
Abstract
Traumatic tympanic membrane (TM) perforation is very common in clinical practice. Several biomaterials have been reported to play a role in TM reparation, whereas their functional recovery is limited when used alone. Meanwhile, the administration of biofactors could promote functional recovery, but rapid distribution and short half-time obstruct their application. To study the effect of traumatic TM regeneration, we prepared collagen membrane (CM) integrated with collagen-binding basic fibroblast growth factor (CBD-bFGF) and implanted into the injury site of perforated TM in Sprague-Dawley rats. The study on CBD-bFGF in vitro showed that CBD-bFGF accelerated the proliferation of human fibroblast cell HS-865 biologically and was released from CM gradually. In vivo study, through the gross anatomy, auditory brainstem responses assay, histological staining, and transmission electron microscopy observation at d7, d14, and d28 after the acute TM perforation, we found that CBD-bFGF-integrated CM promoted the healing rate at an early stage (∼7 days), reduced the healing time of perforated TM, and notably retrieved the structure and hearing of TM. These findings suggest that CM modified with CBD-bFGF could be therapeutically appropriate for the treatment of TM perforation.
Introduction
T
For those who cannot heal spontaneously, invasive surgery like myringoplasty or tympanoplasty may be required, which is a costly procedure because of the need of surgery, anesthesia, and hospital admission.3,4 Furthermore, during the period of conservative treatment, the patients need to face many difficulties such as strenuous sports, and blowing and swimming are prohibited. Meanwhile, bad cold should be avoided. Once infection appears, it may result in acute otitis media leading to ear discharge and hearing loss. In addition, tinnitus and hearing loss during the conservative treatment affect the quality of patients' lives socially and psychologically. Therefore, active treatment of traumatic TM perforation is necessary. The paper patch graft technique is an early treatment of traumatic TM perforations in the out-patient department.5,6 The principle of paper patch technique is to guide cell growth and migrate along with paper patch from perforation edge to the center, which can accelerate TM regeneration.1,4,7,8 However, the technique has its limitations. First, healing rate is not 100%; moreover, the paper patch is incompatible, inflexible, easy detached, and not resistant to infection. 7
To overcome the limitations of paper patch, with the development of tissue engineering, various biomaterials such as calcium alginate, 9 collagen,10,11 chitosan,4,12 and silk 13 have been developed in the application of TM regeneration. Among them, collagen is becoming a potential candidate because of its good biocompatibility and ability to promote the growth of cells. Collagen is the body's main structural protein of extracellular matrix that contains cell adhesion signal peptide sequence Arg-Gly-Asp (RGD), which is responsible for cell adhesion, phenotype, and activities. As a major substance of the TM lamina propria, collagen fibers maintain the elasticity of TM and conduct sound. 2
Besides biomaterials developed, biofactors have also been applied in the regeneration of TM perforations, such as hyaluronic acids,14,15 epidermal growth factor,14,16 basic fibroblast growth factor (bFGF),10,17 platelet-derived growth factor, 18 and pentoxifylline. 16 BFGF known as “trauma hormone” is a kind of extensive role of cytokines and promote cells to participate in wound repair.19,20 Particularly, it could promote fibers to build the middle layer of TM. 17 The healing rate of acute, large TM perforation in patients with bFGF was significantly higher than the group without bFGF. 21 However, short half-time and rapid diffusion of bFGF in vivo limit its further use in clinic.
To find a wound-healing platform for TM perforation, we have constructed a specific collagen-binding domain (CBD) fused with bFGF(CBD-bFGF) that can bind collagen scaffold specifically and efficiently. This functional scaffold can localize and release of bFGF steadily with collagen degradation.22–24 Then, we attempted to apply collagen membrane (CM) targeted with CBD-bFGF (CM-CBD-bFGF) to repair traumatic TM perforations in rats. This can make up for the lack of the biomaterial alone and growth factor local dispersion. The capacity of CM-CBD-bFGF for repairing TM perforation was evaluated by histological observation, pathological assessment, and auditory brainstem responses (ABR) assay.
