
Abstract
The regeneration of cartilage is challenging due to its low metabolic rate and avascular nature. An effective treatment for osteochondral defects remains a clinical challenge. Glycosaminoglycans such as heparan sulfate (HS) bind and enhance the activity of prochondrogenic growth factors and thus hold potential for targeted tissue regeneration without the requirement for exogenous growth factors. In this study, we examine the use of a cell- and growth factor-free HS-based technique for osteochondral repair in a rabbit model. The binding affinity between HS and several reparative proteins (TGF-β1, BMP-2, FGF-2, PDGF-BB, and VEGF165) was studied using surface plasmon resonance. Next, an HS-impregnated gel was implanted in a large osteochondral defect in the femoral trochlea of 19 New Zealand white rabbits to study the efficacy of the treatment. Over a 12-week period, HS showed significantly enhanced subchondral bone regeneration compared with a hydrogel control. Treatment with HS also resulted in an increased presence of hyaline cartilage in the chondral region. The use of HS in osteochondral defects appears to improve both subchondral and chondral tissue repair. Our data suggest that this effect is mediated by the ability of HS to promote endogenous growth factors.
Impact Statement
Repairing damaged joint cartilage remains a significant challenge. Treatment involving microfracture, tissue grafting, or cell therapy provides some benefit, but seldom regenerates lost articular cartilage. Providing a point-of-care solution that is cell and tissue free has the potential to transform orthopedic treatment for such cases. Glycosaminoglycans such as heparan sulfate (HS) are well suited for this purpose because they provide a matrix that enhances the prochondrogenic activities of growth factors normally found at sites of articular damage. In this study, we show the potential of a novel HS device, which is free of exogenous cells or growth factors, in regenerating osteochondral defects.
Introduction
A
To address the issue, exogenous growth factors are often administered at supraphysiological doses to maintain an adequate threshold at the treatment site. 8 Such approaches face significant barriers to clinical translation, as supraphysiological doses of growth factors are frequently associated with undesirable outcomes that include immune reaction, 9 synovial inflammation,10,11 and postoperative complications. 12 Separate to the dosing problem, there is also the need to localize the growth factor(s) to the injury site to prevent it from triggering systemic side effects, such as fibrosis and oncogenesis.13–15 Strategies have been developed to control the release of morphogens, either through a sustained release or a lowered starting dose.16,17 However, challenges remain in the successful delivery of growth factors in an orderly and continuous manner.8,18
In response to these challenges, new strategies are being developed to reduce or obviate the need for exogenous growth factors. Indeed, growth factors such as VEGF and TGF-β1 are naturally present in synovial fluid and serum19–22 and might be sufficient to drive endogenous mesenchymal stem cell (MSC) differentiation 23 if their instability can be addressed. In response, an alternate strategy that enhances the activity of local, endogenously produced growth factors at the defect site is beginning to show promise.
Our group has demonstrated the efficacious use of heparan sulfate (HS) for tissue regeneration in a number of injury models.24,25 HS is a highly sulfated, linear polysaccharide that constitutes one of the major components of the ECM. The ability of HS to bind, stabilize, and potentiate a range of biologically relevant reparative proteins makes it well suited as a biomaterial for tissue regeneration.26,27 Previous studies have shown that administration of HS variants at injury sites can promote both bone healing 28 and angiogenesis 29 without the use of exogenous growth factors. Therefore, we hypothesize that the application of HS to osteochondral defects may help to bind, stabilize, and amplify the activity of endogenous reparative factors and enhance osteochondral repair. In this study, we show that HS binds multiple prochondrogenic and osteogenic growth factors and, when complexed with a commercially available hyaluronic acid gel, is able to enhance the repair of large osteochondral defect model in rabbits in a single-step, point-of-care procedure, which can be readily translated to the clinic.
Materials and Methods
Surface plasmon resonance competitive binding assay
Interactions among TGF-β1 (Peprotech), BMP-2, FGF-2, PDGF-BB, VEGF165 (R&D Systems), and porcine mucosal heparan sulfate (HSPM; Celsus lot No. HO-10697) were measured using surface plasmon resonance (SPR)-based competitive binding assays, as previously described. 30 In brief, 20 mg heparin (H3149; Sigma-Aldrich) was biotinylated at free-amine groups using NHS-biotin (8.6 μM) in dimethyl sulfoxide and excess unreacted biotin removed using a 7 kDa spin column (Zeba spin; Thermo-Fisher). Heparin–biotin was immobilized on a sensor chip SA (GE Healthcare) in HBS-EP 0.05% buffer (150 mM NaCl, 10 mM HEPES, 3 mM EDTA, 0.05% [v/v] Tween-20, and pH 7.4) using the default immobilization program on a Biacore T100 until the desired 40 response units were achieved. Optimal protein concentrations for competitive inhibition experiments were determined by injecting the various proteins at a range of concentrations across the heparin-derivatized surface as previously reported.29–31 The final concentrations used for each protein were as follows: TGF-β1—200 nM, BMP-2—25 nM, FGF-2—8 nM, VEGF165—1.56 nM, and PDGF-BB—50 nM.
