
Abstract
Cutaneous wounds can present significant clinical problems because of abnormal healing after deep dermal damage. Despite technical advances in wound care, there are still unmet needs that result from inefficient treatment. In this study, we aimed to improve skin wound healing using a contractibility band with static magnetic field (SMF), termed a magnetic band (Mb). To examine the effect of the Mb on wound healing, full-thickness 15 × 35 mm excision wounds were surgically created on the dorsum of rats. An elastic and contractile band (nontreatment), or one neodymium magnet (Nd-1) or two magnets with an elastic and contractile band (Nd-2) were topically applied to the wound daily and the wound size was measured from day 1 to 7 after surgery. Nd-2 showed a significant (95%) reduction in the wound size on day 3. Histological analysis showed that proinflammatory cytokine levels were diminished by Nd-2, and granulation tissue and microvessels were increased compared with those in the sham group. During Mb-induced wound healing, apoptosis was significantly reduced and matrix remodeling-related factors were initially regulated. The results suggest that combination therapy comprising an SMF and an elastic and contractile band could be a promising tool to heal cutaneous wounds rapidly.
Introduction
W
Over the past decades, magnetic fields, including static magnetic fields (SMFs) and pulsed electromagnetic fields (PEMFs), have been developed as an alternative, noninvasive therapeutic tool. PEMF is already used clinically to treat vascular and musculoskeletal pathologies. The therapeutic efficacy of PEMF has been proven in wound healing, hemodynamics, inflammation, and microcirculation.5–8 An SMF is based on the diamagnetic anisotropic properties of membrane phospholipids, and results in the deformation of imbedded ion channels, thereby altering their activation kinetics. SMFs are classified as weak (<1 mT), moderate (1 mT to 1 T), strong (1–5 T), and ultrastrong (>5 T).9,10 SMF stimulation has also been investigated in the therapy of the peripheral vascular system, and low-intensity SMF has been used to stimulate microcirculation. The detailed mechanism has not been determined; however, magnetic fields might enhance blood circulation and affect the vascular and lymphatic systems. Furthermore, the biological effect of magnetic field can restore local homeostasis, including (1) blood vessel walls; (2) intravascular plasma conduction; (3) insulating tissue matrix; (4) conducting interstitial fluid; and (5) electrical junctions for redox reactions (transcapillary junctions). The results from treatment of magnetic field may induce sympathetic outflow through vasoconstriction of injury site. 10
SMF stimulation can induce therapeutic effects in many tissue defects.11–14 Recent studies have shown that SMF increased the rate of wound healing.14–16 In the range of 230–4000 mT, wounds were improved in the skin of normal and diabetic model mice for 3 weeks. However, there has been no study on the rapid and effective cutaneous healing in the early phase after wounding.
To treat skin loss, a simple one-stage technique was developed under the name “rubber band technique.” This technique induces gradually wound closure by facilitated mobilization of skin in response to continuous tension. Despite proving to be a safe, simple, and effective way to treat widespread soft tissue damage, it has not escaped much of its conventional treatment. 17 The objective of this study was to evaluate an elastic and contractile band combined with an SMF (magnetic band [Mb]) and determine bidirectionally, through qualitative and quantitative methods, an Mb comprising one or two neodymium magnets covered with an elastic contractile band in a rat model of cutaneous wound healing.
Materials and Methods
Experimental wound model
Two-month-old male Sprague–Dawley rats (280 ± 20.0 g) were obtained from KOATECH (Korea), which was certificated for full accreditation awarded by The Association for Assessment and Accreditation of Laboratory Animal Care International (AAALAC). All experimental procedures were conducted in accordance with the guiding principles of the Committee for the Care and Use of Laboratory Animals, Catholic Kwandong University College of Medicine, and were performed in accordance with the Committee's Guidelines and Regulations for Animal Care, based on the Guide for the care and Use of Laboratory Animals, eighth edition (NIH, 2011). This study was performed according to a protocol approved by the Institutional Animal Care (CKU-01-2014-0001) and Use Committee of Catholic Kwandong University. Rats were housed in a room with a stable temperature (22.5°C ± 1.5°C), humidity (50–60%), and light–dark cycles (8:00 am–8:00 pm, light on).
Animals were divided into three groups (10 rats in each group; 5 rats for histological analysis and 5 rats for biological analysis): one group had their wounds treated with one neodymium magnet covered with an elastic and contractile band (Nd-1), another group had their wounds treated with two neodymium magnets covered with an elastic and contractile band (Nd-2), and the last group had their wounds treated with the elastic and contractile band only (sham control). On days 1, 3, 5, and 7 after surgery, each group was anesthetized with Zoletil™50 (tiletamine:zolazepam = 1:1, 20 mg/kg; Virbac, France) and Rompun 2% (xylazine, 5 mg/kg; Bayer, Germany) and euthanized with an intraperitoneal overdose of sodium pentobarbital at each time point. The wound model was prepared by making an incision in the skin. Before sacrifice, the wound sizes of all rats were measured and photographed with a superimposed grid. Thereafter, wounds and surrounding tissues were sampled for histological and molecular biological analysis. Dressing was performed using an Mb once every 2 days, and the Mb and skin were fixed with a staple (iTool® APEXSUTURE™; Apex (Guangzhou) Tools & Orthopedics Company, China).
