
Abstract
Tissue hypoxia is a critical driving force for angiogenic and osteogenic responses in bone regeneration and is, at least partly, under the control of the Hypoxia Inducible Factor-1α (HIF-1α) pathway. Recently, the widely used iron chelator deferoxamine (DFO) has been found to elevate HIF-1α levels independent of oxygen concentrations, thereby, creating an otherwise normal environment that mimics the hypoxic state. This has the potential to augment the biological properties of inorganic scaffolds without the need of recombinant growth factors. This pilot study investigates the effect of local delivery of DFO on bone formation and osseointegration of an anatomically matched bone graft substitute, in the treatment of segmental bone defects. Three-dimensional printing was used to create monetite grafts, which were implanted into 10 mm midshaft ulnar defects in eight rabbits. Starting postoperative day 4, one graft site in each animal was injected with 600 μL (200 μM) of DFO every 48 h for six doses. Saline was injected in the contralateral limb as a control. At 8 weeks, micro-CT and histology were used to determine new bone growth, vascularity, and assess osseointegration. Six animals completed the protocol. Bone metric analysis using micro-CT showed a significantly greater amount of new bone formed (19.5% vs. 13.65% p = 0.042) and an increase in bone-implant contact area (63.1 mm2 vs. 33.2 mm2 p = 0.03) in the DFO group compared with control. Vascular channel volume was significantly greater in the DFO group (20.9% vs. 16.2% p = 0.004). Histology showed increased bone formation within the osteotomy gap, more bone integrated with the graft surface as well as more matured soft tissue callus in the DFO group. This study demonstrates a significant increase in new bone formation after delivery of DFO in a rabbit long bone defect bridged by a 3D-printed bioresorbable bone graft substitute. Given the safety, ease of handling, and low expense of this medication, the results of this study support further investigation into the use of iron chelators in creating a biomimetic environment for bone healing in segmental bone loss.
Introduction
T
Recent work has shown that synthetic grafts prepared from calcium hydrogen phosphates, brushite, and monetite demonstrate osteoconductive and osteoinductive properties and preferable resorption rates. 3 Their ability to be 3D-printed to match the size and geometry of any defect could further enhance their clinical use.4,5 While these biomaterials have shown promise, the success of any scaffold-based bone regeneration approach relies on the induction of new blood vessels within the construct. 6 Upon scaffold implantation, vascularization occurs primarily from the periphery and is limited to micrometers per day, 7 delaying nutrient and oxygen supply centrally. Numerous attempts have been made to manipulate angiogenesis to create a biomimetic environment for bone healing, but till to date have not yielded a viable autograft alternative. 8 This has been, in part, due to the practical, safety, and financial considerations in producing and administering supraphysiological doses of angiogenic recombinant proteins such as vascular endothelial growth factor (VEGF).
Tissue hypoxia, following injury, itself is thought to be a driving force for angiogenesis. This response is at least partially controlled by hypoxia-inducible factor-1α (HIF-1α), a cellular transcription factor that activates in hypoxic conditions and results in the stimulation of numerous proangiogenic genes. 9 In bone, the HIF pathway has also been shown to modulate the recruitment and function of osteoblast and osteoclast precursors at sites of injury.10,11 As such, the genetic and pharmacologic manipulation of HIF-1α has become an exciting area of investigation. 12 Interestingly, several small molecules known collectively as hypoxia mimics have been shown to activate HIF-1α even in normoxic conditions. 9 Of these, the iron chelator deferoxamine (DFO) has been most extensively studied and shown to induce vascular growth when delivered locally into fractures.13–15 This property, together with its stability, excellent safety profile, and low cost, infers its possible utility in conferring biomimetic properties to inorganic bone scaffolds. No study to date has investigated the effect of a prolonged delivery of DFO in conjunction with a synthetic resorbable calcium phosphate scaffold in a midsized preclinical bone defect model. This study aims to test the hypothesis that DFO can enhance bone formation and osseointegration in 3D-printed monetite grafts used to bridge segmental bone defects.
Materials and Methods
Graft design
A 3D powder printer was used to fabricate 1 cm long microporous dicalcium phosphate dihydrate (brushite) grafts that matched the anatomy of the rabbit ulnar shaft based on several CT scan measurements (Fidex Animage scanner, Pleasanton, CA). Two small pegs (2 mm) were added on either end to stabilize the grafts within the intramedullary canal (Fig. 1b). The 3D printing technique has been previously described. 16 Tricalcium phosphate (TCP mixture of α/β) was first synthesized by heating a 2:1 M mixture of dicalcium phosphate anhydrous (CaHPO4, monetite) (Merck, Darmstadt, Germany) and calcium carbonate (CaCO3, calcite) (Merck, Darmstadt, Germany) at 1400°C for 5 h. This material was crushed and subsequently milled (PM400; Retsch, Germany) for 10 min. Brushite grafts were printed with a 3D-powder printing system (Z-Corporation, Rock Hill, CA) using a 20% phosphoric acid (H3PO4) binder and TCP powder (layer thickness of 125 μm). Samples were retrieved from the powder bed and then soaked in 20% H3PO4 for 3 min to promote conversion of unreacted TCP to brushite. Before implantation the grafts were thermally dehydrated to monetite and sterilized using a standard autoclave (121°C; humidity 100%; 30 min).

