
Abstract
Restoring lost bone is a major challenge in orthopedic surgery. Currently available treatment strategies have shortcomings, such as risk of infection, nonunion, and excessive resorption. Our primary aim was to study if a commercially available gentamicin-containing composite calcium sulfate/hydroxyapatite biomaterial (GBM) could serve as a carrier for local delivery of bone morphogenic protein-2 (BMP-2) and zoledronic acid (ZA) in a tibia defect model in rats. Empty and allograft-filled defects were used as controls. A 3 × 4-mm metaphyseal bone defect was created in the proximal tibia, and the rats were grouped according to defect filling: (1) Empty, (2) Allograft, (3) GBM, (4) GBM + ZA, and (5) GBM + ZA + BMP-2. In vivo microcomputed tomography (micro-CT) images at 4 weeks showed significantly higher mineralized tissue volume (MV) in the intramedullary defect region and the neocortical/callus region in all GBM-treated groups. After euthanization at 8 weeks, ex vivo micro-CT showed that addition of ZA (GBM + ZA) and BMP-2 (GBM + ZA + BMP-2) mainly increased the neocortical and callus formation, with the highest MV in the combined ZA and BMP-2-treated group. Qualitative histological analysis, verifying the increased neocortical/callus thickness and finding of trabecular bone in all GBM-treated groups, supported that the differences in MV measured with micro-CT in fact represented bone tissue. In conclusion, GBM can serve as a carrier for ZA and BMP-2 leading to increased MV in the neocortex and callus of a metaphyseal bone defect in rats.
Introduction
T
In this study, we modified a commercially available gentamicin-containing composite calcium sulfate/hydroxyapatite biomaterial (GBM) by adding ZA and BMP-2 for potential use in clinically challenging conditions with a low chance of success, e.g., after an infected nonunion or an open fracture with substantial bone loss. The primary aim of our study was to determine if this commercially available GBM could serve as carrier for ZA and BMP-2. The carrier function was evaluated in a previously described metaphyseal unicortical tibial bone defect model in rats, where both cortical and intramedullary changes in mineralized tissue were measured using micro-CT. 20 As negative control, we used an empty defect, while an allograft-filled defect was chosen as a current clinical alternative.
Materials and Methods
Study plan
The animals were randomly allocated to one of five groups (n = 10 per group) according to the material used for bone defect reconstruction: (1) Empty defect (Empty); (2) Allograft (Allograft); (3) GBM (GBM); (4) GBM and ZA (GBM + ZA); and (5) GBM, ZA, and BMP-2 (GBM + ZA + BMP-2). In the Empty group, one rat died during anesthesia. In vivo micro-CT imaging was performed at an intermediate time point of 4 weeks. At 8 weeks, all animals were sacrificed using an overdose of pentobarbital sodium. Subsequently, the defect bone region was examined with plain radiography, ex vivo micro-CT, and histology.
Ethical approval
This study was approved by the local ethics board (Ethical approval. No. M79-15) and conducted according to the rules of the Swedish Board of Agriculture.
Materials
The two bone-active substances used in our study were Zoledronic Acid (4 mg/5 mL) (Actavis) and rhBMP-2 (INFUSE® Bone Graft, Medtronic). The gentamicin-containing composite calcium sulfate/hydroxyapatite biomaterial (GBM) was CERAMENT™ G (BONESUPPORT AB, Lund, Sweden). Sprague-Dawley rats (6 weeks of age) with an average weight of 327 g (279–358 g) (Taconic, Denmark) at surgery were used.
Material preparation
Harvesting allografts: The cancellous allografts were harvested from the femora and tibiae of five rats of the same strain, age, and sex as the rats used in the study using a premade cylindrical mold of 2 mm diameter, excluding the articular cartilage and the cortical bone. The grafts were frozen at −80°C and freeze-dried for 48 h in sterile conditions. The recipient animals received allograft from only one donor.
Preparation of the GBM: The GBM was prepared by mixing the powder (60% calcium sulfate, 40% hydroxyapatite), gentamicin, and saline in ratios specified by the manufacturer to form a paste.21–23 The total amount of gentamicin per animal was 0.875 mg. In the groups where ZA was added (GBM + ZA and GBM + ZA + BMP-2), saline (12.5 μL) was replaced by ZA solution, resulting in a final amount of 10 μg ZA per animal. In the BMP-2 group (GBM + ZA + BMP-2), BMP-2 (5 μg) was dissolved in saline and added to the paste along with ZA (10 μg).
The dose of ZA (10 μg) was chosen to match a previously published study, evaluating the codelivery of BMP-2 and ZA from the same GBM as used in our study. 24 The dose of BMP-2 was chosen as per a previous study, which showed no differences when 5 or 10 μg BMP-2 was used in conjunction with a local ZA dose of 10 μg. 25
Surgical procedure
The animals were housed, two per cage, with access to food pellets and water ad libitum. At surgery, the animals were anesthetized using a combination of ketamine (100 mg/kg) and xylazine (11 mg/kg) using an intraperitoneal injection. The surgical site (right tibia) was shaved and sterilized using chlorhexidine alcohol. A 1-cm incision was made on the medial side along the proximal tibia. The periosteum was scraped off in a proximal direction toward the physis. A sharp drill was used to make a hole in the cortical bone distal to the physis in the metaphysis, followed by drilling using a drill bit 3 mm in diameter and 4 mm in depth (Fig. 1).
