
Abstract
We developed a highly elastic customized scaffold for soft tissue regeneration and combined them with bioactive hydrogels with stem cell-inducing ability. This was done to mimic mechanical properties of native soft tissues and improve the viability of transplanted cells as well as efficiency of tissue regeneration. The proposed study was aimed at evaluating various characteristics of scaffolds and investigating their tissue-regenerating ability. Finger-shaped porous scaffolds were successfully fabricated by an indirect 3D printing of poly (L-lactide-co-ɛ-caprolactone) (PLCL), which provides high elasticity for soft tissue engineering. In addition, a self-assembling peptide hydrogel coupled with substance P (RARADADARARADADA/RARADADARARADADA-substance P, RADA16/RADA16-SP) was used to accelerate angiogenesis and recruit intrinsic mesenchymal stem cells (MSCs). This study included three kinds of groups: Group I = PLCL scaffold with human dermal fibroblasts (HDFs) (P+C), Group II = PLCL scaffold with HDFs and RADA16 (P+C+R), and Group III = PLCL scaffold with HDFs, RADA16, and RADA16-SP (P+C+R+S). The samples were implanted into immunodeficient mice subcutaneously and harvested at 1 and 4 weeks. Tissue regeneration was evaluated by histological analysis with hematoxylin and eosin (H&E) and Masson's trichrome (MT) staining. The images showed that a large number of cells were recruited into the scaffolds, and collagen was deposited in the constructs of the P+C+R+S group. Additionally, recruitment of MSCs, angiogenesis, and collagen were observed by immunofluorescence staining. The results show that the P+C+R+S group had more type I and type III collagen, which are formed in soft tissues, and were deposited on the scaffold compared with the other groups. Moreover, more blood vessels and MSCs were induced in the P+C+R+S group than in those of the P + C and P+C+R groups. Consequently, the results suggest that the construct of the customized porous PLCL scaffold and RADA16/RADA16-SP hydrogel could be a good treatment modality to treat skin defects.
Introduction
F
Numerous studies have reported strategies that have focused on the development of biomaterials to enhance angiogenesis and epithelialization for the regeneration of skin tissue.6,7 Three-dimensional printing is used to fabricate scaffolds that have customized shape and complex structures with precise compositions for tissue engineering applications. In particular, the availability of precise and reproducible fabrication enables manufacturing of customized scaffolds that exactly match the dimensions of the injured parts of patients.8,9 Because tissue and/or organs possess a curved surface, an anatomical structure is difficult to be replicated through use of a 2D sheet or structure with a predefined shape. In addition, some researchers have used biomolecules or cells in scaffolds with 3D printing for a biomimetic environment. 10 Hong et al. developed 3D printable highly stretchable and tough hydrogels for regeneration of soft tissue. Polyethylene glycol and alginate formed crosslinking by UV and calcium ion, respectively. It could be printed with cells and form a customized shape. 11 Lee et al. studied the design and fabrication of human skin with three-dimensional bioprinting. They used collagen with keratinocytes and fibroblasts to mimic complex skin tissue. 12 Koch et al. reported 3D skin tissue with laser cell printing. Fibroblasts and keratinocytes embedded in collagen were 3D printed for skin tissue. The appeal is that the system is promising for achieving 3D tissue substitutes for many applications in tissue engineering. 13
Although they have potential to regenerate skin tissue, they still have weak points. Generally, UV-crosslinked hydrogels are nondegradable and they contain additives such as crosslinking reagents. In addition, when noncrosslinked hydrogels were used for 3D printing, they had a weak mechanical property, which lead to a disruption in the shape and size of the constructs.
Implanted biomaterials must be supported so that cells migrate and a vascular supply is established. Scaffolds consisting of synthetic polymers can degrade and mimic the properties of native tissues at the target area. 14 Especially, scaffolds should mimic the extracellular matrix (ECM), which provides not only structure and biological function but also chemical constitution and physical organization. 15 A deficiency in blood vessels results in hypoxia, which means that oxygen tension reaches zero. Therefore, angiogenesis is essential to transport nutrients and oxygen, and growth factors are the required constituents for tissue repair.16,17 Differentiated cells such as pericytes are known to enhance angiogenesis at an injury site by expressing angiogenesis factors.18,19 However, they have some problems; differentiated cells are difficult to harvest in large amounts, difficult to expand in vitro, and difficult to engraft due to their low engraftment capacity. The stem cells have received much attention as a promising alternative source to solve these problems. 20
In our previous studies, we developed elastic scaffolds that have similar mechanical properties to native vascular tissue for soft tissue regeneration.21,22 Poly (L-lactide-co-ɛ-caprolactone) (PLCL), used as the main structural material, has high elasticity when the high molecular weight PLCL comprises equimolar amounts of LA and CL. It is possible to fabricate elastic scaffolds that have certain stiffness by controlling the microstructure of the scaffolds. According to the studies, PLCL scaffolds could mimic the mechanical properties of cartilage or blood vessels, and they enhanced the regeneration of tissues by mechanotransduction.21,23
In previous studies, we confirmed that bioactive peptide hydrogels containing substance P (SP) promoted angiogenesis and tissue formation by recruiting key cells such as CD29+ cells.22,24 Peptide hydrogels are also known as self-assembling peptides (SAPs) that form a nanofibrous network structure with fibrous diameters measuring 6–10 nm in neutral pH and physiological solutions, thereby mimicking ECM.25–28 SP refers to an 11-amino acid neuropeptide extensively found in nervous systems of vertebrates.29,30 Various roles of SP have been reported, including mobilization of CD29+ stromal-like cells, angiogenesis enhancement, cytokine and growth-factor regulation leading to subsequent stimulation of wound healing, and recruitment of mesenchymal stem cells (MSCs).30–33 MSCs migrate to injured sites, support proliferation and differentiation, promote tissue angiogenesis, and regenerate tissues.33–35
In this study, we developed a PLCL scaffold, which possesses an anatomically customized shape and mechanical properties similar to those of the native tissue, by means of indirect 3D printing. 36 A finger-shaped highly elastic scaffold was fabricated to demonstrate that scaffolds could be manufactured by mimicking complex anatomical shapes—one big advantage of the 3D-printing technology—and that highly elastic materials can be employed to this end. Moreover, a SAP hydrogel coupled with SP was used with human dermal fibroblasts (HDFs). We hypothesized that the customized elastic PLCL scaffold could be used clinically because it can maintain the shape after repeated strain. In addition, the SAP hydrogel coupled with SP enhances angiogenesis by recruiting CD29+ cells and accelerates tissue formation. To evaluate the potential of tissue regeneration, an in vivo test was performed, in which the samples were implanted subcutaneously into immunodeficient mice. Explanted finger-shaped constructs with HDFs, RADA, and RADA-SP were analyzed to verify their effect on tissue regeneration.
