
Abstract
Current vascular replacement grafts used in congenital heart defect corrective surgery have poor longevity and growth potential. Recipient patients often require multiple reoperations. Tissue engineering has the promise to produce a graft with the potential to grow, remodel, and repair. In this study, we aimed at developing an amnion-based scaffold suitable for cardiovascular tissue engineering applications and in vivo usage. The developed human amnion-based scaffold was made by an enzymatic decellularization process followed by freeze-drying as a single or multilayered structure. These structures were compared to native amnion for seeded cell viability and biomechanical properties then tested for in vivo biocompatibility. Our results demonstrated that while native amnion tissue supported little cell growth, the decellularized-amnion allowed cell engraftment and survival. In addition, preservation of the scaffold by freeze-drying as a single layer allowed cell engraftment and growth. Multilayering the freeze-dried amnion scaffolds resulted in a similar cell growth potential of the single layered construct but superior mechanical strength. The multilayered construct showed in vitro biocompatibility with endothelial cells, smooth muscle cells, cardiac myocytes, and thymus and cord blood-derived mesenchymal stem cells (MSCs). When implanted in a piglet model of left pulmonary artery grafting, the multilayered construct showed its in vivo suitability and biocompatibility for vascular repair as demonstrated by the development of newly formed endothelium in the intima, a smooth muscle cell-rich medial layer and an adventitia containing new vasa vasorum. In conclusion, our developed amnion-derived scaffold represents an off-the-shelf biocompatible structure that can be seeded with the patient's own MSCs to produce an autologous vascular graft.
Impact Statement
This study aimed at developing an amnion-based scaffold suitable for vascular tissue engineering applications and in vivo usage. We successfully produced a multilayered scaffold with improved biomechanical properties and biocompatibility for in vivo vascular implantation. Our approach not only offers an allogeneic “off-the-shelf” solution for clinical use but also it provides the possibility of personalized medicine using a patient's own amnion and stem cells for the production of tissue engineered grafts for reconstructive heart surgery.
Introduction
C
Tissue engineering offers an alternative source of implants by combining a biofunctional scaffold with allogeneic or autologous stem cells. An ideal scaffold would be nonimmunogenic, nonthrombotic, and biocompatible and have growth and remodeling potential. 6 This scaffold should also have a durable extracellular matrix that can survive in vivo blood pressures.
Human amniotic membrane (AM) offers a potential scaffold as it is an easily obtainable biologic material that has been used for over a century in skin repair and burn treatment.7,8 Later, it was used for conjunctival repair. 9 It has been tested in animal models for urethra repair, ocular surface reconstruction, liver repair, and pericardial closure.10–13 In human patients, it has been used for lower eyelid repair, fistula closures, and neovagina construction.14–16 In addition, it has been shown that amnion has anti-inflammatory and antimicrobial properties.17–21
Biofunctional extracellular matrix is critical in a scaffold for it to be effective in tissue engineering. Studies have demonstrated that the amnion's extracellular matrix is primarily composed of collagen, which is conducive to wound healing, as well as fibronectin, proteoglycans, laminins, and glycosamnioglycans.17,22,23 Although in most studies the amnion has been used without much modification other than dehydration, several investigations have decellularized it beforehand using a range of approaches, including freeze-thawing,24,25 EDTA, 26 and trypsin-EDTA treatment.12,13 The latter method retained structural matrix proteins such as collagen type I and IV, fibronectin, and laminin.12,27
Many studies have demonstrated successful seeding of decellularized amnion scaffolds with differentiated cells such as human dermal fibroblasts, 28 human corneal fibroblasts, 25 and smooth muscle cells. 24 Fewer investigations have been carried out to recellularize amnion with stem cells, an approach that could be more promising for tissue engineering purposes.
Long-term amnion preservation is essential for tissue engineering. While matrix preservation was not considered or attempted in many studies,24–26 the beneficial effects of preservation were demonstrated by others. 28 Reported preservation work utilized different methods, including dehydration,13,28 refrigeration, or freezing. 12 The latter approach resulted in ice crystal formation, contamination, or extracellular matrix protein damage.
In addition to scaffolds, cells represent the second component needed for tissue engineering. Mesenchymal stem cells (MSCs) have been isolated from multiple sources such as bone marrow and adipose tissue. 29 Critically for congenital heart defect repair, MSCs have also been isolated from cord blood and thymus tissue.30–32 MSCs are promising for seeding onto scaffolds as part of a tissue engineered construct for cardiac repair because of their multilineage differentiation potential, ability to regulate the immune response, and because they do not cause teratomas.33–35
In this study, we combined a decellularization and freeze-drying approach to produce an amnion based scaffold suitable for tissue engineering constructs destined for reconstructive heart surgery application. Our data showed in vitro and in vivo biocompatibility of the developed amnion-based construct and its suitability for use in pulmonary artery position. Our developed preserved construct offers an “off-the-shelf” solution for allogeneic clinical use. Furthermore, it represents a key component for personalized medicine, which is possible using a patient's own amnion and stem cells for the construction of a tissue engineered graft.
Materials and Methods
Ethics
Human tissue was collected from patients in compliance with the Human Tissue Act. Perinatal and leftover material (the thymus, cord blood, and placenta) were obtained with parents' consent under NHS ethics license (REC ref. 06/Q2001/197 and 11/SW/0122).
Amnion preparation
Amnion was collected from 25 human cesarean sections. AM was removed from the fetal side of the placenta by blunt dissection. It was washed once in PBS and then repeatedly with water. It was then stored overnight at 4°C in PBS.
Amnion decellularization
AM was decellularized in six-well crown inserts (Scaffdex). Crowns were placed in 0.1% trypsin in 10 mM Tris (Sigma) buffer pH 8.0 and incubated for 3 h at 37°C under gentle rotation. The solution was changed to 500 U/mL DNase (Sigma) in 10 mM Tris buffer and incubated for an additional 3 h at 37°C under gentle rotation. Decellularized-AM (d-AM) was then washed in 10 mM Tris buffer every day for 5–9 days at 37°C under gentle rotation.
Tissue preservation
AM and d-AM were preserved in single or multiple layers by removing from crowns and freezing at −20°C. For freezing, excess liquid was removed, and samples were laid completely flat. Multilayer samples were stacked, cross-sectionally, on top of each other, and all air bubbles were removed. They were then freeze-dried (fd; Edwards) and stored at room temperature. These single (d-AM-fd-single) and multilayered (d-AM-fd-multi) constructs were rehydrated in respective cell culture mediums prior in vitro testing.