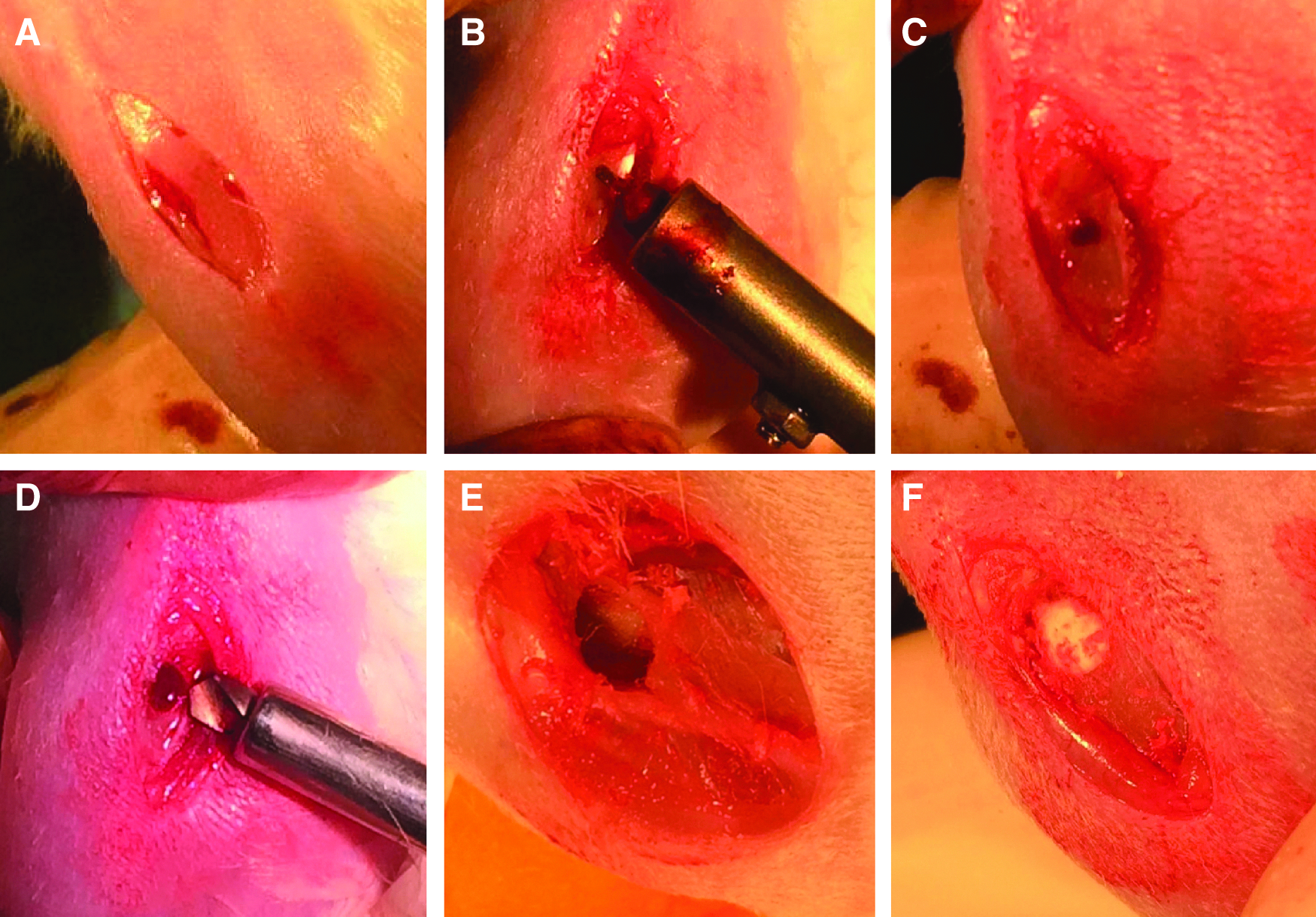
The surgical procedure.
The defect was then cleansed using sterile gauze and filled according to treatment group or left empty. In the Allograft group, the graft was impacted gently to fill the defect. The groups with GBM were filled using 50 μL of the paste added to a graded syringe (1 mL). The paste (50 μL) was extruded onto a sterile dish. Ten-minute waiting time was set after finishing mixing the liquid components to allow the paste to reach a state at which the GBM was getting moldable, yet not hardened. After desired consistency was achieved, a spatula was used to fill the defect with the GBM and gentle pressure applied to the material using a dental filling instrument. The wound was closed using nonresorbable single sutures, and no wound complications were observed postoperatively. Subcutaneous buprenorphine (0.05 mg/kg) was given immediately postoperatively for pain relief.
Radiography
After sacrifice at 8 weeks postsurgery, all tibiae were oriented in a similar manner and analyzed on a clinical grade X-ray machine (GE Healthcare discovery, CT) for visualization (Fig. 2).
