
Abstract
This study used the segmental long-bone defect model to assess the effects of osteoporosis on the formation of new bones and the osteoinductivity of recombinant human bone morphogenetic protein-2 (rhBMP-2). Seventy-two female Sprague-Dawley rats were divided into two groups: an osteoporosis group with ovariectomies and dexamathasone intramuscular injections and a sham group. When they reached 22 weeks in age, each group was further divided into two groups and a 5-mm defect was made in both fibular mid-shafts of each rat. One fibula in each rat was picked randomly and was injected with 0.05 mL of hydrogel carrier; the opposite fibula was injected with the same carrier mixed with rhBMP-2 (10 μg). After rearing for a further 5 and 9 weeks, the ratios of the lengths of the newly formed bones in the fibular defects were determined using micro-CT and undecalcified histology. The sham rhBMP-2-injected group—in all of the 5- and 9-week-kept groups—showed a significantly higher bridging bone formation ratio than the other three groups. The osteoporosis rhBMP-2-injected group showed a significantly higher ratio than both the non-rhBMP-2-injected sham hydrogel and the osteoporosis hydrogel groups. The comparison of the micro-CT parameters of the newly formed bones showed that the sham rhBMP-2 group at both 5 and 9 weeks compared with the osteoporosis rhBMP-2 group had significantly higher percentage bone volumes, trabecular thicknesses, and trabecular numbers, in addition to significantly lower specific surfaces, trabecular pattern factors, and structural model indices. The histology results showed that the sham-rhBMP-2 group began forming bridging bones in the defect areas at 5 weeks, and at 9 weeks, trabeculae and marrow spaces were observed. However, the osteoporosis rhBMP-2 group exhibited a relatively minor level of new bone and trabecula formation. Consequently, the rhBMP-2 group showed significantly increased bone formation in the osteoporosis rat fibular defect model compared with the hydrogel group, whereas the new bone quantities, qualities, and remodeling in the osteoporosis rhBMP-2 group were less effective than those in the sham-rhBMP-2 group, signaling that ovariectomy and corticosteroid-induced osteoporosis significantly undermines rhBMP-2 osteoinductivity.
Introduction
O
Some studies have found that the local delivery of osteoinductive biologics, such as recombinant human bone morphogenetic protein-2 (rhBMP-2) or platelet-rich plasma, enhanced bone formation.11,12 As rhBMP-2 is capable of complete bone regeneration even in difficult cases such as long-bone defect and pseudarthrosis, it is one of the most important growth factors and is widely used in the clinical field.13–16 As rhBMP-2 is water soluble, it needs a carrier. Diverse carriers are currently being used clinically; among them, collagen is often applied in the initial stage 13 followed by the inclusion of ceramics such as hydroxyapatite or tricalcium phosphate.17–19 In carriers that mainly comprise ceramics, the osteoconductivity of the ceramics themselves is high enough to assist rhBMP-2-mediated new bone formation while also presenting mechanical strength. However, it is hard to measure the new bone formation ability of rhBMP-2 itself, and the injection cannot be performed in a desired shape. Moreover, due to the radio-opacity of ceramics, newly formed bones and ceramics are barely distinguishable in radiographic evaluations. 20 In comparison, a hyaluronic acid (HA)-based carrier is injectable 21 and it is radiolucent, enabling an easier evaluation of newly formed bones.
Depending on the anatomical location and host tissue environment, rhBMP-2 shows different levels of new bone formation. The fewer MSCs in the environment, the lower the new bone formation, the smaller the contacting host bone surface, and the poorer the union that is built. Therefore, among the clinical locations that require new bone formation, long-bone mid-shafts containing cortical bone have, for the most part, fewer MSCs and narrower host bone surfaces than most of the other locations. Two representative examples are the fibular mid-shaft and the ulnar mid-shaft.
Some studies have shown that rhBMP-2 increases the fusion rate or bone healing in osteoporosis animal models.22–24 In addition, in ovariectomy sheep models, rhBMP-7 was delivered by inserting a poly-lactic glycolic acid microsphere to improve the vertebral body strength. 25 However, such studies showed only that rhBMP-2 and rhBMP-7 triggered new bone formations in osteoporosis models. No study has compared the rhBMP efficacies of healthy bones and osteoporotic bones to evaluate how osteoporosis affects rhBMP osteoinduction.