Preparation and distribution of the Mb
Neodymium was prepared with a length of 10 × 40 mm, and then covered with an elastic band (Elatex; Alcare Co., Ltd., Japan) on the top of wound dressing foam (Fig. 1A, RenoFoam; T&L, Korea).

Magnetic exposure in the wound model.
The strength of the Mb used was measured using a gaussmeter (model SJ300; Weite Magnetic, China) at 5-mm interval in the horizontal and vertical axes and 2 mm above the magnet. Two- and three-dimensional maps of the magnetic field were graphically represented using Matlab software (The MathWorks, Natick, MA).
Measurement of wound size
Wounds were measured using a previously published method. 18 The wound area was photographed with a superimposed grid, and analyzed using Image J version 1.49 (NIH, Bethesda, MD). The wound closure rate was calculated according to the following formula: Wound relative area (%) = [(Areaday 0 − Areaday n)/Areaday 0] × 100, where Areaday 0 is the initial wound area on day 0 and Areaday n is the area on day n after wounding from day 1 to 7.
Histological evaluation
Skin tissues were fixed in 10% neutral buffered formalin. The specimens were embedded in paraffin, sectioned, and stained with hematoxylin and eosin (H&E). H&E-stained slides were viewed at 100 × and 200 × magnification with BX51/dot slide microscope (Olympus, Japan).
Immunohistochemistry
Immunohistochemical analyses using antibodies recognizing proliferating cell nuclear antigen (PCNA) and α-smooth muscle actin (α-SMA) (Abcam, Cambridge, MA), and cluster of differentiation 31 (CD31) (Santa Cruz Biotechnology, Inc., Dallas, TX) were performed according to the manufacturer's instructions. PCNA-positive cells and CD31-positive capillaries were counted in six nonoverlapping visual fields.
Reverse transcription–polymerase chain reaction
Reverse transcription–polymerase chain reaction (RT-PCR) was performed according to the method used in our previous study. 19 Skin tissue was cut into 5-mm pieces from the end of the wound. RNA was extracted using 1 mL of Trizol® reagent (Sigma-Aldrich, St. Louis, MO). Total cellular RNA was extracted using a chloroform, isopropanol, and 75% diethyl pyrocarbonate in ethanol procedure. RNA was resuspended in nuclease-free water. The quantity and quality of the isolated RNA were determined by calculating the OD260/OD280 ratio using a DU 640 spectrophotometer (Eppendorf, Germany). cDNA was generated using a reverse transcription system (Promega, Madison, WI) according to the manufacturer's instructions. Five hundred nanograms of RNA was reverse transcribed in a reaction mixture containing 5 mM MgCl2, 10 mM Tris-HCl (pH 9.0 at 25°C), 50 mM KCl, 0.1% Triton X-100, 1 mM dNTP, 20 U RNase inhibitor, 0.5 μg oligo-(dT) 15 primer, and 10 U reverse transcriptase for 15 min at 42°C, and the reaction was terminated at 99°C for 5 min. To monitor cDNA synthesis, we used a PCR mixture with primers. PCR oligonucleotides were synthesized by Bioneer (Bioneer, Inc., Korea) (Table 1). The PCR mix contained 10 nM of each primer, together with 200 mM Tris-HCl (pH 8.8), 100 mM KCl, 1.5 mM MgSO4, 1% Triton X-100, 0.1 mM dNTPs, and 1.25 U of Taq polymerase in a total volume of 12 μL. PCR conditions were 94°C for 3 min; followed by 30 cycles of denaturation at 94°C for 30 s, x°C for 30 s (where x was the melting temperature of the primers), and 72°C for 1 min; followed by a final extension step at 72°C for 10 min for many DNA. All RT-PCR products were separated by electrophoresis on a 1.2% agarose gel and visualized using Gel-Doc (Bio-Rad, Hercules, CA) after staining with ethidium bromide (Sigma).
TdT-mediated dUTP nick end labeling assay
The TdT-mediated dUTP nick end labeling (TUNEL) assay was performed according to the method used in our previous study and according to the manufacturer's instructions (Chemicon International, Temecula, CA). 20 In brief, 5-μm slide sections were deparaffinized, rehydrated, and rinsed with phosphate-buffered saline. The sections were pretreated with 3.0% H2O2, subjected to terminal deoxynucleotidyl transferase enzyme for 37°C for 1 h, and incubated in digoxigenin-conjugated nucleotide substrate at 37°C for 30 min. Nuclei exhibiting DNA fragmentation were visualized by adding 3,3-diaminobenzidine (DAB; Vector Laboratories, Burlingame, CA) for 5 min. Last, sections were counterstained with methyl green. A coverslip was placed on top of each section, and the sections were observed by light microscopy. For each group, six slices were prepared and six nonoverlapping regions were observed in each slice.
