
Abstract
Sustained release of bone morphogenetic protein (BMP)-2 by heparin-contained biomaterials is advantageous for bone tissue regeneration using low-dose BMP-2. However, its effect with high-dose BMP-2 is still unclear and should be clarified considering the clinical use of a high dose of BMP-2 in spine and oral surgery. This study aimed to evaluate the efficacy of a heparin-conjugated collagen sponge (HCS) with high-dose BMP-2 delivery by investigating in vivo initial osteogenic regulation and bone healing over 12 weeks in comparison with that of an absorbable collagen sponge (ACS). The in vitro BMP-2 release profile in the HCS exhibited a lower burst followed by a sustained release of BMP-2, whereas that of the ACS showed an initial burst phase only. As a result of a lower burst, the HCS-BMP group showed higher expression of bone-forming/resorbing markers and enhanced activation of osteoclasts than the ACS-BMP group within the scaffold of defect after 7 days, which is presumed to be because of retention of relatively higher amounts of BMP-2. However, the surrounding calvariae were less resorbed in the HCS-BMP group, compared with the aggressive resorptive response in the ACS-BMP group. Microcomputed tomography and histology revealed that HCS-BMP guided more effective bone regeneration of central defect over time inducing minor ossification at the defect exterior, whereas ACS-BMP exhibited excessive ossification at the defect exterior. These results showed that HCS-mediated BMP-2 delivery at a high dose has advantages over ACS, including less early resorption of surrounding bone tissue and higher efficacy in compact bone regeneration over a longer period, highlighting a clinical feasibility of this technology.
Introduction
T
A variety of biocompatible carrier systems for BMP-2 include collagen-based scaffolds, polymers, hyaluronic acid, fibrin, and ceramics. The absorbable collagen sponge (ACS) and synthetic bone substitutes such as hydroxyapatite or beta-tricalciumphosphate are currently used clinically. ACS reconstituted from bovine tendon has provided a satisfactory delivery system for rhBMP-2, independent of the site of implantation. In addition, ACS is the first BMP-2 carrier approved by the FDA for treatment of several bone-related diseases, and it has been used in clinical trials.7,8 However, the low affinity of ACS for BMP-2 causes an initial burst release of rhBMP-2, resulting in an instant and explosive increase into surrounding tissue and undesired effects in the early healing phase.9,10
The different efficacy of carriers might be related to the BMP-2 release rates of each delivery system. 11 Winn et al. also showed that the release kinetics of a carrier system could influence the clinical effects of BMP-2. 12 High-dose application of rhBMP-2 causes diverse adverse effects, which include ectopic bone formation, 13 osteoclast activation, 14 cyst-like bone void formation, 15 severe swelling in the anterior cervical spine, 16 inflammation, 17 bone resorption,18,19 and excessive bone formation and bone at undesired sites (heterotopic ossification).20,21 Therefore, many methods have been used to induce sustained release of BMP-2 by loading a suitable amount, applying the appropriate binding affinity, or controlling processing conditions.5,22–25 Sustained release of BMP-2 controlled by the binding affinity of carriers using a biodegradable poly lactic-co-glycolic acid microsphere system showed faster and more complete bone healing in an animal model than immediate release. 26
Recent studies using heparin are very encouraging for BMP-2 applications.27–29 Heparin, which belongs to the glycosaminoglycan family, can also modulate the functions of heparin-binding molecules, including growth factors, adhesion molecules, and receptors through its affinity.30,31 Because BMP-2 has the basic N-terminal domains as a heparin binding site, BMP-2 release could be modulated through delivery by heparin-associated biomaterials. 32 Kim et al. reported that grafting heparin and immobilizing BMP-2 on Ti surfaces could promote osteoblast activity and inhibit inflammation. 29 Heparin-conjugated fibrin also showed potential as a BMP-2 carrier for bone regeneration, but its efficiency was controversial, depending on the BMP-2 dose or skeletal sites.33–35 Although there are studies using heparin conjugation on a collagen sponge for BMP-2 delivery, the potential of heparin-conjugated collagen sponge (HCS) has not yet been evaluated for high-dose BMP-2 in a critically sized defect.
This study aimed to investigate the capacity of HCS to control the complications associated with high-dose rhBMP-2 and to promote long-term bone regeneration. We fabricated HCS with three different concentrations of heparin, which was characterized in vitro for the BMP-2 release pattern. For each concentration of heparin, the osteogenic effect of HCS was compared with that of ACS for in vitro osteoblast differentiation, mineralization, and high-dose implantation of rhBMP-2 (40 μg/defect) in vivo. We evaluated the potential of HCS for suppression of resorbing activity, reduction of heterotopic ossification, and long-term enhancement of bone mass. Early resorbing activity was evaluated by assessing osteoclast activation and the expression of bone formation/resorption markers 1 week after implantation, within the defect area and in surrounding existing bone tissue. Bone regeneration was evaluated by analyzing bone parameters using microcomputedtomography (micro-CT) 4, 8, and 12 weeks after implantation in an 8-mm critical-sized rat calvarial defect model. Heterotopic ossification was determined by analyzing the total tissue volume (TV) and bone volume (BV) at the exterior area of the defect at 4 weeks.
Materials and Methods
Fabrication of HCS
ACS was fabricated by freeze drying a 1% (w/v) collagen solution (Dalim Tissen Co., Ltd., Seoul, Korea) in 0.1 M acetic acid (Junsei Chemical, Tokyo, Japan). Lyophilized collagen sponges were cross-linked with 20 mM 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide hydrochloride (EDC; Tokyo Chemical, Tokyo, Japan) in ethanol (Merck Millipore, Darmstadt, Germany) for 4 h. The cross-linked collagen sponges were washed out five times to remove residual EDC and ethanol. The collagen sponges were then relyophilized. For heparin immobilization, freeze-dried collagen sponges were soaked in 50 mM 2-(N-morpholino) ethanesulfonic acid hydrate (MES; Sigma, St. Louis, MO) buffer supplemented with 0.2%, 0.5%, and 1.0% (w/v) heparin (Wako Pure Chemical, Osaka, Japan), 20 mM EDC, and 7.8 mM N-hydroxysuccinimide (NHS; Sigma) for 2 h. The resulting collagen sponges were washed out and lyophilized. The collagen scaffolds were 8 mm in diameter and 1.5 mm in thickness for the calvaria defect model and in vitro characterization.
Determination of immobilized heparin
The amount of immobilized heparin was determined using toluidine blue. 36 After preparation of 10 mg heparinized collagen scaffold, the sponges were incubated with 5 mL of 0.04 wt% toluidine blue solution in 0.1 M HCl, 2 mg/mL NaCl, and 0.4 mg/mL toluidine blue O zinc chloride double salt for 4 h at room temperature, resulting in complexation of toluidine blue with heparin. Thereafter, samples were washed with distilled water (twice for 5 min). Subsequently, the scaffold was immersed in 5 mL of a 1:4 (v/v) mixture of 0.1 M NaOH and ethanol to dissolve toluidine blue complexed to heparin. The absorbance of the resulting solution was measured at 530 nm using a microplate reader. The amount of immobilized heparin was calculated from a calibration curve obtained from a heparin/toluidine blue complex after precipitate formation through mixture reaction of 0.04 wt% toluidine blue and various heparin concentrations (0, 2, 4, 8, 16, and 32 μg/mL).
In vitro rhBMP-2 release test
Each collagen matrix of ACS or HCS at heparin concentrations (0%, 0.2%, 0.5%, 1%) was incubated for 1 h at 37°C with 5 μg rhBMP-2 (Novosis®-Dent; BioAlpha, Inc., Seongnam, Korea). After 1 h, the rhBMP-2-loaded collagen sponges were soaked in 2 mL phosphate-buffered saline (PBS; Sigma) in sealed glass vials and then incubated at 37°C while shaking at 15 rpm. The entire incubation medium was collected after 12 h, 1, 2, 4, 7, 14, 21, and 28 days of incubation and replaced with an equal 2 mL volume of fresh PBS at each time point. The amount of rhBMP-2 was determined using a BMP-2 ELISA kit (RHF913CKX; Antigenix America, Inc., Melville, NY) according to the manufacturer's protocol. The initial amount of BMP (5 μg) was verified using the same ELISA kit. The cumulative release of BMP-2 was then expressed as a percentage of the initial loading amount.
Scanning electron microscopy
To investigate morphology and porosity, scanning electron microscopy (SEM) was performed on cross sections and surfaces of scaffolds. The sponges were coated with an ultrathin layer (300 Å) of gold/Pt in an ion sputter (E1010; Hitachi, Tokyo, Japan). The ultrastructure of the sponges was observed by scanning electron microscope (S-800; Hitachi).
Cell proliferation
Bone marrow mesenchymal stem cells (BM-MSCs) that were isolated from femurs and tibias of Sprague Dawley rats (male, 8–12 weeks) were seeded on ACS and HCS at a density of 5 × 104 cells per sponge. Rat BM-MSCs (rBM-MSCs) were cultured in Dulbecco's modified Eagle's medium (DMEM; Gibco, Waltham, MA) supplemented with 10% fetal bovine serum (Gibco) and 1% antibiotics (Gibco) at 37°C in 5% CO2. After 3, 7, and 14 days of culture, an MTT colorimetric assay was performed. The cells on the sponges were incubated at 37°C in 1 mL DMEM containing 10% MTT solution. After an hour, the solution was discarded completely and 800 μL of dimethyl sulfoxide (DMSO; Junsei Chemical) was added to the sponges. Using a microplate reader, the absorbance of DMSO from the sponges was measured at a wavelength of 570 nm.
