
Abstract
Objective:
The objective of this study was to compare the impact of different in vivo incubation sites on the production of tissue-engineered small intestine (TESI).
Materials and Methods:
Green fluorescent protein transgenic rat pups (3–5 days) were used as donors of intestinal organoids. Harvested intestine was exposed to enzymatic digestion to release intestinal stem cell-containing organoids. Organoids were purified, concentrated, and seeded onto tubular polyglycolic acid scaffolds. Seeded scaffolds were implanted in each of five locations in recipient female nude rats: wrapped with omentum, wrapped with intestinal mesentery, wrapped with uterine horn membrane, attached to the abdominal wall, and inserted into the subcutaneous space. After 4 weeks of in vivo incubation, specimens from each site were explanted for evaluation.
Results:
Wrapping seeded scaffolds with vascularized membranes produced TESI with variable lengths of vascularized pedicles, with the longest pedicle length from uterine horn membrane, the shortest pedicle length from intestinal mesentery, and intermediate length from omentum. The quantity of TESI, as expressed by volume and neomucosal length, was identical in TESI produced by wrapping with any of the three membranes. The smallest quantity of TESI was found in TESI produced from insertion into the subcutaneous space, with an intermediate quantity of TESI produced from attachment to the abdominal wall. Periodic acid-Schiff and immunofluorescence (IF) staining confirmed the presence of all intestinal epithelial cell lineages in TESI produced at all incubation sites. Additional IF staining demonstrated the presence of enteric nervous system components and blood vessels. Wrapping of seeded scaffolds with vascularized membranes significantly increased the density of blood vessels in the TESI produced.
Conclusion:
Wrapping of seeded scaffolds in vascularized membranes produced the largest quantity and highest quality of TESI. Attaching seeded scaffolds to the abdominal wall produced an intermediate quantity of TESI, but the quality was still comparable to TESI produced in vascularized membranes. Insertion of seeded scaffolds into the subcutaneous space produced the smallest quantity and lowest quality of TESI. In summary, wrapping seeded scaffolds with vascularized membranes is favorable for the production of TESI, and wrapping with omentum may produce TESI that is most easily anastomosed with host intestine.
Introduction
T
Host intestinal mesentery has been reported as an incubation site for transplanted hepatocytes on polymer constructs, and for pancreatic islet cells in polyethylene glycol maleimide hydrogels.12,13 Uterine horn membrane is only available in females and is commonly used in anti-post-operative adhesion models.14–16 It contains abundant blood vessels, making it suitable for accommodation of developing TESI. The anterior surface of the abdominal wall provides a broad surface area on which multiple cell-seeded scaffolds can be attached. Cell-seeded scaffolds implanted onto the anterior abdominal wall will be exposed to the same environment as host intestine, and will be nourished by peritoneal fluid. We have compared different cell seeding populations and scaffold materials using the anterior abdominal wall as the in vivo incubation site in our previous studies.17,18
In this study, we have performed a direct comparison of five different in vivo incubation sites for the production of TESI: three that involve vascularized membranes (omentum, intestinal mesentery, and uterine horn membrane) and two that do not (subcutaneous space and anterior abdominal wall). We hypothesized that implantation of seeded scaffolds into vascularized membranes would produce TESI of superior quality and quantity, with the vascularized membrane functioning as an intestinal mesentery for the delivery of nutrients and oxygen to the maturing TESI. In addition, this vascularized membrane can be relocated with the TESI segment for eventual anastomosis in line with native host intestine. Since the TESI with its vascularized pedicle will be used as a pedicle graft, the length of the vascularized pedicle will determine how far the TESI can be freed and relocated to the host intestine to treat short bowel syndrome. The results from this study will provide valuable additions to the standard operating procedure used for the translation of TESI to future clinical applications.
Materials and Methods
Isolation of intestinal stem cell-containing organoids
Green fluorescent protein (GFP) transgenic rats were purchased from Rat Resource & Research Center (Columbia, Missouri) and were used to breed pups as cell donors. The breeding and tissue harvesting protocol was approved by the IACUC of the Research Institute at Nationwide Children's Hospital (protocol no. AR12-00001). The isolation of small intestinal stem cell-containing organoids was conducted as we have previously described.18,19 Cell clusters in the size range of 25–70 μm are organoids containing cells from the base of the crypts with surrounding mesenchymal elements (myofibroblasts, fibroblasts, and smooth muscle cells [SMCs]), and were used for cell seeding and implantation. 20 Organoids were suspended in a cell seeding medium (DMEM/F-12 containing 10% fetal bovine serum [embryonic stem cell qualified, ThermoFisher Scientific, Grand Island, NY]) at 106 organoids/mL for seeding onto PGA scaffolds.