Enzyme-linked immunosorbent assay
The enzyme-linked immunosorbent assay (ELISA) was performed according to the manufacturer's instructions (RayBiotech, Inc., Norcross, GA). At 1 and 7 days following wounding, tissue samples were homogenized in protein extraction buffer with protease inhibitors. The lysates were centrifuged at 10,000 g at 4°C for 30 min and the supernatant was retained. Samples were subjected to ELISA to quantify the concentration of vascular endothelial growth factor (VEGF) and interleukin (IL)-1β. The absorbance was measured at 450 nm.
Statistical analysis
Quantitative data were expressed as the mean ± SEM of at least three independent experiments. For the statistical analysis, one-way analysis of variance (ANOVA) with Bonferroni correction was performed using the Prism software (ver. 5.0; GraphPad Software, Inc., La Jolla, CA) if more than three groups were analyzed. A p value less than 0.05 was considered to indicate statistically significant data.
Results
Magnetic bands
Mbs composed of neodymium magnets, wound dressing foam, and elastic and contractile band were produced, and named as “Nd-1” and “Nd-2” depending on the number of magnets (Fig. 1A). In the case of Nd-2, the Mb is strongly coupled by the attraction between the two magnets.
Using a gaussmeter, the magnetic force of the Mbs was measured at a distance of 2 mm from the magnet. Two-dimensional (Fig. 1B) and three-dimensional (Fig. 1C) maps of the magnetic flux were produced using the Matlab program. Based on the center of the magnet, Nd-1 had an intensity of ∼1500 gauss (max. 1780 gauss, min. 1420 gauss), and at a distance of 2 mm, it had an intensity of ∼1000 gauss (max. 1090 gauss, min. 900 gauss). The magnetic field area of Nd-2 was twice as large as that of Nd-1. When the neodymium magnets were separated by 12 mm, the intensity in center of the magnets was ∼2400 gauss, and when the two magnets were attached, the magnetic force increased to ∼3000 gauss. Furthermore, Nd-2 had an intensity average of ∼1800 gauss (max. 2000 gauss, min. 1500 gauss), and at a distance of 2 mm, it had an intensity of ∼1100 gauss (max. 1200 gauss, min. 840 gauss). Nd-2 showed a 1.2-fold increase in the magnetic force and a 2-fold increase in the effective width of the magnetic field compared with Nd-1.
