
Abstract
There is a continuing search for novel synthetic materials as an alternative to autologous bone grafting. Different technologies are explored to promote bone formation, which include the addition of BioGlass™ particles in calcium phosphate (CaP)-based materials and the use of surface modification in the form of submicron surface topographies. In this work, we aimed at comparing the bone formation in a noninstrumented canine interspinous model of moldable formulations of a submicron-surface structured tricalcium phosphate/alkylene oxide copolymer (CaP/AOC) or a tricalcium phosphate/BioGlass/collagen (CaP/BG/C) bone graft material. Intramuscular implantation was carried out as well to evaluate soft tissue responses. Eight mature male mongrel dogs underwent single-level, noninstrumented interspinous implantation, where the bone graft materials were implanted at either side of the spinous processes (L3-L4), with separation by the interspinous ligament ensuring comparison of both materials in each animal (n = 8 per material). The materials were also implanted in paraspinal muscle pouches. Animals were euthanized 12 weeks after surgery and the lumbar spines excised and intramuscular implants retrieved. Undecalcified sections were prepared for histological evaluation and histomorphometry was performed to quantify bone formation and material resorption. After 12 weeks, all submicron structured CaP/AOC implants showed abundant bone formation in the (L3–L4) interspinous space (20.8% ± 6.8%), whereas bone was not found in the CaP/BG/C implants (0% ± 0%). Intramuscularly, the CaP/AOC material triggered significant bone formation (12.0% ± 7.8%), whereas CaP/BG/C did not form any bone. In both the spinal and muscular sites, resorption of the CaP/AOC material was evident by a decrease in Feret diameter of the CaP granules as well as in their histological surface compared with the starting material, whereas CaP/BG/C material had a milder resorption. This study shows that a submicron-surface structured CaP/AOC bone graft material has superior bone-forming properties in both an interspinous implantation model and intramuscularly, as compared with a CaP/BG/C bone graft material.
Introduction
M
Calcium phosphate (CaP) ceramics mimic the chemistry of bone mineral and allow precipitation of bioactive bone-like apatite from body fluids on their surface, which facilitates the infiltration of the host's tissues and cells ultimately leading to bone formation. 2 They are, therefore, the most often used synthetic biomaterials in bone repair,3–7 although their bone regenerative potential is limited due to the lack of osteogenic and osteoinductive properties.
To improve the bone-forming ability of CaP ceramics, osteogenic cells may be introduced into synthetics through cell therapy techniques (e.g., bone marrow aspirate), 8 whereas growth factors (e.g., bone morphogenetic proteins [BMPs] and platelet-derived growth factor [PDGF]) 9 or gene-transfected growth factor-producing cells 10 could also be used. A combination of these approaches may produce a material with comparable bone-forming potential to autograft, but it would still not be the ideal solution because of high costs and complex manufacturing that often lead to not “off-the-shelf” products.
A promising way to improve the bone-forming ability of CaP ceramics is by controlling their physicochemical properties such as geometry, 11 surface microstructure, 12 and chemistry. 13
Surface structural features have particularly been shown essential for enhanced bone formation. For instance, the absence of micropores smaller than 10 μm led to decreased bone formation of CaP ceramics,12,14 whereas decreasing the surface topographical features showed that resorbable submicron structured tricalcium phosphate (TCP) ceramics are osteoinductive in ectopic sites5,15 and have enhanced bone formation in orthotopic sites 16 and a spinal environment. 17 Next to physical modifications of the surface structure, the introduction of ions such as silicon has also been reported to improve the bone-forming ability of CaP ceramics.18,19 Enhanced formation of bone-like apatite and the release of ions (i.e., Ca2+, Na+, and Si4+) are thought to enhance bone formation of CaP ceramics 18 combined with bioactive glasses such as BioGlass™. 20
The objective of the present study was to employ a noninstrumented canine interspinous (IS) implantation model to compare two commercially available moldable synthetic bone graft materials based on either a surface microstructuring technology (AttraX® Putty) or a BioGlass-based technology (Vitoss™ BA). Both materials were also implanted intramuscularly to evaluate soft tissue responses.
Materials and Methods
Bone graft materials and characterization
A calcium phosphate/alkylene oxide copolymer (CaP/AOC) putty material (AttraX Putty®; NuVasive, Inc., San Diego, CA) and a CaP/BioGlass/collagen (CaP/BG/C) composite material (Vitoss BA; Orthovita, Inc./Stryker Corp., Kalamazoo, MI) were obtained from the manufacturers. The CaP/AOC was ready for use, whereas CaP/BG/C was provided in two separated components, BioGlass granules and a CaP/collagen foam strip.
The CaP granules were extracted from the AOC and collagen strip by placing the materials in sinter oven (P320; Nabertherm, Lilienthal, Germany) at 800°C for 3 h and were then characterized. Prior burning out, the samples were weighed to allow the determination of their composition (by weight) in CaP, BG, and organic phases.
The chemistry of the CaP granules was analyzed through X-ray diffractometry (XRD; MiniFlex II, Rigaku, Tokyo, Japan), whereas scanning electron microscopy (SEM, XL30, ESEM-FEG; Philips, Eindhoven, The Netherlands) was employed to observe the surface structure. Granules of both materials were also analyzed with mercury intrusion porosimetry (Micromeritics Instrument Corporation, Norcross, GA) to obtain information on total porosity (i.e., the volume percentage of pores in the materials), macroporosity (i.e., the volume percentage of pores greater than, or equal, to 10 μm in the materials), microporosity (i.e., the volume percentage of pores smaller than 10 μm in the materials), pore size distribution in the ceramic strut and specific surface area.
The organic component of CaP/BG/C is declared as collagen type I by the supplier, and is a well-known material, thus was not further analyzed.
On the contrary, AOC formulation is not precisely claimed by the commercial supplier and is described in the patent US 8,124,687 B2. Therefore, CaP/AOC putty was immersed in chloroform for 12 h to obtain a supernatant, which was then separated from the CaP granules through decantation. The obtained solution was then placed in an oven at 40°C overnight, under vacuum extraction, to finally get a sticky paste-like material (i.e., the AOC component). This paste was subjected to proton nuclear magnetic resonance spectroscopy (1HNMR; Bruker Ascend 400/Avance III; Bruker, Leiderdorp, The Netherlands; d-chloroform, 400 MHz) and attenuated total reflectance Fourier transform infra-red spectroscopy (ATR-FTIR, Spectrum Two; PerkinElmer, Groningen, The Netherlands; ZnSe crystal) to determine its chemistry.