Thymus-derived MSCs
Thymus tissue was collected from patients undergoing congenital heart surgery and placed in sterile PBS from the surgical theatre. The thymus was washed in PBS (Life Technologies), minced into small pieces, and underwent a 2 h collagenase I (Sigma-Aldrich; 0.3 mg/mL) enzymatic digestion. The digested tissue was forced through a strainer and was washed with fresh medium. The resulting cell suspension was centrifuged for 5 min at 420 g at 22°C. The supernatant was discarded, and cells were resuspended in Dulbecco's modified Eagle's medium, low glucose (DMEM; Life Technologies) with 10% HyClone Fetal Bovine Serum (FBS; Thermo Scientific) and 1% penicillin/streptomycin (P/S; Life Technologies) on uncoated plastic, at approximately 1 × 10 6 cells/cm 2 density in a 37°C humidified atmosphere with 5% CO2.
After 72–96 h, nonadherent cells were removed with two PBS washes. Adherent cells were cultured until confluence was reached, with feeding every 48–72 h. At this point, cells were detached using Trypsin-EDTA (0.05%; Life Technologies) and then plated at approximately 1 × 10 4 cells/cm 2 in new flasks for next passage (P1).
Umbilical cord blood MSCs
Human umbilical cord blood (hUCB) was collected in 1% heparin (Leo Pharma) from consenting patients undergoing cesarean section. Blood was diluted 1:2 with P/S PBS and layered onto Ficoll (GE Health care). Tubes were centrifuged at 400 g at room temperature for 30 min with no brake. Mononuclear cells were removed with a 10 mL syringe and washed thrice with P/S PBS. Finally, they were spun at 420 g for 5 min, and the supernatant was discarded. Cells were plated at approximately 1 × 10 6 cells/cm 2 on uncoated plastic and cultured in 95% air, 5% CO2, and 37°C. Nonadherent cells were removed by washing with PBS after 72–96 h. Adherent cells were cultured with DMEM, 10% FBS, 1% P/S with media changes every 48–72 h.
Human umbilical vein endothelial cells
Human umbilical vein endothelial cells (hUVECs) were purchased from Lonza. They were cultured on uncoated plastic in 95% air, 5% CO2, and 37°C in Endothelial Cell Growth Medium (PromoCell), with media changes every 48–72 h.
Cardiac myocytes
Cardiac Myocytes were purchased from PromoCell. They were cultured on uncoated plastic in 95% air, 5% CO2, and 37°C in Cardiac Myocyte Growth Medium (PromoCell) according to manufacturer's instructions.
Arterial smooth muscle cells
Smooth muscle cells were collected from the artery of the umbilical cord. Cord was cut open, arteries were removed and cleaned in PBS, and chopped into pieces. Artery pieces were then cultured in DMEM, 10% FBS, 1% P/S in 95% air, 5% CO2, and 37°C. Smooth muscle cells were outgrown from these arterial pieces in 10 cm petri dishes.
AM cell seeding
AM, d-AM, d-AM-fd-single, and d-AM-fd-multi were sterilized under 295 nm UV for 30 min on each side. They were then seeded with each cell type at 250,000 cells/cm 2 in respective culture mediums. Cell-seeded AM was cultured for 1 week at 37°C in a humidified atmosphere with 5% CO2 with medium changes every 2–3 days. Apart from hUVECs and cardiac myocytes (commercially sourced), a different cell line, prepared from a different sample, was used for each experimental point.
Cell viability
To test cell viability on scaffolds, the Live/Dead Viability/Cytotoxicity Kit, for mammalian cells (ThermoFisher), was used according to manufacturer's instructions with Hoechst (ThermoFisher; 1 ng/mL) in PBS. Samples were imaged on a Zeiss Axio Observer Z1 with Zen Blue software (Zeiss). Cell counts were performed using ImageJ.
Immunohistochemistry
For tissue analysis, samples were embedded in paraffin. First, they were fixed in 4% paraformaldehyde (PFA), washed in PBS, moved in to cassettes (Histosette I, Simport), processed in a Thermo Excelsior AS, and embedded in a Thermo HistoStar machine. Sections were cut on a microtome (Thermo) at 5 μm, floated onto Menzel-Glaser SuperFrost Plus slides (Thermo), and dried overnight. Hematoxylin and eosin (H&E) and van Gieson's (EVG) stains were performed using a Shandon Varistain 24-4 (Thermo). Slides were removed from machine and mounted with DPX (distyrene, a plasticizer, in toluene–xylene; Sigma). Slides were imaged on a Zeiss Axio Observer Z1 with Zen Blue software (Zeiss).
For immunofluorescence analysis, samples were deparaffinized in clearene and rehydrated through an alcohol gradient. Antigen retrieval was performed with 10 mM citrate buffer pH 6.0 heated to boil. Ten percent goat serum (Sigma-Aldrich) in PBS was used to block the samples for 30 min at room temperature. Samples were incubated with the primary antibodies overnight at 4°C. Antibody solutions were prepared as follows: 1:100 Isolectin-B4-biotin (Life Technologies), 1:200 mouse to alpha-smooth muscle actin (Abcam), 1:100 mouse to smooth muscle-myosin heavy chain (Dako), and 1:100 rabbit to calponin (Dako).
Secondary antibodies were then incubated on the sections for 1 h at room temperature in the dark. The secondary antibodies used were as follows: 1:200 streptavidin-Alexa Flour 488 (Life Technologies), 1:300 goat-anti-mouse-Cy3 (Jackson Immuno Research Labs), 1:400 goat-anti-mouse-Alexa Flour 488 (Abcam), and 1:400 goat-anti-rabbit-Alexa Flour 546 (Abcam). Dapi was used to counterstain the nuclei, and the slides were mounted using HardSet mounting medium (VECTASHIELD).
Scanning electron microscopy
Tissue samples were prepared by fixing in 2.5% glutaraldehyde in sodium cacodylate buffer (Electron Microscopy Sciences) for 45 min. Following fixation, samples were washed thrice in 0.1 M sodium cacodylate buffer (from Cacodylate acid, Sigma). Osmium (Electron Microscopy Sciences) solution was prepared with 1% osmium in 0.1 M sodium cacodylate buffer and put on samples for 20 min.
Samples were washed and dehydrated as follows: three changes of 0.1 M sodium cacodylate; one each of water; 25%, 50%, 70%, 80%, 90%, 96% ethanol; and 3 three changes of 100% ethanol with each step of 10 min at room temperature. Samples were dried completely in the critical point dryer (Leica EM CPD300) and mounted on stubs (Agar Scientific) with 12 mm carbon tabs (Agar Scientific). They were then coated at 100 mA for 30 s using an EMITECH K575X sputter coater. Surface details were imaged using a Quanta 200 FEI field emission scanning electron microscope.
Mechanical testing
Samples were analyzed for mechanical properties with pneumatic grips and a 100 N load cell on an Instron 3343B machine. Crosshead speed was 10 mm/min. Samples were measured for tensile stress at break and Young's Modulus using Bluehill software (Instron).
