
Abstract
Introduction:
Tissue engineering may become an alternative to current bladder augmentation techniques. Large scaffolds are needed for clinically significant augmentation, but can result in fibrosis and graft shrinkage. The purpose of this study was to investigate the use of multiple scaffolds instead of one large scaffold, to enhance bladder tissue regeneration and bladder capacity. Second, acellular collagen, collagen–heparin, and collagen–heparin scaffolds with growth factors (GFs) were used and the biological activity of the different scaffolds was compared in a large animal model.
Materials and Methods:
Scaffolds were made of bovine type I collagen with or without heparin (Ø = 3.2 cm). Collagen–heparin scaffolds were loaded with GFs, vascular endothelial growth factor (VEGF), fibroblast growth factor 2 (FGF2), and heparin-binding epidermal growth factor (HB-EGF). Three identical scaffolds prepared from collagen (COL-group), collagen with heparin (COLHEP-group), or collagen–heparin with growth factors (COLHEPGF-group) were implanted in one porcine bladder. The outcome was compared with sham-operated animals (Sham-group), in which no scaffold was used. Urodynamic evaluation was performed before surgery and 3 months after bladder reconstruction, together with histological evaluation.
Results:
Survival rate was 92%, 12 animals completed the study, 3 of every group, 1 animal developed peritonitis due to urine leakage and was sacrificed. The regenerated area was largest in the COLHEP-group, and least in the COL-group (p = 0.002). Histological evaluation revealed a normal urothelial layer and good angiogenesis in all groups, and comparable ingrowth of smooth muscle cells. Urodynamics showed no statistically significant differences in bladder capacity and compliance between groups. Bladder capacity and compliance was very high in this animal model, which made it impossible to study the increase due to augmentation.
Conclusions:
Implantation of multiple collagen–heparin scaffolds in one bladder is feasible in a porcine model, resulting in tissue almost indistinguishable from native tissue involving all cell layers of the bladder. Collagen scaffolds with heparin incorporated resulted in a larger area of regenerated tissue. To reach clinically significant augmentation, multiple larger collagen–heparin scaffolds, with or without GFs, need to be tested to study the largest possible diameter of scaffold and number of used scaffolds still resulting in well-vascularized tissue.
Introduction
B
Several studies have shown that tissue-engineered constructs can be used to regenerate bladder tissue, including urothelium, smooth muscle, vessels, and nerve fibers, in various animal models.5–7 A substantial improvement in bladder capacity was found in the first clinical trial by Atala et al., who showed the feasibility of tissue engineering of the human bladder. Particularly promising results were seen with constructs consisting of collagen and a synthetic polymer, seeded with urothelial and smooth muscle cells (SMCs), and wrapped in omentum. 8 Unfortunately, these results could not be reproduced in a phase 2 study in which 10 patients with spina bifida were treated with this technique. 9 Augmentation of the bladder of five patients with bladder exstrophy with an acellular small intestinal submucosa (SIS) scaffold improved bladder capacity. However, the primary clinical endpoint of improved dry intervals was not reached. 10 These studies clearly show that improvements of the technique are needed to enhance clinical outcome, which is one of the essential steps that need to be undertaken before it can be tested again in a clinical trial. 11
Tissue regeneration in large constructs is hampered by a lack of oxygen and nutrition delivery to the infiltrating cells and inadequate removal of waste products.12,13 The diffusion distance from supplying blood vessels is approximately 150–200 μm, 13 necessitating rapid and extensive angiogenesis. In the current study, the feasibility of implantation of three smaller scaffolds instead of one large scaffold, to reach the same surface area of regenerated tissue, while reducing the problem of oxygen and nutrition delivery in large scaffolds, was examined. We hypothesized that the shorter distance of the vascularized border of the native tissue to the center of the scaffold would reduce the vascularization time of this area, and consequently the period of limited oxygen and nutrient delivery, and improve tissue regeneration.
Growth factors (GFs) play an important role in proliferation, migration, and differentiation of several cell types. The inclusion of GFs in large grafts may therefore assist in quicker and better acceptance.12,14,15 Vascular endothelial growth factor (VEGF), an important factor in angiogenesis, combined with fibroblast growth factor 2 (FGF2) enhances blood vessel formation and maturation. 12 Collagen scaffolds loaded with heparin were used to bind these GFs, together with heparin-binding epidermal growth factor (HB-EGF), which is known to play a role in urothelial regeneration.14–17 This combination of GFs improved regeneration of bladder tissue in a large animal model for diseased bladder, resulting in better ingrowth of urothelium and SMCs, and enhanced angiogenesis. 15 In the current study, collagen–heparin scaffolds loaded with these GFs were compared with a collagen scaffold, a collagen scaffold with heparin alone, and a sham-operated control group.
Materials and Methods
Preparation and characterization of scaffolds
Type I collagen was purified from bovine Achilles tendon as previously described. 18 A 0.67% (w/v) type I collagen suspension in 0.25 M acetic acid was shaken overnight at 4°C and homogenized on ice using a Potter-Elvehjem homogenizer (Louwers Glass and Ceramic Technologies, Hapert, The Netherlands). Air bubbles were removed by centrifugation at 100 g for 15 min at 4°C. The suspension was poured into six-well plates (4 mL per well), frozen at −20°C, and lyophilized. For crosslinking, scaffolds were preincubated with 50 mM 2-morpholinoethane sulfonic acid (MES), pH 5.0, containing 40% ethanol, for 30 min at 20°C. After removal of this solution, scaffolds were incubated with 33 mM 1-ethyl-3-(3-dimethyl aminopropyl) carbodiimide (EDC) and 6 mM N-hydroxysuccinimide (NHS) in 50 mM MES pH 5.0 containing 40% ethanol for 4 h at 20°C with or without 0.25% heparin (Diosynth, Oss, The Netherlands). Scaffolds were washed, frozen, and lyophilized. This resulted in round collagen scaffolds with a diameter of 3.2 cm. Subsequently, 70% ethanol was used to disinfect the scaffolds, followed by washings with sterile phosphate-buffered saline (PBS).