Materials and Methods
Preparation of CBD-bFGF and CM
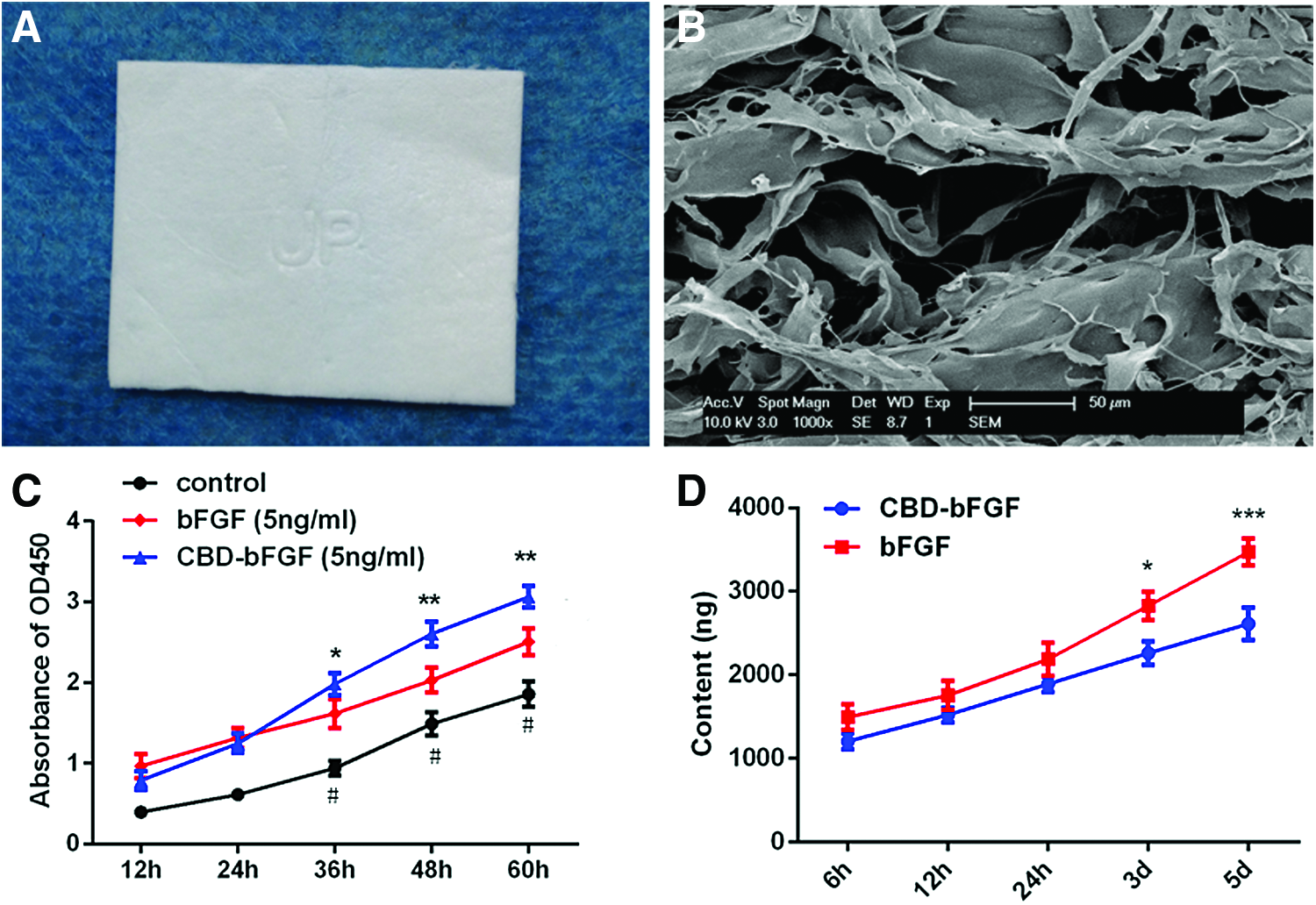
CBD-bFGF protein was prepared as previously described. 23 Briefly, CBD-bFGF protein was expressed in BL21 strain of Escherichia coli (DE3), purified with six histidine tags, concentrated, and quantified. The bovine-derived type-I CMs were obtained from the Zhenghai Biotechnology Company (Shandong, China) and have porous stereoscopic structure (Fig. 1A, B). The sterilized membranes were cut into pieces (diameter = 2.5 mm, thickness = 0.2 mm) for further use.
The characters and biological activity of CM-CBD-bFGF.
The biological activity of the CBD-bFGF
Human fibroblast cells HS-865 (the Cell Bank of the Chinese Academy of Sciences, Shanghai, China) were used to evaluate the biological activity of CBD-bFGF. Cells were seeded (2000 cells/200 μL/well) in 96-well plates and cultured in DMEM containing 10% fetal bovine serum with or without CBD-bFGF (5 ng/mL) and commercial bFGF (5 ng/mL, PeproTech) for 12 to 60 h. To explore the proliferation of HS-865, 4 h before cell culture stopped, the Cell Counting Kit Reagent (CCK-8, 20 μL/well, Dojindo, Japan) was added into wells. The optical density value of the content in each well, 4 h later, was read at 450 nm by microplate reader (BioTek).
The binding and release assay of CBD-bFGF
CBD-bFGF or commercial bFGF (5 μg/piece) was loaded on the CMs. Then, CMs were put into Eppendorf tubes and incubated with 100 μL phosphate-buffered saline (PBS) at 37°C for 6 h to 5 days. The total proteins in the solution were measured by the Bicinchoninic Acid protein assay reagent (Santa Cruz Biotechnology).
Animals and surgical procedure
The experimental protocols were licensed by the Animal Ethics Committees of Soochow University (Approval No. SU 2014-10-022) and all the procedures followed the Guide for the Care and Use of Laboratory Animals of the US National Institutes of Health (NIH).