Effect of Mb on wound closure
We evaluated the effect of the Mbs on the healing rate and wound reduction of skin wounds in three groups of rats. As shown in Figure 2A, we induced wounds on the dorsal skin of rats (15 × 35 mm) to prevent “dog-ear” from sticking to the magnets. Mbs (Nd-1 or Nd-2) were then applied to the dorsal wound area (Fig. 2B), and wound closure and reduction distance were measured at 1, 3, 5, and 7 days after surgery. The Nd-2-treated group showed substantially accelerated wound closure compared with the Nd-1 or sham group on 1 day after wounding. From day 5 to 7, the wound size was significantly reduced in the Nd-1 treatment group compared with that in the sham group (Fig. 2C, D). In particular, at day 3 postwounding, Nd-2 presented a significant 95% reduction in the wound size. In terms of wound width, Nd-2 also decreased the wound width from day 1; however, Nd-1 did not reduce the wound width significantly compared with that in the sham group (Fig. 2E), indicating that Nd-2 therapy accelerated the early cutaneous wound closure.
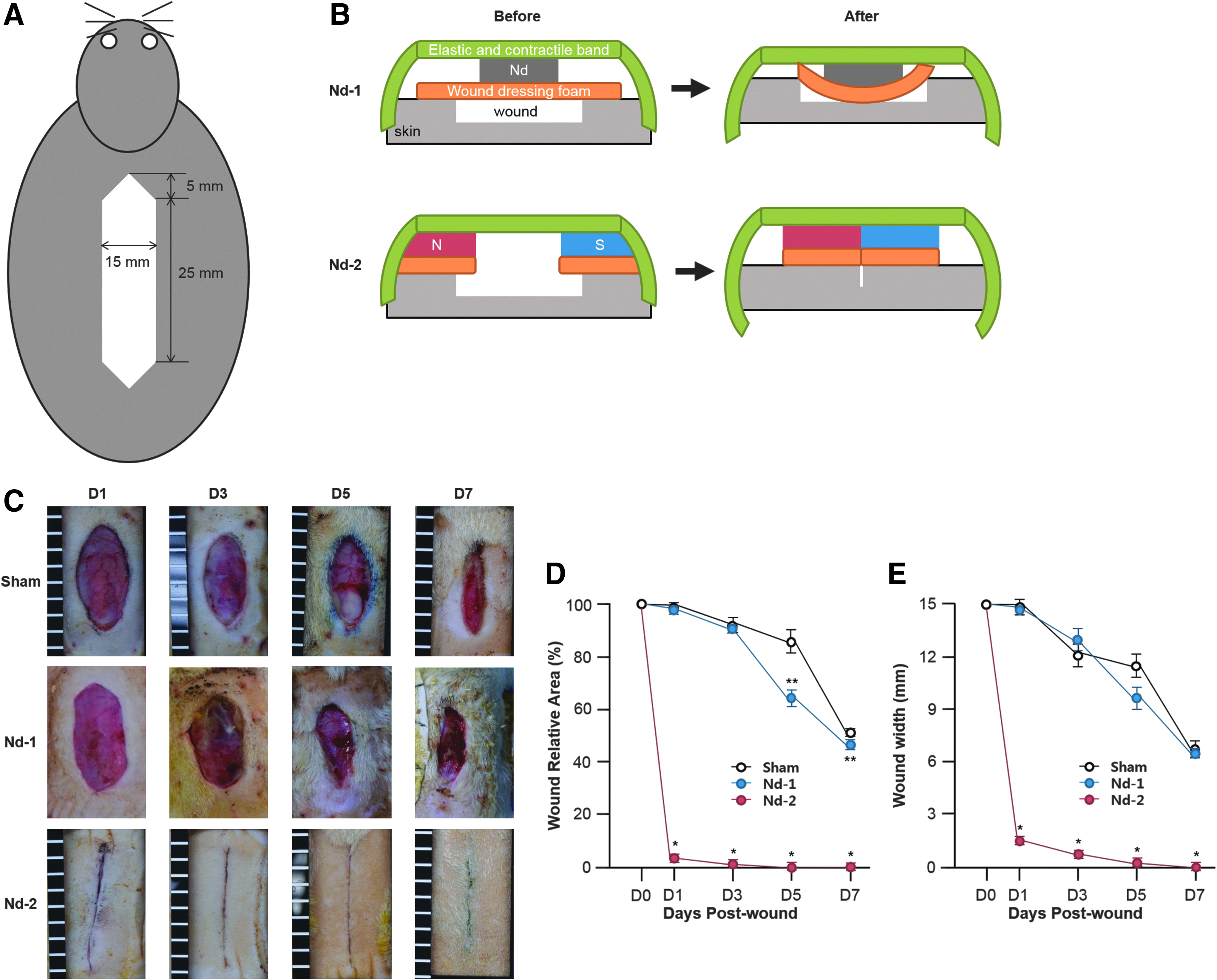
Effect of the Mbs on wound closure.
Histological improvement of the wound site
As shown in Figure 3, from the third day after surgery, advanced fibrin breakdown (white asterisks) was induced at site of the Nd-2-treated wounds. Furthermore, various cells, including fibroblast and macrophages, infiltrated in the Nd-2-treated wound area (white arrowhead). In addition, on day 3–5, increased granulation tissues and a number of branched microvessels were observed in the Nd-2 group compared with those in the Nd-1 or sham group. To examine granulation formation, PCNA and α-SMA were stained with DAB. In the Nd-2 group, PCNA-positive infiltrating cells showed a high proliferation index of more than 50% on day 3, which is early in the phase of proliferation and matrix deposition after inflammation, and is consistent with rapid wound healing (Fig. 4A, B). For the vascularity of the wound site, α-SMA was stained and positive