Therefore, to generate the most difficult environment possible for rhBMP-2 osteoinductivity, this research added a steroid injection to an ovariectomy to trigger severe osteoporosis and then created the critical segmental defect model in the fibular mid-shaft to determine whether rhBMP-2 osteoinductivity is maintained and how much osteoporosis inhibits rhBMP-2 osteoinduction.
Material and Methods
Fabrication of the injectable HA-based powder gel composite rhBMP-2 carrier
The rhBMP-2 carrier used in this research was prepared by mixing porous β-tricalcium phosphate (β-TCP) microspheres with a HA powder gel at a ratio of 1:9. The rhBMP-2 was designed to first load in the HA powder-gel. Porous β-TCP (Cerectron Co., Kimpo, South Korea) microspheres were made using a spray-dry method and the microspheres underwent sintering at 1250°C for 2 h to reach a diameter range of 45–75 μm. 21
The HA powder gel was synthesized through the cross-linking process using HA (MW: 3 million Daltons; Bioland Co., Ochang, South Korea) and the cross-linking agent butanediol diglycidyl ether (Sigma-Aldrich, St. Louis, MO). 21
The composed HA powder gel was lyophilized for 4 days and pulverized until the particle diameter reached 500 μm or under.
The HA-based powder gel composite was put in syringes and sterilized with gamma rays. The complex and rhBMP-2 solution mixing ratio was 1:1 in terms of weight, and the rhBMP-2 concentration was 1 mg/mL.
In vivo study
This research was performed by the Preclinical Testing Laboratory of the Seoul National University Hospital Biomedical Research Institute with approval for animal testing from the Seoul National University Institutional Animal Care and Use Committee (IACUC No. 11-0216). Seventy-two 6-week-old female Sprague-Dawley rats (120–145 g) underwent a 1-week stabilization period. Then, the rats were randomly divided into two groups; the osteoporosis group and the sham group. Solid compress feed and tap water were fed to the rats, and the rearing conditions were identical in the two groups. The 36 rats in the osteoporosis group were intraperitoneally anesthetized with 0.35 mL of diluted Zoletil 20 mg/kg and 0.05 mL of Rompun 2 mg/kg. Their lateral-dorsal area fur on both sides was removed. The area of operation was sterilized with a 10% betadine solution for aseptic manipulation. In the lower part of one lateral-dorsal area, a skin incision of about 1.5 cm was made, followed by muscular and peritoneal incisions that gave access to the abdominal cavity. After exposing the ovary, silk tie was done at the medial side of the ovary with an additional vicryl tie in between the ovary and the silk tie. Ovariectomy by electrocauterization was done in between the two ties. The wound was sutured from the peritoneum to the muscle and to the skin, in that order. The opposite-side ovary was excised in the same manner. After the operation, 0.3 mL of meloxicam was muscularly injected and 0.5 mL of cefazolin, an antibiotic, was intraperitoneally injected. After the ovariectomy, the rats were looked after for 7 weeks; 0.125 mg/kg of solution prepared by diluting 0.1 mL of dexamethasone with 0.5 mL of saline was injected into their thigh muscles twice a week for 5 weeks for a total of 10 rounds of injections. The 36 rats in the sham operation group were identically anesthetized and received skin, muscle, and peritoneum incisions only; they did not receive a dexamethasone injection.
Of the 72, 24 of the osteoporosis group rats and 24 of the sham group rats were intraperitoneally anesthetized with 0.35 cc of diluted Zoletil 20 mg/kg and 0.05 cc of Rompun 2 mg/kg in their 22nd week. In addition, their lower thigh and lower limb was shaved, and for adequate surgical site preparation the assistant fixed the lower limb in a knee flexed position with the fibular lateral aspect facing upward. The area of operation was sterilized with the 10% betadine solution for aseptic manipulation, and a longitudinal skin incision was performed in the lateral side of one lower leg, in addition to fascia, muscle dissection, and periosteum exfoliation in the fibula mid-shaft area. A 5-mm-long defect was created with a saw in the fibular mid-shaft then irrigated with normal saline (Fig. 1A); on the opposite side, an identical 5-mm-long fibular defect was created. On a randomly chosen side, 0.05 mL of an HA-based powder gel composite (HA carrier) was injected, while on the opposite side, a mixture of the HA carrier and rhBMP-2 10 μg was injected (Fig. 1B–1D). After the fascia and skin suture, 0.3 mL of meloxicam was muscularly injected and 0.5 mL of cefazolin was intraperitoneally injected.