Implantation
The surgical protocol was approved by the Ethics Committee for Animal Care of McGill University in accordance with the standards established by the Canadian Council on Animal Care. Eight New Zealand rabbits (3.5–4.0 kg) were used for this study. Following anesthesia, both upper extremities were shaved and the cutaneous surface was disinfected and draped in a sterile manner (Fig. 1c). The subcutaneous boarder of the ulna was identified, and a 15 mm incision was made over it centered in the midaspect of each forearm. The deep fascia was incised and the muscles were removed from the middiaphyseal ulna in a subperiosteal manner. An osteotomy site of 10 mm was measured and cut using a microbur (Stryker) taking into account the diameter of the bur head. The interosseous membrane deep to the ulna was sharply cut exposing the radius. On the proximal aspect of the osteotomy site, a 2 mm slit was created to accommodate placement of the graft peg. A sterile graft was press-fit within the osteotomy site in each limb. The wound was irrigated and closed in layers using absorbable sutures. After surgery, rabbits were allowed free motion and unrestricted access to food and water for the duration of the experiment. Animals were monitored daily for signs of inflammation, lethargy, and for general well-being by an experienced animal care technician. Postoperative analgesia was achieved with IM administration of 5–20 μg/kg buprenorphine every 8 h for 3 days.
Delivery of DFO
Starting on postoperative day 4, all rabbits were injected with 600 μL of 200 μM DFO solution in normal saline (Sigma, Oakville, ON, Canada) directly into the graft site of one limb chosen randomly. The rabbits were mildly sedated before each procedure, and a 26-gauge needle was used to deliver the solution carefully at the graft site. The contralateral limb graft was injected in an identical manner with 600 μL of normal saline as a control. The procedure was repeated every 48 h for a total of six doses with the same limbs always receiving the DFO solution and saline control. The DFO dose and injection schedule were extrapolated from a review of the literature on the use of DFO in animal models of bone healing13,15,17–20 and adapted to our larger animal size.
Postoperative course
All animal limbs were radiographed postoperatively at 2, 4, and 6 weeks using a Fidex Animage scanner (Pleasanton) to monitor for signs of bone bridging. After a total of 8-week implantation time, all animals were euthanized, and the ulna diaphysis containing the stabilized grafts was explanted. The bones were stripped of surrounding soft tissue and immediately fixed in cold 4% formaldehyde for 1 day before further analysis.
Micro-CT
Micro-CT was used to quantify the new bone growth surrounding and within each graft as well as the overall resorption of all grafts. A high-resolution Skyscan 1172 micro-CT instrument (Soquelec, Montreal, QC, Canada) was used at a voltage of 80 kV and power of 10 W, with 0.5 mm aluminum and copper filters to scan all explants. Scans were captured at 13 μm image resolution and 0.45° rotation. Reconstructed axial slices of the explant were analyzed using the associated software. A region of interest (ROI) was created as a fixed square of 9 × 9 mm to encompass the osteotomy site, while excluding the radius bone. This ROI was extrapolated over a constant number of axial slices to create a rectangular volume of interest (VOI) measuring 13.9 mm in length. The most proximal axial cut was selected as the first cut, in which remaining graft was visible. This method created a fixed VOI in each sample for analysis. Using various custom-created threshold and morphological operations, new bone formed in the osteotomy site was distinguishable from remaining graft material. A ratio of new bone volume over a constant total tissue volume (BV/TV) was determined for each sample. Remaining graft volume to total tissue volume was also calculated. To assess the effect of DFO on osseointegration of the monetite graft, the bone-implant contact (BIC) area was determined. This parameter quantifies the intersection surface area of new bone apposed to the implant. These results were compared between the DFO-treated limbs and saline controls. Vascular channels within new bone and the implant were quantified over the same VOI, using an algorithm developed by Bruker (Bruker micro-CT academy 2016 v5.3). The protocol creates volumetric calculation of the network of open channel pores that are continuous throughout the sample and represent sizes that correspond to vascular formations (>50 μm diameter). Quantitative data for vascular channels include vascular channel volume/tissue volume (ChV/TV), vascular channel number (Ch.N), and vascular channel thickness (Ch.Th mm × 10−3).
Histological analysis
Fixed samples were dehydrated in ascending concentrations of ethanol and subsequently infiltrated for 72 h and embedded in polymethyl methacrylate resin (Technovit; Leica Microsystems GmbH, Wetzlar, Germany). Coronal histological sections (15 μm) crossing the centermost point of the grafts were cut using a diamond saw (SP1600 Leica Microsystems Concord, ON, Canada). Sections were stained with methylene blue and basic fuchsin as per Tamimi et al. 4 to qualitatively assess new bone growth, soft tissue, and graft resorption.
Statistical analysis
Student's t-test was used for comparison of means of new bone growth and remaining grafts between the two groups (SPSS version 20). p < 0.05 was determined to be significant.