Surgical procedure, necropsy, and tissue collection
A canine IS implantation model 17 was used to compare bone formation with the two synthetic bone graft materials. The model is a modification from Muschler et al.21,22 in that instrumentation was not used to immobilize the spine, whereas the lamina and facet joints were left intact. Soft tissue response to the synthetic bone substitute materials was determined after intramuscular implantation.5,17,23
Surgery was performed on eight adult dogs (mongrel, male, 10–15 kg, 1–2 year old) at the facility of Chengdu Dossy Experimental Animals Co. Ltd. (Chengdu, China), which is licensed to perform animal experiments [License No. SYXK (CHUAN) 2014-189, issued by the management committee for animal experiments of Sichuan province].
All surgeries were conducted under general anesthesia by an abdominal injection of sodium pentobarbital (30 mg/kg body weight; Merck, Darmstadt, Germany). After shaving and cleaning the surgical site with iodine, longitudinal skin and median fascial incisions were made. The paraspinal muscles were retracted to expose the spinous processes at the L3 and L4 levels. Tissues at both sides of the spine were separated from the intra- and supraspinous ligaments to create two implantation beds next to the L3 and L4 spinous processes. After superficial decortication of either side of the spinous processes with a rasp to create punctate bleeding, 5 cc of each graft material (Fig. 1) was placed at either side of the spinal ridge to bridge the two spinous processes according to a randomization schedule.

CaP/AOC was used as received (Fig. 1) and shaped to fit the defect, whereas CaP/BG/C was prepared according to the manufacturer's instructions. In short, 1 g of BioGlass granules were loaded onto the surface of the TCP/collagen foam strip (10 cc), which was then wet with 9 mL physiological saline and mixed thoroughly to uniformly combine the components. Half of the prepared CaP/BG/C composite (i.e., 5 cc, Fig. 1) was shaped into the spinous defect, whereas 1 cc was used for intramuscular implantation as described later. Once both materials were placed in the spinous defects, the muscles from both sides were tightly closed with silk suture.
Subsequently, two paraspinal muscle pouches were created with blunt separation at least 3 cm away from the spinal bone. One cc of CaP/AOC putty or 1 cc of CaP/BG/C composite was implanted in each muscle pouch and sealed with silk suture. The wound was finally closed layer by layer with silk sutures.
Following surgery, the animals were intramuscularly given buprenorphine (0.1 mg per animal; Merck) for 2 days to relieve pain and penicillin (40 mg/kg; Merck) for 3 days to prevent infection. The animals were allowed full weight bearing and received a normal diet. Calcein (10 mg/kg body weight; Sigma-Aldrich, Steinheim, Germany) was intravenously injected 6 weeks after implantation to monitor the onset of bone formation.
Animals were euthanized at 12 weeks by a barbiturate overdose and the lumbar spines excised and intramuscular implants were harvested with surrounding tissues.
Histology and histomorphometry
The explants were trimmed, fixed in 4% formaldehyde (Sigma-Aldrich) and dehydrated through a series of ethanol (Sigma-Aldrich) before embedding in methyl methacrylate (L.T.I., Bilthoven, The Netherlands) using standard techniques. Nondecalcified sections were made using a diamond saw (SP-1600; Leica, Mannheim, Germany) and stained with 1% Methylene Blue (Sigma-Aldrich) and 0.3% basic Fuchsin (Sigma-Aldrich) for light microscopy and histomorphometric analysis. Fluorescent microscopy was performed on unstained sections using an FITC Texas Red filter (band-pass mirror wavelengths of 510–555 and 585–665 nm; Nikon, Tokyo, Japan). The spines were sectioned in the coronal plane, whereas cross sections of the intramuscular samples were made.
Histomorphometric analysis was done on scanned stained slides (DiMAGE Scan Elite5400 II, model AF5400-2; Konica Minolta, Tokyo, Japan). Bone formation was quantified using the histogram function in Adobe Photoshop (CS5, v12; Adobe Systems Benelux BV, Amsterdam, The Netherlands). The area adjacent to and between both (L3 and L4) spinous processes was selected as the region of interest (ROI) and the number of pixels was read. The ROI for the intramuscular samples was determined as the area of material encapsulated by a thin connective tissue layer. After determining the ROI, material and bone were pseudocolored and pixels read as M and B, respectively. The area percentage of bone in the available space was calculated as B × 100/(ROI−M).
Bone contact with the surface of the granules was determined as the ratio 100 × PB/PG, where PB is the perimeter of bone in direct contact with the surface of the granules, whereas PG is the perimeter of all the granules in the ROI. The perimeters were measured using the “analyze/measure” function in ImageJ (v1.43u; NIH, Bethesda, MD).
The in vivo resorption rate was assessed through measuring the change in the histological area (i.e., the amount of pixels belonging to CaP and BG components, normalized to the ROI) in the explants. For this latter measurement, sections made from poly(methyl methacrylate) (PMMA) blocks containing the starting amounts of CaP and CaP/BG in the two grafts (after burning AOC and collagen out at 800°C for 3 h) were used as time zero controls.
A further demonstration of material resorption was given by comparing the average maximum Feret diameters of the CaP granules before and after implantation. For this measurement, sections made from MMA blocks containing the starting ceramic granules were used as time zero controls.
Before extracting the diameters, all images (at least three slides of each sample) were preprocessed to remove background noise and objects of no interest (e.g., bone tissue) using Adobe Photoshop. Afterward, by using ImageJ, the images were converted into a binary format and analyzed using the “analyze particles” algorithm to finally measure the maximum Feret diameters. The total number of granules measured was about 2000 and the diameters were expressed as mean and standard deviation. Diameters were taken of the longest and shortest length of the granules, provided that they were perpendicular with each other. However, they could be measured only for CaP/AOC samples because severe fragmentation of the CaP granules in CaP/BG/C rendered it impossible to adequately determine their diameters.
Statistical analysis
Statistical analysis was performed using the two-tailed t-test with significance defined as p < 0.05. The power of both spine and muscular experiments was determined with a post hoc power analysis (two-tailed t-test for difference in mean) using the freeware G*Power software. 24
Results
Characterization of the bone graft materials
After burning out AOC and collagen, the content by weight of each component in the two grafts was determined (Table 1). X-ray diffraction showed that the ceramic component in CaP/AOC was comprised of tricalcium phosphate (96% wt.) with a minor phase of hydroxyapatite (Fig. 2a and Table 1), whereas the ceramic component in CaP/BG/C was pure tricalcium phosphate.

