
Abstract
Urethral defects are normally reconstructed using a patient's own genital tissue; however, in severe cases, additional grafts are needed. We studied the suitability of poly(
Introduction
U
Tissue engineering could provide a novel method to overcome problems associated with traditional reconstructive surgery. Several natural tissue grafts, such as bladder acellular matrix graft (BAMG) and collagen and small intestine mucosa with and without cells, have previously been studied for urethral reconstruction. For instance, Orabi et al. studied the BAMG seeded with urothelial and smooth muscle cells for urethral reconstruction in an in vivo beagle model with promising results. They compared the cell-seeded BAMG with the noncellular BAMG and observed that, in the noncellular group, the number of urethral strictures and fistulas was remarkably higher. 4 The disadvantage of natural biomaterials is the high batch-to-batch variation, and large-scale manufacturing and modification of mechanical properties are difficult. Thus, the development of novel graft materials for urethral reconstruction is essential to develop new treatment options for remedying severe urethral defects.2,3,5,6
The selection of an appropriate biomaterial for the application is crucial, and the biomaterial for urethral reconstruction should meet the requirements of being biocompatible, nontoxic, biodegradable without disadvantageous tissue reactions, and able to promote urothelial tissue regeneration. Furthermore, for urethral reconstruction, the biomaterial should be elastic and flexible and should mimic the basement membrane of the urothelium, generating a suitable matrix for urothelial cells to attach and proliferate. Additionally, the biomaterial should be suturable and easily molded into a tubular structure.2,6
Aliphatic poly(α-esters), such as polyglycolide (PGA), polylactide (PLA), polycaprolactone (PCL), and their copolymers, are the most commonly studied synthetic biomaterials for tissue engineering, and they have also been studied in urological applications with promising results.7–9 Tubular PGA:poly(lactide-co-glycolide acid) (PLGA) scaffolds seeded with urothelial and smooth muscle cells were used to reconstruct urethras for five boys suffering from severe urethral defects with favorable results. After the operation, a narrowing of the urethra developed for one patient, but it was repaired with a surgical incision. After a 6-year follow-up, no strictures or diverticula were detected, and the urethral histology was normal after 3 months. 8
Furthermore, PLGA scaffolds were also used to reconstruct de novo bladders for children suffering from neurogenic bladders; however, the results of this study were not positive. In this study, PLGA scaffolds seeded with urothelial cells and smooth muscle cells were used to reconstruct de novo bladders for 10 children. Severe adverse effects, either bowel obstruction or bladder rupture, were detected in four patients.
9
Furthermore, Pariente et al. have demonstrated excellent biocompatibility of PGA, poly-
In our previous studies, we have shown that human urothelial cells (hUCs) attach, remain viable, and proliferate on poly(
Poly(trimethylene carbonate) (PTMC) is a benign, degradable, biocompatible polymer prepared from trimethylene carbonate that possesses good mechanical properties.15,16 PTMC is glass-like at temperatures below approximately −15°C but is flexible at room temperature. 15 PTMC degrades via surface, not bulk, erosion, and enzymatically without acidic end products in vivo.17–20 PTMC has been studied in various tissue engineering applications, for instance, for cardiomyocyte and Schwann cell cultivation, guided bone regeneration and abdominal surgery. Further, PTMC has been studied for vascular tissue engineering applications with good results.15,19 Due to its flexibility, biocompatibility, and potential for soft tissue engineering applications, we considered it an interesting biomaterial for urothelial applications. Further, at least to our knowledge, PTMC has not been previously studied for urothelial tissue engineering.
Due to the unmet medical need of nonurological grafts, we tested PLCL and PTMC membranes for urothelial tissue engineering. The aim of this study was to compare the suitability and in vivo biocompatibility of PLCL and PTMC for urethral reconstruction in an in vivo rabbit model.
Materials and Methods
Biomaterial membranes
The 70/30 poly(
PTMC was synthesized by ring polymerization of trimethylene carbonate (Boehringer Ingelheim, Ingelheim am Rhein, Germany) under a blanket of nitrogen at 150°C, using stannous octoate (Sigma Aldrich, St. Louis) as a catalyst and water as an initiator. The polymer was melted using a compression molder (Fontijne laboratory press THB400, Vlaardingen, The Netherlands) at 160°C and up to 100 kN for 1 min, followed by a two-step compression molding cycle. Membranes with a thickness of 250 μm were obtained; their molecular weight was ∼275 kg/mol. The membranes were cut to appropriate size and packed in PET/ALU/PE peel pouches (Riverside medical packaging Ltd., Derby, United Kingdom), vacuum sealed, and gamma irradiated at 25 kGy using a 60Co source (Synergy Health, Ede, The Netherlands) for sterilization and cross-linking. The PTMC membranes were prepared in a similar manner as described in previous studies.16,17
The X-ray microtomography (μCT) images of PLCL and PTMC membranes were acquired by using commercial Zeiss Xradia MicroXCT-400 (Zeiss, Pleasanton) system (Fig. 1). PLCL and PTMC membranes were imaged, respectively, with the following parameters: 60 kV source voltage, 10 W tube power; 40 mm source-to-object distance; 8 mm object to image-receptor distance; 20 × , 10 × objective; 2 binning; 1600 projections; full 360° projection circle; and 5.0, 2.5 s exposure time. The three-dimensional image stacks were reconstructed using Zeiss Xradia XRMreconstructor software (8.1; Zeiss) resulting in 1.1 and 2.3 μm isotropic voxel sizes and the data were visualized in Zeiss Xradia TXM3DViewer (1.1.6; Zeiss).