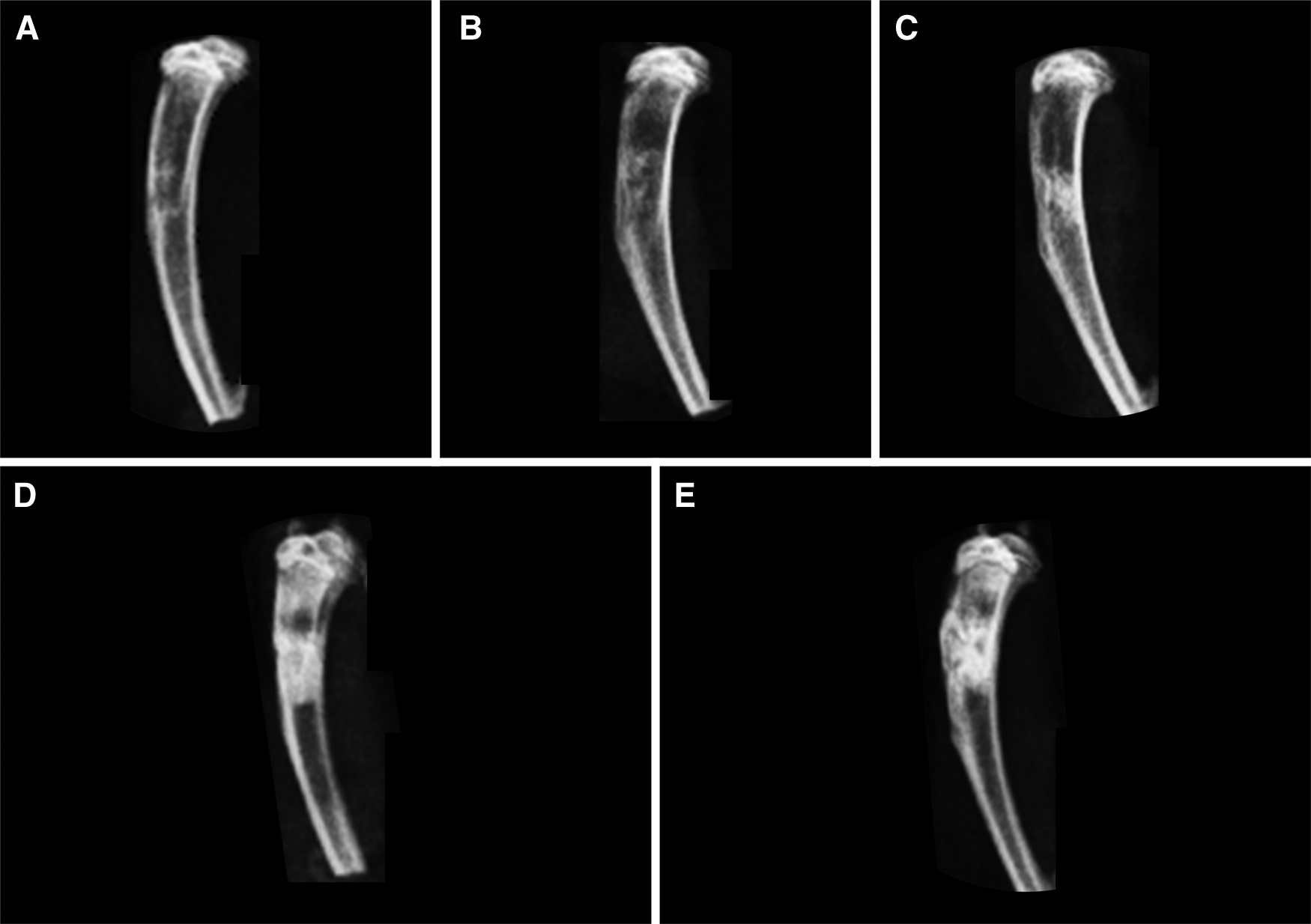
Radiographs of the extracted rat tibiae at 8 weeks.
Micro-CT imaging
Micro-CT imaging was conducted in vivo at 4 weeks postsurgery and ex vivo after sacrifice at 8 weeks postsurgery (details described below). In both cases, the images were acquired with a NanoScan system (Mediso Medical Imaging Systems, Budapest, Hungary) at an operating voltage of 65 k, exposure time of 1300 ms, and using a RAMLAK filter. For in vivo imaging, animals were anesthetized using 2% isoflurane. The images were postreconstructed (VivoQuant 1.22, Nucline software, inviCRO, Boston, MA) using a 27 regular sampling mode to a voxel size of 19 μm. A threshold grayscale value of 105 was chosen. For ex vivo micro-CT scanning, tibiae were placed in 5-mL Eppendorf tubes. The images were postreconstructed with a 27-regular sampling mode to a voxel size of 10 μm. A threshold grayscale value of 110 was chosen. The imaging parameters were chosen to obtain the best possible image resolution with both modalities. Since this resulted in different settings between in vivo and ex vivo images, it was not possible to directly compare the data across time points.