CaP, calcium phosphate; TCP, tricalcium phosphate; HA, hydroxyapatite.
Scanning electron microscopy revealed that the CaP of both materials had a different surface topography and consisted of grains that were different in size (Fig. 2c, d). The ceramic from CaP/AOC had submicron-sized grains (0.8–1.1 μm) and pores (0.3–1.1 μm), whereas the grain and micropore size of the ceramic in CaP/BG/C were 1.9–3.1 and 0.5–4.5 μm, respectively. These findings were corroborated by the mercury intrusion data (Fig. 2b and Table 1), which demonstrated that the ceramic phase of CaP/AOC had a significant larger component of submicron-sized pores than the ceramic in CaP/BG/C.
As already mentioned earlier, collagen type I is the organic component of CaP/BG/C material (Table 1). The binder of CaP/AOC was identified (through 1HNMR and FTIR, Fig. 2e, f) as a mixture or copolymer of poly(ethylene glycol) (PEG) and poly(propylene glycol) (PPG) (Table 1), confirming that AOC is a poloxamer-based formulation as already published elsewhere. 25
Surgery
Both materials were moldable and could be handled in an acceptable fashion during implantation. However, during the preparation of CaP/BG/C composite, it was observed that it decreased its volume of about 30% when it was hydrated with physiological saline. Afterward, we could cut the obtained CaP/BG/C composite into a 5 cc sample (for the spine site, Fig. 1) and a 1 cc sample for the intramuscular implantation. The surgical procedure was uneventful and no postoperative complications were observed. One animal died after 9 weeks due to causes unrelated to the experiment and was excluded from the study.
Histology and histomorphometry of the IS implants
After 12 weeks of implantation, the CaP/AOC implants had largely retained their shape and were larger in volume as compared with the CaP/BG/C implants that seemed to have collapsed (Fig. 3). Formation of new bone tissue was observed throughout the CaP/AOC implants (20.8% ± 6.8% in the available space of the ROI, with a bone/granule contact of 24.1% ± 5.9%), whereas it was absent in CaP/BG/C implants. Bone was not homogenously distributed between L3 and L4 in the CaP/AOC implants and solid spinal fusion was therefore not achieved (Fig. 3).
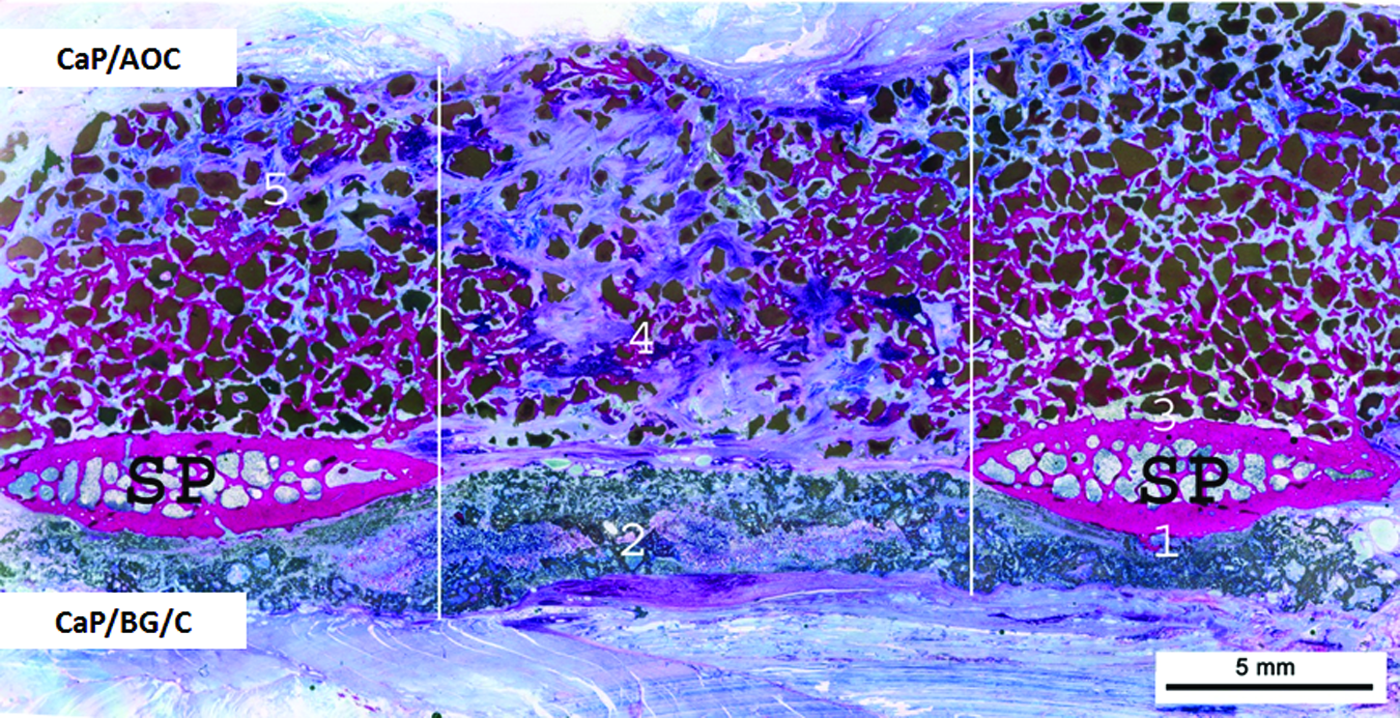
