
Abstract
Recombinant human bone morphogenetic protein-2 (rhBMP-2) has been widely used in spine fusion surgery. However, high doses of rhBMP-2 delivered with absorbable collagen sponge (ACS) have led to inflammation-related adverse conditions. Polyelectrolyte complex (PEC) control release carrier can substantially reduce the rhBMP-2 dose and complication without compromising fusion. The molecular events underlying controlled release and their effects on spinal fusion remain unknown. In this study, a rabbit interbody spinal fusion chamber was designed to provide a controlled environment for profiling molecular events during the fusion process. Study groups included Group 1, PEC with 100 μg rhBMP-2; Group 2, ACS with 100 μg rhBMP-2; Group 3, ACS with 300 μg rhBMP-2; Group 4, autologous bone graft; and Group 5, empty chamber. Manual palpation, microcomputed tomography, and histological analysis showed that Group 1 and 3 achieved bone fusion, while the other groups showed no signs of fusion. Gene expression profiling showed robust induction of osteogenic markers in Groups 1 and 3, with modulated early induction of inflammatory genes in the PEC group. Delivery of 100 μg rhBMP-2 with ACS (Group 2) resulted in less upregulation of osteogenic genes, increased inflammatory genes expression, and upregulation of osteoclastic genes compared to Group 1. These results suggest that the manner of BMP-2 release at the interbody spinal defect site could dictate the balance of in-situ osteogenic and antiosteogenic activities, affecting fusion outcomes. The molecular evidence supports PEC for sustained release of BMP-2 for spinal interbody fusion, and the feasibility of employing this novel interbody spinal fusion chamber for future molecular studies.
Impact Statement
A radiolucent rabbit interbody spinal fusion chamber was developed to study the molecular events during spinal fusion process. The gene expression profile suggests that control release of bone morphogenetic protein-2 (BMP-2) resulted in lower inflammatory and osteoclastic activities, but elicited higher osteogenic activities, while burst release of BMP-2 resulted in predominantly inflammation and osteoclastogenesis with minimum osteogenic activity. This study provides the molecular evidence that underscores the regeneration outcomes from the two different BMP-2 delivery systems. This spinal fusion chamber could be used for future molecular studies to optimize carrier design for spinal fusion.
Introduction
Autologous bone graft (ABG) is the current “gold standard” grafting material for spinal fusion. However, the limitations with the use of ABG in spinal fusion are the high pseudarthrosis rate, donor site pain, 1 increased operation time, and blood loss. The amount of bone graft is often insufficient in patients requiring long fusions and in those who had previous spinal surgery. These limitations have directed research on developing tissue-engineered graft materials to replace ABG. 2
Recombinant human bone morphogenetic protein-2 (rhBMP-2) has been widely used in spine fusion surgery.3,4 However, as absorbable collagen sponge (ACS) carrier has a rather limited capacity to bind and protect rhBMP-2 (half-life of 1.78 days), large doses are used to compensate for rapid growth factor extravasation and degradation loss.5,6 Extended clinical use of BMP-2/ACS has revealed concerns pertaining to inflammation-related adverse events such as seroma, endplate osteolysis, heterotrophic ossification, dysphagia, and airway compression in the neck. 7 To address the problems of high-dose rhBMP-2, various carriers based on core encapsulation, 8 surface adsorption, 9 covalent modification, 10 and matrix entrapment have been developed to control the release of this potent growth factor. We have previously reported a spinal fusion study using a heparin-based polyelectrolyte complex (PEC), which was engineered to bind to rhBMP-2 by ionic interaction, and to release the growth factors in a gradual manner. This carrier lowered the effective dose of rhBMP-2 needed by 20-fold 11 and reduced seroma and heterotrophic bone formation. 11 The in situ molecular mechanism induced by the controlled release versus burst release of BMP-2, pertaining to the different outcome in spinal fusion, however, remains unclear.
