
Abstract
Background:
Fascia-wrapped diced cartilage grafts have become a useful tool in modern rhinoplasty surgery. Unfortunately, fascial harvest is associated with donor site morbidity; therefore, a nonautologous alternative to fascia would be ideal. Decellularized porcine mesothelium (PM), Meso BioMatrix™, is an acellular scaffold that could potentially fill this need. To determine if PM could serve as an acceptable alternative, we histologically compared diced cartilage grafts wrapped in fascia versus PM.
Methods:
Human rib cartilage and temporoparietal fascia were obtained under an IRB-approved protocol. Cartilage was diced into 0.5 mm pieces and implanted in subcutaneous pockets in nude rats. Implanted materials included cartilage alone, cartilage wrapped in fascia, cartilage wrapped in PM, fascia alone, or PM alone. Specimens were harvested at 8 weeks and stained with hematoxylin and eosin, Masson's trichrome, Safranin-O, and Verhoeff's stain to assess cartilage viability, architecture, and regenerative potential.
Results:
Unwrapped diced cartilage showed the highest cartilage viability, but was associated with loss of contour and dispersion of the cartilage pieces. Meso BioMatrix-wrapped grafts maintained contour and cartilage pieces had not dispersed; however, there was a significantly lower number of nucleated lacunae and a greater amount of basophilia than both fascia-wrapped cartilage and unwrapped cartilage. There was no significant difference in cartilage resorption between fascia-wrapped cartilage and Meso BioMatrix-wrapped cartilage or in the proteoglycan or collagen content between all groups.
Conclusion:
Off-the-shelf decellularized PM was associated with lower cartilage viability than unprocessed fascial allograft. No cartilage piece dispersion, fibrosis, resorption, or a foreign body reaction to Meso BioMatrix was observed. PM, although not equivalent to autologous tissue, may be utilized to achieve acceptable clinical results and be a viable alternative that limits donor side morbidity. This experimental study supports further clinical investigation of this material in rhinoplasty procedures.
Introduction
R
The first cartilage grafts were used in the late 1800s. 5 The advantages of a cartilage graft include minimal resorption as well as the ability of the graft to take without revascularization.6,7 Unfortunately, although cartilage can be easily molded at the time of implantation, the graft will often deform or return to its original shape. 8 This problem was first noted in 1920 by Gillies and continues to be a problem in rhinoplasty today. 1 In fact, in a recent systematic review of the complications associated with autologous costal cartilage grafting in rhinoplasty, the most common complication was warping of the graft, which occurred in 5.2% of 1259 patients. 9 In addition, traditional autogenous solid cartilage grafts for rhinoplasty are also associated with other complications, including donor site morbidity, graft fracture, infection, extrusion, malalignment, resorption, and the presence of a visible contour.9,10 There have been several attempts at modifying cartilage grafts to maintain their shape long term, such as carving or crushing the cartilage. 8 However, the implanted crushed or diced cartilage is often visible through the nasal skin. 11 This motivated Dr. Onur Erol to develop the Turkish Delight technique, in which diced cartilage is wrapped in a Surgicel envelope.
Dr. Erol first presented his experience with this technique in 1989 and has since used it in over 9000 patients. He has reported satisfactory results without warping or the diced cartilage being visible through the nasal skin, which is referred to by Erol as late show of the graft. 12 Daniel and Calvert used Erol's technique in a series of 22 patients, but found that the Surgicel-wrapped grafts underwent clinical failure and were associated with resorption, fibrosis, and lymphocytic infiltration on histologic analysis. 13 Daniel and Calvert's negative experience with Surgicel was substantiated with experimental evidence. 5 Therefore, they pioneered the use of deep temporalis fascia, instead of Surgicel, to wrap the diced cartilage. Esthetically pleasing results were achieved with minimal graft resorption. 13 Unfortunately, although fascia has been shown to be superior to alloplastic materials regarding cartilage viability, harvesting the fascia has several disadvantages, such as donor site morbidity and a limited amount of available fascia. As such, various nonautologous materials, other than Surgicel, have been considered potential alternatives for wrapping the diced cartilage. For example, Kim et al. used acellular dermal matrix (AlloDerm; LifeCell Corporation) in a rabbit model and achieved favorable results. 14 To date, however, no one has studied the viability of cartilage wrapped in decellularized porcine mesothelium (PM).
Decellularized PM, or Meso BioMatrix™ (DSM Biomedical, Exton, PA), is intended for implantation to reinforce soft tissues where weakness exists in patients requiring soft tissue repair and/or reinforcement in plastic and reconstructive surgery, including, but not limited to, the following procedures: reinforcement of primary closure such as suture line reinforcement and muscle flap reinforcement. Decellularized mesothelium has been shown to have favorable strength and retain a number of growth factors, making this material a reasonable option for surgical applications, in particular, those where tissue regeneration is desired. 15 We sought to determine if this material would be suitable for use in Turkish Delight Rhinoplasty. The objective of this study was to assess cartilage viability using Meso BioMatrix compared to fascia-wrapped diced cartilage grafts. To achieve these goals, we implanted Meso BioMatrix alone (M), fascia alone (F), diced cartilage alone (DC), diced cartilage wrapped in fascia (DC+F), or diced cartilage wrapped in Meso BioMatrix (DC+M) in the rat dorsal subcutaneous pocket model. We found that cartilage viability was highest in the diced cartilage-alone group, followed by the diced cartilage wrapped in fascia group, and then the diced cartilage wrapped in Meso BioMatrix group. However, cartilage in Meso BioMatrix was not found to be resorbed and no evidence of fibrosis was present on histology. It may be a suitable alternative in patients where the donor site morbidity of fascial harvest is not acceptable.
Material and Methods
Study design
Five groups each with five animals were used. Each group was subject to implantation with a different material (Table 1).
Human tissue harvest
Temporoparietal fascia (TPF) and rib cartilage were collected as excess tissue was available from young healthy individuals undergoing rhinoplasty. Tissue was collected with written consent. The study was approved by the University of Southern California Institutional Review Board. All harvesting of human tissue was performed by the same surgeon (J.W.C.). Costal cartilage was harvested through a lower chest incision. For the TPF, an ∼2 cm linear incision was made 1 cm above and 0.5 to 1 cm posterior to the root of the helix of the ear to get at least 4 cm in diameter fascia, which is large enough to use for the nasal dorsum. At least six different human subjects were required for enough human tissue to complete the study. Due to the limited amount of TPF, complete stratification of human tissue from a single donor was not possible. Therefore, different human donors were used and the harvested tissue was evenly distributed between the groups. It should be noted that the host immune response to the graft was not a concern since nude athymic rats were used, which are immune deficient.
