
Abstract
Osteoarthritis (OA) is a progressive degenerative joint disease, and to date, no disease-modifying OA drug exists. Amniotic membrane and umbilical cord products have been used clinically in several diseases due to their anti-inflammatory and antiscarring properties. In the present study, we sought to evaluate whether a particulate amniotic membrane and umbilical cord (AM/UC) matrix could aid in attenuating disease progression. Lewis rats underwent medial meniscus transection (MMT) to induce OA. Two weeks after surgery, animals received intra-articular injections (50 μL) of either 50 or 100 μg/μL particulate AM/UC or saline control and were subsequently euthanized 1 or 4 weeks later. Cartilage degeneration was assessed using both histological scoring methods and equilibrium partitioning of an ionic contrast agent-microcomputed tomography (EPIC-μCT). EPIC-μCT analysis demonstrated that overall cartilage destruction was attenuated, with a significant increase in both cartilage thickness and volume as well as a significant decrease in total lesion area in animals injected with either dose of particulate AM/UC at 1 week, but only a high dose at 4 weeks postinjection. Osteoarthritis Research Society International (OARSI) histology scores of tibial sections corroborated EPIC-μCT results. Overall joint destruction was attenuated in animals injected with either dose of AM/UC tissue compared with saline-injected control animals at 1 week postinjection. Only high-dose AM/UC-injected animals continued to show less overall joint destruction by 4 weeks postinjection. Intra-articular injection of particulate AM/UC tissue attenuates cartilage degradation in a rat MMT model of OA, suggesting that it may be able to slow joint destruction in patients with OA.
Introduction
O
The osteoarthritic joint is characterized by a loss of proteoglycan content in the cartilage matrix, hypertrophic differentiation of chondrocytes, lesion formation, and calcification of the extracellular matrix.3,5 Inflammation, particularly in early stages of the disease, is now recognized to play an important role in the progression of OA. 6 Several proinflammatory cytokines, including interleukin (IL)-1β, tumor necrosis factor (TNF)-α, and IL-6, have been demonstrated to be upregulated in patients with OA 7 and increased expression of these proinflammatory cytokines is thought to be linked to the development and progression of structural changes and cartilage degeneration in the OA joint. 7
Current conservative treatment options for osteoarthritic patients mostly involve pain management through nonsteroidal anti-inflammatory drugs (NSAIDs), nonacetylated salicylates, and steroids. While these treatments can be effective in the early to mid-stages of OA, they often fail to provide adequate pain relief as the joint further deteriorates.
When conservative treatments fail, injection of glucocorticoids or hyaluronic acid (HA) into the affected intra-articular joint space is an attractive treatment approach for OA. 3 Glucocorticoids have been found to be effective in relieving pain, but their duration is short-lived. Intra-articular injection of HA has presented with mixed results. Some studies report a reduction in pain and potential attenuation of cartilage lesion formation, 8 while others have reported minimal clinical benefit. 9 While several palliative treatment options exist for OA, to date there has not been any disease-modifying osteoarthritis drug that can successfully halt the progression of OA by controlling cartilage erosion. 10
The amniotic membrane and umbilical cord (AM/UC) are fetal-derived tissues that share the same cellular origin as the developing fetus. Embryologically, the AM, together with the placenta, is derived from the epiblast or outer cell mass, while the fetus is derived from the inner cell mass. The AM consists of a single layer of epithelial cells, a thick basement membrane, and an avascular stromal layer. The amniotic epithelium extends up the outside of the umbilical cord. The remainder of the umbilical cord consists of a viscous fetal hydrogel called Wharton's Jelly. 11
One important function of these tissues is to protect the fetus from cellular insults derived from the maternal environment. 12 AM/UC tissues have been used clinically in a number of applications in ophthalmology 13 as well as a dressing for burns and nonhealing skin ulcers and in various surgical procedures14–16 to facilitate wound healing by suppressing excessive surgical or disease-induced host tissue inflammation. 13 Additionally, the clinical success of AM as a potent anti-inflammatory and antiscarring agent has expanded investigations into the use of these tissues in orthopedic reconstructive procedures where they act to decrease local inflammation and adhesion formation following tendon 17 and nerve repair.18–20
In vitro and in vivo laboratory studies have characterized the anti-inflammatory and antiscarring properties21–23 that AM/UC tissues possess. Contained within the extracellular matrix of AM/UC tissues, there is a unique biochemical complex called the HC-HA/PTX3 complex that has been found to be responsible for several AM/UC tissue therapeutic actions.24–26 Considering the pathogenic role of inflammation in OA, it is possible that AM/UC tissues may be helpful in attenuating disease progression. In the present study, the ability of intra-articular injection of particulate AM/UC tissues to attenuate OA disease progression was evaluated using the rat medial meniscus transection (MMT) model of OA.