Materials and Methods
Fabrication of the PLCL scaffolds
The synthesis of PLCL was described in a previous study. 37 PLCL scaffolds were fabricated with indirect 3D printing and a salt leaching technique (Fig. 1). First, the polyvinyl alcohol (PVA) finger structure that was used for the sacrificial mold was printed with a 3D printer (Vistech Korea, Daejeon, Korea) and filled with the dissolved PLCL in chloroform and NaCl (300–400 μm) at a ratio of 10:90 (w/w). The solvent was evaporated for 1 day at room temperature and completely removed under vacuum for 5 days. The PVA and NaCl product was leached in distilled, deionized water with stirring for 3 days and sonicated thrice for 30 min. Then, freeze-drying was done for 3 days to remove any moisture. Finally, the PLCL scaffolds were sterilized with ethylene oxide gas (Person medical Co. Ltd, Gunpo, Korea) before animal testing.

Overall scheme of this study.
Characterization of the scaffolds
The morphology of the PLCL scaffold was examined with scanning electron microscopy (SEM) (Phenom-world, Eindhoven, Netherlands). The surface and cross-section of the samples were observed. To determine mechanical properties of the samples, the PLCL scaffold was compressed using a 10-kN load cell at the rate of 1.5 mm/min (Instron). The compressive modulus is defined as the force per unit area applied to the scaffold during compression, and is calculated as the slope of the initial straight line in the stress–strain curve. Recovery was calculated with the following equation
38
:
where L0 is the original length, L1 is the extended length, and L2 is the final length after releasing the stress. We observed the porosity of the PLCL scaffold with a mercury intrusion porosimeter (MicroMeritics). Fourier-Transform Infrared Spectroscopy with Attenuated Total Reflectance analysis (FTIR-ATR; Thermo Scientific) was performed to verify that the PVA mold was removed. All spectra were performed with 32 scans in the range 4000–600 cm−1 with a resolution of 4 cm−1. A porosimeter (MicroMeritics) was used to determine the porosity of the scaffold. Degradation of the PLCL scaffold was evaluated by measuring the molecular weight of the polymer, 4 weeks after transplantation, through the use of gel permeation chromatography (GPC; Viscotek TDAmax, Malvern Instruments Ltd, Worcestershire, United Kingdom).
In vivo experiments
All mice (BALB/c, immunodeficient mouse, 7-week old, male; Nara Biotech, Seoul, Korea) were treated in accordance with the Institutional Animal Care and Use Committee (IACUC No. 2016–02018) at the Korea Institute of Science and Technology. The mice were temporarily anesthetized with ethyl ether. All equipment for the surgery was sterilized with an autoclave in advance.
HDFs (LONZA, passage number = 4) were collected with trypsin treatment, and the concentration of the cell suspension was 1.5 × 105 cells/mL in minimum essential media (MEM) without L-glutamine (HyClone) supplemented with 10% v/v fetal bovine serum (FBS; HyClone), 1% v/v glutaMAX™-1 (Gibco), 1% v/v sodium pyruvate (Gibco), 1% v/v MEM nonessential amino acids (MEM NEAA; Gibco), and 1% penicillin-streptomycin (Corning).
The peptide hydrogels, which were RADA (AcN-RARADADARARADADA-CNH2) and RADA-SP (AcN-RARADADARARADADAGGRPKPQQFFGLM-CONH2), were purchased from Peptron (Daejeon, Korea). RADA and RADA-SP peptide were dissolved in a 295 mM sucrose solution to produce a 1% (w/v) peptide gel and sonicated 30 min before use. 30
Three hundred microliters of HDF suspension in PBS containing calcium and magnesium ions (5 × 106 cells/mL) was mixed with 300 μL of peptide gel and then, the mixture was seeded into the finger-shaped PLCL scaffold. For in vitro gelation of the hydrogel, cells were complexed with PBS containing calcium and magnesium ions. The constructs were incubated at 37°C in a humidified atmosphere containing 5% CO2 for 4 h before implantation.
