
Abstract
While significant progress has been made toward engineering functional cartilage constructs with mechanical properties suitable for in vivo loading, the impact on these grafts of inflammatory cytokines, chemical factors that are elevated with trauma or osteoarthritis, is poorly understood. Previous work has shown dexamethasone to be a critical compound for cultivating cartilage with functional properties, while also providing chondroprotection from proinflammatory cytokines. This study tested the hypothesis that the incorporation of poly(lactic-co-glycolic acid) (PLGA) (75:25) microspheres that release dexamethasone from within chondrocyte-seeded agarose hydrogel constructs would promote development of constructs with functional properties and protect constructs from the deleterious effects of interleukin-1α (IL-1α). After 28 days of growth culture, experimental groups were treated with IL-1α (10 ng/mL) for 7 days. Reaching native equilibrium moduli and proteoglycan levels, dexamethasone-loaded microsphere constructs exhibited tissue properties similar to microsphere-free control constructs cultured in dexamethasone-supplemented culture media and were insensitive to IL-1α exposure. These findings are in stark contrast to constructs containing dexamethasone-free microspheres or no microspheres, cultured without dexamethasone, where IL-1α exposure led to significant tissue degradation. These results support the use of dexamethasone delivery from within engineered cartilage, through biodegradable microspheres, as a strategy to produce mechanically functional tissues that can also combat the deleterious effects of local proinflammatory cytokine exposure.
Introduction
J
In clinical patients following acute ACL injury, 19 cytokines such as tumor necrosis factor α (TNF-α) and interleukin-1β (IL-1β) were significantly elevated from baseline 24 h after injury. At 1 week, while reduced, these cytokines remained elevated above chronic levels. Tsuchida et al. analyzed the synovial cytokine profiles of patients undergoing microfracture or autologous cell implantation (ACI) for focal defect repair 20 and observed increased concentrations of inflammatory cytokines in the synovial fluid of injured as compared with healthy joints. The increased presence of cytokines in injured joints may contribute to the inferior clinical results observed for ACI in some patients,21–24 as elevated levels of inflammatory mediators have previously been shown to hamper cartilage regeneration.25–27 To this end, data from animal studies and early clinical trials suggest that early inhibition of the intra-articular (IA) inflammatory response (e.g., 4 weeks) and posttraumatic injury of the knee may improve clinical outcomes. 28 Morisset et al. reported an improvement in cartilage repair following IA injection of an adenoviral vector carrying an IL-1ra gene, 29 indicating that modulation of the joint's chemical environment may be beneficial for chondrocyte and tissue health. 30
Palliative strategies for managing joint pain include anti-inflammatory analgesics such as nonsteroidal anti-inflammatory drugs alongside IA injections of glucocorticoids or hyaluronan. 31 IA glucocorticoid injections have proven effective in reducing pain in patients for up to 2 years with no deleterious effects to joint morphology. 32 A residence time of only 36–72 h, however, mandates that the concentration of injected solutions and suspensions be high, upwards of 2 mg/mL. 33 Rapid clearance from the joint space results in excess circulating glucocorticoids, which leads to increased susceptibility to viral infections and delayed wound healing34,35 systemically, as glucocorticoids are effective in suppressing IL-1β and TNF production by leukocytes. 36
Complementary to its use in IA injections, dexamethasone (dex), a synthetic glucocorticoid, has been reported to inhibit collagen degradation of cultured cartilage explants in response to interleukin-1α (IL-1α). 37 Work in our laboratory has found that engineered bovine cartilage constructs with native properties can be protected from the deleterious effects of IL-1α by culture supplementation with dex, in a manner similar to native cartilage explants.38–40 Additionally, preexposure to dex has been reported to prevent proteoglycan degradation and restore biosynthesis of cartilage explants exposed to TNF-α and mechanical injury. 40 Several in vivo studies have demonstrated the chondroprotective effects of dex as well. Repeated IA injection of high-dose dex, for instance, was observed to protect cartilage from damage in a lapine posttraumatic model of OA.41,42 Malfait et al. have demonstrated that dex inhibited proteoglycan degradation induced by IA injection of TNF-α. 43 While effective, the continuous administration of drug through IA injection is not recommended, as this increases the risk of infection and patient discomfort, emphasizing the need for sustained release formulations. 44
Recent work has exploited poly(lactic-co-glycolic acid) (PLGA) systems for the delivery of anti-inflammatory drugs.45–53 Higaki et al. demonstrated that the continuous administration of betamethasone sodium phosphate through PLGA nanoparticles provided increased inhibition of inflammation in an experimental model of OA when compared with the same dosage of betamethasone sodium phosphate delivered three times through IA injection. 54 Dang et al. demonstrated that dex releasing PLGA microparticles are capable of suppressing the host response to implanted polymer materials in a mouse model. Notably, animals that received a higher drug loading treatment suffered an increased incidence of death within 7–10 days after administration, while a low drug loading group maintained healthy body conditions, but still benefited from the drug's anti-inflammatory properties. 45 These studies demonstrate that locally delivered, low concentrations of anti-inflammatory steroids are capable of suppressing the local host response without the systemic impact observed with higher drug concentrations.