Male Sprague-Dawley (SD) rats (250–300 g, Shanghai SLAC Laboratory Animal Co. Ltd, Shanghai, China.) were maintained in the animal facility of the Soochow University and fed with water and food at room temperature (20–24°C). Before the experiment, both ears of each animal were checked by a surgical microscope (Leica, Germany) to exclude middle ear diseases. All the surgical procedures were conducted under general anesthesia with 3% pentobarbital sodium salt (1 mL/kg of body weight, Merck, Germany). Bilateral TM perforations in the anterior half of the pars tensa, measuring 2 mm in diameter, were made by a sterile needle without injuring the umbo/malleus attachment. Seventy-two rats with traumatic TM were randomly allocated into three groups (24 rats/group), one implanted with CM with CBD-bFGF(2 μg/piece, CM-CBD-bFGF group), one with CM with normal saline (CM group), one group without any intervention for spontaneously healing (control group). In addition, a group of rats (n = 12) were named as sham group (without any perforation and CM implantation). Collagen patches were inserted onto the TM perforation using on-lay myringoplasty. Ofloxacin ointment (Tarivid Ophthalmic ointment; Santen Pharmaceutical Company) was applied to the membrane to contact the entire margin of perforation. Specimens were collected at day d0, d7, d14, and d28 after injury for further study.
Gross observation by microscopy
To examine the TMs healing, TM from each group at different time points was observed. The images were acquired by the surgical microscope (Leica, Germany). Two independent observers were requested to observe perforation closure, infection, and thickening blindly. In cases where the perforation was not clearly observed, the patches were lifted off. The healing status of the perforated TMs was evaluated as complete closure or unclosed in each group, and recorded as complete closure number/total number.
ABR
Hearing sensitivities were assessed by ABR thresholds (Otometrics ICS Chartr EP, Denmark). 25 Rats were anesthetized and tested in a soundproof room. Needle electrodes were placed subcutaneously at the scalp vertex (active electrode), both mastoids (reference electrode), and the nose tip (ground electrode). The test stimuli click (low frequencies less than 4 kHz) were presented through an insert earphone. The resulting signal was bandpass filtered (100–3000 Hz), amplified (10,000 × ), and delayed (0.1 ms). Animals were presented with stimulus intensity series from 80 to 0 dB sound pressure level in 10 dB decrements. Until the threshold decrements became 5 dB, a total of 500 responses were averaged over a 10ms analysis period. The thresholds were defined as the lowest intensity to elicit reproducible ABR waveform with typical wave III morphology.
Histological evaluation, immunohistochemistry, and transmission electron microscope
Tympanic bullae were obtained immediately from the rats after euthanasia and fixed in 10% neutral buffered formalin for 24 h. The TMs were removed from the bony annulus and dehydrated in a series of graded alcohols, embedded in paraffin wax, transversely sectioned at a thickness of 4 mm, and stained with Hematoxylin and Eosin (H&E). Masson's Trichrome staining was used to further display the morphology of collagen fibers. For immunohistochemistry, slides were dewaxed in xylol, dehydrated in ethanol, and rinsed with PBS, followed by blocking with goat serum. Sections were incubated in a solution containing anti-rat collagen type II antibody (Cat No.ab7778, Abcam) and visualized by the DAB Kit (Gene, China). The sections of TM were imaged at 400 × magnification by the microscope (Zeiss, Germany).
To find out the microstructure of the healed TM, transmission electron microscope (TEM) was conducted. At d28 after implantation TM samples were collected and fixed in 2.5% glutaraldehyde. After postfixation (1% osmic acid), samples were sectioned and observed with TEM (TECNAI 10, Philips Co., Netherlands) at 80 kV.
Statistical analysis
Healing rate determined by otoscopic observers was compared using chi-square test. Data of ABR were presented as mean ± standard deviation and analyzed by one-way analysis of variance. Statistics were analyzed using the Prism software 5 for Windows. Any p-values less than 0.05 were considered to be statistically significant.
Results
The biological activity of the CBD-bFGF
As shown in Figure 1C, the proliferation curve showed that both CBD-bFGF and commercial bFGF enhanced the proliferation of human fibroblast cells HS-865 significantly compared with medium only after coculture (p < 0.05, respectively). Notably, the proliferation of HS-865 with CBD-bFGF was statistically higher than that with commercial bFGF after coculture for 48 and 60 h, respectively (p < 0.05). It indicated that both CBD-bFGF and commercial bFGF had an effect on the cell proliferation. Moreover, CBD-bFGF has higher biological activity than commercial bFGF.
The binding and release assay of CBD-bFGF
As displayed in Figure 1D, the protein concentration of the commercial bFGF group was significantly higher than that of the CBD-bFGF group in the supernatant at the same time point, starting from 6 h to d5. Interesting, with time going by, the concentration difference of the CBD-bFGF group from the commercial bFGF group became larger and larger after 24 h. Since CM degraded at the same level in the solution, we assumed that commercial bFGF released more than CBD-bFGF, resulting in the concentration difference in two groups. As we expected, this sustained system could significantly slow down the release of bFGF by CBD from collagen scaffolds.