cells were considered to represent myofibroblasts. On day 7, the Nd-2 group had a fourfold higher number of α-SMA-positive cells compared with the sham group. Nd-1 also showed a higher number of positive cells than the sham group, but fewer than that shown by the Nd-2 group (Fig. 4C, D). Taken together, Nd-2 induced the next stage of wound healing earlier compared with the sham or Nd-1 group.
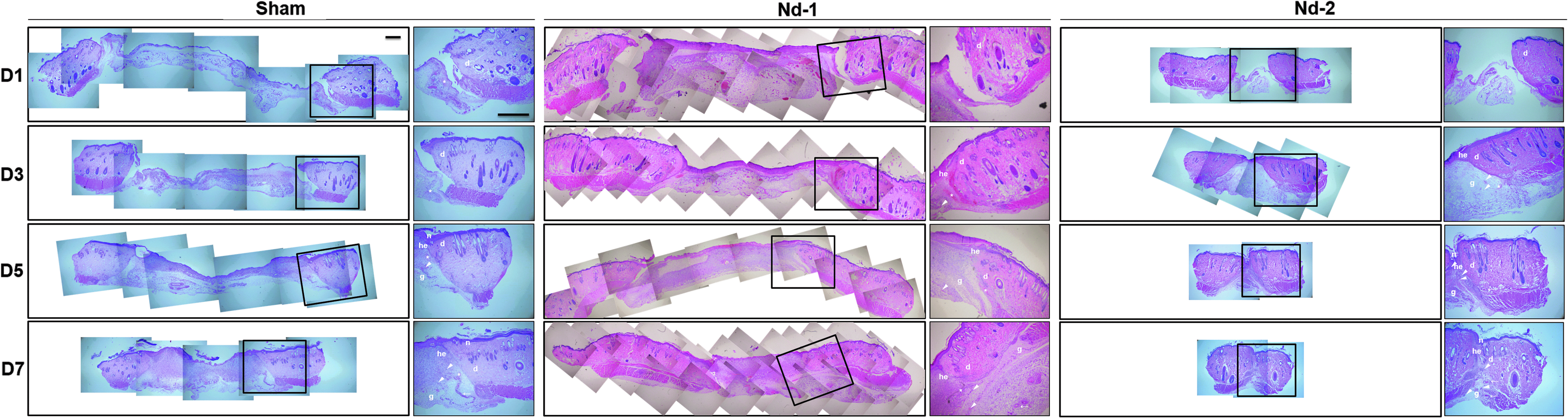
Effect of Mb on wound healing process. H&E staining for granulation tissue formation of excisional skin wounds after therapy. g, granulation tissue; d, dermis; he, hyperproliferative epithelium; n, polymorphonuclear neutrophils; white asterisk, fibrin clot; white arrowheads, capillaries; and white arrows, branched microvessels. Scale bars = 1 mm. Nd-1, one neodymium magnet; Nd-2, two neodymium magnets. H&E, hematoxylin and eosin. For ease of reading, figure labels can be magnified online at http://www.liebertpub.com/tea
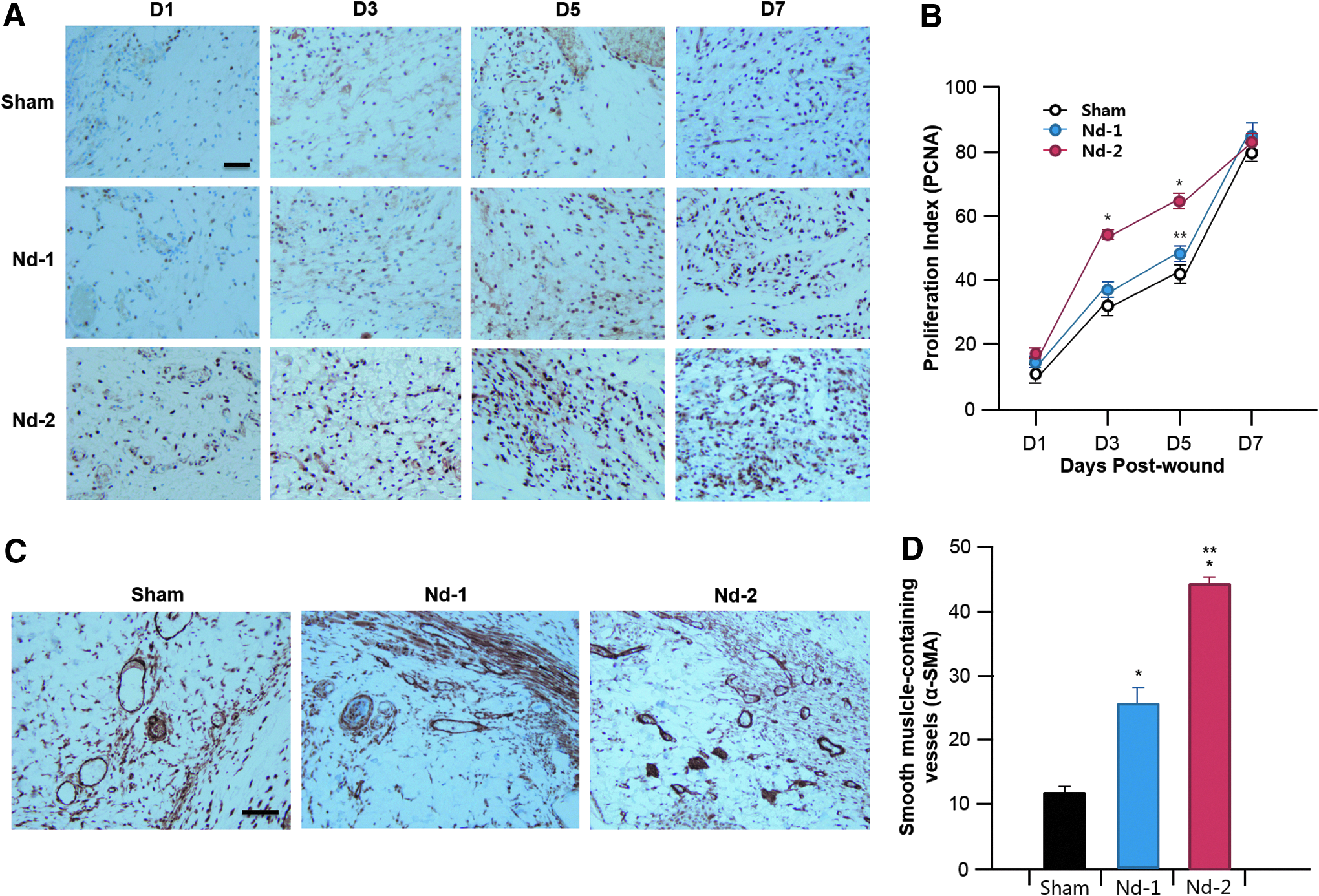
Effect of the Mb on granulation formation.
Regulation of wound-associated inflammation
Wound-associated inflammation is required for clearance of cellular debris at the wound site. Neutrophil infiltration was observed in the samples shown in Figure 3. To analyze the inflammation status of the wound area, inflammation-related gene expression was investigated. The expressions of the mRNAs encoding IL-6 and TNF-α (IL6 and TFNA), as proinflammatory cytokines, were downregulated in the Nd-2 samples compared with those in the sham group. The expression of IL6 was significantly reduced by 3 days postwounding (Fig. 5A). Furthermore, TNFA levels were elevated on day 3, but stabilized until 7 days after surgery (Fig. 5B). At 1 and 7 days postwounding, the protein level of IL-1β in the Nd-2 group was significantly reduced compared with that in the sham group (Fig. 5C). In particular, treatment with neodymium magnets at 7 days postsurgery showed a decrease in IL-1 levels compared with those in the sham group. These results suggest that neodymium magnets, especially Nd-2, could promote wound healing by regulating the early production of inflammatory cytokines.
