
Abstract
The use of biologic scaffold materials adjacent to synthetic meshes is commonplace. A prevalent clinical example is two-staged breast reconstruction, where biologic scaffolds are used to provide support and coverage for the inferior aspect of the synthetic expander. However, limited data exist regarding either the kinetics of biologic scaffold integration or the host tissue response to the biologic scaffold materials used for this application or other applications in which such scaffold materials are used. The present study evaluated the temporal host response to a biological scaffold when placed adjacent to a synthetic material. Evaluation criteria included quantification of material contracture and characterization of the host cell response and tissue remodeling events. Results show a decreased thickness of the collagenous tissue layer at biologic scaffold/silicone interface compared to the abdominal wall/silicone interface during the 12-week experimental time course. All test materials were readily incorporated into surrounding host tissue.
Introduction
B
Several clinical reports have shown improved aesthetic outcomes and a reduction in postsurgical complications (e.g., contracture) with the use of biologic scaffolds compared to a traditional total muscle coverage technique of expander/implant breast reconstruction. However, little has been reported about the rate of scaffold integration and host response to the biologic materials when placed adjacent to synthetic materials. Such a characterization is relevant for this application and others, including abdominal wall reconstruction 3 and pelvic organ prolapse procedures. 4 These naturally occurring scaffolds are composed of extracellular matrix (ECM). The ECM represents a biopolymer composed of the structural and functional molecules secreted by the resident cells of each tissue or organ, and therefore, the composition of each biologic scaffold varies depending on the source tissue from which they are derived. 5 The ideal biologic scaffold is manufactured in a manner that preserves as much of the native three-dimensional ultrastructure and composition as possible, including various collagen isoforms, glycosaminoglycans, 6 and several growth factors.7,8 When appropriately prepared, studies have shown that biologic scaffolds are degraded within weeks to months by host cells9–12 and the resultant degradation products (i.e., matricryptic peptides) promote angiogenesis,13,14 progenitor cell recruitment,15,16 and modulation of the local immune response.17,18 The clinical safety and efficacy of properly prepared biologic scaffolds are now well established.
The present study describes a rodent model to evaluate the temporal host soft tissue response to three ECM materials when they are placed adjacent to a synthetic silicone material. Evaluation criteria included characterization of the degree of material contracture and quantification of aspects of the host cell response and tissue remodeling events using histomorphologic metrics.
Methods
Overview of experimental design
A rodent abdominal wall model, in which various ECM materials were placed adjacent to a silicone sheet, was used to evaluate the temporal host soft tissue response. Dermal scaffolds derived from porcine and cadaveric tissue were evaluated, in addition to different thicknesses of porcine dermal ECM, to encompass the diversity of products that are available for clinical use. Following 4, 8, and 12 weeks, the host response to each scaffold material was determined by quantitative evaluation of material contracture, histologic criteria, and immunolabeling for selected cell types within explanted specimens.
Material preparation
Two of the test articles consisted of porcine dermal ECM scaffolds with a thickness of 0.5 mm (pD-ECM-0.5) and 1.0 mm (pD-ECM-1.0) and were prepared as previously described. 19 Briefly, full-thickness skin sheets were cut into 35 × 50 cm rectangle. The skin was harvested from 6-month-old Yorkshire crossbreed pigs and subsequently delaminated to remove subcutaneous fat, connective tissue, and the epidermis. The harvested sheets of porcine dermis were frozen at −80°C and then thawed and treated with 0.25% trypsin/0.1% sodium dodecyl sulfate/1% Triton X-100 on a vortex shaker (Thermo Scientific MaxQ3000; Thermo Fisher Scientific) at 300 rpm at room temperature. The following solutions were used to complete the decellularization protocol: 0.25% trypsin, 6 h, 1×; deionized water, 15 min, 3×; 70% ethanol, 10–12 h, 1×; 3% H2O2, 15 min, 1×; deionized water, 15 min, 2×; 1% Triton X-100 in 0.26% ethylenediaminetetraacetic acid (EDTA)/0.69% Tris, 6 h, 1×; 1% Triton X-100 in 0.26% EDTA/0.69% Tris, 10–12 h, 1×; deionized water, 15 min, 3×; 0.1% peracetic acid/4% ethanol, 2 h, 1×; phosphate-buffered saline (PBS), 15 min, 2×; and finally deionized water, 15 min, 2×. The pD-ECM sheets were sterilized by ethylene oxide (16 h cycle at 50°C in a Series 3plus EOGas Sterilizer; Anderson Sterilizers, Inc.) before implantation.