Implanted material
Rib cartilage was diced with a scalpel in 0.5 mm pieces and implants were prepared as previously described. 13 Either PM or human fascia was used to wrap the diced cartilage; the wrapping was secured with 6-0 fast gut suture (Fig. 1). An equivalent amount of diced cartilage was used to create the implants and each implant was placed in a subcutaneous pocket in the dorsum of a rat.
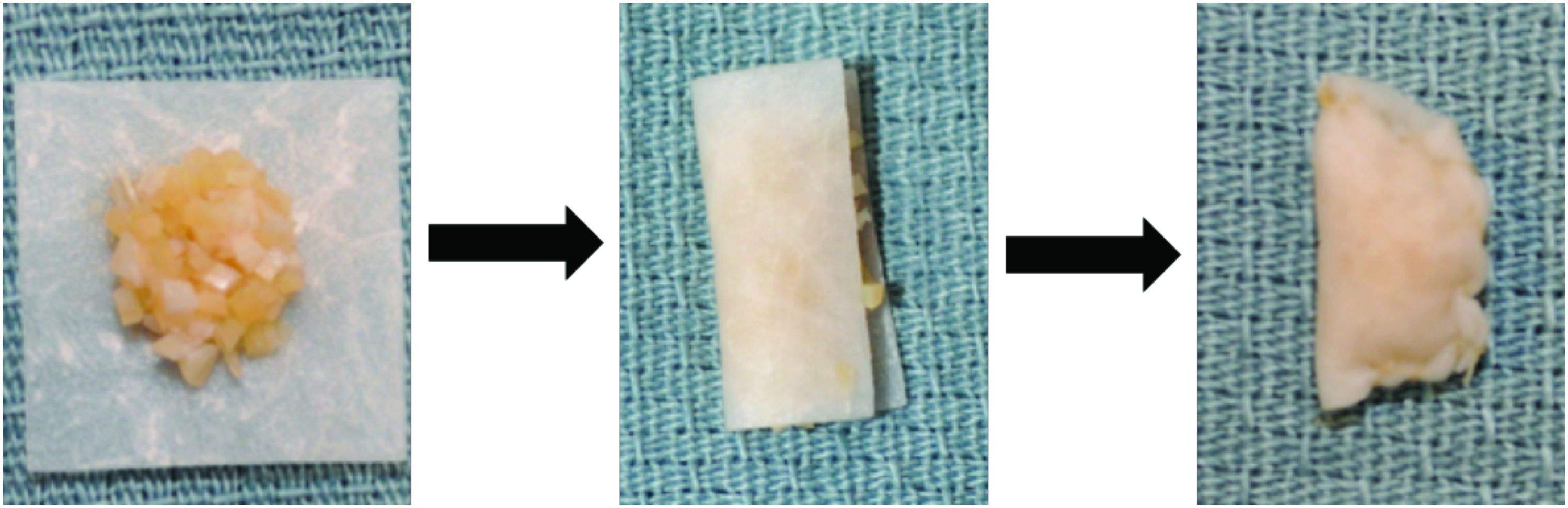
Representative images depicting how diced cartilage was placed into the Meso BioMatrix envelope and then fastened with suture. Color images available online at www.liebertpub.com/tea
Animals
All animal procedures were approved by the Institutional Animal Care and Use Committee at the University of Southern California and in accordance to the Guide for the Care and Use of Laboratory Animals (National Research Council, 8th ed., 2011). Athymic Rowett nude rats between 4 and 6 weeks old were used. All animals were housed in pairs and given access to a normal chow diet and water ad libitum. Five animals were used per group and each rat received only one graft type. No animals suffered complications during the procedure or postoperative course.
Implantation
Creation and implantation of the grafts were performed within hours of obtaining the donor tissue. All rats were anesthetized with 3% isoflurane and prepped and draped in a sterile manner. Two subcutaneous pockets were created 2 cm posterior to the ears in the dorsum of each rat. Two pockets were used to increase the number of biologic replicates. Subsequently, Meso BioMatrix alone (M), fascia alone (F), diced cartilage alone (DC), diced cartilage wrapped in fascia (DC+F), or diced cartilage wrapped in Meso BioMatrix (DC+M) was implanted into the subcutaneous pockets (Fig. 2). The incision was closed with two interrupted 4-0 nylon sutures (Ethicon, Inc.).
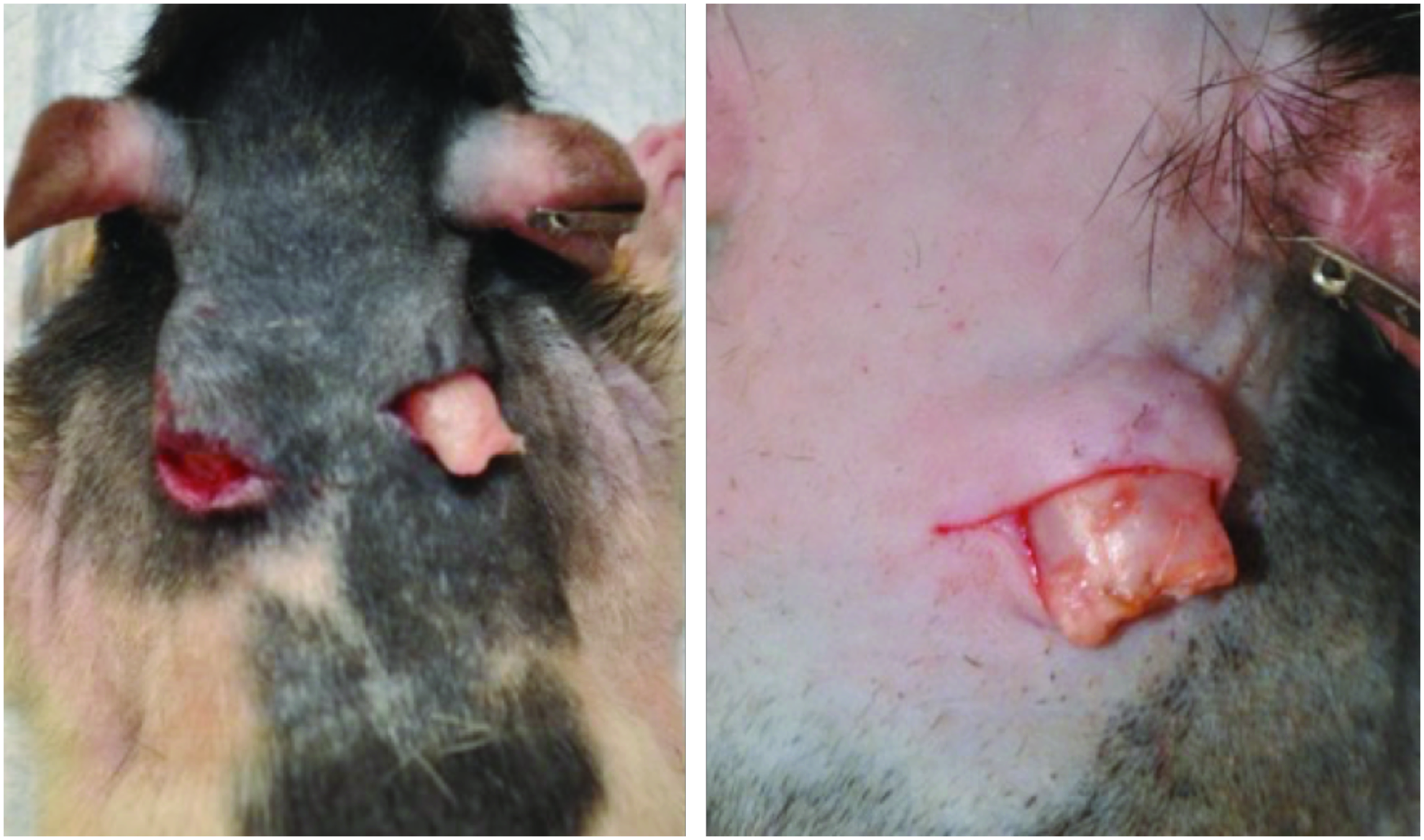
Representative images showing the location of dorsal subcutaneous pockets, in which the grafts were placed. Color images available online at www.liebertpub.com/tea
Graft harvest, fixation, staining, and analysis
At postoperative week 8, the subcutaneous pockets were opened and the implant was removed. As per our clinical experience, composite grafts are typically incorporated into the adjacent tissue by 8 weeks; therefore, this time was chosen for harvest. The gross appearance of each implant was photographed and compared. Specimens were fixed in 4% PFA, sectioned, and stained with hematoxylin and eosin (H&E), Masson's trichrome, Safranin-O, or Verhoeff-Van Gieson stain. In the H&E stain, cell viability was determined by counting the absolute number of nucleated lacunae by blinded observers. Viable chondrocytes maintain nucleated lacunae. The degree