For competitive binding assays, proteins were preincubated with 10 μg (83.3 μg/mL) HSPM in HBS-EP 0.1% buffer before being applied to the heparin-derivatized surface at a flow rate of 30 μL/min for 2 min, followed by a 10 min dissociation period. The chip was then regenerated with two 1-min injections of 2M NaCl in HBS-EP 0.1% buffer. The response was measured as a function of time at 25°C. All data were normalized to the maximum response generated by protein alone (100% bound to chip), after which percentage of protein bound to HSPM in solution was determined by subtracting the normalized response for each protein plus HSPM from protein alone (% protein on chip [protein+HSPM] minus the % protein on the chip [protein alone]. Data constitute mean ± standard deviation (SD) of three independent experiments.
Animal study design
Nineteen male New Zealand white rabbits were used for this study. All animals were healthy with an average age of 9 ± 1 months and body weight 3.9 ± 0.2 kg before the study. Bilateral osteochondral defects were surgically created in the femoral trochlear groove. Of the 38 defects created, 19 were assigned to the current study and the remainder to a parallel study to reduce the number of animals. This practice of “reduction” is in strict alignment with the three Rs (3Rs) that are guiding principles for the ethical use of animals in research. Of the 19 defects, 9 were treated with a hyaluronic acid hydrogel alone (AuxiGel™; Termira AB, Stockholm, Sweden), and 10 were treated with the same hydrogel containing HSPM. The two treatment groups were randomly assigned among all rabbits. Each defect received either 60 μL of the hydrogel (Gel) alone or 60 μL of hydrogel containing 10 μg of HSPM (Gel+HSPM).
Defect creation and gel implantation
The research protocol used for this study was approved by the Institutional Animal Care and Use Committee, Agency for Science, Technology and Research (A*STAR, Singapore, Singapore), and followed all appropriate guidelines (IACUC No. 130833). All surgical procedures were carried out aseptically under general anesthesia, consisting of a combination of ketamine (35 mg/kg) and xylazine (5 mg/kg) injections and 2% isoflurane inspiration. A skin incision was made along the anterior midline from the proximal end of the patellar to the tibial tuberosity. The knee was opened by an anteromedial para-patellar passway. The femoral trochlear groove was then exposed by shifting the patella laterally, and a single osteochondral defect (4 mm in diameter, ≈1 mm in depth) created. Microfractures (0.8 mm diameter, 2 mm depth) were made in three different places within each defect to form an inscribed triangular pattern. Treatments were given by filling the defect with Gel alone or Gel+HSPM. In brief, 36 μL component A (hyaluronic acid solution) and 24 μL component B (PVA cross-linker solution) were mixed and allowed to set for ∼5 min before being implanted into the defect site. For the Gel+HSPM group, 10 μg of HSPM dissolved in 1 μL phosphate-buffered saline was added during the gelation. On-site checking was done immediately after repositioning the patella following 15 joint flexions and extensions to ensure the implant remained in the defect. Prophylactic antibiotics (Enrofloxacin, 10 mg/kg) and analgesics (Buprenorphine, 0.1 mg/kg) were administered subcutaneously for 5 days postsurgery. All rabbits were allowed to move freely in their cages and received a normal diet. At 12 weeks postsurgery, all rabbits were euthanized by lethal dose of sodium pentobarbital, and the distal end of the femurs harvested for gross evaluation, magnetic resonance imaging (MRI), and histological and immunohistochemistry (IHC) analyses.
Gross pathology observation of cartilage repair
The International Cartilage Research Society (ICRS) Visual Assessment Scale (ICRS I) was used for evaluating macroscopic parameters of cartilage repair 32 that included the degree of defect repair, integration to the border zone, and macroscopic appearance. The assessment was made by trained staff unaware of the treatment groups.
Magnetic resonance observation of cartilage repair tissue
MRI data collection was done in an ultra-high-field 9.4T MRI scanner (Bruker Biospin GmbH, Ettlingen, Germany). A turbo spin echo sequence was used with echo time: 6 ms, repetition time: 1200 ms, number of averages: 2, and spatial resolution 117 × 117 × 500 μm. Magnetic resonance observation of cartilage repair tissue (MOCART) scoring33,34 was used for evaluating the cartilage repair in nine parameters—degree of defect repair/filling, integration to border zone, surface, structure, and signal intensity of the repair tissue, subchondral lamina, subchondral bone, adhesions, and synovitis. The assessment was made by a trained staff blinded to the treatment groups.
Histology analyses
After ICRS I scoring and MRI, harvested distal ends of the femurs were fixed in 10% (v/v) neutral-buffered formalin for 1 week under vacuum and decalcified in 5% (v/v) formic acid for 1 week at room temperature. The trimmed specimens were then embedded in paraffin wax and sectioned (5 μm) horizontally from the middle of the defect. Sections were deparaffinized and stained with Masson's trichrome, Alcian blue (pH 1, counterstained with neutral red), and Safranin-O as previously reported. 35
IHC analyses
IHC staining was carried using a Leica Bond™-III Autostainer (Leica Nussloch GmbH) and a Bond Refine Detection Kit (Leica Nussloch GmbH). Sections were deparaffinized with Bond Dewax Solution (Leica Nussloch GmbH) and antigen retrieval carried out by incubating with Proteinase K (20 μg/mL; Sigma-Aldrich) for 15 min at room temperature. Endogenous peroxidase activity was blocked by incubating with 3–4% (v/v) H2O2 for 15 min. Sections were then blocked with 10% (v/v) goat serum for 30 min before incubation with primary antibody (Collagen Type I [1:1000]; Novus Biologicals and Collagen Type II [1:2000]; and Acris Antibodies, Inc.) diluted in Bond Primary Antibody Diluent (Leica Nussloch GmbH) for 30 min at room temperature. Detection of stain was performed as described in the Bond Refine Detection Kit, and nuclei were counterstained with hematoxylin. All washes were performed with 1 × Bond Wash Solution (Leica Nussloch GmbH).