The temporal presence of BMP-2 plays a critical role in achieving optimal outcome of fracture healing. BMP-2 acts directly by stimulating osteoblast function and acts indirectly by modulation of osteoclastogenesis. 12 Following rhBMP-2 implantation, inflammatory cytokines such as tumor necrosis factor alpha (TNF-α), interleukin (IL)-1β, and IL-6 have been upregulated in patients and animal models. 13 Bone fracture healing cascade starts with an inflammatory reaction, in which immune cells release inflammatory cytokines, thus initiating the healing process. 14 On the other hand, excessive inflammatory response causes bone resorption and reduces bone quality. TNF-α and IL-1β have been reported to play an inhibitory role on BMP-2-induced osteogenic differentiation of mesenchymal stem cell. They also enhance the expression of the osteoclastogenic markers such as receptor activator of nuclear factor kappa-B ligand (RANKL).15–17 Suppression of inflammatory cytokine or RANKL activity increases the efficacy of rhBMP-2-induced bone formation.18,19
We hypothesize that the specially designed interbody spinal fusion chamber would provide a suitable platform for the study of the molecular events during lumbar interbody spinal fusion. This interbody spinal fusion chamber should constrain20,21 the penetration of the fibrous tissue and the residual disc tissue into the fusion microenvironment, which might interfere with subsequent molecular evaluation.22,23 It is made of nonabsorbable material that avoids acid dumping problem and provides better sealing properties compared with poly-DL-lactic acid spinal cage. 24 In this study, the effect of controlled delivery (using the PEC carrier) vs burst release (using the ACS) of rhBMP-2 in the spinal fusion chamber for lumbar interbody fusion was investigated in a rabbit model using ABG and empty chamber controls. The rabbit was chosen for this study due to availability of gene microarray, suitable intervertebral disc size, and reasonable cost for multiple time point studies. Gene profiling was performed using arrays of osteogenic, osteoclastogenic, and inflammatory markers, to decipher the molecular events participating in the fusion process.
Materials and Methods
Spinal fusion chamber design
OXPEKK®-IG polymer, a high-performance radiolucent poly-ether-ketone-ketone (Oxford Performance Materials, CT), was used to fabricate the rabbit interbody spinal fusion chamber device. 25
A cylindrical spinal fusion chamber was designed and fabricated using OXPEKK polymer according to the geometrical dimensions of rabbit lumbar spine. The average width, depth, height, and safe depth of the intervertebral disc were 12.9 ± 0.6, 6.9 ± 0.3, 3.6 ± 0.3, and 5.4 ± 0.3 mm, respectively. Based on these parameters, spinal fusion chamber of 5.5 mm in diameter, 4 mm in thickness, and channel diameter of 2 mm was fabricated using compression molding (Fig. 1B). The inner channel of the chamber was a cylindrical space (5.5 mm × 2.0 mm; Ø ≈ approximately 17 mm3 in volume) through which osteoinductive material such as ABG or recombinant growth factor can be placed. The channel connects the superior and inferior surfaces of the adjacent vertebral bodies, allowing the entry of the bone marrow and progenitor cells.

Preparation of rhBMP-2-loaded PEC alginate microbeads
rhBMP-2-loaded PEC alginate microbeads were prepared according to protocols described previously. 11 Briefly, 0.2 g of 8 M Rad γ-irradiated ultrapure medium viscosity sodium alginate (FMC Biopolymer, Princeton, NJ) was dissolved in 5 mL of deionized water and sterilized by 0.2 μm syringe filter. Microdroplets of 4 wt% sodium alginate solution was produced by microbeads encapsulator (Nisco Engineering AG, Switzerland) and crosslinked in 0.2 M strontium chloride solution (Sigma Aldrich, St. Louis, MO). The microbeads were coated by 2 mg/mL protamine (Sigma Aldrich) for 10 min followed by incubation with 0.5% heparin (Sigma Aldrich) for 15 min. rhBMP-2 (Medtronic Sofamor-Danek, Memphis, TN) reconstituted in water at a concentration of 1.5 mg/mL. PEC was incubated with 100 μg/300 μg of rhBMP-2 at 4°C for 30 min before implantation.
Preparation of ACS
A 5 mm × 2 mm × 1 mm ACS was cut and inserted into the spinal fusion chamber, and the same volume of predetermined concentration rhBMP-2 was added into the chamber 30 min before the implantation.
