
Abstract
A new bone healing strategy that is based on localized cold is reported. A murine bone healing model was used, in which a unicortical defect was surgically created bilaterally within the femurs. After daily immersion in an ice bath for 28 days, a large increase in bone regeneration within a femoral cortical defect compared with the nontreated limb was observed. Bone regeneration mechanism within the defect upon cold was studied at 1 and 4 weeks using micro-computed tomography and immunohistochemical analysis and compared with the contralateral limb controls. The more advanced healing stage of the bone structure combined with the increased vascular channel density for the cold-treated group matched with an increased expression of vascular endothelial growth factor (VEGF), and a greater number of CD34+-stained cells in the early phase of repair in the cold group. This indicates an elevation in tissue angiogenesis secondary to VEGF expression in the cold group potentially through a temporary vasoconstriction of the local vasculature leading to a temporary state of relative hypoxia. Local cold therapy may be an unrecognized tool with which to accelerate bone regeneration. The absence of observed systemic or local side effects and enhanced bone healing indicates further study is warranted to develop potential clinical protocols.
Impact Statement
A variety of biological, mechanical, and physical therapeutic modalities of varying complexity, efficacy, cost, and safety profile have been developed to enhance bone healing. There have been sporadic reports of spontaneous bone formation after repeated cold exposure. In this study we report for the first time, the anabolic effect of cold exposure on bone healing in vivo resulting in a doubling of bone volume. Although the precise mechanism is not fully understood, cold is well known to stimulate osteoclastogenesis and modulate inflammation. The impact of this finding is considerable for tissue regeneration because cold application is noninvasive, safe, and easily implemented.
Introduction
Both epidemiological and experimental studies have reported a phenomenon that surfers exposed to cold water (19°C and lower) for prolonged periods of time develop external auditory canal exostosis, commonly known as surfer's ear.1–8 A similar condition has also been reported in paranasal sinuses.9–12 The degree of exostosis showed a significant correlation with cold water exposure time.13–16 The histopathology of the temporal cortical bone overgrowths from the ear canal consists of loosely organized trabecular surrounded by circumferential subperiosteal lamellar bone and numerous osteocytes—seemingly demonstrating a reparative process.2,9,17
Intermittent local cold therapy is historically used as rehabilitation adjunct after musculoskeletal injury to relieve pain and reduce inflammation.18–25 Reported effects include alteration of the tissue metabolism rate,26–29 local vasoconstriction30–32 with resulting hemorrhage33–35 and edema control,36–37 attenuation of the inflammatory response,38–40 and reduction of nerve conduction velocity41,42 resulting in a higher pain threshold.43–45 Although clearly beneficial for symptomatic relief after injury, little is known about the effects of local hypothermia on the regenerative process of healing skeletal tissue and the above phenomena of “surfers ear” implores the exploration of this question.
In vitro studies have shown that the number of osteoclasts differentiated from mononuclear cell cultures derived from mouse marrow showed a 1.5 to 2-fold increase with cold treatment at 34°C. 46 However, the effect of hypothermia on osteoblasts has seen conflicting results in the literature. Patel et al. concluded that hypothermia inhibits rat osteoblast differentiation after their results. They showed a reduction of trabecular bone structures containing osteoblasts by 75% when cultured for 14–16 days at 35.5°C and by 95% when dropped to 34°C. 46 However, human osteoblast cell lines exposed to short-term (e.g., 1–24 h of hypothermia of 14 days in culture) hypothermia exhibited an upregulation of Runx2 and osterix, leading to an increase in osteocalcin expression and alkaline phosphatase (ALP) activity. 47
In vivo study on mice exposed at different temperatures demonstrates changes in bony phenotypes with stunting growth in cold temperatures. 48 The authors propose that environmental temperature may alter limb temperature and perfusion influencing bone growth in the developing skeleton. In vivo, temperature can affect bone formation through its direct effect on bone cell proliferation, differentiation, and bone matrix production, as well as indirectly on the organism for instance by altering bone blood flow through vasoconstriction/vasodilation. Although these results together propose intriguing relationships between temperature and bone homeostasis, the effects of intermittent short period cold therapy on long bone healing are yet to be explored.