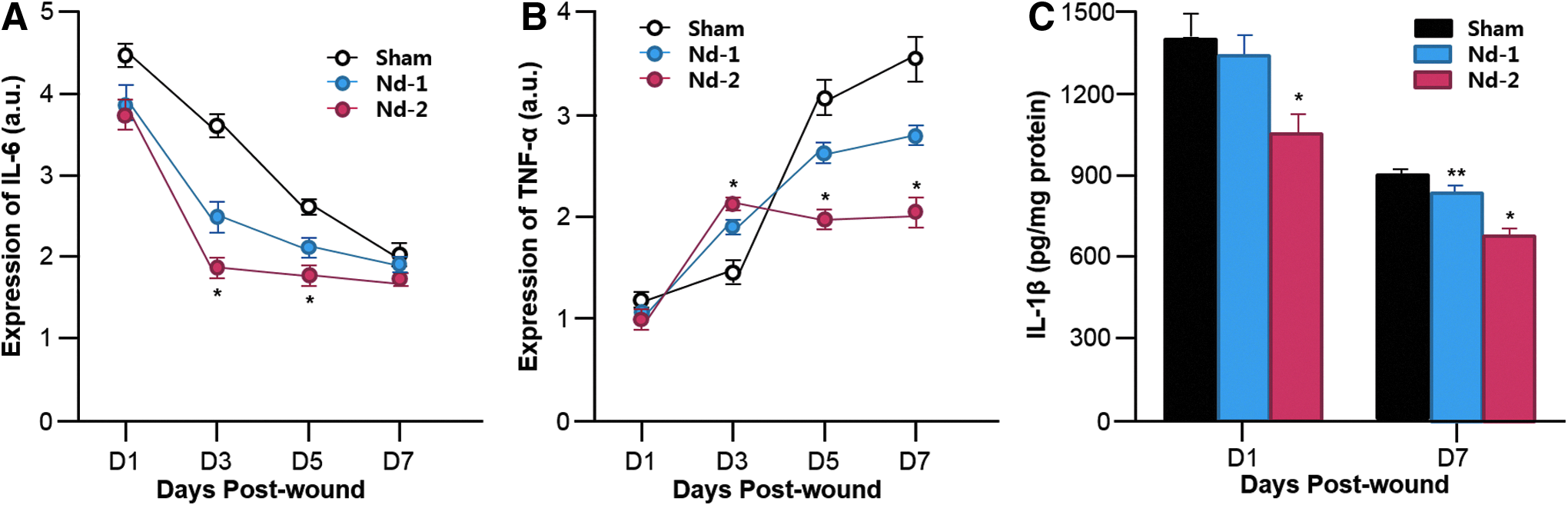
Changes in proinflammatory cytokine levels in the wound site. mRNA expression level of IL-6 (IL6)
Regulation of cell apoptosis
To investigate whether the neodymium magnets could regulate cell apoptosis, histological and molecular biological analyses were performed. Counting of TUNEL-positive cells showed that apoptosis in the Nd-2 group decreased by ∼40%. Nd-1 also reduced cell apoptosis compared with the sham group (Fig. 6A, B). To observe the degree of cell apoptosis of the wound area, apoptosis-related gene expression was investigated. The expressions of the proapoptotic genes, tumor necrosis factor receptor 1 (TNFR1) and BCL2-associated X protein (BAX), in the Nd-2 group were downregulated by about 40% compared with those in the sham group on day 7 (Fig. 6C, D). This suggested that neodymium magnets, especially Nd-2, alleviate apoptosis during wound healing.