Animal surgery
All animal-related procedures were approved by the National University of Singapore's Institutional Animal Care and Use Committee before animal surgery (Protocol no. 2013-5399). Seventy-seven rabbits underwent L5/6 lumbar interbody spinal fusion surgeries. Rabbits were divided into the following groups: Group 1, PEC delivered 100 μg rhBMP-2 (n = 16); Group 2, ACS (Medtronic Sofamor-Danek) delivered 100 μg rhBMP-2 (n = 16); Group 3, ACS delivered 300 μg rhBMP-2 (n = 13); and Group 4, ABG (60 mm3) harvested from the iliac crest (n = 16). The iliac crest was exposed through the same incision. A 60 mm3 bone block was removed and morselized, and the bone chips were packed into the spinal fusion chamber. Group 5, no graft materials inside the chamber channel (n = 16). Four rabbits per group were used for endpoint microcomputed tomography (μCT) and histological analysis.
Ketamine (35 mg/kg) and xylazine (5 mg/kg) were used to induce anesthesia. Around 2–2.5% isoflurane was used to maintain anesthesia during the surgical procedures.
The L5/6 intervertebral disc was exposed through a retroperitoneal approach. The entry points on the vertebral bodies for the screws were determined and marked, and distance between the entry points was measured. Then, the intervertebral disc defect was created using a drilling trephine saw under continuous saline cooling. The entire tissue block was removed with posterior annulus fibrosus preserved, and the adjacent vertebral end plates were decorticated with a drill. Two titanium screws (Ø 1.5 mm, self-drilling, and length 4.0 mm; Synthes, Oberdorf, Switzerland) were placed in the midline of the vertebral bodies. The spinal fusion chamber with growth factor carriers was implanted into the defect. A suture was tied around the screws to retain the spinal fusion chamber (Fig. 1C). The distance between the two screws was measured again to confirm maintenance of the original disc height. After surgery, all animals were housed individually. Prophylactic antibiotics (enrofloxacin 10 mg/kg) and analgesics (buprenorphine 0.05 mg/kg) were administered for 3 and 5 days, respectively.
The rabbits were euthanized by intravenous injection of pentobarbitone (0.25 mL/kg) at 1, 4, and 8 weeks. After harvesting, the lumbar spines were manually palpated at the level of attempted fusion by two blinded observers. Each motion segment was considered fused and scored as 1 only if there was no motion present in all six directions (left and right bending, flexion and extension, and clockwise and anticlockwise axial rotation), otherwise it was read as not fused and scored as 0. Fusion rates were verified for 8-week specimens by μCT. Subsequently, harvested spine specimens were stored at −80°C before μCT and histological evaluations.
Seroma aspiration
The rabbits were observed for seroma formation and any hemoserous fluid was aspirated and quantified by using 5 mL syringe.
μCT analysis
The microarchitecture of harvested segments was evaluated using the Quantum Fx μCT system. The specimens were scanned at 90 kV and 140 μA with 30 μm voxel resolution. Data obtained by the system were reconstructed using 3D Studio Max software version 1.2 (Volume Graphics GmbH, Germany). Volume of interest representing all space inside the spinal fusion chamber was selected and segmented using an optimized density threshold value for quantification of the bone microstructural parameters by using CTAn software (SKYSCAN, Kontich, Belgium), which covered the bone volume (BV) over total volume (TV; BV/TV %), bone surface over TV, trabecular thickness (Tb.Th μm), and trabecular number (Tb.N 1/mm). Bone formation outside the chamber channel was analyzed separately to assess ectopic bone formation.
RNA extraction
Tissue inside the spinal fusion chamber was harvested and stored in Trizol reagent (Invitrogen) at −80°C prior for later processing. A probe sonicator (EpiShearTM Probe Sonicator; Active Motif, Carlsbad, CA) was used to homogenize the tissue in TRIzol reagent. RNA extractions were performed using Qiagen RNA extraction kit (QIAGEN, Dusseldorf, Germany). RNA concentrations and quality were examined with a Nanodrop (Thermo Scientific, Waltham). Total RNA (1 μg) of each sample was converted into cDNA using the RT 2 First Strand Kit (Quanta Biosciences, Gaithersburg) before the real-time PCR.