Materials and Methods
Test material
Human cryopreserved, particulate amniotic membrane/umbilical cord (AM/UC; CLARIX® FLO; Amniox Medical, Inc., Atlanta, GA) was aseptically processed by the proprietary CryoTek® method (U.S. Patent No. 8,153,162; 8,182,840; 8,182,841; 8,187,639;8,420,126; 8,440,235; 8,455,009; 8,460,714) in compliance with U.S. FDA current Good Tissue Practices (cGTP) from donated human placental tissue after determination of donor eligibility and tissue suitability. The amniotic membrane was physically separated from the chorion before processing. This process produces a lyophilized, micronized particulate product that is then terminally sterilized to sterility assurance level (SAL) 10−6 that retains tissue integrity while devitalizing cell viability. Upon use, particulate AM/UC was reconstituted in 0.9% saline (Cisen Pharmaceutical Co., Ltd., Shangdong, China) to the desirable concentrations before injection.
Animals
All procedures were approved by the Institutional Animal Care and Use Committee (IACUC) in compliance with the Principles of Laboratory Animal Care formulated by the National Society for Medical Research of PharmaLegacy Laboratories (Shanghai, China). Male Lewis rats (Sino-British SIPPR/BK Lab. Animal Ltd., Shanghai, China) at ∼8 weeks of age upon arrival were acclimatized for at least 7 days in the laboratory and maintained under climate-controlled conditions on a 12-h light–12-h dark cycle at 19–26°C with a relative humidity of 40–70%. Animals were allowed access to food and water ad libitum throughout the study.
Rat MMT model and treatments
Before surgery, a subcutaneous injection of atropine (0.05 mg/kg) was given to control saliva secretion. All animals were anesthetized by isoflurane at 2.0–3.5% to effect while being mixed with 0.8–1.5 L/min flow rate of oxygen. The right knee was shaved and cleaned using 2% iodine tincture and 70% ethanol. An incision was made over the medial aspect of the femorotibial joint. The medial collateral ligament was exposed through blunt dissection and transected to reflect the meniscus toward the femur. A full-thickness cut was made through the meniscus at its narrowest point. The joint space was returned to normal, and the incision was closed in two layers. The joint capsule was sutured independently from peripheral tissues using dissolvable 5–0 sutures with two to three interrupted stitches, and the skin was closed by skin clips and the animals were allowed to recover. All animals were monitored until they regained consciousness, after which they were permitted full weight-bearing and unrestricted activity.
Two weeks after surgery, animals were randomly assigned into one of three treatment groups (n = 18 per group) receiving intra-articular injection of 50 μL of saline (control), 50 μg/μL particulate AM/UC, or 100 μg/μL particulate AM/UC. Briefly, animals were anesthetized using isoflurane at 2.0–3.5% to effect while being mixed with 0.8–1.5 L/min flow rate of oxygen. Knee joints were cleaned using 70% ethanol and bent into a flexed position. Intra-articular injection of test or control articles was done using a sterile 25G needle. The selected doses (50 and 100 μg/μL) were determined based on earlier in vitro and in vivo studies (data not published). Animals were euthanized by CO2 at either 1 or 4 weeks after injection (n = 9 per group, per time point). At the time of euthanasia, the operated joint was examined for inflammation, wound dehiscence, or any complications before being dissected out and preserved in 10% buffered formalin for 48 h, followed by storage at room temperature in 70% ethanol for equilibrium partitioning of an ionic contrast agent-microcomputed tomography (EPIC-μCT) and histological analysis to assess cartilage degeneration.
Equilibrium partitioning of an ionic contrast agent-microcomputed tomography
Fixed knee joints were subjected to μCT scanning after being immersed in 2 mL of a meglumine diatrizoate compound solution (Cysto Conray II; Hansen Pharm, China) for 30 min. The μCT settings for scanning were as follows: 16 μm voxel size using 45 kVp, 177 μA, and 200 ms integration time. Raw data were reconstructed to two-dimensional tomograms and the articular cartilage surface was contoured and thresholded with global segmentation parameters (Gauss σ = 1.2, support = 2, threshold = 175–225) to isolate the articular cartilage surface from the underlying subchondral bone.
