
Abstract
Introduction:
The surgical treatment of large bone defects continues to pose a major challenge in modern trauma and orthopedic surgery. In this study we test the effectiveness of a tissue engineering approach, using three-dimensional (3D) β-tricalcium phosphate (β-TCP) scaffolding plus bone marrow-derived mononuclear cells (BM-MNCs), combined with a vascularized periosteal flap, in a rat femur critical size defect model.
Methods:
Eighty rats were randomly allocated into four equal groups. Under general anesthesia, critical size defects were created on their femurs and were treated with (1) Vascularized periosteal flap alone, (2) Vascularized periosteal flap+β-TCP scaffolding, (3) Vascularized periosteal flap+β-TCP scaffolding+ligated vascular pedicle, and (4) Vascularized periosteal flap+β-TCP scaffolding+BM-MNCs. After 4 and 8 weeks animals were euthanized and the bone defects were harvested for analysis of new bone formation, vascularization, and strength using histology, immunohistology, micro-CT, and biomechanical testing, respectively.
Results:
Group 1: (P. flap) Increase in new bone formation and vascularization. Group 2: (P. flap+scaffold) Increase in new bone formation and vascularization. Group 3: (P. flap+scaffold+ligated vascular pedicle) No new bone formation and no vascularization. Group 4: (P. flap+scaffold+BM-MNCs) A significant (p < 0.05) increase was seen in new bone formation, vascularization, and strength in bones treated with flaps, scaffold, and BM-MNCs, when compared with the other treatment groups.
Conclusion:
Combining a vascularized periosteal flap with tissue engineering approach (β-TCP scaffolding and BM-MNC) results in significantly improved bone healing in our rat femur critical size bone defect model.
Introduction
T
Vascularized or nonvascularized autologous bone grafts are still the treatment of choice in these difficult nonhealing defects.1,2 Other treatments include the Ilizarov procedure, 3 bone graft substitutes,4,5 and even the “Masquelet” or induced membrane technique.6,7 Each of these treatments provides its own unique benefits, however, each is also associated with its own characteristic drawbacks, resulting in the search for new and better treatment options for these complex wounds.
Recent interest in the development of cell-based tissue engineering approaches for treating large bone defects has generated a great deal of interest in the clinical arena, research circles, and in industry alike.8–10 These approaches generally consist of treating the defect with different combinations of three-dimensional (3D) structural scaffolds, osteo- and/or vasculo-genic cells (mesenchymal stem cell [MSC], endothelial progenitor cells [EPC], and bone marrow-derived mononuclear cell [BM-MNC]), and cytokines (bone morphogenetic protein [BMP], vascular endothelial growth factor [VEGF], and fibroblast growth factors [FGF]).11,12 The potential advantage of this approach is the ability to deliver key factors, known to play an essential role in bone healing, directly into the defect where they are most needed, and thus optimize the healing process.
Three-dimensional structural scaffolds, often made of hydroxyapatite or various forms of β-tricalcium phosphate (β-TCP), or “bone graft substitutes,” as their name implies, have been developed to replace autologous bone grafts.13,14 These substitutes have been specifically engineered to have osteoinductive properties and to integrate with bone tissue while at the same time providing 3D structural support 15 for architectural integrity. Although these substitutes have been successful at reducing the need for autologous bone, their ability to duplicate the inherent osteo- and vasculo-genic properties afforded by autologous bone grafts has yet to be demonstrated conclusively. 16
Several investigators have demonstrated enhanced bone repair using these structural 3D scaffolds seeded with different combinations of bone marrow-derived stem cells. 17 In the previous work we have demonstrated that MSC and/or EPC, or BM-MNC seeded onto β-TCP scaffold 18 and introduced into a rat femur critical size defect resulted in significant improvement in bone mass, mechanical strength, early vascularization, and healing time. 14
Cytokines play a key role in bone healing by paracrine effects on adjacent cells. For example, BMP binds to membrane receptors and stimulates bone healing by the TGF-β-pathway. Taking advantage of this, Vogelin et al. treated rat femur critical size defects with recombinant human BMP-2 (rh-BMP) and demonstrated a significant increase in new bone formation when compared with controls. They demonstrated that this positive effect was most pronounced, leading to complete bone healing, when in addition to treatment with rh-BMP the defect was wrapped with a local vascularized periosteal flap harvested from the animal's medial femur condyle. 11
Periosteum is known to have excellent osteogenic capacity, particularly during growth in the young. It contains a rich blood supply, pluripotent MSC with the potential to form either cartilage or bone, and produces bioactive factors that are known to be chondrogenic. 19 In 1991 Doi and Sakai introduced the concept of using periosteum in the form of a vascularized periosteal flap, harvested from the medial femur condyle, to treat bony defects. Since then this flap has been used, both as a local and a free flap, to repair and reconstruct bony defects in several different anatomical locations. 20 When used to treat large bone defects of the femur shaft, the flap is harvested from the medial femoral condyle on a vascular pedicle and rotated proximally into the defect. In their original description of this flap the authors describe it as being “well vascularized, highly osteogenic and with a thin and pliable structure that makes it easy to mould to conform to different shapes of defects.”21–25
In this study, we combined these powerful osteogenic capabilities of the periosteal flap with a tissue engineering approach (β-TCP scaffold+BM-MNC) and measured new bone formation, vascularization, and biomechanical strength, in a rat femur critical size bone defect model.