Results
Material characterization
X-ray diffraction analysis of the graft confirmed it to be phase-pure monetite, indicating that thermal conversion of brushite to monetite had occurred (Fig. 2).

X-ray diffraction pattern of grafts after production showing the characteristic peaks of monetite (*). Color images available online at www.liebertpub.com/tea
Clinical observations of surgical protocol
Six of the eight animals underwent the surgical procedure without any complications. One animal went into cardiopulmonary arrest in the first 2 h postoperatively and died. In another animal, the radius was accidently penetrated by the bur during the ulnar osteotomy, creating conditions leading to a unicortical fracture in one limb. Postoperatively, upon weight-bearing, the radius fractured, and the animal was euthanized in accordance with the ethical principles of the study. All other animals were weight-bearing on the upper limbs by 24 h after surgery. No local toxicity or abnormal animal behavior was observed after injection of the iron chelators. Upon surgical explantation, there were no signs of foreign body reaction to the implants or to DFO in any of the animals.
Radiological observations and analysis
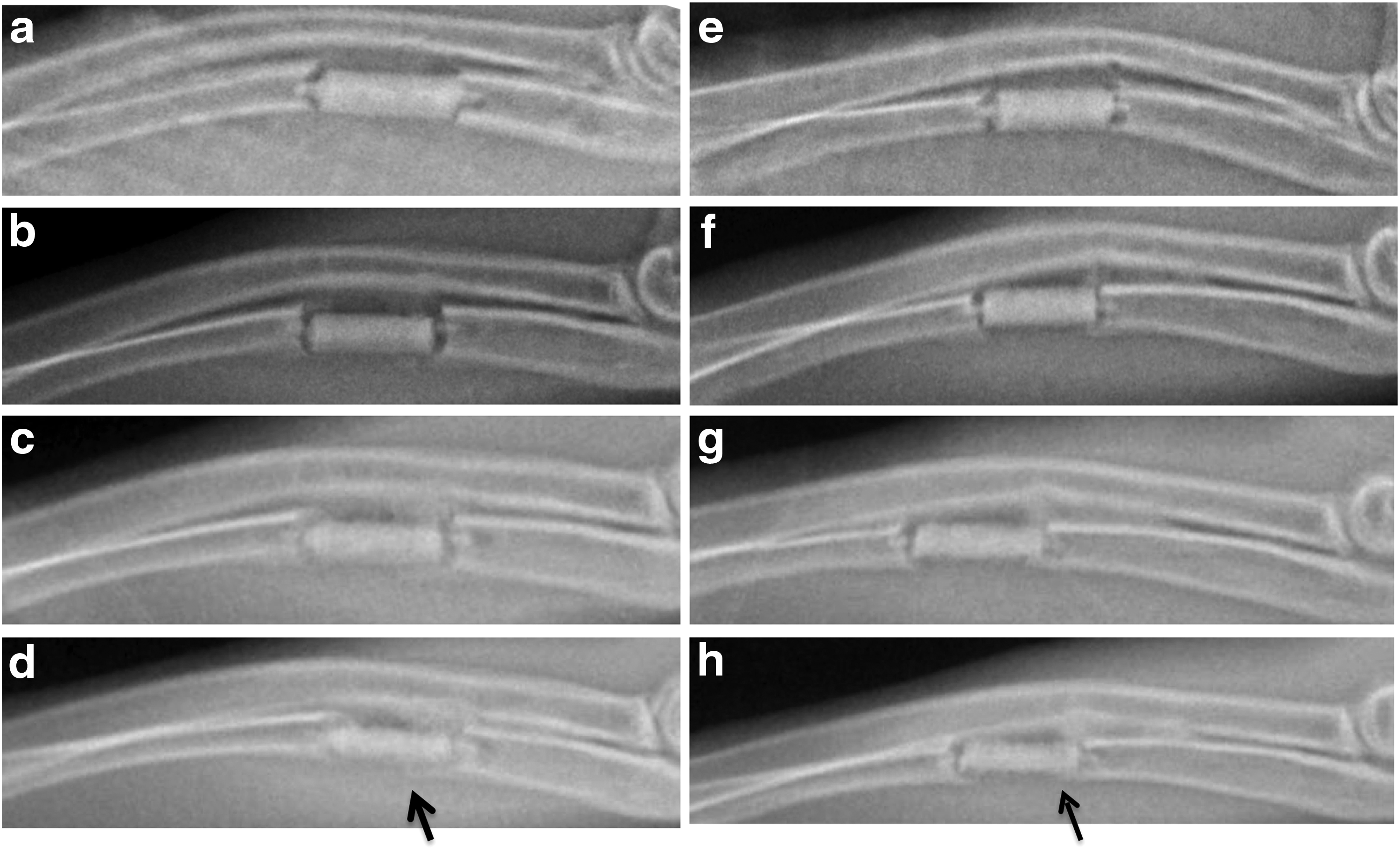
Figure 3 shows sequential X-rays of the implantation site for up to 6 weeks postoperatively. At 4 weeks, we observed some integration of the cortical bone with the graft material in the DFO group, but less so in the saline group (Fig. 3c, g). By 6 weeks, qualitative assessment of the plain films appeared to have more bone growth from the ends of the osteotomy in the DFO group compared with the saline controls (Fig. 3d, h). Following explantation at 8 weeks, micro-CT showed an increase in new bone formation in the DFO group compared with controls (Fig. 4). Bone metric analysis demonstrated an average increase in BV/TV in the DFO group (19.5%) compared with the saline group (13.65%) that was statistically significant (p = 0.042) (Fig. 4). Figure 5 shows the BV/TV in each individual