The third test article consisted of human dermal ECM (hD-ECM; [AlloMax™]), which was provided by the manufacturer (C.R. Bard [Davol], Inc.), and was handled according to its instructions for use. All test materials and silicone coupons (Siltex® Contour Profile® High Breast Implant; Mentor) were die cut to the specified implant dimensions on-site with sterilized instruments before implantation.
Animals
Forty-five (n = 5/group/time point) female Sprague Dawley rats (350–400 g at implantation) were purchased from Harlan Laboratories. Rats were housed on a 12-h light–12-h dark cycle and fed standard laboratory chow and water ad libitum. All animal procedures were approved by The University of Pittsburgh Institutional Animal Care and Use Committee.
Surgical procedure
Animals were anesthetized with 2.5–4% isoflurane inhalant anesthetic and maintained at surgical plane anesthesia with 0.5–4% isoflurane throughout the procedure. The ventral abdomen was prepared for aseptic survival surgery by clipping the fur over the entire abdominal region and cleaning the operative area with three alternating scrubs of providone-iodine surgical scrub and 70% isopropyl alcohol solutions. A final preparation of 70% isopropyl alcohol was applied and allowed to dry, followed by an application of DuraPrep™, which was allowed to dry before applying and placing sterile surgical drape(s) over the entire field.
Following preparation of the ventral abdomen, an ∼5 cm midline skin incision was made, and the skin and subcutaneous tissue were bluntly dissected from the abdominal musculature (Fig. 1A). One 2 × 2 cm sterile silicone membrane was soaked for 1 min in sterile saline and then fixated to the muscle with four interrupted 4-0 PROLENE™ sutures (one at each corner) (Fig. 1B). Each silicone membrane has a rough side and a smooth side; the smooth side was placed against the abdominal muscle (muscularis externa). Following placement of the silicone membrane, a 2.5 × 2.5 cm test article was then fixated directly on top of the rough surface of the silicone membrane using eight 4-0 PROLENE interrupted sutures (bite depth of 1.0–2.0 mm) placed at the corners and at the midpoint of each edge (Fig. 1C). Following placement of the test article, the skin was closed with a continuous (inner) 4-0 VICRYL™ suture (Fig. 1D). Upon completion of the surgical procedure, the inhalant anesthetic gases were discontinued, and the animal was recovered from anesthesia. The animal was allowed access to food and water ad libitum.

Surgical procedure.
Daily monitoring
Daily observations of each animal were made. The abdominal region of each animal was examined to assess both the condition of the wound line and subcutaneous tissues (e.g., dehiscence, seromas, and/or hematomas). Additional skin sutures were applied as necessary, if missing. The skin sutures were removed within 7–10 days postoperatively.
Euthanasia and specimen collection
Euthanasia was achieved by CO2 inhalation and subsequent cervical dislocation, which was performed in accordance with the American Veterinary Medical Association Guidelines on Euthanasia. Following euthanasia, the skin was gently dissected, reflected, and photographs were taken of each test article in situ for offline mesh contracture morphometric analysis. After completion of the initial examination, the entire body wall that included the test article and the silicone membrane was explanted en bloc. The sample was then cut in half and each half immersed in 10% neutral-buffered formalin for histologic analysis.
Contracture analysis
Each test article was photographed in situ at the time of euthanasia (4, 8, or 12 weeks postimplantation). Contracture analysis was performed with ImageJ software using a scale reference. The percent contracture was calculated according to the following formula: (Implant Area − Explant Area/Implant Area × 100 = % Area Contracture), where the implant area was constant (6.25 cm2).