Materials and Methods
Eighty rats were allocated into four equal groups. Large bone defects were created on their femurs and were treated with different combinations of periosteal flap, β-TCP scaffold, and BM-MNC (Table 1). Bone healing at the site of the defect was assessed at 4 and 8 weeks post treatment using immunohistochemistry, histology, and radiology. Bone strength at the defect site was measured at 8 weeks using biomechanical three-point bending tests.
β-TCP, β-tricalcium phosphate; BM-MNC, bone marrow-derived mononuclear cell.
Animal care
We performed a prospective, randomized animal study. All experiments were performed in accordance with regulations established and approved (Project No. F3/21; Regierungspräsidium, Darmstadt, Germany) by our institution's animal care and oversight committee according to German law. Eighty 10-week-old, male, Sprague-Dawley rats (Harlan, Rossdorf, Germany) weighing 350–400 g were used in this study. Animals were kept in individual cages in temperature (21°C), light (12 h light, 12 h dark), and air flow-controlled rooms and fed standard rodent food and water containing Tramadol pain medication (after surgery) ad libitum. Animals were monitored daily in the postoperative period for signs of pain, discomfort, and complications.
Treatment groups
Surgical technique
For the creation of the critical size bone defect and the periosteal flap harvest and transfer, animals were anesthetized with an intraperitoneal injection of a mixture of ketamine chlorhydrate (Ketamin 100 mg/kg) and xylazine hydrochloride (Rompun 10 mg/kg) (Table 1). Their right hind limbs were shaved, cleaned, and disinfected (with chlorhexidine solution) and a medial longitudinal incision was performed over the femur, under aseptic conditions. The fascia was incised, exposing the vastus medialis and biceps femoris muscles, which were separated using blunt dissection to identify the descending genicular artery and vein, running along the femur, nourishing the periosteum at the medial condyle (Fig. 1).
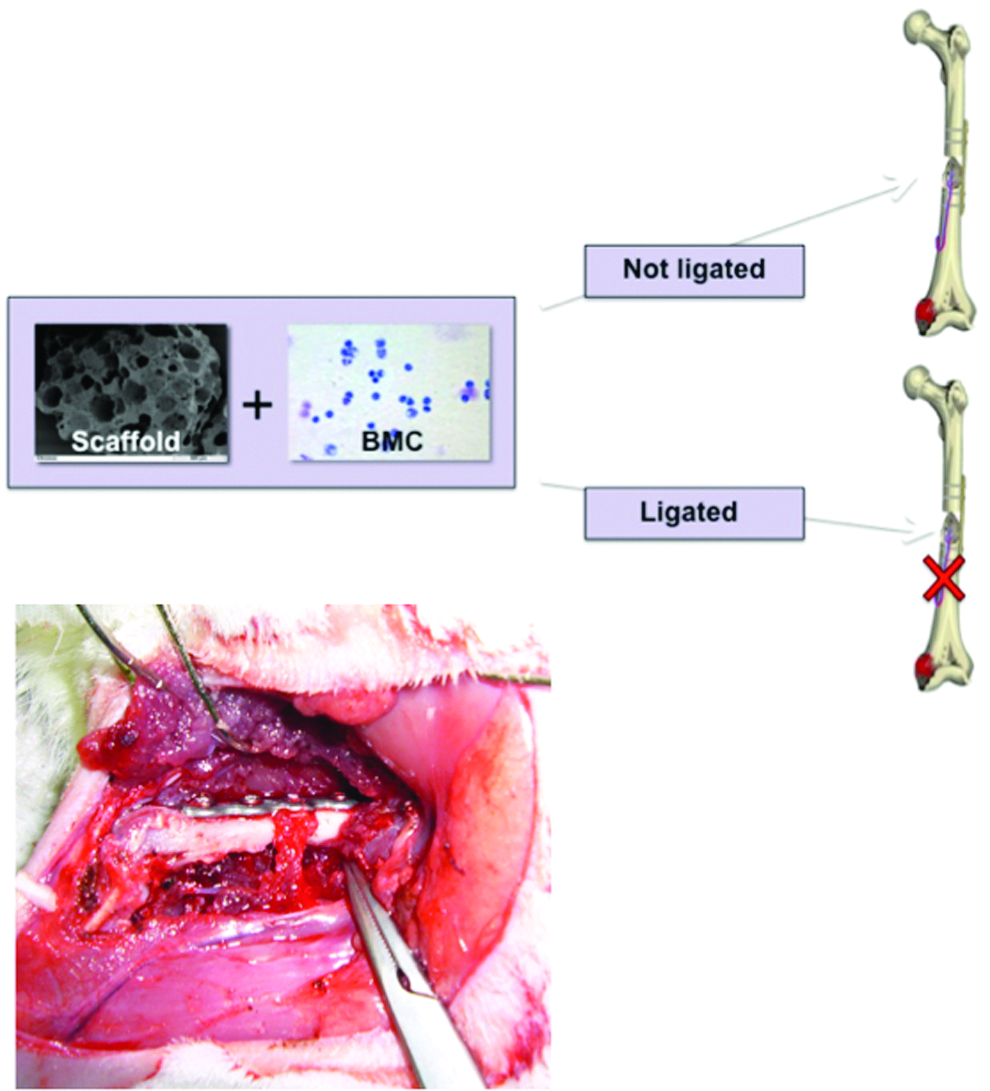
β-tricalcium phosphate (β-TCP) scaffold was seeded with bone marrow-derived mononuclear cell (BM-MNC) and placed into the femur defect. The periosteal flap is harvested from the medial femoral condyle on its vascular pedicle (Descending genicular artery) and rotated proximally into the defect. The vascular pedicle is ligated in group 3. The plate is fixed to the anterior side of the femur shaft bridging the defect; then, the periosteal flap is fixed to the plate facing into the defect.