Samples prepared above were used for in vivo study. Three different groups were examined: Group I, PLCL scaffold with HDFs (P+C); Group II, PLCL scaffold with HDFs and RADA (P+C+R); and Group III, PLCL scaffold with HDFs, RADA, and RADA-SP (200:1; P+C+R+S). 20 Before implantation, the PLCL scaffolds were immersed with media for 4 h at 37°C in a humidified atmosphere containing 5% CO2. Groups I, II, and III were implanted into the mice subcutaneously (n = 3 per group). All analyses were done at 1 and 4 weeks after surgery.
Histological analysis
The samples explanted from the mice were fixed in 10% formaldehyde for 24 h. Fixed samples were embedded in paraffin and sectioned at 6 μm thicknesses for staining. The sectioned samples were stained with hematoxylin and eosin (H&E) and Masson's trichrome (MT).
Quantitative measurement of total soluble collagen
The total soluble collagen content was measured with the Sircol soluble collagen assay kit (Biocolor life science assays, Northern Ireland, United Kingdom). All the samples were digested in acetic acid-pepsin solution overnight at 4°C. The manufacturer's instructions were followed to measure the total soluble collagen content. Finally, the assay was measured at a wavelength of 555 nm with a microplate reader. The total collagen 3D printing technology and produce amount was calculated with a standard collagen curve. All samples were used as wet tissues. For standardization, the amount of the sample was expressed as the amount of collagen per unit weight of the sample.
Immunofluorescence staining
Type I collagen and type III collagen were double stained with anti-collagen I antibody (GeneTex; 1:400) and anti-collagen III antibody (Abcam, Cambridge, United Kingdom; 1:400). To analyze angiogenesis, endothelial cells and smooth muscle cells were double stained with anti-human von Willebrand factor antibody (Abcam; 1:1000) and anti-human α-smooth muscle actin antibody (Abcam; 1:100). To check whether MSCs were recruited, samples were stained with MSC markers (CD90/CD105; Abcam/Abcam; 1:300/1:200). Immunofluorescent stained images were quantified by choosing three random fields ( × 200 magnification). To evaluate whether SP was sustained in the mice after 1 and 4 weeks, the SP was stained with SP antibody (Santa Cruz Biotechnology, Inc.; 1:500). All immunofluorescence staining was observed with a confocal microscope (ZEISS, Oberkochen, Germany.) We calculated the stained area using image analysis program, Image J (Google). The total area was calculated based on the length of the scale bar of the image, and the area stained in the total area was expressed as a numerical value.
Statistical analysis
All samples were assayed at least in triplicate, and the results obtained were expressed as the standard deviations (SD) above and below the mean. All statistical analyses were done with the ANOVA test (GraphPad Prism 6). Results were considered to be statistically significant when the p-value was less than 0.05.
Results
Characterization of the PLCL scaffold
The 3D structured PLCL scaffold was prepared with an indirect 3D printing technique and salt leaching. Its height, diameter, and thickness were 22, 9, and 2.2 mm, respectively (Fig. 2a, b). After bending the PLCL scaffold with a pair of tweezers, it reverted back to its original shape. The PLCL scaffold fabricated with the process described in the Materials and Methods section retained its original elasticity (Fig. 2c). The morphology, especially the porous structure, of the PLCL scaffold was examined by SEM. The surface of the scaffold had stripes on it because of the inherent nature of 3D printing, which deposits materials layer-by-layer (Fig. 2d). The interior of the scaffold had a porous structure, shown in Figure 2e. The SEM results show that the pore distribution was 150–400 μm and had an average pore size of 304.12 ± 76.96 μm (Fig. 2f). The porosity of the PLCL scaffold was measured with a mercury intrusion porosimeter. The porosity was 86.59 ± 1.96. In addition, the Young's modulus of the PLCL scaffold was 0.15 ± 0.06 MPa.