Gene profiling
Gene profiling was evaluated by RT 2 Profiler™ PCR Array, rabbit osteogenesis (#PANZ-026Z), and modified Inflammatory Cytokines & Receptors (#CAPN13074) array plate (QIAGEN, Valencia, CA). Real-time PCRs were conducted using the SYBR green system on specific RT 2 Profiler™ PCR Arrays with ABI 7900HT Sequencing Detection System (Applied Biosystems, CA). The level of expression of the target gene (n = 4), normalized to β-actin, was calculated by using the standard 2−ΔΔCt formula, and presented as fold changes relative to the native trabecular bone tissue.
Histology
Harvested specimens were fixed in 10% buffered formalin for 14 days, dehydrated in the gradient ethanol, and embedded into polymethylmethacrylate resin blocks. Ten-micron sections were made across the sagittal plane of the spinal fusion chamber using a tungsten blade microtome (Leica). After tissue adherence to the slide, embedded resin was removed by soaking the tissue slides in xylene at 37°C for 8 h. The specimens were rehydrated in the gradient ethanol and stained with methylene blue and basic fuchsin and viewed under the Olympus IX 71 microscope (Osaka, Japan). Masson's trichrome staining was performed to distinguish newly formed bone from the existing bone in autograft group. 26
Statistical analysis
Experimental results were reported as means ± standard deviations. One-way analysis of variance with repeated measures was used to evaluate differences between experimental groups by Tukey Kramer Multiple Comparison Test. SPSS Statistics (version 22.0; International Business Machines Corp.) was employed for statistical analyses and p < 0.05 was considered statistically significant.
Result
Seroma formation
Seroma formation was observed at retroperitoneal space on postoperative day 7 in Groups 1, 2 and 3 (Table 1). Seroma formation was most severe in the ASC group delivered with higher rhBMP-2 (300 μg; Group 3). Seroma formation in the PEC was statistically lower than both ASC carrier groups. There was no seroma detected in the ABG (Group 4) and empty chamber group (Group 5).
Seroma Volume
Seroma volume was collected from the retroperitoneal space one week postoperatively.
Denotes statistical difference compared to Group 3.
Denotes statistical difference compared to Group 2.
PEC, polyelectrolyte complex; ACS, absorbable collagen sponge; ABG, autologous bone graft; rhBMP2, recombinant human bone morphogenetic protein-2; ND, not detectable.
Manual palpation
Manual palpation analysis showed that all the specimens in PEC with 100 μg BMP-2 group (Group 1) and ACS with 300 μg BMP-2 group (Group 3) achieved fusion (Table 2). Fifty percent of samples in ACS with 100 μg BMP-2 group (Group 2) was fused, while all the samples in the ABG and empty chamber group (Group 4 and 5) retained motion, indicating the failure of spinal fusion.
Spinal Fusion Rate Measured by Manual Palpation for Eight-Week Specimen
μCT analysis
In the sagittal views (Fig. 2A), all the specimens in Groups 1 and 3 showed solid bone fusion inside the chamber channel, bridging the superior and inferior vertebral endplates (indicated by arrows). Bone formation was observed in Groups 2 and 4 (indicated by arrowhead), but bone bridging was not achieved. There was no bone formation observed in Group 5 (indicated by asterisks). PEC with 100 μg BMP-2 (Group 1) and ACS with 300 μg BMP-2 (Group 3) have higher BV fraction (BV/TV), Tb.Th and Tb.N, than the rest of the groups (p < 0.05) (Fig. 2C–F).