In the context of cartilage tissue engineering, our laboratory has broadly employed dex for its proanabolic and anticatabolic effects in cartilage tissue engineering systems, 55 its proven importance for cultivation of tissues with native properties, and its ability to confer chondroprotection against inflammatory cytokines.38,39,56,57 As these factors can impact clinical success of cartilage tissue engineering strategies, we sought to develop a more clinically focused cartilage tissue engineering approach utilizing the FDA-approved steroid dex. An ideal therapy would retain the benefits of dex on engineered cartilage without the requirement for its exogenous supplementation, obviating the systemic 58 and joint level complications associated with clinical injections of steroids.59,60 As such, the current study tested the hypothesis that the incorporation of PLGA microspheres (MS), with the ability to release dex from within chondrocyte-seeded agarose hydrogel constructs, would promote development of constructs with native mechanical properties and protect constructs from the deleterious effects of IL-1α, laying the foundation for future, clinically focused studies.
Materials and Methods
Experimental design
To assess the potential for chondroprotection through internally released dex, PLGA MS, loaded with the steroid, were embedded in the tissue construct during gelation (Fig. 1). Tissues were cultured in chondrogenic medium for 4 weeks before cytokine exposure to allow for sufficient tissue maturation. 61 Following 4 weeks of culture in a chondrogenic medium, a subset of these tissues were treated with supraphysiological levels of inflammatory cytokine for 1 week (Fig. 2). Following 1 week of treatment, tissues were evaluated for their mechanical and biochemical properties.
Representative schematic of the dex-loaded microsphere strategy employed in this study. PLGA microspheres are embedded alongside chondrocytes in an agarose hydrogel. In this way, dexamethasone is available locally to the cell to optimize the chondroprotective effects of the glucocorticoid against pro-inflammatory cytokines, such as interleukin-1 and tumor necrosis factor alpha. dex, dexamethasone; PLGA, poly(lactic-co-glycolic acid). Color images available online at www.liebertpub.com/tea

Microsphere fabrication and preparation
Dex-loaded PLGA MS were fabricated as described previously. 51 Empty MS were also prepared with the same method, omitting the dex. Before the experiment, 8 mg of dex-loaded and empty MS were weighed and sterilized through ultraviolet light. The release of dex was quantified spectrophotometrically at 242 nm. Ten milligrams of MS were placed in a microcentrifuge tube containing 1 mL of phosphate-buffered saline (PBS) (n = 3). At various time points, samples were centrifuged and releasates were collected and then frozen at −80°C until analysis. The amount of dex in each releasate was quantified by comparison with a standard curve.
Cell culture and sample preparation
Articular cartilage was harvested from stifles of freshly slaughtered 2- to 4-week-old calves. Three joints were used for the experiment and cells were pooled from all joints. Cartilage chunks were digested in 390 U/mL collagenase type IV (Worthington) for 11 h with agitation. Isolated chondrocytes were passaged in Dulbecco's modified Eagle's medium (DMEM) containing 10% fetal bovine serum, 1 ng/mL TGF-β1, 5 ng/mL FGF-2, and 1% antibiotics/antimycotics. Following two passages, cells were prepared for encapsulation in an agarose (type VII; Sigma) hydrogel. For MS-free controls (ctrl, ctrl+IL, ctrl−dex), chondrocytes were seeded at 30 × 106 cells/mL in 2% agarose. For MS-containing samples (dex-loaded [LMS], LMS+IL, and empty microspheres [ULMS]), 1.5 mL of concentrated cell solution was combined with previously prepared MS. This cell/MS suspension was combined with 1.5 mL agarose and cast between glass slides for a final concentration of 2.66 mg MS per milliliter and 30 × 106 cells/mL in a 2% agarose hydrogel. This concentration of MS was selected as it has been previously shown to positively impact biosynthetic activity of human adipose stem cells.
51
Cylindrical constructs (Ø4.0 × 2.34 mm) were cored and cultured in chondrogenic medium comprised of DMEM with 50 μg/mL
Cytokine insult
Following 28 days in growth culture, a subset of ctrl and LMS samples were subjected to 10 ng/mL IL-1α. IL-1α was added at each media change for 7 days. During this period, MS-free samples were starved of dex so as to isolate the potential impact of internally released dex in MS-loaded samples.
Mechanical characterization
A custom unconfined compression device was used to determine the equilibrium compressive modulus (EY) of whole samples at days 0, 14, 28, and 35 (n = 5). An initial 0.02 N tare load was applied, followed by compression to 90% of the unloaded sample thickness, at a strain rate of 0.05%/s. After relaxation, a 2% peak-to-peak sinusoidal strain was applied at 0.01 Hz. EY was evaluated from the equilibrium response of stress–relaxation curves. A custom glass-bottom device mounted on the stage of an inverted microscope63,64 was used to determine depth-dependent properties of ctrl and LMS samples on day 35. Before testing, samples were halved and maintained in a sterile PBS solution containing calcein-AM (Life Technologies). Following staining, samples were positioned with the cross-section facing the objective and initial measurements of thickness were performed digitally. Initial images of the cross-section were acquired, and the samples were then compressed at nominal 5% strain increments to a final compression of 15%. After each compression cycle, samples were allowed to equilibrate for 15 min, with images being acquired immediately before subsequent compression. Digital image correlation was used to obtain accurate axial and lateral strains,63,64 which were combined with incremental compressive loading data to determine depth-dependent mechanical properties.