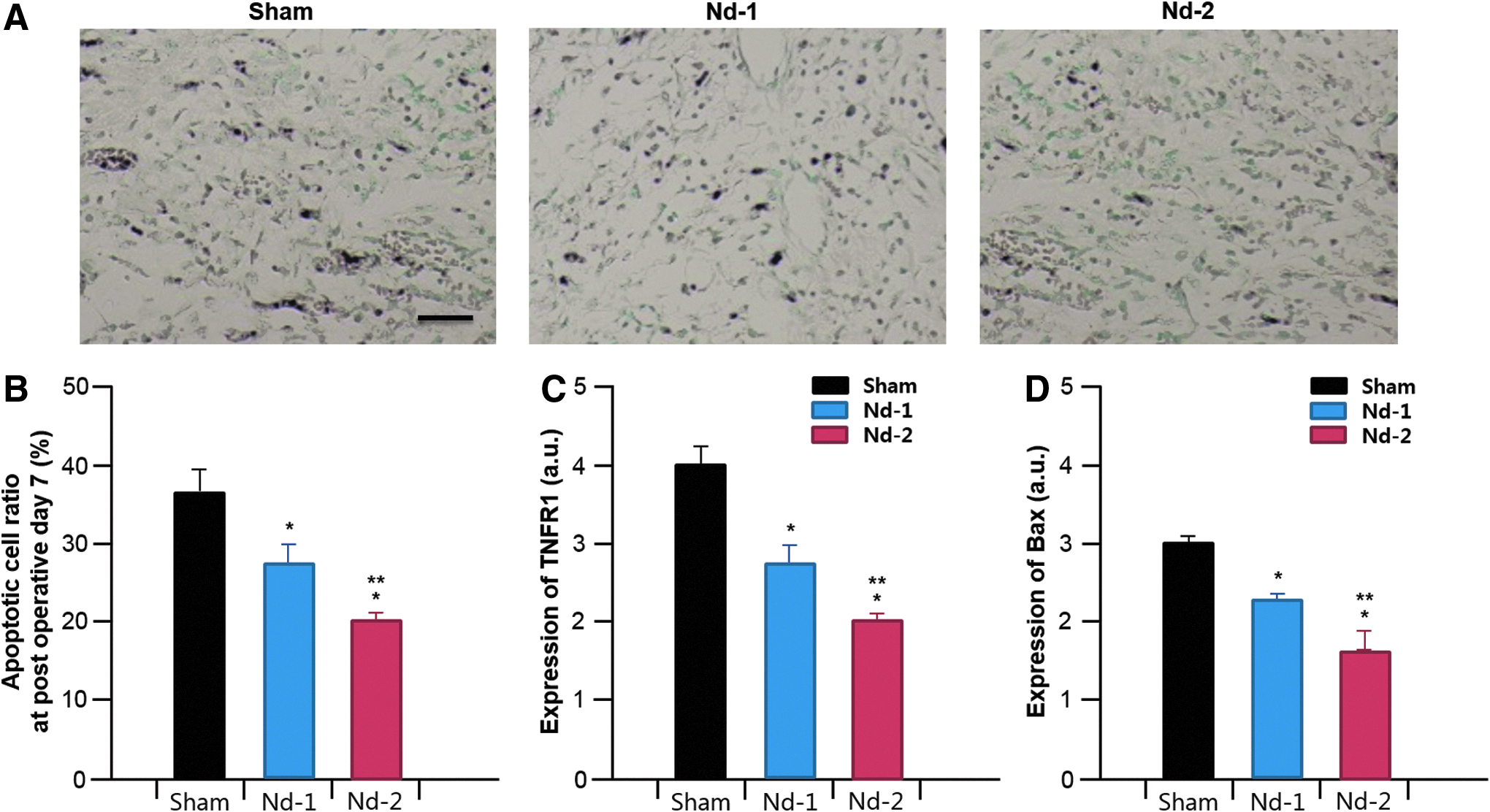
Different biological behavior of wounded skin on day 7.
Promotion of angiogenesis
To determine the generation of microvessels for blood and oxygen supply, CD31 staining was performed in each group of tissues (Fig. 7A). On day 7, about 20 CD31-positive microvessels were observed in the Nd-2 group, which was more than 3.8 times higher compared with that in the sham group and twofold higher compared with that in the Nd-1 group (Fig. 7B). To investigate whether neodymium magnet therapy promotes angiogenesis, the angiogenic factor VEGF was analyzed using an ELISA. There was no significant change in VEGF in all groups on 1 day after surgery; the VEGF level increased by 1.5-fold in the Nd-2 group compared with that in the sham group at 7 days postwounding. These results suggested that the Nd-2 could effectively induce the generation of microvessels and promote angiogenesis by increasing VEGF expression in the wound site.

Change of angiogenic phase during wound closure.
Change in the stages of wound maturation
During the proliferative and matrix deposition phase, fibroblasts migrate into the wound site and secrete collagen. At this time, collagen-III is initially deposited and then collagen-I is induced later. We investigated collagen-related gene expression after surgery. In the case of mRNAs encoding procollagen-III (COL3A1) expression, the neodymium magnets had a strong influence compared with the sham group. At day 3–5, COL3A1 was actively expressed in the Nd-2 treatment group (Fig. 8A). The expression of mRNAs encoding procollagen-I (COL1A1) occurred somewhat later compared with COL3A1. On day 5, COL1A1 expression in the Nd-2 group was ∼1.6-fold higher than that in the sham group, and then there was an ∼3-fold difference in COL1A1 expression between the Nd-2 and sham groups (Fig. 8B).

Induction of wound maturation in the skin.
Matrix metalloproteinases (MMPs) are active in the matrix remodeling phase. We confirmed that MMP2 was highly expressed in the Nd-2 group on day 3 after wounding. Nd-1 also induced higher MMP2 expression from day 3 (Fig. 8C). In the Nd-2 group, induction of MMP9 expression started from the third day, and strong expression was detected on the fifth day (Fig. 8D). In the Nd-1 group, MMP9 expression started to increase later, on day 7, whereas MMP expression was almost absent in the sham group.