Preparation of PGA scaffolds and cell seeding
PGA Biofelt (2 mm thickness and 60 mg/cm3 density) was purchased from Biomedical Structures (Warwick, RI). Tubular scaffolds (0.5 cm diameter × 1.0 cm length) were prepared by wrapping PGA flat sheets around 5 mm diameter stainless steel mandrels and coated with 5 wt% poly-L-lactic acid (PLLA;Sigma-Aldrich, catalog no. P1566-5G) in chloroform. Once the solvent was completely evaporated, scaffolds were soaked in 100% ethanol for 30 min and then washed three times with phosphate-buffered saline (PBS). Scaffolds then underwent an additional 30-min coating with 0.4 mg/mL collagen type I (Advanced BioMatrix, San Diego, CA) followed by three washes with PBS. Scaffolds were lyophilized and sterilized with ethylene oxide, and then coated with heparin-binding epidermal growth factor-like growth factor (HB-EGF) as we have described previously. 19 Briefly, each scaffold was hydrated with 2 μg of HB-EGF in 100 μL of PBS and placed in sterile 50 mL conical bottom tubes with porous caps for lyophilization followed by subcritical CO2 treatment in a stainless steel vessel (Parr Instruments Co., Moline, IL) at 900 PSI for 1 h. Scaffolds were stored at −30°C before use. On the day of cell seeding, scaffolds were brought to room temperature 10 min before seeding. The well-mixed donor cell suspension was pipetted onto a vertically positioned scaffold from the top with a wide open pipette tip, which matched the internal diameter of the scaffolds. The cell-seeded scaffold was then placed into a 2 mL cryovial filled with 500 μL cell seeding medium and gently shaken on an orbital shaker at 4°C until implantation. The duration from cell seeding to implantation was ∼30 min.
Implantation and in vivo incubation of cell-seeded scaffolds
Nude rats (RNU/RNU) were purchased from Charles River (Cleveland, OH) and used as recipients at a body weight of 150–250 g. All surgical procedures were approved by the IACUC of the Research Institute at Nationwide Children's Hospital (protocol no. AR12-00001). Under general anesthesia with 2% isoflurane in oxygen, a midline laparotomy incision was made and five cell-seeded scaffolds were immobilized with 7/0 polypropylene suture at each of the following sites: wrapped with omentum, wrapped with intestinal mesentery, wrapped with uterine horn membrane, attached to the anterior surface of the left abdominal wall, and inserted into the subcutaneous space at the left groin. Incisions were closed in layers with 6/0 polydioxanone monofilament suture. A total of 12 nude rats underwent implantation surgery, which provided a total of 12 replicate samples for each in vivo incubation site. Four weeks after implantation, animals were anesthetized and the implants from each site were located.
Determination of vascularized pedicle length and TESI volume
The length of vascularized pedicles (if present) from each TESI was measured and recorded. The TESI was then excised and its volume measured using the water displacement method as follows: the plunger was removed from a 5 mL syringe and the luer tip was sealed with parafilm. The syringe was filled with 3 mL of PBS followed by the TESI. The difference in volume readings before and after addition of TESI was recorded as the TESI volume. TESI was cut into multiple pieces at 5 mm intervals and fixed in 10% neutral buffered formalin for morphological assessment.
Morphological assessment of TESI
Fixed samples were opened transversely and embedded in paraffin. Four micrometer sections were cut and stained with Periodic acid-Schiff (PAS) to determine the presence of goblet cells. Images were acquired with an Olympus DP71 camera using an Olympus SZX7 microscope at 1.25× and an Olympus BX51 microscope at 10 × . Circumferential neomucosal length, which represents the quantity of TESI produced, was measured by tracking the neomucosa along the circumference of the lumen using ImageJ software. Villus height and crypt depth, representing the quality of TESI produced, were measured from the top to the bottom of villi and crypts using ImageJ software. Sections were also subjected to immunofluorescence (IF) staining to identify intestinal epithelial cell lineages and proliferating cells using antibodies to chromogranin A to detect enteroendocrine cells, lysozyme to detect Paneth cells, villin to detect enterocytes, and ki67 to detect proliferating cells. The presence of enteric nervous system components was evaluated by IF using antibodies to GFAP to detect glial cells, TUJ1 to detect mature neurons, and GFP to detect implanted cells derived from GFP transgenic donor animals. The presence of blood vessels was confirmed with CD31 IF to detect endothelial cells and α-smooth muscle actin IF to detect SMCs. The density of blood vessels was quantified at 5 × magnification around the peripheral of the TESIs. GFP IF was used to identify and quantify the source of cells in blood vessels, in which only blood vessels from implanted cells are identified as GFP positive. All IF images were acquired with a Zeiss HBO 100 camera using a Zeiss LSM 700 confocal microscope at 40 × , in the Morphology Core at the Research Institute at Nationwide Children's Hospital. See Table 1 for the source and concentration of all primary and secondary antibodies used. See Figure 1 for a schematic summary of scaffold preparation, seeding, and implantation.