A histological overview (coronal plane) of CaP/AOC (upper) and CaP/BG/C (down) implanted in the spine region of dog for 12 weeks, showing bone formation in CaP/AOC and no bone in CaP/BG/C (nondecalcified section; 1% Methylene Blue and 0.3% basic Fuchsin staining; SP: spinous process; the region between the lines is the region of interest for histomorphometrical evaluation regarding bone formation and ceramic resorption). The numbers 1–5 on the slide indicate the regions whose details are shown at higher magnification in Figures 4–8. Color images available online at www.liebertpub.com/tea
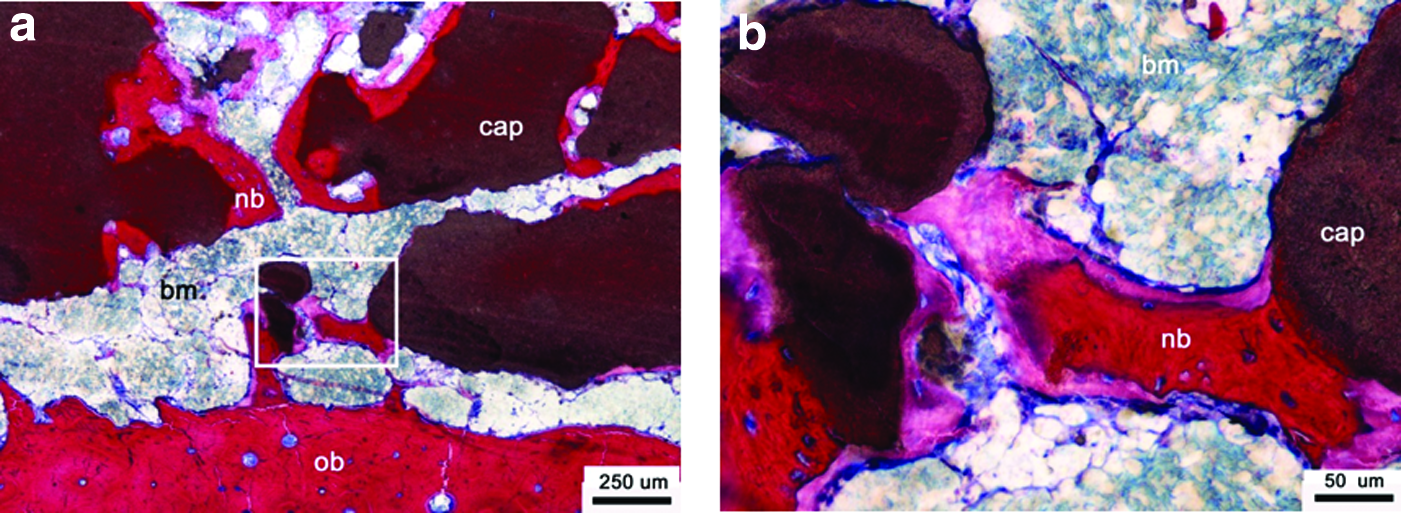
In particular, more bone tissue formed in the regions next to the spinous processes (Fig. 4), whereas less was seen in the central area between both processes. In this central area, fibrous cartilage tissue formation was often detected (Fig. 5). Interestingly, bone formation also occurred far away from the host bone bed of the CaP/AOC implants. When observed in detail, the regions closest to the spinous processes presented osteoid, mineralized bone, and bone marrow (Fig. 4), whereas further away from the host bone bed also fibrous cartilage was observed (Fig. 5a).
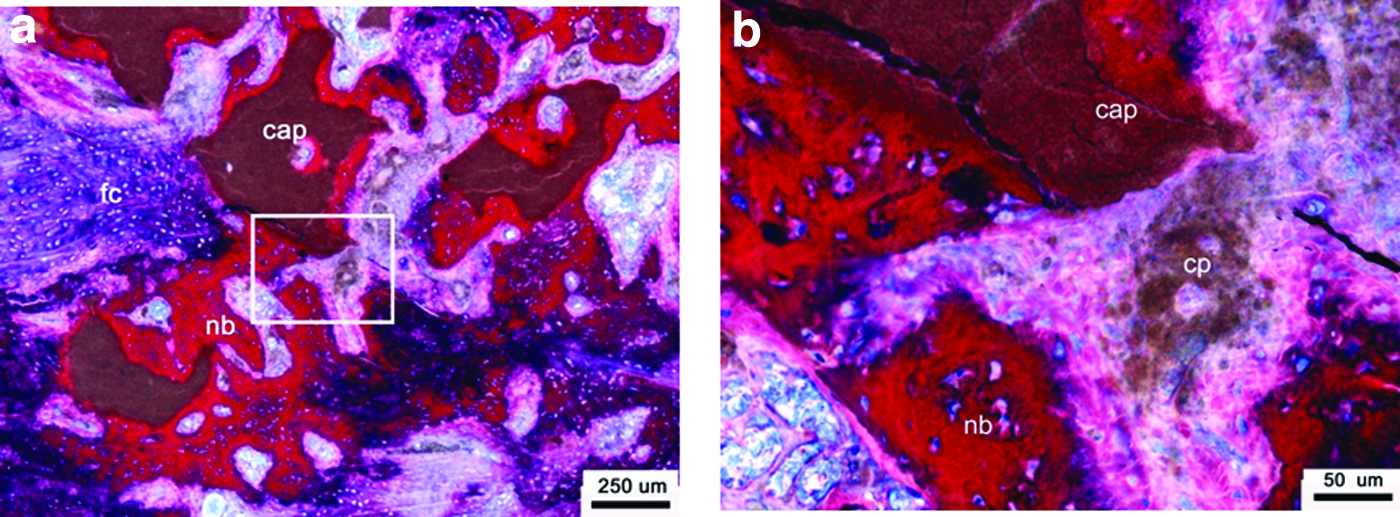
Resorption of the ceramic granules in CaP/AOC implants was more pronounced in sites distant from the host bone as indicated by the presence of small fragments taken up by giant cells (Figs. 5 and 6). Quantitative measurements on the CaP granules showed a 50.8% and 54.9% reduction in their histological area and Feret diameter, respectively, compared with the preimplantation samples (Table 2). These results confirm that resorption of the ceramic granules in CaP/AOC spine explants occurred over a time span of 12 weeks.

The statistical power was calculated for the bone formation in each experiment with post hoc statistical power analysis for t-test of means between two independent groups (significance level at 0.05); the power analysis results show that a number of seven animals, carrying both materials, is sufficient in this study for both the muscular and spine experiments.
As histologically quantified through the area compared to the starting controls.
As granules were severely fragmented, the Feret diameter could not be measured.
Traces of bone formation were observed in the close vicinity of the spinous processes.