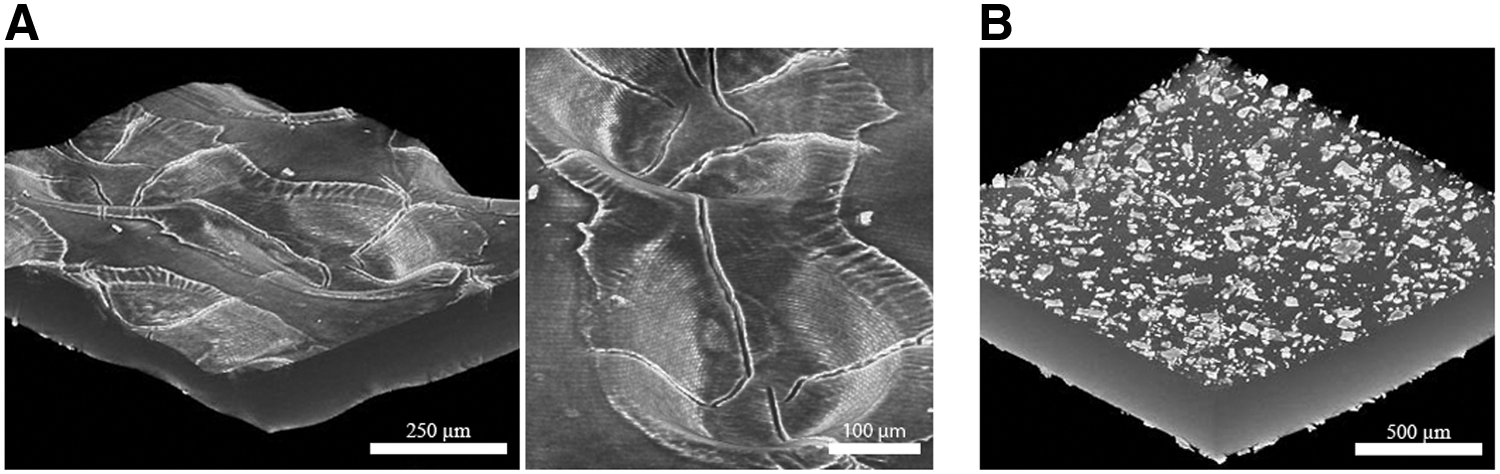
The PLCL
In vitro cell culture
For this study, human urothelial tissue samples were isolated during a routine surgery from one pediatric patient in the Tampere University Hospital with the approval of the Ethics Committee of Pirkanmaa Hospital District, Tampere, Finland (R071609). Further, the urothelial cells were isolated and expanded as previously described.10,21 PLCL and PTMC membranes were attached to the cell culture devices (CellCrown48, Scaffdex, Tampere, Finland) and preincubated for 24 h in urothelium medium containing EpiLife (Invitrogen, MA) supplemented with 1% of EpiLife Defined Growth Supplement (EDGS; Invitrogen), 0.1% of CaCl2 (Invitrogen), and 0.35% of antibiotics (100 U/mL penicillin and 0.1 mg/mL streptomycin; Lonza, BioWhittaker, Verviers, Belgium).
In vitro attachment and viability
The cell attachment was verified by determining the DNA amount using CyQUANT Cell Proliferation Assay kit (Invitrogen). Briefly, 20,000 urothelial cells from one patient were seeded on to three parallel PLCL and PTMC membranes and cultured for 24 h. The cells were lysed with 0.1% Triton-X-100 buffer (Sigma-Aldrich) and stored at −70°C until analysis. The samples were thawed and 20 μL of each sample was mixed with 180 μL of working solution containing CyQUANT GR dye and lysis buffer. The fluorescence at 480/520 nm was measured with a multiplate reader (Victor 1420 Multilabel Counter; Wallac, Turku, Finland).
To verify the viability of hUCs on PLCL and PTMC membranes, we used qualitative live/dead fluorescent staining. The urothelial cells from one patient, 30,000 cells/cm2, were seeded on to two parallel membranes and the viability of urothelial cells was verified after 1 and 2 weeks of cell culture as described before.10,11 Briefly, the cells were incubated at room temperature with a mixture of 0.25 μM calcein AM (green fluorescence; Molecular Probes, Waltham) and 0.3 μM ethidium homodimer-1 (red fluorescence, EthD-1; Molecular Propes) for 30 min. A fluorescence microscope (IX51S8F-2, camera DP71; Olympus, Tokyo, Japan) was used to image viable cells (green fluorescence) and dead cells (red fluorescence).
Quantitative real-time PCR
The relative expression of urothelium marker genes was studied after 14 days of cell culturing on PLCL or PTMC with quantitative real-time reverse transcription–polymerase chain reaction (qRT-PCR). The cell culture polystyrene (PS) served as a control material. For the experiment 50,000 cells/cm2 from one patient was seeded on to three parallel PLCL, PTMC, or PS wells and cultured until analyses. First, the total RNA was isolated with Nucleospin kit reagent (Macherey-Nagel GmbH & Co. KG, Düren, Germany). Thereafter, the RNA was reverse transcribed to cDNA using the High-Capacity cDNA Reverse Transcriptase Kit (Applied Biosystems, Life Technologies). The expression of cytokeratin (CK) 7, CK8, CK19, uroplakin (UP) Ia, UPIb, and UPIII was analyzed. The expression data were normalized to the expression of housekeeping gene RPLP0 (large ribosomal protein P0). The sequences of primers (Oligomer Oy, Helsinki, Finland) and the accession numbers are presented in the Table 1. The qRT-PCR mixture contained cDNA, forward and reverse primers, and SYBR Green PCR Master Mix (Applied Biosystems). The reactions were conducted with AbiPrism 7000 Sequence Detection System (Applied Biosystems) with initial enzyme activation at 95°C for 10 min, followed by 45 cycles at 95°C for 15 s and 60°C for 60 s. The previously described mathematical model was used to calculate the relative expression. 22
In vivo experiment
The animal experiment was conducted under the license of the Board of Animal Experiments (ESLH-2009-06718/Ym-23), and the National Research Council's Guide for the Care and Use of Laboratory Animals was followed. Adult male New Zealand White rabbits (n = 34, Harlan Laboratories, The Netherlands) were housed in the Animal Laboratory of the University of Tampere throughout the study. The rabbits were divided into the following three reconstruction groups: 15 rabbits with a PLCL membrane, 15 rabbits with a PTMC membrane, and 2 rabbits serving as a control group with urethral mucosa for reconstruction.