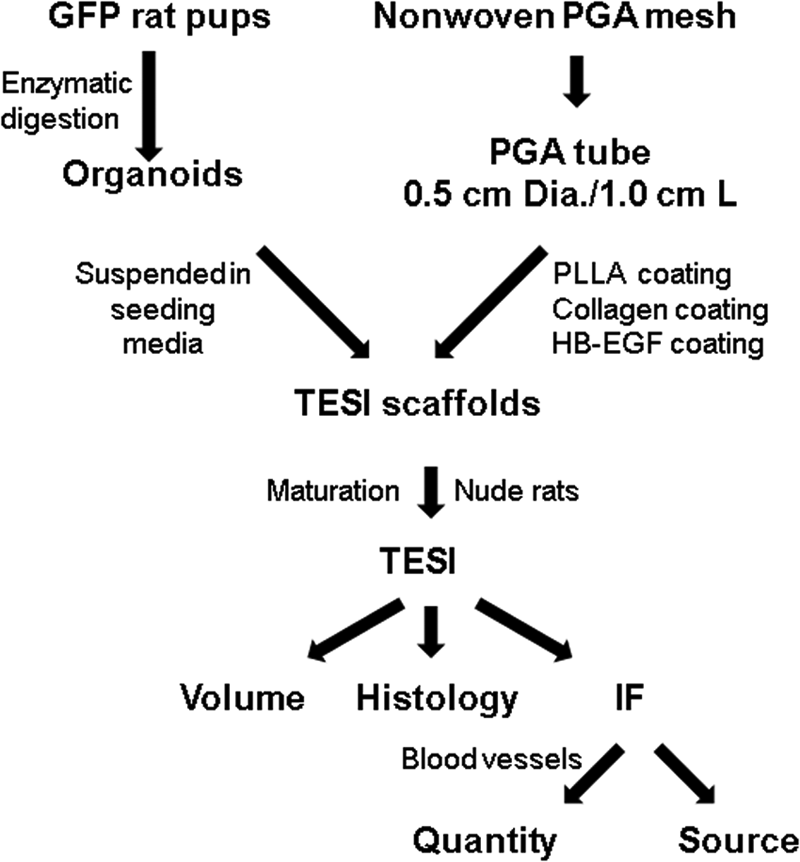
Illustration of scaffold preparation, seeding, and implantation. GFP, green fluorescent protein; IF, immunofluorescence; PGA, polyglycolic acid; PLLA, poly-L-lactic acid; TESI, tissue-engineered small intestine.
GFAP, glial fibrillary acidic protein; GFP, green fluorescent protein.
Statistical analyses
Analyses of pedicle length, volume, neomucosal length, villus height, and crypt depth were performed with GraphPad Prism 7.0 (GraphPad Software, Inc., San Diego, CA) using one-way analysis of variance (ANOVA) (Tukey's method). Analyses of blood vessel counts were conducted with GraphPad Prism 7.0 using two-way ANOVA (Tukey's method). p Values of <0.05 were considered statistically significant.
Results
TESI vascular pedicle length and volume
Five different in vivo incubation sites were chosen to accommodate and mature TESI. Three of them (omentum, intestinal mesentery, and uterine horn membrane) were vascularized membranes with different blood vessel patterns (Fig. 2A, C, F). The omentum contains blood vessels arranged in an arch similar to the intestinal mesentery, but with smaller and denser vessels, whereas the uterine horn membrane has blood vessels aligned along its longitudinal axis. The three vascularized membranes led to the formation of vascularized pedicles, but of different lengths, with uterine horn membrane leading to the longest pedicles, intestinal mesentery leading to the shortest pedicles, and omentum leading to pedicles of intermediate length (Fig. 2B, D, F, G). After the pedicles were removed, the gross view of the TESI was demonstrated and TESI volume was measured (Fig. 3). Implantation into the three vascularized membranes produced the largest volume of TESI, implantation into the subcutaneous space produced the smallest volume of TESI, and attachment to the abdominal wall produced an intermediate volume of TESI. Note that mucous was identified grossly when TESI was cross-sectioned for fixation and histological processing.