Surgical procedures.
From each of the osteoporosis and sham groups, six rats were placed into either a 5-week keeping group or 9-week keeping group and kept for the set period then sacrificed. The experimental groups are described as follows.
(1) Five-week keeping group: sham HA carrier group (SH-5w group), osteoporosis HA carrier group (OH-5w group), sham rhBMP-2 10 μg+HA carrier group (SB-5w group), osteoporosis rhBMP-2 10 μg+HA carrier group (OB-5w group).
(2) Nine-week keeping group: sham HA carrier group (SH-9w group), osteoporosis HA carrier group (OH-9w group), sham rhBMP-2 10 μg+HA carrier group (SB-9w group), osteoporosis rhBMP-2 10 μg+HA carrier group (OB-9w group).
Evaluation
Bone mineral density
Micro-CT (SkyScan 1173, Kontich, Belgium) was used to assess the bone mineral density (BMD) of the lumbar spines and proximal femurs collected at 5 and 9 weeks. The results were used to analyze the vertebral bodies and femoral heads, femoral necks, proximal femurs, and total hips and to compare the osteoporosis group and the sham group.
Micro CT evaluation
After harvesting specimens including the tibia, a micro-CT (SkyScan 1173) 12 μm image was taken of all of the specimens under the conditions of 130 kV and 30 μA. For the fibula defect examination, 30 images were used; a micro-CT image processing software (CT Analyser V1.11.4.2; Skyscan 1173) was used for all of the analyses. In the fibula defect area, a newly formed bone material analysis was performed by setting the region of interest to a 4.25 mm width and a 3.65 mm length in a sagittal plane.
The ratio of the length of the newly formed bone in the fibular defect was assessed. If bone bridging was formed between the upper and lower edge of the defect, such a case was regarded as complete healing. If a newly formed bone was 50% or greater of the defect length, but without complete bone bridging, the case was regarded as grade II healing. If a newly formed bone was less than 50% of the defect, such a case was regarded as grade I healing. When no newly formed bone was observed, the case was regarded as no healing (none). In addition, the percentage bone volume, trabecular number, trabecular thickness, trabecular separation, trabecular pattern factor, specific surface, and degree of anisotropy were examined.
Histology and histomorphometric analysis
The specimens were organized to include the full fibula length and fixated in formalin for 5 days. Gross sectioned tissues were put in a cassette for 6 h of water-washing then dehydrated in 100% alcohol. The tissues were stirred in methacrylate-based chemical curing resin for 2 days. Then, the tissues underwent stirring and embedding in dissolved benzoyl peroxide and the blocks were trimmed. Using EXAKT (Norderstedt, Germany; BS-3000N), the blocks were cut along the fibula's longitudinal axis. In addition, a 4-μm thick section was made along the sagittal plane to include the top and bottom parts of the fibula. With an EXAKT grinding machine (4110), the sections were ground and attached to an acrylic slide. Hematoxylin and eosin staining was performed and the newly formed bone in the defect was observed using light microscopy.
Quantitative assessment for the ratio of newly bone formed bone length was done by histomorphometric analysis, calculating the ratio of the longitudinal length of the gap between proximal and distal part of the remnant bone at the fibular segmental defect to the length of the newly formed bone.
Statistical analysis
As the four groups showed a normal distribution, a one-way analysis of variance (ANOVA) was performed, and the Bonferroni test for a post hoc analysis. In the case of non-normal distribution, the Kruskal–Wallis test was used. The p-values<0.05 were considered significant.
Results
Among 36 rats that underwent ovariectomy, eight rats were lost after the procedure or during the breeding period, there were no loss in the sham operation group. There was also no loss until breeding finished among the 48 rats of the fibular defect model.
Bone mineral density
According to the micro-CT analysis, the BMD in the lumbar spine in the osteoporosis group had significantly lower level than that of the sham group (p<0.0001) (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/tea). The femurs in the osteoporosis group showed significantly lower BMD level in the femoral heads, femoral necks, proximal femurs, and total hips than those in the sham group (p=0.0001, 0.0001, <0.0001, and 0.042, in each area) (Supplementary Table S2).