The aim of this study was to confirm that an internal bone temperature of 19°C achieved through brief daily locally applied cold by immersion in an ice bath of 4–6°C can positively affect bone formation in a murine femoral cortical bone defect model.
Experimental Section
Cortical defect preparation
A murine cortical bone defect model was used to test our hypothesis. This model has proven to generate a reproducible, mechanically stable defect without the need for fixation.49–52 All animal studies were performed after approval by the McGill Facility Animal Care Committee and were conducted in accordance with the Canada Council on Animal Care and the NIH Guidelines for the Care and Use of Laboratory Animals. Eighteen skeletally mature male C3H wild-type mice (Charles River Laboratories, Montreal, QC, Canada) aged 2–3 months (22–26 g) were used. After general anesthesia with isoflurane, the surgical site was disinfected using a 70% ethanol solution. A 5-mm incision was created to access the anterolateral aspect of the proximal femur using the third trochanter as the proximal landmark. The quadriceps fascia was incised, and the femur was exposed using blunt dissection. A 1-mm high-speed burr (Stryker, Hamilton, ON, Canada) was then used to create a 1 × 2.5 mm unicortical rectangular window in the anterolateral aspect of the femoral diaphysis (Fig. 1A). The defects were then completely flushed with phosphate-buffered saline (PBS) to remove all bone fragments. The wound was then irrigated with normal saline and closed with absorbable sutures in layers.
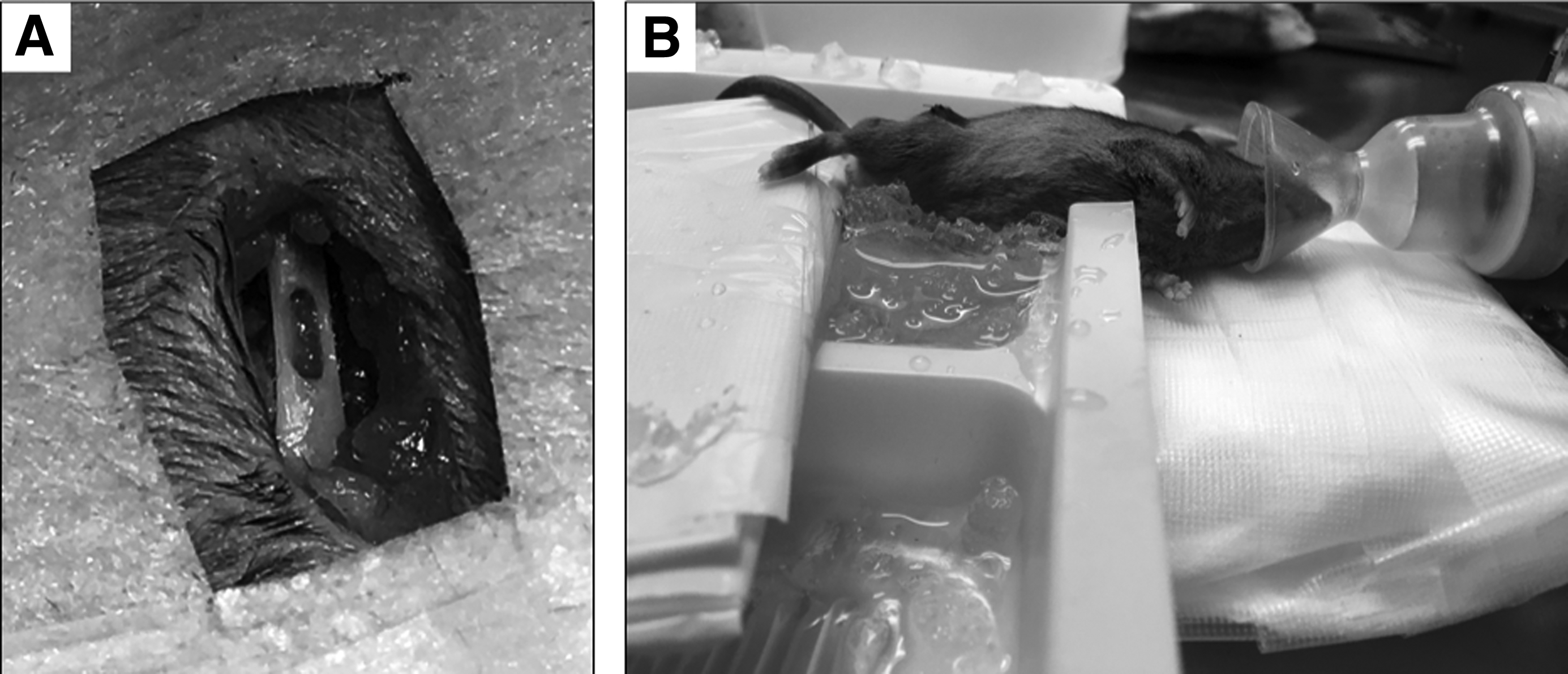
Femoral window defect and application of local cold therapy. Bilateral unicortical defects (1 × 2 mm) were drilled into the mid-diaphysis of 2- to 3-month wild-type C3H mice
Postoperatively the mice received a 5-day course of oral antibiotics (Bactrim; Hoffman-La Roche, Inc., Mississauga, ON, Canada), and were allowed full weight bearing on both lower extremities. Pain control was achieved with daily carprofen injections (5 mg/kg) only during the first 3 days after surgery. Mice were assessed for general health status by weight and grooming behavior and for any signs of fracture or infection.
Implementation of local cold therapy
Both hind limbs of the study animals had a surgically created bone defect as above. One hind limb of every mouse was subjected to daily cold treatments and was designated the experimental group (n = 18). The contralateral hind limb that did not receive any local cold therapy was designated the control group (n = 18). No special care or protection was taken during the cold treatment. However, before and after cold bath treatments, the wounds were visually examined to assess for any skin hypersensitivity or dehiscence.
