
Abstract
Bone marrow-derived mesenchymal stem cells (BMSCs) have potential to accelerate flexor tendon healing and allow for earlier rehabilitation. The ideal BMSC construct and delivery method to the repair site remains unknown. We investigated the efficacy of interposed scaffold-free BMSC sheets on early Achilles tendon healing in rats. BMSCs were isolated from the femora and tibias of male Sprague–Dawley rats aged 8–12 weeks and BMSC sheets were produced on temperature-responsive culture dishes. Ninety-five male Sprague–Dawley rats aged 8–12 weeks were utilized. A bilateral Achilles tendon repair model was created. One side was randomly selected, and the tendon was repaired with the interposed BMSC sheet (BMSC group). The other side was repaired without BMSCs (control group). The bilateral tendons were harvested at 5, 6, 7, 10, and 14 days postoperatively for biomechanical analysis, measurement of the gene expression level of tendon markers scleraxis and tenomodulin by real-time polymerase chain reaction, and histological evaluation. The BMSC group had significantly higher maximum load to failure and stiffness at 5 and 6 days compared with the control group. Moreover, the BMSC group showed significantly increased gene expression of scleraxis and/or tenomodulin at all timepoints. The cross sectional areas in the BMSC group were significantly larger at 5, 6, and 14 days. However, hematoxylin and eosin staining of the central part of the repair site revealed no significant differences at all timepoints. These results suggest that the increased biomechanical strength afforded by BMSC sheet implantation into tendon repair sites may allow for the earlier onset of rehabilitation and improved clinical outcomes in flexor tendon surgery.
Impact Statement
We investigated the efficacy of interposed bone marrow-derived mesenchymal stem cell (BMSC) sheets on early Achilles tendon healing in rats. The tendons repaired with BMSC sheets revealed significantly increased mechanical strength compared with the control repairs (without the BMSC sheet) at 5 and 6 days. These data reveal that BMSC sheet implantation into tendon repair sites may allow for earlier onset of rehabilitation and improved clinical outcomes in flexor tendon surgery.
Introduction
Flexor tendon surgery is often complicated by the formation of adhesions that can lead to poor tendon gliding, loss of range of motion, and joint stiffness. Therefore, the ideal flexor tendon repair would involve accelerating tendon healing to allow for earlier onset of rehabilitation to reduce adhesion formation and improve tendon gliding. However, early motion before adequate healing may promote gap formation or repair ruptures during the early healing process. 1 In addition, although there are numerous approaches to improve rehabilitation protocols, suture technique, and suture materials, gap formation or/and repair ruptures are still seen and the ideal flexor tendon repair remains elusive. 1
Recently, biological augmentation of flexor tendon repair by adding growth factors and mesenchymal stem cells (MSCs) has been explored in an effort to accelerate healing. 2 MSCs are located around perivascular regions and may be purified from several tissues, including bone marrow, adipose tissue, synovial tissue, and umbilical cord blood. 3 MSCs derived from marrow have multilineage differentiation capability and may develop into bone, cartilage, tendon, and fat. 4 Although bone marrow-derived MSCs (BMSCs) make up a small fraction of the bone marrow cell population (about 0.001% to 0.01%), 5 cell-based therapy with BMSCs has been widely used in musculoskeletal clinical trials. 6 Dai et al. 7 showed that BMSCs have higher tenogenic differentiation capacity compared to synovium-derived MSCs and adipocyte-derived MSCs. In our previous in vitro and in vivo studies,8–10 BMSCs were shown to accelerate healing in rat tendon repairs. However, the ideal construct and method of delivery of these cells to repair sites in vivo are still unknown.
Scaffold-free cell sheet engineering using temperature-responsive culture dishes has been utilized in various fields. 11 Komatsu et al. 12 fabricated a tendon-derived stem/progenitor cell (TSC) sheet using temperature-responsive culture plates and implanted the TSC sheet in a rat Achilles tendon defect. The TSC sheet improved the histological properties and collagen content of the tendons at 2 and 4 weeks. 12 However, to our knowledge, there are no reports of the use of BMSC sheets on early tendon healing in vivo.