A 5 × 4 mm periosteal flap, over the medial aspect of the condyle, was identified and harvested from distal to proximal using a micro knife and chisel. The femur was then exposed, along its entire trajectory and a five-hole plate (LCP plate Compact Hand 1.5; Synthes, Umkirch, Germany) was fixed to its anterior aspect. Once secured in place a 7 mm long defect was created on the femur shaft beneath and midway along the plate using a 7 mm drill bit. Care was taken to remove all bone fragments in the defect. The periosteal flap was then rotated on its vascular pedicle to the medial aspect of the defect and gently fixed, with sutures (5-0 Vicryl; Ethicon, Norderstedt, Germany), to the plate bridging the defect zone (Fig. 1). After the defects received their respective treatments (Table 1), the quadriceps muscle was reapproximated and sutured (5-0 Vicryl; Ethicon) in place and the skin was reapproximated using continuous intracutaneous sutures (4-0 Prolene; Ethicon).
After 4 and 8 weeks rats were killed using an overdose of Pentobarbital (150 mg/kg, i.p.) and weighed. The treated femurs were exposed and examined macro- and microscopically for signs of infection or tumors. The bones were then frozen and stored at −80°C for subsequent preparation for immunohistology. Thereafter, the bones were fixed in Zinc-Formal-Fixx (4%; Thermo Electron, Pittsburgh, PA) for 20 h and decalcified over a period of 14 days in a solution containing 0.25 M Trizma base (Sigma-Aldrich, Deisenhofen, Germany). 18
BM-MNC harvest, isolation, and characterization
Femurs were surgically removed from 20 donor rats and bone marrow was flushed from the marrow cavities using a sterile syringe containing diluted (1:5) phosphate-buffered saline (PBS; Biochrom, Berlin, Germany). The resulting marrow/PBS mixture was layered on a ficoll density gradient and centrifuged continuously for 20 min at 800 g. Mononucleated cells were collected, washed three times with PBS (10 min, 800 g), resuspended in PBS, and counted. 26
BM-MNC seeding onto β-TCP scaffold
One million BM-MNC, in a volume of 400 μL, were dripped onto a 4 cm2 monolayer of 0.7–1.4 mm diameter granules of β-TCP (Chronos; Synthes) and was incubated for 10 min at 37°C. This procedure was repeated three times and the granules were then transferred to another well and the number of nonadherent BM-MNC in the remaining supernatant was assessed to calculate seeding efficacy. Then, the β-TCP granules were transported, at room temperature, to the animal facility where they were implanted into the bone defect within 30 min.14,18
BM-MNC-β-TCP-scaffold adherence measurements
To assess BM-MNC adherence to the β-TCP-scaffold some of the granules previously seeded with BM-MNC were fixed in 0.5% formaldehyde solution (10 min, room temperature). The formaldehyde solution was removed and the samples were gently washed three times with PBS and DAPI (1 μg/mL in PBS) (Life Technologies, Darmstadt, Germany) was added. The DAPI solution was removed after 5 min followed by three washings with 1 mL of PBS for each wash. Finally, adherence was assessed by directly viewing the samples at high magnification with fluorescence microscopy (Figure 2).