animal. Bone growth was larger in the DFO limb of all animals except one (R4). In this animal, the initial postoperative radiograph of the limb injected with saline showed a residual cortical bridge of the ulna at the osteotomy site. The ulna was not fully resected. Given that the large amount of remaining ulnar bone was indistinguishable from new bone produced, this limb was excluded from our average bone metric analysis. Graft resorption was similar between the two groups with the remaining graft volume being an average of 75.3 mm3 in the DFO group and 77.8 mm3 in the saline group. Despite similar graft resorption profiles in both groups, BIC area was greater in the DFO group (63.2 mm2 compared with 33.3 mm2 p = 0.03), indicating increased osseointegration of grafts treated with DFO. Using a quantification of continuous, connected channel volume as a measure for vascularity, vessel channels volume/tissue volume was significantly higher in the DFO group compared with controls (20.9% vs. 16.1% p = 0.004) (Fig. 6). Channel number was also significantly higher while channel thickness was similar.
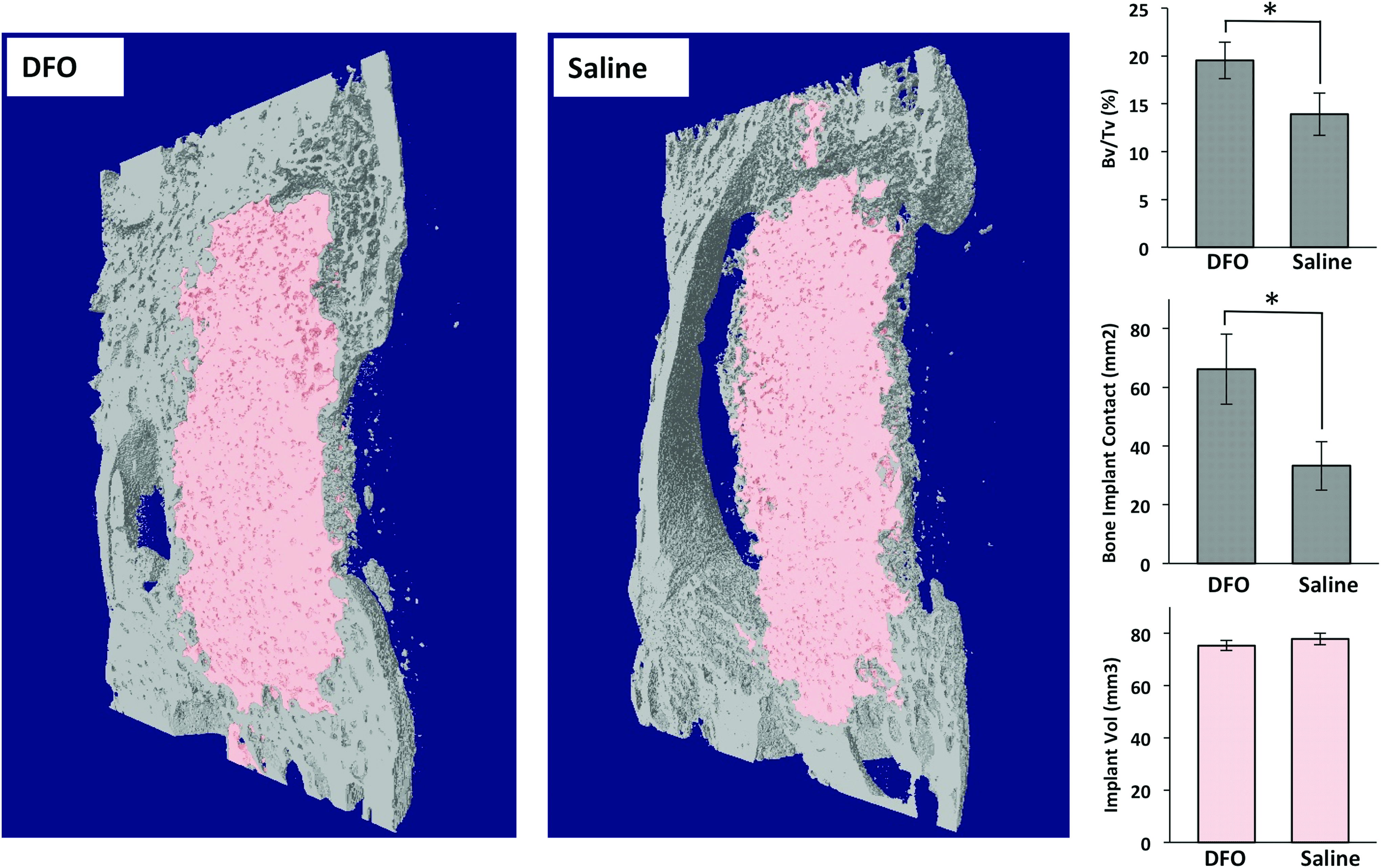
Left: 3D reconstructions of the micro-CT scans of the osteotomy sites postexplantation from the same animal. The pink material represents remaining graft material, and the gray represents bone formation. Increased bone is seen in the DFO-injected limb compared with the saline control explants. Right top: Graph showing the average bone volume/tissue volume (BV/TV) over a uniform volume of interest. A significant difference is observed between the DFO and control groups. Right middle: Graph showing the bone implant contact area over a uniform volume of interest. A significant difference observed between the DFO and control groups. Right bottom: Graph showing the average remaining graft volume postexplantation. No difference was seen between the DFO and control groups. (* represents a p < 0.05). Color images available online at www.liebertpub.com/tea
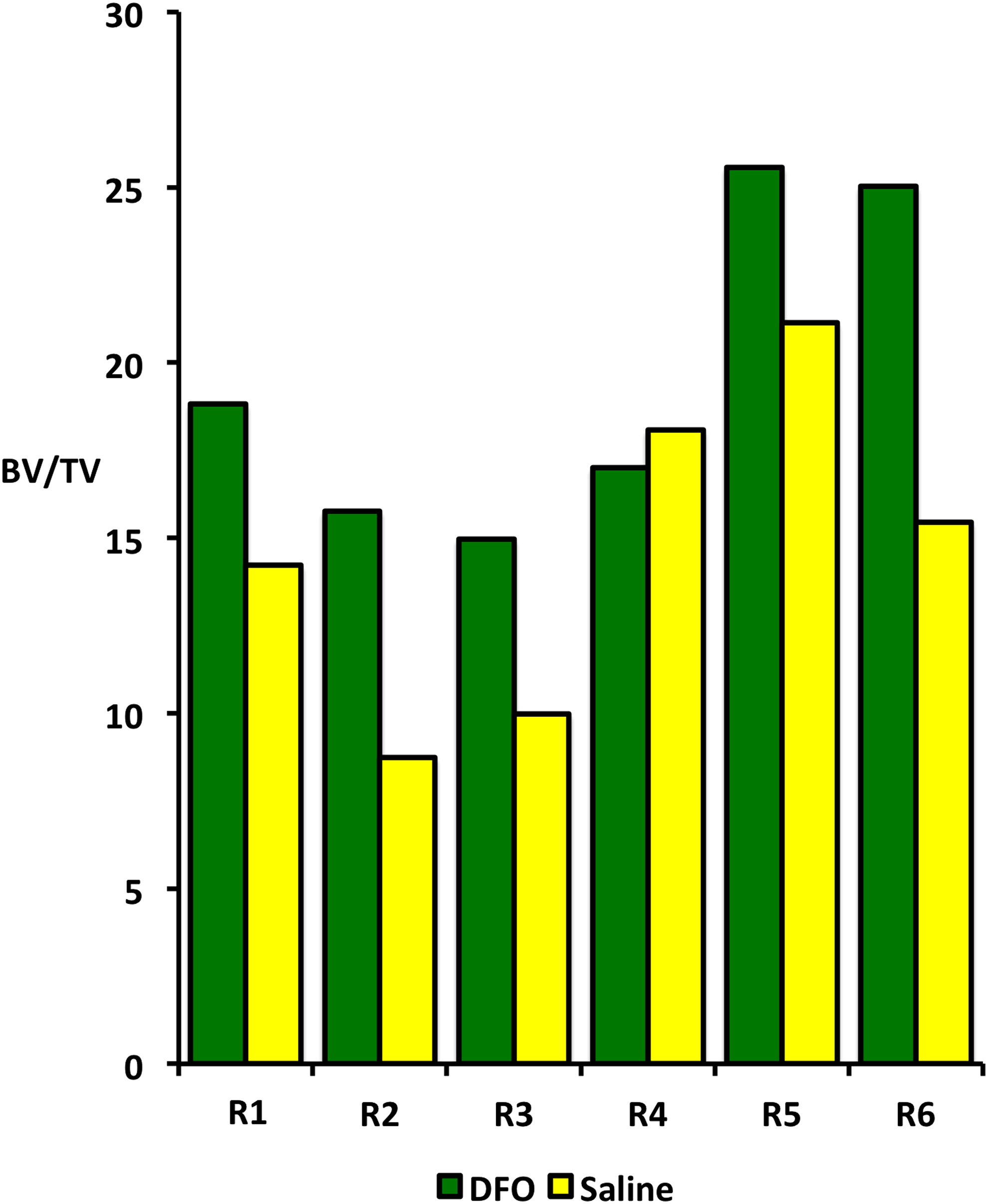