First, the rabbits were weighed and then anesthetized using a combination of 0.3 mg/kg medetomidine (Domitor, Orion, Inc., Espoo, Finland) and 0.3 mg/kg ketamine (Ketalar, Parke Davis, Inc., Caringbah, NSW, Australia), which were given intramuscularly. Additionally, the prophylactic antibiotic 2.5 mg/kg enrofloxacin (Baytril vet 50 mg/mL; Bayer Animal Health GmbH, Leverkusen, Germany) was given intramuscularly prior to the surgery. The rabbits were catheterized using 8F catheters (Mediplast AB, Malmo, Sweden). An incision ∼2 cm long was created in the rabbit skin from the inguinal to the penile region, and the urethral mucosa was exposed (Fig. 2A). First, a 2 × 1-cm oval-shaped defect was created to the urothelial mucosa of the rabbit's anterior urethra. Holding sutures made of 6/0 nonabsorbable polypropylene (Premilene®; B. Braun Medical AS, Melsungen, Germany) were placed in every defect quarter and left in place after the operation as marking sutures. The defect site was replaced with the same sized on-lay PLCL or PTMC membrane (Fig. 2B), which was tailored just before transplantation using surgical scissors. The biomaterial membranes were sutured to the free edges of the urothelial mucosa with bioabsorbable 6/0 poly(p-dioxanone) sutures (PDS II®, Ethicon, Inc., NJ) and aligned with the catheter (Fig. 2C). For control rabbits, we did a sham surgery, removed a similar patch of urethral mucosa and sutured it back as a graft to the defect area to investigate the inflammation caused by the operation and the absorbable suture. After the suturing, the skin wound was closed with an intracutaneous suture using absorbable 4/0 polyglactin 910 sutures (Vicryl®, Ethicon, Inc., NJ), and the catheter was removed. The adequate analgesia was administered, and all the rabbits received 4 mg/kg carprofen (Norocarp vet, Norbrook Laboratories Ltd., Newry, Northern Ireland) and 0.05 mg/kg buprenorphine (Temgesic, Schering-Plough Europe, Inc., Brussels, Belgium) subcutaneously during the operation. The 0.05 mg/kg buprenorphine (Schering-Plough Europe, Inc.) was continued until 24 h after the operation, and the carprofen (Norbrook Laboratories Ltd.) was given daily 2 days after the operation. Pain medication was continued longer, if required. The rabbits in both the PLCL and PTMC groups were followed up for 2, 4, or 16 weeks, individually caged on an ad libitum diet. The sham surgery rabbits were followed up for 2 or 4 weeks.
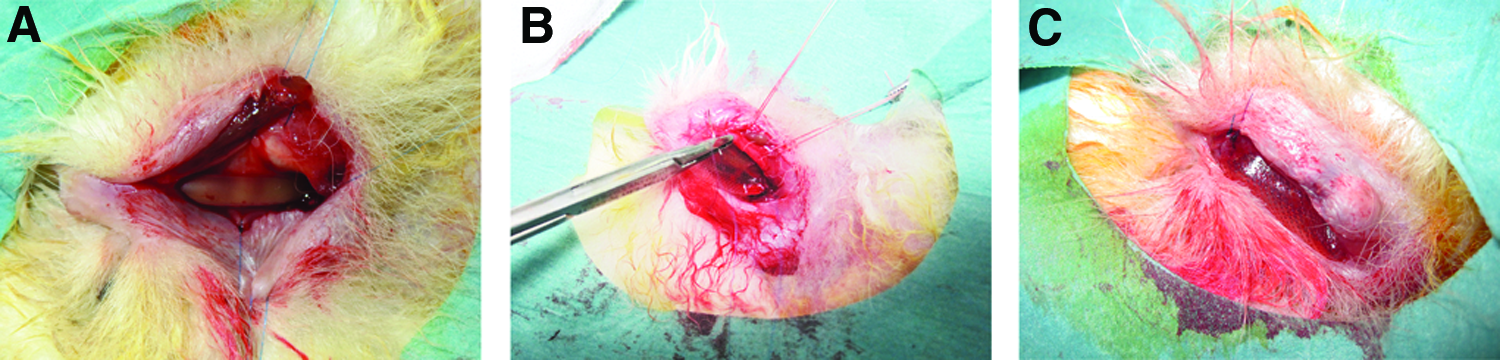
At the beginning of the surgery, the rabbits were catheterized. An incision ∼2 cm long was made in the inguinal region. The urethra was exposed, and a 2 × 1-cm oval defect was created in the rabbits' anterior urethra
In vivo follow-up
After the follow-up, the animals were weighed, anesthetized as described in the In vitro Attachment and Viabilitysection, and subjected to urethrographic examination. The animals were catheterized, and the 8F catheter (Mediplast AB) was fixed with sutures distal from the defect area, which was palpated during catheterization. The urethrographic examination was performed by administering 180 mg/mL iohexol (Omnipaque, GE Healthcare AS, Oslo, Norway) by syringe as a radiocontrast agent via the catheter toward the bladder and by taking simultaneous X-ray pictures (Philips Oralix, Amsterdam, Holland) to detect severe strictures. Severe strictures block urine flow and thus prevent normal urination. After the examination, the animals were euthanized using 1 mg/kg intravenous pentobarbital (Mebunat, Orion, Inc., Espoo, Finland). The defect area was then excised, cut perpendicular from the middle of the reconstructed urethra to get the defect center to the histological analyses, and stored in 4% paraformaldehyde (Sigma-Aldrich) until histolgical analyses.