of basophilia (purple color) around the lacunae as well the presence of dystrophic calcifications and the integrity of the cartilage pieces were also qualitatively assessed. Masson's trichrome stains collagen content blue. Safranin-O stains with red color the proteoglycan content of the cartilage and it is an indicator of the matrix productivity of the viable chondrocytes. Verhoeff-Van Gieson stains black the elastic fibers.
Visual analogue score
A visual analogue Score was used to grade the degree of color staining of each specimen by a pathologist and blinded observers. For each specimen, at least three random 10 × high-power fields (hpf) were chosen. In each hpf, a score was assigned from 0 through 3 based on the percentage of area stained, as previously described, where grade 0, less than 25% of hpf is stained, grade 1, 25–49% of hpf is stained, grade 2, 50–75% of hpf is stained, and grade 3, more than 75% of hpf is stained.14,16,17
Statistical analysis
Statistical analysis was performed with GraphPad Prism 6.00 (GraphPad Software, Inc., San Diego, CA). The three groups were compared with a one-way analysis of variance for continuous variables with a normal distribution and with the Kruskal–Wallis test for continuous variables without normal distributions. The visual analog scores as ordinal variables between two groups were analyzed with the Mann–Whitney U test. A p-value less than 0.05 was considered statistically significant. Bonferroni adjustment was performed for multiple comparisons.
Results
Gross analysis
Upon harvest, the grafts were collected with minimal surgical dissection. Both fascia and Meso BioMatrix alone by the time of explantation at 8 weeks were intact with a fine capillary network observed on their surface. The unwrapped diced cartilage implants showed an obvious loss of contour and dispersion of cartilage pieces. The cartilage that had not dispersed had fused into a mass with irregular surface contour. The diced cartilage wrapped in Meso BioMatrix and the diced cartilage wrapped in fascia maintained their shape with no resorption grossly evident (Fig. 3). Both specimens had a capsule formed from the wrapping material, which was intact with a smooth contour. The underlying cartilage pieces were fused into a cohesive mass. No suture material was evident.
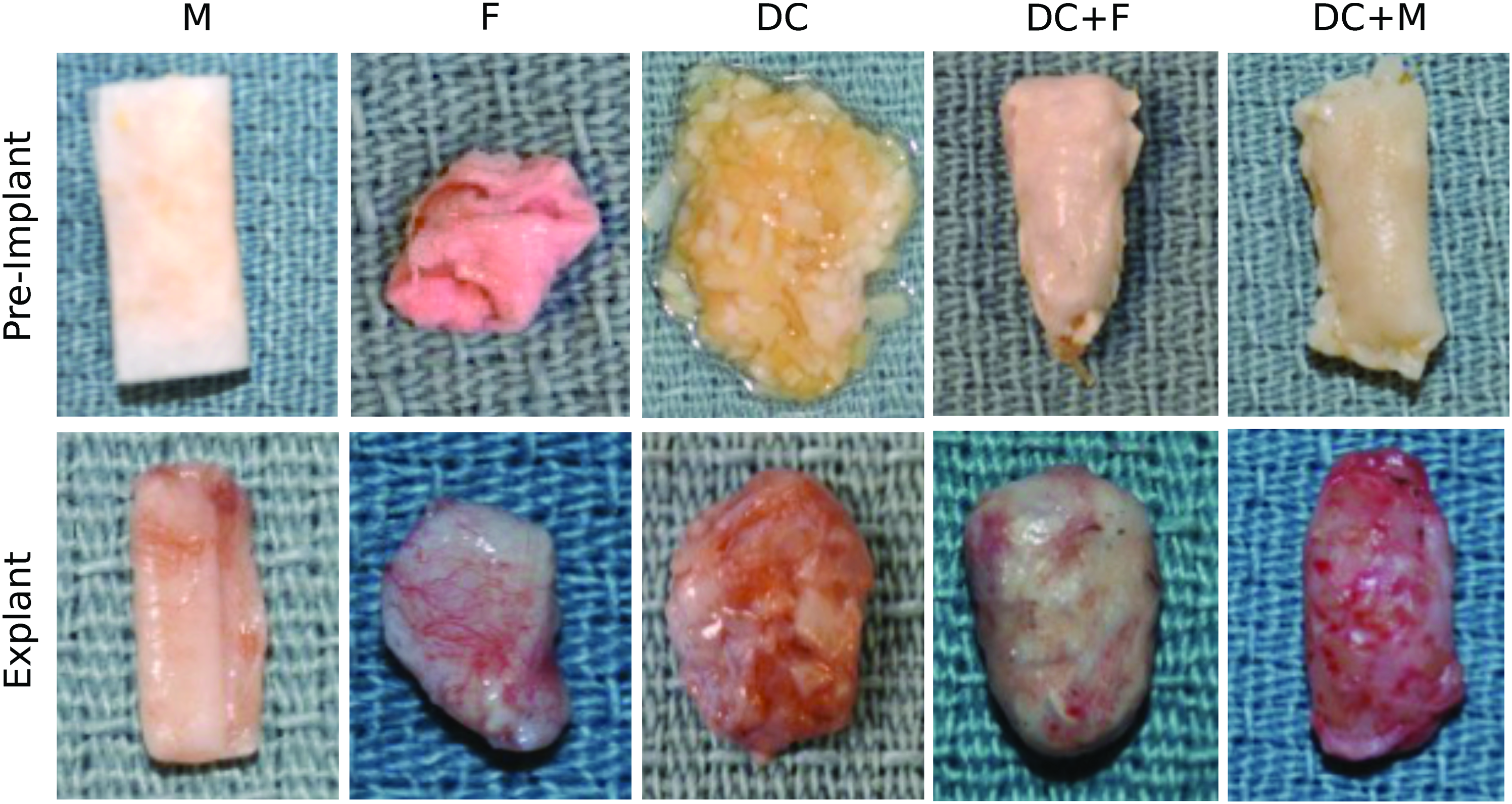
Representative images of the various graft materials before implantation and upon explant. M, Meso BioMatrix; F, Fascia; DC, diced cartilage; DC+FD, diced cartilage wrapped in fascia; DC+M, diced cartilage wrapped in Meso BioMatrix. Color images available online at www.liebertpub.com/tea
Histologic analysis
A summary of the quantitative histological assessment and statistical analysis is presented in Table 2.
