
Abstract
Adipose-derived stem cell (ADSC) transplantation has been proposed to improve cardiac function and acute myocardial infarction (AMI). Recently, cell sheet technology has been investigated for its potential applicability in cardiac injury. However, a detailed comparison of the functional recovery in the injured myocardium between cell sheets and conventional cell injection has not been adequately examined. ADSCs were isolated from the inguinal fat tissue of ICR mice. Three groups of AMI induction only (sham), intramyocardial injection of ADSCs (imADSC), and ADSC sheet transplantation (shADSC) were compared by using rat AMI models. Engraftment of ADSCs was better sustained through 28 days in the shADSC group compared with the imADSC group. Ejection fraction was improved in both imADSC and shADSC groups compared with the sham group. Ventricular wall thickness in the infarct zone was higher in the shADSC group compared with both imADSC and sham groups. Growth factor and cytokine expression in the implanted heart tissue were higher in the shADSC group compared with both imADSC and sham groups. Furthermore, only the shADSC group showed donor-derived vessels at the peri-infarct zone. Taken together, these results indicate that, although shADSC resulted in a similar improvement in left ventricular systolic function, it significantly promoted cellular engraftment and upregulated growth factor and cytokine expression, and, ultimately, attenuated adverse cardiac remodeling in rat AMI models compared with imADSC.
Introduction
M
Cell sheet technology was developed to overcome limitations of traditional cell transplantation methods. Specifically, temperature-responsive culture dishes can be utilized to produce cell sheets of various cell types. These cell sheets easily adhere to various cell sources and can be transplanted into various tissue types. The effectiveness of cell sheet technology has been established through treatment of esophageal strictures after endoscopic submucosal dissection, 9 corneal epithelial disease, 10 and dilated cardiomyopathy.11,12 In particular, cell sheet transplantation is attracting considerable attention as a new therapy for repair of cardiovascular diseases. 13 Transplantation of mesenchymal stem cell (MSC), myoblast, or fibroblast sheet has improved ejection fraction (EF), angiogenesis, and vasculogenesis and inhibited fibrosis in heart disease models.14–16 This approach has allowed for the successful implementation of cell sheet and has shown potentially unlimited clinical applications in myocardial repair, wound healing, and in vivo neovascularization, which would otherwise be limited by existing technology.17,18
Recently, researchers have shown increased interest in a cell-delivery method for cardiac repair. The commonly used intramyocardial injection in previous studies has been shown to have limitations, including: (1) 1% survival rate after transplantation due to massive loss of injected cells, 19 (2) irregular distribution of transplanted cells in the host and lack of reproducibility, 20 and (3) generation of clusters of transplanted cells that increase host-derived inflammatory cells. 21 Conversely, the advantages of cell sheet delivery are: (1) the maintenance of cell–cell interactions via transplantation of cell sheet without any foreign material, (2) usage of nonphysical and nonchemical scaffolds, (3) improvement of cardiac function and acceleration of neovascularization due to enhanced cell engraftment, 22 and (4) a less traumatic and more effective method than intramyocardial injection. 23 Recently, successful clinical transplantation of cell sheet into heart 24 and cartilage 25 has been reported. Despite the earlier mentioned advantages, complications due to manipulation of cell sheet at the time of transplantation are inevitable. 20 Moreover, hypoxia or lack of nutrition supply to cell sheet could result in apoptosis of transplanted cells.
We hypothesized that the multi-layered ADSC sheet transplantation (shADSC) would enhance cell engraftment, growth factor and cytokine secretion, and neovascularization in the injured myocardium after AMI induction compared with the conventional intramyocardial injection of ADSCs (imADSC). In addition, we expected an increase in myocardial regeneration in damaged cardiac tissues. In the present study, we extensively investigated the cellular and paracrine mechanisms of shADSC for myocardial recovery after AMI induction compared with imADSC.
Materials and Methods
Animal care
Animals were strictly handled in accordance with the Guidelines for Animal Care and Use of the Korea University School of Medicine. All protocols were approved by the Korea University Institutional Ethics Committee for animal research (KUIACUC-2014-110) and the Administrative Panel on Laboratory Animal Care at the Korea University School of Medicine.
Preparation of ADSC sheet manipulator
ADSCs were isolated from male ICR albino mice (Orient Experimental Animal Laboratory, Gyeonggi, South Korea). Mouse inguinal fat pads were dissected, minced, and digested with 0.1% Type I collagenase (No. 4197; Worthington Biochemical). The cells were plated in a tissue culture dish after 1× phosphate-buffered saline (PBS) washing and maintained in MesenCult™ basal medium, which was supplemented with MSC stimulatory supplements (No. 05501; StemCell Technologies) and 100 U/mL penicillin/streptomycin (P/S; No. 15140; Gibco). The cells were incubated at 37°C in a humidified incubator. Immortalized ADSCs after infection with retroviruses harboring the pLPCX-TERT-IRES-eGFP were used as previously reported. 26
ADSC sheet was formed by plating 6.25 × 106 cells/well ADSCs onto thermo-responsive six-well plates (UpCell™; Nunc) and incubating them for 24 h. ADSC sheet detached spontaneously at room temperature within 30 min and was then washed once with 1× PBS. The obtained shADSC was 1.2 ± 0.2 cm in diameter, yielding a scaffold-free multi-layered ADSC graft.