Histological scoring
ICRS II scoring was used to evaluate tissue filling and neotissue phenotype. 36 Qualitative analysis of the neotissue was based on cell morphology and ECM content. Hyaline cartilage was characterized by the presence of rounded cells in lacunae that express glycosaminoglycan (GAG) and Type II collagen. Fibrocartilage was defined by cells that produce GAG and Type I collagen. Hybrid cartilage exhibits positive staining for both of the Type I and Type II collagen and GAG, while fibrous tissue is positive for Type I collagen alone. Analysis of the percentage of tissue filling was performed using a grid superimposed over the tissue slide. Assessment was made by a trained staff blinded to the treatment groups.
Statistical analysis methods
Values are expressed as mean ± SD. MOCART variables, ICRS I, and ICRS II parameters were analyzed using the multiple t-test function (one unpaired t-test per variable) in GraphPad Prism 7.03 software. Differences in repair cartilage phenotype and tissue filling percentages were determined using a one-way analysis of variance using Tukey's test. Statistical significance was set at p-value <0.05.
Results
HSPM binds growth factors with varying affinity
To assess the growth factor-binding affinity of HSPM, various proteins that are important for wound repair (TGF-β1, VEGF165, BMP-2, PDGF-BB, and FGF-2) were combined with HSPM and the complex applied to a heparin-coated sensor chip. Protein:HSPM complex formation was indicated by a reduction in the amount of protein binding to the heparin-coated chip surface. A greater reduction in binding suggested that the protein has a higher affinity for HSPM. Because proteins produce variable responses due to variations in binding affinity, 37 different concentrations of each protein were used. Once optimized, each protein was incubated with 10 μg HSPM (83.3 μg/mL) and the complex applied to the sensor chip. Reduced protein binding to the senor chip was observed for all proteins when combined with HSPM (Fig. 1A–E). When normalized to protein alone (no complexation with HSPM), the relative level of protein sequestered into solution versus control was determined (Fig. 1F). HSPM showed varying affinities toward TGF-β1, VEGF165, BMP-2, PDGF-BB, and FGF-2.

Binding of growth factors important to wound healing. Growth factors
HSPM improves the macro- and microscopic healing of rabbit osteochondral defects
All animals survived until the end point, and no adverse events were seen. All the 19 retrieved samples were evaluated macroscopically using ICRS I scoring and were imaged by MRI, but 2 samples were not included for MOCART scoring due to poor positioning of the samples. Post-MRI, one sample in the Gel group was damaged during histological processing and removed from the study. The remaining samples were processed for ICRS II scoring. Scattergrams of data from microscopic evaluations highlighted that one sample in the Gel+HSPM group (ID# Y781L-R) was probably a biological outlier (data not shown). Therefore, a Grubbs' outlier test, 38 with an alpha level set at 0.05, was used to assess the data set (GraphPad Prism, version 7.03; GraphPad Software, San Diego, CA). Examination of the histological sections on this particular sample suggested there were problems during sectioning, and therefore the data point was removed. Therefore, 19 samples were used for ICRS I scoring, 17 samples for MOCART scoring, and 17 samples for ICRS II scoring and additional histomorphometry. Detailed animal usage data are listed in Supplementary Table S1.
The harvested explants were photographed using a Nikon digital camera D3300 and representative images showing the best, and the worst performers of the healed defects from the two groups are presented in Figure 2A. Gross morphological evaluation showed that surfaces of defects treated with Gel+HSPM had a higher degree of integration with surrounding host cartilage and were more intact and smoother in appearance (Fig. 2A). In contrast, scattered fissures and poor tissue healing was more evident for defects treated with Gel. Despite the variation between the best and the worst performers within each group, treatment with Gel+HSPM scored higher in all of the ICRS I parameters, while also having the least coefficient of variation (CV) in treatment outcomes (Fig. 2B). Treatment with Gel+HSPM resulted in an average ICRS I score of 10.40 ± 2.07 and median score of 11 compared with defects treated with Gel that averaged 9.11 ± 2.42 and had a median score of 8 (Fig. 2C). Moreover, treatment with Gel+HSPM resulted in cartilage of “normal” appearance (ICRS I score = 12, Grade I) in 40% (4 out of 10) of defects, compared with 22% (2 out of 9) in the Gel group. A similar result was observed for cartilage of “normal or nearly normal” appearance (score ≥8, Grade II and above) in 78% of Gel-treated defects (7 out of 9) compared with 90% in Gel+HSPM-treated defects (9 out of 10). The difference is, however, not statistically significant (p = 0.23).