Histomorphologic evaluation
The explanted tissues were processed, paraffin embedded, and then 5 μm transverse sections were then cut through the entire explant and stained with Masson's trichrome. Representative images were generated with a Nikon Eclipse E600 microscope (Nikon) and a Nuance Multispectral Imaging System (CRi). Sixteen high-powered representative fields (400 × magnification) were imaged across three distinct regions (i.e., within ECM device, ECM/silicone interface, abdominal wall/silicone interface) of each tissue transverse section (Fig. 2). Photomicrographs were evaluated semiquantitatively by five blinded investigators based upon established metrics using detailed instructions20,21 (Table 1).
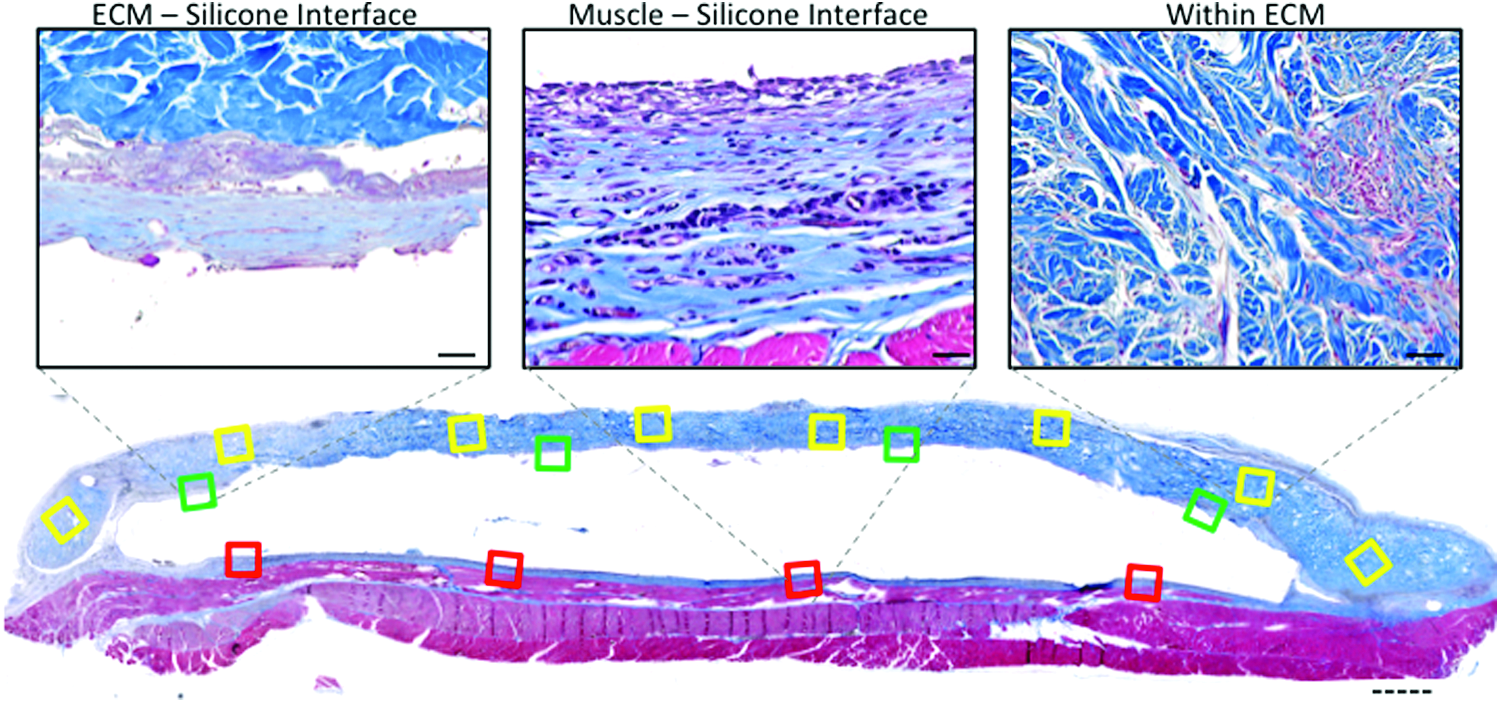
Histomorphologic evaluation scheme. Transverse sections were stained with Masson's trichrome, and 16 representative fields were imaged across three distinct regions of each tissue transverse section: within extracellular matrix (ECM) device (yellow boxes); ECM/silicone interface (green boxes); abdominal wall/silicone interface (red boxes). Solid line scale bar = 50 μm. Dotted line scale bar = 1000 μm. Color images available online at www.liebertpub.com/tea
FoV, field of view. Based on 20 × magnification.