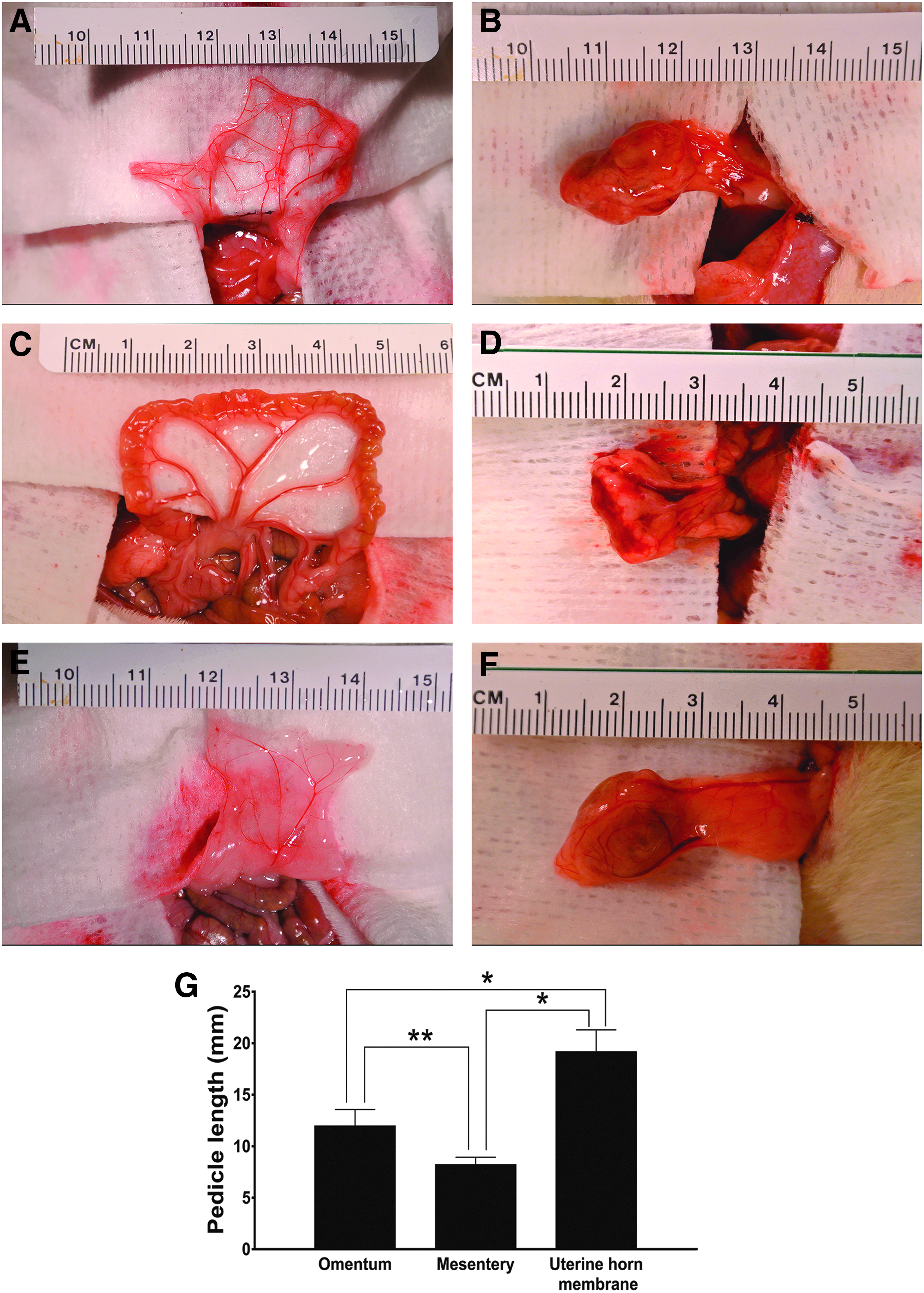
Vascularized membranes used for production of TESI. Shown are the vascularized membranes in which cell-seeded scaffolds were placed
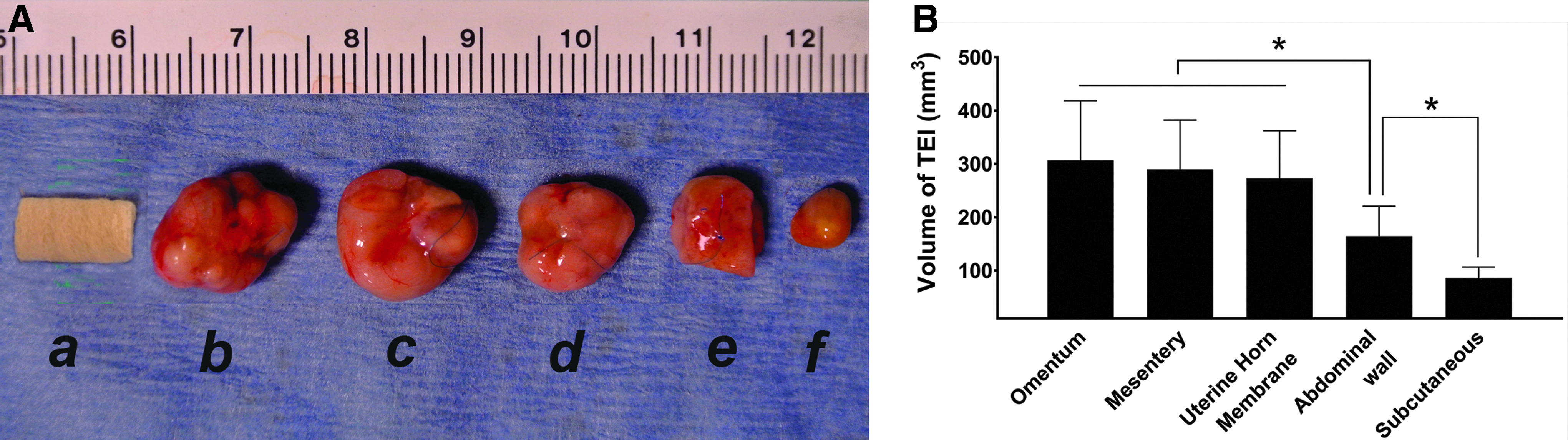
Appearance and volume of TESI produced in different implantation sites.
Neomucosal length, villus height, and crypt depth
PAS staining demonstrated the presence of mucin-positive goblet cells in TESI (Fig. 4). Low magnification (1.25 × ) images of PAS-stained TESI were used to quantify neomucosal length as illustrated in Figure 4A, and high magnification (10 × ) images were used to measure villus height and crypt depth as depicted in Figure 4F. Polarized light microscopy was used to visualize residual unabsorbed scaffold material (Fig. 4). Residual of unabsorbed scaffolds is indicated by the brighter inclusions in or adjacent to the lumen, which are mainly composed of residual unabsorbed scaffold material encapsulated by fibrous tissue. The fibrous tissue is infiltrated with foreign-body giant cells, macrophages, and lymphocytes, which are features of late stage of foreign body reaction (Fig. 5). PAS-positive acellular mucin loosely occupied the lumen of TESI and could be easily removed to confirm the patency of TESI. To prevent the collapse of the lumen after the removal of the mucin during histological processing, the mucin in the lumen was preserved in these sections. Circumferential neomucosal length, representing the quantity of TESI produced, was greatest in TESI produced in vascularized membranes, intermediate in TESI produced by attachment to the abdominal wall, and least in TESI produced in the subcutaneous space (Fig. 6A). Villus height and crypt depth, representing the quality of TESI produced, were equivalent in all implantation sites with the exception of the subcutaneous space, in which villus height was the lowest (Fig. 6B, C).