Quantitative real-time reverse transcription–polymerase chain reaction
Total RNA was isolated from rBM-MSCs cultured on ACS and HCS using the RNeasy Mini kit (Qiagen, Valencia, CA) for mRNA extraction. Equivalent amounts of RNA were reverse transcribed for cDNA synthesis using an Omniscript RT kit (Qiagen). Then quantitative reverse transcription-polymerase chain reaction (RT-PCR) for alkaline phosphatase (ALP), osteocalcin (OCN), and osteopontin (OPN) was performed using a RT-PCR machine (Bio-Rad, Hercules, CA) using the QuantiTect SYBR Green PCR Kit (Qiagen). The PCR cycling was carried out under the following conditions: 15 s at 95°C, 30 s at 58°C, and 30 s at 72°C for 40 cycles after an initial denaturation step for 5 min at 95°C. Oligonucleotide primers for real-time RT-PCR were designed for product sizes under 200 bp using real-time PCR system Sequence Detection Software v1.3 (Applied Biosystems, Foster City, CA). The sequence of each primer is listed in Table 1.
Primers are designed according to rat sequence of each gene.
ALP, alkaline phosphatase; Cbfa1, core binding factor α1; NFATc1, nuclear factor of activated T cells; OCN, osteocalcin; OPG, osteoprotegerin; OPN, osteopontin; RANKL, nuclear factor kappa-B ligand; TRAP, tartrate-resistant acid phosphatase; VEGF, vascular endothelial growth factor.
For real time RT-PCR in vivo, the collagen sponges removed from the calvarial defect or the surrounding calvariae of sponges were separately washed with PBS and chopped into small pieces. After adding 0.5 mL of Trizol reagent (Invitrogen, Life Technologies, Carlsbad, CA) directly to the chopped sponge or bone, total RNA was extracted and then subsequently treated as described in the manufacturer's instructions. Oligonucleotide primers for real-time RT-PCR were designed for product sizes under 200 bp using real-time PCR system Sequence Detection Software v1.3 (Applied Biosystems), and their sequences are provided in Table 1. Fold differences of each gene were calculated for each treatment group using normalized Ct values of the housekeeping gene beta-actin, according to the instructions of Applied Biosystems.
Alizarin Red S staining
To assess in vitro mineralization, collagen-coated microplates were prepared by treating with 300 μL of 1% (w/v) collagen solution in 0.1 M acetic acid. After air drying, a fresh solution of 20 mM EDC in ethanol was added into the microplates for cross-linking of collagen for 4 h. This was then rinsed with PBS for five times. For heparin immobilization, 1 mL of 50 mM MES buffer supplemented with 1% (w/v) heparin, 20 mM EDC, and 7.8 mM NHS was added to the collagen-coated multiwell microplates for 2 h, which was followed by rinsing of the collagen-coated surface with PBS five times. BM-MSCs were cultured on collagen- or heparin–collagen-coated plates with osteogenic differentiation media containing 10 mM β-glycerophosphate (Sigma), 50 μg/mL ascorbic acid (Sigma), and 10 nM dexamethasone (Sigma) for 14 days and then were stained by Alizarin Red (Sigma). Cells were fixed with 10% formaldehyde for 15 min at room temperature and then washed three times with distilled water. Alizarin Red solution (2% w/v, pH 4.2) was added in each collagen-coated plate and cells were incubated for 20 min. Then, excess dye was removed by washing four times with distilled water.
Von Kossa staining
BM-MSCs were cultured on ACS or HCS with osteogenic differentiation media containing 10 mM β-glycerophosphate (Sigma), 50 μg/mL ascorbic acid (Sigma), and 10 nM dexamethasone (Sigma) for 28 days and then were treated with von Kossa staining. Cells-loaded scaffolds were fixed in 10% formaldehyde solution overnight and washed with deionized water. The fixed scaffolds were stained either directly or histologically. Direct staining was followed by incubation with 5% silver nitrate solution for 1 h in the dark and rinsed with deionized water. After rinsing with deionized water, the scaffolds were then incubated with staining solution (5% sodium thiosulfate) for 5 min. The mineralization of the sponges was observed by Leica DMi1 light microscope (Leica Microsystem, Wetzlar, Germany). For histological staining, the scaffolds were then dehydrated in 70% ethanol and embedded in paraffin. Decalcified paraffin sections were cleaned for 10 min with xylene and stained as already mentioned. Digital images of the stained sections were collected using a transmission and polarized light Axioskop microscope, Olympus BX51 (Olympus Corporation, Tokyo, Japan).
Preparation of rhBMP-2-loaded scaffold
Escherichia coli-derived rhBMP-2 powder (Novosis-Dent; BioAlpha, Inc.) was dissolved at a concentration of 5 mg/mL with stabilizing buffer obtained from the manufacturer. The collagen sponges were 8 mm in diameter and 1.5 mm thickness for the calvarial defect model. rhBMP-2 (40 μg) was rapidly loaded onto each scaffold before in vivo implantation in a total volume of 30 μL, which was filled with buffer solution for the rest volume, and controlled at an amount that did not exceed 0.1% of the total scaffold volume. For control experiments, the scaffold was loaded with the same buffers used to dissolve rhBMP-2.
Surgery
Eight-week-old Sprague Dawley rats (total n = 80) were used. The experimental protocol was approved by the Animal Care and Use Committee of Seoul National University. After disinfection of the calvarial skin with 10% betadine (Potadines; Samil Pharm, Seoul, Korea) and subcutaneous injection of 2% lidocaine containing 1:100,000 epinephrine (Lidocaine HCL Injs.; Yuhan, Seoul, Korea), an incision was made along the sagittal suture. The periosteum was elevated and an 8-mm-diameter calvarial bone defect was created with a trephine burr without dural perforation. An rhBMP-2-loaded collagen sponge was then implanted into the defect area. The experimental groups were divided into ACS and HCS groups, and then these two groups were treated with buffer (ACS or HCS, n = 20/each group) or rhBMP-2 (40 μg/defect) (ACS-BMP or HCS-BMP, n = 20/group). Rats in each group were evaluated for RT-PCR and tartrate-resistant acid phosphatase (TRAP) staining 1 week after implantation (each n = 5), and were analyzed after 4- (each n = 5), 8- (each n = 5), or 12-week (each n = 5) healing periods using micro-CT and histological observation to evaluate new bone formation. A calvarium containing an 11-mm radius around the defect from each group was removed 7 days after surgery and separated into collagen sponges and the surrounding calvariae adjacent to the defect. Then, each area was cut in half for RT-PCR analysis and TRAP staining.
TRAP staining
Collagen sponges were implanted onto 8 mm critical sized defects of rat calvariae. After 7 days, whole calvariae including the collagen sponge were removed. Half of each sponge was fixed and decalcified before paraffin embedding. Tissue sections were deparaffinized, dehydrated, and then cut vertically into 5-mm-thick pieces. Tissue sections were stained for TRAP activity to examine osteoclastogenesis as follows. TRAP staining buffer was prepared by dissolving Naphthol AS-MS phosphate disodium salt (5 mg/mL) in 10% formalin, followed by addition of Fast Red Violet LB salt (1 mg/mL; Sigma). Slides were incubated with TRAP staining buffer for 30 min at 37°C, washed for 15 min in tap water, and then immediately stained with hematoxylin and eosin (H&E). After dual staining with TRAP and H&E, the slides were mounted with Crystal/Mount solution. The number of TRAP-positive multinucleate cells (MNCs), which have more than three nuclei per cell, was counted using ImageJ software (NIH, New York, NY) after capture of representative 40× fields under a phase microscope for whole sections of each group.
Immunohistochemical staining
Rankl and Opg expression in vivo were observed 7 days after implantation. The collagen sponges were removed and decalcified through incubation in ethylenediaminetetraacetic acid solution (7%, pH = 7.0) for 3–4 days (the solution was changed on day 2). The specimens were then dehydrated in 70% ethanol and embedded in paraffin. Ten paraffin sections were cleaned for 10 min with xylene, and the deparaffinized sections were treated with an undiluted serum solution for 30 min. Specimens were then incubated with anti-RANKL (1:200; Novus Biologicals, Littleton, CO) or anti-Opg (1:1000; Abcam, Cambridge, England) at 4°C overnight. After incubation, the sections were incubated with R.T.U biotinylated universal antibody using Vectastatin kit (Vector Laboratories, Burlingame, CA) according to the manufacturer's instructions. Staining was detected with diaminobenzidine (Sigma) substrate, and slides were mounted with Crystal/Mount (Biomeda, Foster City, CA). Images of stained cells were captured by bright field microscopy.
Micro-CT analysis
After sacrifice of animals 4 or 8 weeks postsurgery, each calvarium containing a collagen sponge was removed from the skull. New bone formation was analyzed for two regions; one region included only the real defect, whereas the other included both the real defect and the defect exterior. All calvariae were fixed in 10% formalin for 1 week. Micro-CT scans were then taken to quantitatively evaluate new bone formation using the Sky-Scan 1172® Microfocus X-ray System (SkyScan) with CT software, including CTAn 1.8®, CTvol, and NRecon Reconstruction® (SkyScan). The SkyScan 1172 microfocus X-ray system is equipped with a microfocus X-ray tube with a focal spot of 2 mm, producing a cone beam that is detected by a 12-bit cooled X-ray camera CCD that is fiber-optically coupled to a 0.5 mm scintillator. The resulting images were 1000 × 1000-pixel square images and an aluminum filter was used to produce optimized images. Reconstructions and analyses were performed using NRecon reconstruction and CTAn 1.8 software, respectively. A second-order polynomial correction algorithm was used to reduce the beam-hardening effect for all samples.