Connective tissue layer thickness
Thickness of the interface tissue layer (i.e., the connective tissue layer at the biologic/silicone interface and the abdominal wall/silicone interface) was manually measured and quantified using AxioVision 4.8 software by a single-blinded individual to assure consistency of identification of this layer (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/tea).
Immunolabeling
Tissue sections from each test article at each time point were stained for CD31 and CD68 as markers for neovascularization and macrophages, respectively. Paraffin-embedded sections were deparaffinized with xylene and rehydrated through a graded ethanol series. Heat-mediated antigen retrieval was performed with a 0.01
Statistics
Data sets were analyzed with either a one-way or a two-way analysis of variance using SigmaStat 12.2 (Systat Software, Inc.). The Student–Newman–Keuls post hoc test was used to locate the differences between means when the observed F ratio was statistically significant (p < 0.05). Data are reported as mean ± standard error.
Results
Contracture analysis
The degree of contracture observed in hD-ECM and pD-ECM-1.0 groups was equivalent across study time points (Fig. 3). The pD-ECM-0.5 material was found to have an increased amount of contraction at 8 and 12 weeks postoperatively (∼23% and 30%, respectively) compared to both hD-ECM and pD-ECM-1.0 (p < 0.05).
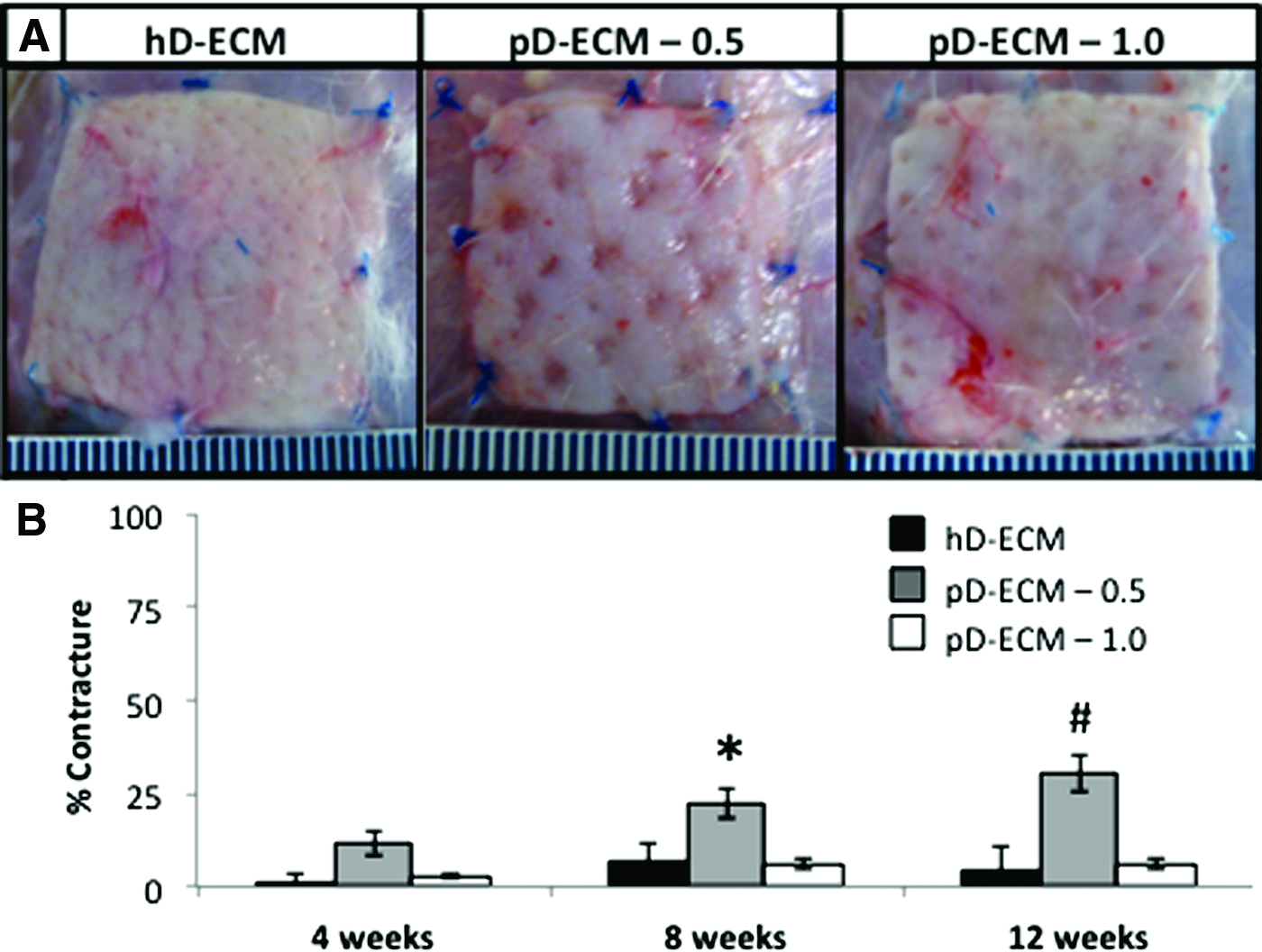