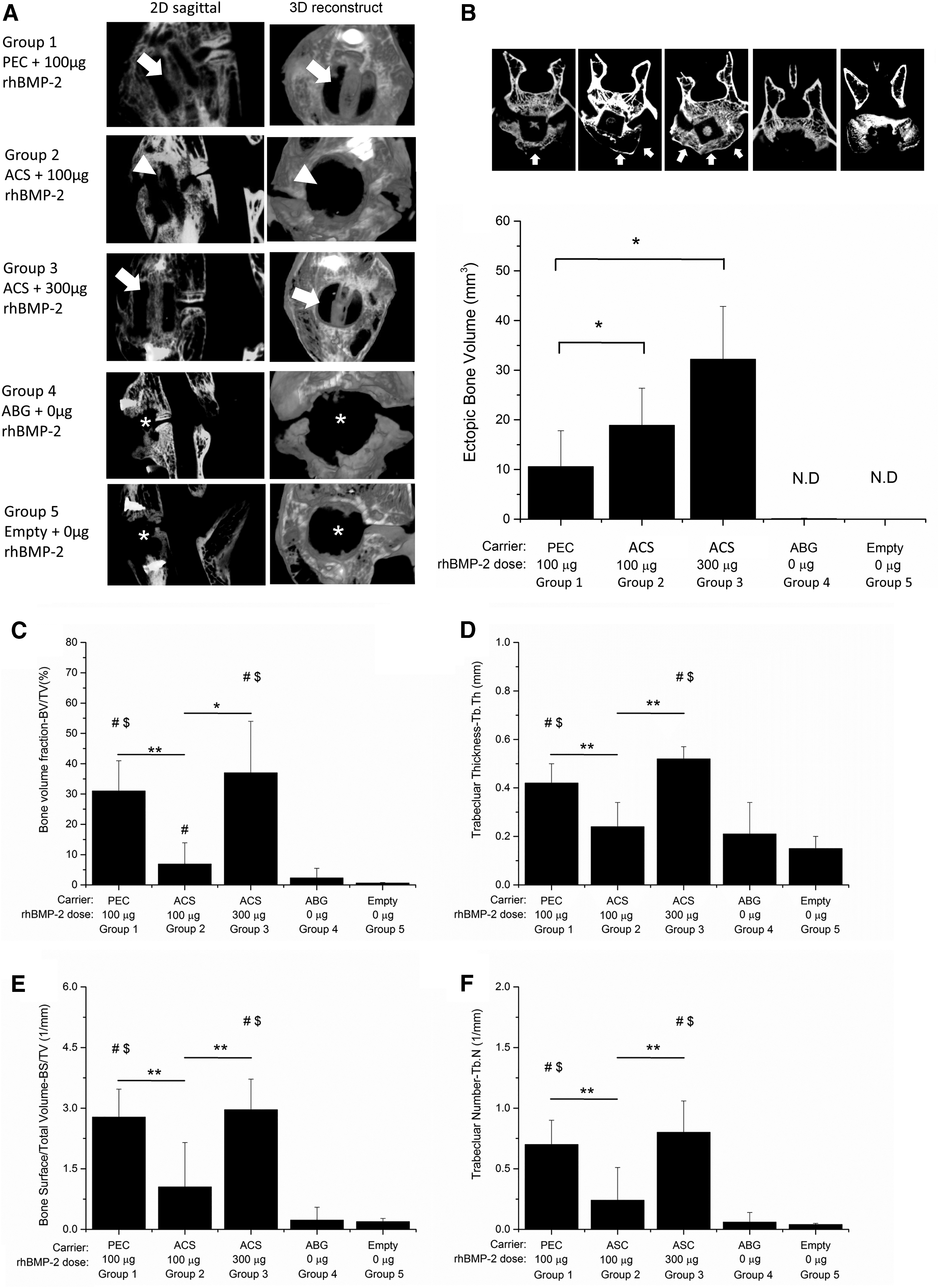
From Figure 2B, a significant increase in ectopic bone growth in front of the spinal fusion chamber (indicated by arrows) was detected in Group 2 (18.9 ± 7.5 mm3) and 3 (33.2 ± 10.6 mm3), compared to Group 1 (10.6 ± 7.2 mm3).
From μCT radiography, PEC with 100 μg BMP-2 group (Group 1) and ACS with 300 μg BMP-2 group (Group 3) achieved fusion (Table 3). Twenty five percent of samples in ACS with 100 μg BMP-2 group (Group 2) was fused.
Mean Radiographic Fusion Scores Eight Weeks Postoperatively
Histology
Newly formed woven bone was found inside the spinal fusion chamber channel in Group 1 (PEC with 100 μg BMP-2) and Group 3 (ACS with 300 μg BMP-2), with lacunae structure and osteocytes observed in the mineralized matrix (Fig. 3). In Group 2 (ACS with 100 μg BMP-2) and Group 4 (ABG), minimal bone deposition was detected. Fusion was not observed. No mineralization was observed in Group 5 (empty chamber). Masson's trichrome staining showed both osteoid (red) and new bone (blue) inside the spinal fusion chamber channel in Groups 1 and 3 (Fig. 3). In Group 4, most of tissue was osteoid with autograft (iliac crest bone), occupying the chamber channel with minimal new mineralized bone.