New bone growth in each of the six rabbits. Five of the six rabbits showed that more bone had regenerated in the DFO limb compared with the saline limb. Rabbit 4 showed more bone in the saline control limb, however, postoperative X rays revealed that an incomplete osteotomy was performed in the saline limb of this animal, therefore, exaggerating the recorded bone regeneration at the osteotomy site. Color images available online at www.liebertpub.com/tea

Left: 3D reconstructions of the micro-CT data of a selected 2 mm thick section of the ososteotomy site of each limb (DFO/Saline) of the same animal. The top two images show the cross-sectional images and the bottom two show the reconstructions tilted 45° from the horizontal. Red represents connected and uninterrupted channels greater than 50 μm in diameter, which are interpreted as vascular channels. Yellow represents bone and gray represents remaining graft. An increase in total vascular channels is seen in the DFO-injected limb compared with the saline control. Within the graft material more channels are seen in the DFO sample. Right top: Graph showing the average vascular channel volume/tissue volume (BV/TV). A significant difference is observed between the DFO and control groups. Right middle: Graph showing the average vessel channel number. A significant difference observed between the DFO and control groups. Right bottom: Graph showing the average vessel channel thickness. No difference was seen between the DFO and control groups. (* represents a p < 0.05). Color images available online at www.liebertpub.com/tea
Histology
Qualitative histological analysis was performed to verify the results of the radiological analysis. Coronal sections through the middle of the graft showed increased bone formation within the osteotomy gap, more bone integrated with the graft surface as well as more matured soft tissue callus in the DFO group (Fig. 7). Higher magnification demonstrated that bone had integrated with the graft surface pores in the DFO group compared with the saline group where soft tissue was observed surrounding most of the graft material (Fig. 7).