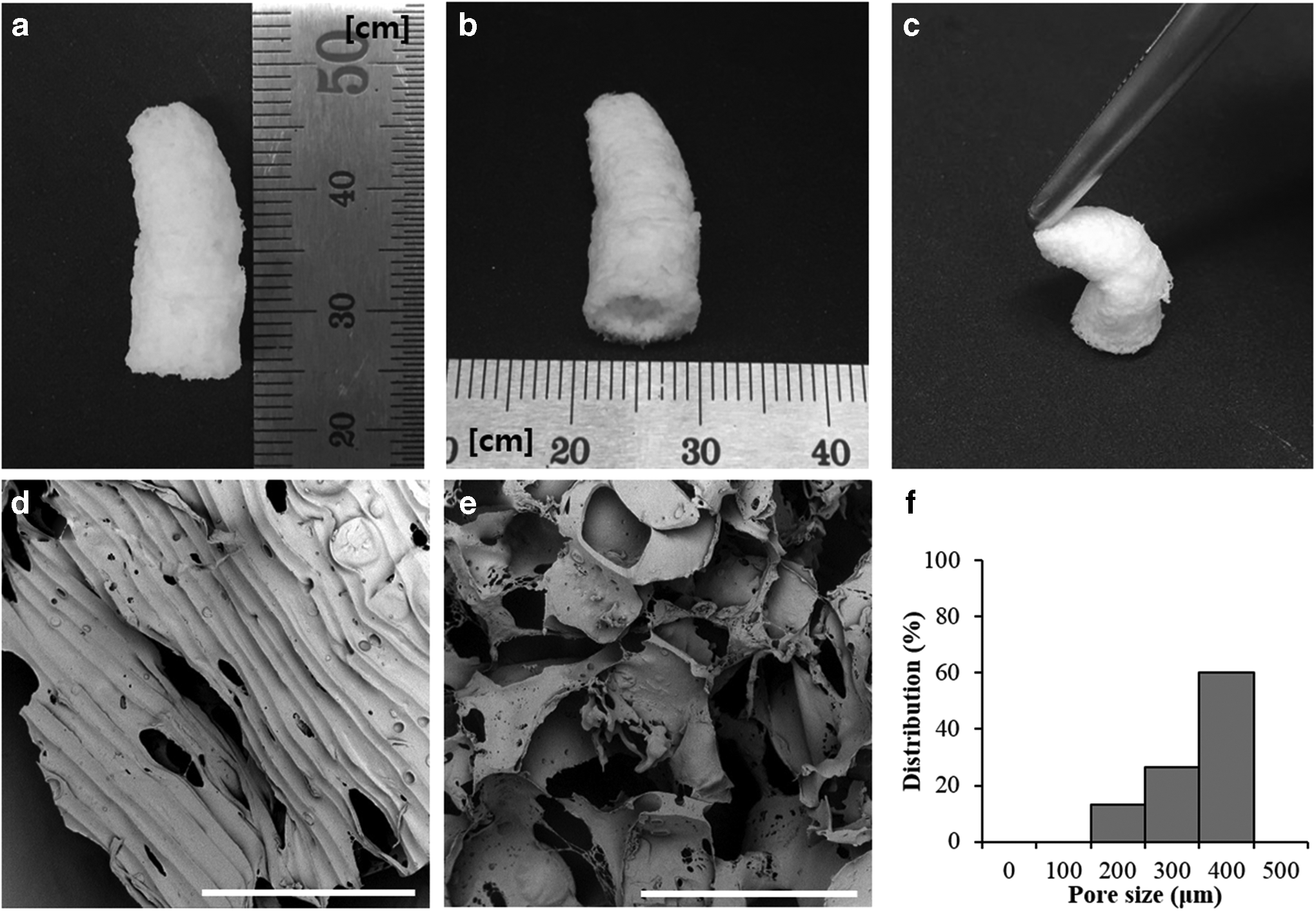
Pictures of the finger-structured scaffold
Figure 3a shows the FTIR-ATR spectra of PLCL (pure PLCL), PVA, and PLCL scaffold. The PVA absorption bands were at 3275–3387 cm−1 (O-H stretching), 2913–2927 cm−1 (alkyl stretching), and 1416–1436 cm−1 (C-H stretching). 39 The pure PLCL absorption bands were at 2934–2956 cm−1 (C-H stretching), 1755–1756 cm−1 (C = O stretching), 1453–1457 cm−1 (CH2 bending), and 1182–1187 cm−1 (C-O stretching). 40 The PLCL scaffold was identical with the pure PLCL trend for FTIR-ATR.
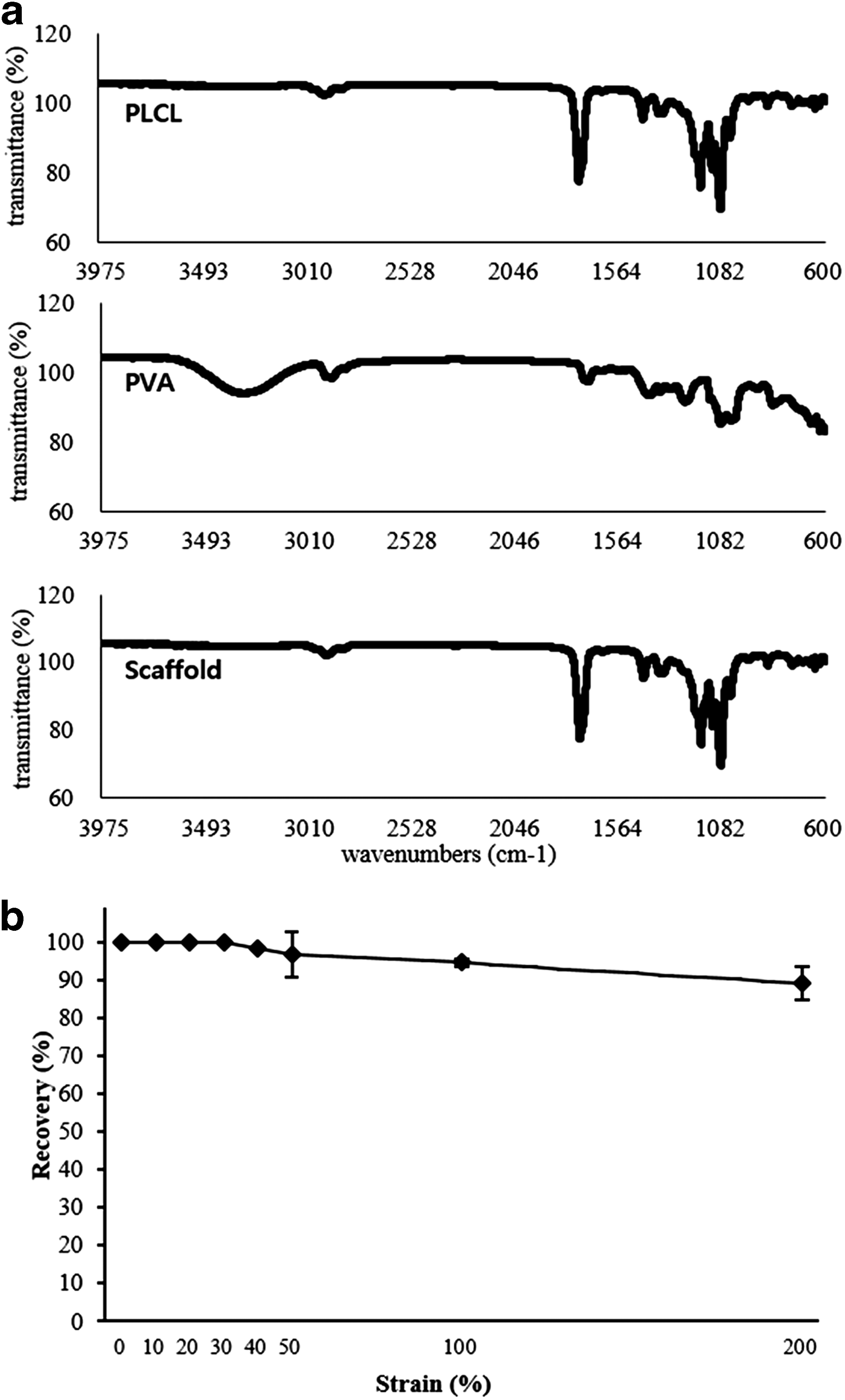
To correctly measure the elasticity, we performed a recovery test. It showed 100% recovery until a 30% strain, 96.61% ± 5.87% recovery at a 50% strain, 94.44% ± 1.64% recovery at a 100% strain, and 88.99% ± 4.49% recovery at a 200% strain (Fig. 3b).
Mechanical properties and degradation test of in vivo samples
To examine the effect of tissue ingrowth into the 3D structured scaffolds, we did an in vivo test with 7-week-old immunodeficient mice that had the scaffolds implanted subcutaneously. The samples that were implanted into the immunodeficient mice were harvested at 1 and 4 weeks after the surgery (Fig. 4). Figure 5 shows the compressive modulus for each group of samples. The increased compressive modulus from week 1 to 4 in all the groups was time dependent. In addition, although the three groups did not have significantly different values, the average of the P+C+R+S group was the highest among the groups. The mean value of the P+C+R+S group was higher about 1.3 times compared to the P + C group. Based on the results, it seems that more cells migrated into the constructs of the P+C+R+S and formed tissue at the site.

The explanted scaffolds after 1 and 4 weeks in nude mice subcutaneously.