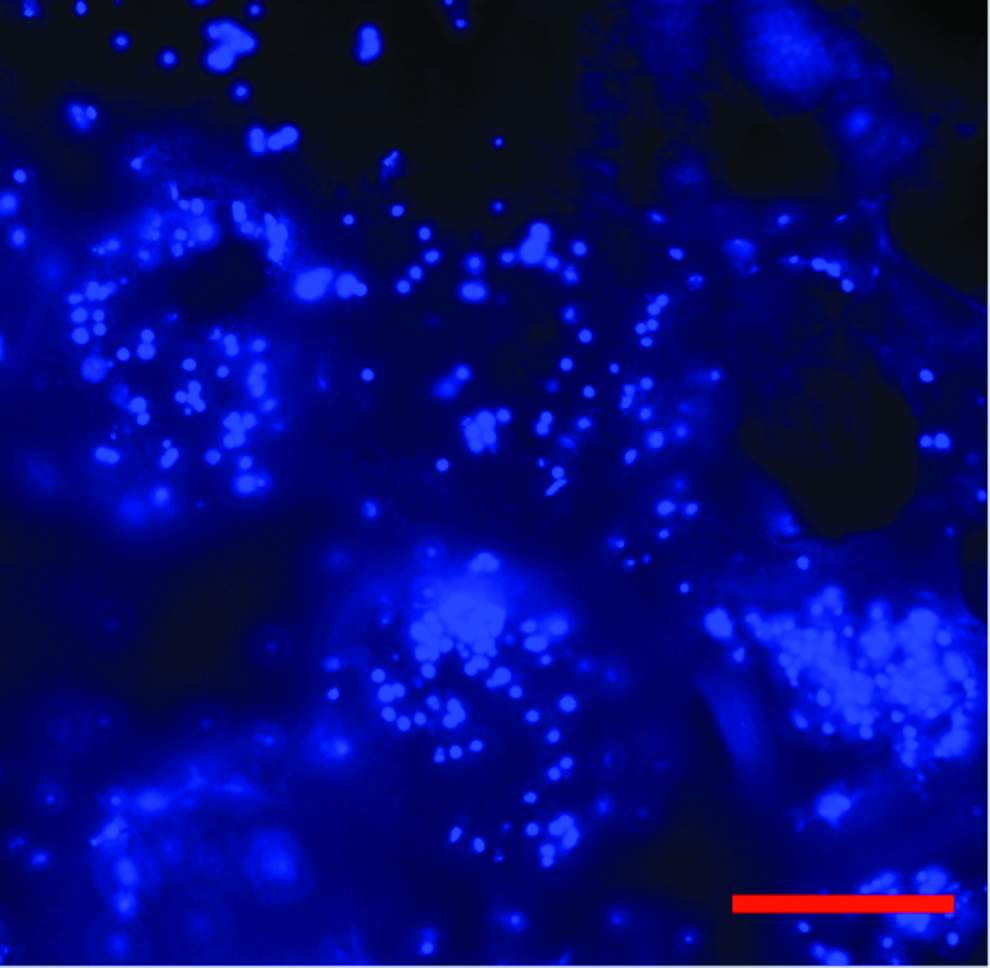
DAPI-stained BM-MNC (blue dots) adhere in great number on the β-TCP scaffold. Aliquots of each BM-MNC preparation were analyzed for adherence of BM-MNC to the scaffold before being delivered into the defect. Red bar represents 200 μm.
Bone vascularization, formation, strength, and healing measurements
At 4 weeks, 6 of 20 femurs in each group were taken for further analysis. Three of six femurs were used to measure new vessel (CD31) and bone formation (hematoxylin and eosin [H&E] staining) and the remaining three were used to measure bone appearance with μCT, and strength by biomechanical testing. At 8 weeks bone formation, strength and healing in the remaining 14 of 20 femurs, was measured using μCT (6 femurs), immunohistochemistry (8 femurs), quantitative histomorphometry (8 femurs), and biomechanical testing (same femurs used previously for μCT). Samples taken from the bone defect zone were decalcified, fixed in 4% formaldehyde, and embedded in paraffin. Sections were stained with H&E or incubated with antibodies directed against CD31 (blood vessels, dilution 1:50, incubation 4°C overnight). Polyclonal horseradish peroxidase coupled secondary antibodies were applied and the sections were incubated with 3-amino-9-ethylcarbazole. Evaluation of new bone formation and antibody-stained cells were performed using Axiovision software (Zeiss, Goettingen, Germany). Defect, membrane-scaffold contact, and scaffold-bone end interface were examined. CD31-positive blood vessels were counted in six nonoverlapping images/slide/animal surrounding the defect zone and the mean number of vessels were calculated. These means were subsequently used for statistical analysis. Cells positive for CD31 were not considered. Imaging and blood vessel counting were performed with blinded specimens examined in random order by an independent observer, blinded to the group setup.14,18
Bone density and micro architecture measurements
To assess bone density and micro architecture at the defect site peripheral quantitative computed tomography (PQCT) and μCT (Skyscan 1176; Bruker, Billerica, MA) were performed on 6 of the 14 femurs harvested at 8 weeks and on 3 harvested at 4 weeks. For imaging, femurs were oriented along their long axis orthogonally to the axis of the X-ray beam (90 kV X-ray source, fully distortion corrected 11Mp X-ray camera). Two-dimensional CT images were scanned and reconstructed using a standard convolution-back-projection procedure. The isotropic voxel size was 18 μm. The analyzed volume of interest was placed at the center of the bone defect with 0.7 mm thickness for all samples. A multi threshold analysis based on attenuation distribution was carried out to separate scaffold, bone, and callus from each other and obtain their volumes. 14
Biomechanical measurements
In bones (six in total), which had already been used for PQCT, biomechanical properties at the defect site were measured by a destructive three-point bending procedure using a material testing machine (Zwickiline Z5.0; Zwick-Roell, Ulm, Germany). The “bending until failure” method was performed by lowering a bar onto the femur, using a constant deflection speed of 0.1 mm/s, and recording the load and deflection continuously. The ultimate load was then calculated using Testexpert-II software (Zwick-Roell). 14
Statistics
Estimation of sample size and power
Sample size calculation was performed on the basis of results obtained in similar former studies using the same bone defect model.14,27 A minimum group size of n = 6 is necessary to calculate significances of existing differences with regard to bending stiffness, vascularization (histology), and new bone formation (histology) between control and test groups using multiple testing. The software BIAS 10.11 (Epsilon, Darmstadt, Germany) was used for group size calculation. For powering the study, we propose an α-error of 0.05, and a β-error of 0.1 (power of 0.9) for the primary outcome parameter (bending stiffness).