We aimed to decrease the local temperature at the defect to ∼19°C. The temperature goal of 19°C was chosen to reproduce the temperature of the cold irrigation protocol that Fowler used to show an increase in guinea pig ear canal bony overgrowth. 5 To confirm this, a temperature sensor was implanted between the femur and extensor mechanism at the defect on two pilot study animals, and its wire connector was tunneled proximally and brought out through the skin on the back of the mouse. The exit site and wires were never placed in the cold bath. The temperature readings confirmed that the local temperature decreased to 19°C after immersion of the whole limb in a 4–6°C cold bath after 2 min. The chosen treatment regimen of 15 min once per day was modeled after the early animal studies of low-intensity pulsed ultrasound that used a similar regimen. 53
Starting on postoperative day 1 (POD-1) and for a total of 7 (n = 6) and 28 (n = 12) consecutive days, one lower extremity of all 18 mice was submerged in a 4–6°C cold water bath for a total of 15 min after undergoing general anesthesia (isoflurane/inhalant) (Fig. 1B). Care was taken to maintain core temperature throughout the treatment using a heating pad.
Femur harvest and micro-computed tomography imaging
Mice were killed at POD-7 or POD-28 by CO2 asphyxiation under isoflurane-induced anesthesia, followed by cervical dislocation. Femurs were dissected free of soft tissue, fixed overnight with 4% paraformaldehyde, washed in sterile PBS, and stored at 4°C before conducting the assessment of bone healing.
Micro-computed tomography (micro-CT) scans were obtained in a Skyscan 1172 scanner (Bruker, Kontich, Belgium) with an Al 0.5 mm filter at a voltage of 50 kV and a current of 200 μA with a spatial resolution of 5 μm/pixel. Three-dimensional (3D) reconstructions of specimens were made with the associate software (NRecon v1.6.10.4) and loaded into the CTAn software v.1.16.4.1 for quantitative analysis. Two different regions of interest (ROIs), centered at the middle of the cortical defect, were selected for bone volume/tissue volume (BV/TV) analysis: ROI A = mineralized tissue occupying the 1.5 × 0.9 × 0.25 mm window defect, and ROI B = a fixed 1 mm diameter circle centered on the medullary canal spanning the entire area of the cortical bone defect—the medullary canal adjacent to the window defect and the mineralized tissue within the window defect. Using Grayscale Index from 55 to 255, the total BV was extrapolated from the region of interest.