Rat AMI model and transplantation
Female Sprague–Dawley rats weighing 180–200 g were purchased from Orient Experimental Animal Laboratory. Forty-two Sprague–Dawley rats were divided into three groups (Sham, n = 11; imADSC, n = 15; and shADSC, n = 16) and received an intraperitoneal (IP) injection of the immunosuppressant cyclosporine A (CsA; 10 mg/kg, Sandimmune, Novartis) starting 3 days before AMI induction and every 3 days thereafter. Sham group rats underwent an operation identical to that of infarct group animals without media injection. IP injection of CsA continued after AMI induction. To induce AMI, Sprague–Dawley rats were anesthetized with a mixture of ketamine (60 mg/kg; Yuhan) and xylazine hydrochloride (7.5 mg/kg; Rompun; Bayer). The left coronary artery was ligated with a 6-0 silk suture, 5 mm from the left coronary atrial appendage. After this, 1 × 106 ADSCs were prepared in 100 μL of culture medium for the imADSC group, whereas 0.6 ± 0.1 cm diameter of ADSC sheet was applied to the infarct zone by using a small amount of Surgiseal (SS-035T; Adhezion Biomedical).
In vivo imaging and analysis
Engraftment values of both imADSC and shADSC within the hearts were assessed in four AMI rats from each group at 4, 14, and 28 days after transplantation. For sacrifice, rats were euthanized by an IP injection with the mixture of ketamine (60 mg/kg) and xylazine hydrochloride (7.5 mg/kg). To detect the transplanted cells, imADSC and shADSC were stained with carboxy-fluorescein diacetate succinimidyl ester (CFDA SE; 10 mM, V12883; Molecular Probes) before transplantation. Measurements of in vivo fluorescence imaging were carried out by using the Maestro™ in vivo fluorescence imaging system (Cambridge Research & Instrumentation) and the Maestro software. CFDA SE-stained cells were detected at a wavelength of 492 nm. The expression of signal against the background was computed for quantification of intensity levels by using Maestro software. These in vitro spectra were measured by using an equal exposure time and under the same measurement conditions for all samples before transplantation.
Echocardiographic analysis
Echocardiography was performed with a commercially available echocardiography system (Vivid 7) with a 10 MHz small linear array transducer (i13L, all from GE Medical Systems). Rat AMI models were anesthetized with a mixture of ketamine (60 mg/kg) via an intramuscular (IM) injection. All measurements were performed by an experienced cardiologist who was blinded to the study group; performed over two consecutive cardiac cycles; and finally averaged. The percentage of fractional shortening (FS) was computed as a representative measure of systolic function. The EF was calculated by using end-diastolic volumes (Voldia) and end-systolic volumes (Volsys), which were calculated by manually drawing endocardial contours at end-diastolic and end-systolic phases in the apical two-chamber view by using the modified Simpson's rule.
Statistical analysis
All statistical values were expressed as mean ± standard deviation of the mean. Analysis of variance (ANOVA) was used to compare normally distributed data from all groups. *p < 0.05 was considered statistically significant. Significant differences between means were determined by using ANOVA followed by the Student–Newman–Keuls test. All statistical analyses were performed by using Sigma Stat 3.1 software (Systat Software).
An expanded Materials and Methods section is available at Supplementary Data (Supplementary Data are available online at www.liebertpub.com/tea).
Results
Characterization of ADSC sheet
Sca-1 and enhanced green fluorescent protein (eGFP) expression in ADSCs were confirmed by immunostaining (Fig. 1A). Furthermore, the multi-differentiation potential of ADSCs was successfully confirmed to adipogenic, osteogenic, cardiomyogenic, and endothelial lineages (Fig. 1B). For production of shADSC, 7.29 × 106 cells/well were determined to be the maximum density of ADSCs that could be cultured on classical or temperature-sensitive surfaces for 24 h (Fig. 1C). An unstable ADSC sheet was formed when plating <6.25 × 106 cells/well, whereas more than 6.25 × 106 cells/well generated a cell sheet that tightly attached to the dish surface, resulting in hampered recovery of the cell sheet (data not shown). Therefore, the optimal plating number of ADSCs for generation of a stable and transplantable cell sheet was determined to be 6.25 × 106 cells/well (Fig. 1C). The ADSC sheet was successfully generated by culturing for 24 h on a temperature-responsive surface (Fig. 1D). The successful generation of the ADSC sheet was confirmed by sustained expression of Sca-1 (Fig. 1E). Also, hematoxylin and eosin (H&E) staining revealed that the ADSC sheet consisted of six layers of ADSCs (Fig. 1F).