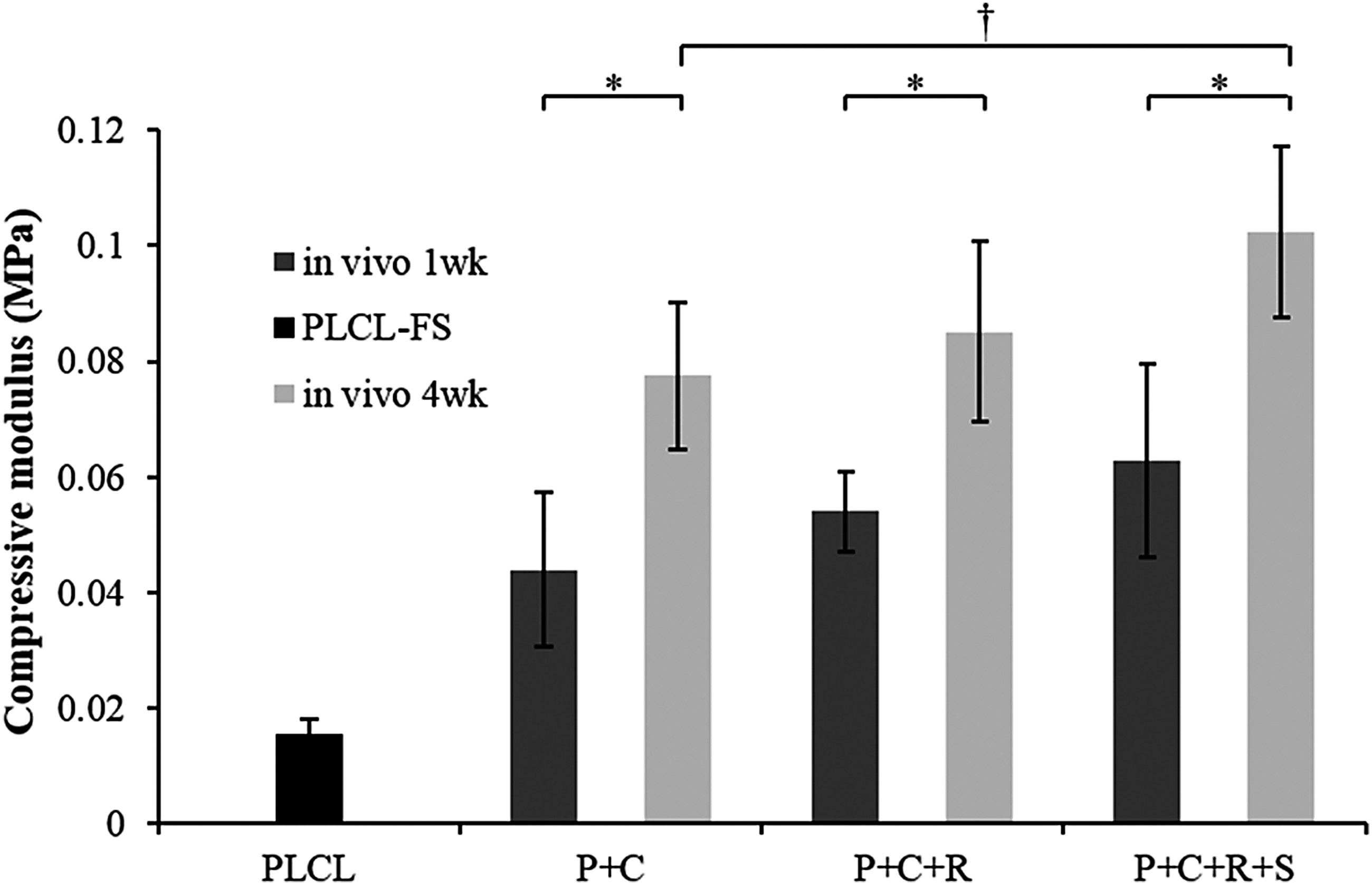
The compressive modulus of the finger-structured scaffold compared with PLCL and in vivo after 1 and 4 weeks. (*p < 0.05, †p < 0.1).
PLCL degradation was evaluated by measuring the molecular weight of the polymer. Samples harvested at the end of week 4 after implantation possessed number-averaged (Mn) and weight-averaged (Mw) molecular weights of 119,000 and 175,400, respectively. When compared against raw PLCL material (Mn = 137,700, and Mw = 195,600), Mn and Mw values of the harvested samples were observed to have decreased by approximately 15.71% and 11.5%, respectively. The PLCL polymer demonstrated high degradation after 4 weeks in the in vivo environment.
Histological analysis
After explanting the samples, H&E and MT staining were performed for histological analysis (Fig. 6a). The P + C group for 1 and 4 weeks had the smallest number of cells recruited to the scaffold based on the H&E staining compared with the P+C+R and P+C+R+S groups. At 1 week, most of the groups showed low tissue regeneration. However, some blood vessels were observed in the P+C+R+S group shown by the H&E staining data. In addition, the P+C+R+S group had a larger number of cells recruited to the scaffold compared with the other groups. At 4 weeks, all the H&E staining images of the groups showed that cells were recruited and new tissue formed in the scaffold compared with at 1 week. Significantly, many blood vessels and new tissue formation were observed in the P+C+R+S group at 4 weeks.

Histological studies of the explanted scaffolds.
The results of the MT staining were similar with the tendency for the H&E staining. The MT staining images showed that the group with the smallest amount of deposited collagen was the P + C group at 1 week (Fig. 6b). However, the P+C+R and P+C+R+S groups had some collagen shown by MT staining at 1 week. At 4 weeks, the amount of collagen was increased in all the groups compared with at 1 week. Most of them, the P+C+R and P+C+R+S groups, had more collagen compared with the P + C group.