To bind the GFs, collagen–heparin scaffolds were aseptically incubated with FGF2, VEGF, and HB-EGF (all human recombinant; R&D Systems, Minneapolis, MN). First, scaffolds were incubated in 7 mL PBS containing 3.5 μg/mL FGF2 for 1 h. Next, VEGF and HB-EGF, each 3.5 μg/mL PBS, were added and incubated overnight at 20°C. Finally, scaffolds were washed in PBS and used immediately.
The number of primary amine groups was analyzed using a 2,4,6-trinitrobenzene sulfonic acid assay to determine the degree of crosslinking.19,20 Heparin content was determined by a hexosamine assay with p-dimethylaminobenzaldehyde, using a standard curve of heparin. 21 GF content was assessed using western blot analysis. 14 Scaffold ultrastructure was visualized using a JEOL JSM-6310 scanning electron microscopy (SEM) apparatus by operating at 15 kV, after gold coating the specimens.
Surgical procedure
This study was approved by the Animal Ethics Committee of the Radboud University Medical Center.
Thirteen female Landrace pigs with a mean weight of 48.5 kg (ranging from 41 to 59 kg) were operated at age 3 months. No significant difference in weight existed within and between groups. Animals were housed individually for 2 weeks after surgery, with a restricted diet and free access to water. After 2 weeks, the animals were housed in a group. Animals were premedicated with intramuscular (IM) injection of midazolam (1 mg/kg; Roche, Woerden, The Netherlands), atropine (50 μg/kg; Pharmachemie BV, Haarlem, The Netherlands), and ketamine (10 mg/kg; Eurovet Animal Health BV, Bladel, The Netherlands). General anesthesia was induced by intravenous (IV) injection of propofol (2–3 mg/kg; B. Braun, Melsungen, Germany), followed by tracheal intubation, and maintained with 0.5–1% isoflurane (Nicholas Piramal, London, United Kingdom) and midazolam (0.6 mg/kg/h, IV). For analgesia, flunixin (2.2 mg/kg; Intervet, Boxmeer, The Netherlands) and sufentanil (5 μg/kg bolus; Janssen Cilag BV, Tilburg, The Netherlands) were given IV, followed by a maintenance dosage sufentanil of 10 μg/kg/h. Vecuronium (0.2 mg/kg; N.V. Organon, Oss, The Netherlands) was given IV as muscle relaxant, and maintained with 0.4 mg/kg/h.
Video urodynamic evaluation was performed using the MMS Solar system (MMS, Enschede, The Netherlands) and a Philips BV-25 C-arm and image identifier (Philips, Eindhoven, The Netherlands). A double lumen 6Fr catheter (Medtronic, Heerlen, The Netherlands) was placed in the bladder. A double lumen 9Fr catheter (Bel Medical B.V., Zwolle, The Netherlands) was placed in the rectum. The bladders were slowly filled with iodinated contrast fluid (Xenetix® 300 [Guerbet Nederland BV, Gorinchem, The Netherlands] diluted with PBS 1:1). Urethral leakage did not occur during urodynamic measurements, so bladder filling was stopped at a maximal pressure of 40 cm H2O and bladder capacity was evaluated at 20 cm H2O. One or two representative evaluations were performed in each animal.
Subsequently, a laparotomy was performed under sterile conditions to expose the bladder (Fig. 1A). Three incisions of 3 cm were made in the bladder, along the vascularization from the lateral side to the middle of the bladder. Animals were randomly assigned to one of the four groups. Three identical collagen scaffolds (COL-group), collagen–heparin scaffolds (COLHEP-group), or collagen–heparin scaffolds with GFs (COLHEPGF-group) were sutured into the defects using 5-0 poliglecaprone (Monocryl®; Ethicon, Inc.) running sutures (Fig. 1B). In the sham group, the bladder was closed in one layer using a 5-0 poliglecaprone running suture (Fig. 1C). Four 5-0 polypropylene (Prolene®; Ethicon, Inc.) nonresorbable marking sutures were placed at the edges of the scaffold. A 12Fr silicon catheter (Coloplast, Amersfoort, The Netherlands) was used as suprapubic catheter. The bladder was filled to ensure that no urinary leakage occurred along the suture line. The peritoneum was closed using 4-0 poliglecaprone. The abdominal wall was closed using 0 polyglactin (Vicryl®; Ethicon, Inc.) interrupted sutures for the fascia and 1-0 polyglactin for the skin. The suprapubic catheter was fixed to the skin using 1-0 polyglactin sutures, and was removed after 2 weeks. Buprenorphine (10 μg/kg, IV; Schering Plough, Segre, France) was given once, and flunixin (2.2 mg/kg, IM) for 3 days as postoperative analgesia. Amoxicillin (10 mg/kg, IM; Aurobindo Pharma BV, Zwijndrecht, The Netherlands) was given twice daily during 3 days.
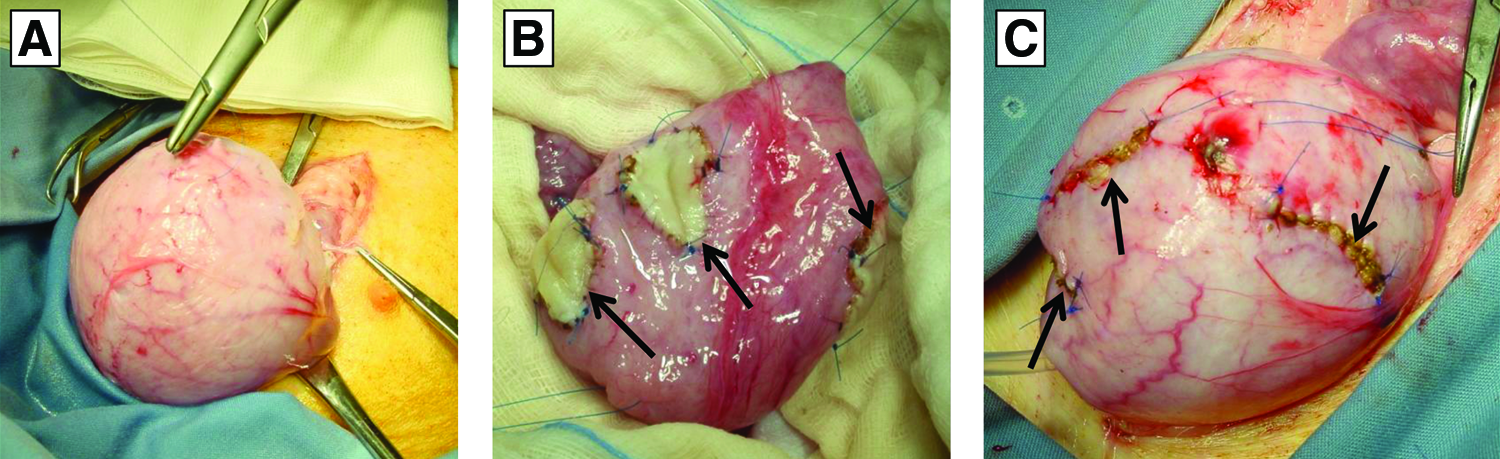
Representative macroscopic overview of the implantation procedure.