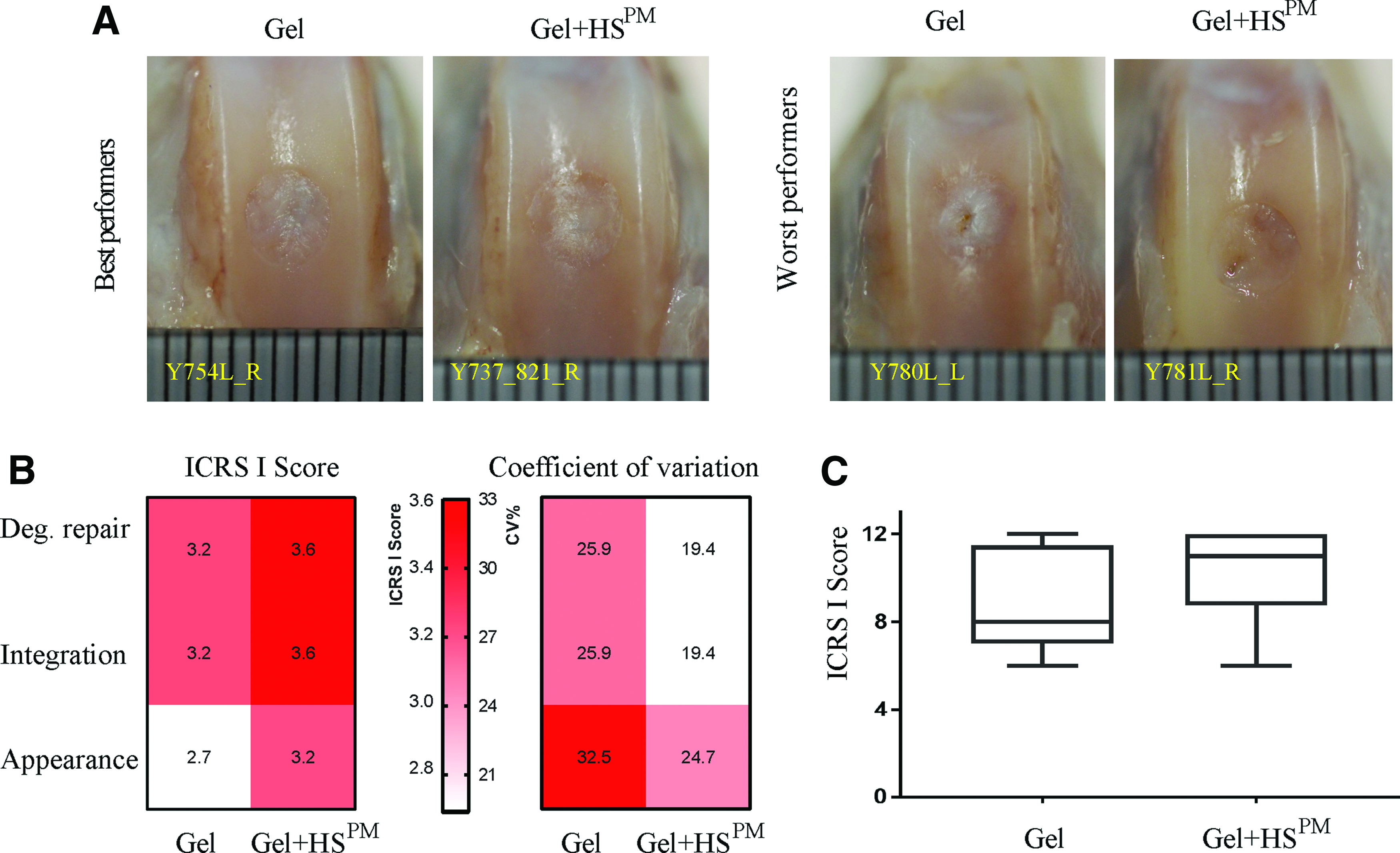
ICRS I Scores 12 weeks posttreatment.
MOCART scoring using MRI images (Fig. 3A) showed that the repair tissue in defects treated with HSPM had higher scores in all nine parameters (Fig. 3B, C). Specifically, HSPM treatment significantly improved the intactness of the surface of repair tissue (p = 0.016) and subchondral bone (p = 0.048) as well as the signal intensity of the repair tissue (p = 0.0342) (Fig. 3B). As a result, the overall MOCART score was significantly higher for treatment with Gel+HSPM (12.25 ± 1.91) compared with Gel alone (8.78 ± 3.15), suggesting a more complete and homogeneous restoration of repair tissue in defects treated with Gel+HSPM (p = 0.0165) (Fig. 3B, C).

MRI and MOCART scores.
Decalcified sections were stained with Masson's Trichrome, Safranin-O, Alcian blue, or immunostained for the presence of Type I and Type II collagen (Fig. 4). Most of the cartilage formed was hybrid cartilage, characterized by the expression of GAG and both Type I and Type II collagen (Fig. 4). When defects were treated with Gel+HSPM, an abundance of bone filling the defect to the level of the tidemark in the uninjured host tissue was observed in most of the samples. This was not observed in the Gel-alone-treated defects; instead, Safranin O-positive staining was observed below the height of the host tidemark, indicating on-going endochondral bone formation (or remnant hyaluronic acid gel) in the subchondral region. Overall, this suggests inadequate growth of subchondral bone when Gel+HSPM was omitted (Fig. 5A, B). In Gel-alone-treated defects, we observed cartilage deposited on regenerated subchondral bone, but the cells in the chondral layer were unordered and had an elongated, spindle-shaped morphology (Fig. 5C). In contrast, defects treated with Gel+HSPM contained cells with a clear chondrocyte-like morphology that were oval shaped and stacked within well-organized lacuna in the regenerated chondral layer (Fig. 5D). The ICRS II scores also reflected this difference, with Gel+HSPM-treated defects scoring higher than Gel-treated defects in all 13 parameters (Fig. 6A), with significantly higher scores for cell morphology (p = 0.0415) and subchondral bone regeneration (p = 0.0159) compared with Gel (Fig. 6B). Also, Gel+HSPM treatment produced more consistent ICRS II scores (a lower CV) for all parameters (Fig. 6A), indicating a more reliable outcome. The overall ICRS II assessment (Fig. 6C) showed significantly higher scores for the Gel+HSPM (89.15 ± 6.03) group compared with the Gel group (78.26 ± 8.46), suggesting that the use of HSPM leads to better repair outcomes in osteochondral defects (p = 0.0075).