All images were reoriented using Data Viewer (Skyscan, v. 1.4) to ensure similar 3D orientation of all samples and analyzed with CTAn (v. 1.9.1.0 Skyscan, Belgium). Three regions of interest (ROIs) were chosen to cover (1) the neocortex and callus (neocortex/callus ROI); (2) the intramedullary defect (intramedullary ROI); and (3) a whole-bone section (3 mm in height) in line with the bone defect (3-mm whole-bone section) (Fig. 3). To avoid errors contributed by the original cortical bone in the intramedullary ROI, the region was kept dynamic in terms of where the bottom 2-mm diameter circle was placed. Thus, all analyses were based on the same total volume, but the position varied to only include the defect.
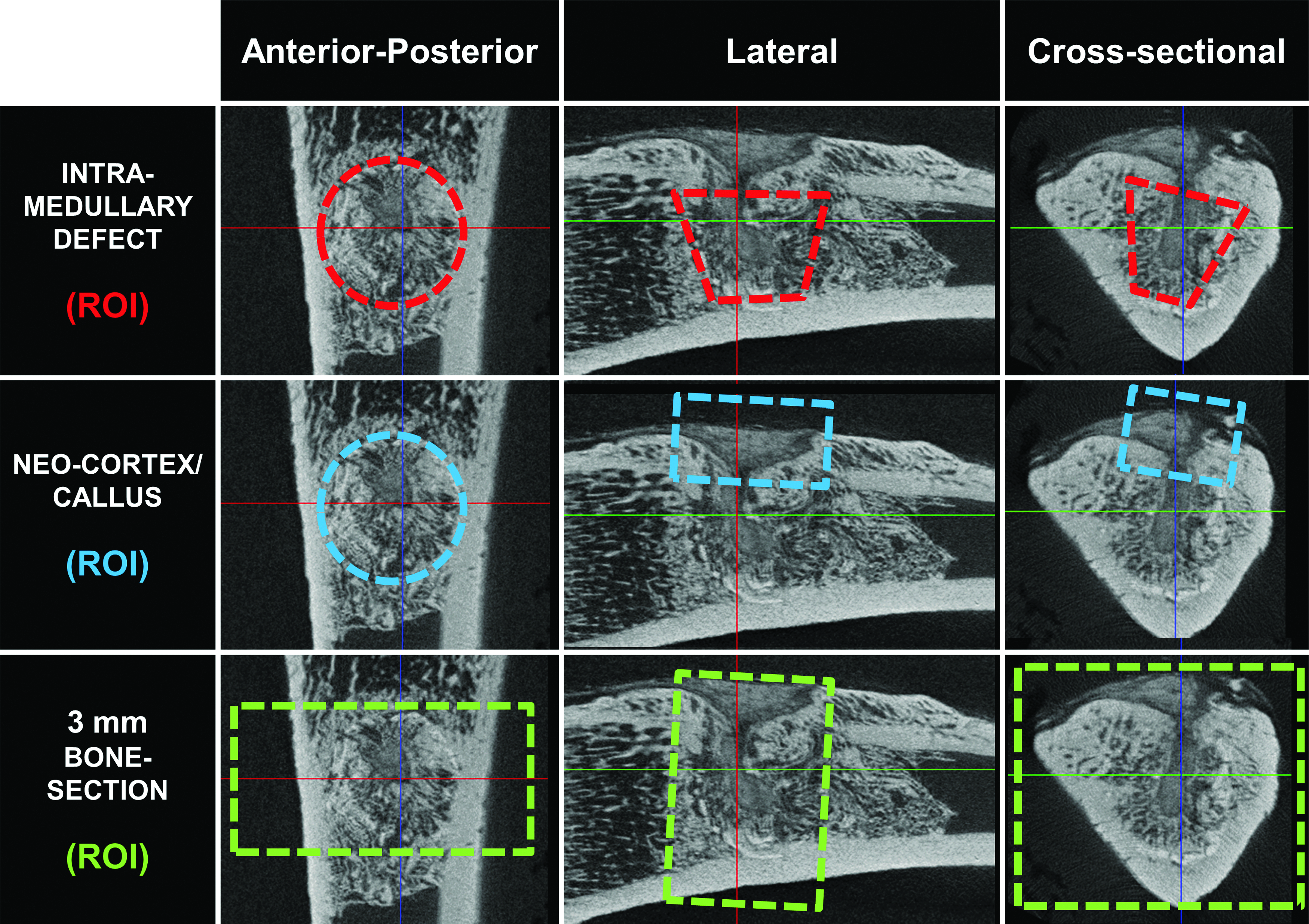
Three ROIs for the micro-CT analysis. Top row: The intramedullary defect region (flexible diameter): a 1.5-mm-deep region with the shape of a conical frustum, starting at the central border of the original cortex (3 mm diameter), continuing inward to cover the deep area along the axis of the original bone defect, and ending just before the opposite cortex (2 mm diameter). Middle row: The neocortex and callus region: a 3-mm-wide cylindrical region, beginning at the central border of the original cortex and continuing outward to cover the superficial area along the axis of the original bone defect. Bottom row: The 3-mm whole-bone section: this bone section is oriented perpendicular to the longitudinal axis of the bone, along the axis of the defect, and includes all bone in and around the original defect. ROIs, regions of interest.
Mineralized tissue volume (MV) inside the three ROIs was quantified by calculating the number of pixels with a grayscale value above a chosen threshold. The threshold was determined by visual inspection. It was called mineralized tissue volume instead of traditional bone volume since it included mineralized bone tissue as well as remnants of the allograft or GBM.