Radiographic results
Bridging bone formation ratio
The micro-CT results showed that the ratio of the newly formed bone length to the fibular defect length at both 5 and 9 weeks was significantly higher in the sham rhBMP-2 10 μg+HA carrier group (SB-5w group) than in the remaining three groups (Tables 1 and 2). The osteoporosis rhBMP-2 10 μg+HA carrier group (OB-5w group) showed a significantly higher ratio than the carrier-injected SH-5w and OH-5w groups (Table 1 and Figs. 2, 3).

Micro-CT results for the 5-week groups.

Micro-CT results for the 9-week groups.
The SB-5w group showed a significantly higher ratio than the other three groups. The OB-5w group presented a significantly higher ratio than the SH-5w and OH-5w groups. The Student-Newman-Keuls test was used for all of the pairwise comparisons.
Sham HA carrier group 5 weeks group.
Osteoporosis HA carrier group 5 weeks group.
Sham rhBMP-2 10 mg+HA carrier group 5 weeks group.
Osteoporosis rhBMP-2 10 mg+HA carrier 5 weeks group.
The SB-9w group showed a significantly higher ratio than the other three groups. The OB-9w group presented a significantly higher ratio than the SH-9w and OH-9w groups. The Student-Newman-Keuls test was used for all of the pairwise comparisons.
Sham HA carrier group 9 weeks group.
Osteoporosis HA carrier group 9 weeks group.
Sham rhBMP-2 10 mg+HA carrier group 9 weeks group.
Osteoporosis rhBMP-2 10 mg+HA carrier 9 weeks group.
The complete healing ratio, that is, cases where a bridging bone was fully formed in the fibular defect area in the sham rhBMP-2 10 μg+HA carrier group (SB-5w and SB-9w), was 91.7% at both 5 and 9 weeks. The grade II healing ratio, referring to a bridging bone formation of 50% or greater of the fibular defect, was 8.3% in both the 5- and 9-week groups (SB-5w and SB-9w) (Table 3). However, the osteoporosis rhBMP-2 10 μg+HA carrier group had 55.6% and 72.7% of grade II healing ratios at 5 and 9 weeks, respectively, the grade I healing ratios were 33.3% and 18.2% and the nonhealing ratios were 11.1% and 9.1%, respectively (Table 3 and Figs. 2, 3).
The SB-5w and SB-9w groups were found to have complete healing of 91.7%, and the healing level at grade II or over was 100%. However, the OB-5w and OB-9w groups did not show complete healing at all, with grade II healing being 55.6% and 72.7%, respectively.
Quantity and quality of newly formed bone
In the 5-week kept group, the bone quality of the fibular defect center showed statistically significant differences in all of the parameters (p<0.0001) (Table 4). According to the Bonferroni-based post hoc analysis, the sham rhBMP-2 10 μg+HA carrier group (SB-5w group) had a significantly higher percentage bone volume, trabecular thickness, and trabecular number than the non-rhBMP-2-injected SH-5w and OH-5w groups. In addition, the SB-5w group's specific surface, trabecular pattern factor, and structural model index were significantly lower than in the SH-5w and OH-5w groups. The OB-5w group also showed a significantly higher percentage bone volume and trabecular number than the SH-5w and OH-5w groups, while presenting significantly less trabecular separation.
All of the parameters showed statistically significant differences (p<0.0001). Percent volume (BV/TV): Group SB-5w>Group SH-5w, OH-5w, p-values are both<0.0001; Group OB-5w>Group SH-5w, OH-5w, p-values are both <0.0001.
Specific surface (BS/BV): Group SB-5w<Group SH-5w, OH-5w, OB-5w, p-values are 0.01, <0.0001, 0.003, repectively.
Trabecular pattern factor (Tb.Pf): Group SB-5w<Group SH-5w, OH-5w, p-values are both<0.0001; Group OB-5w<Group SH-5w, OH-5w, p-values are 0.003 and 0.014, respectively.
Structure model index (SMI): Group SB-5w<Group SH-5w, OH-5w, OB-5w, p-values are all<0.0001; Group OB-5w<Group SH-5w, p=0.006.