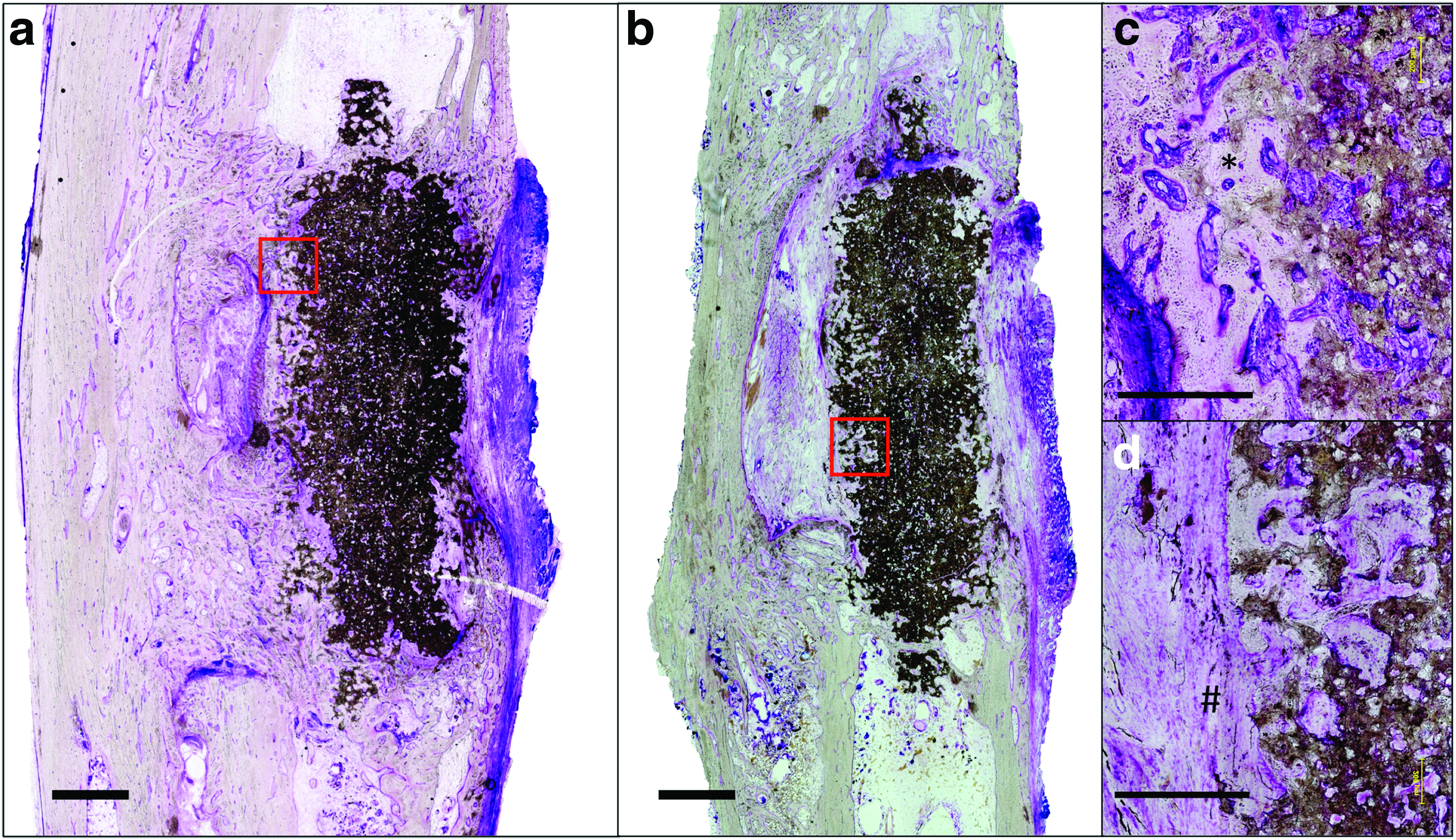
Histological coronal sections taken through the center of the graft site. Increased bone regeneration is seen in the DFO group
Discussion
This pilot study demonstrates that the local delivery of low doses of the iron chelator DFO promotes bone growth and osseointegration of bioceramic scaffolds in a long bone defect. Through radiological and histological analysis, we observed that more bone had grown within the osteotomy site in the DFO group. Moreover, the new bone integrated thoroughly with the surface pores of the graft material in the DFO group. In the saline group, large areas of soft tissue surrounded the edge of the graft material. Clemens and colleagues first reported preclinical outcomes using DFO for bone regeneration. 20 In this study, mice undergoing tibia distraction osteogenesis had five doses of DFO (20 μL of a 200 μM solution) or saline control locally injected within the distraction gap. At day 31, micro-CT and histological analysis demonstrated significantly increased vascularity and bone volume within the distraction gap in the DFO treatment group. 20 In a follow up study, similar results were observed in a mouse fracture model. 13 Since then, numerous studies have built on this work, further demonstrating the potential of iron chelators to improve vessel and bone growth in fracture models and distraction osteogenesis.17,18,21,22 However, few studies have examined this medication on osseointegration of bioresorbable bone substitutes within long bone defects. Steward et al. examined the angiogenic and osteogenic response to a DFO-loaded polypropylene fumarate/tricalcium phosphate scaffold compared with a nonloaded control in rat femoral defects. 23 Only surrounding vessel number increased significantly in the DFO scaffolds, while new bone growth did not. 23 Zhang et al. incorporated DFO within a bovine bone ceramic scaffold by soaking the graft with a 4 mM DFO solution before implantation within a rabbit ulnar defect. They showed increases in several measured radiological bone metrics in the DFO group compared with the control scaffolds. 