In vivo implantation of the multilayered decellularized freeze-dried amnion
Two 3-week-old female Landrace pigs of 10–15 kg were used in this study. No mortality was recorded. Animals were treated in accordance with the “Guide for the Care and Use of Laboratory Animals” published by the National Institutes of Health in 1996 and conforming to the “Animals (Scientific Procedures) Act” published in 1986.
Surgical procedures were performed under general anesthesia and neuromuscular blockade (Pancuronium Bromide; 2 mg/mL). Anesthesia was induced by intramuscular injection of 15 mg/kg Ketamine, 0.4 mg/kg Midazolam, and 5 mg/kg Dexmedetomidine and then maintained with inhalation of 1–2% Isoflurane. A left posterolateral thoracotomy was performed, and patches of different multilayered freeze-dried amnions were inserted in the Left Pulmonary Arteries (LPAs). Both animals were successfully recovered from the surgical procedures and intensively monitored for 24 h.
Analgesic and antibiotics were administered according to the needs. A combination of 10 mg/kg Paracetamol, 0.2 mg/kg Morphine, 20 mg/kg Cefuroxime, and 0.4 mg/kg Meloxicam was regularly administered intravenously during this period. The animals were monitored with a two-dimensional Doppler Echocardiography (VividQ; GE Healthcare) prior the surgery, immediately after the surgery, and after 2.5 months to assess the LPA patency and blood flow at the level of the patch. After 2.5 months of follow-up, pigs were euthanized with an intravenous injection of 150 mg/kg Euthatal. The pulmonary arteries were dissected from the heart and then fixed in 4% PFA or fresh-frozen in liquid nitrogen.
Statistical tests
Statistical testing was carried out with t-test or one-way ANOVA with Tukey post hoc testing as appropriate, using R. A value of p < 0.05 was considered statistically significant.
Results
Amnion dissection and composition
Human placenta was collected, dissected, and cleaned to isolate the control AM (Fig. 1a). The native epithelial cell layer had a cobblestone-like morphology, which was observed on the surface of the amnion using scanning electron microscopy (Fig. 1b). Histological characterization was performed using H&E and EVG staining. H&E showed a single layer of epithelial cells on the surface of the membrane (Fig. 1c), while EVG indicated a collagen matrix (Fig. 1d).

MSCs seeded on native human amnion do not survive on the nonviable epithelial cell layer.
The surface of the control nonprocessed amnion does not allow survival and growth of seeded MSCs
Thymus-derived MSCs were isolated and seeded on the surface of the AM. Cell viability staining demonstrated the lack of viable cells (green Calcein fluorescence). Numerous nuclei were observed on the surface; however, all were positive for Ethidium III (red) indicating cell death of the amnion's epithelial cells, as well as seeded cells. There was no observed positive calcein (green) staining for viable seeded cells, showing that MSCs did not survive on the matrix, due to either the lack of adherence because of the presence of residual epithelial cells or perhaps the presence of factors released by the dying native AM cells that triggered MSC death (Fig. 1e).