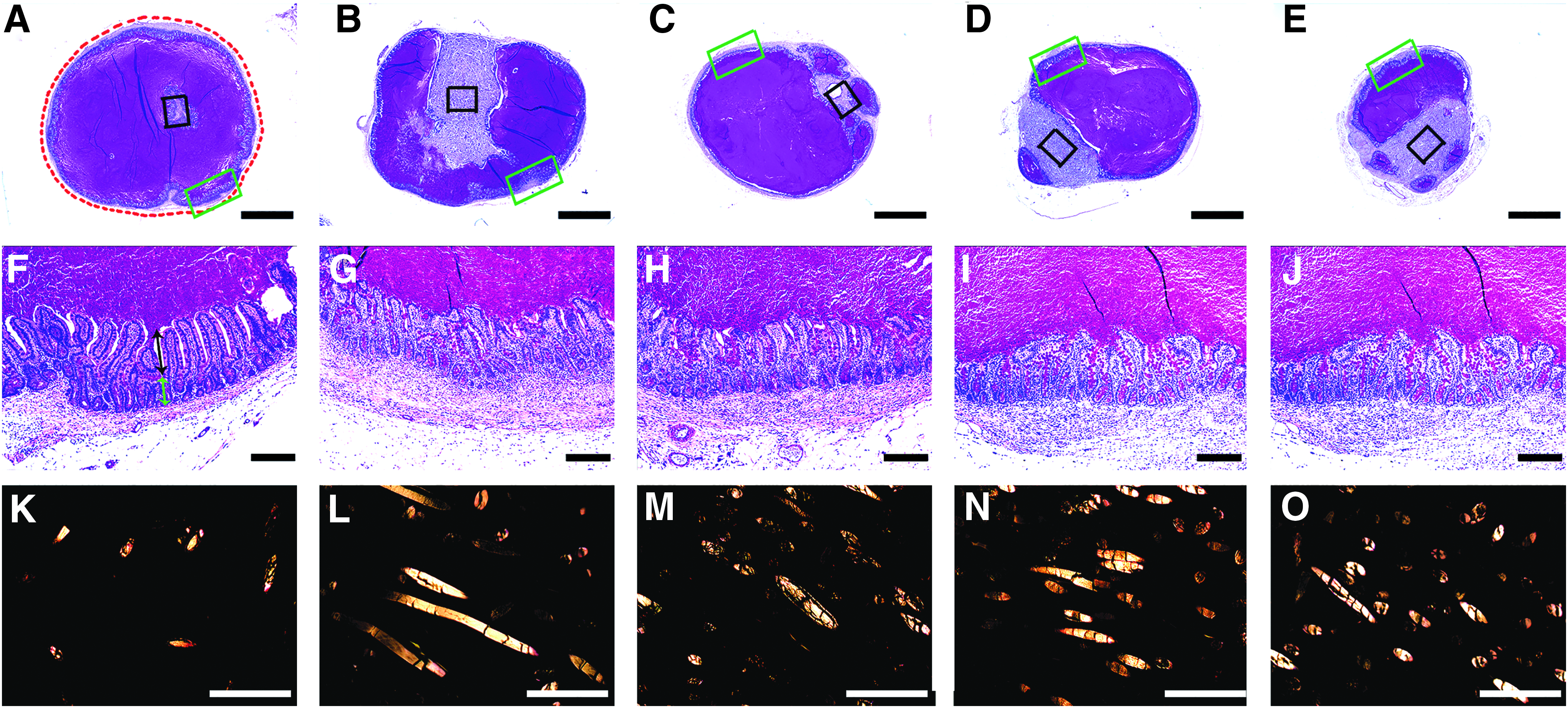
Histologic appearance of TESI produced in different implantation sites. PAS staining of TESI produced in different in vivo incubation sites.
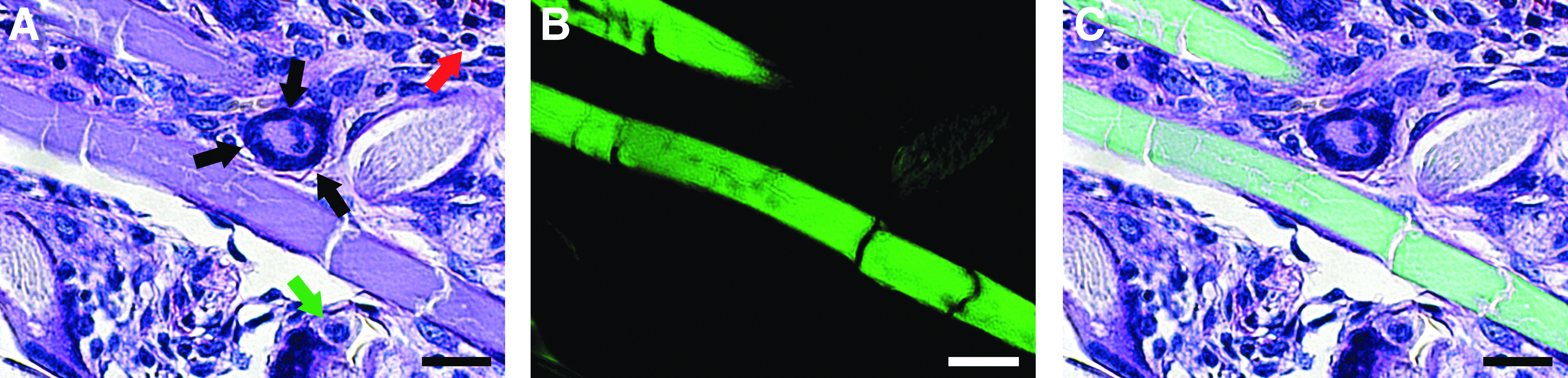
Foreign body reaction to implanted scaffold material. Images represent high magnification (60 × ) views of the area indicated by the black box in Figure 4A to demonstrate the relationship of unabsorbed scaffold material with surrounding tissue as visualized by:

Neomucosal length of TESI produced in different implantation sites.
