A). Bone regeneration predominantly occurred outside the implant (Fig. 6B; outer BV 9.7±5.6 mm3 vs. 4.4±1.8 mm3) and to some extent inside the implant (Fig. 6C; porous BV 6.0±2.9 mm3 vs. 3.7±1.9 mm3), but the amount of bone formed within the medullary canal was similar for osteostatin-coated and uncoated implants (Fig. 6D; inner BV 2.8±0.9 mm3 vs. 2.3±1.5 mm3).
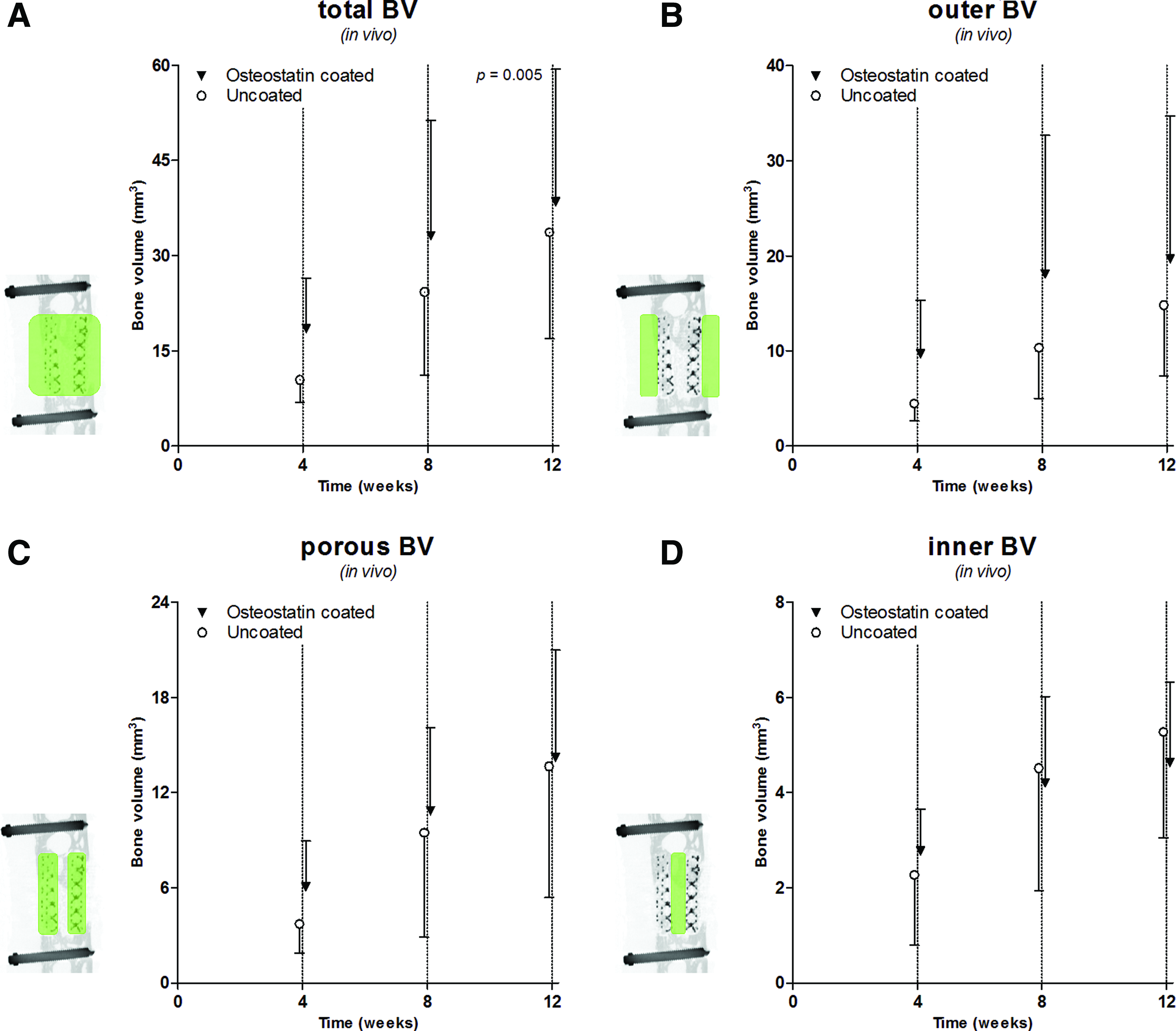
Bone regeneration quantified on in vivo microcomputed tomography (μCT) scans made after 4, 8, and 12 weeks. Green areas within the μCT images indicate the volume of interest for which bone regeneration is quantified.