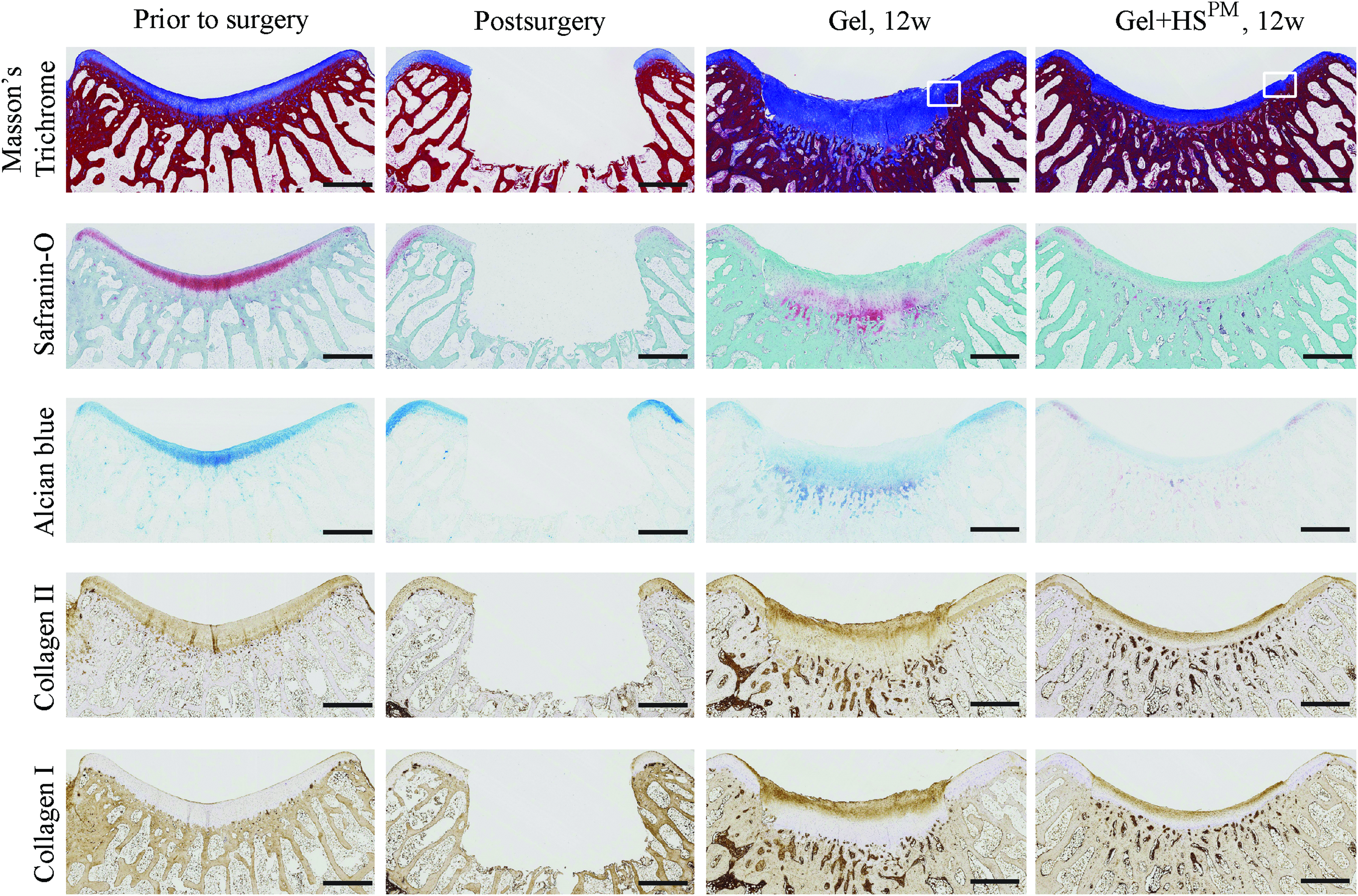
Representative histology of a normal trochlea before surgery (left column), the defect postsurgery (second column), and 12 weeks posttreatment with Gel (animal ID: BLK516L-R) or Gel+HSPM (animal ID: BLK785L_L; N = 17). Sections were stained with Masson's Trichrome to detect collagen (blue), cell cytoplasm (red) and nuclei (black), and Safranin-O and Alcian blue to detect GAGs (red and blue, respectively). Immunohistochemistry was used to assess the distribution of Collagen type I and II. Scale bar: 1 mm. Boxed areas in Masson's trichrome-stained images are shown at a higher magnification in Figure 5A and B. GAGs, glycosaminoglycans. Color images are available online.

Representative histology at the margins of defects.