Functional evaluation
Animals were evaluated after 3 months. Animals were anesthetized and urodynamic evaluation was performed as described above. Thereafter, the animals were sacrificed with IV pentobarbital (60 mg/kg; AST Pharma, Oudewater, The Netherlands). The bladder was removed, filled with 300 mL PBS, inspected, and the size of the regenerated tissue was measured between marking sutures (Fig. 2). The regenerated area was assumed to be of elliptical shape, the surface area was calculated using the formula (0.5 × diameter 1) × (0.5 × diameter 2) × π. Kidneys were examined for signs of infection, hydronephrosis, or stone formation.

Macroscopic overview 3 months postsurgery.
Histological staining
Tissue samples were obtained from the regenerated tissue (COL-group, COLHEP-group, and COLHEPGF-group) and the scar tissue (sham group), fixed in 4% (v/v) buffered formalin and paraffin embedded. Sections (4 μm) were cut in the center of the tissue along the longest axis and stained with Hematoxylin and Eosin (H&E). Multiple levels were analyzed using H&E staining and a representative level was chosen for immunohistochemistry and the Masson Trichrome/Verhoeff stain.
For immunohistochemistry, sections were deparaffinized in xylene, followed by graded series of ethanol and rehydration in PBS. Slides were immersed in 1% (v/v) H2O2/PBS for 30 min at room temperature (RT) to block endogenous peroxidase. Antigen retrieval methods and primary antibodies are shown in Table 1. Slides were preincubated with 5% goat serum, incubated with the antibody of interest, pancytokeratin, Cytokeratin 7, smooth muscle actin or smoothelin, washed and incubated with poly-HRP-anti mouse IgG (Immunologic, Duiven, The Netherlands) which was preincubated with 10% swine serum for 30 min at RT. For vimentin and desmin staining, slides were peroxidase blocked and preincubated with 5% horse serum. After primary antibody incubation for 1.5 h, sections were washed and incubated with a biotin-labeled secondary antibody (30 min, horse-α-mouse, 1:200; Vector Laboratories, Burlingame, CA). Next, the slides were washed and incubated with peroxidase-labeled streptavidin/biotin complex (1:100 Avidin reagent and 1:100 Biotin reagent, 30 min preincubation; Vector Laboratories) for 45 min followed by washings in PBS. All stainings were developed with Bright-DAB (Immunologic) for 10 min and counterstained with Hematoxylin (Klinipath, Duiven, The Netherlands).
A, heat mediated in sodium citrate buffer (10 mM; pH 6.0; 10 min; 100°C); B, with 0.1% pronase (30 min at room temperature); C, without antigen retrieval.
Histological evaluation was performed microscopically by L.A.J.R., P.K.J.D.d.J., and P.J.G. and scored independently in a blinded fashion. Quantitative analysis of SMC ingrowth was performed using ImageJ (NIH). Using a rolling ball method (50 px), background was corrected for desmin stained slides. The browns were extracted and converted to binary, followed by plotting the pixel intensity along the native muscle and the regenerated tissue. The intensity thereby is higher when more muscle tissue is present (Fig. 3). The distance of muscle ingrowth was determined. In addition, the area under the curve ([AUC] amount of positive pixels, derived from curves as shown in Fig. 3) was analyzed to approximate the amount of muscle tissue in the regenerated and native tissue. This was standardized to show the average amount of pixels per mm of tissue (AUC/mm).
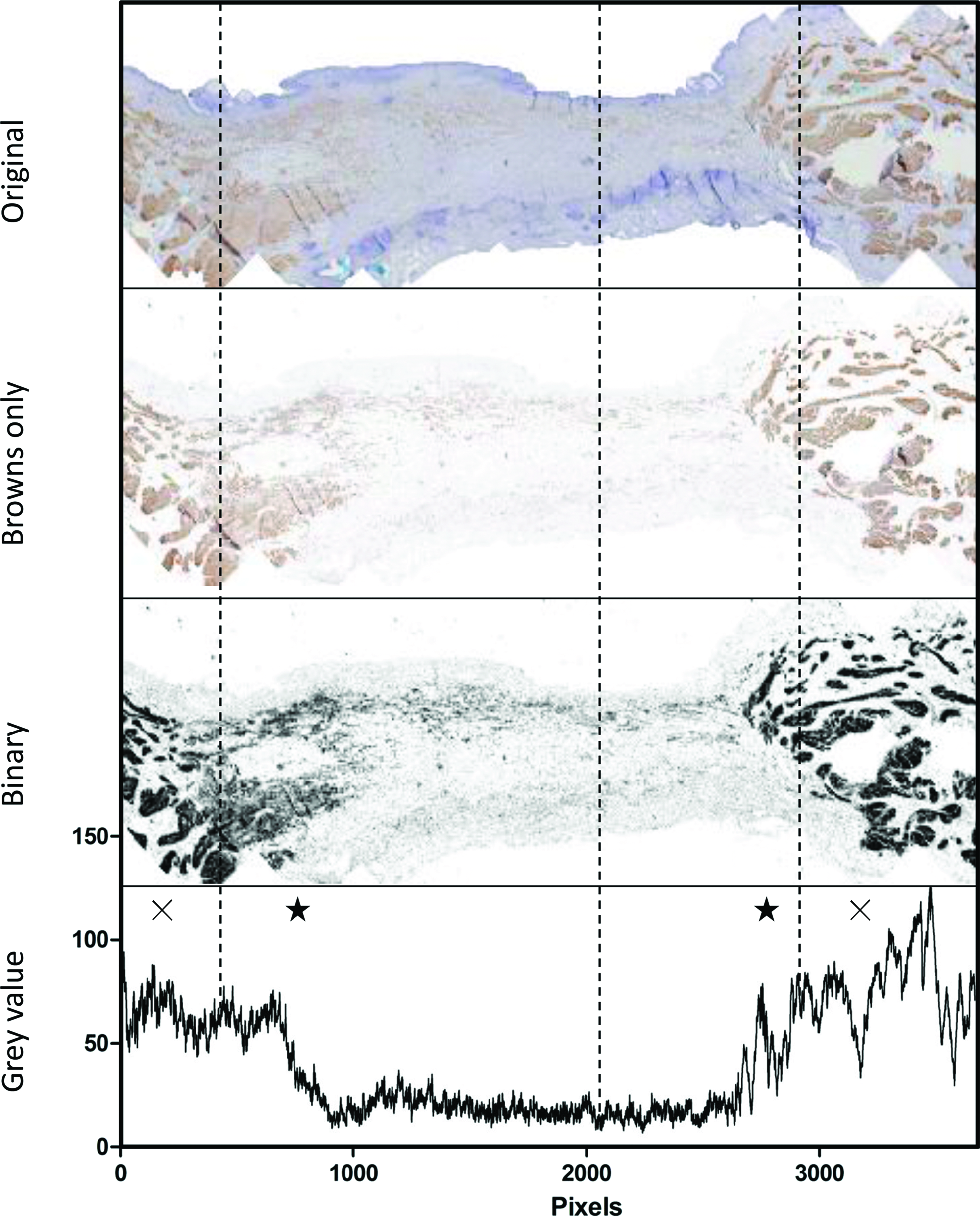