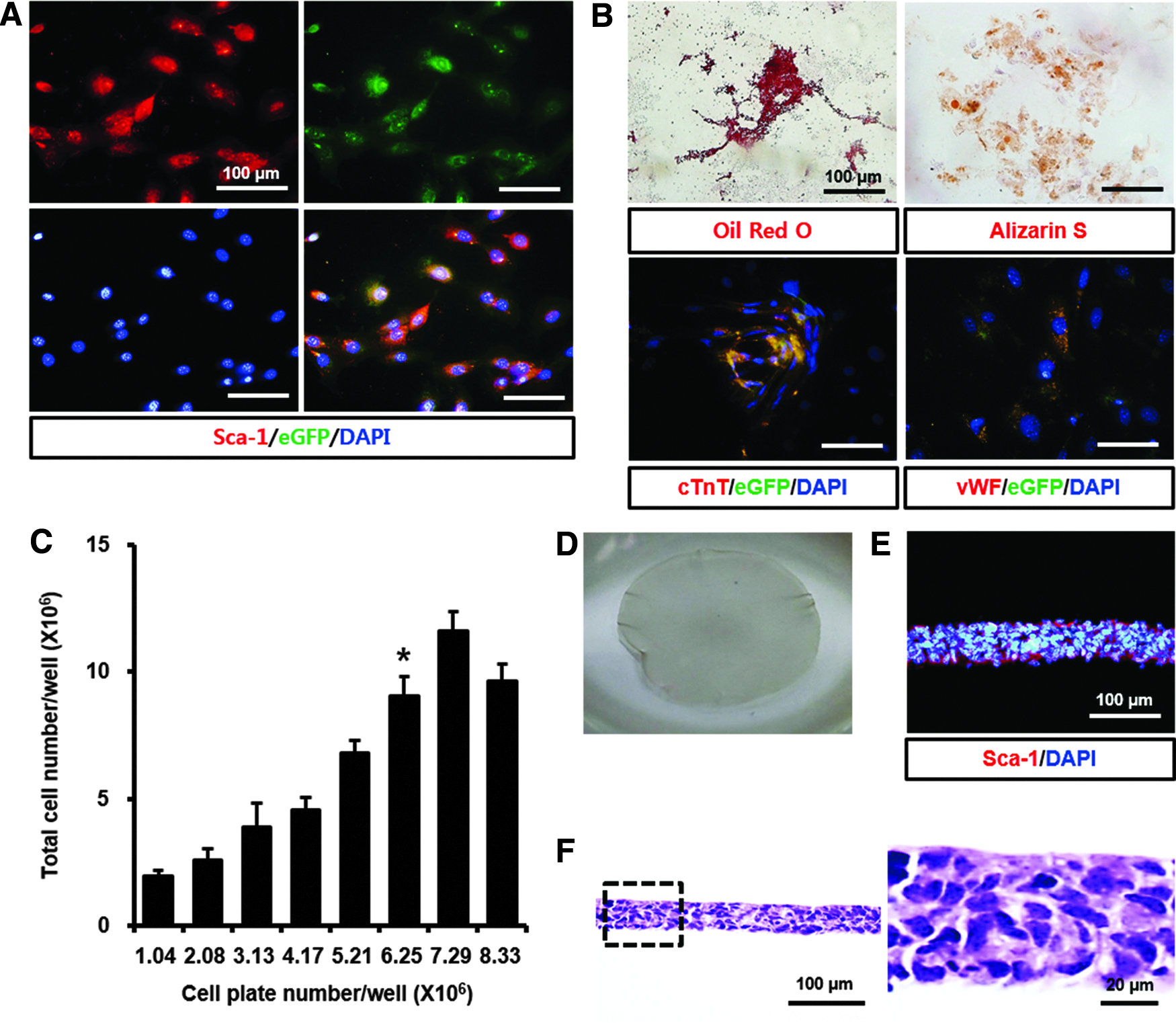
Successful development of cell sheet from ADSCs.
High expression of growth factors and high survival rate in high-confluency ADSCs
Secretion of growth factors and survival rates were confirmed in ADSCs under conditions of low confluency and high confluency, which were similar to those of the ADSC sheet (Fig. 2A). A comparison of real-time polymerase chain reaction (PCR) results between low- and high-confluency ADSCs showed differences in secretion of various cytokines after culture for 24 h. Higher messenger RNA (mRNA) levels of Adiponectin, MCP-1, CT-1, IL-1α, SDF-1, VEGF-A, IGF-1, bFGF, TGF-β1, Collagen I, Laminin-α1, Laminin-α4, Fibronectin, and Vimentin in high-confluency ADSCs were detected compared with those of low-confluency ADSCs (Fig. 2B). Flow cytometry results showed that the number of apoptotic cells was significantly lower in high-confluency ADSCs (1.38%) compared with low-confluency ADSCs (3.72%; Fig. 2C, D).