Histology
Paraformaldehyde-fixed tissue samples from rabbit urethras were embedded in paraffin and stained with hematoxylin and eosin (H&E) (Reagena Oy, Finland) or Masson's trichrome (Sigma-Aldrich) for microscopic examination. Epithelial integrity and structure were determined from the H&E-stained samples 2, 4, and 16 weeks after the operation. Epithelial integrity was categorized as discontinuous or continuous, whereas epithelial structure was categorized as no structure, monolayered or layered, that is, stratified structure. 23 Edema and the presence of inflammatory cells in the H&E-stained samples were evaluated to discover inflammation. Edema was scored from 0 to 3: 0 = none, 1 = mild, 2 = moderate, and 3 = severe. 23 Similarly, the presence of inflammatory cells was scored from 0 to 3. Normal inflammatory cell appearance was scored as 0; less than 25% of all cells was scored as 1; 25–50% was scored as 2, and over 50% was scored as 3. 24 The epithelial integrity and structure and inflammation-related parameters were examined at 40 × magnification. Fibrosis was determined from Masson's trichrome-stained samples and scored. A score of 0 indicated no fibrosis, 1 indicated mild fibrosis (less than 25%), 2 indicated moderate fibrosis (25–50%), and 3 indicated severe fibrosis (more than 50%). 25 The histological examination was performed without knowing the group to which the sample belonged.
Immunohistochemistry
Immunohistochemistry with the pancytokeratin marker was used to study the urothelial epithelium after 2, 4, and 16 weeks of follow-up. Briefly, the samples were fixed with 5% paraformaldehyde and embedded in paraffin. The antigen retrieval was performed by microwaving the samples in 10 mM EDTA buffer (pH 9; Sigma-Aldrich), after which the samples were blocked in 3% hydrogen peroxide (Sigma-Aldrich). The samples were incubated overnight in diluted primary antibody (1:100, AE1/AE3; Thermo Fisher Scientific, MA). On the following day, the secondary antibody (1:200, goat anti-mouse IgG; Thermo Fisher Scientific) was used to detect the primary antibody.
Statistical analysis
Statistics were analyzed using IBM SPSS Statistics version 22 (IBM Corp., Armonk, NY). Edema, inflammation cell appearance, epithelial structure, fibrosis, and cell attachment on membranes were analyzed using the Mann–Whitney U test. Kruskal–Wallis test with Dunn's multiple comparison test was used with qRT-PCR results. Significant differences in epithelial integrity were analyzed using Fisher's test. Statistical significance was set to a p-value of <0.05.
Results
Cell attachment and viability on PLCL and PTMC membranes in vitro
The QyQUANT assay illustrated that there was small, yet statistically significant difference on the hUCs attachment on PLCL or PTMC membranes after 1 day of cell implantation (Fig. 3A, p < 0.05). Live/dead staining confirmed that the majority of cells were viable on both the PLCL and PTMC membranes and that the number of dead cells was negligible after the 1- and 2-week assessment periods (Fig. 3B). According to the qualitative analysis, the number of urothelial cells was notably lower on PLCL compared to the PTMC, especially after 1 week of cell culture.
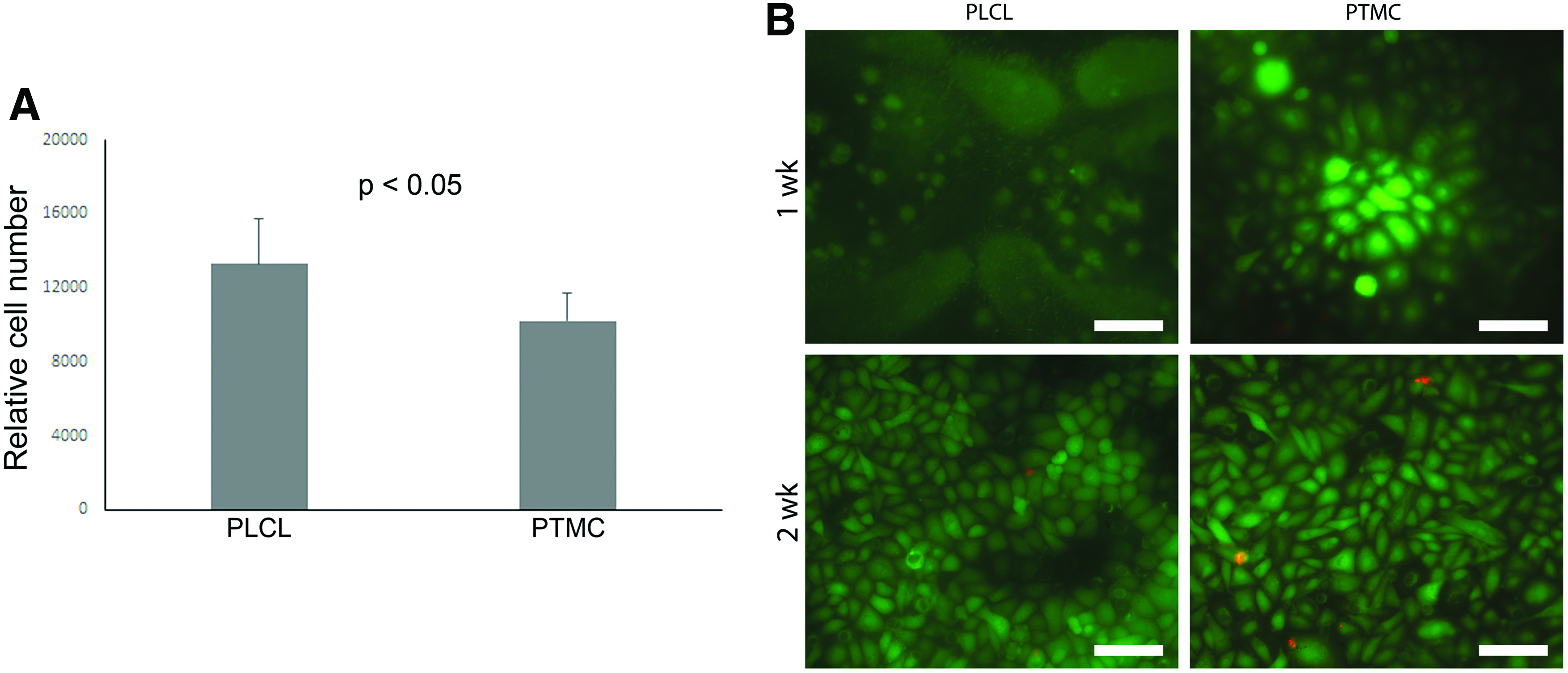
The adhesion of urothelial cells on PLCL and PTMC was assessed after 1 day of cell implantation
Expression of urothelium markers
The expression of different urothelial markers was studied after 14 days of cell culture on PLCL and PTMC membranes with qRT-PCR (Fig. 4). On both PLCL and PTMC membranes, the hUCs expressed CK7, CK8, and CK19, which are known to be present in all layers of multilayered urothelium. On the PLCL, the expression of CK7 and CK8 was statistically higher compared to the PS and PTMC, respectively (p < 0.05). However, the CK19 expression of hUCs was significantly lower on PLCL compared to PS (p < 0.05). Additionally, on the PTMC the hUCs expressed all the studied UPs, UPIa, UPIb, and UPIII, which are more specific markers for urothelial cells. The hUCs on the PLCL expressed only the UPIb marker, whereas, no UPIa and UPIII expression was detected. The expression of UPIa was statistically higher with PS and the expression of UPIb and UPIII was statistically higher with PTMC compared to the PLCL (p < 0.05).