Trabecular thickness (Tb.Th): Group SB-5w>Group SH-5w, OH-5w, OB-5w, p-values are 0.003, <0.0001, <0.0001, repectively.
Trabecular number (Tb.N): Group SB-5w>Group SH-5w, OH-5w, p-values are both<0.0001; Group OB-5w>Group SH-5w, OH-5w, p-values are both<0.0001.
Trabecular separation (Tb.Sp): Group SB-5w<Group SH-5w, p<0.0001; Group OB-5w<Group SH-5w, HB-5w, p-values are both<0.0001.
Degree of anisotropy (DA): Group SB-5w<Group OH-5w, OB-5w, p-values are both 0.001; Group OH-5w<Group SH-5w, SB-5w, p-values are 0.016 and 0.024, respectively.
The structural model index of the SB-5w and OB-5w groups was significantly higher in the OB-5w group, whereas trabecular thickness was significantly higher in the SB-5w group.
The 9-week kept groups had statistically significant differences in all of the parameters (p<0.0001) (Table 5). The Bonferroni-based post hoc analysis showed that the SB-9w group had a significantly higher percentage bone volume, trabecular thickness, and trabecular number than the SH-9w and OH-9w groups, whereas its specific surface and structural model index were significantly lower than the SH-9w and OH-9w groups. The OB-9w group also presented a significantly higher percentage bone volume and trabecular number and a significantly lower trabecular separation and trabecular pattern factor than the SH-9w and OH-9w groups.
All of the parameters showed statistically significant differences (p<0.0001).
BV/TV: Group SB-9w>Group SH-9w, OH-9w, OB-9w, p-values are each<0.0001, <0.001 and 0.05, respectively; Group OB-9w>Group SH-9w, OH-9w, p-values are<0.0001 and 0.014, respectively.
BS/BV: Group SB-9w<Group SH-9w, OH-9w, OB-9w, p-values are 0.001, <0.0001 and<0.0001, respectively.
Tb.Pf: Group SB-9w<Group SH-9w, OH-9w, OB-9w, p-values are<0.0001, <0.0001 and 0.008, respectively.
SMI: Group SB-9w<Group SH-9w, OH-9w, OB-9w, p-values are all<0.0001.
Tb.Th: Group SB-5w>Group SH-5w, OH-5w, OB-5w, p-values are<0.0001, <0.0001 and 0.001, respectively.
Tb.N: Group SB-9w>Group SH-9w, OH-9w, p-values are both<0.0001; Group OB-9w>Group SH-9w, OH-9w, p-values are 0.001 and 0.043, respectively.
Tb.Sp: Group SH-9w>Group SB-9w, OB-9w, p-values are both<0.0001.
DA: Group SH-9w>Group OH-9w, OB-9w, p-values are<0.0001 and 0.001, respectively; Group SB-5w>Group OH-5w, OB-5w, p-values are<0.0001 and 0.001, respectively.
For the SB-9w and OB-9w groups, specific surface, trabecular pattern factor and structural model index were significantly higher in the OB-9w group, whereas percentage bone volume, trabecular thickness, and degree of anisotropy were significantly higher in the SB-9w group.
Histological results
The undecalcified histology results of the 5-week group found almost no new bone formation in the SH-5w group, with only some partial hydrogel. The OH-5w group was observed to have no new bone formation and hydrogel remnants in the defect area. The SB-5w group demonstrated a connection between remnant bone and newly formed bone to form a cortical bone along with a partial trabecular bone. The OB-5w group showed a mixture of new bone and hydrogel in the defect area, but no full bone bridging formation (Fig. 4).