The scanning electron micrographs still showed a similar cobblestone-like morphology, but the epithelial cells appeared damaged; smooth elongated MSCs were not observed (Fig. 1f). H&E cross-sections of AM-seeded grafts illustrated the epithelial cells on the surface of the AM but no additional cells (Fig. 1g). Collagens were intact as shown by EVG (Fig. 1h). In summary, the seeded MSCs did not adhere or survive on the surface of the AM. The latter only showed dead epithelial cells on the surface.
Trypsin decellularization completely removed epithelial cells and allowed for MSC adherence and survival
Trypsin decellularized amnion (d-AM) was stained with viability stain and H&E to verify removal of cellular components (Fig. 2a). No nuclear stain was detected. Furthermore, the epithelial cells were no longer visible on the surface of the matrix confirming successful decellularization with no visible cells or cell fragments (Fig. 2a). EVG demonstrated no disruption to the matrix following treatment; the collagens were preserved (Fig. 2a). Extracellular matrix fibers made up the surface of the matrix, as visualized by scanning electron micrographs (Fig. 2a).
MSCs seeded on the surface of the decellularized matrix were viable (Fig. 2a). The elongated structure of the cells indicated the survival of the MSCs. Nuclei were observed on the surface of cross-section H&E, although in small numbers (Fig. 2a). EVG showed an intact collagen matrix although with a small amount of loose collagen that could potentially be made by seeded cells (Fig. 2a). Surface micrographs illustrate elongated MSCs on the surface of the d-AM, with a few extracellular matrix fibers still visible between the cells (Fig. 2a).
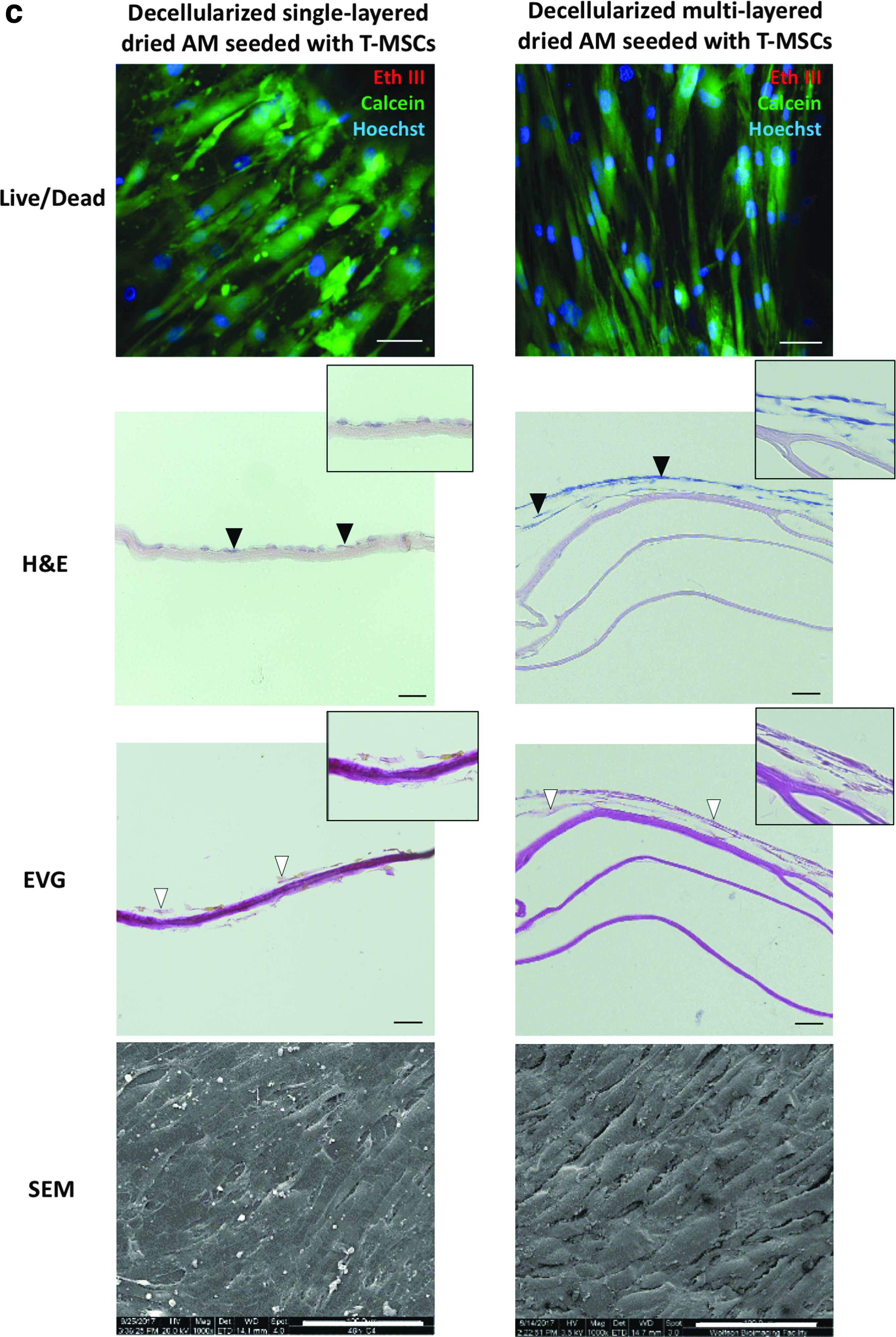
Preservation of the Amnion as a single and multilayered structure resulted in better growth of seeded cells
For long-term preservation of the matrix, the d-AM was freeze-dried as a single or a multilayer. Single layer decellularized freeze-dried amnion (d-AM-fd-single) and multilayer decellularized freeze-dried amnion (d-AM-fd-multi) produced a paper-like structure (Fig. 2b, respectively). H&E staining illustrated no residual cellular material in d-AM-fd-single (Fig. 2b), while EVG demonstrated that the collagens became more compact (Fig. 2b). The compact collagen fibers of the extracellular matrix are visible in the scanning electron micrograph (Fig. 2b).
Cell survival was then tested on the d-AM-fd-single seeded with MSCs. After 7 days in culture, viability staining showed elongated viable MSCs (Fig. 2c). This layer of cells is also seen in the cross-section of the H&E (Fig. 2c). Loose collagens are shown in the EVG (Fig. 2c). The scanning electron micrographs show confluent MSC layer on the surface of the preserved matrix (Fig. 2c).
For improving the ease of handling and strength, the material was then layered (d-AM-fd-multi) (Fig. 2b). The d-AM-fd-multi had no residual nuclear material, as shown by H&E (Fig. 2b). EVG showed that the collagens were undamaged but again became far more compact (Fig. 2b). Surface morphology indicated extracellular matrix fibers much the same as after decellularization (Fig. 2b). These results indicate that the matrix could be preserved and handled by layering and freeze-drying.