Biochemical characterization
Samples were thawed, lyophilized, weighted dry, and digested with 0.5 mg/mL proteinase K in 50 mM Tris-buffered saline containing 1 mM EDTA and 1 mM iodoacetamide. DNA content was quantified using a PicoGreen assay (Life Technologies). Glycosaminoglycan (GAG) content was quantified using 1,9-dimethylmethylene blue dye-binding assay 65 with shark chondroitin-6-sulfate standards (Sigma). The digests were further hydrolyzed in 12 N HCl at 110°C for 16 h for quantification of total collagen content through orthohydroxyproline colorimetric assay. 66 The collagen and GAG contents were normalized to the construct wet weight. The swelling ratio was also determined from tissue volumes at each time point normalized to average day 0 tissue volumes. Tissue maturity was assessed qualitatively and quantitatively (ImageJ) through histology, before freezing, and day 35 samples were fixed in acid formalin ethanol. Following fixation, samples were then paraffin embedded, sectioned (8 μm), and stained with Alcian Blue (GAG) and Picrosirius Red (collagen).
Results
Microsphere fabrication and preparation
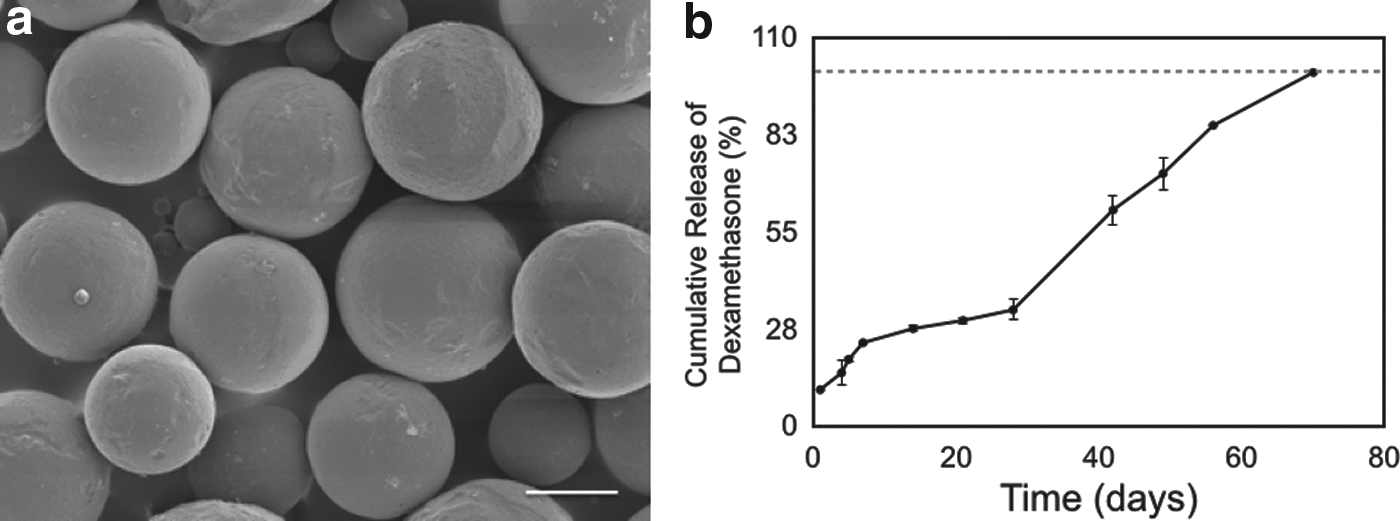
MS were observed through scanning electron microscopy (Fig. 3a) and determined to have an average diameter of 10 μm. A burst release of 10.2% ± 0.8% of initial dex content was observed after 24 h. A linear fit of subsequent release data (R2 = 0.97) yielded a daily release rate of 250 ng dex per milligram MS (Fig. 3b). After 28 days in culture, 32.8% ± 1.1% of dex had been released. The loading capacity was 19.9 ± 1.9 μg dex per milligram MS. These results have been confirmed through high-performance liquid chromatography.50,67
Bulk mechanical characterization
At day 0, there were no significant differences between MS and ctrl samples (4.8 ± 2.5 kPa vs. 2.7 ± 1.7 kPa). All groups displayed significant growth from day 0 to 28 (p < 0.05) (Fig. 4). By day 28, EY of all groups achieved ∼200 kPa (Fig. 4a). ULMS and ctrl−dex samples developed similarly to this time point, indicating minimal negative or positive impact from PLGA degradation. Following treatment with IL-1α, the equilibrium modulus of ctrl+IL tissues dropped significantly (p < 0.05). At day 35, ctrl tissues reached 527 ± 74 kPa, whereas ctrl+IL tissues dropped to 194 ± 98 kPa from 297 ± 101 kPa at day 28 (Fig. 4d). LMS tissues reached 387 ± 80 kPa at day 28. Following cytokine exposure, LMS+IL tissues continued to mature to 645 ± 136 kPa, similar to LMS tissues that grew to 717 ± 99 kPa at the same time point. ULMS tissues, those that received neither dex nor IL-1α, reached 269 ± 49 kPa by day 35. As a result of its inferior mechanical properties at day 35, ULMS tissues were excluded from analysis in Figure 4e and f.

Mechanical and biochemical development of tissue-engineered cartilage throughout culture. ctrl−dex is provided as a reference for the first 28 days of growth. ULMS tissues exhibited poor growth at day 35 and were not included in other metrics.