To measure newly formed bone, a circular area of predefined size was selected as the region of interest (ROI) in two-dimensional images. The pixel zone representing ossification in the defined ROI was then reconstructed in 3D by creating a volume of interest (VOI) in the lower and upper ranges of the threshold using grayscale units. After using CTAn 1.8 on each reconstructed BMP file, BV, TV, trabecular number (Tb.N), trabecular thickness (Tb.Th), trabecular spacing (Tb.Sp), and the relative ratio of BV/real defect were obtained using a CT-analyzer in 3D based on a surface-rendered volume model according to the manufacturer's instructions. To measure bone mineral density (BMD), attenuation data for ROI or VOI were converted to Hounsfield units and expressed as a value of BMD using a phantom (SkyScan). This phantom contained rods of calcium HA (CaHA) with a standard density corresponding to mouse or rat bone, which ranges from 0.25 to 0.75 g/cm3. BMD values were expressed in grams per cubic centimeter of CaHA in distilled water. A zero value for BMD corresponded to the density of distilled water alone (no additional CaHA), and a value greater than zero corresponded to nonaerated biologic tissue.
Histological staining
After micro-CT reconstruction, the operative field of each calvaria was removed and decalcified through incubation in ethylenediaminetetraacetic acid solution (7%, pH = 7.0) for 3–4 days (the solution was changed on day 2). The specimens were then dehydrated in 70% ethanol and embedded in paraffin. Decalcified paraffin sections were cleaned for 10 min with xylene and stained with H&E and Masson's trichrome (MT) for the detection of cells and bone structures, respectively. Digital images of the stained sections were collected using a transmission and polarized light Axioskop microscope, Olympus BX51 (Olympus Corporation).
Statistical analysis
All data are presented as means ± standard errors of the mean for in vitro tests, or as standard deviations for in vivo animal experiments. Statistical analyses were performed using IBM SPSS statistics 22.0 software (IBM, Armonk, NY). Groups were compared using a one-way ANOVA or two-way ANOVA using Bonferroni's test. Differences with p < 0.05 were considered significant.
Results
In vitro rhBMP-2 release
HCS was prepared with multiple heparin concentrations (0.2%, 0.5%, and 1.0%) to determine the appropriate dose. ACS that contained no heparin was used as a control. In vitro release kinetics of rhBMP-2 from HCS and ACS and the biological properties of HCS were compared over 28 days (Fig. 1A). The cumulative release of rhBMP-2 from 0.2%, 0.5%, and 1.0% HCS was 27.0%, 30.4%, and 32.9% (all, p < 0.05) in 1 day, compared with 57.1% from ACS. All types of HCS showed a low burst release pattern of rhBMP-2, which corresponded to 54.3–67.3% of the loaded rhBMP-2 over a period of 28 days. ACS had an initial burst, releasing more than 90% of the rhBMP-2 within 4 days. All HCS concentrations exhibited sustained release of rhBMP-2 for 28 days, indicating that HCS could stably control rhBMP-2 release for a longer time than ACS. The amount of rhBMP-2 released from HCS differed slightly based on heparin concentration; the 1.0% HCS showed the lowest level of cumulative release during the first 4 days.
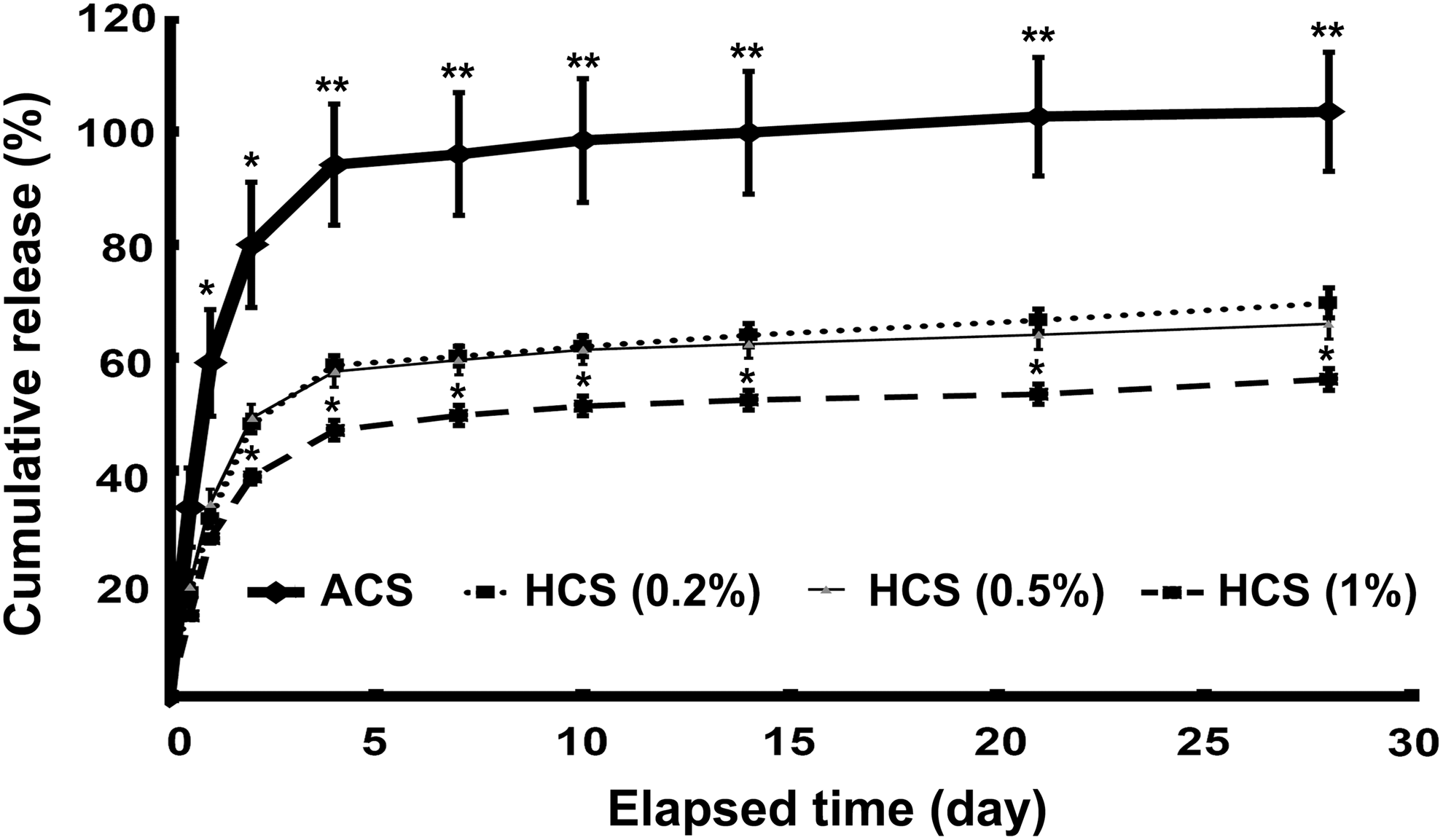
In vitro release of BMP-2 at 5 μg dose from ACS and HCS at different heparin concentrations (0.2%, 0.5%, and 1%) over a 28-day period. The amount of rhBMP-2 was determined with a BMP-2 ELISA kit. The cumulative release of BMP-2 was then expressed as a percentage of the initial loading amount. There was a significance in the difference in the amount of rhBMP-2 between ACS and each HCS at all time points (*p < 0.05, **p < 0.01); between 1% HCS and 0.2% or 0.5% HCS from day 2 (*p < 0.05). ACS, absorbable collagen sponge; BMP, bone morphogenetic protein; HCS, heparin-conjugated collagen sponge; rhBMP-2, recombinant human BMP-2.
Characterization and bioactivity of HCS
Immobilization of heparin to collagen in HCS was determined using a toluidine blue assay (Fig. 2A). The amount of immobilized heparin increased with increasing heparin concentration, although the fraction (%) of incorporated heparin to initial heparin declined as the heparin concentration increased. The percentage of incorporated heparin was 16.0%, 13.4%, 12.2%, and 6.8% with concentrations of 0.2%, 0.5%, 1.0%, and 2.0% heparin, respectively. The actual amount of immobilized heparin increased with increase in heparin concentration; however, there was not much of a difference in the actual amount incorporated from 1.0% to 2.0% heparin. Preliminary animal studies using 1% heparin sponge showed low efficiency compared with a scaffold control in an osteoinductivity test (shown in Supplementary Figure S1; Supplementary Data are available online at www.liebertpub.com/tea). Based on the in vitro release BMP-2 test and preliminary animal test, further in vitro and in vivo studies were performed using HCS with an initial heparin concentration of 0.5%.