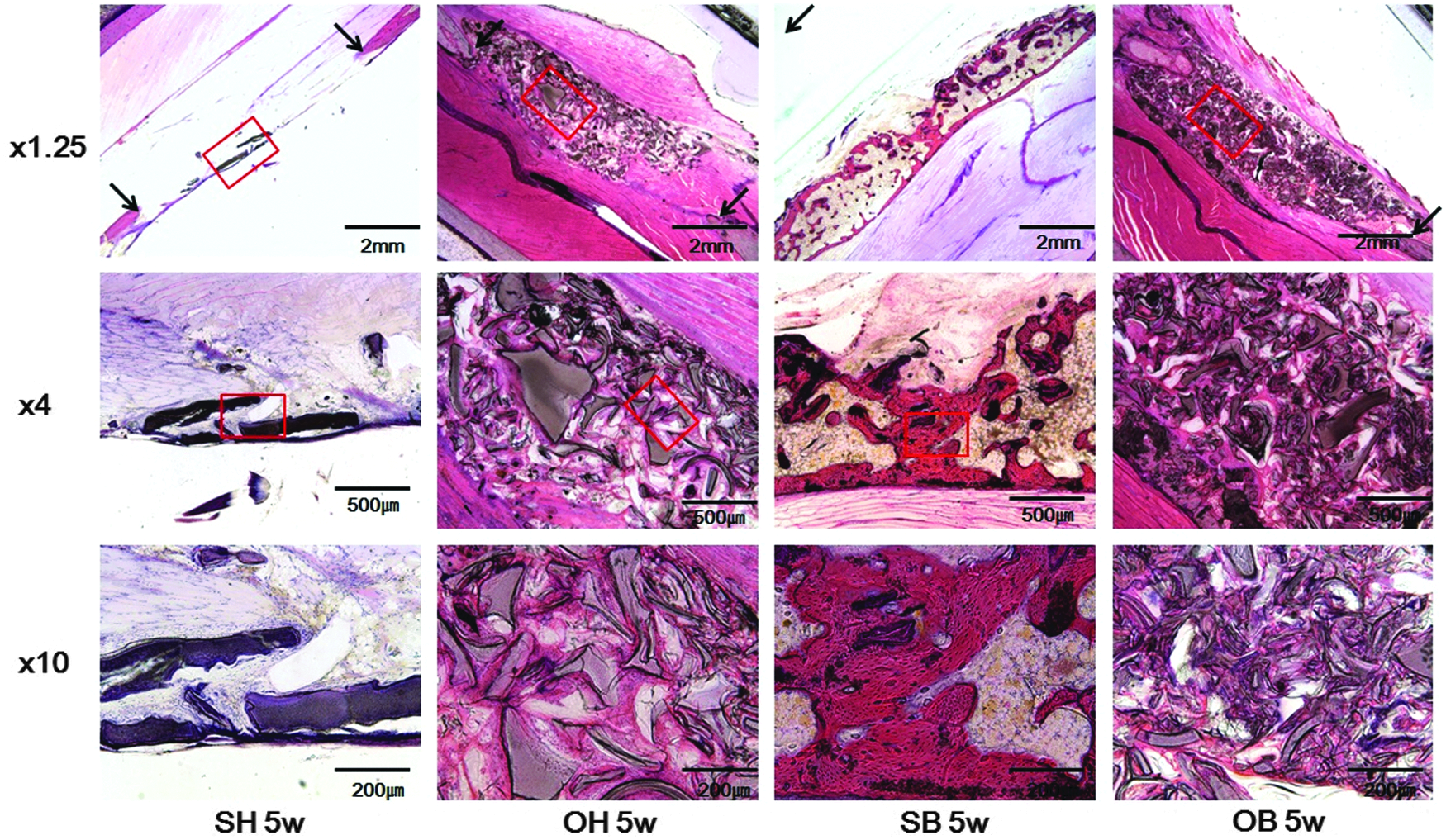
Histological results for the 5-week groups. Hematoxylin and eosin (H&E) staining. The SH-5w group showed almost zero new bone formation and some hydrogel remained. The OH-5w group showed neither new bone formation nor hydrogel remnants in the defect. The SB-5w group showed a connection between the remnant bone and the newly formed bone to form a cortical bone along with some partial trabecular bones. The OB-5w group showed a mixture of new bones and hydrogel in the defect but not complete bone bridging. SH-5w group, in the sham group and HA-carrier group; OH-5w, in the osteoporosis group and HA-carrier group; SB-5w, in the sham group and rhBMP-2 10 μg-containing HA-carrier group; OB-5w, in the osteoporosis group and rhBMP-2 10 μg-containing HA-carrier group. Arrow, remnant fibular bone margin; Rectangular box, magnified area.