Usual bone parameters were measure for quantification of bone mass and structure such as percentage of BV/TV, trabecular number (Tb.N), bone mineral density (BMD), trabecular pattern factor (Tb.Pf), structural model index (SMI), degree of anisotropy (DA), trabecular thickness (Tb.Th), trabecular separation (Tb.Sp), and porosity (Pocl). Using a quantification of continuous, connected channel volume as a measure for vascularity developed by Bruker (Bruker micro-CT academy 2016 v5.3),50,54 blood vessel morphology was assessed at 4 weeks PO. The protocol to calculate the volumetric calculation of the blood vessel network only includes open pores with a diameter >50 μm. Quantitative data for vascular channels include blood vessel volume/tissue volume (BVV/TV), blood vessel number (No./mm 3 ), blood vessel thickness (μm), blood vessel spacing (μm), and connective density (μm).
Immunohistological analysis
After micro-CT analysis, the limbs were decalcified with 10% ethylenediaminetetraacetic acid, embedded into paraffin, and 5 μm sections prepared with a LEICA 2255 microtome (Leica Microsystems, Concord, ON, Canada). Hematoxylin–eosin (H&E) staining was used to assess the morphology of tissue. For histochemical study, samples were stained to identify ALP activity in osteogenic cells, tartrate-resistant acid phosphatase (TRAP) to identify osteoclasts, CD34 for endothelial vascular cells, and vascular endothelial growth factor (VEGF) as a potent angiogenic factor. Immunohistochemistry was performed according to the manufacturer instructions. The sections were incubated overnight with primary antibodies specific for VEGF (ABS82; 1:1000; Millipore) and goat antirabbit was used as secondary antibody. Antibody binding was detected using the DAKO antigen retrieval system (DAB kit, K3468). The sections were counterstained with hematoxylin, dehydrated, cleared, and mounted.
Microscopic images of the stained samples were captured using a Zeiss Axioskop 40 microscope (Carl Zeiss, Toronto, ON, Canada) or captured with Aperio digital pathology slide scanners from Leica Biosystems. All samples underwent histomorphometric calculation of the percentage of stained cells within defined regions of interest using the software ImageJ v.1.6.0 (NIH, Bethesda, MD). SPSS version 20 (IBM) was used to compare the means of the parameters measured in the control and experimental groups using a paired Student t test. Statistical significance was set at p < 0.05.
Results
A total of 18 mice underwent the operative procedure on both lower extremities without complications. Furthermore, there were no perioperative/PO fractures, surgical site infections, or signs of deteriorating general health up to the time of killing.
Histomorphometric analyses
After 1 and 4 weeks, all femora were subject to histomorphometric analysis with micro-CT to calculate the amount of new bone formation (Fig. 2). Total BV/TV of each bone was calculated to estimate the bone formation. BV/TV was highest in the cold group at 18.94 ± 9.23 compared with the control limb (7.97 ± 5.13) (p = 0.001). Bone vessel volume/tissue volume (BVV/TV) was calculated at POD-28 and found to be higher in the cold group than in the control group (7.8% vs. 6.7%, p < 0.001) (Supplementary Fig. S1 and Supplementary Table S1 in Supplementary Data; Supplementary Data are available online at www.liebertpub.com/tea) and the trabeculae in the defect of cold-treated mice appeared to be thicker, with more dense bone at 4 weeks (Supplementary Fig. S2 and Supplementary Table S2).