The generated three-dimensional images were used to determine articular cartilage thickness and volume, as well as the total area and ratio of the articular cartilage surface that had been degraded. To quantify the average articular cartilage thickness and volume, an identical volume of interest (VOI) was defined for each condyle extending from the middle of the cartilage to both sides for 100 slices with a total of 200 slices, or 3140 μm. To determine the total area and ratio of the articular cartilage surface that had been degraded, the entire medial tibial plateau was used as the VOI for all animals.
Histological analysis
After EPIC-μCT scanning, tibiae were decalcified using a formic acid/formaldehyde solution, dehydrated, and embedded in paraffin. Samples were sectioned in the frontal plane and stained using both hematoxylin and eosin stain and Safranin-O. Stained tibial sections were examined and scored in a masked manner for cartilage degeneration, the presence of osteophytes, calcified cartilage, subchondral bone damage, and synovial membrane inflammation using the Osteoarthritis Research Society International (OARSI) scoring system for rats, as previously described. 27
Statistical analysis
Quantitative data from EPIC-μCT and histological scoring are expressed as mean ± standard error. For EPIC-μCT data, a one-way analysis of variance (ANOVA) was conducted. Where statistical differences were indicated, Tukey's multiple comparison test (Tukey's HSD) was used to determine differences among means. For histological scoring, a nonparametric one-way ANOVA was used to test for statistical differences between treatment groups. Where statistical differences were indicated, a Mann–Whitney U test was performed to detect between-group differences. A calculated probability (p) value less than 0.05 (p < 0.05) was considered statistically significant.
Results
Equilibrium partitioning of an ionic contrast agent-microcomputed tomography