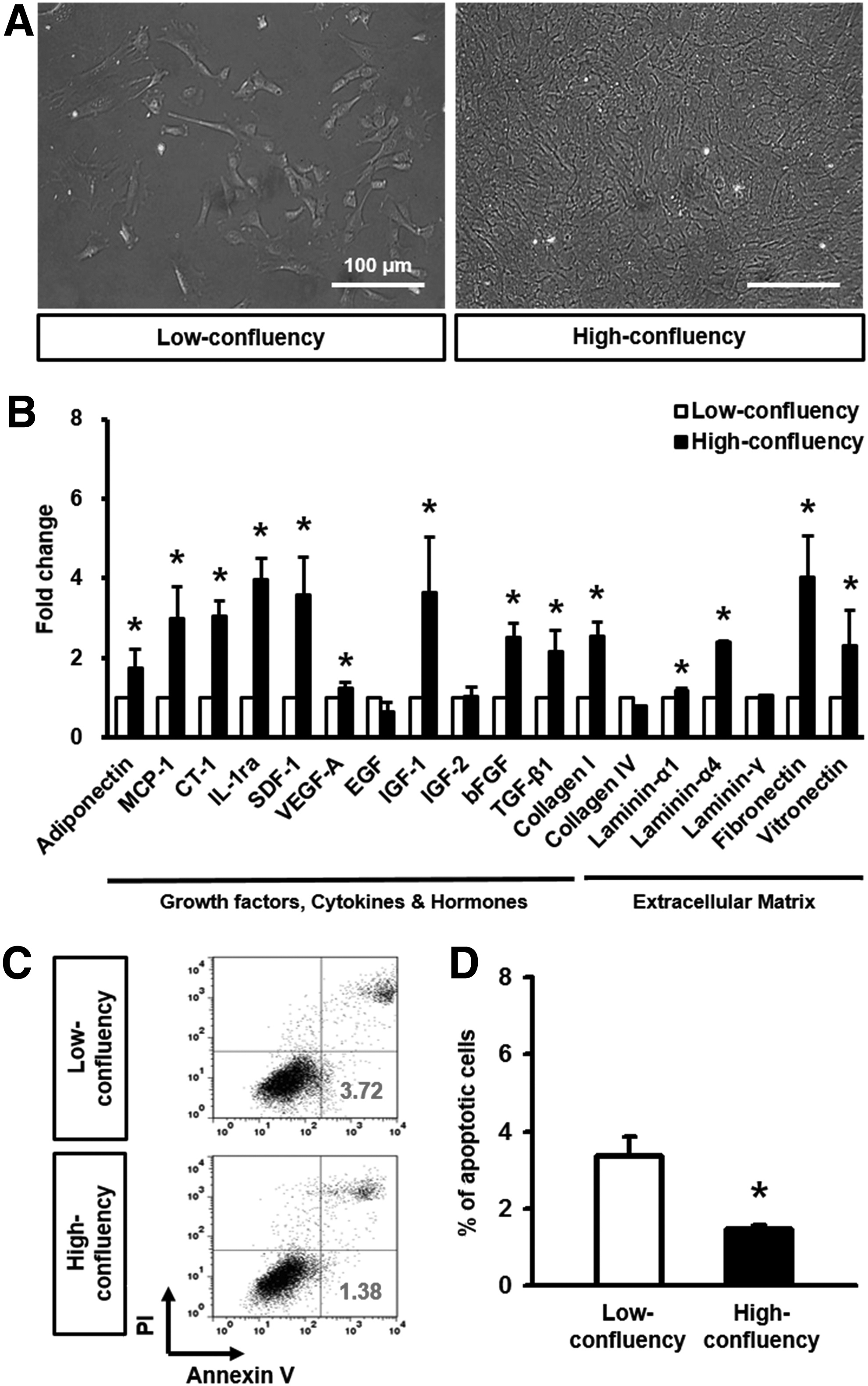
The effects of cell sheets on cellular apoptosis and expression of various growth factors from ADSCs.
High engraftment rate of shADSC
AMI was induced by ligating the left coronary arteries of rats. Cardiac function was assessed at 4, 14, and 28 days post-transplantation. AMI rats were sacrificed at 28 days, and isolated hearts were used for several histological analyses (Fig. 3A). shADSC attachment to the infarct zone of heart tissues (see arrowheads in Fig. 3B) was confirmed by visual inspection at 28 days after AMI induction (Fig. 3B). Both imADSC and shADSC grafts were detected by using an in vivo imaging system at 4, 14, and 28 days (Fig. 3C). The fluorescence intensity of CFDA SE-stained cells was decreased in imADSC (384.2 ± 270.4, 98.3 ± 30.3, and 2.0 ± 4.0 at 4, 14, and 28 days) and shADSC (880.4 ± 255.1, 344.0 ± 103.9, and 227.3 ± 36.7 at 4, 14, and 28 days) groups (Fig. 3D). The fluorescence intensity of CFDA SE-stained cells was significantly higher in the shADSC group than in sham (not detected) and imADSC groups at 4, 14, and 28 days (Fig. 3D). At 14 days after sheet transplantation, we demonstrated that shADSC was well maintained on the surfaces of the infarct and peri-infarct zones by H&E staining (Fig. 3E). The presence of transplanted ADSCs was confirmed by staining with antibodies for Sca-1 and eGFP. Both imADSC and shADSC groups were found to contain transplanted ADSCs. However, the relative amounts of transplanted ADSCs were higher in the shADSC group (Fig. 3F). A higher engraftment rate was found in the shADSC group than in the imADSC group.

Increased in vivo engraftment of shADSC in rat AMI models.