The aim of this study was to evaluate the effects of BMSCs delivered as cell sheets to the repair site of a rat Achilles tendon repair model. We hypothesized that the BMSC sheets would improve the initial repair strength and resistance to gap formation and decrease time to healing.
Materials and Methods
Isolation of bone marrow-derived mesenchymal stem cells and creation of the bone marrow-derived mesenchymal stem cell sheet
BMSCs were isolated in typical manner as previously reported. 13 In brief, bone marrow cells were collected from the femora and tibias of male Sprague–Dawley rats aged 8–12 weeks. 14 Institutional guidelines for the care and use of laboratory animals were followed. Freshly euthanized rats were sterilized sequentially in 95% and 70% ethanol for 5 min before dissection. Under sterile conditions, the rat femora and tibias were isolated and transected to expose the medullary canals. The cells were flushed from the cavities with an 18-gauge needle using Dulbecco's modified Eagle's medium (DMEM) (Gibco, Carlsbad, CA) and passed through a 70 μm strainer, centrifuged, and resuspended in DMEM supplemented with 10% MSC fetal bovine serum with 1% antibiotic/antimycotic (MSC culture medium). The fresh medium was replaced the next day to remove the unattached cells (Passage 1). Cells between passages 1–3 were utilized in this study.
The BMSC sheets were created as previously reported. 12 In brief, 1 × 106 cells were seeded and cultured on specially designed 3.5 cm temperature-responsive culture dishes (UpCell™, CellSeed, Tokyo, Japan) containing MSC culture medium for 3 days. Immediately before the surgery, the plate was incubated at room temperature for 20 min. During that time, the cells were detached from the plate and suspended as a complete sheet (Fig. 1). This sheet was then utilized in animal surgery.
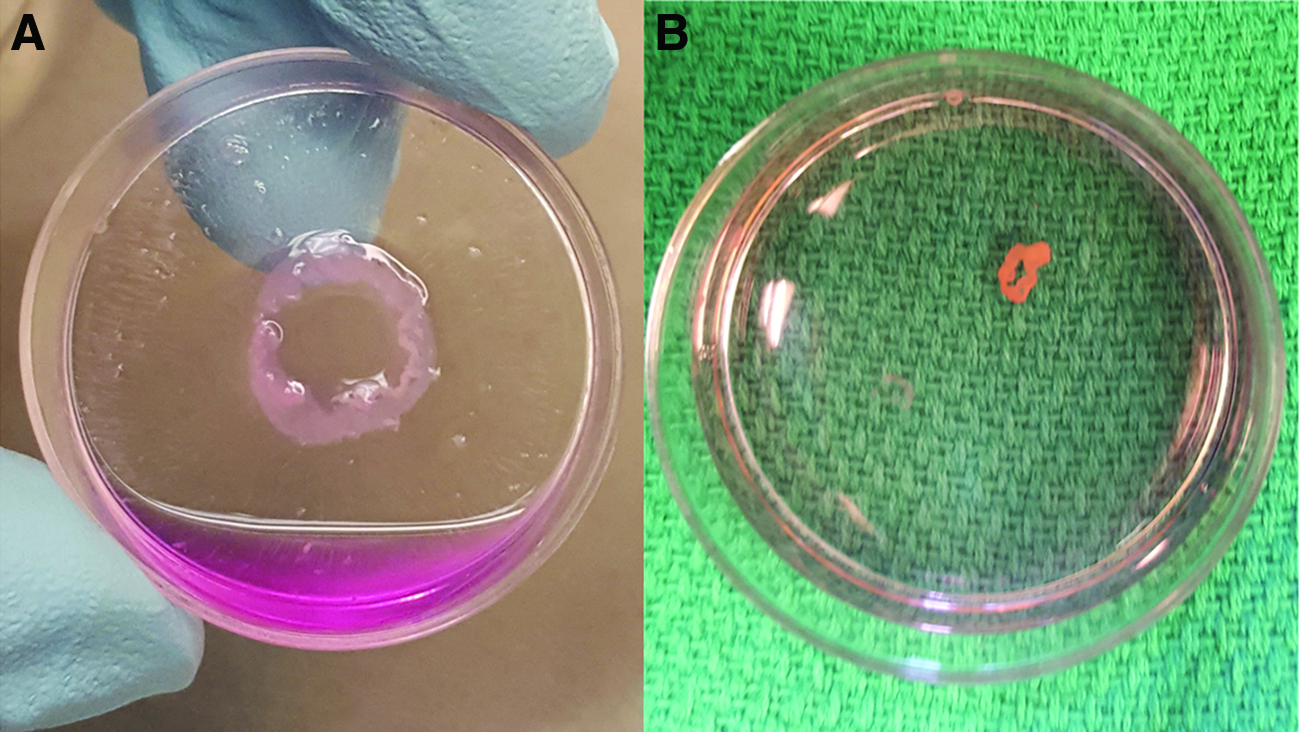
BMSC sheet. Immediately before surgery, the dish is incubated at room temperature for 20 min
Animal surgery
All animal experiments were performed according to protocols approved by our Institutional Animal Care and Use Committee (Protocol number: 21561, the date of approval: 10/19/2017). Ninety-five male Sprague–Dawley rats aged 8–12 weeks were utilized. The surgical procedures were performed in the prone position, under general anesthesia using inhaled isoflurane (3% for induction and 2% for maintenance) with oxygen flowing at 1.0–2.0 L/min. First, the bilateral sciatic nerves were cut. A 2 cm skin incision was made over the