d-AM-fd-multi was then tested for seeded cell survival. Cell viability indicated extensive cell population after 1 week in culture (Fig. 2c). This was further confirmed by H&E staining which showed two to three cell layers on the surface of the d-AM-fd-multi (Fig. 2c). The EVG demonstrated loose collagen above the compact layers of amnion suggesting that this collagen could be newly made by the seeded cells (Fig. 2c). The cells on the surface in the scanning electron micrographs were compact and extracellular matrix fibers were no longer visible (Fig. 2c). The cell population growth on the freeze-dried matrices (d-AM-fd-single, d-AM-fd-multi) was as good (if not slightly better in case of d-AM-fd-multi) as growth on wet decellularized amnion (d-AM) that was not freeze-dried.
Quantification of cell survival on the surface of the decellularized amnion
Control amnion was freeze-dried (AM-fd) and rehydrated to be directly comparable to d-AM-fd-single-seeded and d-AM-fd-multiseeded. The cell survival and viability of the MSCs on the surface of the AM-fd were compared to d-AM-fd-single and d-AM-fd-multi (Fig. 3). Cell viability images were counted for the number of green viable cells. Representative AM-fd-seeded (Fig. 3a), d-AM-fd-single seeded (Fig. 3b), and d-AM-fd-multiseeded (Fig. 3c) images show fewer viable cells on the dry-AM-seeded compared to the d-AM-fd-single-seeded and d-AM-fd-multiseeded.
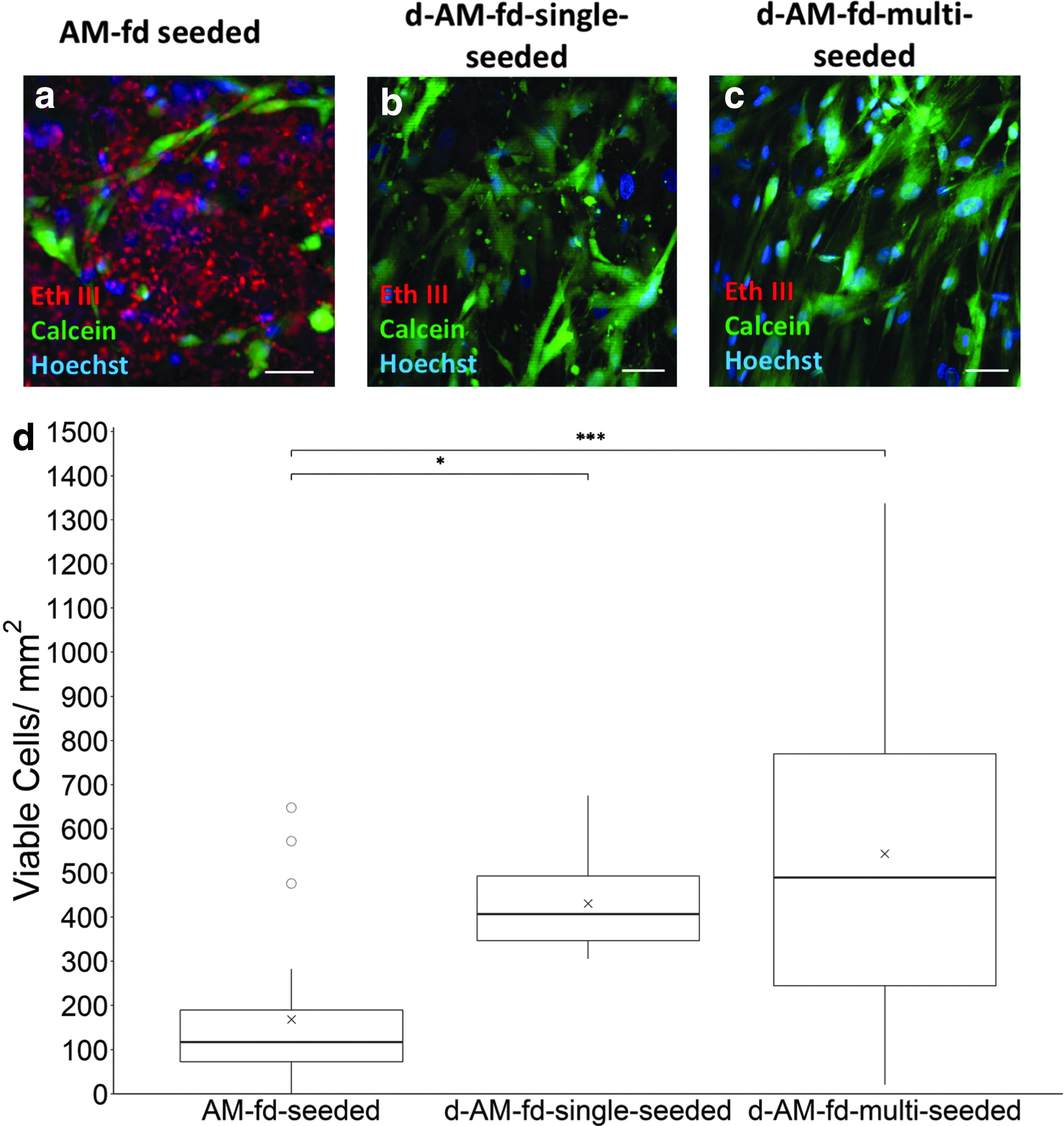
Quantification of improved cell viability on the surface of dried decellularized matrix. Cell viability staining indicated that the dried native amnion
The data demonstrated significantly higher cell viability on the surface of the d-AM-fd-single-seeded (430.7 ± 32.3 cells/mm 2 , n = 3, technical triplicate) and d-AM-fd-multiseeded (543.4 ± 70.5 cells/mm 2 , n = 7, technical triplicate) than on the AM-fd-seeded (168.4 ± 35.8 cells/mm 2 , n = 6, technical quadruplet; p = 0.023 and p < 0.001, respectively, Fig. 3d). There was no significant difference between the d-AM-fd-single and d-AM-fd-multiseeded (p = 0.45, one-way ANOVA, Tukey post hoc testing).
Mechanical strength of the amnion
The ultimate tensile strength (UTS) and Young's Modulus were calculated to determine the strength and elasticity of the different engineered amnion constructs (Fig. 4). Amnion was measured and pulled to break point to determine the UTS (Fig. 4a). The native AM was compared to the d-AM, the d-AM-fd-single, the d-AM-fd-multi, and the d-AM-fd-single and d-AM-fd-multi which had been seeded with MSCs and were in culture for 7 days (d-AM-fd-single-seeded and d-AM-fd-multiseeded). AM (1.94 ± 0.20 MPa), d-AM (1.98 ± 0.27 MPa), d-AM-fd-single (2.47 ± 0.24 MPa), and d-AM-fd-single-seeded (1.17 ± 0.19 MPa) had the lowest UTS with no significant difference in values. The d-AM-fd-multi (7.33 ± 1.15 MPa) and the d-AM-fd-multiseeded (6.49 ± 1.22 MPa) had significantly higher UTS than AM (p < 0.0001; p = 0.004), d-AM (p < 0.0001; p = 0.011), d-AM-fd-single (p < 0.0001; p = 0.021), and d-AM-fd-single-seeded (p < 0.0001; p = 0.0126), respectively. No significant difference in UTS was observed when comparing the unseeded d-AM-fd-multi and d-AM-fd-multiseeded (p = 0.96).
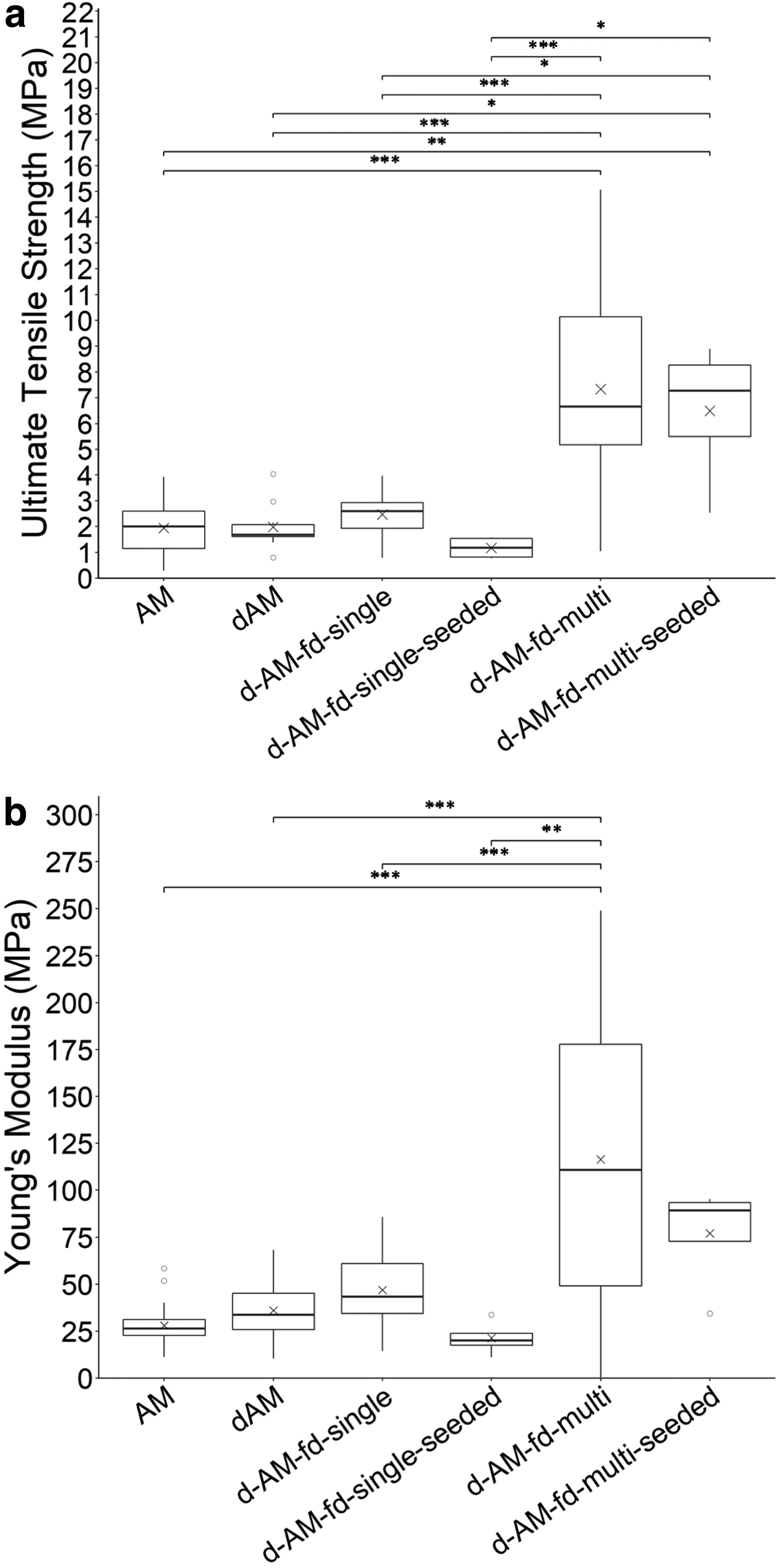
Ultimate tensile strength and Young's Modulus of the amnion. Native (AM, n = 4), decellularized (d-AM, n = 4), single layer decellularized dried and seeded (d-AM-fd-single, n = 4; d-AM-fd-single-seeded, n = 4, respectively), multilayered decellularized dried (d-AM-fd-multi, n = 4), and d-AM-fd-multiseeded (n = 4) cultured for 7 days were compared for ultimate tensile strength and Young's Modulus.