Material contracture analysis. Each test article was photographed in situ at the time of euthanasia (4, 8, or 12 weeks postimplantation) for subsequent analysis of contracture.
Morphologic analysis
Upon gross examination, all test articles showed incorporation into the adjacent tissue and showed neovascularization (Fig. 4). Histologically, the host tissue response to the implanted test articles was characterized by a cellular accumulation at the periphery of the material at 4 weeks, followed by an inward progression of cell infiltration into the center of the device over time (Fig. 4).
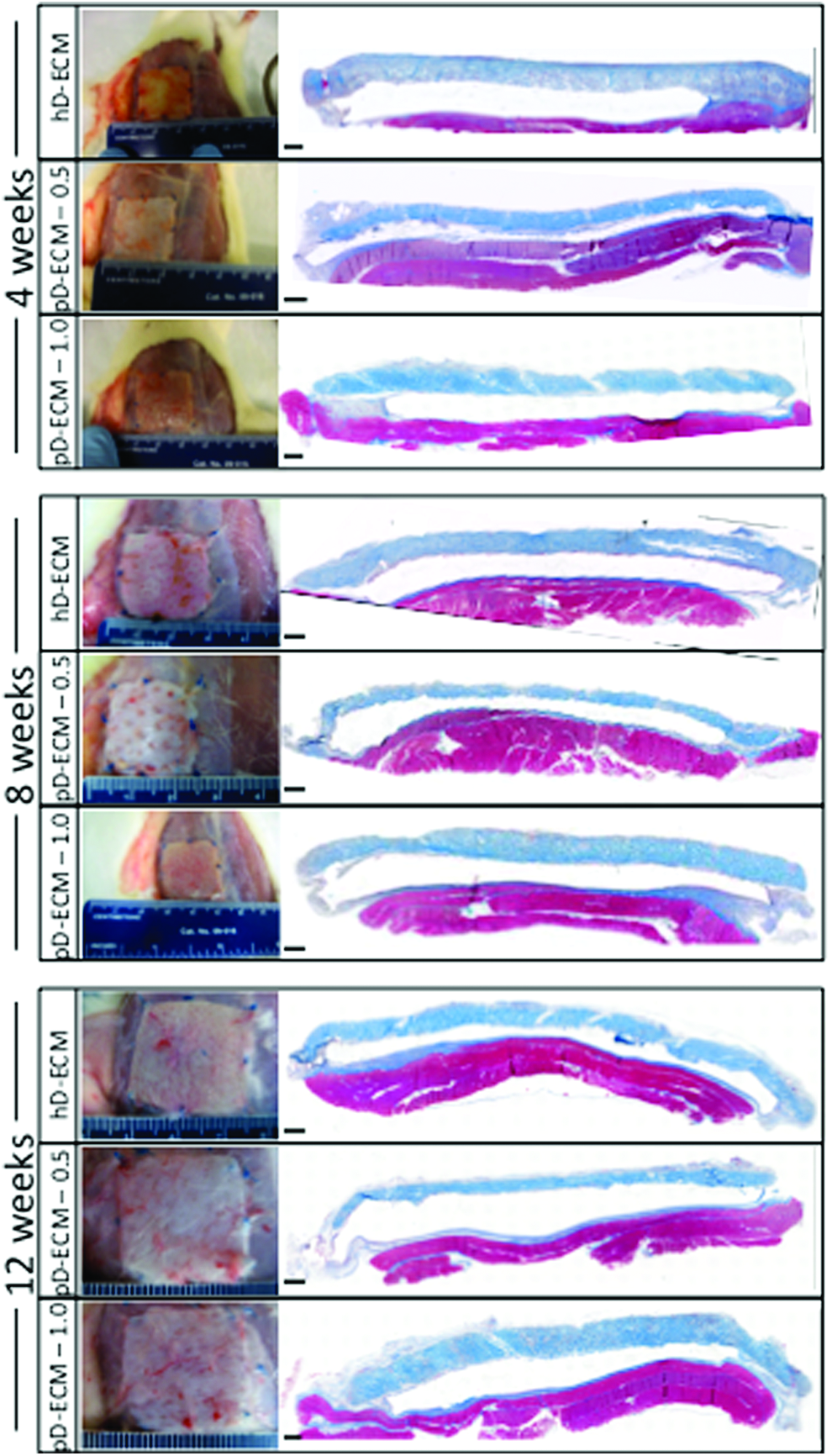
Representative macroscopic and Masson's Trichrome stained cross-sectional mosaic images for each material at each time point. Scale bar = 1000 μm. Color images available online at www.liebertpub.com/tea
Representative images at 4 weeks postoperative show the presence of a connective tissue layer at both the biologic/silicone interface and at the muscle/silicone interface (Fig. 5A). The thickness of this connective tissue was less (p < 0.001) at the biologic device/silicone interface compared to the abdominal wall/silicone interface across time for all samples (Fig. 5B). The thickness in hD-ECM samples was less (p < 0.001) at 4 weeks (40.01 ± 3.00 μm) compared to 8 and 12 weeks (107.87 ± 6.00 μm and 92.32 ± 4.54 μm, respectively). There was no difference in the thickness of the connective tissue layer at the abdominal wall/silicone interface as a function of time.

Connective tissue layer evaluation.