The total BV of grafted defects continued to increase throughout the follow-up. Osteostatin-coated implants resulted in a total BV of 33.2±18.1 mm3 (vs. 24.3±13.1 mm3 with uncoated implants) after 8 weeks and a total BV of 38.5±20.9 mm3 (vs. 33.7±16.8 mm3 with uncoated implants) after 12 weeks. Most bone had formed outside the implants: outer BV was 49%±15% of the total BV for osteostatin-coated implants and 43%±7% of the total BV for uncoated implants. Porous BV reached 14.2±6.8 mm3 with osteostatin and 13.6±8.3 mm3 without osteostatin, meaning that, respectively, 25%±13% and 23%±13% of the porous space was occupied by regenerated bone.
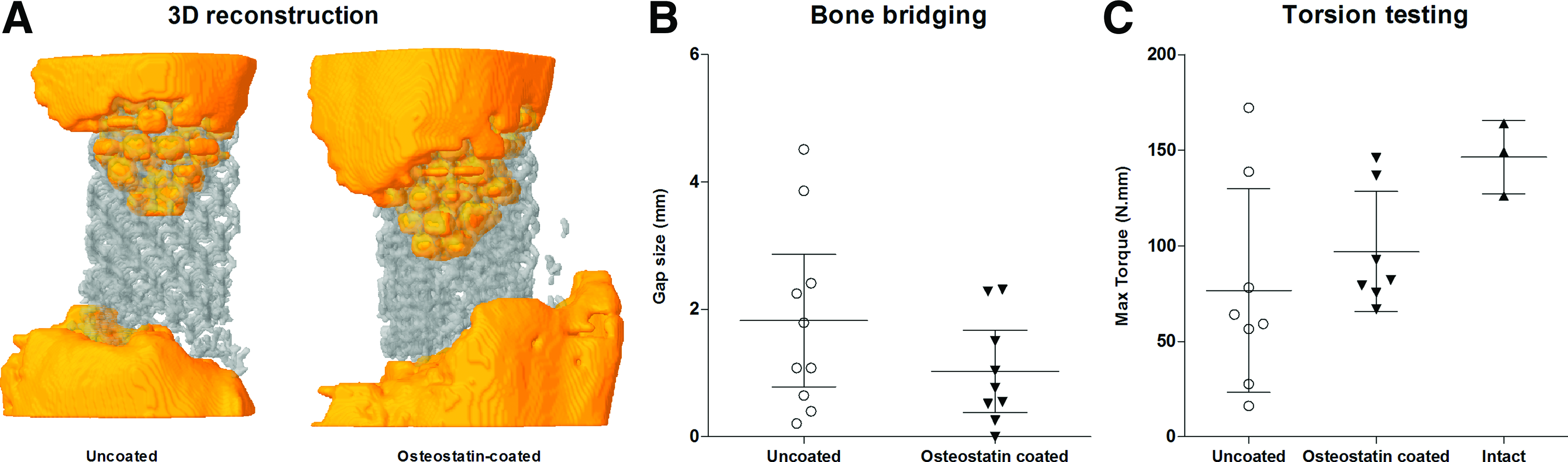
Bone bridging of grafted defects progressed throughout the 12-week follow-up and this is clearly shown on in vivo μCT scans (Fig. 7). Between 8 and 12 weeks, bone resorption of adjacent cortical bone was seen when uncoated implants were used (Fig. 7). After 12 weeks, the remaining gap of defects grafted with osteostatin-coated implants measured 1.0±0.8 mm, which was not significantly different from the uncoated implants where a remaining gap of 1.8±1.5 mm was measured (Fig. 8A, B). Nearly complete bridging (defined as gap <0.5 mm) was seen in three defects grafted with osteostatin-coated implants and in two defects grafted with uncoated implants.