Overview of muscle quantification process. From the original image, only the brown colors (desmin-positive cells) were extracted. Next, the image was converted to a binary image. Finally, a profile was plotted, which showed the pixel intensity along the tissue. Higher intensity indicates a higher number of desmin-positive cells. ×Indicates the native muscle tissue. ★Indicates the anastomosis site. Note the change of morphology and decreasing intensity toward the center. Color images available online at www.liebertpub.com/tea
Renal tissue of all pigs was processed and examined for inflammation or dilated nephrons by H&E staining.
Statistical analysis
Data analysis was performed with IBM SPSS statistics version 22 (IBM, New York, NY), using the one-way analysis of variance (ANOVA) test, followed by the least significant difference (LSD) post hoc test. p < 0.05 was considered statistically significant.
Results
Scaffolds
The collagen scaffolds consisted of homogenously distributed honeycomb-like pores with an average size of 100–150 μm (see Hosper et al. 22 who used identical scaffolds). After crosslinking, primary amine groups were reduced by 46% ± 6% for collagen scaffolds and 48% ± 8% for heparinized collagen scaffolds. Heparin bound to heparinized collagen scaffolds was 12% ± 5%. The GF content bound per mg collagen–heparin scaffold was 0.2 ± 0.2 μg for VEGF, 0.7 ± 0.2 μg for FGF2, and 0.8 ± 0.3 μg for HB-EGF. Results are given as mean ± standard deviation.
Animal surgery
Overall survival rate was 92%. One out of 13 pigs had a peritonitis due to urinary leakage and was sacrificed. At autopsy we found a rupture of the scaffold at the border where it was sutured. One other animal was sacrificed 1 day before the intended date of sacrifice because of illness, and no clear diagnosis was made after autopsy. This animal was included in the histological analysis. Both animals were from the COLHEPGF-group. Three months after operation, the mean weight was 108.3 kg (range 90–120 kg), no significant differences existed within and between groups. This was an increase of 123% (Table 2).
No significant differences in weight existed within and between groups. No statistically significant differences in bladder capacity were found between groups. The largest amount of tissue was regenerated in the COLHEP-group, which was statistically significant compared with the COL-group (p = 0.002) (also see Fig. 4A), but not compared with the COLHEPGF-group (p = 0.083). Several values are not available due to drop out before 3 months or technical failure.
Catheterization impossible; bsacrificed.
3 Months, 3 months after operation; NA, not available; Preop, preoperative; SD, standard deviation.
Functional evaluation
All pigs voided normally, without signs of incontinence or urinary tract infection. Catheterization was impossible in one animal before operation and two animals at 3 months. On urodynamic evaluation, none of the pigs showed detrusor overactivity. No statistically significant differences in capacity were found between groups (Table 2).
No structural abnormality of the bladders, for example, no diverticula or leakage were seen when the bladders were filled after sacrifice (Fig. 2A).
Macroscopic evaluation
No scaffold remnants were visible in the scaffold groups (Fig. 2B). The bladder wall appeared slightly thinner at the implantation site in these groups. A small scar was visible in the sham group. The native bladder had a normal appearance in all groups, without signs of stone formation (Fig. 2C). The sum of the regenerated area is shown in Figure 4A and Table 2. The largest amount of tissue was regenerated in the COLHEP-group, which was statistically significant compared with the COL-group (p = 0.002), but not compared with the COLHEPGF-group (p = 0.083). No significant difference was seen between the COL-group and COLHEPGF-group (p = 0.215).