Positive effects of shADSC on LV remodeling
Functional improvement of the LV after ADSC transplantation was assessed by using two-dimensional echocardiography at 4, 14, and 28 days. FS values were significantly increased in imADSC (16.38% ± 1.47%, 20.26% ± 1.82%, and 25.19% ± 1.68%, respectively) and shADSC (15.99% ± 1.38%, 19.98% ± 1.36%, and 23.22% ± 0.88%, respectively) groups compared with the sham group (16.40% ± 0.38%, 16.53% ± 1.14%, and 18.16% ± 0.55%, respectively; Fig. 4A). Also, EF values were significantly higher in imADSC (39.35% ± 3.03%, 46.37% ± 3.42%, and 54.95% ± 2.52%, respectively) and shADSC (38.45% ± 2.78%, 46.18% ± 2.58%, and 61.96% ± 1.58%, respectively) groups compared with the sham group (38.90% ± 0.79%, 39.19% ± 2.30%, and 42.43% ± 0.97%, respectively; Fig. 4B). The FS and EF values analyzed by echocardiography showed similar correlations in all the examined groups (Supplementary Fig. S1A). However, no significant difference in FS or EF value was observed in imADSC and shADSC groups.

Potential of shADSC to improve functional recovery of the infarcted heart.
To examine the impact of shADSC on cardiac remodeling, Masson's trichrome (MT) staining was performed. In agreement with previous H&E staining results (Fig. 4C), shADSC was observed in the infarct and peri-infarct zones (see arrowheads in Fig. 4C). Fibrosis areas in imADSC (13.0% ± 4.21%) and shADSC (16.0% ± 4.68%) groups were significantly reduced compared with those in the sham group (30.0% ± 5.32%). However, no significant difference was found between imADSC and shADSC groups (Fig. 4D). At 4 weeks, an increased wall thickness in the infarct and peri-infarct zones of the shADSC group (2.38 ± 0.27 and 3.97 ± 0.63) was found compared with those of sham (1.00 ± 0.33 and 1.63 ± 0.24) and imADSC (1.30 ± 0.29 and 2.13 ± 0.26) groups (Fig. 4E), as determined by MT staining. However, differences between body and heart weights were not significant (Supplementary Fig. S1B, C).
High expression of cytokines in shADSC after AMI induction
Cytokine array was performed on ischemic hearts at 28 days after ADSC transplantation. Five growth factors and four cytokines were highly detected in the shADSC group (Fig. 5A). The array was then used to quantify changes in growth factors (IGF-1, bFGF, TGF-β1, IGF-2, and EGF) and inflammation-related cytokines (MCP-1, IL-1α, CT-1, and IL-ra). High concentrations of IGF-1, bFGF, TGF-β1, IGF-2, EGF, MCP-1, IL-1α, CT-1, and IL-ra in the shADSC group were found compared with those of imADSC and sham groups (Fig. 5B). However, no significant difference was found in the level of IGF-2 in the imADSC group compared with the shADSC group. In addition, differences in protein levels of all nine factors between sham and imADSC groups were not significant (Fig. 5B).