Depth-dependent mechanical characterization
MS remained visible in the tissue at day 35 (Fig. 5a). At day 35, strain distributions from both ctrl and LMS samples displayed tissue inhomogeneity consistent with previous work68,69 (Fig. 5b). While LMS tissues displayed a significantly higher (p < 0.05) local equilibrium modulus than ctrl in 67% of the thickness of the tissue, tissue inhomogeneity does not appear to be impacted by the local delivery of dex.
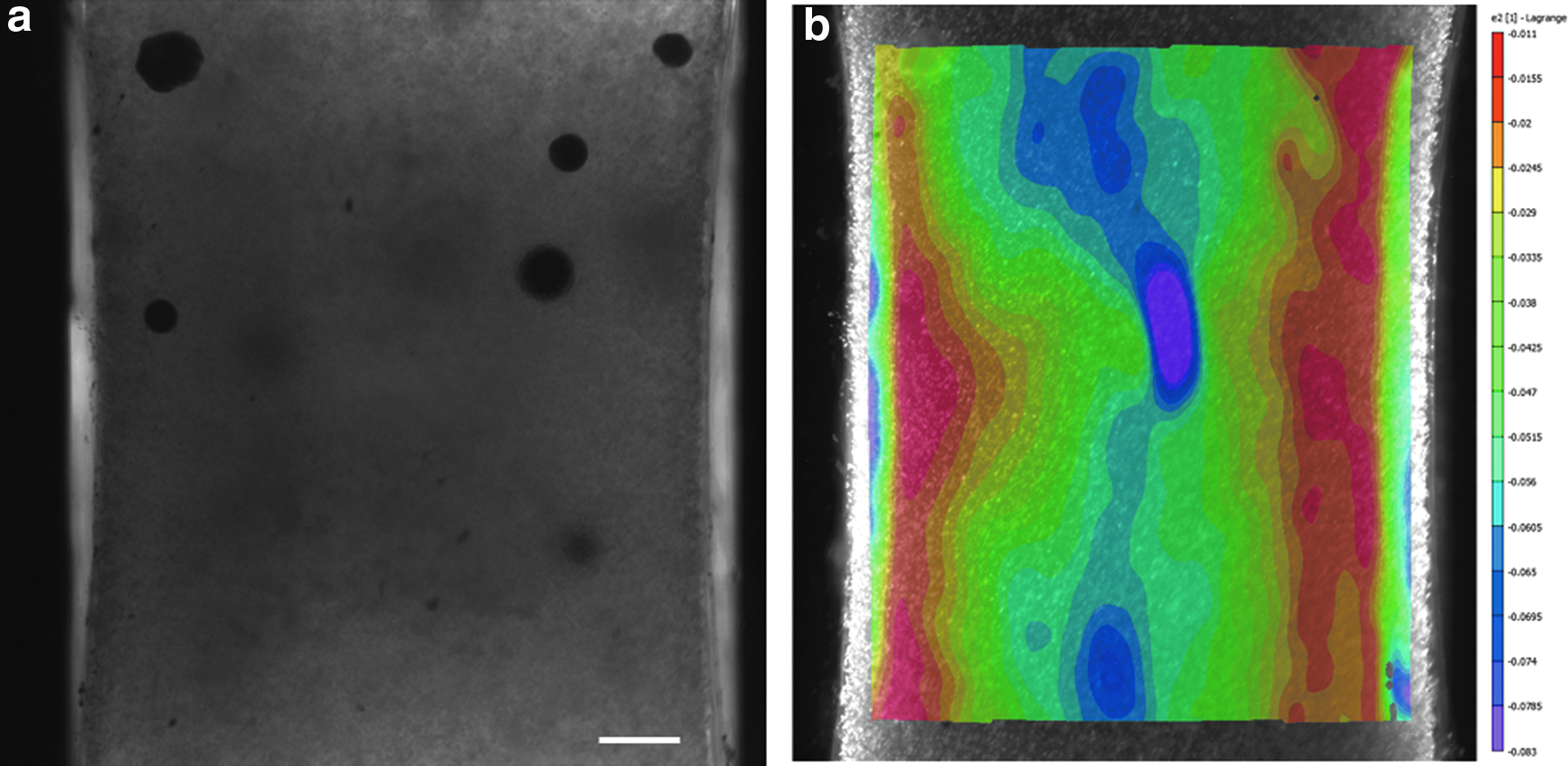
Cross-section of samples prepared for depth-dependent mechanical testing using a custom designed microscope testing device.
Biochemical characterization
Cellularity
The DNA content of all tissues increased throughout time in culture (Fig. 6a). At day 28, ctrl tissues contained 2.04 ± 0.20 million cells per construct. Following IL-1α treatment, the number of cells in ctrl+IL tissues was significantly lower (1.53 ± 0.19 million) compared to ctrl tissues (1.96 ± 0.23 million cells, p < 0.05). Similarly, LMS tissues contained 2.09 ± 0.17 million cells at day 28. Unlike ctrl+IL tissues, the cellularity of LMS+IL tissues was preserved at day 35 (1.92 ± 0.15 million cells) as compared to LMS samples (2.01 ± 0.10 million cells). Uniquely, by day 35, the number of cells in ULMS tissues increased to 3.49 ± 0.52 million cells per construct, a 2.76-fold increase above day 0 values.