Mean ± SEM; * significance is p < 0.05.
DC, diced cartilage; DC+F, diced cartilage wrapped in fascia; DC+M, diced cartilage wrapped in matrix; SEM, standard error of the mean.
Hematoxylin and eosin
In cartilage tissue, H&E stains nuclear chromatin and lacunar glycosaminoglycans. This was used to assess cartilage viability, chondrocyte injury, and resorption. Viable chondrocytes will maintain nucleated lacunae. Resorption and chondrocyte injury are marked by dystrophic calcification. We found that the unwrapped diced cartilage grafts maintained the highest cartilage viability. The number of nucleated lacunae in the unwrapped diced cartilage implant was significantly higher than in the diced cartilage wrapped in fascia, which had a significantly higher number of nucleated lacunae than the diced cartilage wrapped in Meso BioMatrix. Similarly, there was significantly less basophilia in the unwrapped diced cartilage and fascia-wrapped diced cartilage compared to the diced cartilage wrapped in Meso BioMatrix. The diced cartilage wrapped in fascia showed the least amount of basophilia (Fig. 4). The unwrapped diced cartilage group showed significantly less cartilage resorption than both the diced cartilage wrapped in fascia and diced cartilage wrapped in Meso BioMatrix. There was no significant difference in resorption between the cartilage wrapped in fascia versus Meso BioMatrix (Fig. 4).
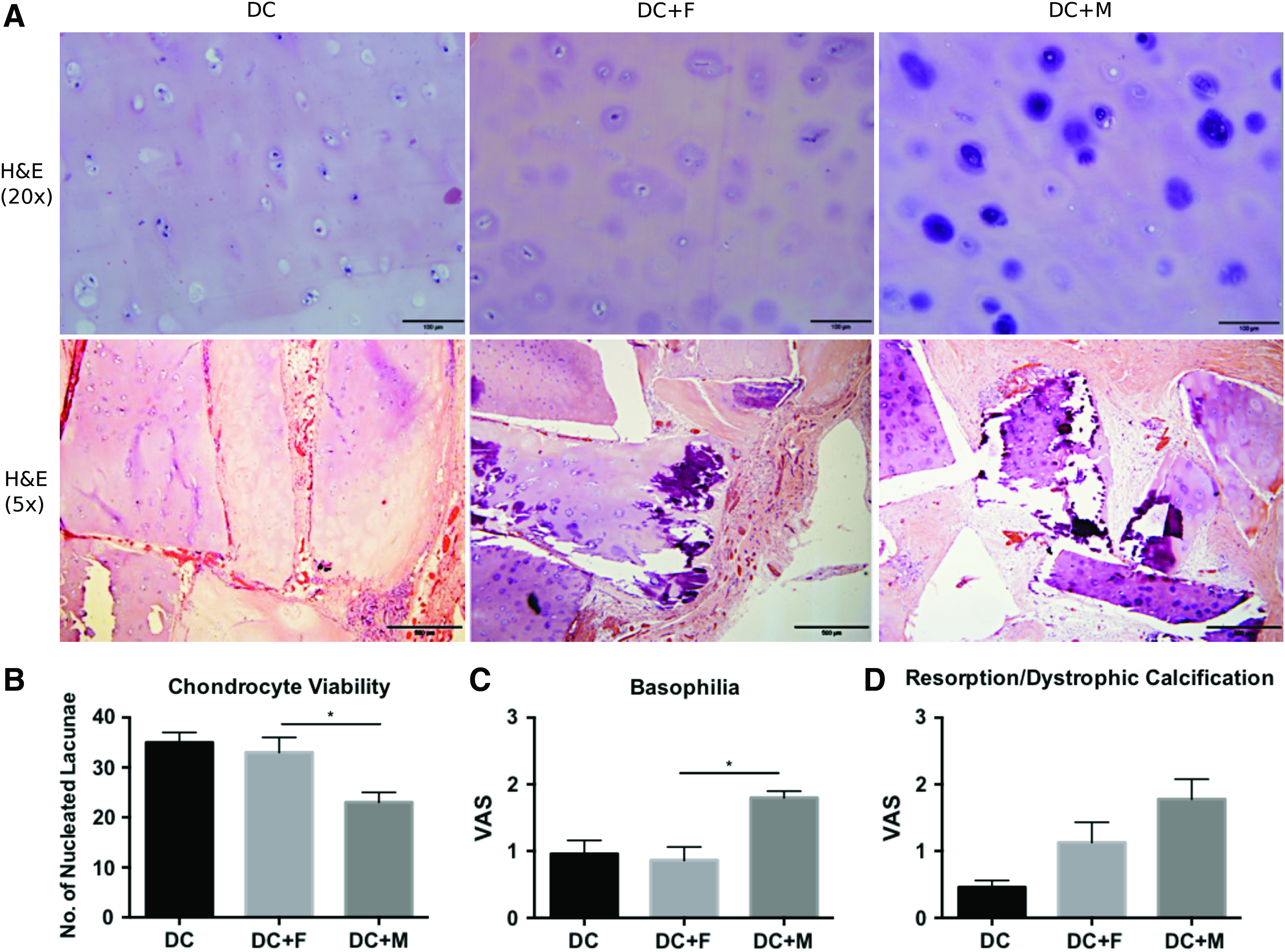
H&E staining and visual assessment of diced cartilage (DC), diced cartilage wrapped in fascia (DC+F), and diced cartilage wrapped in Meso BioMatrix (DC+M).