Discussion
Magnetic fields affect cellular behavior, including cell proliferation, migration, and differentiation, to induce homeostasis and regenerate damaged tissues.21–23 There have been studies on PEMF and SMF from the viewpoint of regenerating poor condition tissues. The application of PEMF (20 Hz, 4 ms, 8 mT for 1 h per day) accelerated delayed wound healing in diabetes mellitus. 24 In addition, the induction of static and high-power magnetic fields (0.4–4 mT) using SMF can improve wound healing. 15 In diabetic rat models, the wound healing effects of 230 mT SMF were demonstrated by evaluating the wound area reduction rate, the mean time to wound closure, and the wound tensile strength. 16 However, these studies have serious limitations in many areas. First, regardless of wound size, healing needs to occur quickly. A scar from permanent skin injury can have an effect on healing delay, resulting in scar contracture and hypertrophic scars.25,26 Second, an ancillary system is required that can keep the magnetic field stable, safe, and effective. Magnetic scaffolds, including nanocomposites, induce the combined application of external and internal magnetism; however, these scaffolds are not suitable to fix it to prevent further wound opening or promoting wound healing. 23 Finally, there is a lack of histological and pathophysiological analyses on wound healing using magnetic fields. Our study aimed to utilize an effective magnetic field and to improve the speed of wound healing. Therefore, we hypothesized that a combination of a magnetic field with contractility might generate synergistic effects to induce and accelerate cutaneous wound healing. To test this hypothesis, the capacity of an elastic and contractile band with an SMF, termed Mb, was examined in terms of functional improvement in the cutaneous wound healing process (I. Inflammation, II. Cell proliferation and matrix deposition, and III. Matrix remodeling) in an incision model of rats.
The Nd-2 Mb had an average magnetic force of about 1800 gauss ( = 180 mT). In a previous study, the effect of a 180 mT moderate-intensity gradient SMF in diabetic wound healing was assessed. From 5 to 19 days after wounding, the SMF treatment group showed about a 10–30% lower wound healing rate than the normal control group, although the types of models were different. 27 Another study used 230 mT SMF exposure and reported that the SMF treatment group showed faster wound healing of 5.2%, 10.5%, and 21.2% on days 7, 14, and 21 compared to the diabetic sham group. 16 However, the results of this study suggested that the combined effect of an SMF and an elastic and contractile band increased the wound healing rate (compared with that of the sham group) by ∼90% at 1 day after wounding (Fig. 2C, D).
In general, the wound healing process is divided into three stages: I. Inflammation, II. Cell proliferation and matrix deposition, and III. Matrix remodeling. In this process, intercommunication and various complex reactions occur, which involve many growth factors and cytokines. 28 Inflammation occurs to precipitate the blood clot and encourage platelet aggregation and infiltration of leukocytes (neutrophil and macrophages) into wound site. 29 We found neutrophil infiltration and proinflammatory reduction at day 1–3 after surgery (Figs. 3 and 5). This demonstrated that wound healing began quickly, over 1–2 days. Under normal physiological conditions, granulation tissue, including fibroblasts, macrophage, and neovasculature, is increased at 5 days. In our case, the expressions of PCNA and α-SMA, which are responsible for cell proliferation, increased from day 3 after wounding (Fig. 4), and the angiogenic phase, as measured by the induction of CD31 and VEGF, increased by about fourfold on the seventh day (Fig. 7). One week after injury, maturation occurs by collagen deposition.3,30 This process involves the transfer of various proteases, such as urokinase-type plasminogen activator (uPA), tissue-type plasminogen activator (tPA), and MMPs, into the newly formed tissues of the epidermis. In our study, procollagen and MMP were rapidly released at a relatively high rate (Fig. 8).
A major problem with wound healing is the loss of cellular integrity because the damage may cause acute physiological imbalance and, ultimately, disability. 29 However, we believe that the Mb, which combines neodymium magnets with an elastic and contractile band, is able to hold the collapsed tissue and improve the cellular integrity to restore homeostasis rapidly.
The exact mechanism of the therapeutic effect of an SMF on wound healing remains unclear. When wound sites are exposed to an SMF, several studies noted an improvement of blood circulation.31–34 Functional improvement of vascular circulation by an SMF is consistent with our rapid neovascularization and angiogenesis data. However, further mechanistic studies are required. For example, functional evaluation could be completed by measuring the tension between skin edges after treatment with Mbs. Furthermore, analysis of the population of various infiltrated cells in early wound healing could help to reveal the mechanism of action of Mb. Taken together, although this was a preliminary study, we believe that Mbs will become important tools for inducing rapid wound healing and scarless skin.
Conclusions
This study demonstrated combination therapy of applying an SMF within a contractility band on cutaneous wound healing. Rapid healing by the Mb (especially Nd-2) could be explained through wound closure, histological changes, reduction of proinflammatory cytokine levels, and proapoptotic cell death, increased angiogenesis, and fast maturation. These findings suggested that combination therapy of SMF and elastic and contractile band encouraged fast wound healing. The developed bioengineering tool could be a therapeutic approach to improve damaged skin rapidly and effectively, and is a potential tool for clinical application in wound healing therapy.
Footnotes
Acknowledgments
This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning [grant number NRF-2015R1C1A1A02037693]; and by research fund of Catholic Kwandong University International St. Mary's Hospital [grant no. CKURF-201407060001].
Disclosure Statement
No competing financial interests exist.