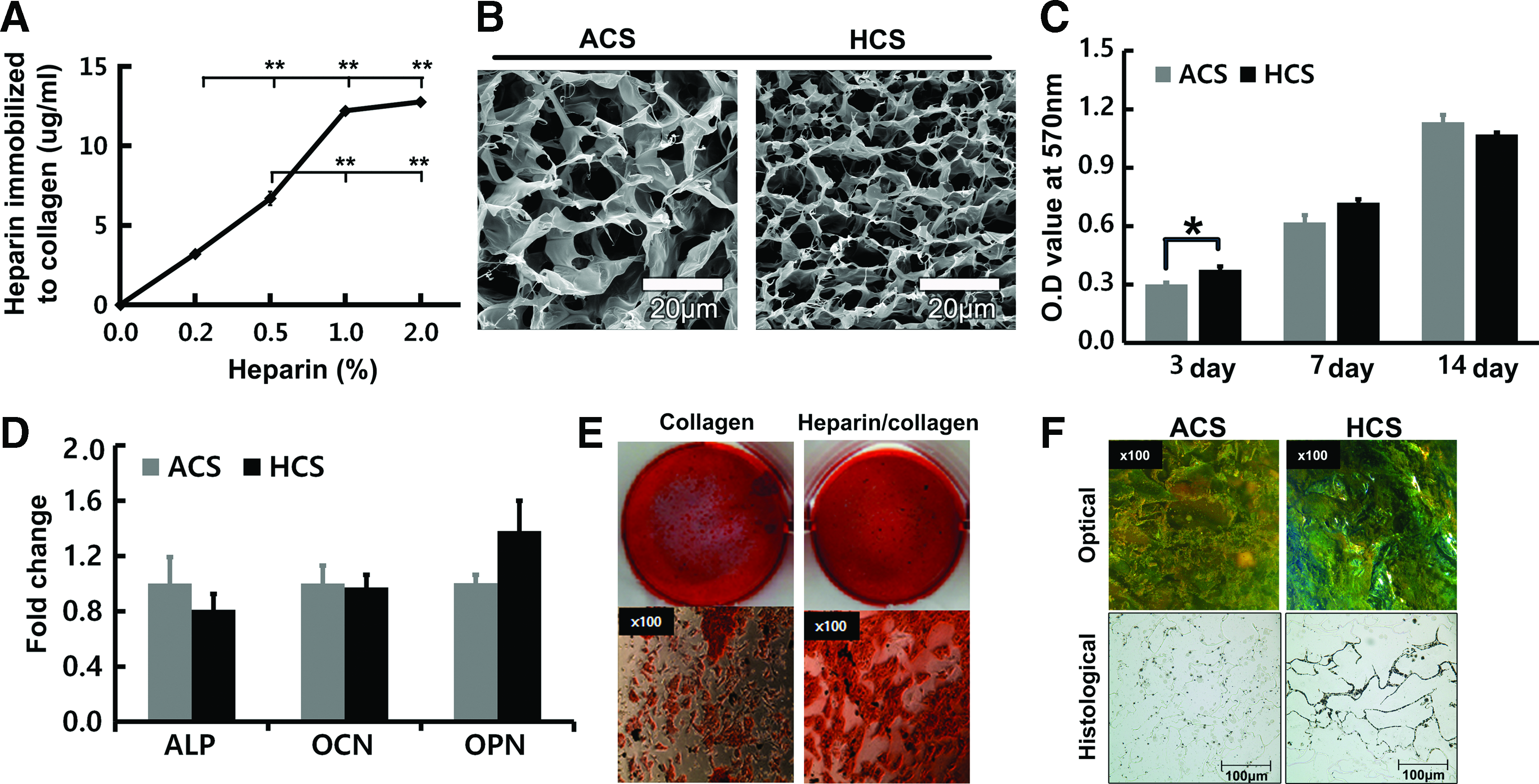
Characterization and bioactivity of HCS.
HCS with 0.5% heparin was characterized in vitro by SEM, MTT assay, real-time PCR, and Alizarin Red S staining. SEM photographs revealed that average pore diameters on the surface differed significantly between ACS and HCS. The HCS pores were 0.75- and 0.77-fold smaller than ACS pores on the surface of the sponges (Fig. 2B). Proliferation of BM-MSCs was 1.3-fold higher (p < 0.05) on HCS than ACS at 3 days, but there was no significant difference at 7 and 14 days (Fig. 2C). There was little difference (p > 0.05) in the expression of osteogenic marker genes (ALP, OCN, and OPN) in BM-MSCs cultured both on ACS and HCS (Fig. 2D). In vitro mineralization of BM-MSCs was examined both by Alizarin Red S staining on heparin/collagen-coated plates at day 14 and von Kossa staining on collagen sponges at day 28 (Fig. 2E, F). Alizarin Red S staining in heparin-coated plates showed more intensive staining than in collagen-coated plates. In von Kossa staining, cells cultured both on ACS and HCS were well mineralized, but direct microscopic observation showed a similar tendency as the test on the plate, in which cells on HCS built more densely mineralized nodules than those on ACS.
Early osteogenic regulation of HCS-BMP in vivo
We examined the early osteogenic process after the implantation of rhBMP-2 near the collagen sponge-implanted defect and the surrounding calvariae to examine the local and peripheral effects of BMP-2 release in vivo. The gene expression of bone-forming and bone-resorbing markers was examined by real-time PCR 1 week after rhBMP-2 implantation. We investigated early bone resorption by assessing RANKL and OPG expression, calculating the relative ratio of RANKL to OPG (R/O), and counting the number of TRAP-positive MNCs (Figs. 3B and 4B). rhBMP-2 increased RANKL expression in HCS and ACS at the defect area, although it increased 14.9-fold in HCS (p < 0.01) and 2.4-fold (p < 0.01) in ACS over each vehicle control (Fig. 3A, B). However, RANKL expression in the surrounding calvariae showed a consistent 6.5-fold increase (p < 0.05) in ACS-BMP, whereas it was slightly increased without significance in HCS-BMP.
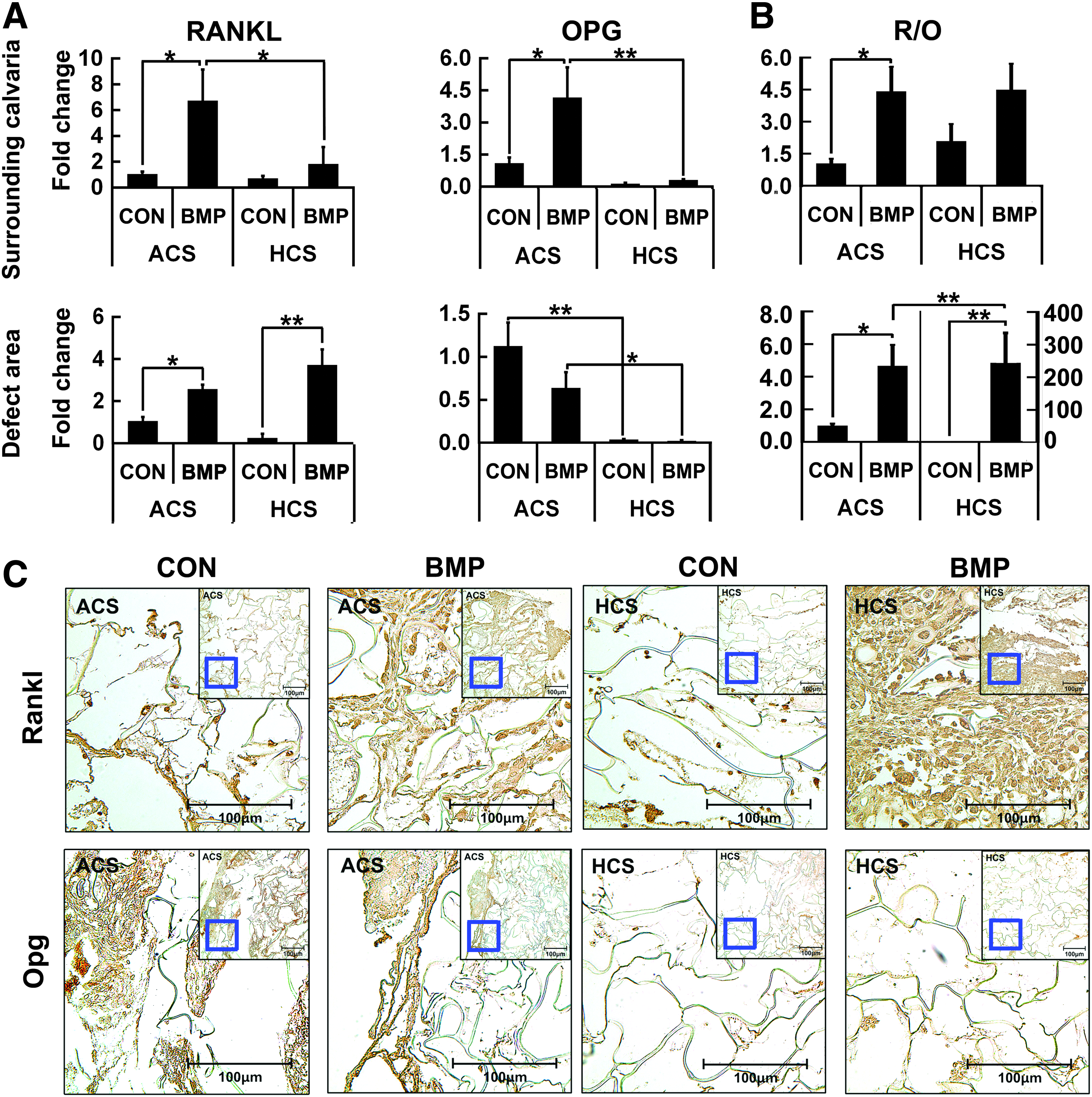
RANKL and OPG expression at the initial phase of high-dose rhBMP-2 delivery using ACS and HCS. Calvariae containing an 11-mm radius around the defect from vehicle alone (CON) and rhBMP treatment (BMP) of ACS or HCS were removed 7 days after surgery and separated into collagen sponges and the surrounding calvaria adjacent to the defect. Then, total RNA was extracted from the collagen sponge or bone of each group.