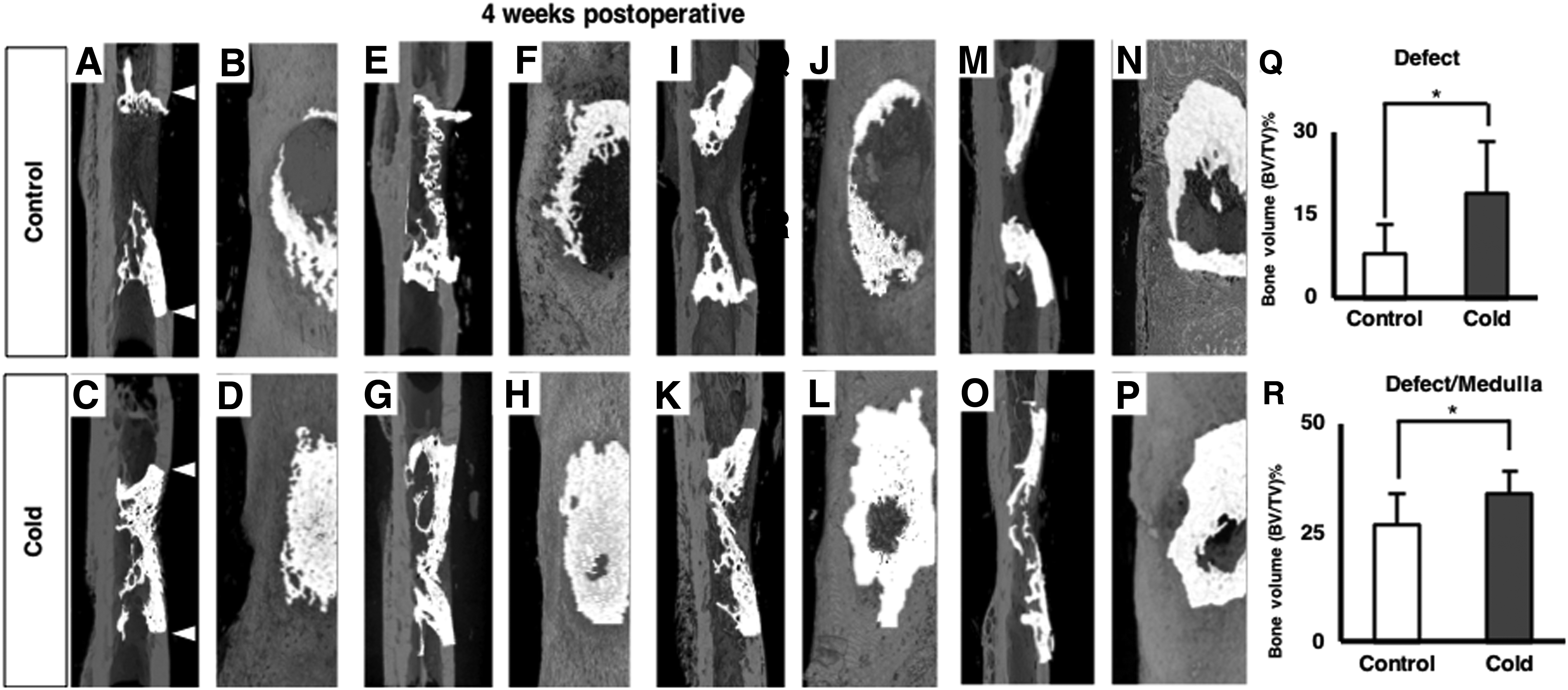
Macroscopic evaluation of bone repair in the window defect. Cold-treated and control femora were scanned at a resolution of 5 μm on a Skyscan 1172 instrument. Representative 3D models from paired femora were reconstructed from 2D images to display healing on the defect at 4 weeks PO. Significant new bone (white) is seen at the level of the defect in the cold group
Histological observations
Qualitative histological analysis of thin sections of decalcified bone was performed to corroborate the results of the histomorphometric analysis. The staining results for ALP, TRAP, presence of vascular endothelial cells (CD34), and VEGF at both POD-7 and POD-28 are summarized in Supplementary Table S3. ALP staining (Fig. 3A–D) revealed the low number of ALP-positive cells at the bone defect at POD-7 in both noncold (Fig. 3A) and cold groups (Fig. 3B). After 4 weeks, quantification of ALP-stained cells revealed to be significantly decreased (p < 0.001) in the experimental group (Fig. 3D) compared with the control group (Fig. 3C). Adjacent sections of decalcified bone were stained with TRAP to identify osteoclasts (Fig. 3E–H). A significantly higher number (p = 0.02) of TRAP-positive cells were seen at the proximal ends of the defect at POD-7 in the cold group (Fig. 3F). This suggests an increase in bone turnover at the defect site in the cold-treated femora. At POD-28, an extensive number of TRAP-positive-stained cells has been detected for the cold group (1.73 ± 0.5) (Fig. 3H), compared with the nontreated bones (1.54 ± 0.4) (Fig. 3G), although it did not reach statistical difference.