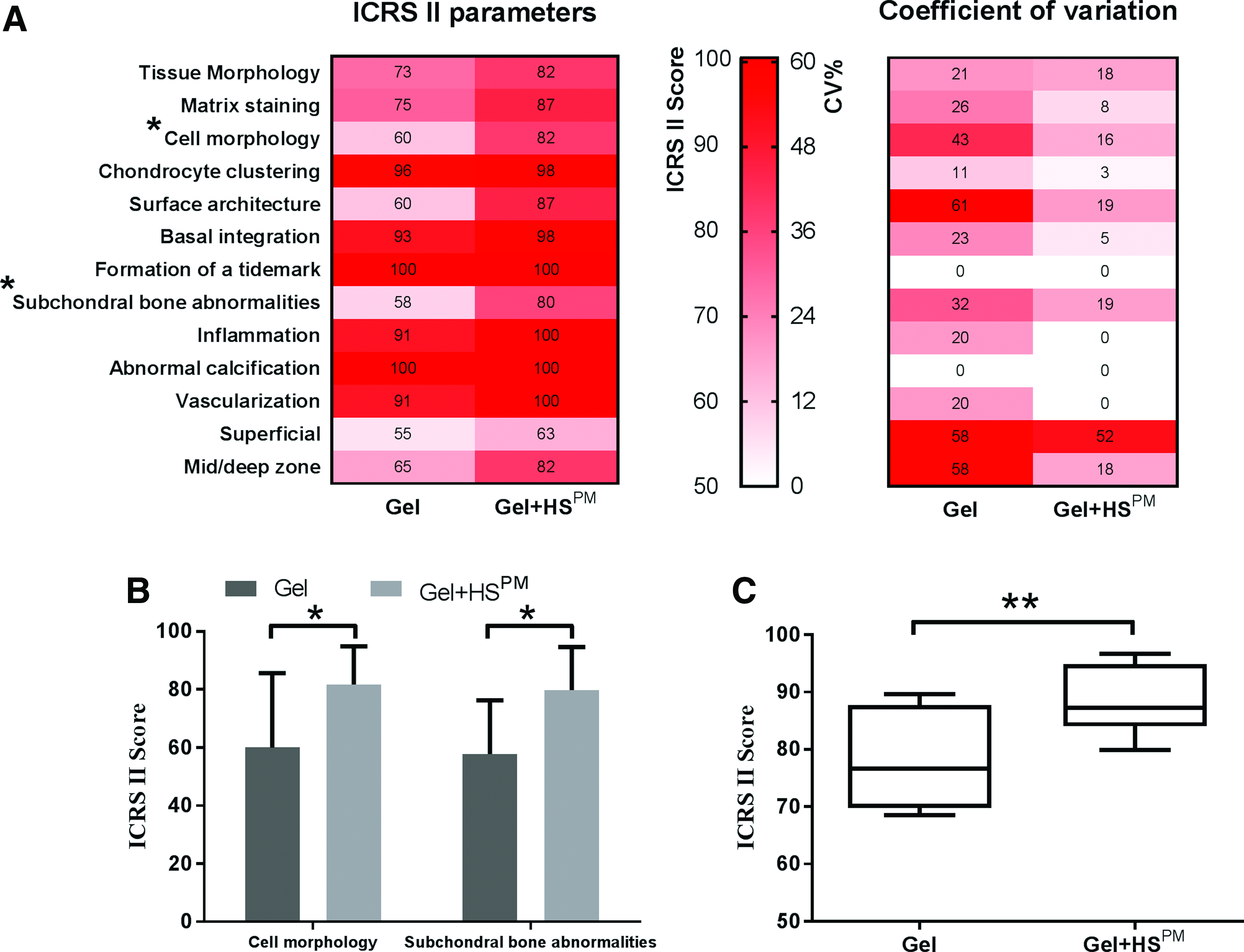
ICRS II Scores 12 weeks posttreatment (N = 17).
Further analysis of the amount of tissue filling the defect (total tissue filling %) showed no significant difference between the two treatments (p = 0.09), irrespective of the tissue layer (Fig. 7A). However, rather than simply assessing the amount of tissue, it is more important to determine the relative amounts of bone tissue in the subchondral layer (Fig. 7B) and cartilage in the chondral layer (Fig. 7C). The data show that when defects were treated with Gel+HSPM, significantly more bone tissue filled the subchondral layer (79.77% ± 4.94%, p = 0.0393) compared with the Gel group (61.19% ± 6.75%) (Fig. 7B). However, the amount of newly formed cartilage in the chondral region was similar for both treatments (87.50% ± 35.36% for Gel versus 85.71% ± 33.50% for Gel+HSPM) (Fig. 7C). The data also show that most of the cartilage formed was hybrid cartilage, with no fibrocartilage being observed (Fig. 7D). Interestingly, hyaline cartilage was observed in two out of nine (22%) Gel+HSPM-treated defects, but not in any Gel-treated defects (Fig. 7D).