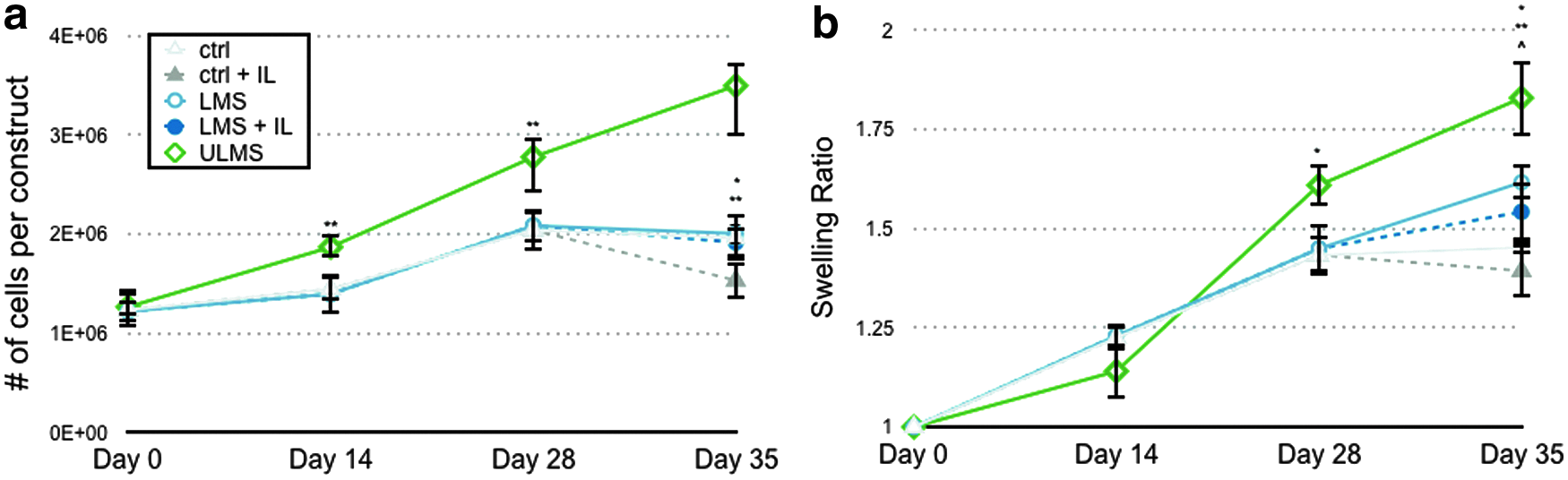
Cellular proliferation and tissue swelling throughout the entire culture period.
GAG incorporation
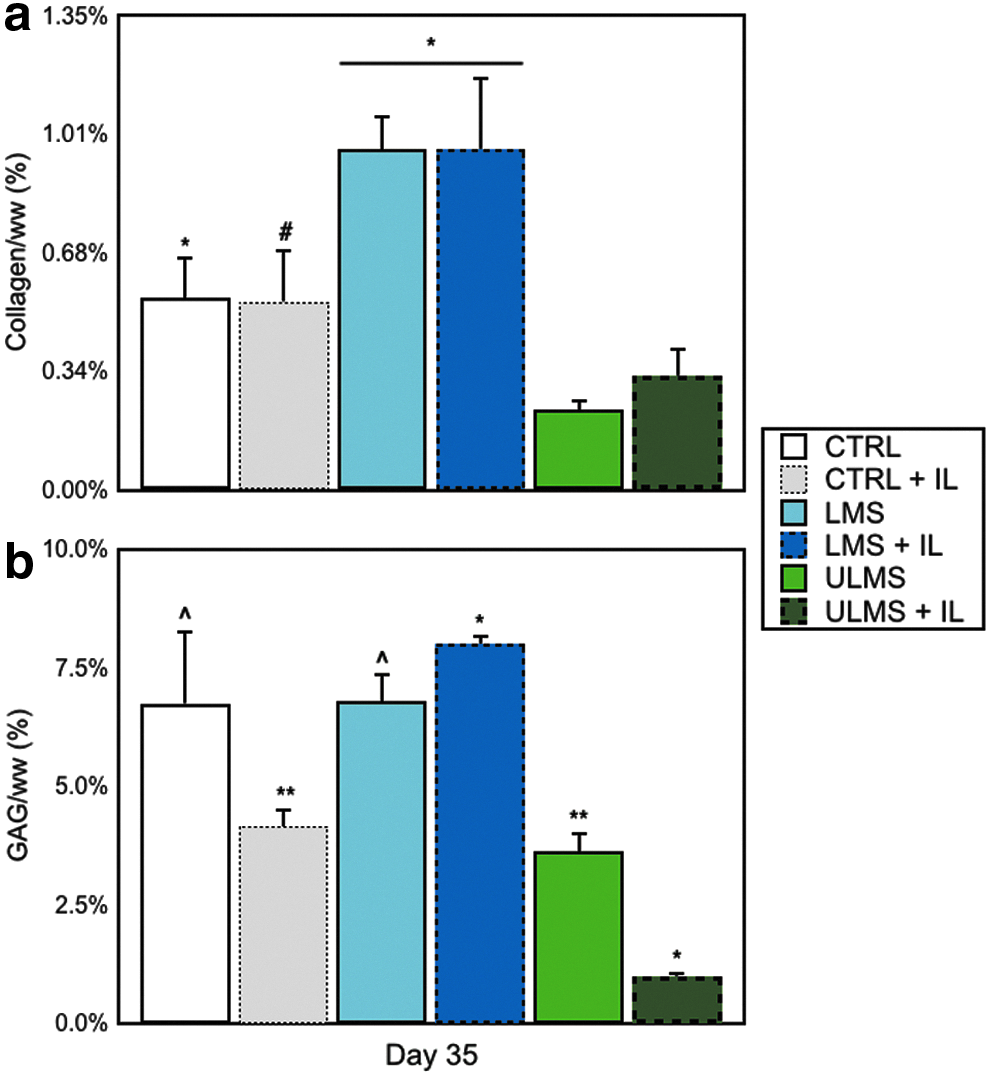
At day 28 in culture, all tissues contained at least 4.69% ± 1.07% GAG per wet weight (GAG/ww) (Fig. 4b). Following IL-1α treatment, GAG content of ctrl+IL samples (5.07% ± 1.15% GAG/ww) was significantly lower than respective controls (7.91% ± 0.46% GAG/ww, p < 0.05) (Fig. 4e). In contrast, LMS+IL tissues continued to grow following the initiation of cytokine treatment, reaching 9.29% ± 1.26% GAG/ww by day 35, similar to LMS controls that achieved 10.99% ± 1.32% GAG/ww at the same time point. ULMS tissues reached 7.65% ± 1.17% GAG/ww by day 35 in culture.