Representative two-dimensional tomograms of tibiae from healthy animals as well as animals injected with either saline (control) or particulate AM/UC tissues (50 or 100 μg/μL) showed the development of significant cartilage lesions (Fig. 1B; arrow) and fibrillation/thinning (Fig. 1C; arrow) of the tibial articular cartilage surface. The three-dimensional reconstruction of the articular cartilage surface displayed the presence of lesions (dark green areas) as well as areas of thicker articular cartilage (yellow–red areas) across the surface of the tibia in animals subject to MMT compared with healthy uninjured animals (Fig. 1E–H).
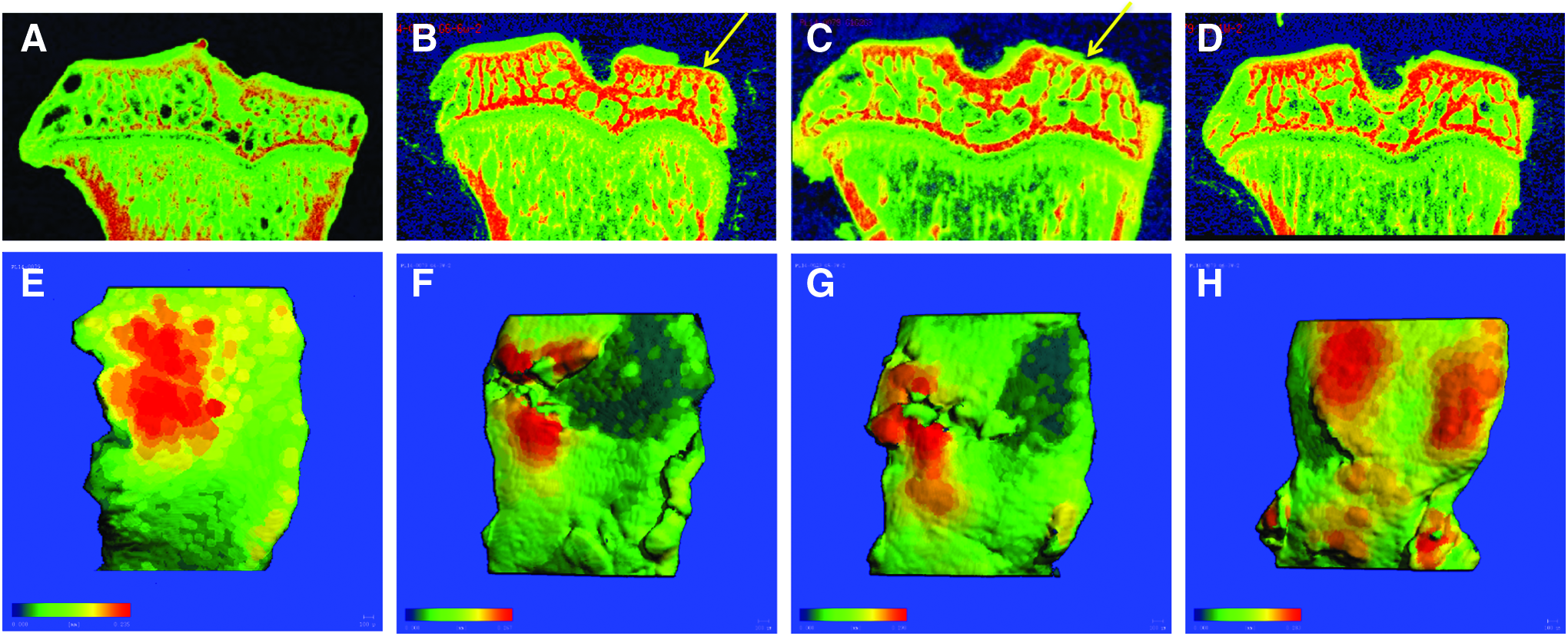
EPIC-μCT Images of Explanted Joints 1 Week Postinjection. Representative two-dimensional images of healthy uninjured animals
Quantitative analysis of both articular cartilage thickness and volume of the medial tibia in animals injected with 50 μg/μL of particulate AM/UC tissues showed no significant difference compared with saline-injected control animals at 1 week after intra-articular injection (Fig. 2A, B; black bars). However, in animals receiving 100 μg/μL particulate AM/UC tissues, both articular cartilage thickness and volume were significantly greater than not only control animals (p < 0.05, Tukey's HSD) but also 50 μg/μL particulate AM/UC-injected animals (p < 0.05, Tukey's HSD). No differences were observed between the three treatment groups for both cartilage thickness and volume by 4 weeks after intra-articular injection (Fig. 2A, B; gray bars).
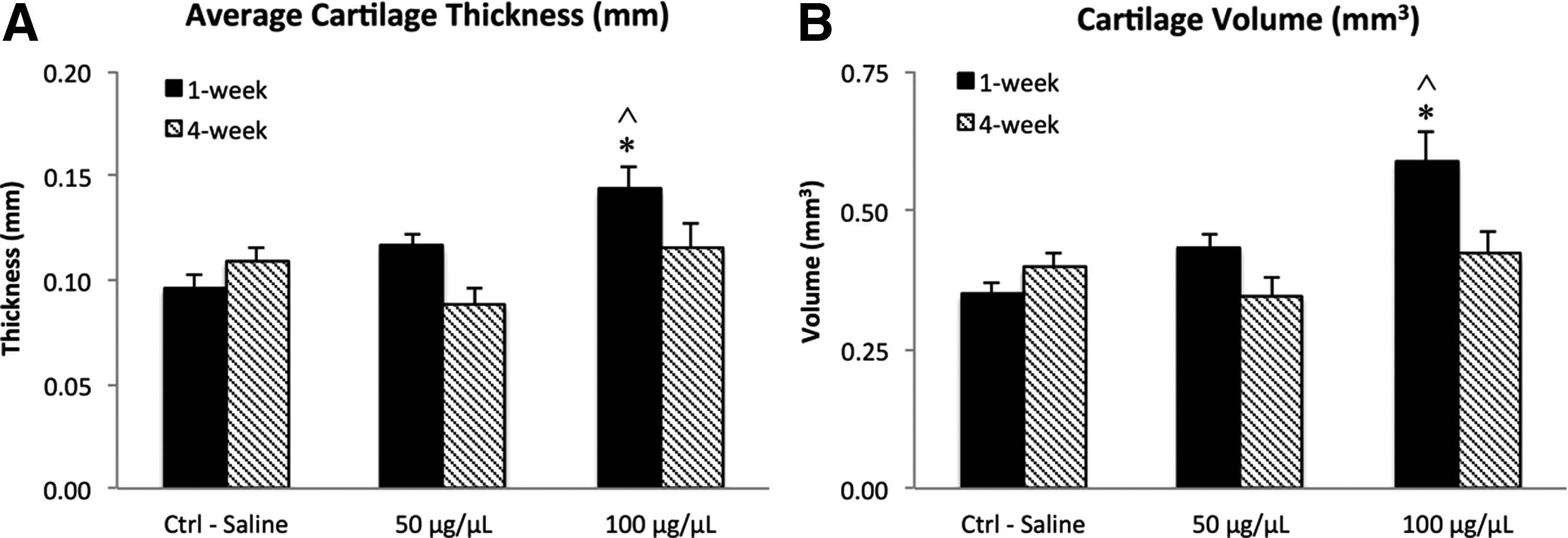
Quantitative Analyses of EPIC-μCT Data of Cartilage Thickness and Volume. The average cartilage thickness
EPIC-μCT was used to examine both the total lesion area and the percentage of the medial articular cartilage surface that had been degraded. In contrast to average cartilage thickness and volume, there was a significant reduction in both the total lesion area and the percent area of the tibial surface that had been degraded at 1 week postinjection in animals receiving either dose of particulate AM/UC tissue when compared with saline-injected control animals (p < 0.05, Tukey's HSD) (Fig. 3A, B; black bars). Furthermore, at 4 weeks postinjection, animals receiving 100 μg/μL of particulate AM/UC tissue continued to show a significantly smaller lesion area and a significant decrease in the percent total lesion area when compared with not only saline-injected control animals but also animals receiving 50 μg/μL of particulate AM/UC tissue (p < 0.05, Tukey's HSD) (Fig. 3A, B; gray bars).