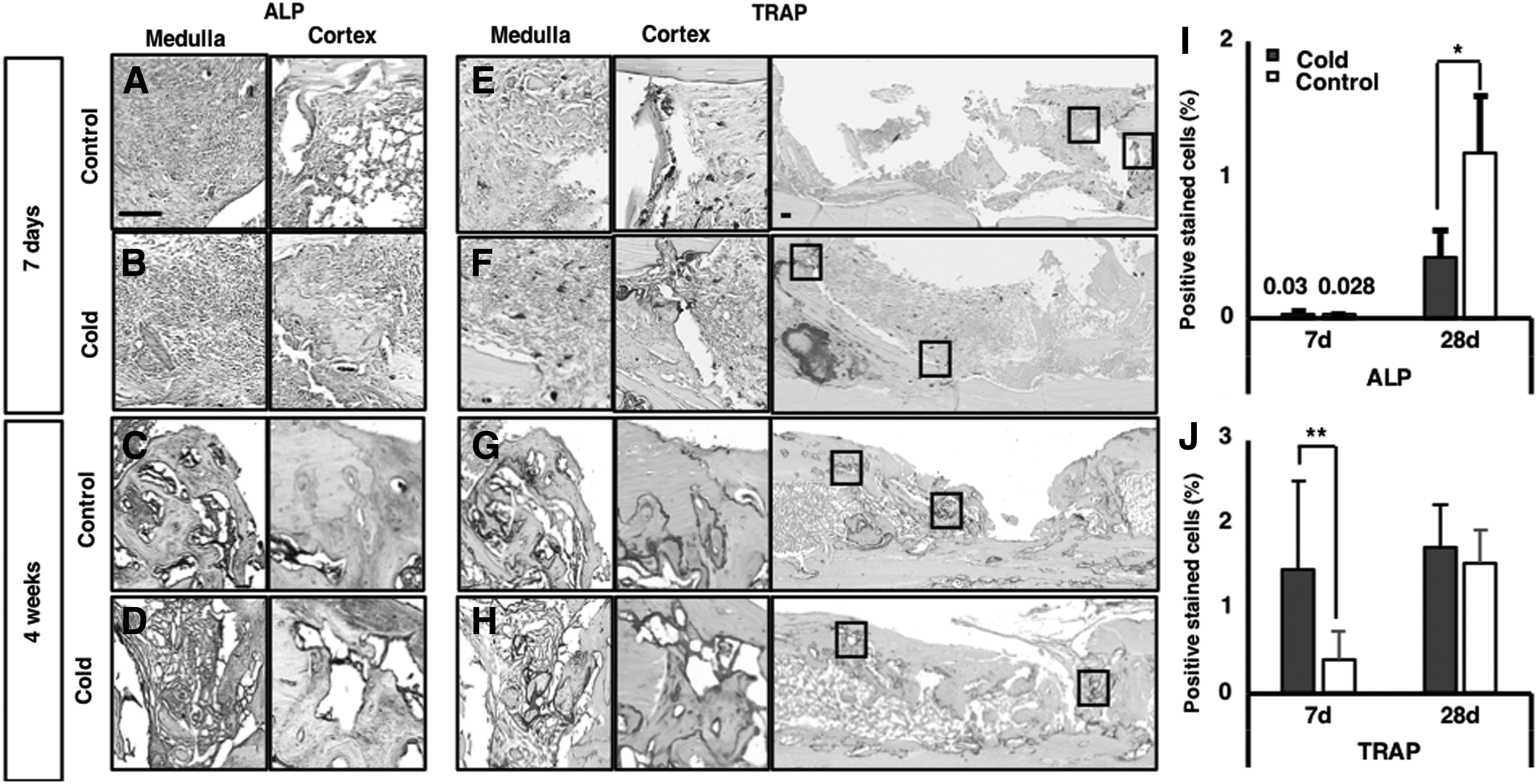
Identification of bone-resorbing osteoclasts and bone-forming osteoblasts in regenerating bone. Midsagittal sections were harvested from decalcified, paraffin-embedded paired femurs of control and cold therapy at 1 and 4 weeks PO and adjacent sections were stained for quantitative analyses of cell composition. ALP staining for osteoblasts showed no difference between control
After H&E staining, fibrous tissue filling the defect area is observed (Fig. 4A1, A2) at POD-7 in both groups. A coarse meshwork of trabecular bone can be seen at POD-28 with bridging of the defect area in the cold-treated limbs (Fig. A3), whereas the defect site in control limbs still displayed fibrous stroma with reactive bone formation on the defect edges (Fig. A4).

CD34 and VEGF immunohistochemistry in regenerating bone. Paired bones were decalcified embedded in paraffin and 5 μm sections stained immunochemically for CD34, and VEGF expression for analysis of the inflammatory phase (POD-7) and the remodeling phase (POD-27) of bone healing. Low-magnification images of hematoxylin and eosin-stained sections at 1 and 4 weeks for control
Immunohistochemical observations
CD34 was used as a sensitive marker for vascular endothelial cells in soft tissue and bone (Fig. 4C1–C4). The staining showed a significantly higher number of CD34 cells in the cold group (1.03 ± 0.42) (Fig. 4C2) at 7 days than in the control group (0.15 ± 0.09, p = 0.038) (Fig. 4C1).
The positively stained cells were clearly organized into vascular channels. By 4 weeks PO, only a few CD34-positive cells persisted in the cold-treated femora (p = 0.030) (Fig. 4C4), whereas there was a higher expression of CD34-positive-stained cells in the control group (Fig. 4C3). VEGF staining was performed to assess the activity of the major angiogenesis pathway (Fig. 4D1–D4). 