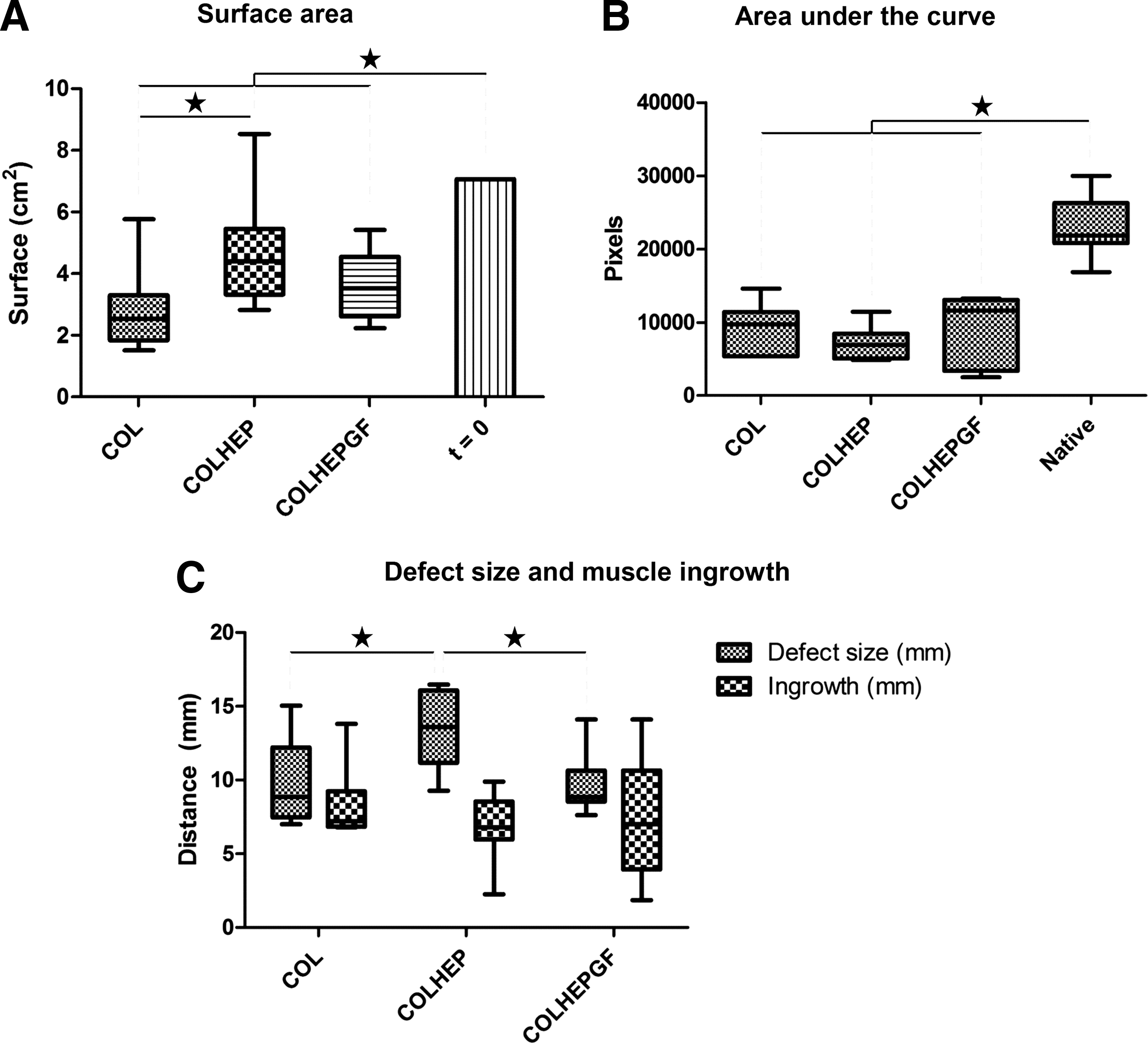
Results of the quantitative and statistical analysis. Statistically significant differences are marked with a ★.
All kidneys appeared normal.
Histological evaluation
Figures 5–7 show representative sections from the different study groups.
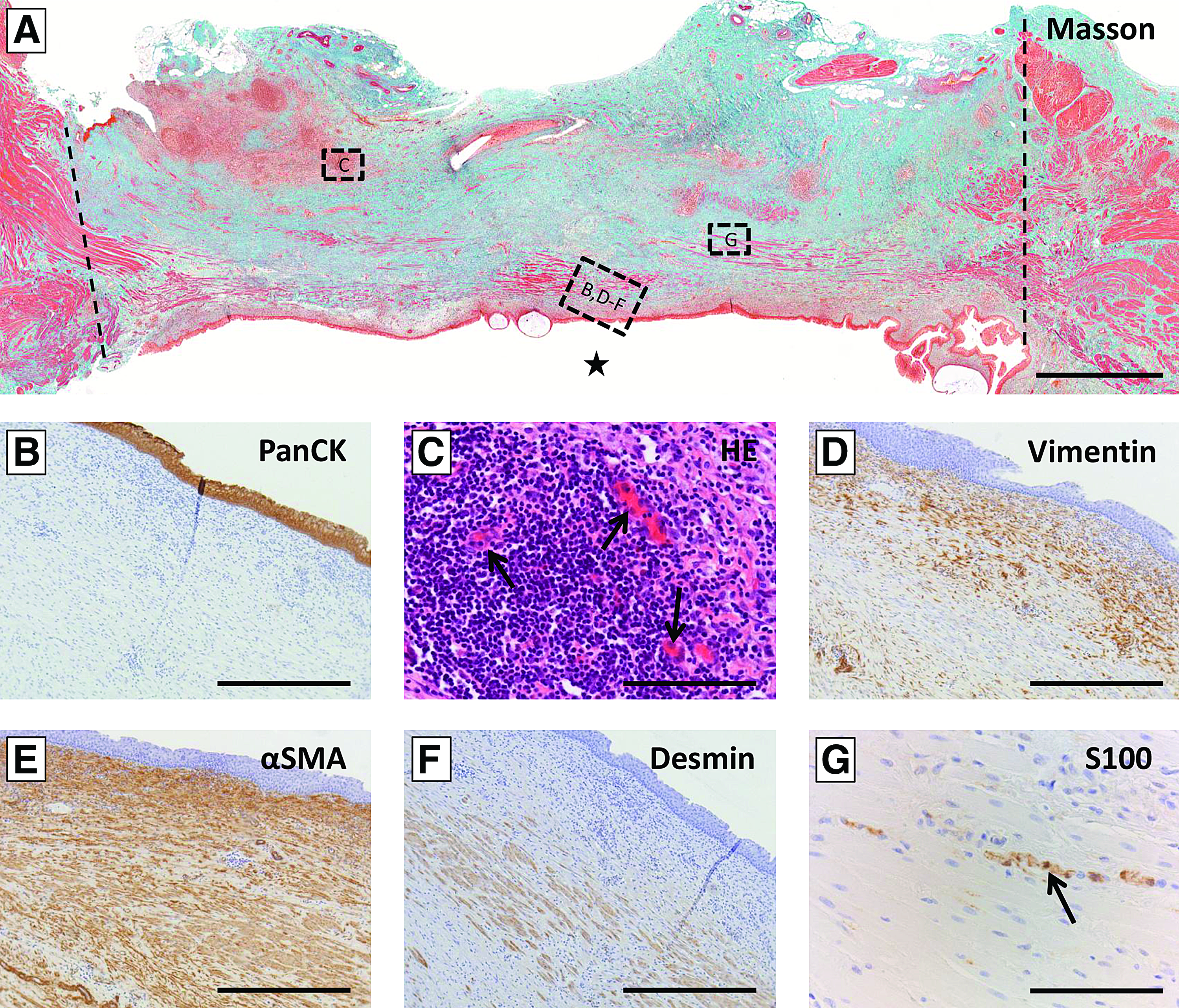
Representative histological overview of COL group after 3 months.