The mineralized tissue volume/total tissue volume (MV/TV) of the intramedullary ROI, as well as MV in the neocortex/callus ROI and 3-mm whole-bone section, were calculated and compared between groups. The 8-week scans were used to evaluate cortical healing. The size of the cortical defect was defined as the largest diameter at the narrowest point of the defect and classified as small (<1 mm) or large (>1 mm). In case of a bridging cortex, it was classified as bridged.
Histology
Histology specimens were fixed in formalin for 24 h, followed by ethylenediaminetetraacetic acid (EDTA) decalcification for 2 weeks, with regular changes of EDTA solutions every 2 days. The samples were processed and embedded in paraffin using standard histological procedures. Five-micrometer sections were cut with a microtome (HM355S, Thermo Fischer Scientific, MA) and stained using hematoxylin and eosin stain (Thermo Fischer Scientific).
Statistical analysis
Statistical analysis was performed using SPSS statistics (Version 22.0; IBM Corporation, NY). Data are presented as mean with 95% confidence interval (95% CI), and graphically as mean with the standard error of the mean (SEM). One-way ANOVA was used to analyze differences between groups, and in case of unequal variances, the Welch's test was performed, and the Games–Howell post hoc test was used to compare differences between groups. A p-value below 5% was considered statistically significant.
Results
Intramedullary defect healing
Micro-CT
At 4 weeks, the degree of intramedullary defect filling was markedly higher in the GBM-treated group compared with the Empty and Allograft groups; however, these differences reduced substantially from 4 to 8 weeks (Table 1 and Fig. 4). The addition of ZA led to a tendency toward an increased degree of defect filling at 8 weeks compared with GBM alone (mean difference: 17.1% [95% CI: −6.3–40.5%, p = 0.220]). Further addition of BMP-2 led to the lowest degree of defect filling among the GBM-treated groups at 4 weeks, but conversely the highest degree at 8 weeks. At 8 weeks, this difference was higher compared with the GBM group (mean difference: 28.2% [95% CI: 5.6–50.8%, p = 0.011]), but not if compared with the GBM + ZA group.
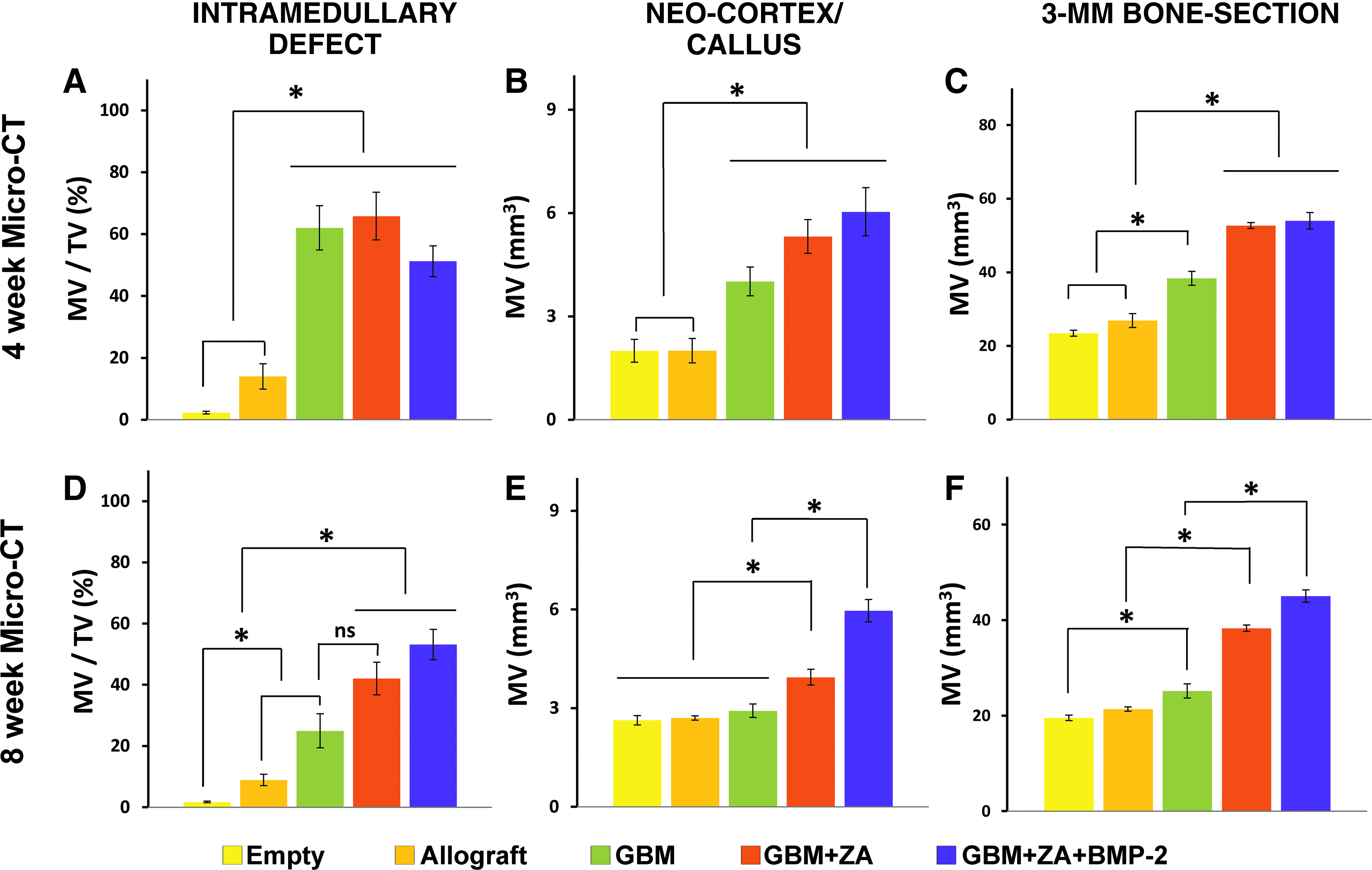
Quantitative micro-CT results in the three regions: intramedullary defect (MV/TV), neocortex and callus (MV), and 3-mm whole-bone section (MV). The upper row
All data are presented as mean and with 95% confidence interval. Welch's test (on the right) determines equality of means between groups (p < 0.05 indicates unequal means).