Differences between the groups were compared using the nonparametric Kruskal–Wallis test followed by multiple Conover–Iman comparison with Bonferroni–Holm-correction. To avoid excessive multiple testing, defined groups were compared post hoc, depending on the particular question. An adequate α-alignment for multiple comparisons was conducted. The nonparametric Wilcoxon test was applied to analyze changes during the follow-up period (4 weeks vs. 8 weeks). A p-value below 0.05 was considered significant.
Results
Of the 80 rats operated no deaths occurred during surgery or in the immediate postoperative period. No abnormal behavior of the animals was detected in daily postoperative monitoring. However, at the time the femur bones were harvested for measurements, signs of infection were detected at the defect site in two femurs, and three plates were found dislocated in group 3 in which the flap pedicles were ligated.
Morphological observations
In group 1 (flap only), in all cases, both at 4 and 8 weeks, a thick calcified structure was found growing into the defect from the medial side (where the flap was placed) and no other signs of healing were observed. In group 2 (flap+β-TCP scaffold), in all animals, both at 4 and 8 weeks, a thick bony formation was seen in the defect and initial signs of healing were observed. In group 3 (flap+β-TCP scaffold+ligated vascular pedicle), in all femurs, at both 4 and 8 weeks, a necrotic flap and no signs of bone healing were observed. In two animals, in this group, infection was detected at the site of the defect. In group 4 (flap+β-TCP scaffold+BM-MNC), in all femurs, both at 4 and 8 weeks, a thick bony formation was seen in the defect and new bone was seen growing throughout the entire defect zone.
Vascularization, bone formation, strength, and healing
Bone formation was observed in close proximity to the periosteal flap, both at 4 weeks, and more so, at 8 weeks, in all cases, except for defects treated with flaps with ligated vascular pedicles (Fig. 3A–D). In groups 1, 2, and 4, with varying degrees, new bone formation could be seen protruding from the flap and in the defect zone. Histological analysis confirmed this observation, demonstrating a close correlation between the periosteal flap and cortical bone formation at 8 weeks in all cases (Fig. 3). In group 3 (ligated vascular pedicle) minimal bone formation was observed at the defect, and the periosteal flap was found to be partially (4 weeks) and completely (8 weeks) reabsorbed (Fig. 3C).
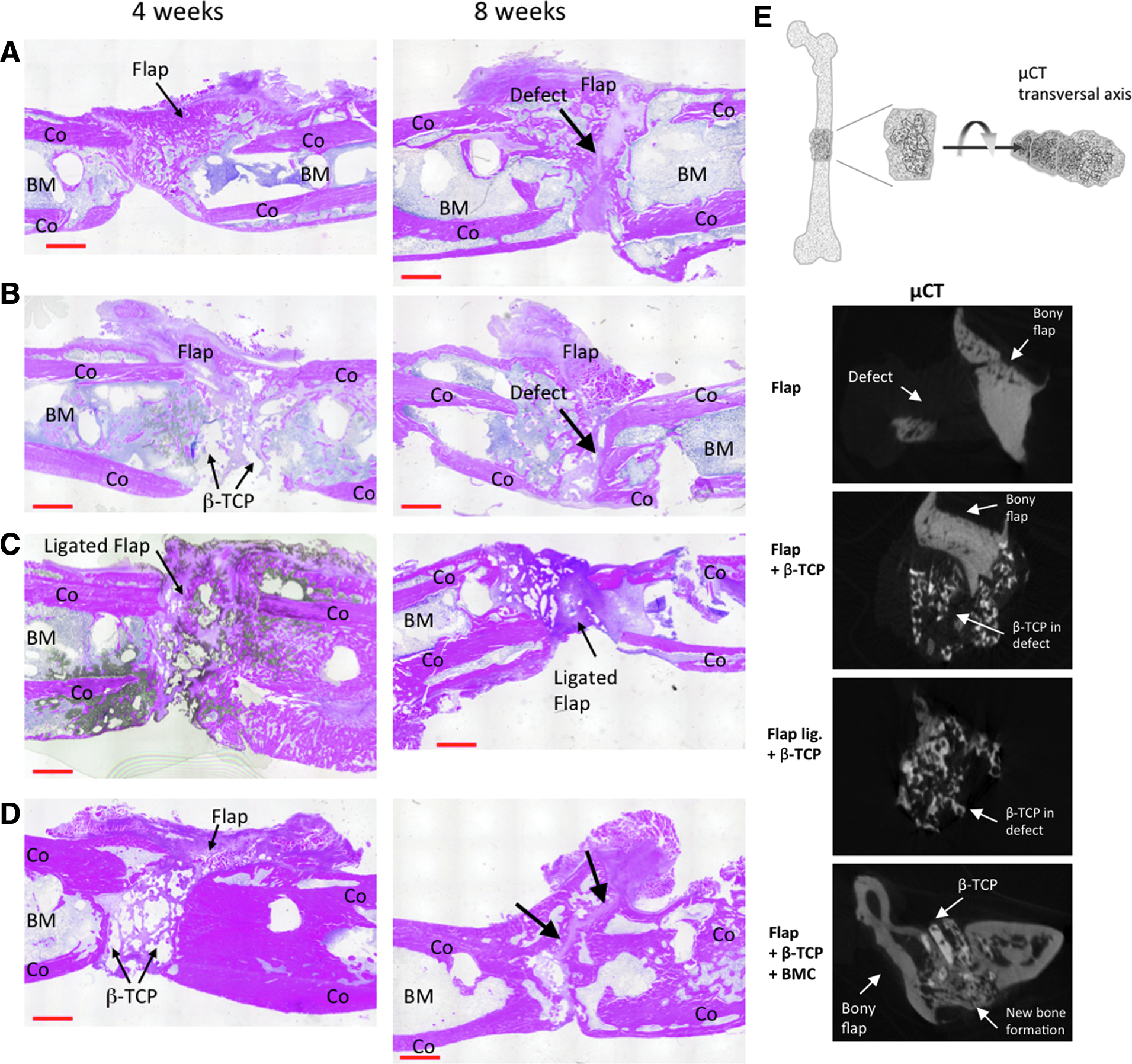