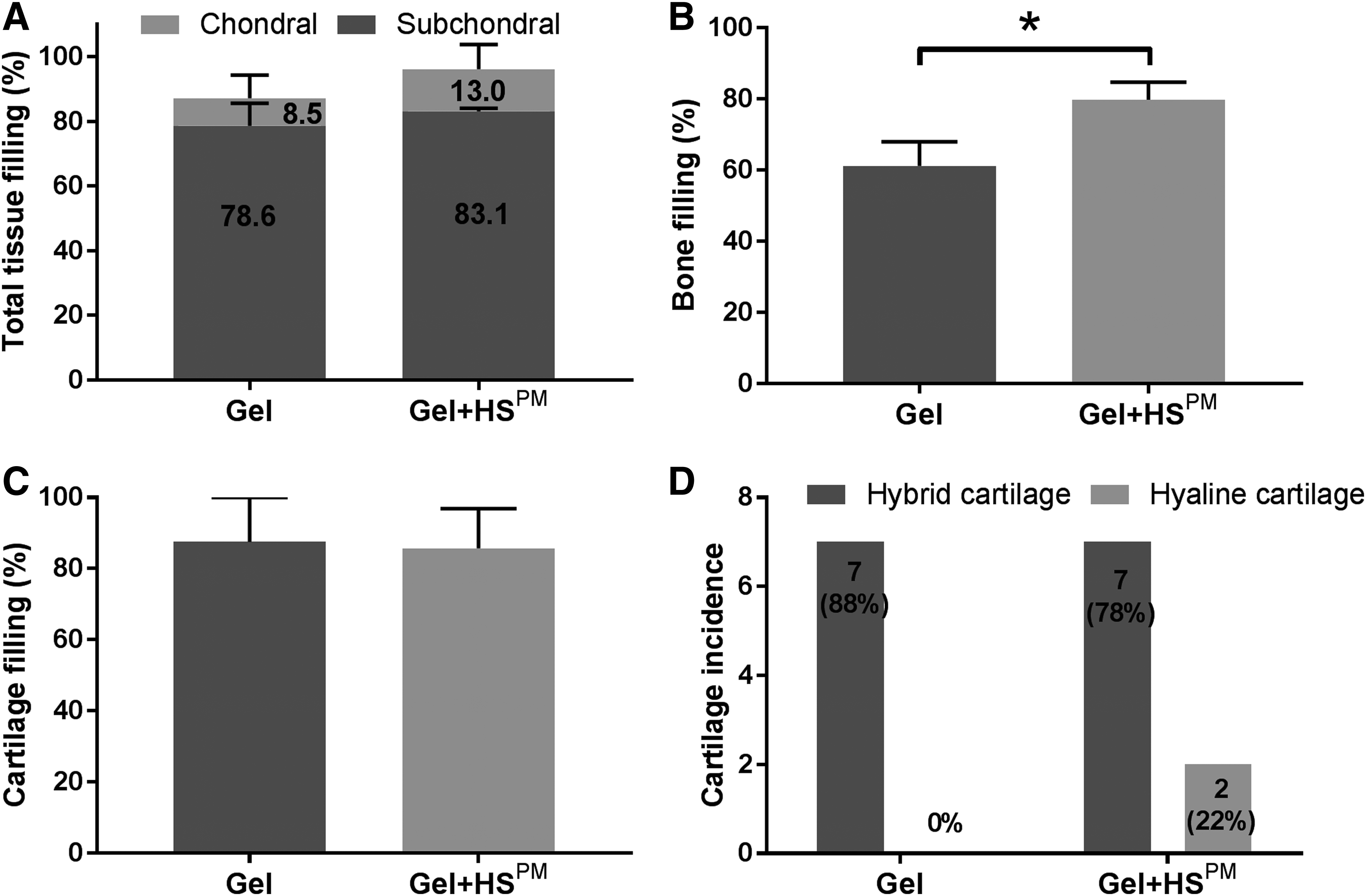
Tissue filling regenerated osteochondral defects 12 weeks posttreatment (N = 17).
Discussion
Autologous chondrocyte implantation for the treatment of large, full-thickness osteochondral defects is gaining clinical momentum.39–43 However, significant donor site morbidity and a high percentage of fibrocartilage at the repair site continue to plague its therapeutic efficacy. 44 As an alternate strategy, we chose to examine a cell-free matrix that does not require surgical harvesting of donor tissue, which therefore provides a point-of-care treatment option for patients. Key to this strategy is the development of an implantable device with the ability to integrate with the host and fully restore the structure and function of the lost tissue. GAGs such as HS are well-suited for this purpose because they provide a matrix that enhances the prochondrogenic activities of endogenous growth factors found at sites of articular damage. In this study, we evaluated the ability of an HS-impregnated gel to repair large osteochondral defects in the femoral trochlea of rabbits over a 12-week period.
The use of SPR enables an assessment of the interactions between two components, such as HS and a HS-binding protein, in a label-free system. In the context of cartilage repair, SPR allows HS to be screened for binding against many proregenerative HS-binding proteins, with higher binding representing higher affinity toward a protein. When HS displays a high affinity or ability to bind large quantities of proregenerative proteins in SPR assays, it is likely that this HS can retain and stabilize these factors within a wound site or defect, enhancing the endogenous healing response. Using SPR-based analytics, we show here that high-affinity complexes are formed between the rich mixture that is HSPM and many notably reparative proteins such as TGF-β1, BMP-2, FGF-2, PDGF-BB, and VEGF165. We observed considerable binding variability that highlights the heterogeneity of HS—while some HS chains may contain an enrichment of binding sites for one protein, they may lack binding sites for others. Despite the varied affinity profile, this study showed that HSPM was able to bind the pro-osteogenic factor BMP-2 45 as well as the prochondrogenic factor TGF-β1. 46 Also notable was the binding of HSPM to the progenitor mitogen FGF-2 47 as well as the provascular factors VEGF16548,49 and PDGF-BB. 50 This mixed binding profile is important because the repair of osteochondral injuries involve the restoration of both subchondral bone and the overlying cartilage, together with blood vessels and other tissues at the repair site. Although HSPM containing scaffolds were not preloaded with protein growth factors, the addition of HSPM may bind endogenous growth factors, 51 enhancing the biological signals that help to mediate the repair cascade.52,53
We have previously shown that HS stimulates the proliferation of MSCs in an FGF-2-dependent manner54–56 and that heparin/HS preparations enhance TGF-β1-induced SMAD2/3 signaling, an important initiator of the chondrogenic signaling cascade. 30 We have also shown that affinity-selected HS prolongs BMP-2-mediated SMAD1/5/8 signaling 28 and osteogenic differentiation, as well as the formation of VEGF165-mediated vascular networks. 29 This suggests that HS-containing scaffolds may favor the proliferation and differentiation of stem cells toward those desired cellular responses needed for osteochondral repair, thus highlighting the potential of HS preparations as reparative agents in a rabbit femoral trochlear grove defect model.