Masson's Trichrome
Masson's Trichrome stain was used to assay for collagen content to compare between groups. There was no significant difference in collagen content between any of the groups; however, the diced cartilage wrapped in Meso BioMatrix tended to have the least amount of collagen (Fig. 5). The fascia implanted alone tended to have a greater amount of collagen than the Meso BioMatrix implanted alone (Fig. 6).
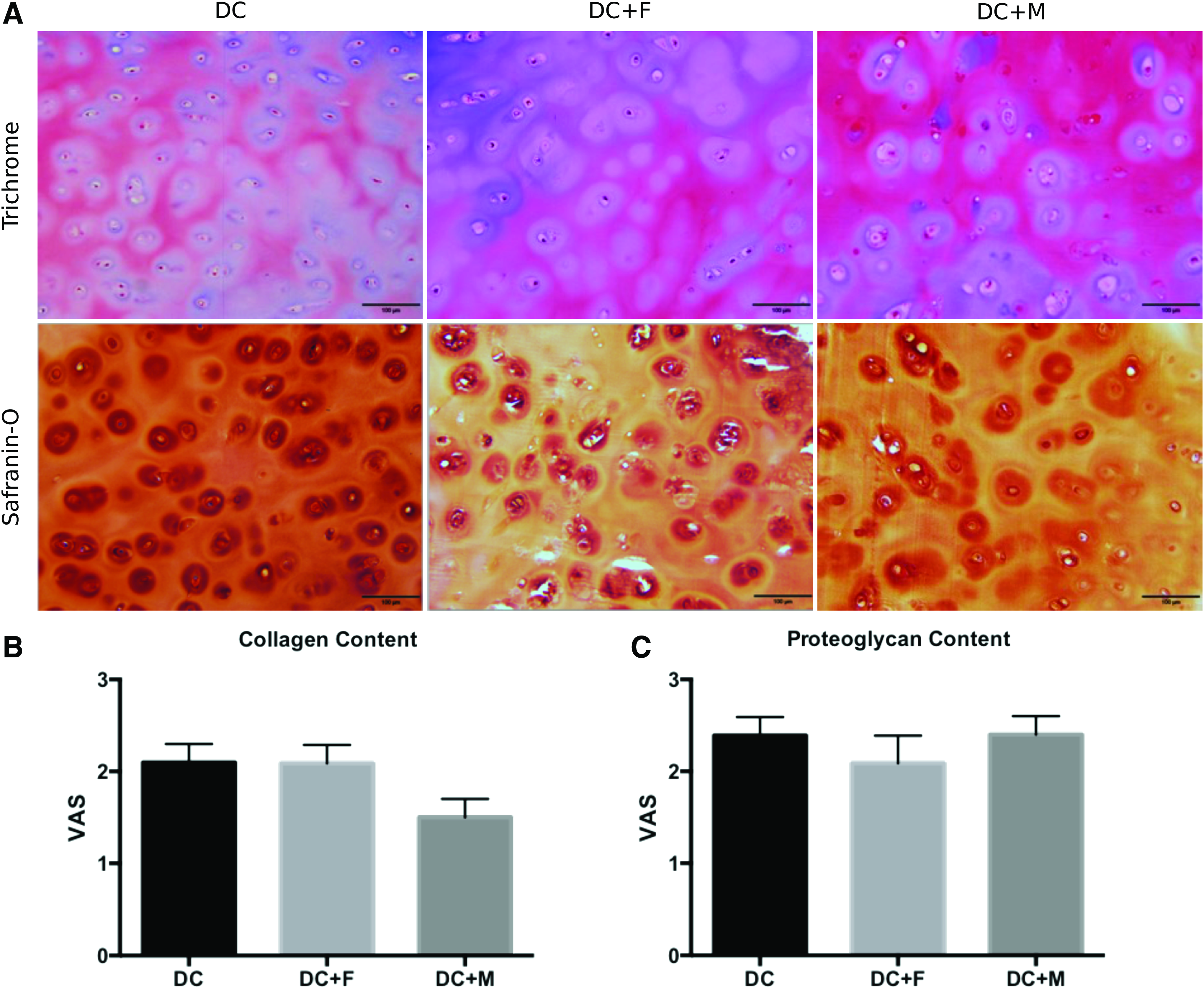
Masson's trichrome and Safranin-O staining, and visual assessment of diced cartilage (DC), diced cartilage wrapped in fascia (DC+F), and diced cartilage wrapped in Meso BioMatrix (DC+M).