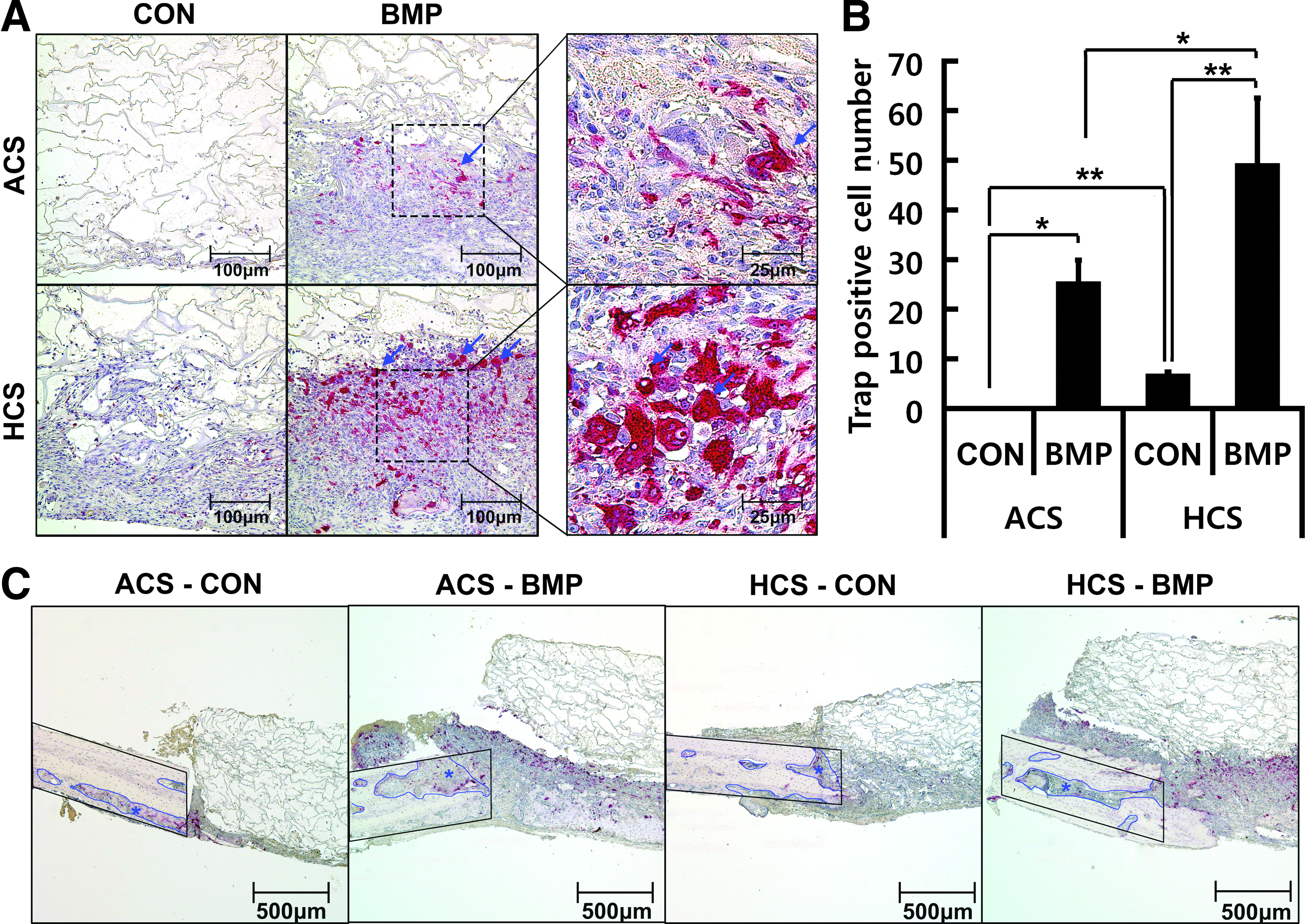
Early bone resorption in the ACS-BMP and HCS-BMP groups. A calvaria containing an 11-mm radius around the defect after vehicle alone (CON) and rhBMP treatment (BMP) of ACS or HCS was removed at 7 days after surgery and stained with TRAP and H&E.
OPG expression exhibited a different response to rhBMP-2 between the defect area and the surrounding calvariae. The expression of OPG was reduced by rhBMP-2 in the defect area in ACS-BMP and HCS-BMP. In particular, OPG expression in HCS alone was significantly reduced (p < 0.01) over ACS alone in the defect area. BMP-2 increased OPG expression 3.8-fold (p < 0.05) in ACS in the surrounding calvariae compared with the vehicle control. However, HCS-BMP did not change OPG expression compared with the HCS control, and the level was even less than ACS alone, although the difference in OPG level between ACS alone and HCS-BMP was not significant. As OPG expression in HCS showed lower levels, the resulting increased fold of R/O ratios of HCS-BMP and ACS-BMP over each control differed significantly, with a 145.0-fold (p < 0.01) and a 4.7-fold (p < 0.05), respectively, in the defect area; therefore, the HCS-BMP group showed a 51.9-fold (p < 0.01) higher level in the increasing rate of R/O than the ACS-BMP group. In the surrounding calvariae, ACS-BMP and HCS-BMP had a similar R/O ratio. ACS-BMP showed a 4.3-fold (p < 0.05) increase in R/O ratio over the ACS control, but the increased value of the R/O ratio of HCS-BMP was not significant. Immunohistochemical staining for Rankl and Opg was consistent with real-time PCR data for RANKL and OPG expression in the defect area (Fig. 3C).
TRAP-positive MNCs, which have more than three nuclei per cell, were counted as an index of osteoclast activation (Fig. 4). Consistent with our previous study, ACS-BMP increased the number of TRAP-positive MNCs to about 25.6, whereas the ACS control showed almost zero counts (Fig. 4A, B). However, the number of TRAP-positive MNCs in the HCS vehicle control was about 7.0, whereas HCS-BMP had 49.4 MNCs, which was 1.9-fold higher (p < 0.05) than ACS-BMP. We observed bone erosion at the margin of the defect scaffold in the ACS-BMP and HCS-BMP groups, which is probably caused by initial BMP-2 release (Fig. 4C). The existing bone at the scaffold margin showed an irregular bone surface and activated osteoclasts in both BMP groups, whereas the ACS and HCS groups without rhBMP-2 showed a relatively sharp defect margin around the scaffold. The total marginal area of necrotic bone in the ACS-BMP group was greater than that of the other groups including the ACS-control or HCS-BMP, indicating that ACS might cause aggressive release of rhBMP-2.
Next, we examined the expression of osteoblast activation-related markers (ALP, osterix, VEGF, and Cbfa1) and osteoclast activation-related markers (TRAP, cathepsin K, c-fos, and NFAT-c1) in the defect area and the surrounding calvariae (Fig. 5). The expression of these genes was similar to RANKL or OPG expression. ACS-BMP significantly increased the expression of bone-forming and bone-resorbing genes both in the defect area and the surrounding calvariae, except for ALP and c-fos. The HCS-BMP group showed different trends between bone-forming genes and bone-resorbing genes, especially in the surrounding calvariae. The expression of bone-forming genes (osterix, VEGF, and Cbfa1) in the HCS-BMP group was not changed compared with the HCS control, except for the ALP gene (p < 0.01) that was induced in the surrounding calvariae. Resorbing markers (TRAP, c-fos, and NFAT-c1, all p < 0.01) were all upregulated over the HCS control, with the exception of cathepsin K. As seen in RANKL expression, HCS-BMP in the defect area increased the expression of most bone formation- and resorption-related markers (ALP, osterix, and Cbfa1; NFAT-c1 and cathepsin K, all p < 0.01), and HCS-BMP increased their expression more than ACS-BMP.
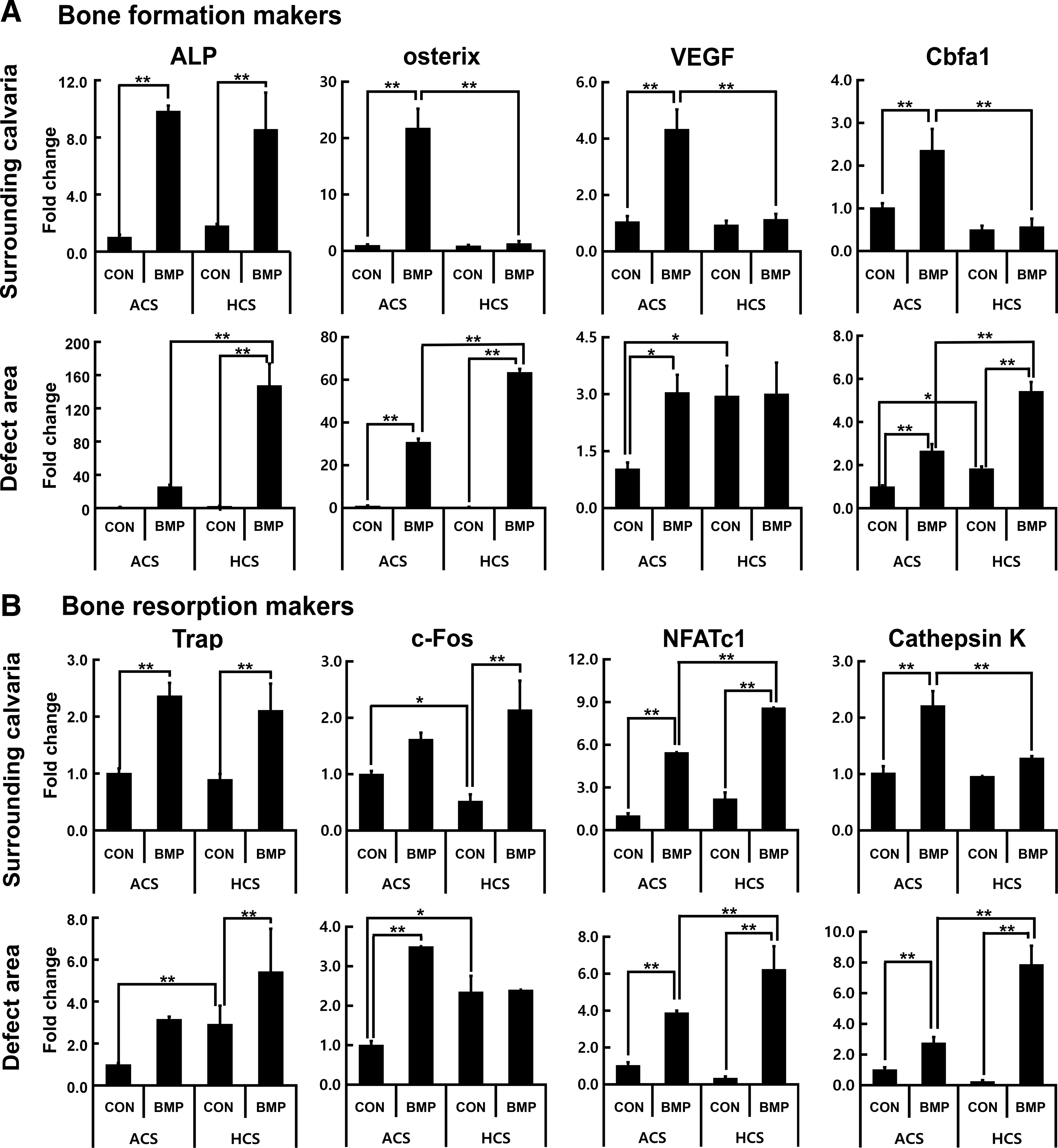
The effect of rhBMP-2 on the expression of bone formation-related markers and resorption-related markers in vivo. Total RNA was prepared from the collagen sponges removed from the calvarial defect or the surrounding calvariae of sponges 1 week after surgery as described in the Materials and Methods section. Real-time RT-PCR analysis was performed for
Comparison between HCS-BMP and ACS-BMP in bone regeneration in vivo
We chose an extremely high dose (40 μg/mL) for an 8 mm defect in rats to imitate a supraphysiological dose in clinical therapy. Bone regeneration was evaluated after a 4-, 8-, and 12-week healing period using micro-CT and histological staining (Figs. 6–8 and Table 2). Micro-CT-based evaluation was performed to analyze new bone formation at two areas of the central defect and outside the defect area. We assessed the central defect area to evaluate how efficiently HCS guides new bone formation within this targeted defect area. In addition, we assessed excessive bone formation at the defect exterior to evaluate whether HCS could minimize bone formation outside the defect as an index for heterotopic ossification.