Clinical observation following implantation
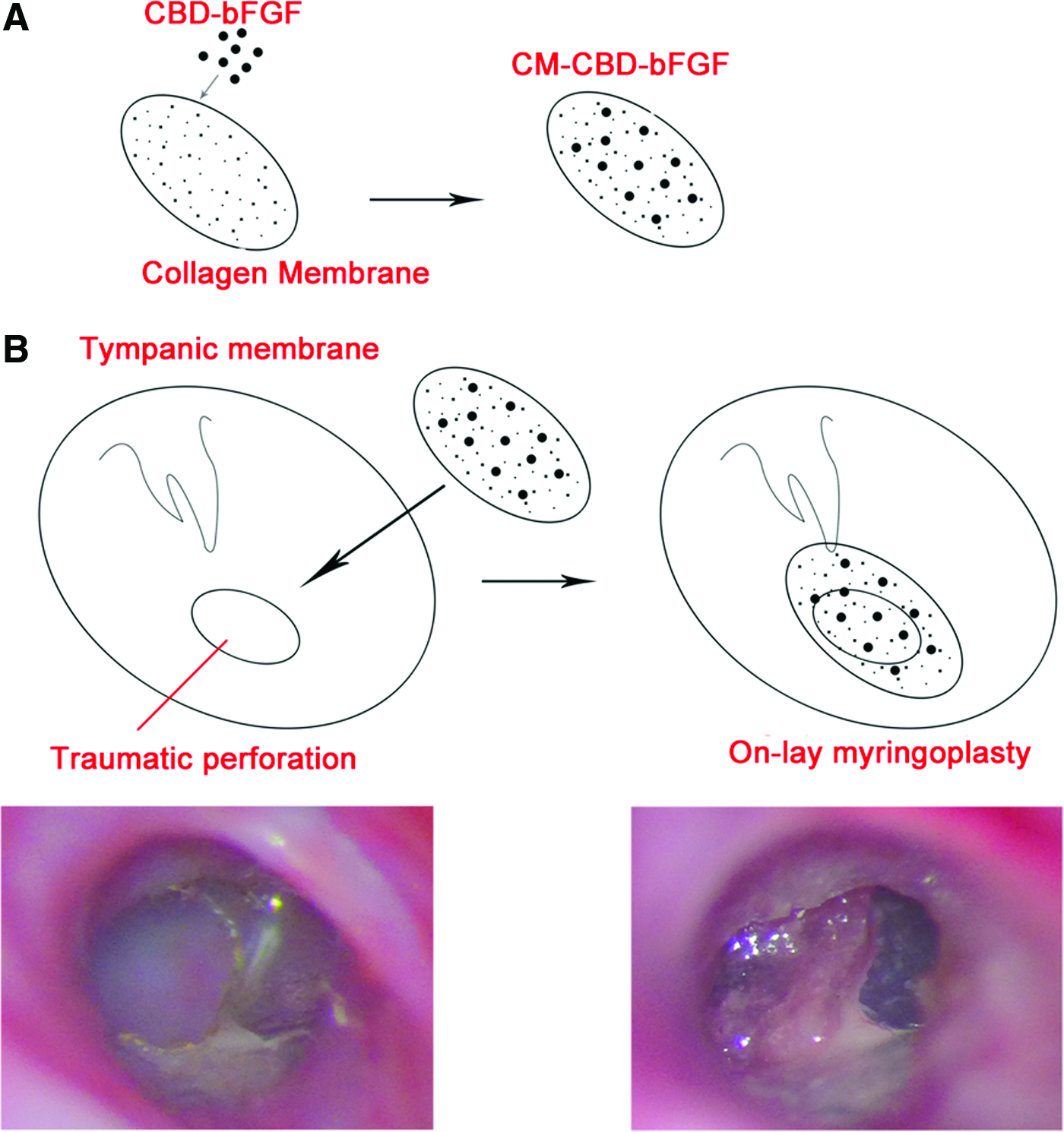
On the basic results in vitro, CBD-bFGF was fused with CMs (Fig. 2A) and the compounds were implanted into injury sites of traumatic TMs (Fig. 2B). After the implantation surgeries, all animals survived. No signs of middle ear infection or complications were observed. It was suggestive that CM has good biocompatibility. The healing rates are summarized in Figure 3A. At d7 after implantation, the healing rate of TM perforations in CM-CBD-bFGF group (14/16, 87.5%) was significantly higher compared with that of CM group (5/16, 31.25%) and control group (2/16, 12.5%) (p < 0.001, respectively). At d14, all perforations from CM-CBD-bFGF group (16/16) were closed, whereas most perforations were healed in the CM (12/16) and control group (11/16). At d28, perforation closures were 100% in CM-CBD-bFGF group, compared with 81.25% (13/16) both in CM and control groups. Compared with the sham rats, the regenerative TMs in CM-CBD-bFGF group turned slightly thicker at d7 and d14 after injury, then changed to transparent and smooth at d28 (Fig. 3B). By contrast, the healed TMs in CM group were quite thickened and scarred at each time point. However, at d28 the scars were lessened compared with the ones at d14. The TMs in control group were more transparent and thinner than those in the other experimental groups at the same time point.