In the 9-week group, the SH-9w group showed hydrogel remnants, and no new bone formation. The OH-9w group showed hydrogel remnants, but no new bone formation. The SB-9w group showed new bone formation in the whole defect area and remodeling was underway with clearer trabeculation along with marrow space. The OB-9w group exhibited new bone formation and bridging, but minor trabeculation compared to the SB-9w group while presenting more hydrogel remnants (Fig. 5).

Histological results for the 9-week groups. H&E staining. The SH-9w group showed only HA-carrier remnants and no new bone formation. The OH-9w group showed HA carrier remnants but no new bone formation. The SB-9w group showed new bone formation in the whole defect together with marrow space and clearer trabeculation to allow remodeling. The OB-9w group provided new bone formations and bridging, but only minor trabeculation compared with the SB-9w group, while also having higher amounts of HA carrier remnants. SH-9w group, in the sham group and HA-carrier group; OH-9w, in the osteoporosis group and HA-carrier group; SB-9w, in the sham group and rhBMP-2 10 μg-containing HA-carrier group; OB-9w, in the osteoporosis group and rhBMP-2 10 μg-containing HA-carrier group. Arrow, remnant fibular bone margin; Rectangular box, magnified area.
The histomorphometric analysis showed that the ratios of the newly formed bone lengths to the fibular defect lengths of the SB-5w (95.5±3.5%) and SB-9w groups (98.7±1.4%) were significantly higher than those of the OB-5w (46.5±18.5%) and OB-9w groups (55.8±21.4%) (p=0.0004 and 0.0021, respectively). However, no significant difference was found between the SH-5w group (5.5±3.6%) and the OH-5w group (2.3±1.5%), nor between the SH-9w group (10.7±6.3%) and the OH-9w group (4.8±2.7%).
Discussion
This study is the first to compare rhBMP-2 osteoinductivity in osteoporosis and sham animals using a segmental long-bone defect model. To evaluate rhBMP-2 osteoinductivity in the most difficult environment for bone healing, a fibular segmental defect model was selected because it had a far smaller remnant bone area than the femur, tibia, or radius; furthermore, it consists of only cortical bone, so bone healing is even more difficult. 26 To create an osteoporosis case with severely compromised bone stock, dexamethasone together with an ovariectomy was used for the intramuscular injection model. The ovariectomy model is the most frequently used model for simulating osteoporosis, but it is limited in that it does not stimulate severe osteoporosis. However, if ovariectomies and steroid injections are performed simultaneously, osteoporosis cases that are more severe than when using ovariectomies alone can be triggered (based on this research authors' unpublished data). Therefore, in this study, we selected the most difficult environment for rhBMP-2 osteoinductivity.
As for the results of Micro-CT, compared with the rhBMP-2-treated sham group, the rhBMP-2-treated osteoporosis group showed significantly lower value in percentage bone volume and trabecular thickness which are the indicators for bone quantity at the fifth and ninth week.
Additionally, as the trabecular pattern factor showed significantly high value, this can be interpreted as that the ovariectomy and corticosteroid-induced osteoporosis rat fibular segmental defect model to show quantitative and qualitative inhibition on rhBMP-2-mediated new bone formation. Furthermore, progression of bone healing showed difference between fifth and ninth week, depending on the factor of osteoporosis. The new bone coverage ratio at the fibular defect area of the rhBMP-2-treated sham group was 99.4% from the fifth week; therefore, there could not be a significant increase at the ninth week. However, the percentage bone volume or trabecular number was found to be incrementally higher for those of the ninth week than for those of the fifth week.
On the contrary, though the new bone coverage ratio at the fibular defect site of the rhBMP-2-treated osteoporosis group, showed an increase at the ninth week compared to the fifth week, there was no tendency of bone quantity and quality improvement in the micro-CT.
This means that in the sham group, bone quantity and quality showed improvement between the fifth week and the ninth week, however, the results in the osteoporosis group showed that there was progression of bone healing between the fifth week and the ninth week but the pace of bone healing was slower compared with that of the sham group.
Such findings are interpreted to mean that osteoporosis has a critical effect on MSCs. Furthermore, in the osteoporosis animal model, the postfracture callus cross-sectional area is known to decrease. 27 Additionally, in our study, we assume that the 10 times injected corticosteroids during the 5-week period had a detrimental effect on MSCs 28 to decrease the osteoinductivity of rhBMP-2.