BMP-2, bone morphogenic protein-2; CI, confidence interval; GBM, sulfate/hydroxyapatite biomaterial; MV/TV, mineralized tissue volume/total tissue volume; ROIs, regions of interest; ZA, zoledronic acid.
Qualitative histology
Specimens belonging to the Empty group appeared to be empty in the middle, while specimens from the Allograft group were filled with marrow-like tissue. In the group treated with GBM alone, the defects were filled with a matrix of fibrous tissue, parts with viable newly formed bone, and parts with remnants of GBM. The addition of ZA appeared to increase the ratio and thickness of the newly formed trabecular bone within the bone marrow canal, while the addition of BMP-2 further increased trabecular bone thickness (Fig. 5).
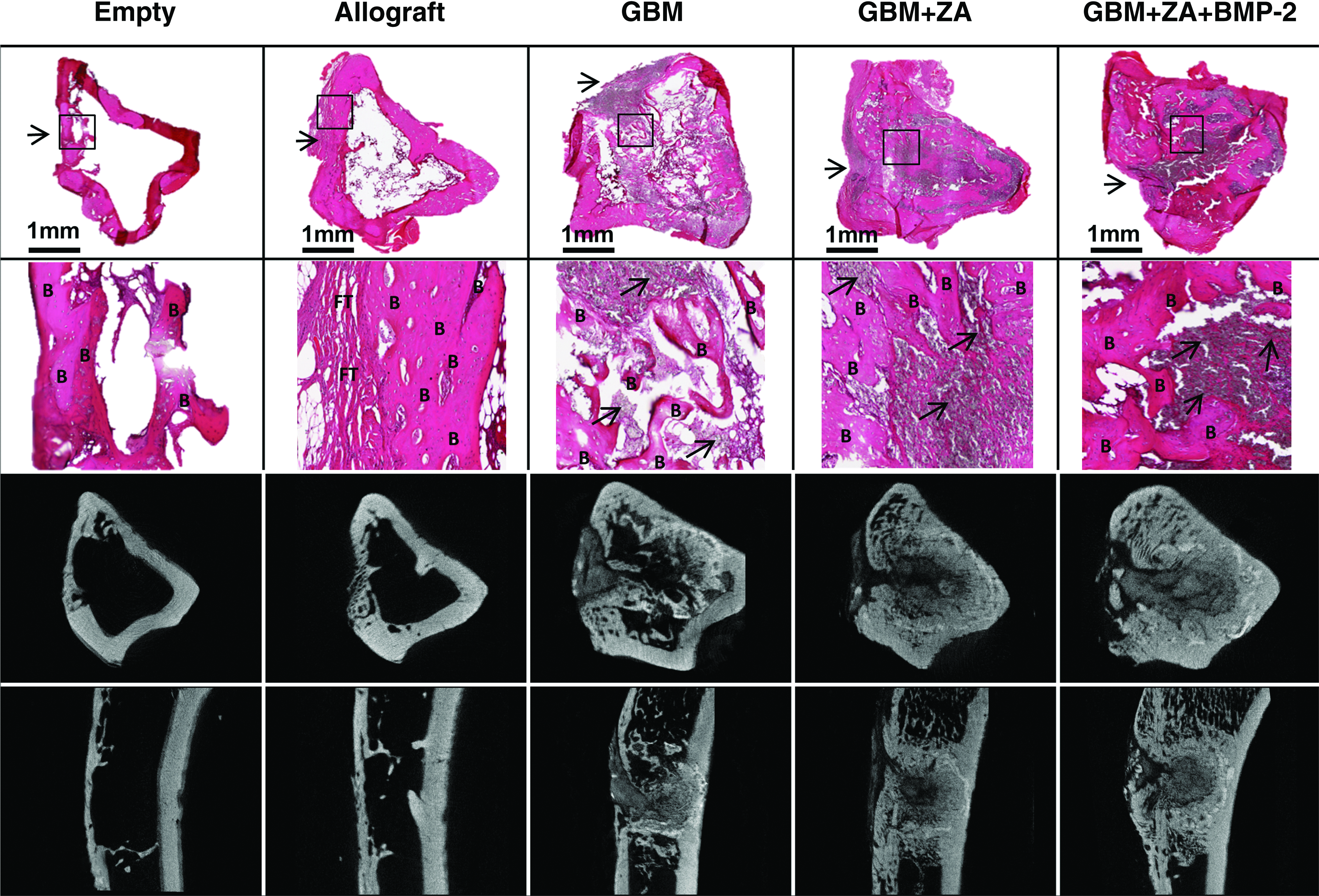
Qualitative histology from representative specimens. Top panels show H&E-stained slices from the defect regions in each group (20× magnification). The arrows indicate the defected cortex, and the box indicates the selected area for further magnification. The scale bar represents 1 mm. Middle panels show higher magnified (200 × ) areas from each group. B indicates new bone formation, arrows point to residual GBM, and FT indicates fibrous tissue. Bottom rows show matched CT slides from each group. Compared with histology, the high-density mineral/tissue within the defect not only represents remnants of the material entirely but also appears to be new bone tissue.