Collagen content
Collagen content of ctrl and LMS tissues reached 1.43% ± 0.33% collagen normalized to wet weight (collagen/ww) and 1.53% ± 0.34% collagen/ww, respectively, at day 28 (Fig. 4c). ULMS tissues contained 1.86% ± 0.18% collagen/ww at the same time point. Following cytokine insult, collagen content significantly decreased in ctrl+IL tissues (p < 0.05) when compared with ctrl, LMS+IL (Fig. 4f), and ULMS tissues.
Swelling ratio
All tissues exhibited significant swelling by day 35 in culture (Fig. 6b). ULMS displayed a significantly greater (p < 0.05) swelling ratio at day 35 when compared with all other groups, swelling to nearly 2× its original volume.
Histological/morphological characterization
Histology (Fig. 7a–i), through ImageJ analysis, indicates weaker staining for GAGs in ctrl+IL samples (Fig. 7b) when compared with other groups at day 35. Weaker intercellular staining was observed in ctrl+IL samples (Fig. 7f) at the same time point when compared with other groups. This response is contrasted with LMS+IL samples (Fig. 7d, h), which maintain the intensity of their staining following treatment with IL-1α.
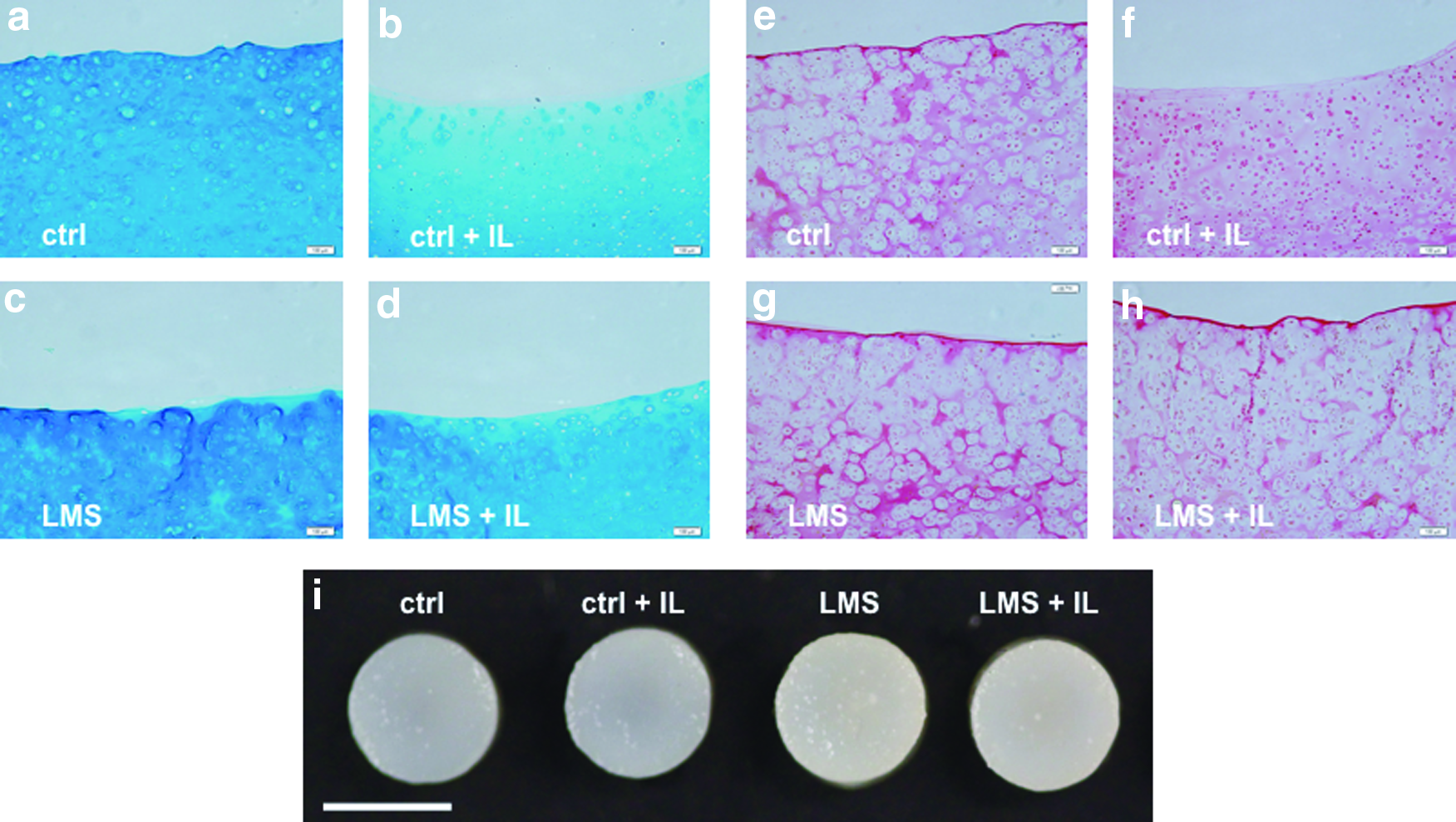
Histological sections from day 35. Alcian Blue staining indicates loss of GAGs following treatment with IL
Discussion
This study demonstrated that dex-loaded PLGA MS embedded in chondrocyte-seeded agarose hydrogels promote development of mechanically functional cartilage tissue in culture. This local dex-delivery system also provides chondroprotection against the deleterious effects of IL-1α, a ubiquitous cytokine known to play a major role in the innate immune response and articular cartilage degeneration.