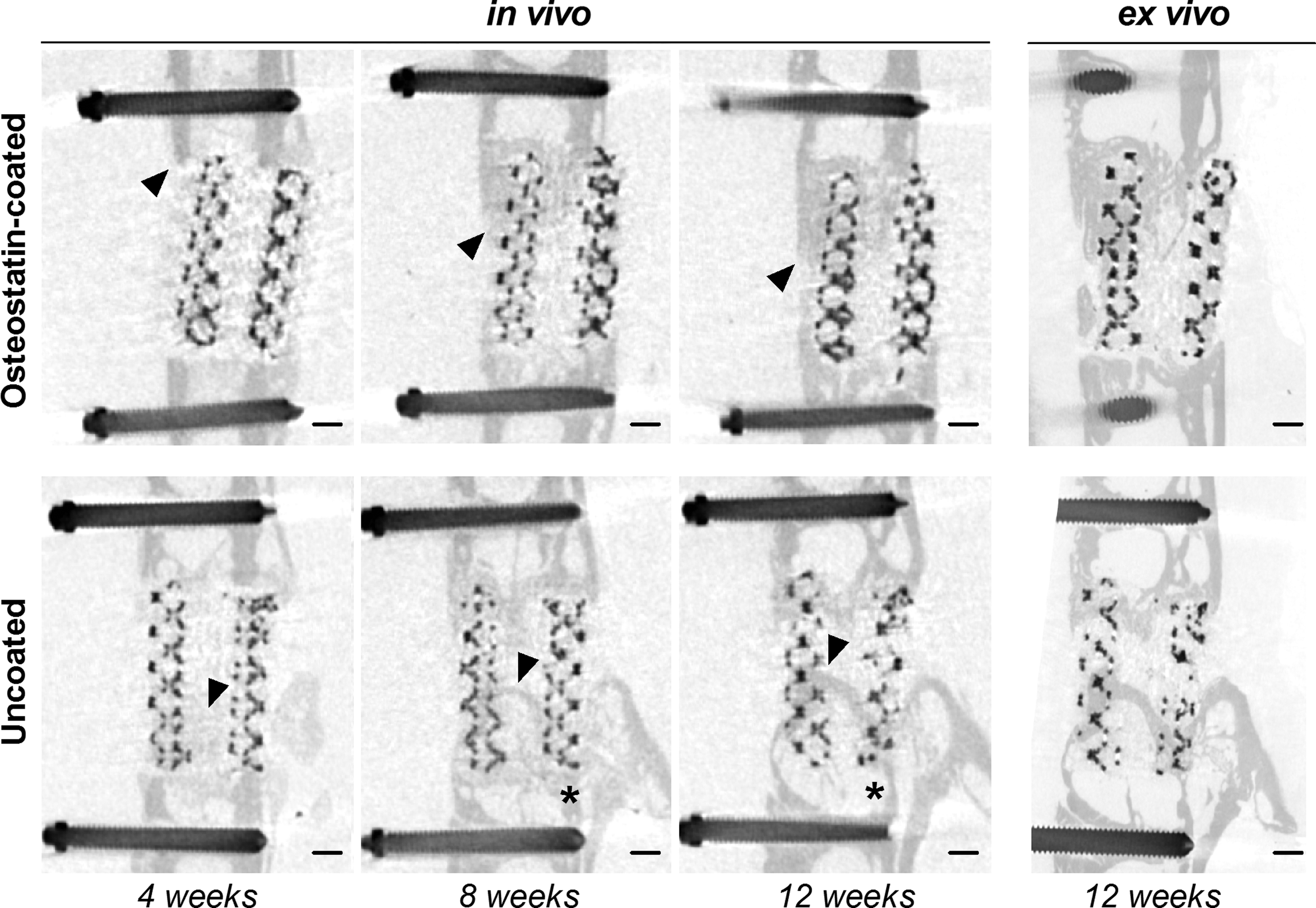
Representative in vivo and ex vivo μCT images of a femur defect grafted with osteostatin-coated (top row) or uncoated (bottom row), porous titanium implants (longitudinal cross section). Titanium implants and fixation screws appear in black, whereas bone appears in dark gray. Arrowheads indicate progression of bony bridging during the follow-up period. Asterisk depicts area of bone resorption. Scale bar indicates 1 mm.
Biomechanical evaluation
Seven femurs grafted with osteostatin-coated implants, eight femurs grafted with uncoated implants, and three intact femurs were successfully embedded in epoxy resin and subjected to torsion testing. The average maximum failure torque with the osteostatin-coated implant was 97±31 N·mm compared with 77±53 N·mm with uncoated implants (Fig. 8C); this was not statistically significant. All femurs failed to form the interface of bone implant except for one, which failed through the implant. Failure torque of femurs with osteostatin-coated implants and uncoated implants reached, respectively, 66% and 53% of that of intact femurs, that is, 146±19 N·mm.
Histological evaluation
Histological evaluation showed no distinct differences in terms of bone morphology or bone–titanium interface between osteostatin-coated and uncoated porous implants at 12 weeks (Fig. 9A, B). Regenerated bone consisted mainly of nonwoven bone, and direct bone–titanium contact was observed at the proximal and distal sites of the implants (Fig. 9C, D). The remaining nonbridged bone gap was mainly filled with fibrous tissue (Fig. 9D, E). Occasionally, there were also areas of the bone–titanium interface found with a cartilage-like or fibrous-like zone in both groups (Fig. 9C, F).