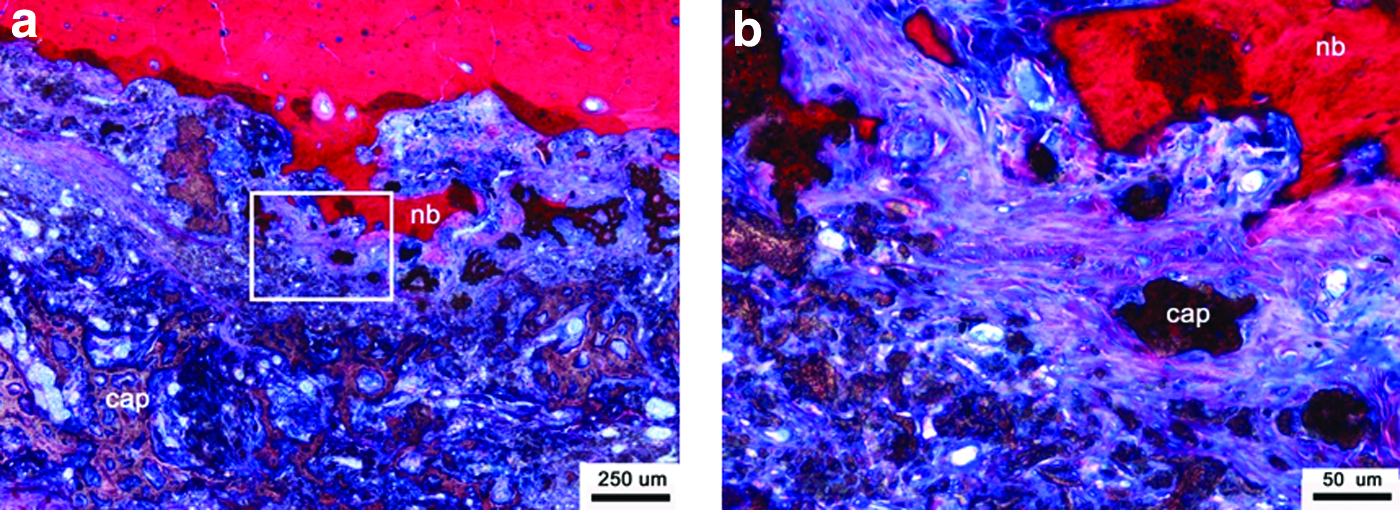
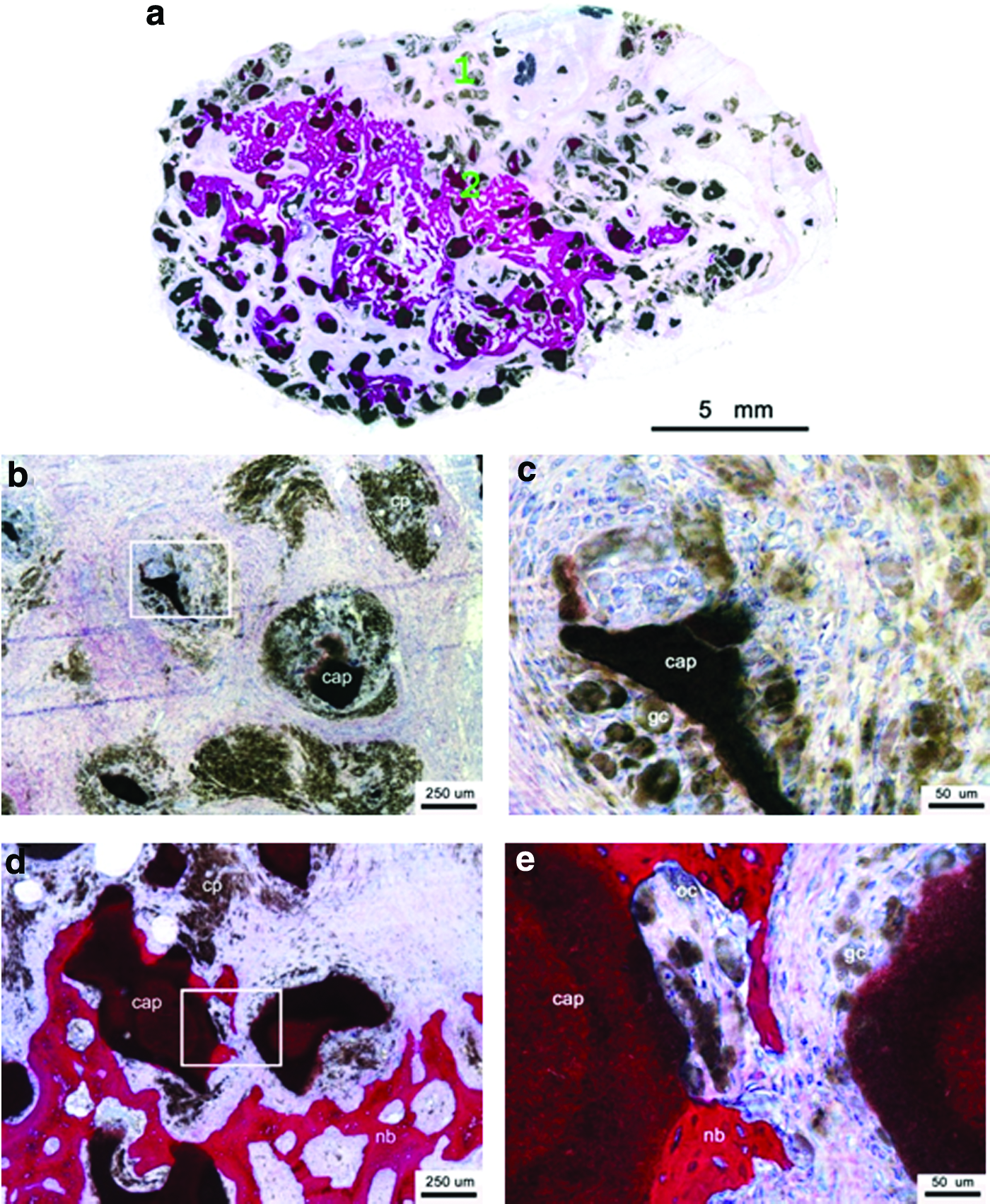
A limited amount of bone had formed between the spinous processes in CaP/BG/C implants (0% ± 0%). Even close to the host bone bed, new bone formation was sporadically seen (Fig. 7a). Fragments of TCP granules were seen phagocytized by giant cells and were sometimes embedded in areas of new bone formation (Fig. 7b). Fibrous tissue was usually seen infiltrating between the granules of BioGlass and TCP fragments (Figs. 3 and 8).
The severe fragmentation of the CaP/BG/C implants may have led to their collapse in the surgical site, and hindered the ability to quantify its resorption rate via the Feret diameter. However, it was possible to measure the histological area of the TCP material (i.e., remaining granules and fragmented residuals) and BioGlass fragments. In particular, the area of the TCP and BioGlass components decreased by 37.6% and 32.9%, respectively (Table 2), indicating that resorption of TCP and dissolution of BioGlass particles occurred after 12 weeks of implantation.