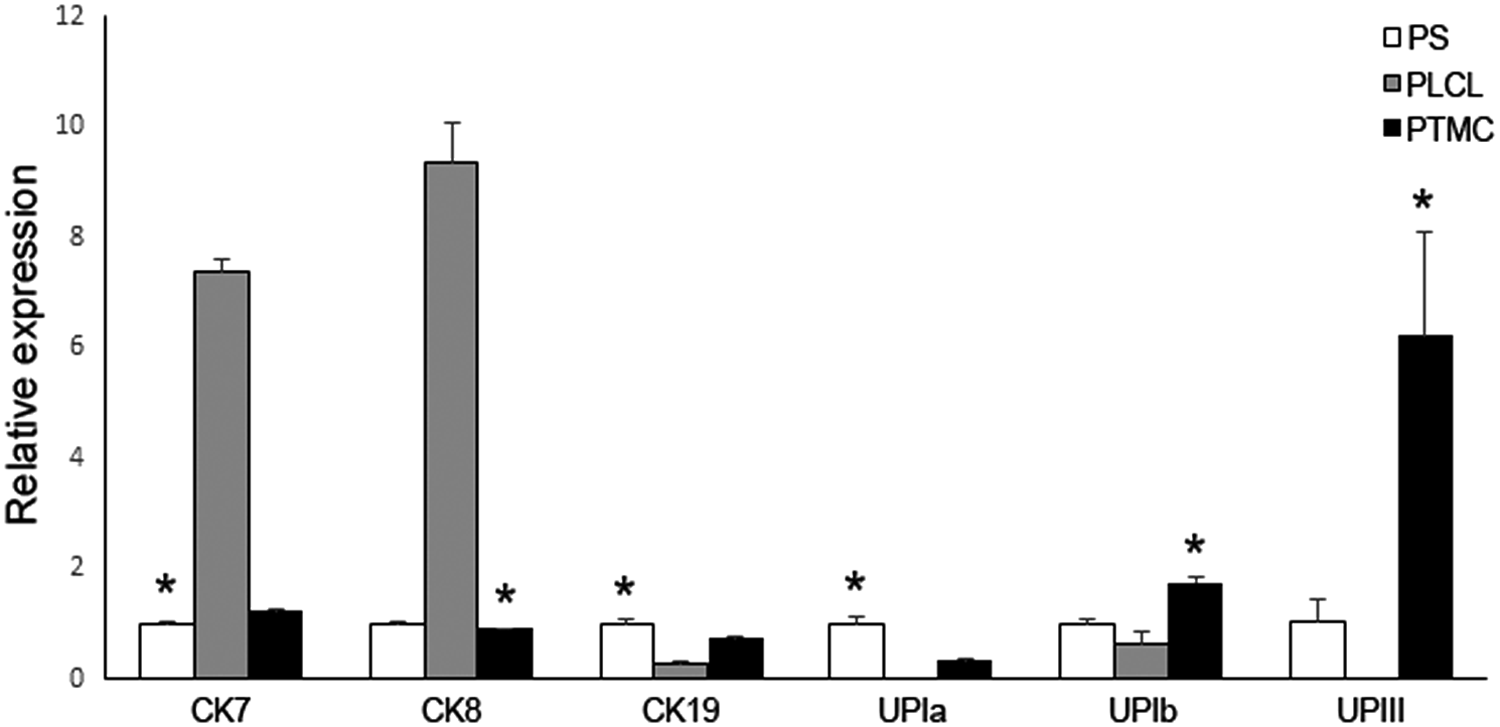
The urothelial cells cultured on PLCL, PTMC, and PS expressed different urothelial markers, CK7, CK8, CK19, UPIa, UPIb, and UPIII, after a 2-week in vitro assessment period. *p < 0.05 with respect to PLCL. CK, cytokeratin; PS, polystyrene; UP, uroplakin.
In vivo experiment
During the operation, the PTMC membranes appeared more flexible and were easier to suture and mold into tubular structures around the catheter compared with the PLCL membrane.
The rabbits recovered well after the operation. Most of the rabbits started to eat and drink normally and urinated spontaneously 1–3 days after the surgery. One rabbit from the PLCL group did not urinate and eat normally until 4 days after the operation. Further, two rabbits from PTMC group died 2 days after the operation, and those rabbits were excluded from the study. Both rabbits underwent autopsy, which revealed no biomaterial related causes of death.
The urethrographic examination performed at 2, 4, and 16 weeks detected no severe strictures, and the radiocontrast agent passed through the defect area in all rabbits (Fig. 5). The postoperative spontaneous urination supported our urethrographic findings. The biomaterials in both the PLCL and PTMC groups could not be seen anymore at the 16-week time point.