Representative hematoxylin and eosin (H&E)-staining, histological overview of the defect zone at 4 and 8 weeks after implantation of the periosteal flap (flap);
Histological analysis of all defects, treated with vascularized flaps, revealed thick bony tissue formation. Bone density, thickness, and integration into the defect zone were visibly greater in group 4 (flap+β-TCP scaffold+BM-MNC). In contrast, in animals where the vascular pedicle of the periosteal flap was ligated very little bone formation was observed. Finally, β-TCP resorption appeared to be more advanced in these animals.
Bone density and micro architecture
Results observed in histological analysis were confirmed by the μCT-analysis (Fig. 3E). In groups 1, 2, and 4 the thick bony flap and increased healing could be seen in the defect, while in group 3 (ligated vascular flap) only loose noncalcified tissue was observed.
Biomechanical results
Bone mineral density values and biomechanical stability at weeks 4 and 8 were highest in group 4 (flap+β-TCP scaffold+BM-MNC), compared with all other groups (Figs. 4 and 5). Bone mineral density at 4 weeks was significantly (p < 0.05) higher in group 4 (flap+β-TCP scaffold+BM-MNC) than in group 2 (flap+β-TCP scaffold) and group 3 (ligated vascular pedicle). In group 1 (flap only), at 4 weeks, bone mineral density was slightly increased, though not significantly (p < 0.06), compared to group 4 (flap+β-TCP scaffold+BM-MNC). Biomechanical stability at 4 weeks was significantly (p < 0.05) higher in group 4 (flap+β-TCP scaffold+BM-MNC) than in group 1 (flap only) and group 3 (ligated vascular pedicle) and slightly (p < 0.08) higher than in group 2 (Fig. 5A, B). Biomechanical stability at 8 weeks was significantly (p < 0.05) higher in group 4 (flap+β-TCP scaffold+BM-MNC) than in group 3 (ligated vascular pedicle) and slightly (p < 0.12) higher than in group 1 (flap only). The increase in biomechanical stability from week 4 to 8 in group 4 (flap+β-TCP scaffold+BM-MNC) was also significantly (p < 0.05) greater than in all other groups.

Bone mineral density (BMD) in the defect zone;

Biomechanical testing of the femur after
Discussion
Vascularized and nonvascularized bone grafts provide an ideal mix of structural 3D scaffolding, bone forming cells, cytokines, and vascularization to promote optimal bone healing, and consequently result in the best outcomes, to date, in the treatment of large bone defects. In this study we attempted to reproduce this “ideal mix” by treating large bone defects created on the rat femur, with a combination of 3D scaffold, BM-MNC, and vascularized periosteal flaps (Fig. 1).