CM-CBD-bGFG was implanted into traumatic TM of SD rats.

The healing status of different groups at different time points.
Hearing recovery detection by ABR
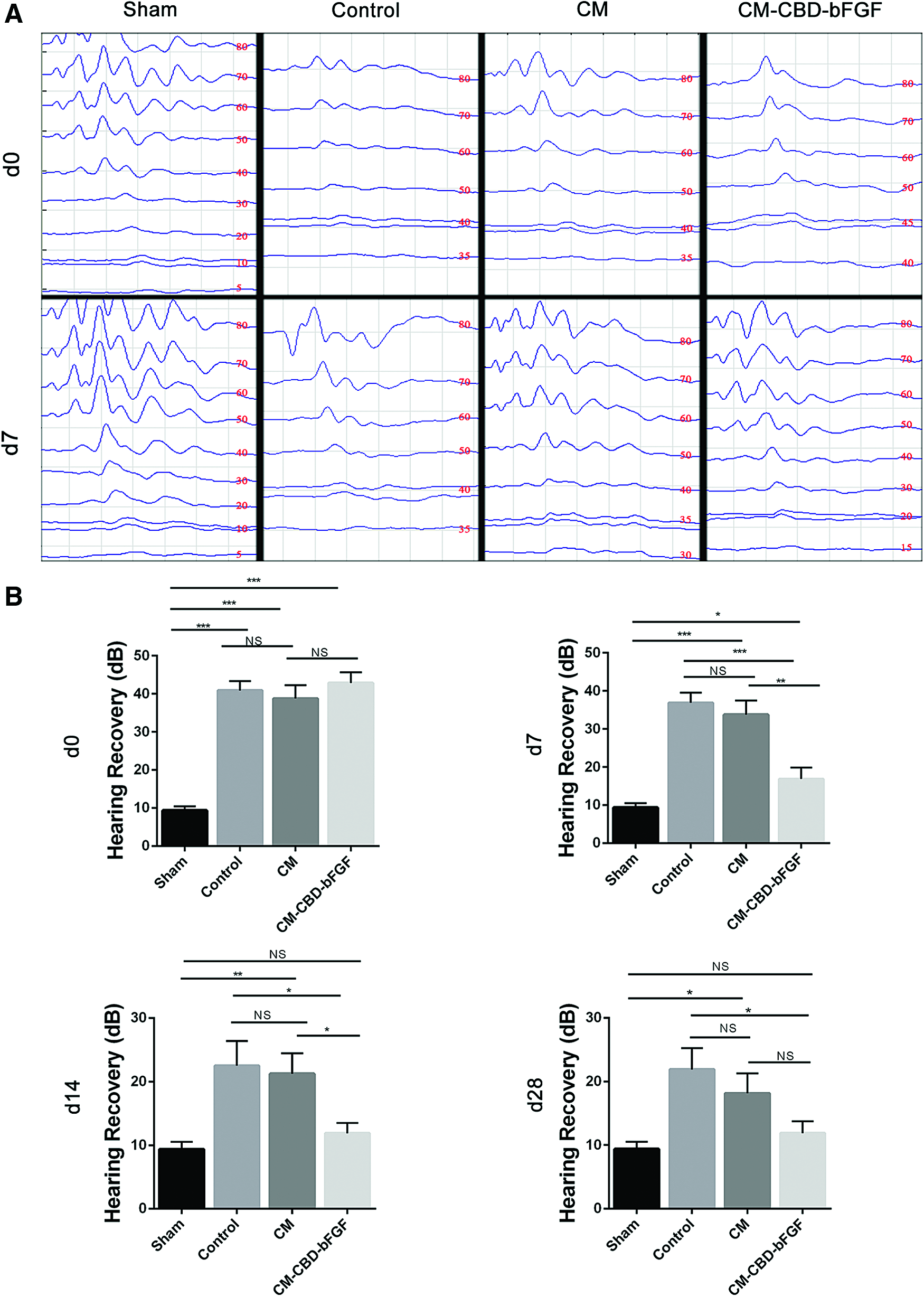
Hearing recovery of the healed TM was evaluated by an ABR (Fig. 4).The average hearing threshold of sham group was 9.375 ± 2.997 dB, whereas the threshold of other three TM-perforated groups was 40.833 ± 5.512 dB (d0, Fig. 4A). It was well demonstrated that TM perforations led to hearing loss. Interestingly, at d7 postinjury, hearing threshold of CM-CBD-bFGF group was 16.875 ± 7.881 dB, suggesting that hearing recovery in CM-CBD-bFGF group was significantly better than in CM group (33.750 ± 9.922 dB, p < 0.01) and in control group (36.875 ± 7.043 dB, p < 0.001). Animals from the CM group (21.250 ± 8.570 dB) and control group (22.500 ± 10.308 dB) recover hearing statistically during 7–14 days (Fig. 4B). Fourteen days after operation, hearing threshold of all groups became steady. At d28, there was no significant difference between two CM-implanted groups. But, hearing recovery in CM-CBD-bFGF group was still statistically superior to the control group.