Quantification of the total soluble collagen
Collagen is an ECM component, secreted by transplanted and recruited cells. Results of this study demonstrate that in all groups, the amount of collagen was higher at the end of week 4 compared to that during week 1. This implies that at week 4, after transplantation of the construct, the accumulated number of recruited cells is higher. Comparing this result with those obtained for different groups, it was observed that the amount of collagen in groups 2 and 3 containing hydrogel was relatively higher compared to that in group 1. However, in groups 2 and 3, it was confirmed that similar amounts of soluble collagen were contained within the structure.
By analyzing the quantity in detail, at 1 week, the P + C group had 14.81 ± 0.67 μg/mg of collagen, and it is significantly the lowest value compared with the other groups. However, there was no statistical difference between the P+C+R and P+C+R+S groups at 1 week. By 4 weeks, the total soluble collagen levels were significantly higher than those at 1 week in the P+C, P+C+R, and P+C+R+S groups. Especially, the P+C+R+S group had the highest total soluble collagen level among the groups, which was 64.61 ± 0.16 μg/mg. The P + C group at 4 weeks had the lowest level of total soluble collagen at 46.47 ± 0.57 μg/mg, while the P+C+R group had a total soluble collagen level of 62.04 ± 1.19 μg/mg. The P + C and P+C+R+S groups had significantly different total soluble collagen levels; however, there was no statistically significant difference between the P+C+R and P+C+R+S groups.