Young's Modulus for the different materials was also calculated (Fig. 4b). The d-AM-fd-multi had the highest Young's Modulus (116.4 ± 22.2 MPa) and was significantly different to Young's Modulus of AM (28.0 ± 2.8; p < 0.0001), d-AM (36.1 ± 5.6; p = 0.00044), d-AM-fd-single (46.9 ± 5.2; p = 0.00077), and d-AM-fd-single-seeded (21.3 ± 4.1; p = 0.0033). There was no significant difference between the d-AM-fd-multi and the d-AM-fd-multiseeded (77.1 ± 14.3), and no other significant differences were noted in the other comparisons. All the tested materials had UTS and Young's modulus values higher than those of native LPA (UTS = 0.46 MPa, Young's modulus = 1.40 MPa).
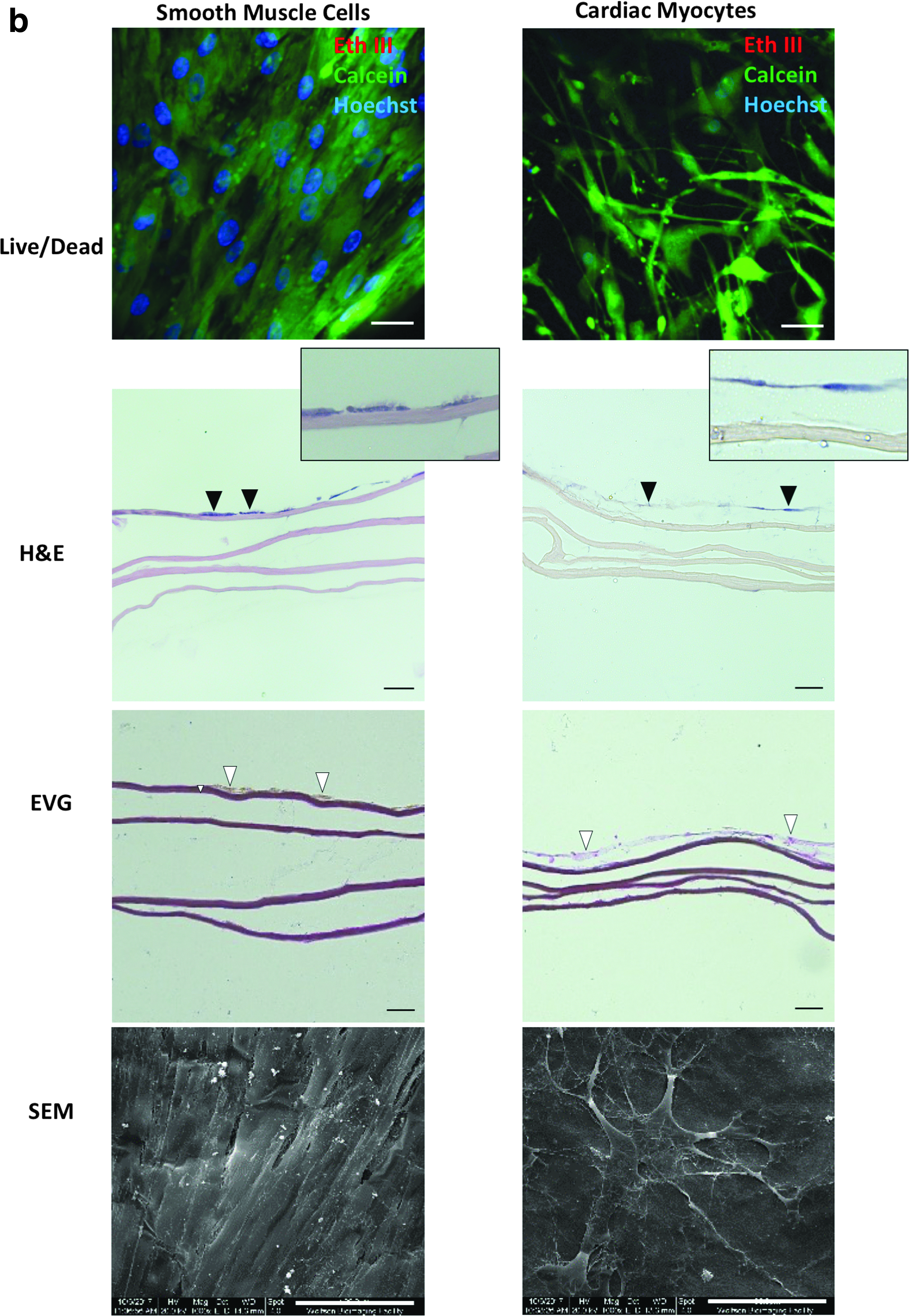
d-AM-fd-multi supports cell survival of other cell types
MSCs isolated from human umbilical cord blood (hUCB-MSCs) represent another population of cells for tissue engineering applied to congenital heart defect corrective surgery. These cells were expanded and seeded on the surface of the d-AM-fd-multi matrix. The hUCB-MSCs survived on the matrix as demonstrated by viability and H&E stainings (Fig. 5a). The seeded cells completely covered the surface of the material as shown by scanning electron microscopy (SEM) (Fig. 5a). hUVECs were also able to survive on the matrix (Fig. 5a) and created a sparse cell layer on the surface of the material as shown by H&E and SEM (Fig. 5a).
d-AM-fd-multi was able to support the cell growth of different cell types suitable for cardiovascular tissue engineering. hUCB-MSCs
Smooth muscle cells offer a potential for vascular tissue engineering. Smooth muscle cells isolated from umbilical artery were seeded on the surface of the d-AM-fd-multi. These smooth muscle cells survived and covered the matrix as shown by live cell staining, H&E, and SEM (Fig. 5b). Cardiac myocytes are another important cell type for congenital heart defect repair. Seeded cardiac myocytes survived and covered the surface of the matrix as shown by live cell staining, H&E, and SEM (Fig. 5b).