24 This work did not quantify the amount of DFO in each sample nor did it formally assess the release profile of DFO from the scaffold making it difficult to infer the length of time and the local concentration of DFO in the healing site. Our study is the first to examine the effects of a prolonged delivery of micromolar doses of DFO on bone regeneration in a midsized animal bone defect.
While the molecular mechanisms responsible for the observed osseous response to DFO were not explored in the current study, previous work strongly suggests that this process is occurring through the induction of the HIF-1α pathway. 9 HIF-1α acts as a cellular oxygen sensor.11,25 It is constitutively expressed in cells but the protein product is rapidly degraded in well-oxygenated tissues by specific prolyl-hydroxylase (PHD) proteins.26,27 Under hypoxia, the oxygen-dependant enzymatic activity of PHD proteins is diminished, resulting in a functional expression of HIF-1α. 28 In addition to oxygen, PHD proteins depend on a number of cofactors, including iron (Fe+2), that is critical for the hydroxylation reaction that targets HIF-1α for degradation. 29 Iron chelation can therefore indirectly increase the level of HIF-1α by inhibiting PHDs, thus creating a hypoxia mimicking microenvironment.30,31 HIF-1α expression triggers a transcriptional cascade of multiple hypoxia response genes involved in angiogenesis, cellular survival, and regeneration. Within bone, HIF-1α specifically couples angiogenesis and osteogenesis by regulating the VEGF-dependant recruitment of vessels and contributing to the release of growth signals from invading vessels themselves, resulting in the recruitment and activity of osteoprogenitor cells. 9 From this effect, iron chelators have a potential to confer biomimetic properties of hypoxia-regulated bone repair to inorganic materials.