Immunofluorescence staining
Type I and type III collagen, which consist of soft tissue mainly, were analyzed quantitatively with immunofluorescence staining at 1 and 4 weeks (Fig. 7a, b). All the groups investigated had gradually increased values for both type I and type III collagen. Type I collagen in the P + C group increased from week 1 to 4; however, there was no difference statistically. Nevertheless, in the P+C+R and P+C+R+S groups, the quantity of type I collagen increased by approximately two to three times when comparing week 1 with week 4 (Fig. 7c). There was a statistical difference between the P + C and P+C+R groups as well as between the P + C and P+C+R+S groups (*p < 0.05). Type III collagen showed a statistical difference between all the groups when comparing week 1 with week 4. Especially, the P+C+R+S group had the highest level of type III collagen, respectively, and was statistically different from the P + C group (**p < 0.01).

To examine angiogenesis, we did immunofluorescence staining of von Willebrand factor (vWF) and α-smooth muscle actin (α-SMA), which are factors in endothelial cells and smooth muscle cells, respectively, to detect angiogenesis in the groups. (Fig. 8a, b) The quantitative results of vWF show that there are statistical differences between week 1 and 4 for all the groups. At 4 weeks, there was a statistical difference between the P + C and P+C+R groups, although it was not a large difference (†p < 0.1). The P+C+R and P+C+R+S groups exhibited the same tendency (†p < 0.1). However, there was a statistical difference between the P + C and P+C+R+S groups (*p < 0.05). α-SMA, which is a factor in smooth muscle cells, had a similar trend as vWF. There were statistical differences between week 1 and week 4 for all of the groups. The level of the angiogenesis factors, vWF and α-SMA, was time dependent and had the highest value in the P+C+R+S group at 4 weeks. (Fig. 8c)

Representative immunofluorescence staining images of ECs and SMCs
We did immunofluorescence staining of CD 90 and CD 105, which are MSC markers, to evaluate the ability to recruit MSCs at 1 and 4 weeks after surgery (Fig. 9). The results show that the tendency of staining for CD90 and CD 105 was increased by time in all groups. In particular, the P+C+R+S group had the most recruited MSCs among the groups at 1 and 4 weeks. At 1 week, the P+C+R+S group had the largest number of stained cells, and a similar tendency was observed at 4 weeks. The P + C group had the smallest number of MSCs compared with the other groups, both at 1 and 4 weeks. The results suggest that the P+C+R+S group was most effective in the regeneration of tissues.

Representative images of MSC recruitment.
We hypothesized that the reason behind the presence of different amounts of collagen between groups was the difference in the amount of recruited cells, and that the amount of recruited cells and degree of angiogenesis were different owing to the amount of remaining SP in each group (Fig. 10). The P+C+R+S group demonstrated presence of the largest amount of SP during the first week; however, this amount was observed to have decreased by the end of week 4. Notably, a statistical difference was observed in the remaining amount of SP in the P+C+R+S group when compared against the P + C and P+C+R groups at the end of week 4 (P+C, 4698.44 ± 1036.49 μm2/mm2; P+C+R, 7890.06 ± 907.60 μm2/mm2; and P+C+R+S, 12929.28 ± 1849.21 μm2/mm2, **p < 0.01). It was determined that SP, which is conjugated to RADA, remained inside the scaffold until week 4.

Immunofluorescence analysis. Representative pictures of each group showing the detection of substance P.
Discussion
Dermal substitutes have to meet several conditions to heal injuries and to form new tissues as follows: (i) repair the anatomy and functions of the skin, (ii) be biocompatible, (iii) be able to infiltrate cells, and (iv) have the proper mechanical properties.41,42 The 3D PLCL, which was fabricated using indirect 3D printing, could mimic the acute anatomy of the injury site of a patient. In addition, it was observed to be biocompatible and biodegradable as well as possess a porous structure and good mechanical properties. To enhance cell affinity, the RADA16 hydrogel, which mimics the ECM in 3D structured PLCLs, was employed. Especially, SP coupled with RADA16 was used for long-term delivery of SP during tissue formation. 29 We believe that the occurrence of angiogenesis and recruitment of MSCs occurred owing to the presence of SP, and this could be effectively employed as a dermis substitute during dermis regeneration.
First, we determined that the PLCL scaffold has a porous structure with the SEM images. The distribution of the pore size was from 150 to 400 μm, and its porosity was 86.59% ± 1.96%. Lee et al. reported that a pore size distribution of approximately 210–500 μm was more effective in the proliferation of HDFs compared to a pore size range that was not dispersed. 43 The PLCL scaffold has a suitable pore size range for dermis regeneration because it enhances the cell affinity. PLCL exhibits elastic properties due to the phase separation of the PLA and PCL segments, which build the hard domain and soft domain, respectively; thus, it has been used in various engineered tissues, including vascular, tendon, cartilage, and skin.44,45 After the fabrication of the PLCL scaffold, the recovery test showed that it maintained its elastic property.
An in vivo test was performed in immunodeficient mice subcutaneously up to 4 weeks using three test groups. First, we observed the compressive modulus of each group after explantation. The increase in compressive modulus was observed to be time dependent. This is because the transplanted and recruited cells secrete ECM in the scaffold and fill pores of the scaffold during tissue formation. The P + C group demonstrated the lowest compressive modulus when compared to the P+C+R and P+C+R+S groups. We observed that the RADA hydrogel positively affects tissue formation by providing a 3D environment. SAPs are known to create a 3D environment that mimics the native ECM and contains much water, more than 99%. 46 However, the compressive modulus ratio of the P+C+R and P+C+R+S groups compared with the P + C group at 4 weeks was decreased more than at 1 week. We believe that the reason for the decrease in the modulus ratio, which was higher in the P+C+R and P+C+R+S groups compared with the P + C group, is the degradation of the RADA hydrogel.