Significance between ACS-CON and ACS-BMP or between HCS-CON and HCS-BMP at each time point, *p < 0.05, **p < 0.01.
ACS, absorbable collagen sponge; BMD, bone mineral density; BMP, bone morphogenetic protein; BV, bone volume; HCS, heparin-conjugated collagen sponge; Tb.N, trabecular number; Tb.Sp, trabecular spacing; Tb.Th, trabecular thickness; TV, tissue volume.
In the central defect area, the ACS-BMP and HCS-BMP groups showed significant increases over the control vehicle group in bone parameters, including BV/real defect volume, Tb.N, and BMD (Fig. 6). On the contrary, the Tb.Th of the ACS-BMP and HCS-BMP groups was reduced (Fig. 6C and Table 2). The Tb.Sp of HCS-BMP and ACS-BMP groups was reduced at 8 and 12 weeks, meaning a denser structure over vehicle control (Fig. 6E and Table 2). HCS-BMP group exhibited higher values of BV/real defect volume and Tb.N by 31% (p < 0.05) and 61% (p < 0.01) at 8 weeks and by 23% (p < 0.05) and 34% (p < 0.01) at 12 weeks, respectively, over ACS-BMP, whereas the difference between these groups was minor at 4 weeks (Figs. 6D and 7B). ACS and HCS without BMP-2 showed few differences.
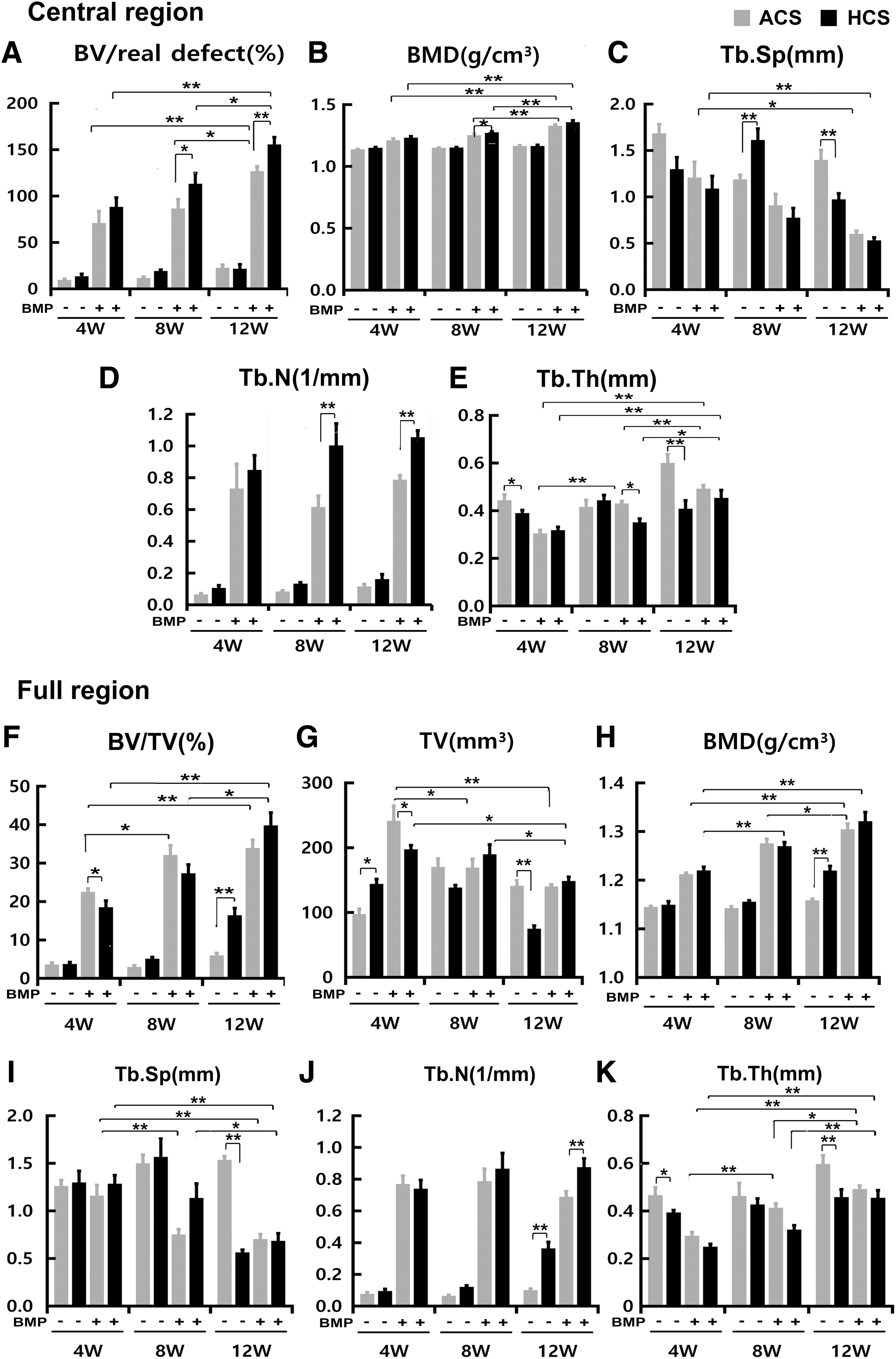
Quantitative micro-CT analysis of the effects of BMP-2 delivery from ACS and HCS on bone formation in rat calvariae defects. The experimental groups were implanted with ACS or HCS disks of buffer-loaded control (ACS-CON and HCS-CON) or rhBMP-2-treated disks (40 μg/defect; ACS-BMP, HCS-BMP). Micro-CT-based evaluation for new bone formation was performed for two regions after a 4-, 8-, or 12-week healing period; one region is the real defect

Comparison of the effect of HCS-BMP and ACS-BMP on heterotopic ossification or bone regeneration.
Heterotopic ossification was determined by measuring TV and BV at the full region. The TV of the ACS-BMP and HCS-BMP group showed a 147% and 37% increase (both, p < 0.01) compared with each vehicle control at 4 weeks (Fig. 6G). However, the TV of the ACS-BMP group significantly declined between 4 and 8 weeks, whereas the TV of the HCS-BMP group was nearly equivalent at the same period. There was minor change in TV between 8 and 12 weeks in both BMP groups. As the TVs showed a decreasing tendency with passage of time, the BV/TV of ACS-BMP group gradually increased with time despite similar values during whole period (Figs. 6F and 7C).
In full region, the BV of the HCS-BMP group was 0.7-fold lower (p < 0.01) at 4 weeks, equivalent at 8 weeks, and 1.2-fold higher (p < 0.01) at 12 weeks than that of the ACS-BMP group. However, Figure 7D shows that half new bone formation of ACS-BMP occurred at defect exterior at 4 weeks, whereas the bone formation at defect exterior of HCS-BMP group was minor. The ACS-BMP group had an 8.2-fold higher value in excessive BV outside the defect than the HCS-BMP group, but this declined over time and completely disappeared at 12 weeks (Fig. 7D). For HCS-BMP, excessive bone, which was one-eighth of ACS-BMP at 4 weeks, temporarily increased to about 50% of the level of ACS-BMP at 8 weeks, although the excessive bone completely disappeared at 12 weeks. This transient increase in bone formation at 8 weeks is probably because of sustained release of BMP-2 and the resulting osteogenic capacity of HCS.
Micro-CT images showed that all animals implanted with both HCS-BMP and ACS-BMP had bony union in the defect region (Fig. 8A). Histological observation using MT-stained sections was consistent with micro-CT-based evaluation (Fig. 8B). New bone formation outside the defect area in the vertical section was observed in both the ACS-BMP and HCS-BMP groups. The central defect space in the HCS-BMP group was more densely filled with new mineralized bone than that in the ACS-BMP group over the whole period. Successful union with existing calvarial bone was detected in both the ACS-BMP and HCS-BMP groups, although there was bone erosion at the margin of the defect at 7 days. In addition, HCS-BMP resulted in less excessive bone formation outside the defect than ACS-HCS did, indicating less heterotopic ossification in the HCS-BMP group. At 12 weeks, HCS-BMP showed a compacted bone structure whereas ACS-BMP resulted in remodeled regenerated bone that was less compact than HCS-BMP.