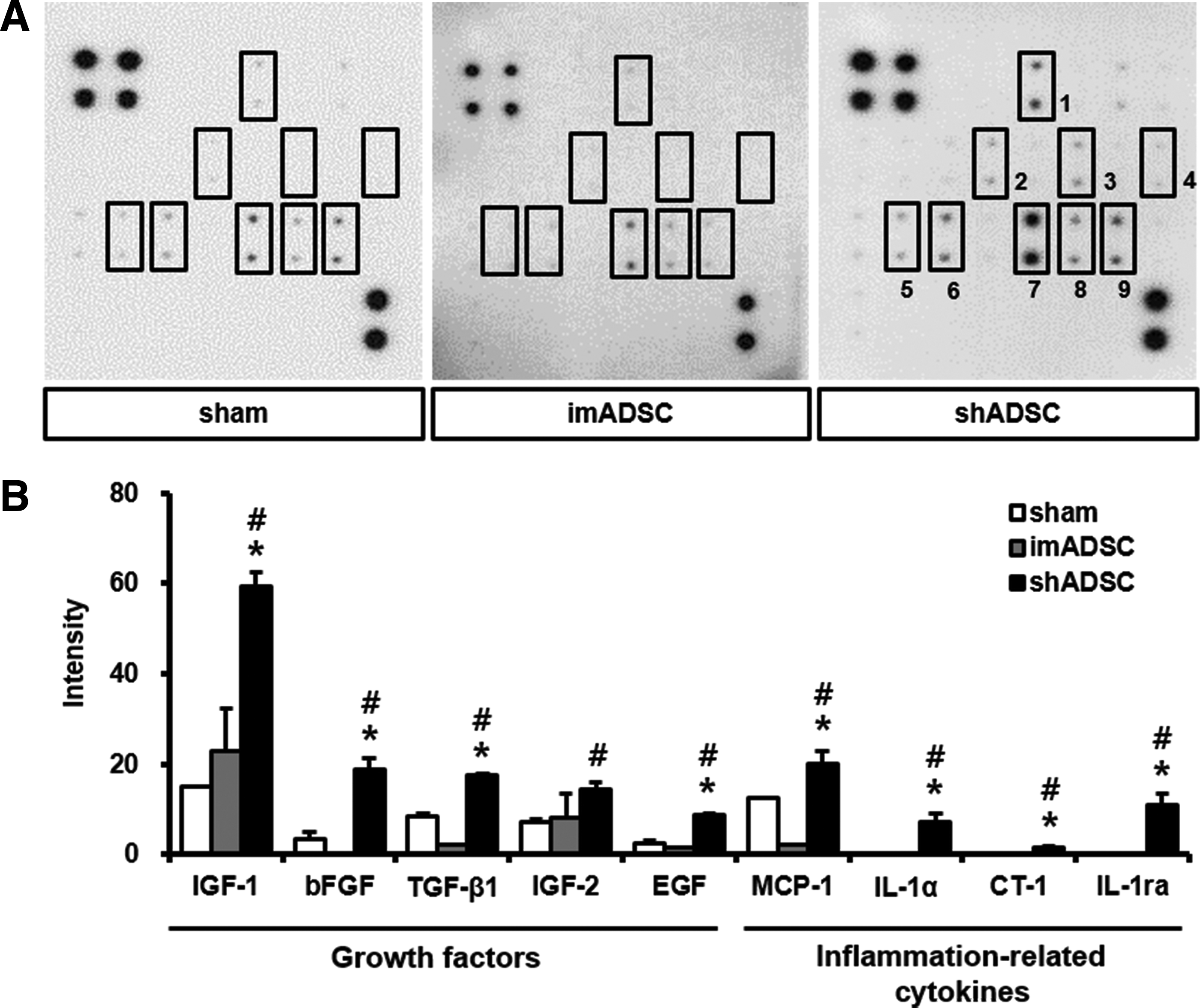
Secretion of various growth factors and cytokines by shADSC.
Improved neovascularization by shADSC
At 14 and 28 days after the procedures, transplanted sites were opened and the grafts of transplanted ADSCs were evaluated. The levels of neovascularization in the infarct and peri-infarct zones of heart were investigated by staining with anti-rat CD31, which binds to an endothelial-specific surface antigen (Fig. 6A). The proportion of CD31-positive vessels was significantly increased in both the infarct and peri-infarct zones of the shADSC group (9.80% ± 1.48% and 16.20% ± 1.92%) compared with those of sham (3.20% ± 1.30% and 5.80% ± 0.84%) and imADSC (6.20% ± 1.10% and 11.6% ± 1.14%) groups (Fig. 6B). von Willebrand factor (vWF) and eGFP double-positive ADSCs were identified in the shADSC group (Fig. 6C), but not in sham and imADSC groups (Fig. 6C). This implies that sheet transplantation exerts positive paracrine effects on endothelial differentiation as well as on engraftment.
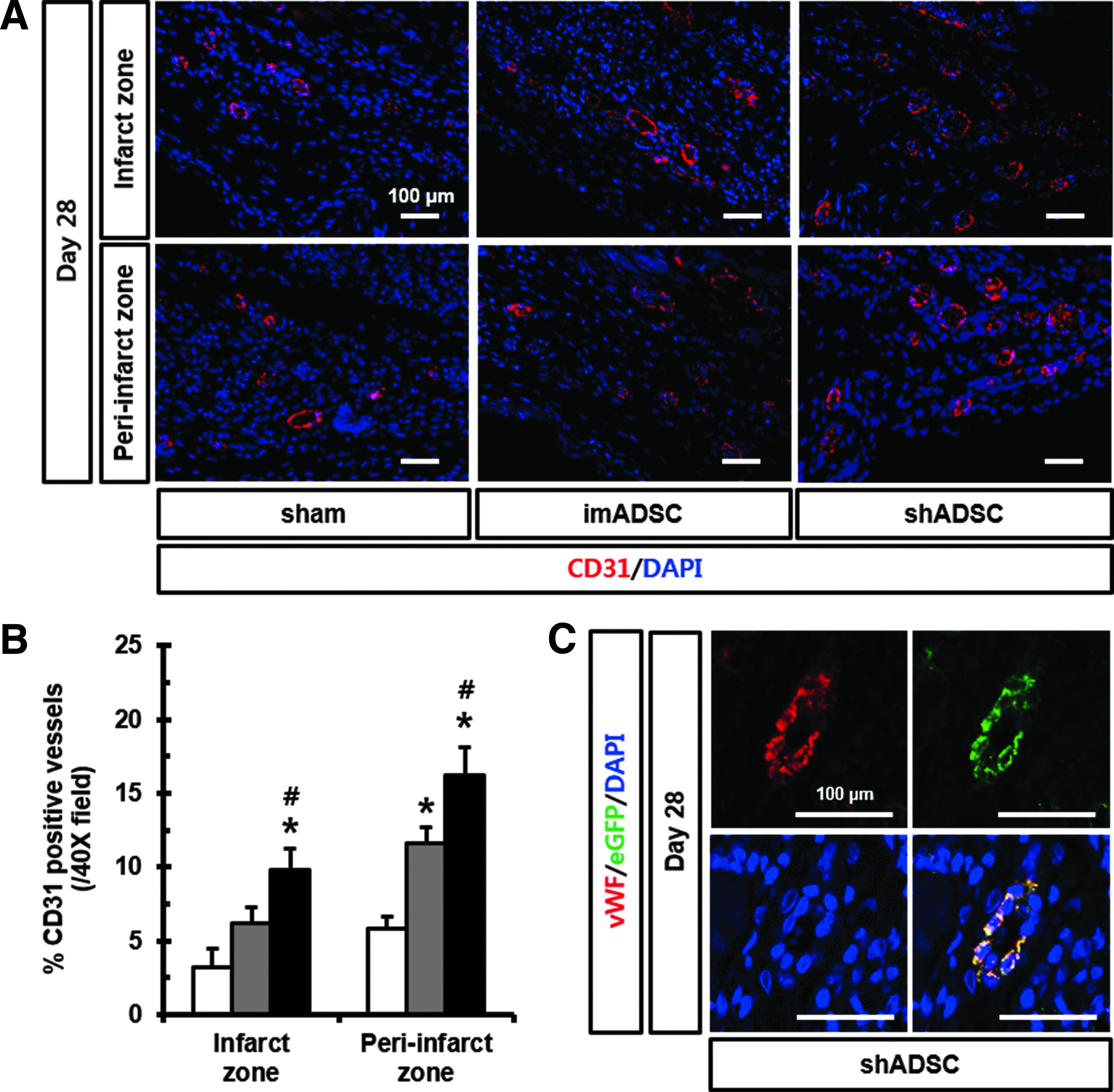
Regeneration of shADSC to endothelial cells in the infarcted heart.
Discussion
The novelties of this study were that: (1) the ADSC sheet significantly improved cell engraftment in the infarcted myocardium; (2) the ADSC sheet attenuated infarcted ventricular wall thinning, suggesting favorable cardiac remodeling after AMI induction; and (3) the ADSC sheet upregulated angiogenic growth factors and cytokine expression and induced donor-derived vessel formation in the implanted infarcted myocardium.
The clinical application of Sca-1-positive cells has been hampered, because the human ortholog of the Sca-1 protein has not been identified. Recently, Smits et al. 27 have successfully isolated Sca-1-positive cells from the adult human heart and further demonstrated their ability to differentiate into cardiomyocytes. Furthermore, Dey et al. 28 isolated Sca-1-positive cells representing a primitive stem cell potency by magnetic cell sorting using Sca-1-coupled magnetic beads from the human fetal heart. Even though existence of Sca-1-positive cells in fetal and adult human heart remains to be further verified, recent studies have raised the possibility of the clinical utility of Sca-1-positive cells.