This study used a dose of DFO and an administration cycle known to induce HIF-1α in rodent models. 9 We increased the fluid volume administered to best suit the larger sized animal model. We observed a significant increase in vascular channel number and volume within the new bone and graft material in DFO-treated samples. Quantitative vascular data was obtained using an established protocol of extrapolating vascularity from a volumetric calculation of open continuous channels representing sizes that correspond to vascular formations. While microangiography using a contrast agent injected through a central artery may result in a more robust measurement of vessel volume, our findings of an increase in channel number and volume, but not channel thickness, can confidently be interpreted as an increase in number of similarly sized vessels within the DFO-treated samples compared with controls. This finding supports the hypothesis that DFO increases bone regeneration through HIF-1α-regulated angiogenic–osteogenic coupling. 20 Future work should aim to characterize the gene expression patterns within the constructs following DFO administration to gain further insight into the molecular mechanisms governing the observed phenotypic response to iron chelation. For instance, HIF-1α activity may have a direct influence on mesenchymal stem cell (MSC) differentiation with reported findings showing both support and inhibition of osteogenic differentiation of MSCs.32–34
The dicalcium phosphate, monetite (CaHPO4), was used in this study, given its osteoconductive and osteoinductive properties as well as its favorable in vivo degradation profile.3,35 Moreover, monetite sustains its phase composition in physiological conditions and does not convert to hydroxyapatite allowing sustained resorption and remodeling into host bone.36,37 In addition, we have previously shown that a sustained delivery of DFO does not impart any phase conversion reactions on implanted monetite grafts. 38 In this model, DFO did not affect the overall resorption of the graft material. HIF-1α has been shown to increase osteoclast differentiation and resorptive function.10,39,40 Moreover, the positive effects of VEGF activation on osteoclast recruitment and resorptive function have been well documented.41,42 Therefore, we could expect an increase in graft resorption in the DFO group. However, other in vitro studies demonstrate that DFO can inhibit osteoclast differentiation possibly through HIF-independent mechanisms.43–46 Thus, depending on whether bone in synthetic grafts is formed by replacement of a soluble osteoconductive matrix or by cellular remodeling, hypoxia biomimicry may either promote or inhibit graft remodeling. Indeed, we have recently shown that two different iron chelators inhibit in vivo osteoclast-mediated resorption and reduce bone formation in a nonweight-bearing onlay graft model. 38 In vivo, bioceramic graft resorption occurs by both passive material dissolution and cell-mediated resorption.47,48 In a weight-bearing model, persistent graft loading and surrounding muscle contractions create high fragmentation forces on the material and increase surrounding fluid circulation. Therefore, fragmentation and dissolution, which are constant variables in the two groups of this study, might have a greater influence on monetite degradation and possibly overpower any differences in cell-mediated resorption that may also be occurring.
Established technology in our laboratory on 3D powder printing and calcium phosphate chemistry was used for the rapid fabrication of the bioceramic implants in this study. 49 The novelty in the current work was the addition of two small pegs on either side of the implanted graft that add several advantages to the implant. They maintain an accurate orientation of the graft material during press-fitting. They also stabilize the graft in a centralized position within the intramedullary canal of the ulna without the use of implants. No rabbits in our study demonstrated significant displacement of the graft material from the osteotomy site during healing. This work presents a grafting model that can be used for further assessments of materials and biologics.
In this study, we used six repeated injections of DFO to deliver the agent to the grafting site. Repeated injection into healing tissues limits the clinical translation of the delivery technique compared to preimplantation absorption of DFO to monetite. However in our experience, DFO completely dissipates from calcium phosphate materials in vitro within the first 24 h of physiologic incubation. 38 Hertzberg et al. attempted to use calcium sulfate pellets as a carrier agent of DFO. Using a mouse metatarsal angiogenesis assay, they showed an increased vascular response to DFO-loaded pellets compared with nonloaded controls. 50 However, when the loaded pellets were immersed in a control media for 30 min before the angiogenesis assay, vascular growth diminished, indicating that DFO rapidly released from the material. This further illustrates the difficulty of using ceramic carrier agents for the controlled delivery of this water-soluble drug. Saito et al. incorporated DFO within a gelatin hydrogel and demonstrated that after an initial release of 60% of the drug by diffusion, the remaining incorporated DFO released in a similar profile to the degradation of the gel by tissue collagenases. 51 Most interestingly, Jia et al., recently added DFO to porous poly(Lactic-co-glycolic acid) scaffolds. They demonstrated a sustained release of DFO, with approximately 20% released by 48 h and nearly 80% by 7 days. Incorporation of this scaffold within femoral bone defects of an osteoporotic rat model resulted in significantly more bone and vasculature within the defects compared with controls. This system shows promise and highlights the likely need of combining polymeric and ceramic scaffolds in further exploration of tissue-engineered hypoxia biomimetic constructs. 34
Although the small sample size in this study of n = 6 in the treatment group and n = 5 in the control group limits the confidence level, it is important to highlight the primary outcome reaching statistical significance. A power analysis based on previous literature surrounding the administration of DFO determined that a sample size of n = 4 was needed in the study to observe a 20% difference in bone volume between the two groups. In this pilot study, we selected an animal number of n = 8 to account for unexpected variability and any unforeseen loss of animals from postsurgical complications. The findings from our study add to the literature supporting a strong potential of iron chelators in bone regenerative procedures, 9 nevertheless, further work using a larger number of animals needs to be performed.
In conclusion, this study shows a significant increase in bone growth and osseointegration after the delivery of hypoxia mimicking DFO in a rabbit long bone defect bridged by a 3D-printed bioresorbable bone graft substitute. These results are observed in a weight-bearing model, in which graft fragmentation and passive dissolution are likely predominant mechanisms of graft degradation allowing for subsequent bony ingrowth. This study adds to the body of literature surrounding the use of iron chelators as a hypoxia biomimetic agent for bone regeneration. Given the safety, ease of handling, and low expense of DFO, translation of this widely used medication into clinical trials is of great interest to the orthopedic community.
Footnotes
Acknowledgments
This work was supported by A.O. Trauma North America and Foundation of Orthopedic Trauma (J.D.). NSERC Discovery Grant (J.B.), MDEIE Québec-Bavaria collaboration grant, (J.B., U.G.).
Disclosure Statement
No competing financial interests exist.