Fluorescence microscopy showed a calcein label in the host bone (i.e., the spinous processes) and in the CaP/AOC and CaP/BG/C implants (Fig. 9a). Calcein labels were mainly observed in areas of new bone formation near the host bone bed in the CaP/AOC implants (Fig. 9a, b). In the CaP/BG/C implants, calcein labels were found throughout the implantation area (Fig. 9a), where it was uniquely related to the surface apatite layer formed on BioGlass granules (Fig. 9c). This indicates that bone formation in the CaP/AOC implants and surface apatite formation on BioGlass granules of the CaP/BG/C implants started before 6 weeks.
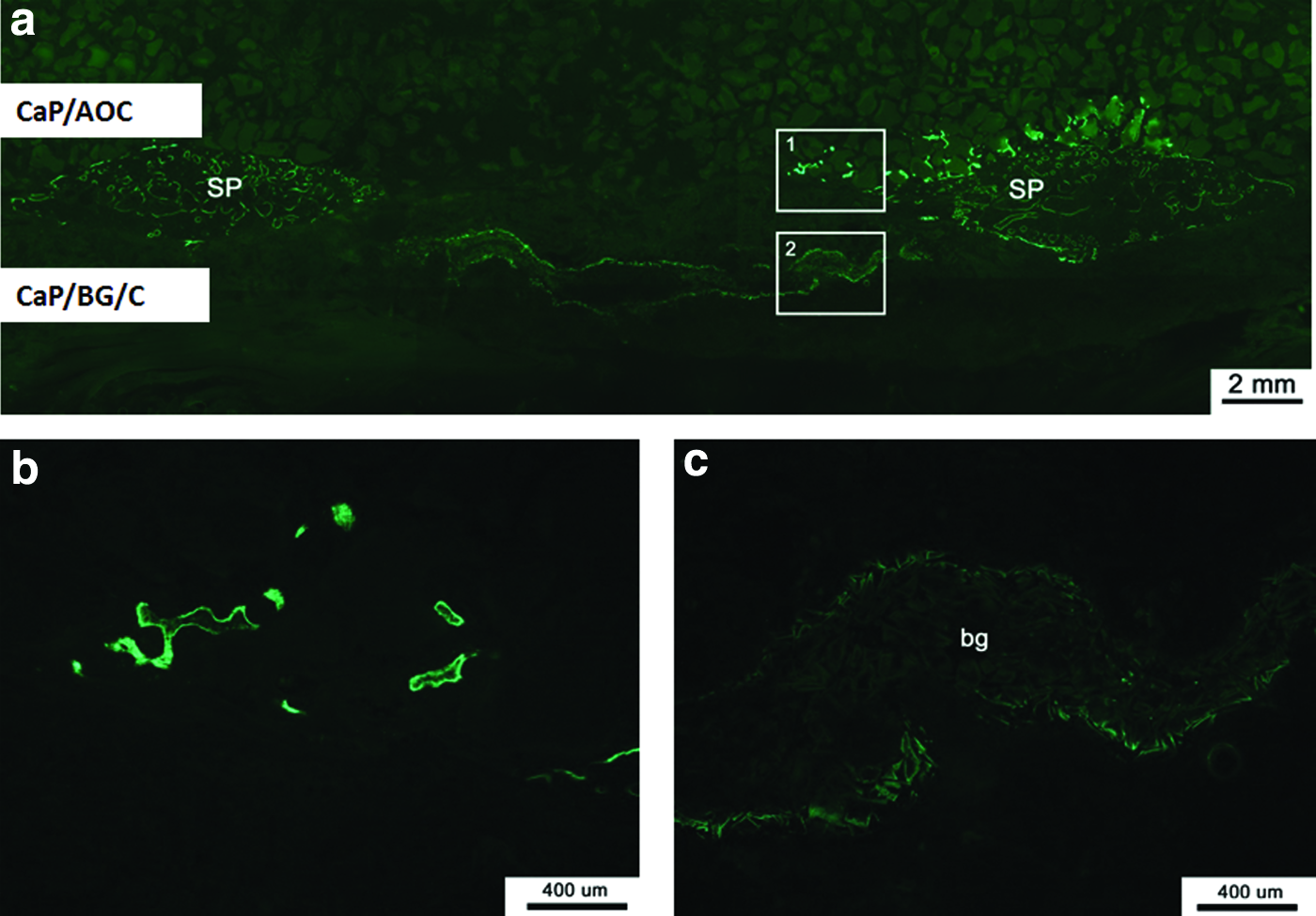
Fluorescent observations of spinal implants.
Tissue response to the intramuscular implants
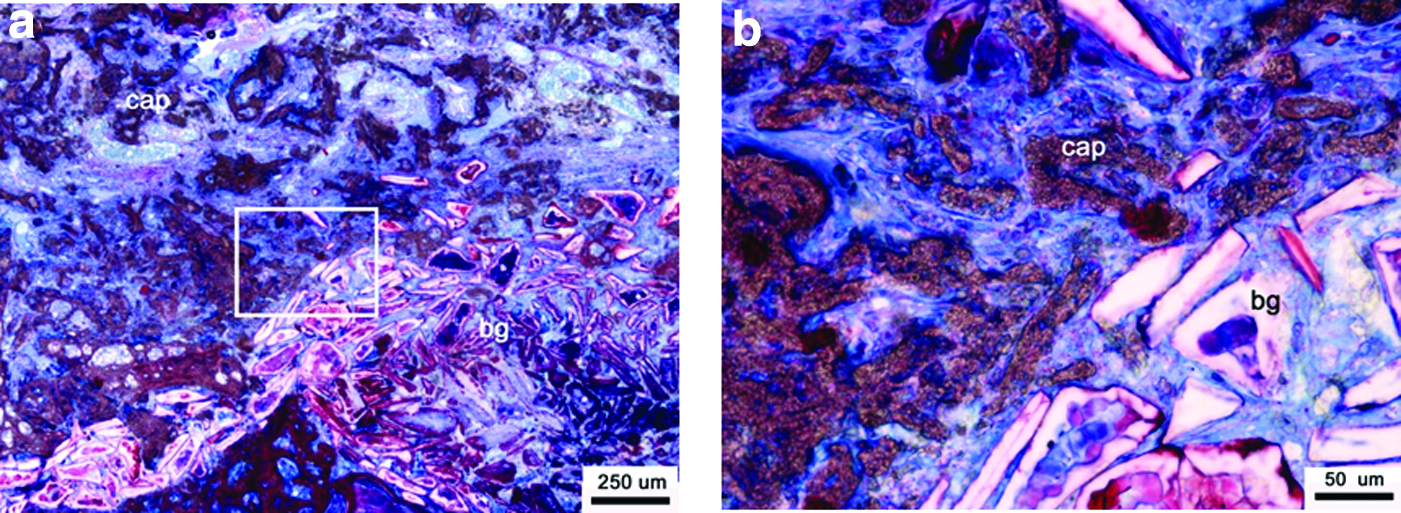
CaP/AOC: At harvest, a thin connective tissue layer encapsulated the CaP/AOC explants without clear signs of an inflammatory reaction. Histological examination of the explants showed the presence of soft tissues, bone, and CaP ceramic granules (Fig. 10a). Areas of de novo bone formation occurred mainly in the core of the explants and the amount of newly formed bone varied among the samples. Quantitatively, 12.0% ± 7.8% mineralized bone tissue was seen in the available space of the ROI (i.e., the space between the ceramic granules), whereas bone contact with the granules was 21.9% ± 7.1% (Table 2).