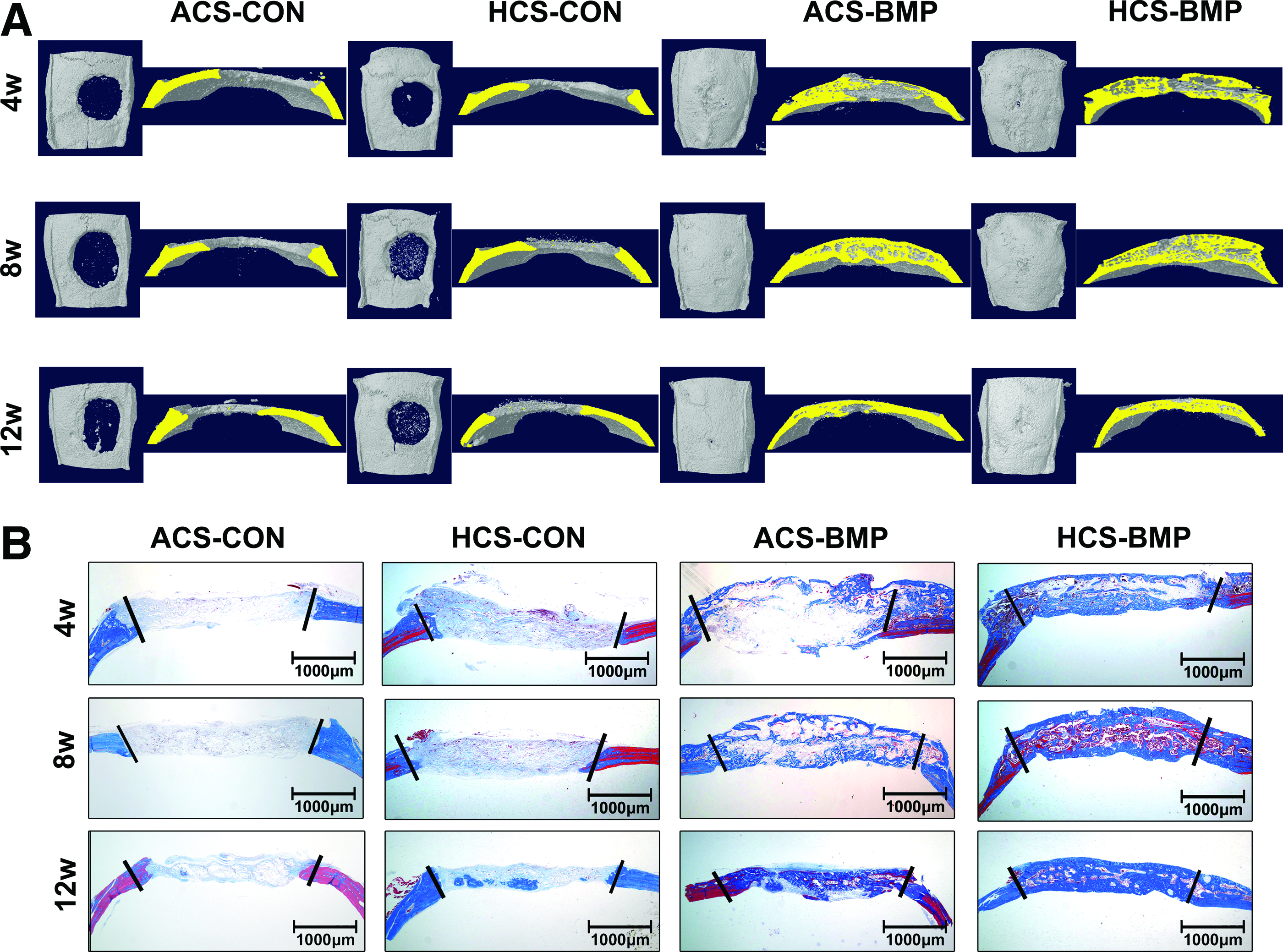
Three-dimensional reconstructed images and histological staining of regenerated defects.
Discussion
To achieve successful outcomes in BMP-2 therapy, current investigations have focused on developing a smart delivery vehicle to control BMP-2 release and finding appropriate doses of BMP-2 in skeletal sites. Although an initial burst has a negative effect, a recent report suggested that a sufficient burst followed by a sustained release is more favorable for efficient bone formation than only a high burst with no sustained release. 27 Nevertheless, controlled release of BMP-2 might be critical for patient safety if severe postoperative swelling occurs in the treatment of alveolar bone healing.37,38 Because this poor stability arises in high BMP-2 dosing, scientists have developed a variety of alternatives associated with established bone grafts or scaffolds to avoid initial burst and induce sustained release.23–26
Heparin-associated delivery enhances bone formation at low doses of BMP-2. 33 However, there is no evidence for heparin application with a collagen sponge for high-dose BMP-2, which is critical for clinical applications. We evaluated the potential of HCS as an alternative high-dose rhBMP-2 delivery vehicle. We investigated the ability of HCS to overcome clinically relevant and undesired effects induced by high-dose BMP-2 and to enhance short- and long-term bone formation through controlled BMP-2 release.
Despite successful bone formation outcomes without immune rejection in vivo, ACS showed an initial burst release of BMP-2 similar to other kinds of scaffolds. 16 Heparin shows binding affinity for BMP-2 and slowly releases it from the matrix in vivo. 39 To take advantage of this, we manufactured HCS using three different concentrations of heparin. Although we intended to test 40 μg of BMP-2 in animal experiments, in vitro release profiles of BMP-2 were assessed at lower 5 μg to avoid an experimental error in ELISA because the initial released amount of rhBMP-2 when 40 μg is loaded would be above the detection limit of the ELISA. The in vitro BMP-2 release data shown in this study may not agree with in vivo release rates, because they are expected to be faster because of enzymatic activities. 40
Because of this expectation, we used the in vitro release test of BMP as a reference test to determine whether a heparin collagen sponge is able to attenuate the initial burst of BMP compared with a collagen sponge. Thus, a 5 μg dose of BMP-2 was sufficient for this objective. An in vitro BMP-2 release profile revealed that the HCS exhibited a lower burst followed by a sustained release phase for BMP-2, whereas the ACS released most BMP-2 within the first 4 days. Our manufactured HCS successfully immobilized BMP-2, leading to release of BMP-2 in a controlled manner, like other heparin-conjugated materials.27,41–43 Recent studies using heparin-conjugated fibrin or hydrogel showed controversial results that were dependent on BMP-2 dose or ectopic versus orthotopic bone formation.9,35,44 This is a unique study that has directly compared ACS and HCS in high-dose BMP-2 delivery for clinical applications. Johnson et al. reported that precomplexed BMP-2 and heparin may be more effective than a collagen/heparin matrix at a low dose of BMP-2 in bone regeneration of femoral defects. 44 Although we concluded that a collagen/heparin matrix is ineffective when used for low-dose BMP-2 delivery, HCS was effective in high-dose BMP-2 delivery.
The rat calvarial defect model is most commonly used to determine bone regeneration capacity in response to certain stimuli, but its results have limited applications for patients. When determining the appropriate heparin concentration for bone regeneration, a 1% concentration of heparin had the most consistent results and a higher heparin incorporation and lower initial burst than 0.5% heparin. However, we selected 0.5% heparin for animal studies because of the lower efficiency of osteoinductivity when using a 1% heparin collagen sponge in preliminary animal experiments (shown in Supplementary Fig. S1). We chose a dose of 40 μg in an 8 mm defect to imitate a supraphysiological dose in human patients because 5 μg is a sufficient dose to fill a defect of this size completely at 4 weeks.10,45 By implanting an overdose of BMP-2, we intended to evaluate the clinical feasibility of HCS. However, calvaria defects in rodents do not normally undergo swelling as a critical side effect, which sometimes occurs when a supraphysiological dose of rhBMP-2 is applied in alveolar bone regeneration. Instead, we examined other side effects that can be observed in the rodent model. These include early transient bone resorption, excessive bone formation, and bone at undesired sites, also called heterotopic ossification. 21
We analyzed the capacity of HCS to efficiently deliver high-dose BMP-2 in three ways. First, we evaluated its ability to suppress early bone resorption induced by BMP-2. The early osteogenic response was examined 7 days after BMP-2 administration in the central defect area and the surrounding calvaria because we hypothesized that different release profiles of HCS-BMP and ACS-BMP might be reflected in the early osteogenic process in these two regions. The influence on the surrounding calvaria is important because previous reports warned that rhBMP-2 delivered in a collagen sponge for metaphyseal fracture repair should be avoided because of severe transient bone resorption of surrounding tissue induced by a supraphysiological dose of rhBMP-2. 19
The initial osteogenic process accompanied the simultaneous amplification of bone formation and resorption during bone regeneration in a BMP-2-loaded scaffold in the defect area. 10 In addition, the absence of a BMP dose-dependent increase in bone mass was attributed to concurrent bone resorption and formation. We used double the concentration of BMP-2 (40 μg), which resulted in a higher number of activated osteoclasts than the previous study (data not shown). As expected, the early osteogenic process in bone formation and resorption was correlated with the in vitro release profile of BMP-2 from HCS and ACS. Within the defect area, the HCS-BMP group had greater bone resorption indices, including TRAP-positive MNC number, R/O ratio, and cathepsin K expression, than the ACS-BMP group, probably because of a lower initial burst and higher long-term BMP-2 levels. However, the surrounding calvaria showed the opposite; the ACS-BMP group had greater bone resorption indices than the HCS-BMP group. Moreover, the HCS-BMP group had significantly increased activated osteoclasts on the scaffold than the ACS-BMP group at the defect area, which was correlated with the R/O ratio. Although the HCS-BMP and ACS-BMP groups showed no difference within the scaffold because of greater osteoclast activation, the use of HCS might be beneficial because HCS alleviates the exposure of surrounding tissue to the rhBMP-2 burst, resulting in relatively weakened bone necrosis. As already mentioned, HCS probably effectively diminishes the potential risk of high-dose rhBMP-2 use for metaphyseal fracture repair better than ACS. 19
The expression of bone forming markers (ALP, osterix, and Cbfa1) trended with bone resorption indices both in the defect area and in surrounding calvariae in the ACS-BMP and HCS-BMP groups, respectively. VEGF expression was also induced in ACS-BMP group and HCS group, compared with ACS group. The increase in VEGF expression with rhBMP-2 treatment indicates enhanced angiogenesis, which is a critical prerequisite for promoting bone formation, suggesting that rhBMP-2 application enhances both angiogenesis and osteoblast differentiation during early phase healing. 46 It is reported that heparin binds to VEGF and stimulates VEGF signaling by binding to the VEGF receptor, leading to enhanced angiogenesis. 47 VEGF has a heparin binding domain; however, the effect of heparin on VEGF expression has not been clearly established. Our results showed that VEGF expression was increased in HCS to a level similar to ACS-BMP even without BMP-2. This topic would be interesting to examine further in future studies.