TESI histology
IF staining demonstrated the presence of enteroendocrine cells, Paneth cells, brush border enterocytes, and actively proliferating cells in crypts (Fig. 7). Enteroendocrine cell density was quantified using ImageJ software and expressed as the number of cells/mm3 neomucosal surface area. Enteroendocrine cell density showed a similar pattern to villus height and crypt depth measurements in TESI produced in the five incubation sites. The presence of glial cells and mature neurons confirmed the presence of enteric nervous system elements in the TESI produced. GFP staining confirmed that the cell source of the enteric nervous system components was from GFP-positive implanted donor cells (Fig. 8). Figures 7 and 8 show representative images from TESI produced from implantation of cell-seeded scaffolds into omentum, but these components were also present in TESI produced in all other implantation sites.

TESI IF to detect intestinal epithelial cell lineages and proliferating cells. IF staining of TESI produced from implantation of cell-seeded scaffolds into omentum.

TESI IF to detect ENS components. IF staining of TESI produced from implantation of cell-seeded scaffolds into omentum.
TESI vascularization
The presence of blood vessels in TESI, and the differences in blood vessel densities between groups, was confirmed by IF staining for endothelial cells and SMC (Fig. 9). GFP, CD31 and α-smooth muscle actin costaining was used to track the cell source of blood vessels in TESI, since only implanted donor cells derived from transgenic GFP rats stain GFP positive (Fig. 9). This