For bone healing, including fracture healing, the progenitor cell property is known to be very important along with the biological environment. 29 The MSCs of osteoporosis patients have been reported to have lower proliferation rates and tend to proliferate more easily toward adiopogenesis rather than osteoblastogenesis. 30 The actions of rhBMP-2 are dependent on MSC proliferation and differentiation. Our study found that the ovariectomy and corticosteroid-induced osteoporosis model had a significantly lower rhBMP-2-mediated bone formation in the fibular defect area than the sham group, partly because of the lower level of rhBMP-2-led MSC osteoblastic differentiation in the osteoporosis model than in the sham model.
However, in the rhBMP-2 treatment both the osteoporosis and the sham groups showed significantly higher bone formations than the HA carrier-injected groups. Therefore, it was proven that rhBMP-2 helped maintain osteoinductivity in the osteoporosis fibular defect model, thus demonstrating its bone healing effect.
This study is limited in several aspects. First, the bone formation of the fibular defect area was compared using micro-CT and histomorphometric analyses, but a biomechanical test was excluded. In fact, the clinical significance of newly formed bone is more meaningfully viewed through mechanical strength. However, it is not straightforward to perform a three-point bending test in the 5-mm defect rat fibula model. Another limitation is that the β-TCP microsphere-HA-based powder gel composite carrier used in this study as the rhBMP-2 carrier might have affected rhBMP-2 osteoinductivity to some extent. Actually, collagen, fibrin, and calcium phosphates, such as hydroxyapatite and tricalcium phosphate are frequently used as rhBMP-2 carriers.19,31,32 However, to evaluate properly the ectopic bone formation effect, carriers containing high-osteoconductivity hydroxyapatite or tricalcium phosphate for the main part are not appropriate. In addition, for morphologically natural injections into the bone defect area, an injectable carrier in the correct shape is considered more appropriate. Therefore, we used an HA-based carrier containing only a small amount of β-TCP microspheres. 21 The third limitation is the pertinence of the fibular defect model used in our research as a proper animal model to evaluate the osteoinductivity of rhBMP-2 in osteoporosis. The fibula is mainly composed of cortical bone, and an ovariectomy stimulates estrogen deficiency, which in turn results in cancellous bone loss. Thus, relatively less cortical bone loss occurs. Although, in this study, bone loss in fibula itself was not assessable, it could be assumed that the bone loss to be less than that of the vertebra and hip. However, rhBMP-2 osteoinductivity triggers bone formation through the osteoblastic differentiation of the host MSCs. Therefore, as in this research, if a sufficient level of osteoporosis is caused by an ovariectomy combined with a corticosteroid injection, it seems possible to evaluate the BMD reduction degree in osteoporosis, regardless of the reduction in the fibula itself. The fourth limitation is from the fact that, corticosteroid-induced osteoporosis has pathologic difference compared with other types of osteoporosis. 33 Corticosteroid is known to inhibit differentiation and function of the osteoblast, to induce apoptosis, and to show antiapoptotic effect to the osteoclast.34,35 As for this study, we induced severe osteoporosis by ovariectomy and corticosteroid injection, which has different pathophysiology from general osteoporosis, which makes it a limitation to generalize our results.
In sum, in the rat fibular mid-shaft critical defect model, rhBMP-2 was found to have maintained its osteoinductivity in the osteoporosis group, contributing to significant bone healing but not achieving complete healing. In comparison, in the sham group rhBMP-2 led to complete bone healing in the defect area and bone quality improvement over time. Based on these findings, the ovariectomy and corticosteroid-induced osteoporosis is considered to reduce rhBMP-2 osteoinductivity significantly.
Therefore, when using rhBMP-2 in patients with osteoporosis, doses that are the same as those given to patients without osteoporosis may undermine treatment effectiveness.
Conclusion
Overall, rhBMP-2 was found to maintain osteoinductivity in the osteoporotic rat fibular defect model. However, the complete healing observed in the normal rats could not be achieved in the ovariectomy and corticosteroid-induced osteoporotic rats and thus ovariectomy and corticosteroid-induced osteoporosis is considered to reduce rhBMP-2 osteoinductivity significantly.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2013R1A1A2061858). The authors thank Daewoong Pharmaceutical for providing the rhBMP-2. We also thank Dr. A. Young Lee for editing the article.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.