By releasing dex from within engineered cartilage, our therapeutic strategy targets the complicated autocrine control system of chondrolysis, through which cartilage damage is triggered by proinflammatory cytokines produced from leukocytes and the synovium.70,71 Compared to strategies that target specific proinflammatory cytokines, such as IL-1 receptor antagonist,72,73 dex has been shown to mitigate the deleterious effects of IL, TNF-α, and other cytokines associated with inflammation. Once internalized, dex acts directly and indirectly by activating anti-inflammatory proteins,74,75 upregulating their production through glucocorticoid-responsive elements located on DNA,76,77 and by interfering with the translocation of other transcriptional factors, such as nuclear factor-kappa B.78,79
As a culture supplement, dex is known to perform a variety of roles, including as a promoter of chondrogenesis in mesenchymal stem cell populations.80–82 Additionally, as reiterated in this study, dex is a critical element in the development and maturation of tissue-engineered cartilage. Here, all tissues developed similarly for the first 2 weeks of culture (Fig. 4a), regardless of dex supplementation. Tissues receiving dex achieved an EY within the native range 83 by the end of culture and were ∼2-fold higher than tissues receiving no dex (ULMS) (Fig. 4d). Moreover, dex-loaded MS expedited this tissue development (day 35).
While delivery of dex from within constructs cultivates tissues with EY in the range of native values, the internal delivery of dex from homogeneously distributed MS was not observed to modulate the axial inhomogeneity of tissue properties reported in chondrocyte-seeded agarose constructs of similar dimensions. 68 This inhomogeneity can be described as a U-shape, with stiffer regions of tissue located at the periphery.84,85 (Fig. 5b), and is thought to reflect nutrient gradients associated with free-swelling culture. This finding suggests that dex is not responsible for the nonuniform tissue development observed in our current study. Recent work suggests that other media components, such as insulin and glucose, may play a role in this phenomenon.86,87 The high binding affinity of active TGF-β3, an ∼25 kDa molecule (compared with 400 Da for dex), to agarose and cartilage matrix has also been implicated in contributing some part to the development of tissue heterogeneity. 88
The EY values observed here are interestingly in tandem with cellular density and swelling ratio. With respect to cellularity, tissues that received no dex throughout the study (ULMS) proliferated to a cellular density ∼2.75-fold higher than those that did (ctrl, LMS) (Fig. 6a). The antiproliferative effects of dex seen here are consistent with work in 2D chondrocyte cultures. 89 While a higher cellularity yielded near-native GAG levels (∼7% GAG/ww, data not shown) and GAG levels comparable to those in ctrl tissues, EY remained significantly lower at the final time point (Fig. 4d), despite minimal variation in collagen content across tissue groups. Furthermore, ULMS tissues experience greater swelling and inferior mechanical properties compared to LMS, attributed to the absence of dex. We speculate that dex influences the biosynthetic behavior of chondrocytes that dictates the structural organization of the collagen network and collagen–proteoglycan interactions that serve to combat tissue swelling.6,90,91
In addition to the physical demands of the joint, its harsh inflammatory environment will likely impact the performance of engineered cartilage. The presence of IL-1β upregulates the expression of aggrecanases, the primary proteases identified in pathological aggrecan degradation in human OA, 92 and has a predominant effect on the GAG content of engineered cartilage. Previous studies have shown that GAG content of IL-1-treated engineered cartilage is depleted ∼4-fold as compared with controls. 38 It is also known, however, that dex supplementation reduces sulfated GAG loss and rescues proteoglycan synthesis in cartilage explants exposed to inflammatory cytokines. 40 In the study presented here, LMS and ctrl tissues were treated with IL-1α beginning at day 28 in culture. The time point selected for cytokine insult was informed by work in our laboratory and others suggesting that construct maturity plays an important role in the tissue's response to cytokine and in vivo outcomes,38,61,93 with delayed exposure to insult being beneficial to tissue health. Following 7-day treatment of IL-1α, ctrl+IL tissues contained ∼36% less GAG than their respective controls (Fig. 4e), resulting in an inferior tissue with equilibrium moduli measuring ∼2.75-fold lower than ctrl tissues. LMS tissues, however, did not experience a similar depletion of GAGs. In fact, LMS tissues exposed to cytokine continued to elaborate their extracellular matrix beyond day 28, increasing GAG content nearly 2-fold by day 35 (Fig. 4d). The continued biosynthetic activity of LMS tissues in the presence of a supraphysiological dose of IL-1α (10 ng/mL vs. 0.288 ng/mL 94 in moderate OA joints), compared with the significant decline in synthesis by ctrl+IL tissues, is encouraging in the context of using dex-loaded MS as a strategy to promote cartilage repair in vivo. 61
Recent work demonstrates the successful translation of this dex microsphere strategy to engineered constructs seeded with adult human chondrocytes 95 from three donors (Fig. 8), supporting the need for continued research efforts pursuing dex-loaded MS. Similar to constructs derived from juvenile bovine chondrocytes, coencapsulation of adult human chondrocytes and dex-loaded MS were able to promote cartilaginous tissue development similar to exogenous dex supplementation of the culture media and afforded chondroprotection against IL-1α.