Cortical defect healing
Micro-CT
At 4 weeks, the mineralized tissue volume (MV) of the neocortex/callus ROI was markedly higher in the GBM group compared with the Empty and Allograft groups; however, no differences were seen at 8 weeks (Table 1 and Fig. 4). Addition of ZA led to an increased MV at 8 weeks compared with GBM alone (mean difference: 1.0 mm3 [95% CI: 0.1–2.0 mm3, p = 0.033]). Addition of BMP-2 led to a further increase in MV at 8 weeks compared with GBM + ZA (mean difference: 2.0 mm3 [95% CI: 0.8–3.3 mm3, p = 0.001]).
Cortical bridging
All cortices bridged with a thin new cortex in the Empty and Allograft groups. In the GBM and GBM + ZA + BMP-2 groups, 2 of 10 had bridging cortices, whereas all cortices healed with a varying sized cortical defect in the GBM + ZA group (Fig. 6).

Micro-CT scanning slides from each group (left: axial view, right: lateral view). Below is the evaluation of cortical healing.
Qualitative histology
On the defect side, the neocortex is thin, but apparently normal, in the non-GBM-treated groups. In the groups treated with GBM, a small gap is seen in the neocortex. The gap is filled with a matrix of fibrous tissue and remnants of GBM, which extrudes into the callus region. Addition of ZA appears to increase both newly formed and existing cortical bone thickness, while addition of BMP-2 even further increases the callus size. (Fig. 5)
The 3-mm whole-bone section
Micro-CT
The MV was higher in the GBM group compared with the Empty and Allograft groups at 4 and 8 weeks (Table 1 and Fig. 4). Addition of ZA led to an increased MV compared with the GBM group at 4 and 8 weeks (mean difference at 8 weeks: 13.1 mm3 [95% CI: 7.9–18.3 mm3, p < 0.001]). Addition of BMP-2 further increased MV at 8 weeks compared with the GBM + ZA group (mean difference: 6.7 mm3 [95% CI: 2.1–11.3 mm3, p = 0.003])
Discussion
We evaluated the ability of a composite calcium GBM to deliver BMP-2 and ZA in a metaphyseal tibial defect in rats by measuring changes in mineralized tissue volume (MV) using micro-CT. We speculated that the present composite biomaterial could be used as an efficient carrier for BMP-2 and ZA to regenerate bone, thereby possibly avoiding the drawbacks of systemic ZA and high-dose BMP treatments. Addition of ZA to the GBM increased MV in the neocortex/callus region and the 3-mm whole-bone section, and addition of BMP-2 further increased MV in both regions. Qualitative histology supported micro-CT findings and showed the presence of newly formed trabecular bone in all GBM-treated groups.
Ceramic biomaterials were originally developed as alternatives to bone grafting and several studies have documented clinical outcomes using composite hydroxyapatite/calcium sulfate biomaterials.26–28 However, for treatment of more challenging bone defects, addition of bone-active substances or proteins seems to be needed. In this study, we chose to add the substances ZA and BMP-2.