Proof-of-concept: d-AM-fd-multi shows in vivo integration and regeneration of vascular tissue
To assess the in vivo biocompatibility of the developed multilayered freeze-dried amnion scaffold, a piglet model of LPA grafting was used (Fig. 6a). A small cut was made in the LPAs of two piglets, and two different d-AM-fd-multi constructs were inserted. Immediately after the surgery (Fig. 6b) and at 2.5 months postoperatively the LPA was patent with no stenosis or rupture (Fig. 6d). Macroscopic inspection of the graft after explantation demonstrated smooth luminal surface with no sign of thrombosis and tissue degradation (Fig. 6c). The blood velocity through the LPA, assessed by Doppler, showed maximum values less than 2.5 m/s indicating normal blood flow. These results were similar to the blood flow through the LPA immediately before surgery (Fig. 6d).
d-AM-fd-multi implanted into the pig model produced a viable graft.
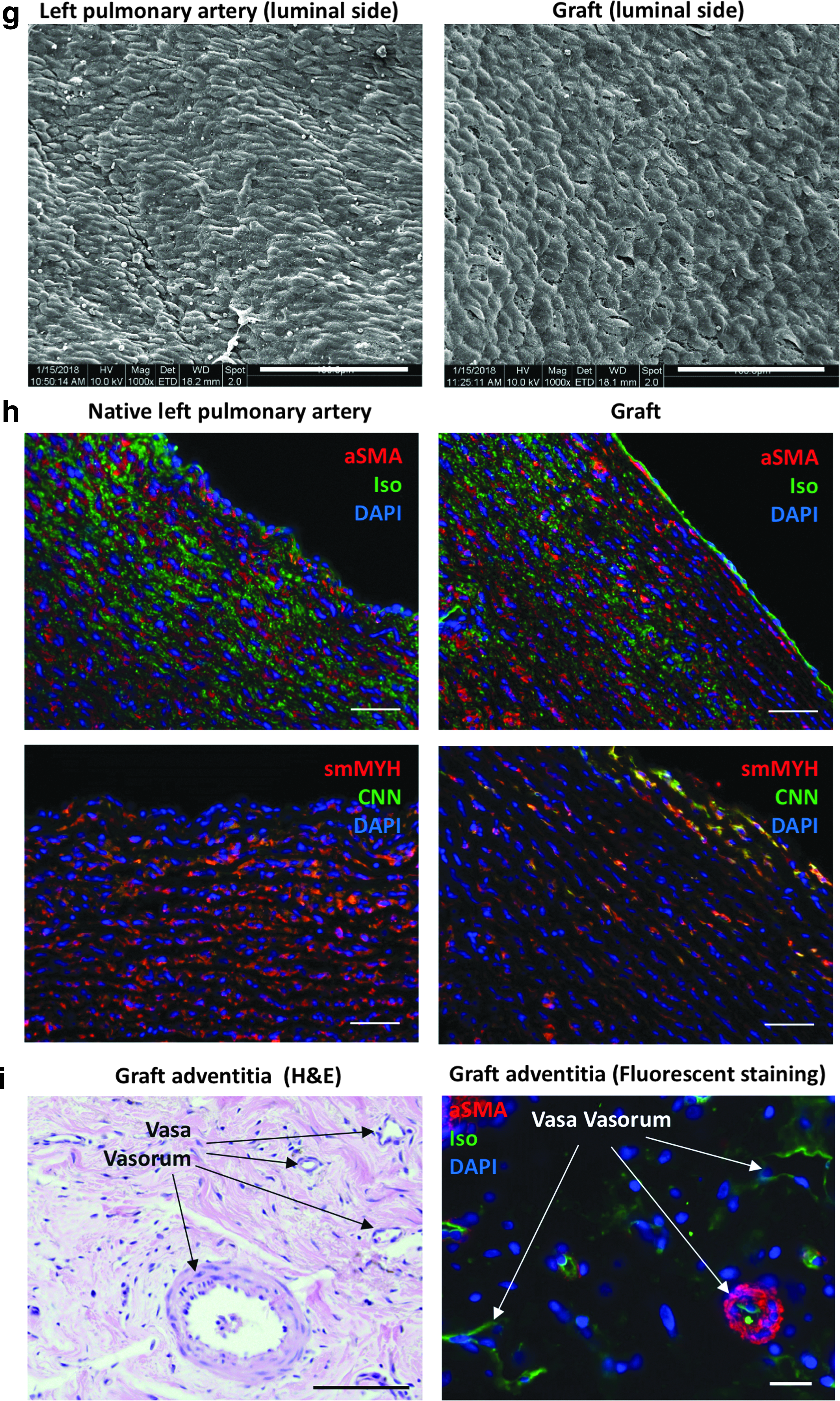
Histological assessment of the graft demonstrated extensive nucleation throughout its structure (Fig. 6e). Graft thickness resembled the neighboring native LPA, although not quite as thick (Fig. 6e). Histological assessment of inflammation in the graft showed no inflammatory cells within the newly formed tissue and away from sutures (Fig. 6f). However inflammatory cells, mainly lymphocytes and granulocytes, were present near the sutures (Fig. 6f). The presence of inflammatory cells near sutures is common following cardiovascular surgery. The inner side of the graft exhibited a newly-formed organized endothelial cell layer as shown by SEM and cross-sections of isolectin staining (Fig. 6g, h,).
The immuohistochemical analysis of graft cross-sections demonstrated an organized multilayer of smooth muscle cells comparable to the native LPA as illustrated by alpha-smooth muscle actin, smooth muscle myosin heavy chain, and calponin staining indicating a vessel-like phenotype (Fig. 6h). Finally, new vessels (vasa vasorum) were observed in the adventitia of the graft indicating neo-vascularization that is crucial for oxygen and nutrient supply to the graft (Fig. 6i). These results provide evidence of the suitability of our amnion-derived construct for in vivo use and particularly for vascular repair application.
Discussion
AM has been used for over a century now. Its use was warranted by its easy and wide availability, as well as its antimicrobial and anti-inflammatory properties. In this study we developed a method that produced an amnion-derived construct that is biocompatible and strong enough for cardiovascular application. Our adopted strategy to decellularize then freeze-dry the AM improved the viability of the seeded cells compared to nonfreeze-dried nondecellularized material and offered a method of preservation and storage that is critical for an “off-the-shelf” clinical product. In addition, layering the decellularized amnion, during the freeze-drying process, created a 4-ply construct with significantly improved tensile strength and elasticity that made it possible to use in preclinical reconstructive heart surgery.