The β-TCP scaffold we used in this study is sold commercially as Chronos®, and is readily available for clinical use. In previous in vitro experiments, we compared six different, commercially available scaffolds (Chronos, Vitoss®, Actifuse®, Biobase®, Cerabone®, and Tutoplast®) and found Chronos to be superior in its osteoconductive and osteoinductive properties, that is, number of invading cells, cell location, differentiation rate, and potential.5,14,28
In the above study, to test the biocompatibility and effectiveness of the different scaffolds we seeded them with MSC. MSC were chosen because of their known potential to differentiate into chondrogenic and/or osteogenic cells. In an attempt to further enhance the bone forming capacity of MSC, we and others have used genetically modified MSC, 29 BMP,11,12 VEGF, 30 FGF, 31 and EPC. 14 So far the best results have been seen when a combination of osteogenic and angiogenic proteins are used.32,33 Using the same rat femur model as in this study, we demonstrated that treating defects with both MSC and EPC, through a synergetic effect, further improved bone healing. 14
While these attempts to improve upon the bone forming capacity of MSC have met with varying degrees of success, using a cell-based approach, even if the ideal mix is found, will inevitably be faced with the logistical hurdles of applying these cells in the clinical setting. In adult bone marrow aspirates, MSC are present at concentrations of <1 in 100,000–500,000 nucleated cells; therefore, to obtain sufficient numbers to insure treatment efficacy they must be expanded in culture.14,34,35 This process may take 2–3 weeks after which, in a second operation, the MSC are delivered into the bone defect. Separately, once EPC are extracted and isolated they must be differentiated for at least 5 days before they can be reintroduced into the patient. To eliminate the need for multiple surgeries, separated by the 1- to 3-week delay we substituted our original MSC+EPC treatment approach with BM-MNC, which can be harvested, filtered, and reintroduced into patients in a single surgery.36–38 Recent clinical studies using BM-MNC to treat patients with myocardial ischemia have reported improved cardiac function and claim that the observed benefits are due to increased vascularization of the myocardium. 38 To determine whether BM-MNC was as effective as MSC+EPC, in healing bone we tested it in our rat femur critical size defect model, and found it to be equal if not better. 39 Based on these findings and the logistical advantages mentioned above, in this study, we chose BM-MNC to treat the defects in our rat femur model.
Eight weeks following treatment, in all animals that received vascularized periosteal flaps (groups 1, 2, and 4) we observed increased bone mass in the defects. This effect was greatest in animals that received β-TCP scaffold+BM-MNC and the vascularized periosteal flaps (group 4) and least in animals whose defect was treated with only β-TCP and vascularized periosteal flaps. This suggests that while the flap+β-TCP (group 2) did cause an increase in bone mass, the flap alone, without BM-MNC, was not sufficient to provide complete healing of the defects. These results differ from those of Vogelin et al., who found that treating rat femur defects with vascularized periosteal flaps+scaffold (in their case OPLA-HY) resulted in no bone formation, after 8 weeks. However, like in our findings, the authors showed that defects treated with flaps+scaffold+rhBMP-2 did go on to form “regular, dense bone” in the defects.11,12
Histologically, the periosteum can be seen as having an outer “fibrous” layer, containing fibroblasts, collagen, elastin, nerves, and vessels, and an inner “cambium” layer contiguous with the bone, containing mesenchymal progenitor cells, differentiated osteogenic progenitor cells, osteoblasts, and fibroblasts. Like the outer layer, the inner layer has its own network of nerves and blood vessels. While its thickness and osteogenic activity diminishes with age, the periosteum continues to play an important role in bone repair, even in adulthood. Of note, particularly in adulthood, is the important role played by the periosteum's rich blood supply.
The presence of vascularization was confirmed in this study by immunohistological CD31 staining, of the medial and lateral aspect of the defects, which indicated the presence of blood vessels. The medial and lateral aspects of the bone defects treated with vascularized periosteal flaps+BM-MNC contained significantly more vascularization, after 8 weeks, in comparison with all other groups (Fig. 6C–E). In contrast, in the animals whose bone defects were treated with periosteal flaps with ligated vascular pedicles (group 3), no vessel formation was found in the vicinity of the defect and there were no signs of bone healing. This observation was also described by Rossi et al., who in a rat fibula defect model, showed that occluding a periosteal flap's vascular pedicle, impeded bone healing. 40 Furthermore, it was in this group (with ligated vascular pedicle) that the only two cases of infection and loosening of the fixation plates (three cases) occurred. These observations demonstrate and reemphasize the importance of good blood supply for good bone healing. In our model good blood supply promoted healing, directly, by promoting osteogenic activity and indirectly, by avoiding complications like necrosis, and infection.