Effective local delivery of a bisphosphonate using a calcium phosphate-based biomaterial has recently been described, but we wished to test if it was possible for an already commercially available product.20,29 We expected ZA to increase the overall bone volume by protecting existing and newly formed bone from osteoclast resorption. The findings of significantly increased MVs in two of three micro-CT regions in the GBM + ZA groups, compared with the GBM group, strongly indicate that the GBM acted as a carrier for ZA in our study.29–33 ZA has been shown to preserve callus formation in fracture models, which could explain why we found the strongest influence of ZA in the neocortex/callus region.30–32 Delayed resorption of GBM is another explanation for the ZA-induced increases in MV as locally and systemic administered ZA is known to preserve bone grafts in bone chamber models in rats.34–36 However, inside the intramedullary defect, we found no statistical difference between the GBM and GBM + ZA groups, where a difference would be expected if more of the GBM was preserved in the GBM + ZA group. This indicates the existence of an actual ZA-induced increased bone volume surrounding the intramedullary defect, which is supported by increased cortical thickness on the qualitative histology slides. Although debated, increased cortical thickness could prove beneficial to avoid a postoperative fracture after treatment of bone defects. Some animal studies have found an association between callus volume and bone strength, whereas other studies found unchanged strength despite larger callus volume, possibly due to incomplete fracture healing.30–33
The ZA-induced effects seen in our study were achieved by adding 10 μg of ZA. Previous studies have indicated 0.1 mg/kg as the optimal dose of systemic ZA to protect new bone from premature resorption.32,33,37,38 A local dose reduction by 2.5 times has been shown to produce equivalent results compared with systemic treatment using a different bisphosphonate, and compared with the optimal systemic dose of ZA, we have reduced the dose by 3.3 times by using local treatment. 39 This could be favorable to avoid possible side effects associated with systemic ZA treatment. However, there are described side effects to local administration as well. High local concentration of ZA is known to be cytotoxic to different cell types and interfere with osteoblast proliferation, leading to impaired bone formation.30,36,40 We have recently demonstrated in vitro that ZA added to the GBM is not released in cytotoxic doses to A549 cells due to a high affinity of ZA to HA particles inside the material, which is advantageous compared with non-HA-containing biomaterials. 24 Although delivered locally, systemic effects of ZA can probably not be completely avoided, as found in previous studies.30,31
Delivery of BMPs using calcium phosphate-based materials has also been described; however, similar studies on combined delivery of ZA and BMP are limited.41–43 BMPs have been combined with ZA using other carriers, resulting in increased callus size and bone strength, compared with single BMP or ZA treatment.33,37,38 This is in line with our findings, where a combination of BMP and ZA led to an even higher mineralized tissue volume in the neocortex/callus region and the 3-mm whole-bone section, which indicates that BMP was delivered locally using the GBM. Many options for BMP delivery have been described; however, the only clinically available solution used currently for the delivery of BMP-2 is a Food Drug Administration-approved collagen sponge (Medtronic INFUSE) as an alternate approach to bone grafting. 44 There has been a growing body of research indicating the drawbacks associated with its use, which is suspected to be the result of supraphysiological doses delivered.11,45 A segmental bone defect study in rats found dose-dependent effects of BMP-2 leading to tissue inflammation and cyst-like bone voids with poorer bone quality at local doses above 11.25 μg. 46 This dose is many times lower (in terms of body weight) than administered clinically, where BMP-2 doses range from 4000 to 12,000 μg per kit. 11 This indicates that clinically relevant measures to reduce dosage are preferable. Compared with one of the first human studies describing the use of BMP-2 on a resorbable collagen sponge in a lumbar fusion study, we were able to reduce the amount by 3.3–7.6 times (in terms of body weight), and nearly five times compared with a study performed in nonhuman primates, while still achieving an effect on bone remodeling in our defect model.47,48
The model used in our study was not critical in regard to cortical healing since all cortices bridged in the control groups. Surprisingly, small cortical defects were seen in the GBM-treated groups (Fig. 6). Similar findings were described by Jungbluth et al. in 2010 where a calcium phosphate cement (CPC) was compared with autograft in a unicortical defect of the proximal tibia in minipigs. They found delayed cortical healing in the CPC group, with no cortices bridged, compared with 5/8 in the autograft group. 49 We speculate that the GBM leaked toward the healing cortices (also seen in micro-CT and histology slices), thereby delaying the cortical bridging. In contrast to cortical healing, however, trabecular bone regeneration inside the intramedullary defect was only achieved in GBM-treated groups, whereas the Empty and Allograft groups appeared empty.
We acknowledge that the present study has a number of limitations. First, micro-CT analysis is unable to distinguish between viable bone, unremodeled bone allograft, and the composite biomaterial. The mineralized tissue volume can therefore not be directly translated into viable bone volume, which makes comparison difficult between groups treated with or without a graft material. However, differences in mineralized tissue volume caused by addition of bone-active substances can be analyzed between groups treated with the GBM as equal amounts of the composite biomaterial were used. A treatment group with GBM and BMP-2 would have helped us to fully understand the individual and combined effects of BMP-2 and ZA. Second, the age and skeletal maturity of the rats could have had an effect on potential bone remodeling. The rats used in this study were not fully skeletally matured and might have had a superior healing potential compared with adult rats. To make our defect critical, the diameter of the cortical defect should probably have been at least 4 mm, which was impossible due to the small bone diameter of the 6-week-old rat tibiae. 50 As we intended to investigate the properties of GBM to regenerate not only cortical but also trabecular bone in the bone marrow canal, we chose younger rats with a higher differentiation ability of bone marrow-derived mesenchymal stem cells compared with older rats. 51
Conclusion
In conclusion, the gentamicin-containing composite biomaterial (GBM) used in this study was able to carry the anabolic and anticatabolic agents: BMP-2 and ZA. The addition of ZA to GBM leads to an increased mineralized tissue volume of the neocortex and callus, and codelivery of BMP-2 and ZA leads to an even larger callus formation.
Footnotes
Disclosure Statement
L.L. is a board member of Bonesupport AB, Lund, Sweden. An institutional research grant from Bonesupport AB was used to fund part of the PhD work of P.H. None of the other coauthors have any financial conflicts of interest related to this study.