In our animal study, osteochondral defects treated with Gel+HSPM showed higher MOCART and ICRS I scores compared to the Gel alone group, indicating improved filling of the defects and integration with surrounding host tissue. MRI analyses showed more intact surface and subchondral bone in defects treated with Gel+HSPM. The majority of defects treated with Gel+HSPM (90%) had a surface morphology that appeared normal or nearly normal (ICRS I scores ≥8, Grade II and above) compared with those treated with Gel alone (78%). Detailed histological assessment using ICRS II scoring indicated abundant new subchondral bone reaching the level of the tidemark in adjacent host bone was formed following Gel+HSPM treatment, but not with Gel alone. The reduced amount of new bone formation may be due to less absorption of the HA gel, or insufficient calcification of newly formed ECM in the absence of HSPM. Importantly, regenerated hyaline cartilage in the chondral layer was only observed following treatment with Gel+HSPM. Although hybrid cartilage was found in nearly all defects, more oval-shaped chondrocytes were observed with Gel+HSPM treatment. Such improvement in the cartilage layer following treatment with Gel+HSPM can be attributed to enhanced subchondral bone regeneration because articular cartilage growth relies on a sufficiency of subchondral bone for mechanical support and nutrition.57,58 Furthermore, there is growing evidence that biochemical and molecular crosstalk occurs between cells in cartilage and subchondral bone.59,60 It is plausible that HSPM helps to mediate the interdependence between the two compartments by stabilizing and enhancing the actions of reparative factors at the injury site. 61 Also, by virtue of its anti-inflammatory qualities,62,63 HS may help swing the balance in favor of regeneration rather than degeneration that typically dominates this type of injury. Future efforts will focus on improving the quality rather than the amount of repaired tissue, including the restoration of aggrecan levels and the mechanical properties of the repaired cartilage tissue.
In the present study, the biodistribution of HSPM and the presence of augmented growth factor(s) were not assessed. Therefore, the observed HSPM-enhanced tissue regeneration may have resulted from an improved microenvironment during the early stages of wound healing, or through medium/long-term changes in the available pool of reparative factors and cells. Also, the biological variation in the animal study 64 and the numbers of animals used may have an impact on the outcome. Also, clinical variation is common in medical practice and may cause unexpected results. 65 In assessing such variability, we noted that the Gel+HSPM treatment group not only promoted tissue repair but also reduced the CV for all 3 parameters of the ICRS I score and all 14 parameters of the ICRS II scoring system. It is therefore possible that improved outcomes with HSPM had a major contribution toward reducing the variable healing responses between animals, a finding that has important implications for future clinical studies.
Our results highlight that the restoration of subchondral bone is an important pillar for cartilage regeneration. Moreover, full restoration of osteochondral defects demands a multiphasic engineering approach. A variety of biphasic scaffolds mimicking the structure of osteochondral tissues have been studied in the presence or absence of exogenous growth factors. 66 Future investigations focusing on biphasic scaffolds loaded with HS variants to manipulate the biodistribution of endogenous growth factors are needed to further fine-tune osteochondral responses. The data presented here emphasize the considerable therapeutic potential of medical devices containing HS at articular sites, warranting their further development as biomaterials that support tissue restoration.
Conclusion
We have shown that HSPM materials can enhance osteochondral tissue regeneration, possibly by helping to orchestrate the activities of endogenous growth factors and cells, highlighting their therapeutic value in harnessing endogenous repair cascades. We believe that the development of such an HS-based strategy for osteochondral repair may spare the need for exogenous applications of growth factors or cell transplantation.
Footnotes
Acknowledgments
The authors acknowledge the funding support of Singapore's Agency for Science, Technology and Research (A*STAR) and Institute of Medical Biology (IMB). Funding was also provided by the National Medical Research Council (NMRC), Singapore (No. CIRG16may052).
Authors' Contributions
V.N., J.H.H., and S.M.C. obtained the funding. J.H.L., V.N., J.H.H., K.S., and S.M.C. designed the study. J.H.L. and R.A.A.S. performed the in vitro studies. J.H.L., X.R., and T.C.T. conducted the surgeries. J.H.L., X.L., X.R., T.C.T., R.A.A.S., K.S., S.S., K.B., and S.M.C. analyzed and interpreted the data. J.H.L., R.A.A.S., and X.L. assembled the data and drafted the article. All authors revised the article and gave final approval of the article.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.