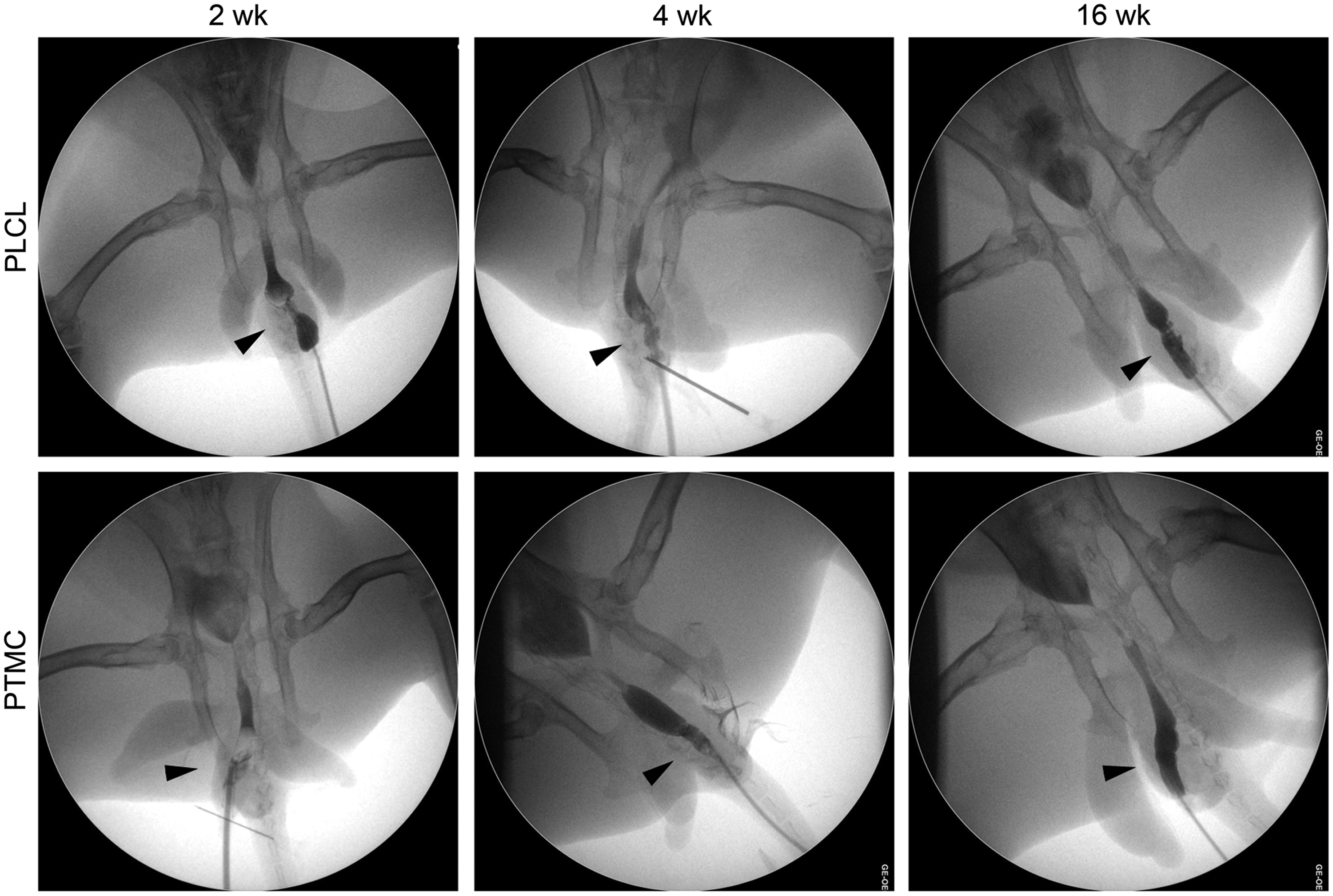
Urethrographic examination illustrated the free passage of the radiocontrast agent through the defect area. After the follow-up, no severe strictures were detected in the PLCL or PTMC biomaterial groups. The arrowhead is indicating the graft area.
Histology
The histological examination showed that the epithelial integrity approached that of the normal urothelial state in both groups (Figs. 6 and 7). By week 16, the epithelium was continuous, and, in the majority of samples, the epithelium was stratified (Table 2). Within the PTMC group, the difference in epithelial integrity between the 2- and 16-week follow-up was statistically significant (p = 0.048). In the sham surgery rabbit group, inflammation was negligible after the 2- and 4-week follow-up (Fig. 8). The biomaterials used in this study caused only mild inflammation throughout the follow-up period. The highest scores of inflammatory cells (score 2 [0–3]) were discovered at the 4-week time point in the center defect area in the PTMC group, but the difference between the groups was not statistically significant (p = 0.310). However, especially in the PLCL group, edema (score 0) and inflammatory cells (score 0) appeared to decrease by the last 16-week time point without a significant difference from the PTMC group (score 1 [0–2] and score 0 [0–2], respectively). No differences in edema or presence of inflammatory cells could be detected in any samples between the groups. Signs of fibrosis varied from mild to moderate during the follow-up. There were no statistically significant differences between the groups. At the 4-week time point, fibrosis was mild in the PLCL group and moderate in the PTMC group (Table 2). In the histological examination, there were no membrane remnants at the 16-week time point in either group.