Histological analysis of samples from the in vivo test suggested the formation of tissues, which were observed visually. The P + C group showed no tissue formation at 1 week. However, the P+C+R+S group showed that new tissue was formed as well as new blood vessels at 1 week. There were more new tissues and blood vessels formed at 4 weeks than at 1 week in the P+C+R+S group. We believe the reason for these results is because of the SP, which affects angiogenesis and new tissue formation. Moreover, MT staining showed newly deposited collagen in the scaffold. Similar with the H&E staining, there was little collagen present in the scaffold at 1 week for all the groups. However, at 4 weeks, the outcome changed with considerable collagen observed in the P+C+R and P+C+R+S groups. Thus, next, we did a quantitative analysis of collagen formed in the groups.
We measured the quantity of the total soluble collagen deposited in the samples from in vivo study. The P+C+R+S group at 4 weeks had the highest value for total soluble collagen among the groups. This outcome suggested that the P+C+R+S group is the most effective for the synthesis of collagen, which is one of the main components of the ECM. 14 Similar with this result, immunofluorescence staining showed that the P+C+R+S group at 4 weeks had the most type I and type III collagen. Human skin has various types of collagens, especially type I and type III collagen in the dermis. These collagens are the main component in soft tissue.47,48 Therefore, the P+C+R+S group is the most effective group for collagen synthesis and deposited ECM, especially type I collagen and type III collagen, which are found in the dermis and soft tissue.
Angiogenesis is critical in the regenerative medicine field. One of the abilities of stem cells is angiogenesis. 16 Our results had statistically different values for angiogenesis formation among the groups. In particular, the P+C+R+S group showed enhanced angiogenesis formation in the scaffold compared with the other groups. The P+C+R+S group contained the RADA hydrogel immobilized with SP. Thus, we suggest that SP positively affects angiogenesis because it has the ability to recruit MSCs to an injury site.
MSCs are known to enhance cell proliferation, regeneration of damaged tissue, and angiogenesis. 49 SP has the ability to recruit MSCs to an injury site, which subsequently leads to tissue regeneration and angiogenesis at the injury site. In this study, MSCs were recruited to the scaffold that contained SP. This SP-induced MSC recruitment could explain the differences in collagen and angiogenesis among the groups. Interestingly, the P+C+R+S group had more recruited MSCs at 1 week than at 4 weeks. MSCs have reported some limitations such as a low engraftment and survival in an injury site. 50 In this study, we could solve this problem by recruiting MSCs to injured sites. We believe the reason for the difference in recruited MSCs among the groups is the SP. We demonstrated that SP is sustained within the scaffold for up to 4 weeks (Fig. 10). Moreover, SP, which was covalently bonded with the RADA hydrogel, was released gradually over time; thus, its effect was to recruit MSCs to the scaffold. However, the amount of SP remaining within the scaffold at week 4 decreased compared to that at week 1. This result suggests that the RADA hydrogel was degraded, so that SP was released. 21 Notably, SP was also observed to be present within the P + C and P+C+R groups, although only in small amounts. This could be explained on the basis of several reports reporting the presence of SP in the nervous system of mice, rats, cats, and humans. 51
Biomaterials used in this study include a biodegradable polymer called PLCL and peptide hydrogel called RADA/RADA-SP. PLCL is hydrolyzed and eventually degrades within the body. The peptide hydrogel is also degradable within the body and gets absorbed in the form of amino acids. In the case of PLCL, the degradation rate is slower compared to other polyesters, such as poly(lactide-co-glycolide), as demonstrated by experimental results. For this reason, no occurrences of inflammatory reaction caused by lactic acid in PLCL are observed. Peptide hydrogel is also developed by synthesis, and since the final product is an amino acid, it can also be considered free from inflammatory reactions.52,53
In this study, customized elastic scaffolds were developed by combining 3D printing and gel-pressing methods. Scaffolds fabricated using this method were observed to possess mechanical properties similar to native soft tissues as well as enhance tissue regeneration. We believe such scaffolds could be used as substitutes for damaged portions of the skin. To mimic the total skin structure, we propose to introduce a direct 3D printing technology and produce a hierarchical structure as part of our next work. In addition, to employ the scaffolds/hydrogel/cell constructs developed in this study in clinical applications, it is necessary to perform repeated validation of the results obtained in this study using various cell populations and scaffolds.
Conclusions
In this study, we successfully fabricated a customized PLCL scaffold with indirect 3D printing. It is expected that this scaffold can act as a dermis substitute. To mimic the native ECM, RADA hydrogel, which is a SAP, was used in the 3D structured PLCL. Moreover, SP was covalently immobilized to the RADA to promote angiogenesis and the recruitment of MSCs to improve tissue regeneration. In conclusion, the 3D structured PLCL scaffold with RADA-SP promoted angiogenesis, recruitment of MSCs, and tissue regeneration.
Footnotes
Acknowledgments
This work was supported by a grant of Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (2016R1A2B2009550)
Disclosure Statement
No competing financial interests exist.