ABR of different groups at different time points.
Histological evaluation of the TM regeneration
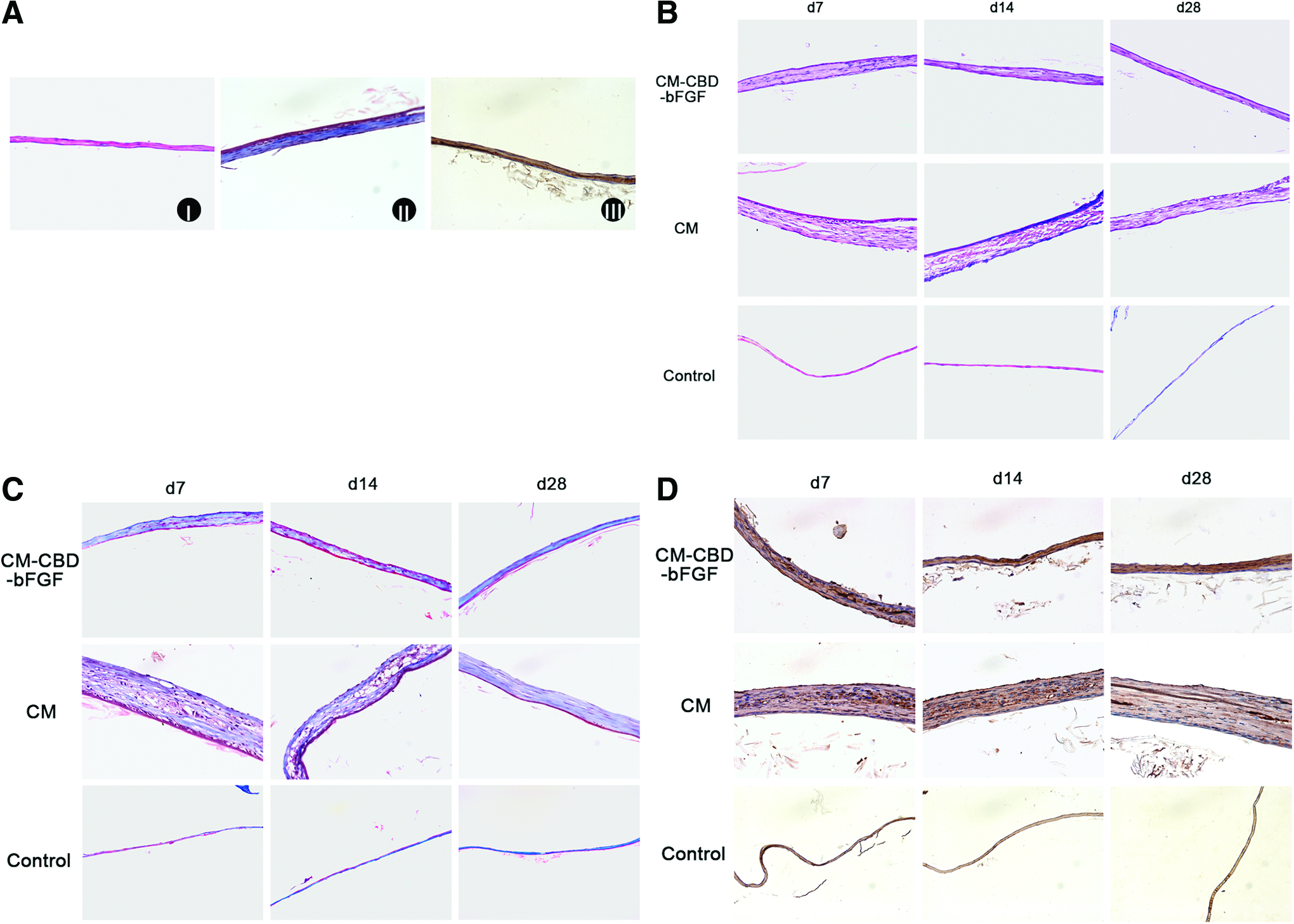
Corresponding to the hearing recovery, the morphology of TMs showed a same trend. As shown in Figure 5B for H&E staining, at different time points after implantation, the TMs from CM-CBD-bFGF group remarkably showed well-organized tissue layers, including an outer epidermal layer, a middle fibrous layer, and an inner mucosal layer, which were similar to the structure of the normal TM (Fig. 5A). Remarkably, the middle fibrous layer was more compact and organized at d28 than at d7 and d14. In the CM group, the healed TMs still showed loose and immature fibrous layers even after 28 days. Expectedly, the control group was thinnest among three TM injury groups, due to poorly developed middle layer.