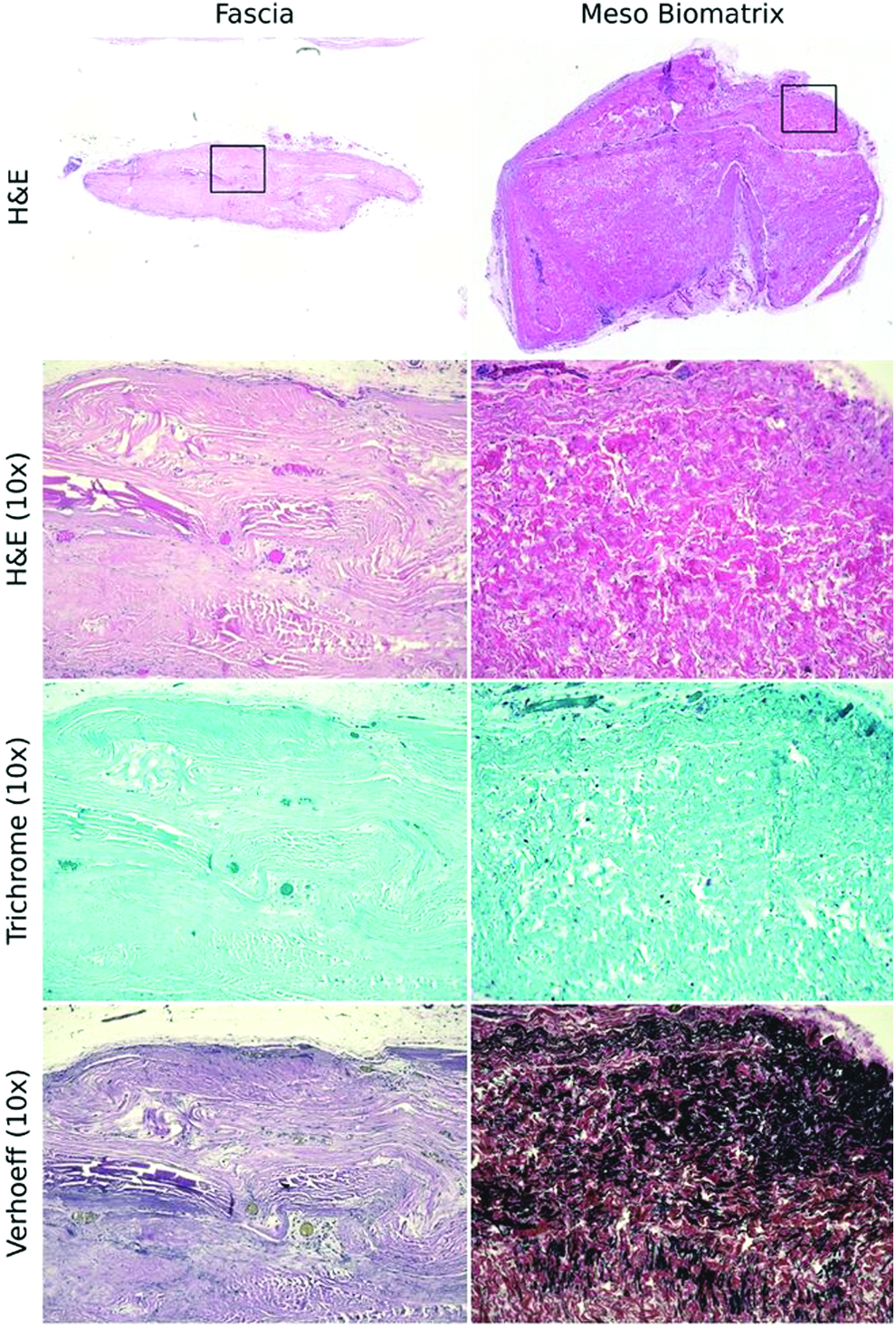
H&E-, Trichrome-, and Verhoeff-stained specimens of fascia and Meso BioMatrix that had been implanted without cartilage. The solid boxes indicate the high power images (10 × ) taken. Color images available online at www.liebertpub.com/tea
Safranin-O
Safranin-O stains proteoglycan. In cartilage tissue, proteoglycan content is a measure of chondrocyte viability since living chondrocytes maintain the proteoglycan content of their matrix. There was no difference in proteoglycan content between groups (Fig. 5).
Verhoeff's stain
Verhoeff's stain is specific for elastic fibers, which are a natural component of cartilage tissue. This was used to compare elastin content between groups. Elastic fiber content was qualitatively greater in the diced cartilage wrapped in Meso BioMatrix group than in the other groups (Fig. 7). Similarly, the Meso BioMatrix that was implanted alone tended to have substantially more elastic fiber content than the fascia implanted alone (Fig. 6).
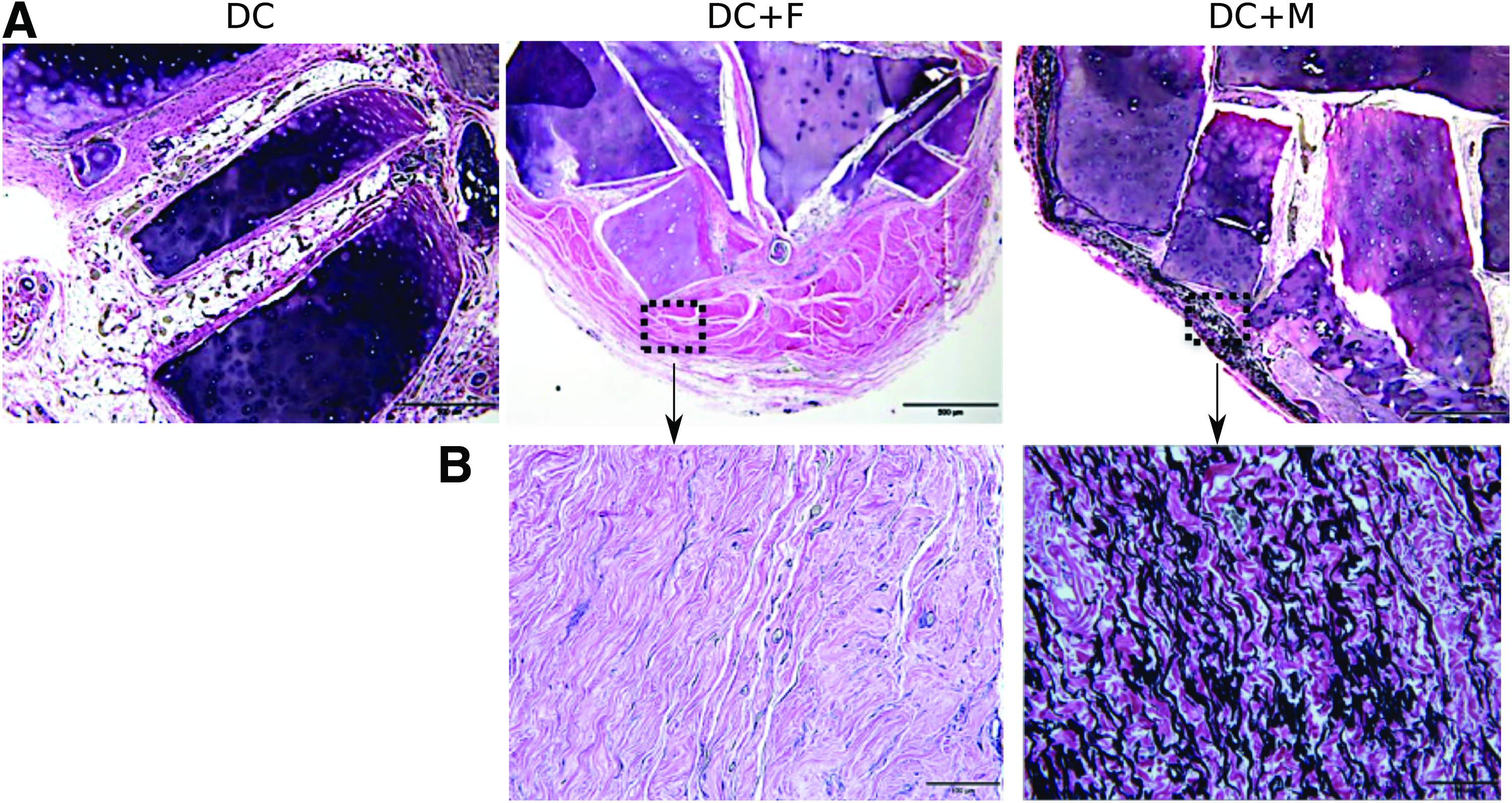
Verhoeff's stain of elastic content in specimens of diced cartilage (DC), diced cartilage wrapped in fascia (DC+F), and diced cartilage wrapped in Meso BioMatrix (DC+M).