Quantitative Analysis of EPIC-μCT Data of Cartilage Lesion Area and Percentage of Lesion Area. Reconstructed three-dimensional tomograms of the medial cartilage surface were analyzed to determine the mean total lesion area
Histopathology analyses
Following EPIC-μCT analysis, tibiae were stained using both hematoxylin and eosin and Safranin-O. Representative histology images are shown in Figure 4 for animals receiving injection of saline (Fig. 4A, D), 50 μg/μL of particulate AM/UC tissue (Fig. 4B, E), and 100 μg/μL of particulate AM/UC tissue (Fig. 4C, F).
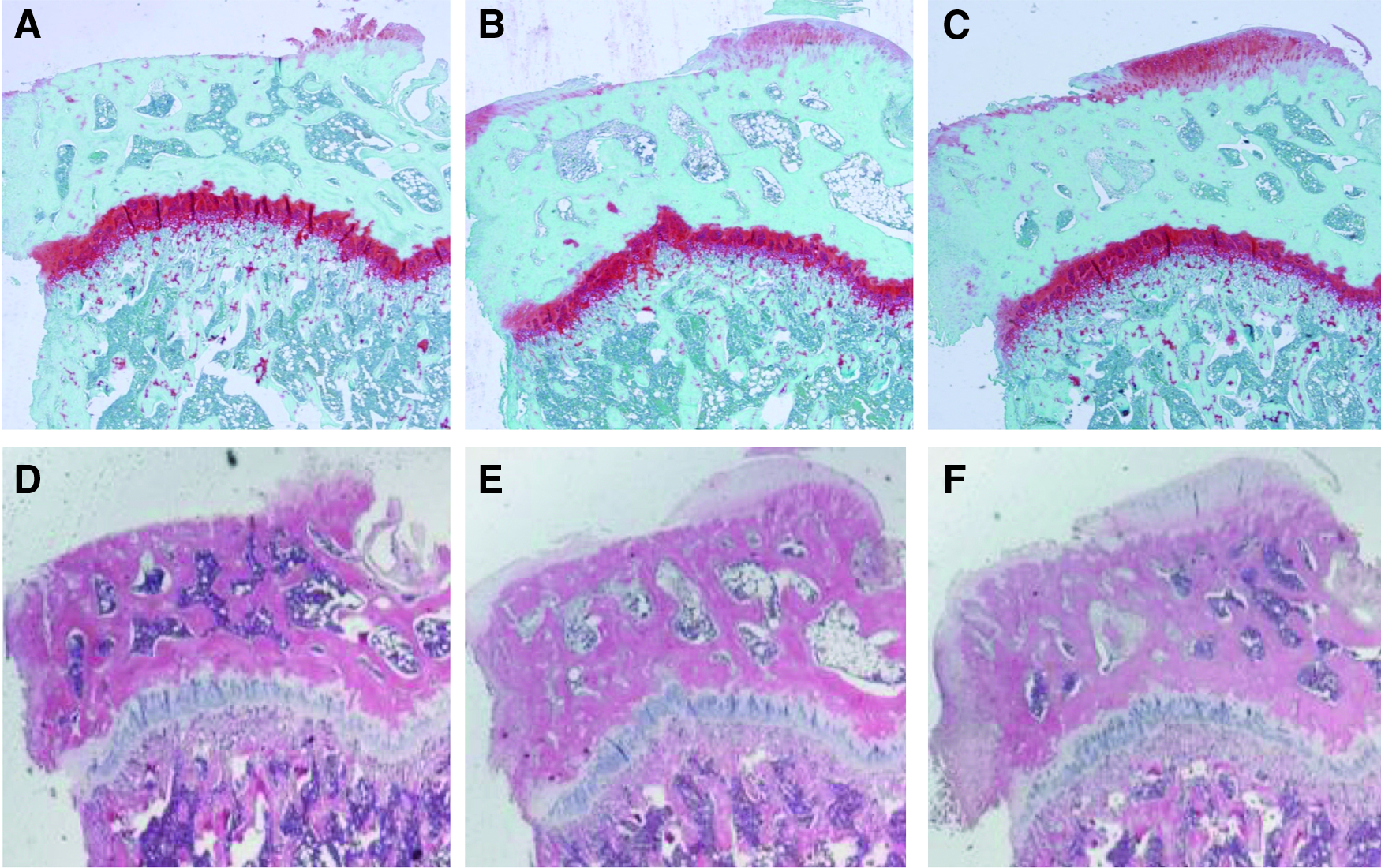
Histological Sections of Explanted Tibial Joints. Following EPIC-μCT scanning, tibiae were processed for histological staining using Safranin-O and hematoxylin and eosin. Representative sections for saline control
Quantitative analyses of the damaged cartilage were assessed by a blinded reviewer using the OARSI recommendations for histological assessments in the rat. OARSI scoring demonstrated that there was a significant reduction of the extent of cartilage degeneration (p = 0.002) and the amount of calcified cartilage (p = 0.003) in animals injected with 50 μg/μL of particulate AM/UC tissues when compared with saline-injected control animals at 1 week postinjection. Similarly, in animals receiving 100 μg/μL AM/UC, both cartilage degeneration (p = 0.005) and the amount of calcified cartilage (p = 0.006) were significantly reduced compared with saline-injected control animals (Fig. 5A, B; black bars). In addition, the total OARSI scores of animals injected with either dose of particulate AM/UC tissues were significantly lower than those of saline-injected control animals (50 μg/μL p = 0.014; 100 μg/μL p = 0.023), indicating that the overall joint damage was lessened by injection of particulate AM/UC after 1 week (Fig. 5D; black bars).
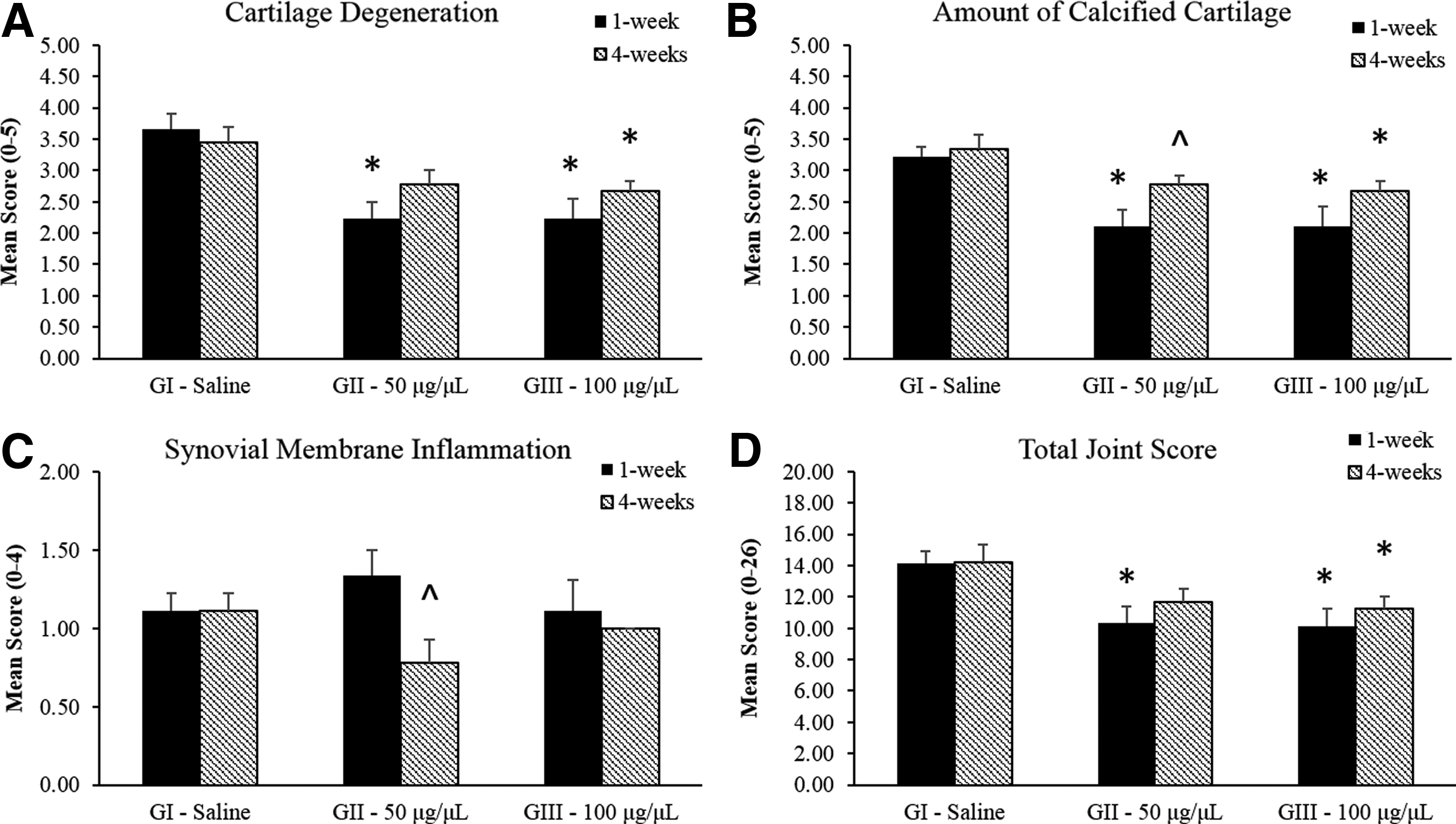