demonstrated that some blood vessels were derived from implanted GFP-positive cells and some blood vessels migrated from the host (GFP negative). The numbers of blood vessels from different sources were quantified using ImageJ software (Fig. 10). Migrated host blood vessels dominated in TESI produced in omentum, mesentery, and uterine horn membrane, while host and donor cells contributed equally to the blood vessels formed in TESI produced by attachment to the abdominal wall or in the subcutaneous space.
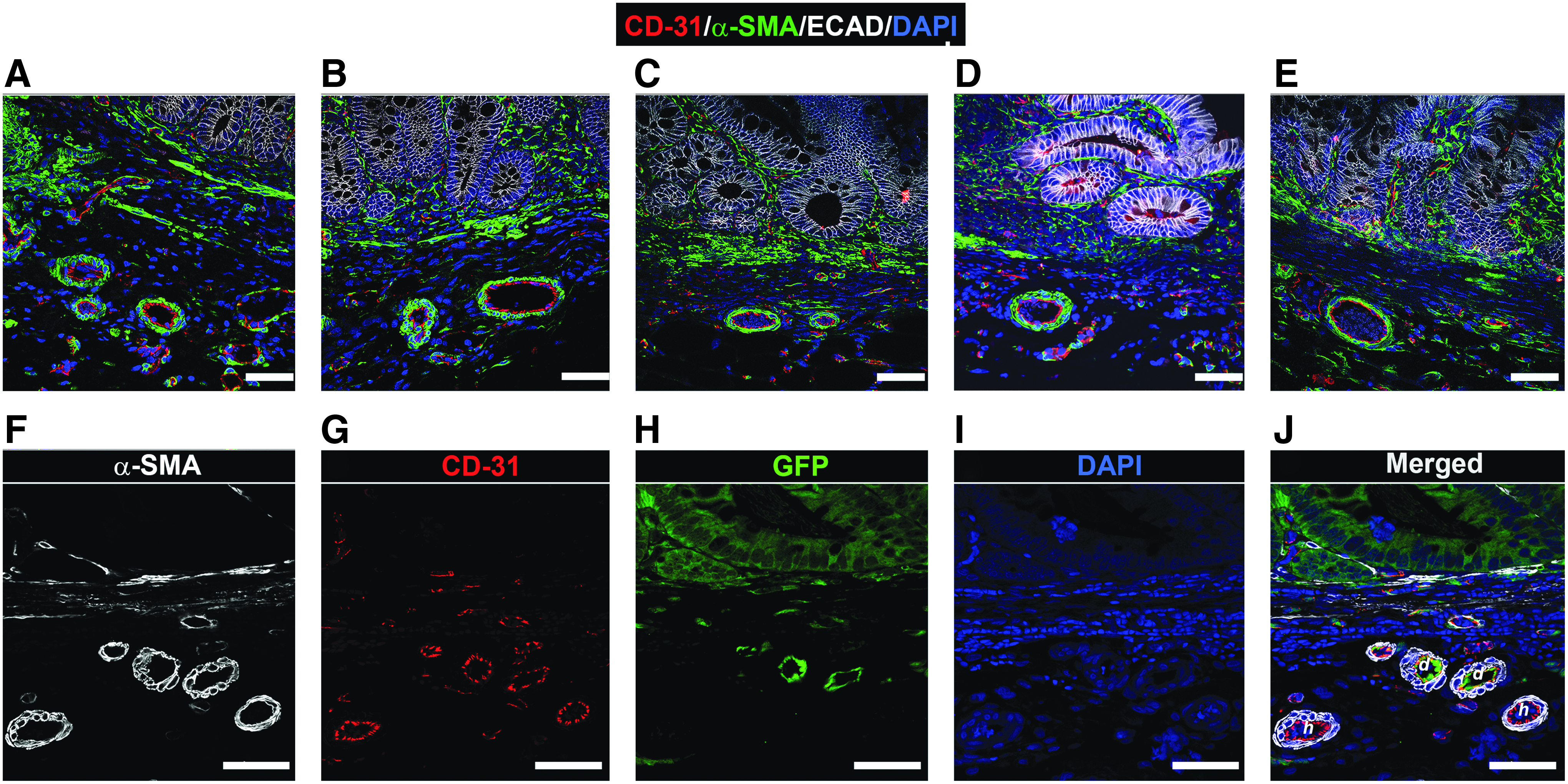
TESI IF to detect blood vessel density and cell source. IF staining of TESI produced in the following implantation sites:
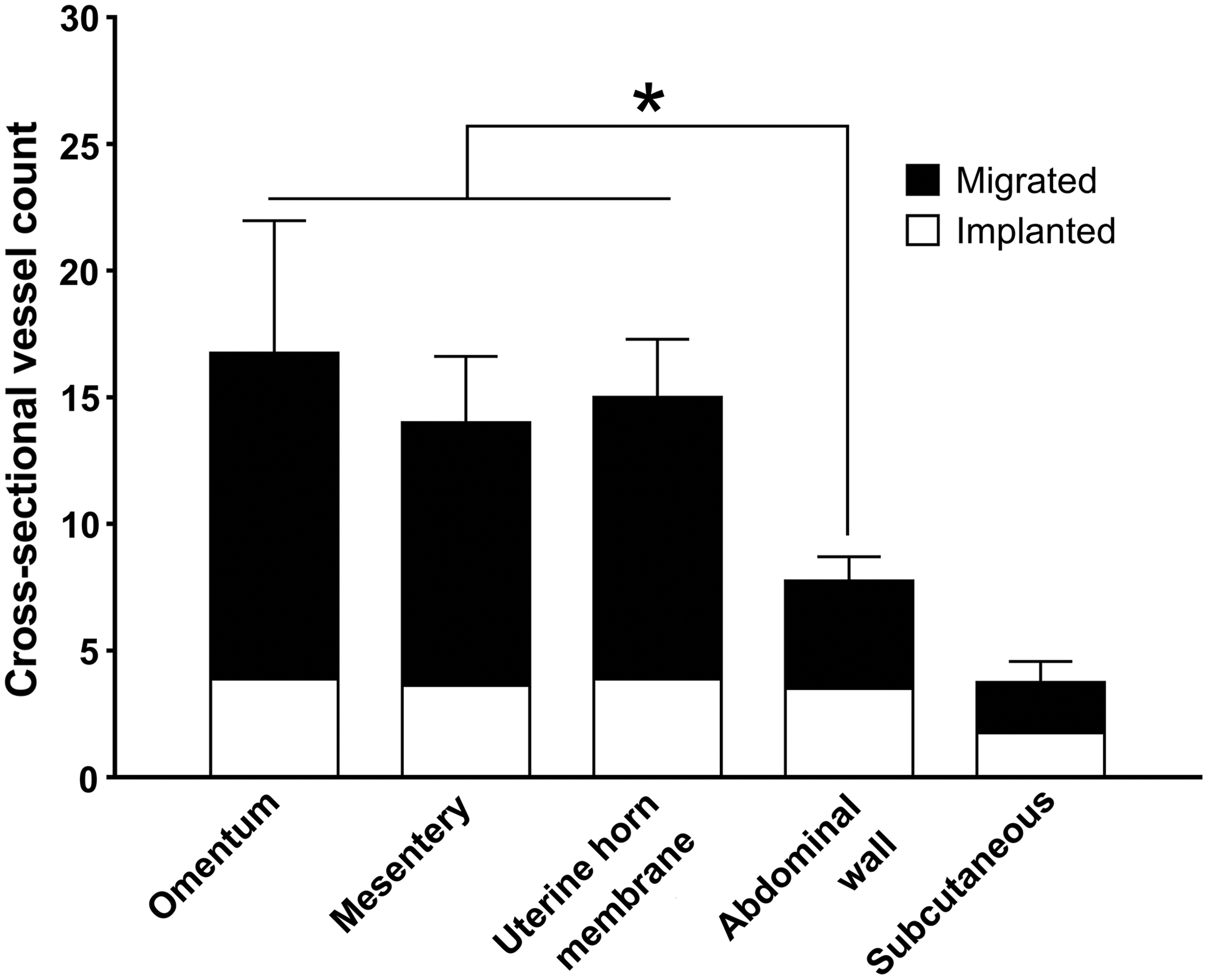
Quantification and source of blood vessels in TESI produced in different implantation sites. Blood vessels were quantified in TESI produced in different in vivo incubation sites. Since the cells from transgenic GFP donor rats were implanted into non-transgenic nude rats, we differentiated cells that migrated from the host (GFP negative) from GFP-positive donor cells. *p < 0.001.
Discussion
This study was designed to determine which in vivo incubation site is best for TESI maturation. Five different in vivo implantation sites were chosen for side-by-side comparison—four in the abdominal cavity and one in the subcutaneous space. Three of the implantation sites (omentum, intestinal mesentery, and uterine horn membrane) provided vascularized pedicles for TESI incubation. Vascularized pedicles play a very important role in assuring eventual successful anastomosis of TESI with host intestine.