Representative photomicrographs of basic fuchsin and methylene blue staining (left). Histological evaluation showed larger bone areas in Groups 1 and 3 compared to minimal bone formation in Groups 2 and 4. There was no bone formation in Group 5. rhBMP-2: Representative photomicrographs of Masson's Trichrome staining (right). Masson's trichrome staining showed both osteoid (red) and new bone (blue) inside the spinal fusion chamber channel in Groups 1 and 3. In Group 4, most of tissue was osteoid. Lacunae indicated by yellow triangle. Low magnification 40 × . High magnification 400 × .
Gene profiling
Relative change of the osteogenic genes in the spinal fusion chamber among the five groups at 1, 4, and 8 weeks postoperation was analyzed (Supplementary Table S1). Osteogenic genes having greater than fourfold changes were selected. Upregulation of early osteogenic markers, collagen 1 subtype A (COL1A1 and COL1A2), and late osteogenic markers, bone gamma-carboxyglutamate protein osteocalcin (OCN), were detected in Groups 1 and 3 at week 4 (Fig. 4). Despite the large variation, COL1A1 and OCN levels were significantly higher compared to Group 2 (p < 0.05). The high expression level of these genes persisted to week 8. The expression of osteogenic genes was at significantly lower levels in Groups 4 and 5 (p < 0.05). Genes associated to osteoclastic absorption (activities), including RANKL, osteoprotegerin (OPG), CXCL1, and lymphotoxin B, registered heightened expression at week 1, specifically in Group 2 (p < 0.05) (Fig. 5). Expression of OPG, CXCL1, and lymphotoxin B was not detectable in Group 1 and 3 at all time points. The expression of RANKL was also upregulated in Group 4.

Expression of osteogenic markers (COL1A1, COL1A2, and OCN) at 1, 4, and 8 weeks. Gene expression were normalized to their respective β-actin expression and expressed as fold changes relative to native trabecular bone tissue. n ≥ 3 per group, mean ± SD. *Statistically significant at p < 0.05. SD, standard deviation; COL1A, collagen 1 subtype A; OCN, osteocalcin.

Expression of osteoclast genes (RANKL, OPG, CXCL1, and Lymphotoxin B), at 1, 4, and 8 weeks. Gene expression was normalized to their respective β-actin expression and expressed as fold changes relative to native trabecular bone tissue. n ≥ 3 per group, mean ± SD. *Statistically significant at p < 0.05. OPG, osteoprotegerin; RANKL, receptor activator of nuclear factor kappa-B ligand; CXCL1, Chemokine (C-X-C motif) ligand 1.
The relative change of the inflammatory genes among the five groups was compared (Supplementary Table S2) and selected inflammatory genes presented in Figure 6. A transient increase of inflammatory markers was detected at week 1 and subsided thereafter. Most inflammatory markers were highly upregulated in Groups 2 and 3 (rhBMP-2 released from ACS), while the expression level of these markers was significantly lower in Groups 1 (rhBMP-2 released from PEC) and 4 (ABG), and was negligible in Group 5 (empty chamber). Groups 2 and 3 had higher expression of the proinflammatory genes (IL-1β, IL-1R1, IL-6, Chemokine (C-C motif) ligand 2 (CCL2), Chemokine (C-C motif) ligand 4 (CCL4), and interferon gamma [IFN-γ]) than Group 1 (Fig. 6A), of which increase in CCL2, CCL4, and IFN-γ was significant in Group 2. On the other hand, the expressions of IL-1A, IL-17, Chemokine (C-C motif) receptor type 3 (CCR3), Chemokine (C-C motif) type 5 (CCR5), and Chemokine (C-X-C motif) type 5 (CXCR5) were singularly prominent in Group 2 (Fig. 6B), at a significantly higher level to Group 1. Notably, anti-inflammatory markers, IL-10, IL-4, and IL-4R were also highly expressed in Group 2 compared to Group 1, at significant levels. No significant difference was detected between Group 1 and Group 3 for the markers listed in Figure 6B and C, and was hardly detectable in the other groups.