OARSI Histopathology Scores. Stained tibial sections were scored by a blinded reading according to the OARSI histopathology initiative guidelines for rats for cartilage degeneration
At 4 weeks after injection, the OARSI scores in animals injected with 50 μg/μL particulate AM/UC tissue were not different from those in saline-injected control animals (Fig. 5A, B; gray bars). However, the OARSI scores for cartilage degeneration (p = 0.02), amount of calcified cartilage (p = 0.04), as well as subchondral bone damage (p = 0.04)), and the total OARSI score (p = 0.038) of animals injected with 100 μg/μL of particulate AM/UC tissue remained significantly lower than those of saline-injected control animals at the 4-week time point (Fig. 5A, B, D; gray bars). In addition to showing less overall joint destruction, injection of human particulate AM/UC tissues at either dose (50 or 100 μg/μL) into the joint space of nonimmunocompromised rats did not have any significant effect on synovial membrane inflammation using the OARSI scoring method for synovial tissue thickness, proliferation, and infiltration of inflammatory cells (Fig. 5C, p > 0.05 vs. control).
Discussion
The present study demonstrates the efficacy of intra-articular injection of particulate AM/UC tissue in reducing cartilage damage in the MMT rat model of osteoarthritis.28,29 This well-established model mimics human OA pathologies and exhibits progressive degenerative changes to the cartilage, including chondrocyte hypertrophy, proteoglycan loss, fibrillation, and osteophyte formation, by 3 weeks postsurgically 30 and has been used to evaluate the efficacy of intra-articular injection of several different compounds, including glucosamine as a therapeutic for OA, 31 the ability of Chinese herbal formulations to inhibit cartilage degeneration, 32 and to evaluate the ability of matrix metalloproteinase inhibitors to attenuate joint damage. 33