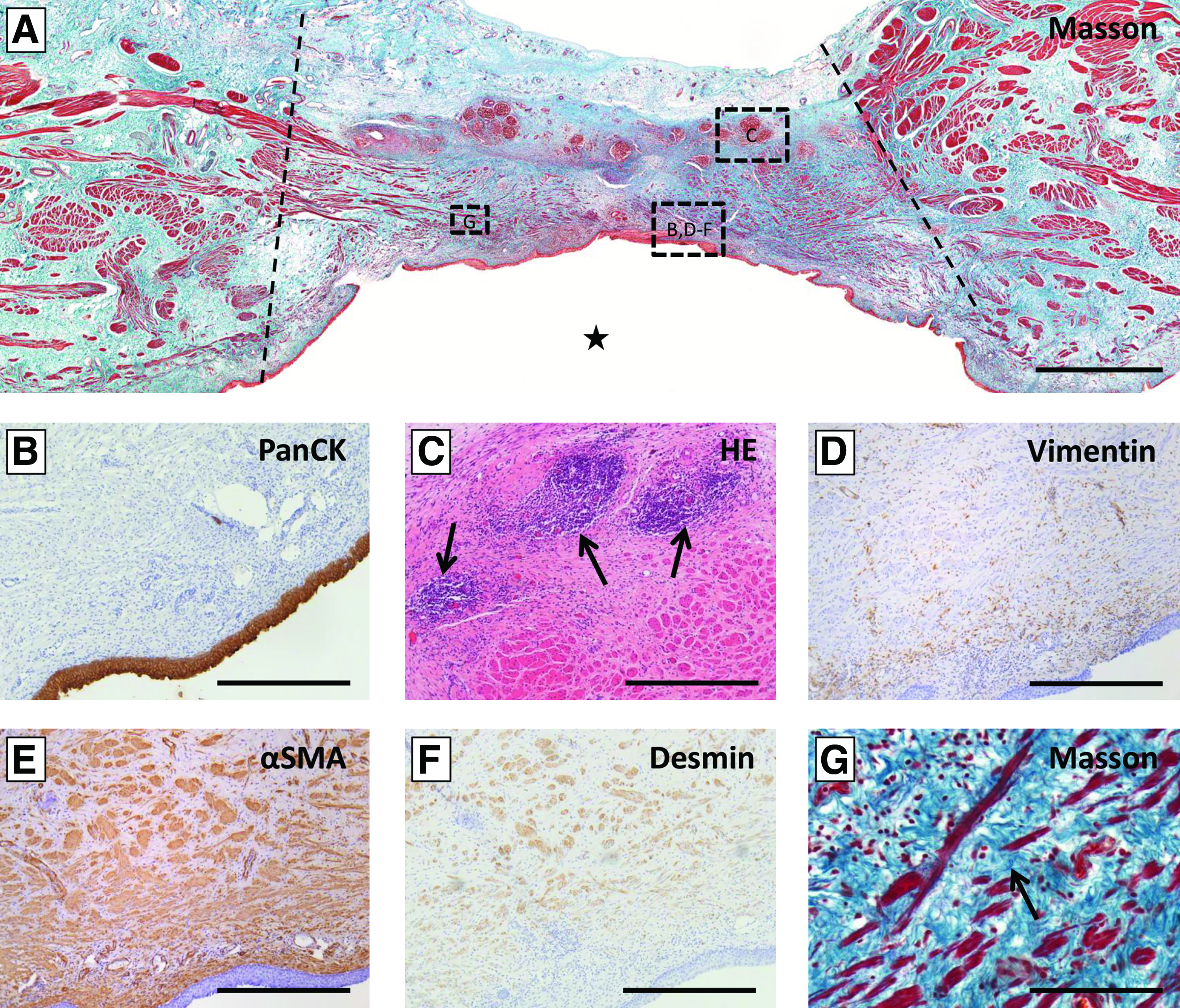
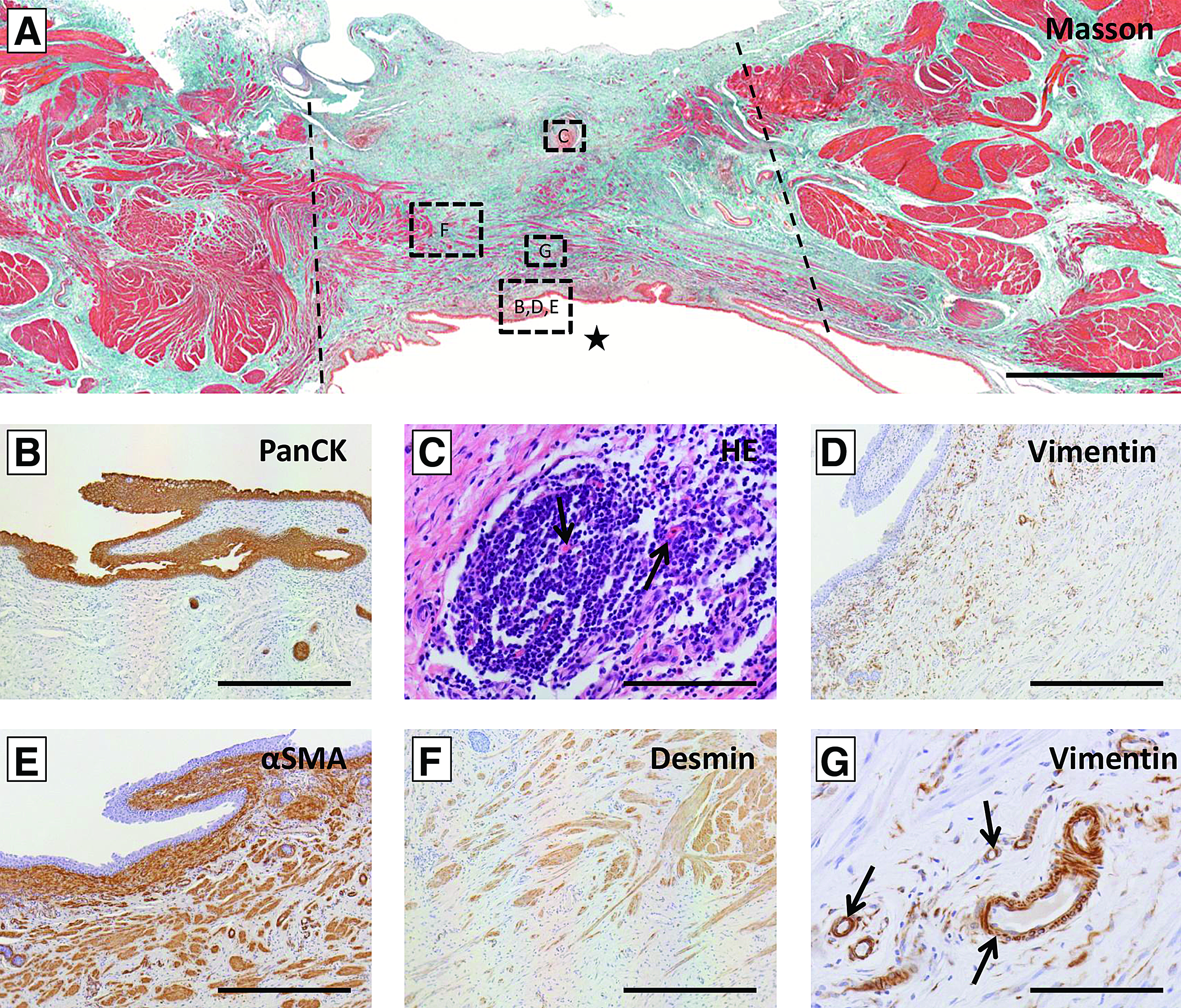
Representative histological overview of COLHEP-group after 3 months.
Representative histological overview of COLHEPGF group after 3 months.
Sham group
A confluent, normal-appearing multilayered lining of urothelial cells was observed, containing a basal layer and umbrella cells. The architecture of the tissue was generally like native tissue, including smooth muscle formation. Only few fibroblasts and myofibroblasts were found in the wound (data not shown).
Regenerated bladder tissue in scaffold groups
The histological results are shown in Table 3. The regenerated tissue showed a confluent, well-differentiated, urothelial layer in all groups (Figs. 5A, B, 6A, B, and 7A, B) (data cytokeratin 7 not shown). Submucosal tissue consisted of connective tissue with fibroblasts, myofibroblasts, and dense collagen (Figs. 5A, D, E, 6A, D, E, and 7A, D, E). Directly under the urothelium the multilayered structure of vimentin- and α-SMA-positive cells, similar to native bladder tissue, was visible in approximately half, and all animals, respectively. No difference was seen between groups (Figs. 5D, E, 6D, E, and 7D, E). Fibrosis was comparable between groups, and slightly more evident in the COLHEP-group, with slightly denser extracellular matrix (ECM) and slightly more fibroblasts and myofibroblasts. Angiogenesis was visible throughout the entire regenerated area and comparable between groups (Table 3). Mature blood vessels were present, evidenced by vimentin-positive cellular linings and the presence of erythrocytes (Fig. 7G). In the COL-group and the COLHEPGF-group hardly any scaffold remnants remained. In the COLHEP-group scaffold remnants were visible, mainly at the serosal side (Figs. 5A, C, 6A, C, and 7A, C). Inflammatory cells were mainly visible around scaffold remnants, mainly consisting of lymphocytes. Slightly more inflammatory cells were observed in the COL-group.
COLHEP showed more vimentin and α-SMA-positive cells than COL or COLHEPGF, as well as more scaffold remnants and elastic fibers. ECM was also slightly more visible in COLHEP, although not visible in table due to round off in categories. More inflammation was seen in COL compared with COLHEP and COLHEPGF. No other differences were found.