Histology of CaP/AOC implanted in muscle of dogs for 12 weeks.
The polymer carrier (i.e., AOC®) was not observed in any of the explants and resorption of the ceramic component was evident by the presence of multinucleated cells and small ceramic fragments in surrounding phagocytes.
Resorption of the ceramic granules varied with their location within the implants. At sites where only fibrous tissues were present (Fig. 10b, c), small fragments detached from the ceramic bodies (Fig. 10b) and were phagocytized by macrophages and foreign body giant cells (Fig. 10c). In areas where bone had formed (Fig. 10d, e), the surface of ceramic granules was covered by newly formed bone and the resorption was less pronounced (Fig. 10d), and giant cells were phagocytosing ceramic fragments (Fig. 10e). Resorption of the ceramic occurred in areas of bone remodeling, suggesting cell-mediated resorption of the ceramic. The pronounced in vivo resorption of the ceramic component in CaP/AOC observed histologically was quantitatively corroborated by a significant decrease of the area (−39.3%) and Feret diameter (−47.8%) of the granules when compared with the starting baseline.
CaP/BG/C: At harvest, a soft tissue capsule was observed around the CaP/BG/C explants, without clear signs of inflammation. Although properly mixed during implant preparation and placement, the BioGlass granules were mainly present in the core of the explants (Fig. 11a) and bone was never observed. The available space between the TCP and BioGlass granules was infiltrated by fibrous tissues (Fig. 11b, c) and the collagen component of CaP/BG/C could not be detected. Foreign body giant cells were seen colonizing the granules and mineralization occurred on BioGlass as suggested by the presence of a dark red layer of basic Fuchsin stain (Fig. 11b, c).
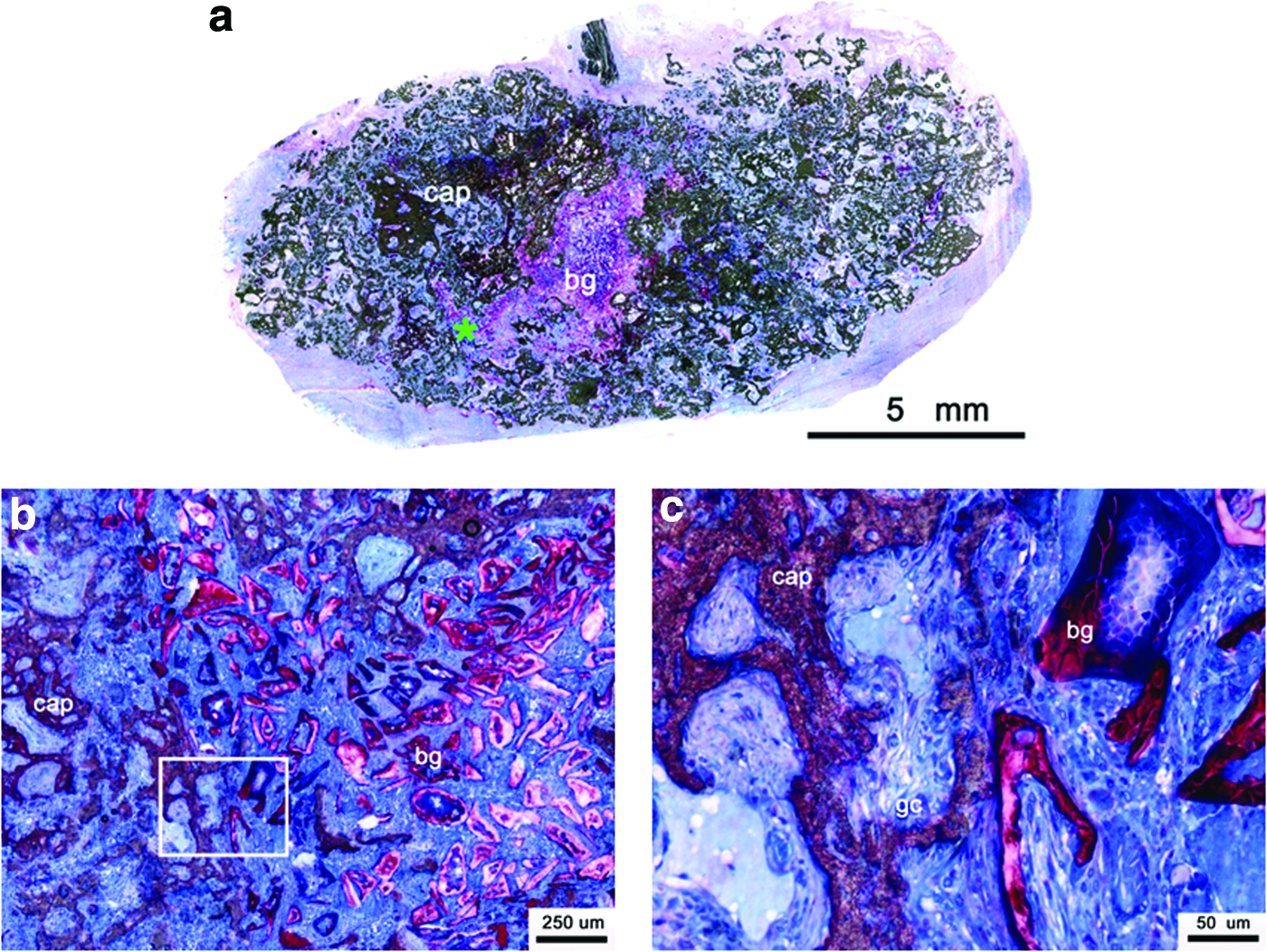
Histology of CaP/BG/C after intramuscular implantation in dog for 12 weeks.