In the present study, male Lewis rats of age 8 weeks were used. After MMT, these animals showed joint damage and loss of articular cartilage. Several other studies using both chemically induced as well as surgically induced OA have used animals aged 7–10 weeks and have demonstrated significant joint destruction similar to that observed in the present study.34–38
In this study, explanted knee joints were scanned using μCT in conjunction with the use of an ionic contrast agent (EPIC-μCT) to generate nondestructive high-resolution two-dimensional and three-dimensional images of the tibial articular cartilage surface. Images of a healthy uninjured animal demonstrate a smooth and relatively uniform thickness articular cartilage layer. Our results showed a significant reduction in both the total lesion area and percent lesion area in joints receiving intra-articular injections of both 50 and 100 μg/μL of particulate AM/UC at 1 week after injection and an increase in articular cartilage thickness and volume in animals receiving 100 μg/μL AM/UC tissue compared with saline-injected control animals. Furthermore, in animals receiving 100 μg/μL of particulate AM/UC, both lesion area and percent lesion area at 4 weeks postinjection remained significantly lower compared with not only control injected animals but also compared with animals injected with 50 μg/μL AM/UC tissue (Figs. 1–3), suggesting a dose-dependent effect of cryopreserved, particulate AM/UC tissues in attenuating the progressive degeneration of the articular cartilage surface.
These findings were corroborated by histological analysis using the OARSI scoring system by independent observers blinded to the study treatments (Figs. 4 and 5). OARSI scoring at both 1 and 4 weeks for both doses of AM/UC tissues revealed a similar extent of synovial membrane inflammation in animals receiving particulate AM/UC tissue and animals receiving injection of saline, suggesting that injection of human particulate AM/UC tissue in a nonimmunocompromised rat did not induce a xenogeneic immune response.