Using our amnion-derived graft as a patch inserted in the LPA of a piglet model demonstrated clear in vivo suitability. The grafted LPA was patent and exhibited normal blood flow up to 2.5 months postoperatively. In addition, the explanted graft displayed a newly formed endothelium in the intima, a smooth muscle cell-rich medial layer, and an adventitia containing new vasa vasorum. Using preserved human amnion with thymus-derived MSCs, a completely autologous graft could be constructed for use in corrective heart surgery for congenital heart defect patients.
The observed limited cell growth on the surface of native amnion led us, like others, 28 to use decellularization as a way to improve cell viability and growth on this material. Our data demonstrated the advantage of decellularization for MSCs' growth on decellularized amnion. Similar results were obtained when seeding differentiated fibroblasts on decellularized and nondecellularized amnion. 28 Another advantage of decellularization of the amnion is to reduce immune response in the recipient if used in an allogeneic manner.
A variety of techniques have been used to decellularize the amnion.15,24,26,28 We optimized a trypsin-EDTA, nuclease decellularization protocol that eliminated cell and nuclear materials from the amnion. While other groups have used their amnion material for body surface repair like foot ulceration repair,36,37 lower eyelid repair, 16 and fistula reconstruction, 15 we have focused on an internal cardiovascular application for our developed amnion based bioscaffold.
For cardiovascular reconstructive surgery, porcine materials have commonly been used for cardiovascular repair because of their wide availability and good mechanical properties. Decellularization is frequently used to remove porcine cells' remains that could trigger an immune response in the human recipient.38,39 When decellularization is incomplete, it can result in rejection, in the recipient patient, due to the galactose-α1-3-galactose (α-gal) epitope present on nonhuman mammalian cells.40,41
The human amnion offers an alternative solution for some applications with the advantage that it doesn't contain the α-gal epitope that could be responsible for triggering the immune response. In addition, using a patient's own autologous tissue could represent a further improved solution as it prevents other potential allogeneic immune response. For these reasons decellularized amnion represents a good alternative to nonhuman tissue-derived scaffolds.
This is the first study, to our knowledge, where the decellularized AM has been prepared by preserving layered tissue, tested for cell seeding to form a tissue engineered construct, and finally tested for biocompatibility, feasibility, and safety in an in vivo vascular repair model. The pig model is an ideal organism for in vivo testing of cardiovascular grafts because of its rapid growth potential and cardiovascular anatomy similar to humans. Preservation of the matrix allows for an “off-the-shelf” solution that can be easily transported and used. It also results in improved cell survival compared to control dehydrated matrix.
Our developed protocol is scalable in a setting where amnion harvest is carried out systematically with a streamlined ethical approval. However, scalability wouldn't be an issue for using the material in an autologous manner where a patient's own amnion and stem cells will be used for producing a tissue engineered graft.
EpiFix is a commercially available dehydrated amnion, equivalent to our control dehydrated matrix. The manufacturer suggests that keeping the AM intact (nondecellularized) would help preserve the cytokines useful for regenerating damaged tissue. 42 In our in vitro system, cell adherence and viability were very poor when MSCs were seeded on nondecellularized amnion. They improved dramatically when MSCs were seeded on decellularized material. These results question the advantage of not decellularizing the AM. Furthermore, our in vivo experiment using decellularized bioscaffold showed infiltration of endothelial cells in the intima and smooth muscle cells in the media of the graft. Cell infiltration is a crucial process for tissue regeneration, and decellularizing the amnion seems to be compatible with this process.
In support of our results, it has been reported that when nondecellularized amnion was applied to ischemic rat hearts, no cell infiltration was observed after 90 days in vivo. 43 Other in vivo work using nondecellularized amnion has shown inflammatory infiltrate.10,20 Decellularization may have removed cytokines from the amnion, but the remaining extracellular matrix seems to sufficiently support cell infiltration and regeneration in vivo. In addition, seeding MSCs on the decellularized amnion should further improve the regenerative capacity of the tissue engineered graft.
Consistent with previous findings, no significant difference in tensile strength was found following decellularization. 44 We showed, as it has previously been demonstrated, that the collagens and extracellular matrix proteins in the extracellular matrix are not damaged by the decellularization process. 27 The strength of the amnion was not compromised when decellularized or after drying for preservation. Furthermore, its tensile strength improved significantly when it was dried and layered. This strength was important for in vivo implantation in a vessel position. After 2.5 months, the preserved amnion-derived graft was still intact and able to withstand the in vivo blood pressure. Furthermore, it integrated well within the surrounding LPA tissue and displayed a typical vessel-like structure composed of intima, media, and adventitia. Other natural materials, such as decellularized carotid arteries and small intestine submucosa extracellular matrix, have shown similar results. When seeded and implanted in vivo, the grafts displayed an inner luminal layer, a medial smooth muscle layer, and some adventitia.32,45 Similar results were obtained using synthetic scaffolds seeded with bone marrow mononuclear cells. 46
Babies born with heart defects usually need surgery within the first 6 months of life, and using reconstructive materials with growth and remodeling capacity would reduce the number of surgeries the child has to endure. The growth potential of our developed construct remains to be tested in further investigations. However, our proof-of-concept in vivo study demonstrates a remodeling potential for this material. While the nonantimicrobial and anti-inflammatory properties17,18 of our amnion-based construct warrant potential allogeneic use, these properties could be further improved by potentially using the patient's own amnion collected at birth (autologous use).
In conclusion, we successfully produced a multilayered scaffold with biomechanical properties and biocompatibility suitable for in vivo vascular implantation. Our approach not only offers an allogeneic “off-the-shelf” solution for clinical use but also it provides the possibility of personalized medicine using a patient's own amnion and stem cells for the production of a tissue engineered graft for reconstructive heart surgery.
Footnotes
Acknowledgments
This study was supported by the Sir Jules Thorn Charitable Trust, the Enid Linder Foundation, the British Heart Foundation, and the NIHR Bristol Biomedical Research Centre.
Author Contributions
M.T.G. and M.C. conceived and designed the research. M.M.S. performed the in vitro experiments. M.C., M.T.G., A.A., and D.I. carried out the animal work. M.M.S., M.T.G., and A.A. analyzed data. M.M.S. and M.T.G. interpreted results of experiments. M.M.S. prepared figures. M.M.S. and M.T.G. drafted and edited the article. M.T.G., M.M.S., M.C., A.A., and D.I. revised the article. All authors read and approved the final version of article.
Disclosure Statement
The authors have no conflicts of interest to disclose.