The more rapid release of rhBMP-2 from ACS may stimulate an increased response in the surrounding calvariae when compared with the HCS, which controlled the release of rhBMP-2 better. Higher BMP-2 concentrations in the defect area in the HCS-BMP group may stimulate a more aggressive response of infiltrated cells to BMP-2. This result was consistent with a carrier-dependent differential response to rhBMP-2, which is attributed to the release rate of rhBMP-2 from the carrier.19,48 In the initial response to BMP-2, HCS enhances bone formation in the defect area better than ACS, but this was counterbalanced by amplified bone resorption, finally leading to no difference in bone mass between the two groups.
OPG expression in vivo after high-dose BMP-2 implantation differed between the defect area and the surrounding calvariae, whereas RANKL expression showed a consistent increase in response to BMP-2 treatment. Opg, which was secreted from osteoblasts, reduced RANKL signaling as a decoy receptor for RANKL, which plays a critical role in the regulation of bone resorption.49,50 rhBMP-2 induces OPG expression in murine cells in vitro.51,52 In contrast, our previous study revealed that high-dose rhBMP-2 reduced OPG expression at the defect area in vivo and in rat mesenchymal stem cells in vitro. 10 In addition, OPG expression was reduced by BMP-2 both in human mesenchymal stromal cells and human osteoblasts. 53 In this study, in vivo OPG expression was also significantly reduced in the defect area in ACS-BMP over ACS alone, consistent with our previous study. 10 In addition, OPG expression in HCS alone and HCS-BMP was minor compared with that of ACS alone in the defect area, consistent with reports that heparin can enhance osteoclastic bone resorption by inhibiting OPG binding activity. 39 As a result, the R/O ratio in the HCS-BMP group at the defect area was enormously increased, which was consistent with a greater level of osteoclast activation than ACS-BMP.
TRAP staining consistently showed abundantly distributed osteoclasts within the defect area, and this increased significantly in the HCS-BMP group. However, BMP-2's effect on OPG expression was completely different between the surrounding calvariae and the bone defect. BMP-2 increased OPG expression in existing bone areas of the surrounding calvariae, whereas it did the opposite in the defect area, which undergoes new ossification. This difference can probably be attributed to differential BMP-2 concentrations caused by release kinetics or to the differentiated stage of cells localized in each tissue. Further study is necessary to confirm the effect of rhBMP-2 on OPG expression, depending on a diverse range of dosages of rhBMP-2 or time.
We then investigated the effect of HCS on heterotopic ossification 4 weeks after surgery. Heterotopic ossification occurs when a supraphysiological dose of BMP-2 is rapidly released, resulting in less compact bone formation at the desired site and excessive bone formation at undesired sites outside the original defect region. 21 Lateral growth of the newly formed bone was induced outside and inside the original defect area in BMP-2-treated scaffolds. Linde and Hedner showed that high-dose rhBMP-2 (10 μg) could induce excessive bone formation, spreading outside the original contour in rats. 20 rhBMP-2 may affect new bone formation differently inside and outside the membranes. 54 Therefore, the effect of the delivery vehicle on early heterotopic ossification, especially at high doses of BMP-2, might indicate the release rate of BMP-2.
We evaluated the effect of HCS on excessive bone formation by assessing new bone formation at the central defect only or in the full region including the central and exterior defect. Micro-CT-based evaluation showed little difference in new bone formation between HCS-BMP and ACS-BMP at the central defect at 4 weeks. This was probably because of greater bone resorption of HCS-BMP at the initial phase, which might counteract bone formation. ACS-BMP had much greater BV in the defect exterior than HCS-BMP when compared with the BV formed at the central defect. Although the excessive bone in the ACS-BMP group was rapidly remodeled and almost disappeared at 12 weeks, this result indicates a suppressive effect on excessive bone formation by HCS. Histological observation using MT-stained sections showed that total tissue and dead space within new bone tissue are definitely less in the HCS-BMP group over the whole period. This is probably caused by a lower burst and better controlled release of BMP-2, implying that HCS is able to alleviate early heterotopic ossification and may reduce adverse effects of an initial burst of high-dose BMP-2.
Finally, HCS was evaluated to determine whether sustained release of rhBMP-2 could continuously induce bone formation. Johnson et al. showed that heparin alone was incorporated in a collagen matrix to potentially sequester endogenous BMP-2 at the defect site. 44 However, our data did not show any difference between HCS and ACS alone in new bone formation, but demonstrated an excellent effect when exogenous BMP-2 was delivered by HCS. Many researchers expected that a heparin-mediated sustained release of BMP2 would increase bone formation in the long term. However, these systems have been mainly tested within 4 weeks and have not been evaluated over 12 weeks. Moreover, most studies used low-dose BMP-2 or an ectopic assay. A research group investigated the effects of heparin on long-term bone formation at 12 weeks, and reported that heparin addition failed to increase bone formation over a collagen sponge with or without low-dose BMP-2 (3 μg). 44 In contrast, our results showed that HCS was more effective than ACS at long-term formation of new bone at 8 and 12 weeks when used with high-dose BMP-2 (40 μg).
ACS-BMP showed trends similar to HCS-BMP, but formed excessive bone at the defect exterior more than at the central defect, which rapidly disappeared as time passed, implying bone remodeling. Bhakta et al. proposed that BMP-2 delivery from a collagen sponge after an 8-week observation of an ectopic assay relies mostly on desorption rather than on physical entrapment, 55 thus failing to sustain release if the collagen sponge is fully degraded. 9 However, the collagen sponge is almost degraded within 4 weeks, as shown by MT staining in the ACS-BMP and HCS-BMP groups. BMP-2 dosed with either ACS or HCS continued to form new bone in the implanted defect region at 8 and 12 weeks despite the degradation of the collagen sponge. Micro-CT and histological staining revealed that heparin-immobilized rhBMP-2 developed compact bone structure and exerted active osteogenic activity to form new bone more efficiently than a nonconjugated collagen sponge over 12 weeks.
Under in vivo conditions, the release of BMP-2 from collagen is reportedly more sustained, exhibiting a burst release followed by a sustained release until day 14. 56 Although we did not present in vivo pharmacokinetic data for BMP-2 from HCS and ACS, our in vivo data from 7 days to 12 weeks were consistent with the prediction derived from the in vitro release profile and reflected the estimate derived from lower initial burst and sustained release of rhBMP-2 from HCS. Improved long-term bone formation in HCS-BMP was presumed by sustained release of BMP-2 from HCS. However, HCS-BMP had slightly better effects on early osseous healing than ACS-BMP despite a greater level of bone resorption and formation, which was assumed by the lower initial burst and the resultant higher retention of BMP-2 on the scaffold. The half-life of exogenous BMP-2 rapidly declines. However, HCS- and ACS-delivered BMP-2 guided new bone formation over 12 weeks in the central defect, despite degradation of the bulk of the collagen sponge within 4 weeks. This indicates that a bound form of BMP-2 with heparin might form new bonds with endogenously formed extracellular matrix, which may allow it to be continuously active in vivo or protected from proteolysis. Taken together, the HCS used here may be advantageous for rhBMP-2 delivery at high doses and may reduce the associated safety concerns that counteract the benefits of BMP-2 in patients.
Conclusions
This study approached HCS-mediated BMP-2 delivery as an alternative to overcome limitations of high-dose BMP-2 application. We proved the advantage of HCS use in BMP-2 delivery on the basis that HCS induces a lower burst and subsequent sustained release of BMP-2. This led to less initial bone resorption at the surrounding bone tissue, alleviated early heterotopic ossification, and enhanced compact regeneration at the target bone defect over a longer period. However, HCS-BMP does not accelerate early osseous healing of the target area at 4 weeks, presumably because of a simultaneous increase in bone formation and resorption, despite the fact that HCS-BMP had a greater increase in bone-forming activity than ACS-BMP. These findings suggest that HCS is a useful alternative to lessen early adverse effects and continue bone formation over a longer period in the clinical use of high dose of BMP-2 in spine and oral surgery.
Footnotes
Acknowledgments
This research was supported by a grant from the Korea Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A120850). We thank Novosis® -Dent, BioAlpha, Inc. for providing the rhBMP-2.
Disclosure Statement
All other authors confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.