Expression of inflammatory and anti-inflammatory genes at 1, 4, and 8 weeks. Inflammatory genes were grouped according to upregulated expression in Group 1, 2, and 3
Discussion
A rabbit interbody spinal fusion chamber was designed and fabricated with polyetherketoneketone to study the microenvironments of bone healing during interbody spinal fusion (Fig. 1). The biocompatibility and stability of the inserted spinal fusion chamber system were confirmed with good survival rate through the 8-week study period, and absence of device dislocation. There was no fusion observed in the empty chamber group (Group 5), indicating that this was a critical-size spinal defect model. The ability of the spinal fusion chamber to support spinal fusion was investigated with the delivery of ABG, and rhBMP-2 using two carriers, the clinically approved ACS 27 and a sustained-release PEC carrier. 28
In contrast to the result from μCT and histological analysis, manual palpation analysis predicted 50% fusion success in Group 2. This discrepancy was likely due to ectopic bone formation outside of the chamber (Fig. 2B). ACS carriers when delivered at a clinically equivalent dose of rhBMP-2 (300 μg rhBMP-2/per level; Group 3), resulted in 100% fusion rate, reaching quantitative parameters comparable to 100 μg rhBMP-2 loaded in PEC. The requirement of large doses of the rhBMP-2 delivered by ACS to induce spinal fusion agreed with previous animal experiments.28–30 The superior fusion performance of the PEC delivered with lower doses of rhBMP-2, relative to ACS delivery, matched previous posterolateral and interbody spinal fusion studies.28,31 Histologically, the autologous iliac bone graft (Group 4) implanted inside the spinal fusion chamber was replaced by small bone particles and fibrous tissue (Fig. 3). It is likely that insufficient autologous bone grafted into the inner chamber to induce spinal fusion in this critical-size defect model.
PEC had lower seroma formation than ACS carrier with 100 μg BMP-2 and 300 μg BMP-2. At a similar dose, the poor modulation capacity of ACS carrier released half of the rhBMP-2 within the first 3 days, 32 while PEC released 25–39% of rhBMP-2 in the first 7 days. 33 The higher release rate of the BMP-2 of the ACS carrier resulted in increased inflammatory response and seroma formation, which were consistent with the results from our previous rodent model. 11 The supraphysiological dose of the rhBMP-2 and the leakage issue associated with ACS carrier have been closely associated to the clinical observations of seroma and symptomatic ectopic bone formation.34,35 Since rabbit has been used in many spine fusion studies and BMP-2 structure is highly conserved during evolution,36–38 it is unlikely that inflammation is caused by species difference.
Osteogenic PCR array results indicate that COL1A1 gene was highly upregulated in Groups 1 and 3 at week 4, compared to Group 2 in which upregulation was detected later at week 8. Expression of Col1A2 was upregulated in all experimented groups (Groups 1, 2, and 3) at week 8, with early and enhanced expression of this marker in Group 3. The late osteogenic marker, OCN, was significantly upregulated in Group 1 and 3 at week 4, compared to Group 2. Col1A1 and Col1A2 genes encode for Collagen I pro-α1 and pro-α2 chains, which are critically important to form the collagen type I fiber for bone formation, 39 together with increase in OCN expression, would have further promoted the bone mineralization in Group 1 and 3, compared to the rest of the groups. The expression pattern of these osteogenic genes in PEC-rhBMP-2 and the two ACS-rhBMP-2 groups correlated well with the successful spinal fusion in the chambers of Groups 1 and 3, contrasting to the reduced bone deposition and absence of spinal fusion with ACS-100 μg rhBMP-2 (Group 2). Low expression of these genes in the ABG (Group 4) and empty chamber (Group 5) also correlated well with the lack of bone formation in these two groups.