55 A detailed examination of VEGF-stained cells in the defect area revealed more pronounced staining at POD-7 in the cold group (15.63 ± 3.51, p = 0.038) than in the control group (2.07 ± 0.36) (Fig. 4D1). At POD-28, this trend was inverted, with VEGF expression significantly higher in the control group (Fig. 4D3) than in the cold group (2.07 ± 0.36 vs. 0.38 ± 0.54, p = 0.034) (Fig. 4D4) and followed the same trend as CD34 staining at POD-28.
Discussion
This study investigates the effects of a short-term localized cold therapy on bone regeneration in an animal long bone defect. Our primary study question showed that 15 min of daily immersion in ice cold bath resulted in an increase in bone regeneration within a femoral cortical defect after 28 days of healing time. The similarity in early ALP activity, a marker of osteogenic differentiation, between the cold and control groups supports the hypothesis that the cold-induced bone growth might not be mediated by osteoblast activity differences in the early phase of repair. Given that the most probable explanation for the surfer's ear phenomenon is an increase in osteoblast activity, 6 here the mechanism appears to be different given that no sign of elevated osteoblast activity has been observed.
Chiba et al. has described the distribution of ALP expression in a rat healing model, showing peak expression between days 7 and 14, after which the expression declined as the trabecular bone remodeled. 56 Given that the cold limb group at POD-28 exhibited a coarse meshwork of trabecular bone at the remodeling phase, it could explain the small amount of ALP expression at that time point. The cold-treated femora might be further along the remodeling phase compared with the control group. The advanced stage of healing of the bone structure in the cold group compared with the control was correlated with an increase in the estimated vascular channel density at this time point. Both CD34 and VEGF were elevated in the cold therapy group compared with controls at the 7 days indicating an elevation in tissue angiogenesis secondary to VEGF expression in the cold group.