The degree of cellularity and number of multinucleate giant cells at each interface was evaluated using a histomorphologic scoring system20,21 (Figs. 5 and 6). A differential biologic response to porcine versus human-derived scaffolds was present at the biologic/silicone interface (Fig. 5). Cellularity was greater (p < 0.001) at the hD-ECM/silicone interface at 8 weeks (2.60 ± 0.20) and 12 weeks (2.23 ± 0.15) compared to 4 weeks (1.11 ± 0.32). In contrast, both of the porcine-derived scaffolds had more (p < 0.001) cellularity at 4 weeks compared to 8 and 12 weeks (Fig. 5C). Similarly, hD-ECM scaffolds were associated with the highest score (p < 0.001) for multinucleate giant cells at 8 weeks, whereas the pD-ECM scaffolds were associated with higher scores (p < 0.001) earlier that decreased over time (Fig. 5D). Histologic scoring within the biologic test articles showed that the hD-ECM material had a higher cellularity score (3.09 ± 0.09) at 4 weeks compared to 8 and 12 weeks (1.758 ± 0.09 and 2.413 ± 0.12, respectively) (p < 0.001) (Fig. 6B). In contrast, both pD-ECM-0.5 and pD-ECM-1.0 had more cellularity at 8 weeks (p < 0.001) compared to 4 and 12 weeks (Fig. 6B). Multinucleate giant cell scores for hD-ECM was greatest (p < 0.001) at 4 weeks (3.09 ± 0.09) compared to 12 weeks (2.41 ± 0.12), which was greater (p < 0.001) than 8 weeks (1.76 ± 0.09). Multinucleate giant cell scores for pD-ECM-0.5 (0.06 ± 0.02) and pD-ECM-1.0 (0.29 ± 0.07) were lowest (p < 0.001) at 12 weeks compared to 4 and 8 weeks.