Representative morphological observation of TMs at different time points (400 × ).
For Masson Trichrome staining shown in Figure 5C, few collagen fibers was observed in the control group. As time went on, the arrangement of collagen fibers in the middle layer was more dense and organized in the CM-CBD-bFGF group than in CM group.
Since collagen type II was the major collagen in the pars tensa of TM, sections were stained with anti-collagen type II specific to rat (Fig. 5D). Collagen bundles were evidenced at all time points in the CM-CBD-bFGF group. Collagen fibers formed a compact and continuous layer between the outer epidermal layer and inner mucosal layer. Especially at d28, collagen bundles were more uniform and organized compared with d7 and d14, closed to the sham group. However, in the CM group, collagen fibers were fewer and more irregular compared with the CM-CBD-bFGF group at the same time point. In the control group, collagen fibers were rare and absent.
Ultrastructure of TM
To further demonstrate the ultrastructure of regenerated TM, TEM was performed. In the CM-CBD-bFGF group, three-layer structure of TM was obvious, and the middle connective layer was compact and had a good arrangement, which resembled the normal TM (Fig. 6). However, in the CM group, the collagen bundles were disordered and loose, accompanying obvious edema. In the control group, the connective layer was unobvious, but slight edema existed.
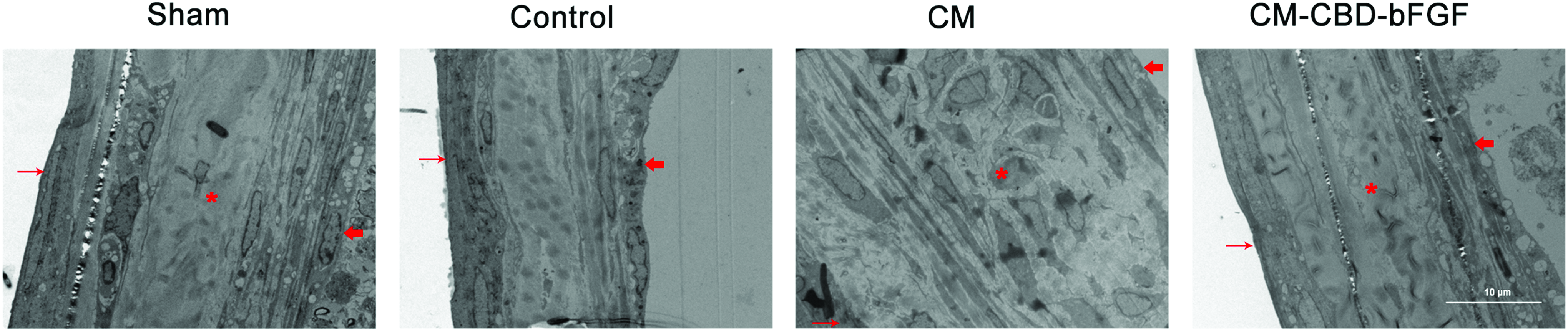
The representative ultrastructure of TMs scanned by transmission electron microscope at d28 (1800 × ). Fine arrow indicated the mucosal layer, asterisk indicated the connective layer, thick arrow indicated the epidermal layer. Color images available online at www.liebertpub.com/tea
Discussion
Traumatic TM perforation is common in otolaryngology outpatients. If a traumatic TM perforation is not healed on time, it can lead to a series of complications such as middle ear discharging, secondary cholesteatoma, and hearing lost. 1 Then, myringoplasty is usually necessary although it indicates operative time and costs, additional incision, and donor site morbidity. Collagen is approved by the Food and Drug administration in clinic, which posses excellent characters. 26 In this study, the rats' implanted CMs as scaffolds showed no inflammatory response and no collagen leftover, further confirming that collagen has good biocompatibility and biodegradability. Collagen acting as scaffolds could provide physical support so that cells can migrate, but the ability of recruiting cells and promoting cell growth is weak. Thus, additional biofactors are needed to synergize the function.
BFGF is a potent growth factor that not only stimulates the proliferation and differentiation of endothelial cells, fibroblasts, and keratinocytes at the perforation margins, but also increases blood supply to the TM. 27 Previous studies have shown that continuous supply of bFGF can induce proper connective tissue with good arranged collagen fibers and promote the remolding of matrix, induce the regenerated TM with a normal three-layer structure.24,27 Lou et al. have applied bFGF in human moderate and large traumatic TM perforations and subacute TM perforations for clinical study, which shortened the closure time.28,29 However, using bFGF locally, only a small amount of bFGF can be retained at the administrated site because of rapid diffusion and short half-life time. Thus, to be released continuously, the conception of bFGF applied on a constant basis to repair TM was proposed in this study. To retain the effective concentration at the target sites, a specific CBD derived from the mammalian collagenase was acquired and integrated with BFGF to specifically bind the collagen. 30 In our previous animal studies, CBD-bFGF effectively accelerated the reconstruction of injured abdominal wall, repaired long facial nerve injury, and restored extrahepatic bile duct defects and the uterine horn defects.23,30–32
In this study, we first evaluated the biological activity of CBD-bFGF with human fibroblast cells HS-865, since fibrous layer is the middle layer of TM maintains structural integrity of the TM. The data in vitro showed that CBD-bFGF had a better biological activity and could sustain specifically to CMs stronger than commercial bFGF.