Many previous attempts have been implemented to understand and improve the vascularization of TESI. Gardner-Thorpe et al. found that capillary density remained constant during a 1-, 3-, and 8-week period of in vivo TESI incubation, and that the levels of vascular endothelial growth factor (VEGF) and basic fibroblast growth factor were significantly lower in TESI compared to juvenile rat intestine. 21 Rocha et al. reported that addition of VEGF in poly(lactide-co-glycolide) microspheres during cell seeding produced larger intestinal constructs with significantly increased epithelial proliferation and capillary density compared to those without growth factor addition. 22
The intestinal mesentery is the main source of blood supply to native intestine. It is formed by a double fold of peritoneum that attaches the intestines to the posterior abdominal wall. 23 It emerges from the “root region,” which corresponds to the attachment of the superior mesenteric artery to the aorta. 24 From this point, the mesentery extends radially up to the intestinal margin. 23 It contains lymphatic, neurological, vascular, and connective tissues. Whether the mesentery should be viewed as part of the intestinal, vascular, endocrine, cardiovascular, or immunological systems is debatable, as it has important roles in all. Its effects are being investigated at the hematological, immunological, endocrine, metabolic, and other levels.25–28
Due to the important function of the intestinal mesentery and its crucial relationship to the attached intestine, production of TESI with a vascularized pedicle that can function as an intestinal mesentery will be key to successful implantation of TESI in line with the host intestine. In this study, of the five in vivo incubation sites tested, three membranes formed blood vessel-containing pedicles. Uterine horn membrane produced the longest pedicles, intestinal mesentery the shortest pedicles, and omentum an intermediate length of pedicle. Longer pedicle length gives the TESI more freedom for eventual relocation to the target site with anastomosis in line with host small intestine for the treatment of short bowel syndrome. Even though uterine horn membrane provides the longest pedicle to the TESI, omentum may be more clinically translatable since the uterine horn membrane is only present in females, and implantation into the mesentery carries a risk of damage to the remaining native intestine.
Implantation of seeded scaffolds into vascularized membranes also positively impacts the TESI produced, leading to increased quantity (volume and neomucosal length) and quality (villus height and crypt depth) of TESI. This may be attributable to the presence of blood vessels in the pedicle attached to the TESI, providing more abundant nutrients to the implanted cells. As confirmed by blood vessel quantification and source, there was increased blood vessel migration from the host into the TESI when scaffolds were implanted into vascularized membranes.
The blood supply to TESI impacts the patency of the TESI produced as well as the degradation of scaffold material. Patency of TESI is a very important factor that will impact the successful eventual anastomosis of TESI with host intestine to treat short bowel syndrome. The lumen of TESI is filled with acellular mucin produced by goblet cells, which can be easily removed to restore patency of TESI for future anastomosis. Unabsorbed scaffold material leads to late-stage foreign body reaction, which can impact the patency of TESI. The presence of a well-vascularized pedicle leads to faster scaffold degradation and removal of residual scaffold material with less fibrous tissue infiltration, improving the patency of the TESI produced. In this study, the TESI produced from the three vascularized pedicles has the least fibrous tissue interrupting the circumference of the neomucosa and occupying the lumen compared to TESI produced without vascularized pedicles, thus providing better patency and a thinner TESI sidewall, which should improve TESI function, a focus of our future studies.
In this study, attachment to the abdominal wall does not result in vascularized pedicles for the TESI produced, but does provide a beneficial environment for the seeded cells in the peritoneal cavity. This environment allows the seeded cells to be exposed to peritoneal fluid, which acts as a nutrient reservoir23,29 and may dilute the inflammatory reaction evoked by the scaffolds and their acidic degraded byproducts. 30 Without a vascularized pedicle, the TESI produced is of decreased quantity (TESI volume and neomucosal length), but similar quality (villus height), and contains blood vessels equally contributed by migration and implantation. One benefit of implantation into the abdominal wall is that its broad surface area allows multiple implantations of cell-seeded scaffolds for side-by-side comparisons of different factors that can affect the TESI produced.17,18
The poorest quantity of TESI produced in the subcutaneous space may be attributable to an inflammatory environment evoked by the scaffolds. Due to the limited space and limited fluid in the subcutaneous space, an inflammatory reaction with acidic degraded byproducts may occur locally and harm the seeded cells. In addition, the infiltration of inflammatory cells and fibroblasts may increase the formation of fibrous tissue in the TESI produced. 31 Although probably not clinically translatable, the subcutaneous space may be a useful site for screening and evaluating biomaterials as scaffolds for the production of TESI due to ease of access and localization of implanted materials for biocompatibility and biodegradation assessment.32,33
Conclusions
Among the five in vivo implantation sites, the three vascularized membranes (omentum, mesentery, and uterine horn membrane) produced vascularized pedicles, which likely provide increased blood supply and nutrients to the cells seeded onto the scaffolds for improved production of TESI. In addition, the vascularized pedicles produced have the potential to function as a mesentery, improving eventual successful anastomosis to native host intestine. The peritoneal cavity is the ideal local environment for in vivo TESI incubation. These findings should provide important insight for the clinical production of TESI in the future.
Footnotes
Acknowledgments
This study was supported by NIH R43 DK107168 and by the Research Institute at Nationwide Children's Hospital. The authors especially thank Cynthia Mcallister, Patricia Craig, Melanie Herring, and Kandace Joy for their assistance in sample preparation for histological assessment.
Disclosure Statement
No competing financial interests exist.