Histomorphologic analysis.
Neovascularization
Neovessel formation was identified by CD31+ staining throughout each of the test articles across all study time points (Fig. 7). Representative images at 12 weeks postoperative show the presence of CD31+ vessels in the center of the matrix material (Fig. 7A) and at the biologic/silicone interface (Fig. 7C). The number of CD31+ vessels within the ECM scaffolds trended to increase with time for the hD-ECM and pD-ECM-1.0, while the pD-ECM-0.5 remained relatively constant across time points (Fig. 7B). The number of vessels at the biologic/silicone interface remained unchanged across time points for hD-ECM and pD-ECM-0.5, while there was a trending increase for the pD-ECM-1.0 that did not reach significance. The pD-ECM-1.0 had the highest number of vessels both within and at the silicone interface on average compared to hD-ECM and pD-ECM-0.5. The number of CD31+ vessels at the muscle/silicone interface remained unchanged across time points.

Neovascularization. Representative immunolabeling images and quantification for each material, location, and time point. Within ECM location
Macrophage quantification
Macrophages, identified by CD68+ staining, were present at each biologic/silicone interface and at the muscle/silicone interface (Fig. 8A). The number of macrophages at the silicone interface of muscle, pD-ECM-0.5 and hD-ECM remained relatively constant across all time points. The number of macrophages at the silicone interface in the pD-ECM-1.0 group was higher (p < 0.05) at 12 weeks (207.73 ± 17.40) compared to 4 (179.72 ± 18.55) and 8 weeks (167.52 ± 21.72) postoperatively.

Macrophage accumulation.
Discussion
The present study describes a method for preclinical evaluation of the temporal host tissue response to three biologic scaffold materials when placed adjacent to a synthetic silicone material. The host response was characterized using established quantitative metrics at various host tissue–implant interfaces. All test materials were associated with robust cell infiltration, neovascularization, and a decreased thickness of collagenous tissue at the biologic device/silicone interface compared to the abdominal wall/silicone interface across time.
Biologic scaffolds have been used for soft tissue reconstruction in multiple body systems.22–24 These ECM-based scaffolds are routinely used for pelvic, abdominal, and chest wall reconstruction. Biologic scaffolds derived from dermal tissue have been widely used for expander/implant breast reconstruction. The use of such scaffolds eliminates the need for autologous tissue transfer and associated donor-site morbidity. Additional benefits of using biologic scaffolds include increased support and coverage for the inferior pole of the breast, a decreased volume expansion time for two-staged procedures, and improved aesthetic outcomes. The use of biologic scaffolds, however, is not without complications, and the ideal scaffold for expander/implant reconstruction remains to be determined. A number of studies have reported increased risk of infection 25 and increased seroma formation25,26 with the use of dermis-derived biologic materials compared to without their use. These dermal-derived scaffolds are routinely used in potentially contaminated fields (e.g., for abdominal wall reconstruction), but relatively little has been reported regarding the host tissue response to such biologic scaffolds when placed adjacent to synthetic constructs.