Early upregulation of the critical osteoclastogenic factors, 40 RANKL, CXCL1, and lymphotoxin B in Group 2 compared to all other groups (Fig. 5), indicating higher osteoclastic activity induced by burst release carrier of rhBMP-2. OPG upregulation may partially counteract the osteoclastic effect of RANKL. 41 The lower osteogenic activity of ACS with 100 μg rhBMP-2 coupled with the higher osteoclastogenic activity from the burst release probably accounted for the failure of the fusion. In view of the overall enhancement of osteoclastic genes, we speculate that osteoclastogenesis might be dominant in Groups 2 and 4 (which had early upregulation of RANKL). These results are in accordance to the clinical observation that patients experienced transient osteolysis or bone cyst around the vertebral endplate postoperatively after the rhBMP-2 treatment in the lumbar interbody fusion surgery.42,43 Comparatively, lower expression of osteoclastic genes with delivery of PEC with 100 μg rhBMP-2 and ACS with 300 μg rhBMP-2, accompanied by robust osteogenic gene expression, could account for successful osteogenic induction and spinal fusion.
Various inflammatory cytokines and their cognate receptors in and around the fracture site play a crucial role in tissue formation throughout the bone regeneration process.44,45 The profile of inflammatory markers within the spinal fusion chamber was monitored and correlated to the expressions of osteogenic markers and the bone fusion outcomes. We detected upregulation of inflammatory markers at week 1 in the chambers with rhBMP-2 compared to empty and ABG groups (Fig. 6A). Notably, several inflammatory cytokines were distinctly enhanced only by ACS with 100 μg rhBMP-2, including IL-1A, IL-17, CCL2, CCL4, CCR3, and CCR5 (Fig. 6B). The negative impact of IL-1 and IL-17 on osteogenesis has been shown in both in vitro and in vivo studies. IL-1 plays an important role in the bone resorption and subcutaneous injection of IL-1, resulting in an increase in osteoclast number and enhancement of the osteoclastic activity.46,47 IL-17 induces the expression of proinflammatory cytokines in stromal cells and macrophages,48,49 and promotes osteoclastogenesis by upregulating RANKL expression on osteoblasts and synovial fibroblasts.50,51 Although the increase of the anti-inflammatory genes was detected in the same group (Fig. 6C), the high expression of proinflammatory genes, indicated an exaggerated inflammatory environment triggered by ACS 100 μg rhBMP-2, probably accounted for the inhibition of bone formation and the active osteoclastic effect inside the chamber channel.
BMP-2 dose-dependent induction of inflammation and bone resorption has been reported.15,41 Despite the apparent enhancement of several inflammatory genes with the delivery of ACS with 300 μg rhBMP-2 (Fig. 6A), other inflammatory genes associated to bone resorption were substantially lowered in this group (Fig. 6B), which paralleled the low expression of osteoclastic genes (Fig. 5). Interestingly, we detected a distinctive increase of IFN-γ at week 1, with another smaller increase at week 8, in Group 3, which was not observed in Group 1. IFN-γ has been reported to stimulate ALP activity in osteoblasts, 52 while suppressing the in vitro differentiation of osteoclasts. 53 IFN-γ receptor-deficient mice have increased osteoclast formation in the presence of bone inflammation, indicating that IFN-γ has a protective antiresorptive effect. 53 Furthermore, local administration of IFN-γ promoted bone formation in autogenous bone grafts by regulating osteoclastogenesis and TNF-α expression. 54 It is therefore possible that the presence of IFN-γ in Group 3 has modulated the in situ osteoclastic activities in favor of the osteogenic activity, resulting in the success of spinal fusion and ectopic bone formation. Although transcription profiling does not always predict protein synthesis levels, the overall gene profiling results is consistent with an interpretation that the PEC-rhBMP-2 test group induces bone formation responses, while minimizing the osteoclastic activities and inflammatory genes expression.
Conclusion
Our results indicate that by sustained release using the PEC carrier, the inflammatory responses induced by BMP-2 can be modulated, harnessing the beneficial inflammatory signaling necessary for bone generation, while avoiding the osteoclastic activities triggered by the exaggerated inflammatory response from growth factor burst release using ACS carriers. The molecular evidence supports the use of PEC for sustained release of BMP-2 for spinal interbody fusion in the future, and the feasibility of employing this novel interbody spinal fusion chamber for further molecular study.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.