Representative histological transversal sections of bone defects grafted with osteostatin-coated (upper row) and uncoated (bottom row), porous titanium implants. Sections are stained with basic fuchsine and methylene blue. Basic fuchsine stains bone purple and methylene blue stains fibrous tissue blue.
Discussion
An ideal bone graft substitute provides immediate mechanical support and enhances bone regeneration that allows repair of critical-sized bone defects in a short period of time. 1 A promising biomaterial suitable to provide sufficient mechanical support to load-bearing bone defects is porous titanium. 9 In this study, we showed that the performance of porous titanium can be improved with an osteostatin coating since osteostatin-coated implants showed an increase in bone regeneration in vivo (Figs. 6 and 7).
Osteostatin is a pentapeptide domain (107–111) of PTHrP. PTHrP consists of three major domains and acts as an important modulator of bone formation and bone remodeling. 31 The actions of its N-terminal domain (1–36), which shows homology to PTH, are a consequence of the interaction with the PTH/PTHrP receptor 1 (PPR1). However, the native C-terminal domain (107–139), including osteostatin, seems to act through a PPR-unrelated receptor and increases osteoblast survival and osteoblastic differentiation in vitro.23,32,33 In addition, osteostatin was found to enhance bone regeneration in vivo in metaphyseal bone defects in rabbits.25,34 These trophic effects, together with its short peptide sequence (Thr–Arg–Ser–Ala–Trp) warranting its stability, make osteostatin an interesting peptide to use as an organic surface coating aimed to enhance bone regeneration of porous titanium.
The SLM-produced porous titanium underwent a postproduction alkali-acid-heat treatment, 35 resulting in a titanium dioxide layer on the surface and altering the surface topography (Fig. 2), which has been shown to increase bone regeneration.21,36 Subsequently, this titanium surface was coated with osteostatin by a soaking method used previously for loading osteostatin onto ceramics.23,34 Osteostatin adhesion onto the titanium surface is most likely based on van der Waals interactions between the indole ring in the C-terminal tryptophan of osteostatin and titanium dioxide and this resulted in a low dose of osteostatin on the surface (0.02 ng/mm2). These relatively weak van der Waals interactions also explain the fast release of osteostatin (Fig. 1B). This prompt release was similar to the release of osteostatin from ceramics and had been capable to enhance trabecular BVs of metaphyseal bone defects in rabbits.25,34 This fast release might even be a requisite since a constant delivery of PTH results in bone resorption, whereas only intermittent administration of PTH and PTHrP improved bone mass and bone healing.37–41 Intermittent administration induces a transient increase in RankL that could result in more osteoclastic resorption. 42 The release of osteoblastic growth factors from the resorbed bone matrix can be a source of osteogenic signals that contribute to PTH-induced anabolism. RankL may also stimulate the secretion of osteoblastic factors by osteoclasts. 42 Intermittent administration of PTHrP (107–139) also reduced the RankL:OPG ratio in human osteoblastic cells in vitro. 43 These observed differences on bone regeneration between constant and intermittent administration of PTH and PTHrP suggest that altering the pace or dose of osteostatin administration could not only potentially improve but also diminish its trophic effects on bone regeneration, and improving the osteostatin coating on titanium surfaces is therefore an interesting topic. Osteostatin coating on titanium surfaces might be improved using more advanced titanium surface treatments. One treatment that we previously have applied to our porous titanium implants is an anodizing technique that results in the formation of regular and adjustable TiO2 nanotubes. 21 Anodizing is especially interesting since others have shown that the size of these TiO2 nanotubes can be tailored to function as a small drug reservoir 44 and this could be used to improve the osteostatin administration in future research.