Capsular contracture is a common and serious complication with plastic and reconstructive procedures of the breast. The incidence of clinically significant implant contracture ranges from 2% to 51% in patients who have not been exposed to radiation.27–29 In the setting of irradiation, this incidence rises to as high as 100%. 30 Several large animal models have been developed to investigate mechanisms of capsular contracture.31,32 Clinical and preclinical studies have suggested a role for implant texture,33,34 bacterial colonization at the surgical site,35,36 and various inflammatory cytokines37–39 on contracture formation. However, the definitive etiology of capsule contracture remains unknown. The present study provides a useful screening method to assess whether different biologic scaffold materials influence the extent of capsule formation around a silicone material, thereby impacting the likelihood of contraction. The cause of the greater contracture observed in the pD-ECM-0.5 group is unknown, but since the source tissue and processing methods were identical to those used for the pD-ECM-1.0 devices, it can be surmised that the thickness and associated rate of cell infiltration and scaffold degradation are relevant factors.
Commercially available scaffolds vary in source tissue and, more importantly, processing methods. Varying methods for preparing biologic scaffolds are known to effect material properties and, in turn, host tissue remodeling outcomes. Use and choice of terminal sterilization methodology will also alter ECM structure. It should be noted that many human cadaveric-derived biologic scaffolds (e.g., AlloDerm) are not subject to terminal sterilization. The temporal host tissue response for materials to be used in reconstructive procedures can provide useful information. The presence and rate of vascularization and tissue integration are important considerations for timing and expansion of staged procedures.
The present study describes a high-throughput screening tool for development and testing of biologic scaffolds to be used adjacent to silicone or other synthetic material devices. As with all preclinical studies, it is important to recognize that there are limitations to the use of rodent models to predict clinical response. The rodent model has also been used in many studies designed to evaluate the host response to biologic scaffold materials11,17,24,40–49 and has proven to be an acceptable predictor of the human response. In addition, such models are required by regulatory agencies for numerous biocompatibility tests.
In conclusion, the present study showed neovascularization and incorporation of all dermal ECM test articles into the adjacent tissue. Contracture analysis showed a differential response across groups with contraction being the greatest in the thin (0.5 mm) porcine-derived dermal scaffold. The host tissue response to the implanted test articles was characterized by a cellular accumulation at the periphery of the material at 4 weeks with subsequent progressive cell infiltration toward the center of the device and a uniform pattern of neovascularization. The collagenous tissue layer at the biologic scaffold/silicone interface was decreased compared to the abdominal wall/silicone interface throughout the 12-week experimental time course. This preclinical model has the potential to yield useful information for clinical implications in which a biologic scaffold material is used in combination with a synthetic material.
Footnotes
Acknowledgments
The authors acknowledge Ms. Lisa Carey, Dr. Peter Crapo, Dr. Alexander Huber, Mr. Ricardo Londono, Ms. Janet Reing, and Dr. Matthew Wolf for their assistance with data analysis; Deanna Rhoads of the McGowan Histology Center for histologic section preparation; and Randy McKinsey for the illustration of ![]() . This material is based upon work supported, in part, by the National Science Foundation Graduate Research Fellowship under Grant No. DGE-1247842 (to T.J.K.). Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors(s) and do not necessarily reflect the views of the National Science Foundation. This work was supported, in part, by C.R. Bard, Inc. U.S. Government Disclosure: C.L.D. is an employee of the U.S. Government. This work was prepared as part of his official duties. The opinions or assertions contained in this article are the private views of the authors and are not to be construed as reflecting the views, policies, or positions of the Department of the Army, Department of Defense, nor the U.S. Government.
. This material is based upon work supported, in part, by the National Science Foundation Graduate Research Fellowship under Grant No. DGE-1247842 (to T.J.K.). Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors(s) and do not necessarily reflect the views of the National Science Foundation. This work was supported, in part, by C.R. Bard, Inc. U.S. Government Disclosure: C.L.D. is an employee of the U.S. Government. This work was prepared as part of his official duties. The opinions or assertions contained in this article are the private views of the authors and are not to be construed as reflecting the views, policies, or positions of the Department of the Army, Department of Defense, nor the U.S. Government.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.