GAG content from preliminary study using adult human chondrocytes. Chondrocytes were isolated from the femoral articular cartilage of three donors. Following casting at 40 million cells per milliliter in 2% agarose hydrogels, tissues were cultured as described previously. At day 28, samples were divided and a portion was treated with 0.1 ng/mL IL-1.
While simplistic, the use of a single proinflammatory cytokine, IL-1α, is a well-established culture model for OA38,40,71,72,96–98 proven to provide valuable insight on the impact of cytokines on articular cartilage. The use of IL-1, specifically, exploits the cytokine's importance in inflammation. 99 IL-1, along with TNF-α, is responsible for the majority of degradation of the extracellular matrix in vivo 100 and both cytokines share a common set of pathways, including the activation of nuclear factor-kappa B (NF-κB). 101 The utilization of dex is therefore unique, as glucocorticoids have been shown to physically interact with the p65 subunit of NF-κB and transrepress its function. 102 While anti-inflammatory cytokines such as IL-4 and IL-13 are known to directly regulate IL-1 function in the joint,103–105 the use of dex in the context of cartilage tissue engineering is critical for functional maturation of the tissue (as shown in this work) and has been demonstrated to confer chondroprotection against both IL-1α and TNF-α. 40
This study demonstrates the ability of dex-loaded MS to cultivate tissues that are mechanically viable (within native levels of compressive modulus) while simultaneously providing chondroprotection. In addition to the benefits of dex-loaded MS in culture, a controlled release approach to steroid administration is particularly advantageous in the context of current therapies for early intervention in OA. While it has been reported that IA injections lead to improved outcomes at 2-year follow-ups, 32 the inherently short duration of therapeutic action for corticosteroids 106 and dex (6–8 days 107 ), in particular, the result of rapid systemic absorption suggests that more frequent injections may obtain ideal joint pain outcomes. The accumulated availability of glucocorticoids through repeated injections, however, has been shown to lead to gross morphological cartilage changes 108 alongside lowered viability and biosynthetic activity of chondrocytes. 109 Successively elevated systemic levels of glucocorticoid also impact the hypothalamus–pituitary–adrenal (HPA) axis, 110 inhibiting the immune system's ability to respond to infection. The dual impact of rapid systemic absorption, both inside and outside the joint, suggests that sustained delivery of low levels of glucocorticoids may address these concerns while improving patient outcomes.
Low dose, sustained delivery of glucocorticoids, as presented in this work, provides a forward thinking strategy for improved cartilage repair and healing. The MS used in this study have been shown to release drug for up to 70 days (Fig. 2b), maintaining a consistent level of drug release throughout culture and ensuring local availability of the steroid beyond the 5 weeks observed in this study. Daily release of the drug is measured at only ∼19 ng per construct. This amount is 35× lower than the amount used in standard tissue culture 38 and 11× lower than commonly used triamcinolone acetonide IA injection dosages.97,107,111,112 Additionally, this strategy has been shown to minimize the potential effects on the HPA axis, having been employed in vivo and shown to promote tissue formation with minimal systemic impact. 52
We further anticipate a strategy of chondroprotection where a glucocorticoid, administered from the locale of the injury/repair site in a manner that provides its sustained release at much lower levels than clinical injections, can also impact tissue healing and repair of the engineered graft upon implantation.41,42 While future plans are aimed at further optimization of the dex microsphere strategy, including the testing of other proinflammatory cytokines such as TNF-α and the evaluation of tissue integrative repair in a cartilage explant ring model,113–115 the efficacy of our approach on cartilage repair will necessarily have to be evaluated in vivo.
Conclusion
In this study, we have demonstrated that the internal release of dexamethasone, an anti-inflammatory and FDA-approved synthetic glucocorticoid, can promote the development of mechanically functional engineered cartilage and simultaneously provide protection against a supraphysiological dosage of the proinflammatory cytokine IL-1α. As such, this study presents a strategy for delivery of dexamethasone from within engineered cartilage as a potential strategy for improving the success of cartilage repair in vivo.
Footnotes
Acknowledgments
The authors would like to thank the Musculoskeletal Transplant Foundation Established Investigator Grant (C.T.H.), National Institutes of Health (AR060361 [C.T.H., G.A.A.], AR068133 [C.T.H.], 5T32AR059038 [B.L.R.]), and National Science Foundation Graduate Research Fellowship Program under Grant No. DGE-11-44155 (B.L.R.).
Disclosure Statement
No competing financial interests exist.