Culturing osteoprogenitor cells in vitro on porous titanium scaffolds showed a significant effect of osteostatin on the RankL:OPG gene expression ratio, leading to a reduction of this ratio at day 1 (Fig. 5). As already mentioned, the RankL/OPG system is a major signaling pathway that regulates differentiation and function of osteoclasts. 45 RankL promotes, whereas OPG inhibits, bone resorption 46 and this is consistent with the observed accelerated bone regeneration after 4 weeks in vivo (Fig. 6). These results are in line with previously published in vitro experiments using a mouse osteoblast cell line (MC3T3-E1), showing that RankL expression was significantly reduced by addition of osteostatin to cultures at days 2 and 4. 23 Moreover, in the latter cell line, it was found that osteostatin increased both OPG and VEGF gene expression through Src activation, which presents a mechanism for modulation of osteoblast activity and function. 47 The fact that we did not see a difference in VEGF gene expression or expression of osteogenic genes upon osteostatin treatment of hPDCs—in contrast to previous observations in MC3T3-E1 cells23,47—may be explained by differences in (i) used cell type or (ii) time-dependent effects of osteostatin. MC3T3-E1 cells represent immature osteoblasts, whereas hPDCs are multipotent mesenchymal stem cell-like osteoprogenitors, and in previously conducted experiments, the upregulation of osteogenic genes (e.g., ALP and OCN) was already found to be time dependent. 23
Grafting cortical bone defects with osteostatin-coated, porous titanium implants showed significantly more bone regeneration (Fig. 6). After 4, 8, and 12 weeks, the difference in total BV was, respectively, 8, 9, and 5 mm3 and this suggests that the advantage of osteostatin coating decreased over time. However, the interaction of time and treatment only showed a statistical trend (p=0.09); more power is necessary to support this observation. In addition, no significant differences in bone regeneration or biomechanical strength were found ex vivo. Again, we believe this is mainly caused by the limited power of our study design. Due to variability in the surgical procedure and animal response, this bone defect model has a large SD. The group size was not suitable for detecting statistically significant differences that were smaller than 35%. Thus, the observed differences of defects grafted with osteostatin-coated, porous titanium implants found after 12 weeks (14% more bone regeneration, 13% increase in biomechanical strength) did not pass the significant threshold imposed by the group size used and require the use of a larger sample size. Additionally, we have recently shown that there is a large variation in the degree of implant fixation in our model. 48 This variation, which may allow for excessive micromotion, can explain the observation of a fibrocartilage interface at certain areas of the titanium–bone interface (Fig. 9C, F) and needs to be reduced by improving implant fixation.
Porous titanium implants were shown to enhance bone regeneration through osteoconduction.19,49–52 However, to become suitable for grafting load-bearing defects, they should be strong enough to sustain mechanical loading, but not overly stiff to avoid stress shielding and implant loosening. The mechanical properties of the porous titanium implants used were measured earlier18,52 and are as follows: 14 MPa compression strength, 0.4 GPa Young's modulus, and a fatigue life long enough to allow bone ingrowth and osseointegration. This is sufficient to allow immediate weight bearing in femur defects and restored up to, respectively, 53% (uncoated group) and 66% (osteostatin-coated group) of its original strength (Fig. 9). Restoration of mechanical strength is one of the main goals of bone grafting, but the minimal difference in favor of the osteostatin-coated group found here was not significant. A power calculation made based on these data (α-value=0.05, β-value=0.80) indicates that an n=50 per group would be required to determine if this difference is significant. However, these results were in line with previous experiments20,52 and underline the potential of porous titanium as a load-bearing osteoconductive scaffold. Combining this load-bearing osteoconductive scaffold with an osteostatin coating capable of enhancing early bone regeneration further improves and accelerates the repair of cortical bone defects grafted with porous titanium implants and might lead to the development of new implants suitable as bone graft substitutes or implants in trauma and orthopedic-related or craniomaxillofacial surgery.9,53
Conclusions
In this study, osteostatin was used as an organic surface coating to improve bone regeneration upon implantation of porous titanium. In vivo experiments showed that porous titanium scaffolds coated with osteostatin enhanced early bone regeneration in critical-sized femoral bone defects in rats. In vitro experiments showed that osteostatin results in an early upregulation of OPG gene expression, altering the RankL:OPG ratio, which might be the mechanism of action through which in vivo early bone regeneration is increased. Optimizing the dose and pace of osteostatin release from the titanium surface remains an interesting topic for future in vivo experiments and may show more profound long-term effects of osteostatin on bone regeneration of cortical bone defects grafted with porous titanium implants.
Footnotes
Acknowledgments
This research forms part of the Project P2.04 BONE-IP of the research program of the BioMedical Materials Institute cofunded by the Dutch Ministry of Economic Affairs. D.L. has a postdoctoral contract from Spanish Comunidad Autónoma de Madrid (S2009/MAT-1472). Y.C.C. is a postdoctoral fellow of the Research Foundation-Flanders (FWO: 1.5.172.13N—Interdisc).
Disclosure Statement
FtI BV (Boxmeer) has cosponsored this research through a grant from EFRO (OP-Zuid).