Similarly to what was discussed earlier, fragmentation of the CaP component prevented quantitative determination the Feret diameter, but a 20.9% decrease of the histological area was measured. Furthermore, the histological area of BioGlass particles had a 26.3% decrease over the implantation period.
The 6-week fluorescent signal was not observed in any of the CaP/AOC groups, whereas it was seen in the CaP/BG/C implants (data not provided). As fluorescence was confined to the surface of BioGlass granules, it suggests the formation of a surface apatite layer. These observations furthermore indicate that intramuscular bone formation did not start before 6 weeks in the CaP/AOC implants.
Discussion
In this study, we evaluated two moldable CaP-based bone graft materials in a noninstrumented canine IS model and intramuscularly over a 12-week implantation period.
The bone-forming potential of the materials was either “enhanced” by creating a submicron surface topography (i.e., in CaP/AOC) or by adding BioGlass particles (i.e., in CaP/BG/C). Clear performance differences were observed between both material types. First, considerable bone formation and implant resorption was observed with the submicron structured CaP/OAC implants in the spine model, whereas negligible bone formation and severe fragmentation were seen with the CaP/BG/C implants. Second, although both materials showed a mild inflammatory response after intramuscular implantation, de novo bone formation was seen in all CaP/AOC implants, whereas only fibrous tissue infiltration was seen in the CaP/BG/C implants.
The ability of submicron structured ceramic materials, such as CaP/AOC, to give rise to heterotopic bone formation has been reported before5,11–16 and is not a new finding. This material property may also have contributed to the meaningful bone formation of CaP/AOC observed in the noninstrumented spinal site since the CaP/BG/C material was unable to form bone.
Muschler et al. reported that providing instrumentation and decortication of the lamina and facet joints in a similar spinal fusion model in mongrel dogs is ineffective to obtain fusion upon implantation of a collagen ceramic composite graft material, even when mixed with cancellous bone graft or autologous bone marrow.21,22 These studies also showed that spinal fusion is challenging in dog IS models because it was not always reached even when using the golden standard autograft in the presence of instrumentation and decortication.21,22
Although in our study fusion was also not observed, the presence of cartilaginous tissue in the center of the fusion mass with CaP/AOC (Fig. 5) is indicative of mechanical instability, which is known to hamper bone formation.26,27 It is probable that a less sensitive model to the one we used, that is, using instrumentation and decorticating the lamina and facet joints as done by Muschler et al.21,22 may have allowed fusion to occur with this material.
In this study the CaP component of the two composites slightly differed since traces of HA were present in the inorganic component of CaP/AOC (Fig. 2a and Table 1), whereas pure TCP was found in the CaP component of CaP/BG/C. The effects of these chemical differences on bone formation may have been minor compared with the potentially larger role of the surface structural dimension. In fact, as recently suggested by Davison et al. in a study testing the influence of several CaP material parameters (surface microstructure, macrostructure and surface chemistry), the microstructural dimensions were reported to be the most critical factors promoting bone formation. 28
The CaP phase in both graft materials contained micropores (Fig. 2c, d) with similar microporosity, but the granules in CaP/AOC had significantly larger fraction of submicron porosity (Fig. 2b and Table 1). Only the composite containing submicron structured material triggered instructive bone formation (Figs. 10 and 11), suggesting that not only the presence of micropores, but also their dimension plays a major role in CaP-directed bone formation.5,15,17
It is well known that CaP ceramics can degrade through both chemical dissolution and cell-mediated resorption. 29 Intramuscularly, the latter phenomenon appeared histologically evident in CaP/AOC and less in CAP/BG/C (Figs. 10 and 11), which suggests a possible influence of the submicron structured surface (Fig. 2c) on the activity of phagocytes.28–30 This would be in agreement with the findings of Davison et al. who reported that cell-mediated resorption of biomaterials and osteoclastogenesis is a prelude to material-directed bone formation. 30
Surface mineralization and silicon ion release are reported to enhance the bioactivity of BioGlass.19,20,31 Although we did observe in vivo surface mineralization on BioGlass granules in CaP/BG/C (Fig. 9), no signs of osteoinduction were detected intramuscularly. In the spine, the material was severely fragmented and also showed negligible bone formation.
Similar disappointing results were reported by Walsh et al., who implanted CaP/BG/C combined with a bone marrow aspirate in a rabbit posterolateral spinal fusion model for up to 26 weeks and did not see any bone formation in the middle of the fusion mass. 32 Conversely, Epstein reported successful fusion in humans when the TCP component of CaP/BG/C was implanted in the instrumented posterolateral spine. 33 It should be noted that in the study of Epstein, TCP was used in a large volume (30 cc granules), mixed with bone marrow aspirate and combined with the same amount of autograft. Similarly, when the same TCP granules were combined with autogenous bone marrow aspirate (BMA), it was reported to lead to high fusion rates in human posterior cervical spine, 34 which suggests the need for autologous bone and osteogenic elements to support and enhance the biological activity of the TCP component in CaP/BG/C.32–34 As a result, this may explain why CaP/BG/C was not efficacious in this study.
Within the limits of this study, the submicron structured CaP/AOC implants supported bone formation in the canine noninstrumented IS implantation model and showed bone induction after intramuscular implantation. Bone formation was not sufficient to achieve a solid fusion, which is likely the result of the noninstrumented nature of the model. 26 The bone-forming potential of CaP/BG/C implants was limited in the spine, which is likely due to the collapse and severe fragmentation of the implant either during implant preparation or after surgical placement and postoperative movement.
Conclusions
The results of this study show that a submicron-surface structured CaP/AOC bone graft material has superior bone-forming properties in both an IS implantation model as compared with a CaP/BG/C bone graft material. It also shows that the CaP/AOC material has osteoinstructive properties, which could have aided in the bone formation shown in the spine. Further investigation is warranted to verify the link between ectopic and orthotopic bone formation and the influence of (micro) motion on bone formation in this model.
Footnotes
Disclosure Statement
D.B. is employee of Xpand Biotechnology BV. H.Y. is employee and shareholder of Xpand Biotechnology BV. A.S.I. is employee of NuVasive, Inc. J.D.d.B. is employee and shareholder of Xpand Biotechnology BV.