++, Abundant; +, present; +/−, limited; ECM, extracellular matrix; SMCs, smooth muscle cells (desmin positive cells); Sp, sporadically present.
SMC ingrowth was present throughout almost the entire regenerated tissue in most animals of the COL and COLHEPGF groups, appearing as fascicles or separate cells. While the distance of ingrowth was similar between all groups, the ingrowth in the center of the new tissue was limited in the COLHEP group due to the larger overall surface area. (Figs. 5A, F, 6A, F, and 7A, F) (data smoothelin not shown). SMC ingrowth occurred from the borders inward, originating from the native detrusor muscle. No clear difference in the amount of ingrowth of SMCs was visible between groups on microscopic evaluation. Quantitative analysis of smooth muscle ingrowth showed comparable amount of SMCs per mm of regenerated tissue (Fig. 4B). In view of the larger regenerated area of the COLHEP-group, a larger total amount of SMCs was present in the regenerated area of this group. The distance of ingrowth of these cells (when evaluating length of ingrowth from the anastomosis inward) was comparable between groups (Fig. 4C).
Elastic fibers were scarcely found between the newly formed muscle fibers, and slightly more in the COLHEP-group (Fig. 5G) indicated by purple/black fibers in the Masson Trichrome/Verhoeff stain. Nerve fibers were sporadically seen, only at the borders of the regenerated tissue, and no differences between groups were seen (Fig. 6G).
Kidney tissue
No abnormalities were found in kidney tissue (data not shown).
Discussion
In this study, we evaluated regeneration of bladder tissue in a large animal model and used multiple smaller scaffolds instead of one large scaffold. We showed the feasibility of this technique, and were able to regenerate bladder tissue that was almost indistinguishable from native bladder tissue with ingrowth of all essential components of the bladder wall and no necrosis in the scaffold areas. The urothelial layer was completely regenerated in all groups, vasculature was present in the whole tissue, and SMCs were growing into the regenerated area, as well as sporadic small nerve fibers.