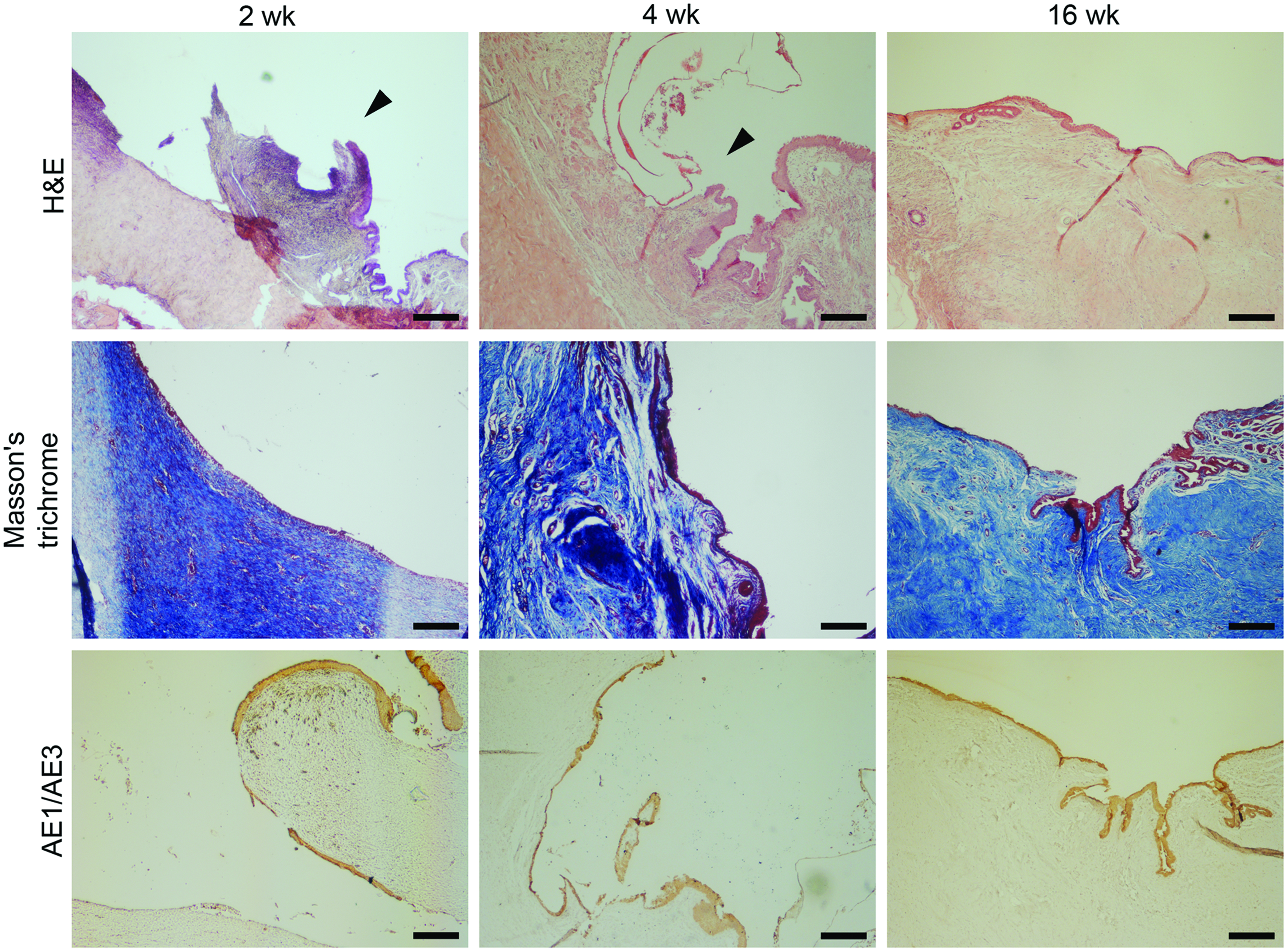
Images show example histological views of the PLCL group at the 2-, 4-, and 16-week (n = 5) time points stained with H&E and Masson's trichrome. The third row of histological images shows pancytokeratin (AE1/AE3)-staining. The implantation area in each panel is located in the centrum of the specimen view. The scale bar is 250 μm and the arrowhead is indicating the margin of natural tissue and biomaterial graft. H&E, hematoxylin and eosin. Color images available online at www.liebertpub.com/tea

Images show example views of the PTMC group at 2-, 4-, and 16-week time points stained with H&E, Masson's trichrome, or pancytokeratin (AE1/AE3). The implantation area in each panel is located approximately in the center of the specimen view. The arrowhead is indicating the margin of urothelium tissue and biomaterial graft and the blue spheres are nonbiodegradable marking sutures. Scale bar 250 μm. Color images available online at www.liebertpub.com/tea

Images show the effect of sham surgery at 2- and 4 week time points. The H&E staining illustrates that the inflammation and fibrosis after 2 and 4 weeks is extremely low indicating the small effect of sham surgery and sutures. Scale bar 250 μm. Color images available online at www.liebertpub.com/tea
Inflammation and fibrosis scores are represented as median and range scores. Parameters related to the epithelium are represented as percentages and sample count. Significance was set to a p-value of <0.05. Epithelial integrity within the PTMC group between weeks 2 and 16 was statistically significant (p = 0.048).
PLCL, poly(
Immunohistochemistry
Immunohistochemical staining with the CK marker (AE1/AE3) demonstrated the formation of de novo urothelium (Figs. 6 and 7). Hence, in the stainings, no differences between the PLCL and PTMC biomaterial groups were detected at any time point. Further, the de novo urothelium developed toward normal stratified urothelium during the assessment period.
Discussion
In this study, we investigated the suitability of the PLCL and PTMC membranes for urethral reconstruction in a rabbit model. Reconstruction of severe urethral defects is problematic because additional nonurological tissue grafts are needed, and those operations are highly susceptible to complications. Furthermore, nonurological grafts should fulfill the versatile challenging requirement, from biocompatibility to formable structure.
PLCL was selected because our previous in vitro studies have shown its suitability as a growth surface for hUCs.10,11 It is a biocompatible biomaterial that has been studied in various soft tissue engineering applications with encouraging results.12,14 Furthermore, Kloskowski et al. have previously demonstrated that PLCL was more suitable for ureter segment reconstruction compared with the acellular aortic arch in a rat model. 26 Additionally, PTMC has been shown to be a biocompatible biomaterial, and it has been studied in particular in soft tissue engineering applications with promising results.15,19 At least to our knowledge, this is the first study comparing the synthetic biomaterials PLCL and PTMC for urethral reconstruction.
We demonstrated that the attachment of hUCs was significantly higher on PTMC compared to PLCL. However, the hUCs retained their viability on both materials, which was expected since both PLCL and PTMC are known to be biocompatible. During this study we also evaluated the phenotype of hUCs after 2-weeks in vitro culturing period on both biomaterials. We analyzed the markers CK7, CK8, and CK19 since those are generally expressed in multilayered epithelium and throughout all layer in urothelium. Further, the UPs were analyzed due to their specificity for superficial urothelial cells.21,27 Both biomaterials appeared to support the maintenance of the hUCs phenotype further indicating their potential for urothelial applications. Interestingly, the PTMC appeared to support the expression of UP markers superiorly compared to the PLCL, however, evaluating the significance of these results requires further in vitro and in vivo studies.