Previously, ADSCs were reported to have distinct cellular characteristics compared with other stem cells. Zachar et al. 29 showed increased vascularization and migration of ADSCs in hypoxic conditions and several researchers have also reported that ADSCs held increased differentiation potential, proliferation, and expression of various growth factors, cytokines, and chemokines (TGF-β2, Angiogenin, Thrombospondin-2, αFGF, βFGF, IGF, PLGF, IFN-γ, Endostatin, IL1-ra, Collagen I, II and III, Decorin, MMP-1, and -2) compared with bone marrow derived-stem cells (BMSCs)30,31 Recently, Yu et al. 32 showed abundant deposition of extracellular matrix (ECM) molecules, such as Collagen, Fibronectin, and Laminin in the ADSC sheet, which is similar to our results. Therefore, ADSCs could be a promising cellular resource for cell therapy in AMI considering the pathologically poor microenvironment of the infarcted myocardium.
The proposed advantages of cell sheet technology for cell therapy are the establishment of a scaffold-free cell-dense environment, increased engraftment, and biological cell–cell interactions. 33 Indeed, recent studies of the transplanted cell sheet have reported increased engraftment, histologically decreased apoptosis, and formation of thick vascularized tissues in ischemic heart disease models.34,35 Similarly, in this study, we observed a decrease of apoptosis in our in vitro data (Fig. 2). Thus, these potential advantages of cell sheet technology are very attractive for its application in cell therapy. Recent studies36,37 have increased the stability of cell sheets by stacking cell sheets detached from a temperature-responsive culture dish. Nevertheless, cell sheet technology has several limitations, such as the need for a surgical procedure, limitations on the size of the sheet, and the large number of cells contained therein.
To determine the optimal plating number of ADSCs, growth rate and density of cells, multilayered cell sheet, equally distributed and transplantable cell sheet, and morphology of obtained cell sheet were considered. In this study, to generate an ADSC sheet for transplantation into rat AMI models, 6.25 × 106 ADSCs were plated and cultured for 24 h. Under these conditions, we finally obtained an ADSC sheet of 1.2 ± 0.2 cm diameter by plating the optimal number of ADSCs. The size of the ADSC sheet was 0.6 ± 0.1 cm in diameter and contained 1 × 106 ADSCs, resulting in the ADSC number being similar between shADSC and imADSC.