Animals were allowed to have full weight bearing for 2 weeks after MMT to adequately develop lesions on the articular cartilage surface before injection, which has been demonstrated to occur in the MMT model in rats by this time.
Allowing such focal cartilage destruction to occur before intervention has been used previously for testing intra-articular injection of various compounds as treatment for OA. The chondroprotective efficacy of intra-articular injection of hyaluronate, tenoxicam, and vitamin E was compared in a rat model of surgically induced OA with injections of each compound starting at 2 weeks postoperatively and continuing weekly for 5 weeks. 39 Injection of all three compounds resulted in significantly lower Mankin histological grading scores at 8 weeks compared with saline-injected control animals; however, no difference in the extent of chondroprotection was observed between treatments. Intra-articular injection of deoxycholic acid every 3 days beginning at 4 weeks after MMT resulted in significantly less cartilage degeneration compared with control animals. 38 By allowing cartilage destruction to begin, the efficacy of test compounds in attenuating disease progression can be evaluated.
The efficacy of intra-articular injection of amniotic membrane-derived tissues has also been examined in this model. Willett et al. 5 injected a dehydrated human amnion/chorion membrane product (dHACM) in a rat MMT model 24 h after MMT surgery. Although they also noted fewer defects and a smaller lesion volume compared with saline-injected control animals using EPIC-μCT at 21 days postinjection, it remains unclear whether this product might achieve the same efficacy if injected at a later time point after cartilage destruction had begun. In addition, the injected dose of dHACM into the joint space was not reported in this study, and the authors were unable to perform histopathological analysis, which is considered as the gold standard for evaluating potential therapeutics of OA, so a direct comparison of the results between the two studies cannot be made. Our study demonstrates a dose-dependent benefit of particulate AM/UC tissue in attenuating further joint destruction in an already osteoarthritic joint.
For OA, while initially viewed as primarily a noninflammatory disease resulting from mechanical stresses to the joints, more recently, the role of inflammation in the joint space in contributing to disease progression has been recognized. For instance, several cytokines, including both proinflammatory cytokines such as IL-1β, TNF-α, and IL-6 and anti-inflammatory cytokines such as IL-4, IL-10, and IL-13, and the ratio between them may be related to OA disease progression. 7 Increased levels of IL-6 have been found to correlate with the intensity of lesions in patients with OA. 40 IL-4 has been found to inhibit the degradation of proteoglycans, while IL-10 has been found to stimulate type II collagen and proteoglycan synthesis.41–43
These studies highlight the importance of inflammation as a contributor to OA, and current therapies for OA primarily target relieving pain associated with OA by reducing inflammation, as is the case with NSAIDs, corticosteroid injections, and HA injections. The current experiment demonstrated efficacy in reducing not only the area of degeneration but also the depth of disease progression, possibly through altering the inflammatory induction milieu.
AM/UC tissues have been reported to have potent anti-inflammatory actions. A number of studies have demonstrated that transplanted cryopreserved AM/UC can upregulate the expression of anti-inflammatory cytokines such as IL-10, while downregulating proinflammatory cytokines, including TNF-α, IL-6, and IL-12. 44 These anti-inflammatory actions have been found to be attributed to a unique biochemical component of the extracellular matrix in AM/UC tissues called HC-HA/PTX3.24,45,46
This complex consists of pentraxin-3 closely associated with a complex between heavy chain 1 (HC) from the inter-α-inhibitor complex and HA. The latter complex is formed through the catalytic action of TSG-6,24,45,46 which is constitutively expressed in AM/UC tissues. TSG-6 has also been found to have a chondroprotective effect in animal models of antigen-induced arthritis.47,48 The demonstrated anti-inflammatory actions of AM/UC tissues may allow such tissues to be a novel therapeutic strategy to modulate the inflammatory processes associated with OA and subsequently attenuate overall disease progression.
Taken together, these data suggest that particulate AM/UC tissue may attenuate progressive cartilage degeneration in a small animal model of OA and that there also may be a dose-dependent effect of particulate AM/UC tissue on joint degradation, with animals receiving 100 μg/μL AM/UC showing less cartilage degradation and joint destruction as long as 4 weeks after injection. Further studies examining the effect of dosing and/or multiple injections on the efficacy of intra-articular injection of AM/UC tissues in prolonging the prevention of cartilage degradation are warranted.
Footnotes
Disclosure Statement
Andrew L. Raines and Julie O'Connell are employees of Amniox Medical, Inc. Lorraine Chua, Chen-Wei Su and Scheffer CG Tseng are employees of Tissue Tech, Inc. All other authors report no competing financial interests.