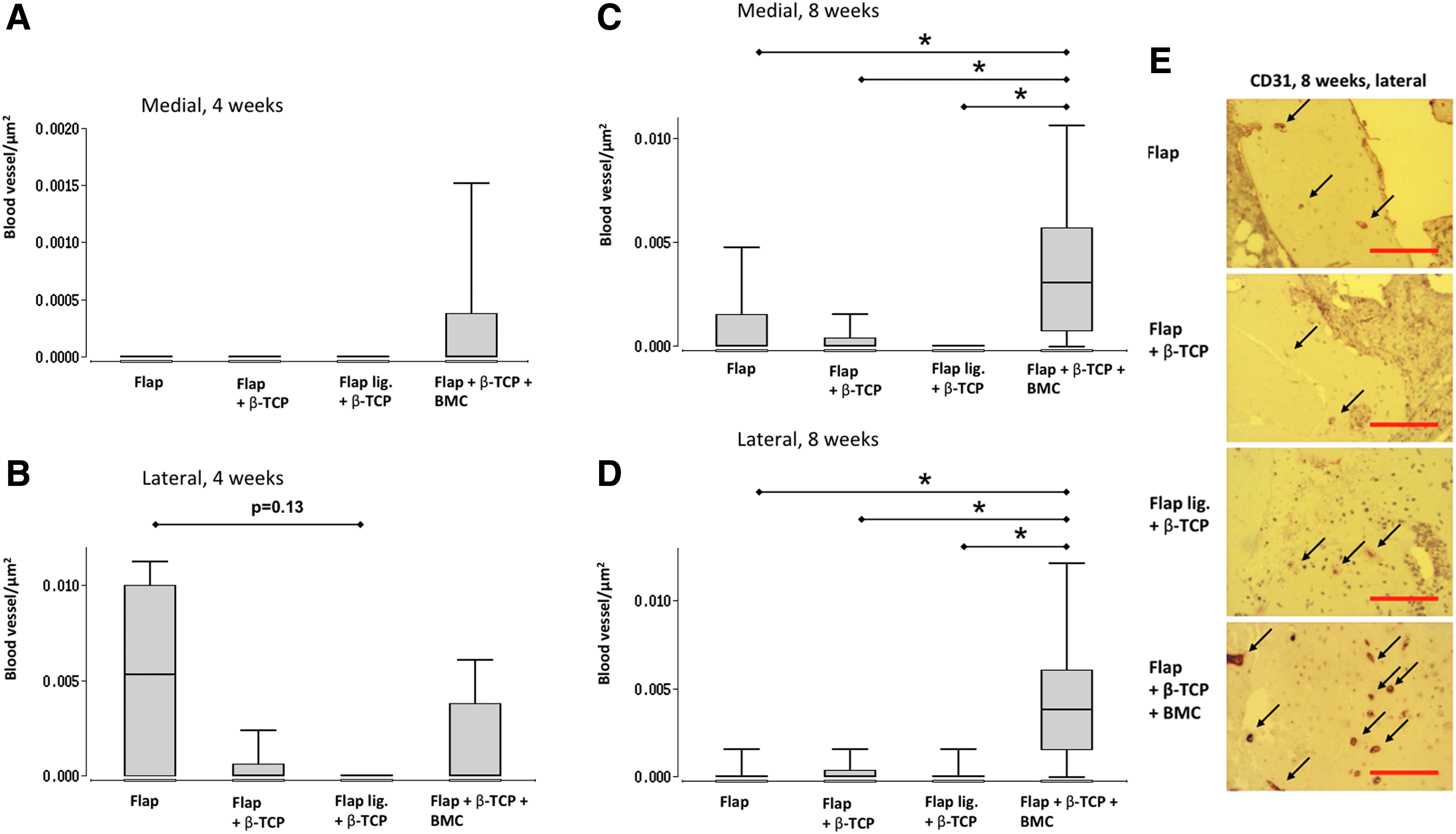
Vascularization of the defect zone as measured by Immunohistology with CD31 staining. Blood vessel density was analyzed on the medial and lateral aspect of the femur defect at
We also compared the results of this study with those of a former study entitled “Bone marrow-derived mononuclear cells (BMC) improved bone healing of large bone defects in rats” by Seebach et al. 27 In the previous study we used the same protocol with the same testing machines compared to our current study but without the periosteal flap. Bone stiffness was found to be clearly higher with the vascularized periosteal flap (median = 42 N vs. 29 N) in contrast to using β-TCP seeded with BM-MNCs alone.
In summary, in this study we combined a conventional, vascularized flap method with a still experimental, cell-based tissue engineering approach. The critical blood supply, afforded by the flap added to the osteoinductive and osteoconductive properties provided by the β-TCP scaffold seeded with BM-MNC, was the best combination tested for promoting bone healing, in our model. As new tissue-engineering treatments proposed and introduced into the clinical arena it is important to not lose sight of benefits that conventional, time tested methods have, and can continue to contribute to the development of these new treatments.
Footnotes
Acknowledgments
This project was funded in part by a LOEWE Center for Cell and Gene Therapy Frankfurt grant from the Hessian Ministry of Higher Education, Research, and the Arts [Ref No.: III L 4-518/17.004 (2010)] and the Friedrichsheim Foundation (Frankfurt, Germany).
Disclosure Statement
No competing financial interests exist.