Indeed, transplantation of ADSCs showed improvements in LV contractile function after ischemic events.38,39 ADSCs are well known for their superior capacity for vessel reparability and recovery of the myocardium after cell transplantation to BMSCs.40,41 In ischemic heart disease models, ADSC transplantation resulted in recovery of the myocardium and angiogenesis due to paracrine effects such as increased secretion of VEGF, bFGF, and IGF-1. 42 Terrovitis et al. 43 showed that myocardial retention rates of cardiac stem cells were 17.6% ± 11.5% as determined by PCR and 17.8% ± 7.3% as examined by positron emission tomography at 1 h after transplantation. Our result overcame those limitations of shADSC to the damaged myocardium, resulting in an improvement of engraftment rate up to 30% at 28 days after transplantation (Fig. 3).
Wang et al. 44 reported that transplantation of the MSC sheet to the infarcted myocardium increased vascular density and engraftment and decreased enlargement of the infarcted region via an interaction between the host and transplanted sheet. Another report showed that the ADSC sheet augmented angiogenesis and cardiomyogenesis in AMI models. 45 In the present study, we demonstrated that shADSC into a rat AMI model leads to beneficial cardiac remodeling via improved engraftment and paracrine actions (angiogenesis and cardiac protection) of upregulated growth factors (Figs. 5 and 6). Simpson et al. 46 reported that 20% ± 3% of engrafted human MSCs (hMSCs) were found in the infarcted region not covered by hMSC patch at 7 days after hMSC patch transplantation. However, no hMSCs or residual patch were detectable at 4 weeks. In the present study, we found eGFP-positive ADSCs in the endocardium at 28 days after shADSC, suggesting that ADSC can engraft in the long term and migrate away to the endocardium from the cell sheet (Supplementary Fig. S3).
In this study, shADSC failed to show a superior effect on the recovery of left ventricular systolic function compared with imADSC (Fig. 4). This result could be explained by: (1) the limited cardiomyocyte differentiation potential of ADSCs or (2) the limited pro-survival function of ADSCs to rescue the impending necrotic host cardiomyocytes.
Interestingly, the present study showed that shADSC attenuated ventricular wall thinning and ventricular end-diastolic volume compared with imADSC. This suggested that the ADSC sheet induces a favorable ventricular remodeling process in the infarcted myocardium. Large cellular loss of the infarcted myocardium induced the ventricular wall thinning, which also contributed to ventricular dilatation. 44 Maintaining the ventricular wall thickness caused by shADSC in the present study might contribute to promoting the progression of the ventricular remodeling process. Similarly, Yeh et al. 47 showed that treatment of the human amniotic fluid stem cell (hAFSC) sheet to the infarcted myocardium improved wall thickness and reduced the infarct size compared with those of dissociated hAFSCs. Christman and Lee 48 also reported that injecting biocompatible polymer directly into the ischemic heart effectively promoted the ventricular remodeling process.
In the present study, shADSC also showed higher expression of various growth factors and cytokines in the peri-infarct zone. MCP-1 was previously reported to selectively inhibit pro-inflammatory monocytes and to prevent adverse cardiac remodeling. 49 IL-1ra has also been associated with favorable cardiac remodeling in a mouse model of severe ischemic cardiomyopathy. 50 On the contrary, IL-1α has been associated with the postinfarction inflammatory response. 51 CT-1 expression has been associated with improved cardiac performance, reduced infarct size, and inhibited cardiomyocyte apoptosis in mouse AMI models. 52 IGF-1/-2, 53 bFGF, 54 TGF-β1, 55 and EGF 56 have been associated with the downstream signaling pathway of myocardial angiogenesis in AMI.57,58 These data indicate the complex paracrine effects of the transplanted ADSC sheet. Detailed mechanisms of each growth factor and cytokine on the cardiac remodeling process remain to be further studied.
Recent studies have also demonstrated ADSC-derived vessels after IM injection of ADSCs in hind limb models. 59 They explained the underlying mechanisms regarding transplanted ADSCs-derived vessels as: (1) cell fusion with pre-existing vascular endothelial cells or (2) direct differentiation into endothelial cell and in vivo neovessel formation. In the present study, ADSC-derived vessels were clearly shown in the peri-infarct zone of shADSC, suggesting in vivo endothelial cell differentiation potential of ADSCs (Fig. 6). Moreover, increased expression of angiogenic growth factors in the peri-infarct zone might also contribute to this interesting observation.
Footnotes
Acknowledgments
The authors thank Chi-Yeon Park, I-Rang Lim, Ha-Rim Seo, and Ji-Hyun Choi for their technical assistance. This research was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A120275).
Authors' Contributions
J.-H.K., H.J.J., S.-C.C., and D.-S.L. contributed to study design, laboratory work, sample collection, data analysis, and statistical analysis; contributed to study design; and drafted the article. S.-C.C. and M.K. participated in study design and coordination, contributed to the study design and drafting of the article, and performed echocardiography. D.-S.L., S.J.H., and J.I.L. conceived the study, contributed to its design and coordination, secured funding, and critically revised the article for important intellectual content. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.