Discussion
Since the introduction of Turkish Delight Rhinoplasty by Dr. Erol, a range of both autologous and nonautologous materials has been used as a wrapping for diced cartilage grafts in augmentation rhinoplasty. Examples of autologous tissues that have been used to wrap diced cartilage grafts include fascia, perichondrium, tensor fascia lata, and amniotic membrane. Nonautologous materials include Surgicel, AlloDerm, Esterified Hyaluronic Acid, and now, Meso BioMatrix.
Fascia
To date, autologous fascia has been shown to be one of the most effective materials in terms of graft resorption and cartilage viability. The use of deep temporalis fascia for this application was initially pioneered by Daniel and Calvert. 13 They attempted to reproduce Dr. Erol's Turkish Delight technique in which cartilage is diced, wrapped in a Surgicel envelope, and then implanted; however, they were unable to reproduce his clinical results. This prompted the use of deep temporalis fascia as a wrapping for diced cartilage. In their hands, they found that fascia was superior to Surgicel, in that cartilage viability was maintained and there was no resorption, fibrosis, or lymphocytic infiltrate.10,13,18 Fascia may have several properties that make it advantageous for this application. It has been suggested that the fascia may serve as a neoperichondrium since an intact perichondrium is associated with greater cartilage viability and less absorption.10,19 It is also known that fascial grafts can act as a scaffold for host tissue incorporation, in addition to having properties that promote cell proliferation.20,21 The benefits of using autologous fascia as a wrapping for diced cartilage grafts have been supported by both clinical and experimental data. Positive clinical outcomes have been reported by As'adi et al., 22 Kelly et al., 23 Guerrerosantos et al., 24 Calvert et al., 10 and Daniel and Calvert. 13 Positive experimental outcomes have been reported by Brenner et al. 16 and Coskun et al. 25 Autologous fascia is well established as a highly useful material for wrapping of diced cartilage grafts. Donor site complications, such as wound infection or alopecia, remain a concern, as a 2–3 cm temporal scalp incision is needed for deep temporalis fascia harvest.
Perichondrium
Perichondrium has also been used to wrap diced cartilage grafts. Perichondrium is a native structure involved in cartilage viability and repair. When left in place on cartilage grafts, perichondrium improves cartilage viability compared to cartilage where the perichondrium has been stripped. 26 Kemaloglu and Tekin have shown, in a rabbit model, that cartilage grafts wrapped in perichondrium can actually result in higher chondrocyte viability than fascia-wrapped grafts. 19 However, clinically, there is limited amount of perichondrium that can be harvested from the coastal area and additional donor areas are needed.
Tensor fascia lata
Some have wrapped diced cartilage grafts in tensor fascia lata to create a graft with greater structural support. Experimentally, in a rabbit model, tensor fascia lata-wrapped grafts were shown to have decreased graft weight and less new cartilage formation upon explant, compared to diced cartilage alone. 27 However, it should be noted that in this study, tensor fascia lata was not compared to other wrapping types. In contrast, Kim and Kim have applied tensor fascia lata-wrapped diced cartilage grafts clinically with positive results. 28 This technique provides a semirigid graft and is, hence, advantageous for use in severe nasal defects where bone grafting is typically favored. 28
Amniotic membrane
Amniotic membrane has been used in ophthalmologic disorders, in abdominal surgery to prevent adhesions, and as a biologic dressing for cutaneous wounds such as chronic ulcers and burn injuries. 29 Amniotic membrane has recently been considered for use in wrapping diced cartilage grafts since it is easily available and would avoid the donor site morbidity associated with fascial harvest. It has been suggested that amniotic membrane may pose a nonsignificant barrier to diffusion of nutrients to the enveloped diced cartilage graft, since the membrane is 0.3 mm thick. 30 Studies done in animal models have shown that diced cartilage graft viability is maintained and no fibrosis, necrosis, calcification, or inflammatory reaction is observed. 30 Atespare et al. found that diced cartilage grafts wrapped in amniotic membrane showed greater cartilage viability than diced cartilage alone. 31 Although these experimental results are positive, as per our review of the literature, amniotic membrane has yet to be used in rhinoplasty clinically.
Surgicel
Surgicel is composed of oxidized methylcellulose and has traditionally been used as a hemostatic agent. Dr. Erol was the first to use Surgicel to wrap finely diced cartilage grafts for rhinoplasty, a technique he termed Turkish Delight Rhinoplasty. Dr. Erol has since used his technique with impressive results in over 9000 patients. 12 A large amount of clinical data have been published reporting esthetically satisfactory results with Surgicel-wrapped diced cartilage grafts. Dr. Erol has published multiple case series with over 9000 patient in total.11,12,32 Elahi et al. reviewed 67 cases in which this technique was applied and concluded that there were pleasing results with an acceptable complication rate. 33 Finally, Velidedeoglu et al. used Surgicel in 23 patients with positive results. 34 In contrast, there are data that suggest that Surgicel undergoes absorption and prompts a foreign body response resulting in fibrosis, lymphocytic infiltration of the graft, and decreased cartilage viability.5,10,13,25,35–37 In summary, there remains some uncertainty over whether Surgicel or fascia is superior as a wrapping material for diced cartilage grafts. It has been proposed that the contrasting results are secondary to the use of these grafts for different end goals in rhinoplasty. 13
AlloDerm
AlloDerm is acellular human cadaveric dermis that has been aseptically processed. Its components include collagen type IV and VII, laminin, elastin, and residual dermal matrix. 14 Acellular dermal matrices (ADM) were first used as a dermal replacement in the treatment of full-thickness burns. 38 In augmentation rhinoplasty, the use of AlloDerm is not a new concept.39–43 It was not until recently, however, that AlloDerm was used to wrap diced cartilage grafts in rhinoplasty. Specifically, Kim et al. used thin AlloDerm (9 to 13/1000 inches thick) meshed 1:1 to wrap diced cartilage grafts in an animal model and found it to be superior to fascia regarding chondrocyte regeneration potential, matrix collagen content, and metaplastic bone formation. 14 Gordon et al., who termed this technique the “American Delight,” has used AlloDerm for this purpose in 83 patients. Of these patients, 75% found the results satisfactory, 5% were undecided, and 15% found the results unsatisfactory. Complications were limited to one case of cutaneous erythema that resolved with antibiotics, one case of undercorrection corrected with hyaluronic acid filler injection, and one case of 1 mm lateral graft displacement. 44 AlloDerm appears to be a suitable option for wrapping diced cartilage grafts in nasal augmentation.