Macroscopic evaluation showed that the largest quantity of tissue was regenerated in the COLHEP-group. This was statistically significantly higher compared with the COL-group, but not compared with the COLHEPGF-group. The larger amount of regenerated tissue in the COLHEP-group might be explained by lesser contraction during regeneration due to the highly negative charge of the incorporated heparin with its sulfate and carboxylic groups. The negative charge may protect collagen from proteolysis, and has an inhibitory effect on the macrophage adhesion, hereby delaying degradation of the collagen scaffold which may reduce contraction.14,23 This also explains the larger amount of scaffold remnants at the time of evaluation in the COLHEP-group. This slower degradation process of the collagen scaffold may have resulted in improved regeneration of bladder tissue due to a slower remodeling process. The larger number of myofibroblasts may explain the larger amount of collagen produced in the regenerated tissue. Earlier evaluation is needed to determine whether myofibroblast content or delayed scaffold degradation cause the improved regeneration.
In contrast to previous findings, GF loading did not show a beneficiary effect in this study when bladder regeneration was evaluated after 3 months. In the previous work, we observed improved ingrowth of urothelium, SMCs, and improved vasculature 1 month after implantation with a collagen scaffold loaded with the same GFs as used in the current study. 15 In the previous study, only a beneficial effect on SMC ingrowth was seen after 3 months. 15 This suggests that initially the GFs have a stimulatory effect on ingrowing cells, but this effect seems to wane. The availability and activity of GFs most likely declined after a given time, although GFs were bound to the scaffolds through the use of heparin, which also stabilizes GFs and protects them against proteolytic degradation, creating a sustained release system. 24 Pieper et al. studied the in vitro release profile of FGF2 from a collagen scaffold loaded with heparan sulfate in PBS. 24 Following an initial burst release of 13% at day 1, 53% was gradually released during 4 weeks of incubation. Kanematsu et al. showed similar release profiles of FGF2 loaded to a bladder acellular matrix (BAM) scaffold in PBS or urine in an in vitro study. 25 Furthermore, biological activity was maintained even after 4 weeks when implanted in the subcutis of mice. 25 Clearly, the subcutis and bladder are incomparable, in the bladder the implanted scaffolds are exposed to urine flow, which could increase the wash out of GFs. Data on in vivo release kinetics and activity of GFs incorporated in a collagen scaffold implanted in the bladder are lacking, and particularly important long-term results. Our results of the current and previous studies suggest that the beneficial effects of GF loading can be achieved even in an environment with high urine flow, but that this effect is limited. Furthermore, COLHEP scaffolds may have attracted and bound GFs from the wound environment and hereby improved regeneration. Indeed, heparin can bind a wide variety of proteins and GFs involved in wound healing, like TGF-β. 26 However, by incorporating GFs in a scaffold it is possible to guide regeneration in a favorable way. For instance, TGF-β plays an important role in wound healing, the isoform β1 was considered to increase fibrosis, whereas TGF-β isoform 3 may result in scarless wound healing. Incorporation of these GFs may be optional, although the exact mechanism of TGF-β still needs to be elucidated. 27
In the current study, we used three smaller scaffolds to reach the same regenerated surface area as with one larger scaffold. This decreases the area of tissue remodeling per scaffold to overcome the problem of angiogenesis in large scaffolds. Hereby, the vascularized border of the native tissue will be closer to the center of the scaffold, shortening the time, until this area will be vascularized and reducing the distance for cellular ingrowth. It may be possible to implant more than three scaffolds to improve the augmentation of the bladder. However, one should take into account the sideways alignment of bladder vasculature, which may mean that scaffolds cannot be implanted next to each other; otherwise regeneration may be hampered by insufficient delivery of nutrients and oxygen for regeneration. We used scaffolds of 3.2 cm in diameter to make this study comparable to previous work in which we also used scaffolds of this size.15,28,29 The normal functional capacity of a human bladder is ∼300 mL, at which the bladder has a surface area of 216 cm2. The total area of implanted scaffolds was 21 cm2, which is 10% of the functional capacity of a normal human bladder. To reach clinically significant augmentation, the largest possible diameter and number of scaffolds still resulting in well-vascularized tissue need to be studied.
With larger scaffolds, the strength of the scaffolds may need to be improved. In the current study, we had one animal with urinary leakage due to a rupture of the scaffold at the side of the sutures. Inclusion of a degradable polymer may be a possible solution. Different polymers have already been tested for this purpose, with favorable results of a combination of collagen with vicryl. 30 Additionally, incorporation of autologous urothelial cells and SMCs may improve tissue regeneration. However, harvesting, culturing, and seeding of cells is time and cost consuming. Furthermore, when these cells are harvested from diseased bladders they may behave dissimilar to normal cells, making their use for tissue engineering questionable. 29
We used a porcine model because pigs are of comparable size to humans, have similar abdominal anatomy, and results of smaller animal models often cannot be extrapolated to humans. 31 Urodynamic evaluation showed very high bladder capacities in the studied animals, and it was not possible to study the increase of capacity due to the augmentation. Tu et al. 32 found comparable urodynamic outcomes in their porcine study on bladder tissue engineering. We conclude that the porcine model is inappropriate for studying bladder augmentation by tissue engineering due to the very high compliance and capacity of porcine bladders. Alternatively, goat or sheep models may be more useful for this purpose. 31
Conclusions
Implantation of multiple collagen–heparin scaffolds for bladder augmentation may be a good alternative compared with one large scaffold. We show that this approach is feasible in a porcine model, resulting in tissue almost indistinguishable from native tissue involving all cell layers. Collagen scaffolds with heparin incorporated resulted in a larger area of regenerated tissue, which was statistically significant when compared with the COL-group. To reach clinically significant augmentation, multiple larger collagen–heparin scaffolds, with and without GFs, need to be tested to study the largest possible diameter of scaffold and number of used scaffolds still resulting in well-vascularized tissue. This needs to be performed in a large animal model that is better representative for humans, preferably in preclinical models using dysfunctional/diseased bladders.
Footnotes
Acknowledgments
This work was funded by the European Union, FP6-project EuroSTEC, contract LSHB-CT-2006-037409; “AGIKO stipendium” ZonMw, “The Netherlands Organization for Health Research and Development,” and Radboud University Medical Center, The Netherlands, project No. 920-03-456; Noviotissue: “Pieken in de delta” (PID 101020). The authors would like to thank the employees of the Central Animal Laboratory, Radboud University Medical Center, for their outstanding assistance at the performed animal operations.
Disclosure Statement
No competing financial interests exist.