The majority of the rabbits recovered well after membrane implantation and started to eat and urinate within a few days after the operation. One rabbit from the PLCL group had a slight delay in recovering. Two rabbits from the PTMC group died the second postoperative day. These rabbits did not eat after the operation and drank only remotely before they died; however, both rabbits urinated after the operation. The other rabbit had a hematoma at the defect area, but no specific reason could be identified for the death. Nevertheless, we concluded that the deaths were unlikely to be biomaterial-related.
In this study, we also evaluated the applicability of the biomaterial membranes for urological applications. During the operation, PTMC was easier to suture and mold into a tubular structure than PLCL, even though both biomaterials were flexible and easy to handle.
An appropriate biomaterial for urethral reconstruction should not cause disadvantageous tissue effects, such as excessive scar formation, leading to urethral strictures, causing decreased urinary flow and predisposing the patient to urinary tract infections. In our study, the animals were sacrificed 2, 4, or 16 weeks after the operation, and urethrographic examinations were performed to ensure the openness of the urethra. At the 2-week time point, a narrowing of the urethra was detected in both biomaterial groups, but this may be due to the inflexibility of the biomaterial membranes compared to the native urothelial tissue. No severe strictures were detected at the 16-week time point. However, in the PLCL group, a mild narrowing of the urethra was detected at the proximal defect area, whereas the distribution of the radiocontrast agent was uniform when the urethra was reconstructed with the PTMC membrane.
According to a visual inspection after sacrifice, both the PLCL and PTMC membranes were still present after the 4-week follow-up but had fully degraded by 16 weeks, which is consistent with previous degradation studies.11,17,18 However, at the 2- and 4-week time points, the PLCL membrane appeared to be more unevenly degraded or more peeled off than the PTMC membranes. PLCL was more rigid than PTMC at 2 and 4 weeks when the defect area was revealed. However, visual inspection showed no substantial differences in the de novo urethral membrane after the 16-week assessment period, and there were no macroscopically observable strictures or fibrosis.
The histological results based on the H&E and AE1/AE3 staining showed that the urothelium in both groups developed toward a normal urothelium with regards to integrity and epithelial structure. The positive staining of AE1/AE3 further illustrates the epithelial phenotype of these cells. We hypothesized that the urothelial cells could migrate on the biomaterial membranes from the margin of the graft from the intact urothelium. The development of epithelial integrity was significant in the PTMC group between the 2- and 16-week follow-ups. After 2 weeks, the margin between the defect area and the normal urothelium was evident in both biomaterial groups. However, the defect margin was no longer distinguishable after 16 weeks, and the de novo epithelium showed stratification characteristic of the urothelium.
Invasive treatment always causes fibrosis of some degree. The fibrotic changes on a histological level in our study varied from mild to moderate. The level of observed fibrosis did not cause clinically demonstrable problems, such as urinary retention. Our urethrographic examination proved that the postoperative urethral lumen was open and that the animals started to urinate rapidly after the operation, in other words no severe strictures were detected. In urothelial tissue engineering, the studied biomaterials should not cause severe inflammatory responses. 3 Regarding PTMC, van Leeuwen et al. concluded that the tissue reaction on a histological level to PTMC membranes implanted in the mandible was mild and transient. 16 There are no previous data on the tissue response of the urethra to PTMC, but our low inflammatory cell and edema counts suggest that the reaction is mild. Likewise, our results showed mild inflammatory tissue responses in the PLCL group as well. Some results show that PLCL causes an even milder cellular inflammatory response than collagen, which might be related to the slow biodegradation process of PLCL. 28 Based on our histological evaluation, both PLCL and PTMC caused only mild inflammation throughout the follow-up, which establishes their potential.
Conclusion
Our aim was to investigate and compare the use of PLCL and PTMC for urethral reconstruction in a rabbit model. In addition, we confirmed the attachment, viability, and phenotype of hUCs on both biomaterials in vitro, which further indicated the excellent biocompatibility of the PLCL and PTMC membranes. Our urethrographic examination results and reversion of spontaneous urination after the operation did not reveal clinically remarkable problems, such as strictures. Further, there were no significant differences between the PLCL and PTMC groups in the integrity or structure of the de novo urothelium, and therefore, both biomaterials could be considered potential for urothelial applications. However, PTMC showed significant development of urothelial integrity. Based on our histological evaluation, both PLCL and PTMC caused only mild inflammation throughout the follow-up. Invasive treatment naturally always causes fibrosis to some degree, but the fibrotic changes on the histological level in our study varied only from mild to moderate, and the fibrosis did not cause clinically demonstrable problems. Both biomaterials showed suitability for this purpose without significant differences from each other. In particular, PTMC, which has not been previously investigated for urethral reconstruction and was easier to handle than PLCL, should be considered as a potential biomaterial for urological tissue engineering. The limitation of this research was that we used unseeded biomaterial grafts, and therefore, our next step is to study cell-seeded PLCL and PTMC grafts for urethral reconstruction. Additionally, in the future it would be beneficial to compare these biomaterials to, for instance, PGA or BAMG, which are one of the most frequently studied biomaterials for urethral tissue engineering with promising results.4,8 Further, it would be interesting to study different composite biomaterials, as PLCL or PTMC meshes combined, for instance, with polyethylene glycol (PEG) hydrogel 29 for urethral reconstruction to facilitate the regeneration of urethra.
Footnotes
Acknowledgments
We most deeply thank our colleagues in BioMediTech, Pirkanmaa Hospital District and University of Twente. We sincerely appreciate the expertise of pathologist Marita Laurila, statistician Heini Huhtala, and laboratory technologist Sari Kalliokoski. Without the knowledge and experience of the personnel in the animal laboratory of the University of Tampere, this study would not have been completed. This study was financially supported by the Finnish Research Foundation of Children's Diseases, Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital and The Finnish Cultural Foundation.
Disclosure Statement
No competing financial interests exist.