Esterified hyaluronic acid
Hyaluronic acid is an endogenous polysaccharide common to synovial fluid and the extracellular matrix. 45 As such, hyaluronic acid has been a longtime interest to those studying and treating osteoarthritis. As reviewed by Altman et al., the beneficial effect of hyaluronic acid on articular cartilage acts through numerous mechanisms, some of which may be disease modifying for osteoarthritis. 46 The chondroprotective effects of hyaluronic acid make it a logical consideration for wrapping diced cartilage grafts in nasal reconstruction. Kazikdas et al. used a rabbit model to compare diced cartilage wrapped in hyaluronic acid to diced cartilage wrapped in Surgicel. They found that hyaluronic acid-enveloped diced cartilage grafts showed vascularization, chondrocyte proliferation, minimal fibrosis, and minimal inflammation. 37 As noted by the authors, these results are promising and warrant further experimental and clinical evaluation.
Porcine mesothelium
To date, this is the first study assessing the utility of PM, or Meso BioMatrix, for wrapping diced cartilage grafts to be used in nasal augmentation. Meso BioMatrix is a thin acellular scaffold derived from PM. It been approved by the FDA for reinforcement and repair of soft tissue. Decellularized mesothelium retains a number of growth factors, which theoretically make this material advantageous for surgical applications where tissue regeneration is desired. 15 In vitro, it has been shown that Meso BioMatrix supports cell infiltration and promotes migration and chemotaxis signaling more effectively than other decellularized extracellular matrix-derived scaffolds, such as Veritas (Baxter, Deerfield, IL), OASIS Wound Matrix (Cook Biotech, Lafayette, IN), AlloDerm, and Surgisis (Cook Biotech). 47 Given these biologic properties, we thought Meso BioMatrix could be an effective material for use in wrapping diced cartilage grafts. In addition, from a technical standpoint, PM has greater elastin content compared to other commercially available decellularized extracellular matrix-derived scaffolds; therefore, in our hands, it is more pliable during the construction of diced cartilage grafts.
In our experimental study, cartilage absorption by visual analogue score is not significantly different between the temporoparietal and Meso BioMatrix groups. When one strictly examines cartilage viability in terms of basophilia and preservation of lacunar nuclei count, we found that Meso BioMatrix-wrapped diced cartilage is less optimal when compared to both diced cartilage alone and diced cartilage wrapped in fascia. In fact, this was not unexpected. Cartilage is inherently avascular and therefore depends on imbibition of surrounding nutrients. 48 Logically, it follows that a barrier to diffusion between cartilage and the surrounding nutrient supply would increase the risk of cartilage necrosis. As it has been suggested by Yilmaz et al. regarding Surgicel, a Meso BioMatrix wrapping may impose a relative hypoxia on the cartilage and decrease the regeneration potential. 5 Our results are consistent with this concept since diced cartilage without a wrapping was the most viable and fascia was the next best alternative to no wrapping. While the exact mechanism that underlies why fascia is more optimal than Meso BioMatrix remains to be elucidated, we suspect that the latter requires additional time to become recellularized, whereas fascial allograft does not require this step. Other possible mechanisms leading to decreased cartilage viability, such as evidence of a foreign body reaction to the Meso BioMatrix, were not observed.
Although statistically significant, we believe that the observed difference in chondrocyte viability is not clinically relevant. Preliminary follow-up data from human patients who had Meso BioMatrix rhinoplasty (data not shown; observations from J.W.C.) suggest that nasal reconstruction revision rates are not significantly different from comparable patients with autologous fascia and nasal contour is maintained. Obviously, these clinical observations will need to be substantiated by a formal retrospective review (in process) or a randomized clinical trial.
Although not equivalent to autologous fascia, Meso BioMatrix might be a good option in cases where the donor does not want additional surgical incisions to harvest fascia from his or her own body. A high preauricular incision in the temporal area is necessary to harvest fascia graft. While all incisions carry the risk of possible dehiscence or surgical site infection, this access incision is also associated with alopecia. From a technical point of view, because Meso BioMatrix is thinner and has a higher elastic content than other comparable allogenic materials, it offers enhanced plasticity and conformability that make the construction of the wraps easier.
Of note, this study has some inherent limitations. We used athymic Rowlett nude rats that are immunocompromised and may underestimate the host's response toward the implanted materials. The immunocompetent response toward angiogenesis and the xenogenic material is mediated by macrophages and theoretically should not affect Rowlett athymic rats in which severe defects only in T cell-mediated immunity exist. 49 The degree of absorption and viability of the cartilage in the early period depends more on the supply of adequate nutrients. This, in turn, depends on the diffusion gradient created between the chondrocytes and the neocapillaries. The speed and degree of vascularization of the new implanted material play a far more important role for the survival of the diced cartilage rather than the immune response. The latter is important for the degradation of the wrapping material that usually occurs through several months mediated by macrophages. 50 By then, the cartilage pieces in their new conformation have been stabilized and are well vascularized.
Last, it would be interesting to study if a meshed or more porous Meso BioMatrix would be more efficacious than the tested Meso BioMatrix. Theoretically, this could improve imbibition through the scaffold. For example, when placed under a skin graft, acellular dermal matrix with pores 500–800 μm in diameter has been shown to improve imbibition and increase the rate of skin graft take compared to nonporous ADM. 51 By maximizing imbibition through the PM to the diced cartilage, cartilage viability may be improved.
Conclusion
While Meso BioMatrix-wrapped diced cartilage constructs display less chondrocyte viability than autologous fascia-wrapped grafts, cartilage resorption, which represents the clinical endpoint, was not different between these two experimental groups. As such, Meso BioMatrix may be a viable alternative to autologous graft material, especially since it minimizes donor site morbidity. Nevertheless, further clinical correlation is warranted before Meso BioMatrix is widely used as an alternative to autologous fascia in Turkish Delight rhinoplasty.
Footnotes
Acknowledgments
We appreciate guidance from Lillian Young regarding preparation of specimens for histology.
Disclosure Statement
The study was funded through an investigator-initiated research grant from DSM, who provided the matrix at no cost. The authors declare no other conflicts of interest relevant to this study.