During the in vivo study, we applied CM-CBD-bFGF to repair TM perforation in SD rats. CM-CBD-bFGF obviously accelerated the healing of TMF functionally. In the CM-CBD-bFGF group, CM acted as a physical scaffold to give the wounded margin support, and not let it dry and shrink. At d7 and d14 in CM-CBD-bFGF group, most of the traumatic TMs were healed. With the passage of time, at d28, healing rate among the three groups showed no significant difference, indicating CM-CBD-bFGF accelerated the regeneration of TM in the early phase. For the structure of regenerated TM, CM-CBD-bFGF promoted TM to regenerate a three-layered structure at the early phase accompanying dense and tight connective tissues. With the extension of observation period, the three-layered structure is more obvious, similar to normal TM. The morphological results suggest that CM-CBD-bFGF promotes collagen arrangement orderly, which is the vital structure of TM. It has been reported that spontaneous TM is easy to be invalidated and perforated again because of lack of middle fibrous layer, which will cause adhesive otitis media and cholesteatoma.2,33
OFLX is a kind of antibiotic and widely used in clinic, including otitis and myringitis. However, several studies suggested that OFLX acts as an inhibitor of fibroblast.34,35 In our study, we used extremely little OFLX ointment to stick the CMs in place during grafting. Although we found that extremely little OFLX did not affect the closure rate of the rats with traumatic TM perforation (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/tea), the inhibition of OFLX to the fibroblasts should be considered because of the high dose and long-term use.
As we know, TM perforation disturbs sound conduct and causes hearing loss. The treatment of CM-CBD-bFGF not only accelerates the healing structure of TM physically, but also promotes the hearing recovery faster and better, probably through the good recovery of middle fiber layer, which was evidenced by H&E staining, Masson staining, immunohistochemistry, and TEM observation. Middle fibrous layer is vital in maintaining the TM integrity. It maintains the mechanical tension of TM, makes sound transmission effectively. 36 In CM and control groups, due to improper middle fibrous layer, TM lacked sufficient elasticity which affects conduction of sound. We compared the hearing of TM-closured rats in control and CM-CBD-bFGF groups at the same time points, and there was no significant difference between them (Supplementary Fig. S2). Collagen fibers are necessary for sound induction, especially for the high-frequency sound over 4000 Hz. 36 ABR assay applies a kind of click stress, where the stimulation frequency is less than 4000 Hz. It can be used to detect average threshold of hearing. However, for detecting high-frequency sound over 4000 Hz, ABR assay may not be the best choice.
CM-CBD-bFGF displayed its attribution to TM regeneration at an early stage in this study. It may be attributed to several mechanisms. Epithelial cells of TM migrated to each other and closed the perforation. Meanwhile, sustained release of bFGF increased the growth of cells and blood vessels, which accelerated the regeneration of TM perforation. Moreover, bFGF enhanced to form the middle fiber layer.
According to our study, CM-CBD-bFGF exhibits several advantages as a potential candidate in clinical application. First, both CM and CBD-bFGF are easy to be obtained. If a patient's fascia fails to repair traumatic TMs in the clinic, to obtain fascia again is more difficult. Besides, temporal myofascia needs additional incision. 37 Second, this treatment could be adopted as paper patch technique, which is carried out in outpatients without hospitalization, anesthesia, and surgery. It may shorten the time of treatment, and reduce the cost. Finally, functional scaffolds are easy to be handled when the outpatients are treated.
There were also some limitations in this study. In this study, CM-CBD-bFGF repaired successfully TM perforation in the rat with acute traumatic TM perforation. But its repair effect on chronic TM perforation remains to be further investigated. In addition, functional scaffolds also need to be applied to large animals in future research. Due to the lack of temporal myofascia in rats and poor adhesion ability of fascia, we did not use the temporal myofascia (the gold standard) as control in this study. 38 Frequent activities of rats made the fascia fall off the margin easily, which influenced the repair effect. Furthermore, the cellular and molecular mechanism of CM-CBD-bFGF repairing TM perforation also requires intense research.
In conclusion, CM targeted with CBD-bFGF was developed and applied to repair the traumatic TM perforation in rats. The CM-CBD-bFGF group notably retrieved the better structure and function of TM compared with spontaneous regeneration and CM groups. CM-CBD-bFGF not only shortened the TM healing period, but also recovered hearing faster and better. It is suggestive that this functional scaffold has a potential clinical application for traumatic TM regeneration.
Footnotes
Acknowledgments
Financial support was provided by the National Natural Science Foundation of China (81101369, 81572131), the Strategic Priority Research Program of the Chinese Academy of Sciences (XDA01030000), and the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.