VEGF is an essential factor for vascular formation during angiogenesis and vasculogenesis, 57 appropriate callus architecture, and mineralization in response to bone injury. 58 Overexpression of VEGF may induce earlier bone formation and repair compared with normal-level controls.59,60 Intermittent cold immersion can stimulate the expression of VEGF-regulated angiogenic response through hypoxia, endothelial cell stimulation, and direct effect on either bone or blood products. Although several studies have shown that short-term47,61–63 and long-term46,64 hypothermia can have completely opposite effect on bone mineralization, hypoxic stimuli for bone growth has recently been approached by several authors.54,65,66
The critical driver in this study may be the intermittent hypoxic microenvironment created during the cold application. Indeed, localized cooling has been shown to cause a decreased blood flow and metabolism in bone, 33 and significant vasoconstriction continues beyond the cooling period of 20 min, despite skin temperatures returning toward baseline values.31,38 Bearing in mind that maintenance of bone oxygen pressure is closely related to the blood flow, 67 these results might indicate additive factors affecting the defect model. Cold applied to the bone defect area may cause intermittent hypoxia through vasoconstriction along with the usual disruption of the local blood flow after injury, which in turn has been shown to promote osteogenesis, through its upregulation of the angiogenesis pathway66,68—whether this is the entire mechanism for cold delivery remains to be seen. In response to a hypoxic environment, hypoxia-inducible factor is activated and stimulates the transcription of multiple genes with effects on angiogenesis, osteogenesis, precursor cell recruitment, and differentiation.66,68
Finally, osteoclast number was higher in the cold group during the early phase of repair compared with the controls. A stimulatory effect of cold temperature on the formation of human and mouse osteoclasts has been observed in vitro where osteoclast number was increased by ∼1.5–1.7-fold under continuous hypothermic conditions. 46 However, given the intermittent brief nature of hypothermia in our experiment, the observed elevation in osteoclasts is unlikely to be only explained by a direct effect of temperature change. The elevation of VEGF supports an underlying role of intermittent hypoxia as a potential mechanism for enhancing the bone osteoclastogenesis and the subsequent bone remodeling process.69–71 The positive effects of VEGF activation on osteoclast recruitment and resorptive function have been well documented.72,73
In this study, we suggest as potential mechanism that localized cold application enhances the bone healing process indirectly, through a temporary vasoconstriction of the local vasculature. This could create a temporary state of relative hypoxia that in turn may lead to upregulation of angiogenic transcription factors (VEGF), thereby improving revascularization and the bone remodeling potential. VEGF and CD34 cells persisted at elevated levels in the control group at 4 weeks, whereas there was a reduction in these markers in the cold-treated group indicating diminishing hemopoietic progenitor cell recruitment at this later time point in the cold group. This is potentially explained by the presence of a more advanced cortical bridging of the defect that is further along the healing sequence in the cold group.
Conclusion
In conclusion, to the best our knowledge, our study is the first to investigate the effects of local cold therapy on bone healing. Our results demonstrate that daily local cold therapy for 4 weeks accelerates/enhances bone healing in a murine model of intramembranous bone repair. Our study supports the hypothesis that the increase in osteogenesis may be mediated by the upregulation of the VEGF pathway. This could be the result of an intermittent cold-induced hypoxia; however, this warrants further investigation to unravel the cold treatment mechanism on bone healing. Further studies exploring the mechanism of action of local cooling on bone healing, as well as the optimal treatment dose, duration, and frequency are warranted based on the results of this pilot study. If proven effective, local cold therapy can be introduced as a novel, cost-effective, and noninvasive treatment modality to enhance bone healing in a clinical setting.
Footnotes
Acknowledgments
The research was supported by the Orthopedic Trauma Association resident grant as co-first authors. D.C. and M.C.-G. contributed equally to this work as co-first authors. E. Harvey and G. Merle contributed equally to this work.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.