Achilles tendon. The plantaris tendon was resected. The Achilles tendons were transected 2 mm proximal to the calcaneal insertion and repaired with a 4-0 polyester nonabsorbable suture in a 2-strand Kessler configuration. To provide an internal control, each of the limbs was randomly selected. The BSMCs group consisted of randomly assigned tendons repaired with a BMSC sheet interposed within the repair site (Fig. 2). The contralateral side was repaired without the addition of cells (Control group). The wounds were closed using 4-0 nonabsorbable sutures.

Rat Achilles tendon repair model. The tendons were transected 2 mm from the calcaneal insertion and repaired with a Kessler stitch using 4-0 polyester nonabsorbable suture
The rats were allowed normal activity and diet and were euthanized at 5, 6, 7, 10, and 14 days after surgery. Euthanasia was performed by placing the animals in sealed chambers with induction of 5% isoflurane for sedation. Once sedated, the chamber was filled with carbon dioxide. The bilateral tendons were harvested from the proximal musculotendinous junction to the entire calcaneus. Fourteen tendons in 10 rats had visible gapping between the tendon ends with partial or complete loss of continuity. 15 These 10 rats were excluded, and 85 rats were used for analysis: 60 rats (n = 20 at day 5, n = 12 at day 6, n = 10 at day 7, n = 9 at day 10, and n = 9 at day 14) for the biomechanical testing, and 25 rats (n = 5 at each timepoint) for gene expression and histological assessment. In preparation for the biomechanical testing, the suture material and any adjacent tissue were removed to ensure testing of only the repair tissue and the specimens were stored at −20°C.
Gross measurements/biomechanical analysis
The bilateral tendons harvested at each time point were studied as matched pairs. The tendons were thawed to room temperature on the day of mechanical testing. Tensile testing was performed on an Instron 5944 materials testing system using a 2kN load cell (Instron Corp, Norwood, MA). The proximal end of the tendon was bonded to 100-grit sandpaper using cyanoacrylate (CA) glue and then attached to the upper grip on the test machine. The calcaneus was attached directly to the base grip. Before testing, spherical markers (2 mm diameter) were attached ∼7 mm proximal and distal to the repair site using CA glue.
Before mechanical testing, a 1 N preload was applied to each sample and photographs were taken in two planes (sagittal and coronal). The images were used to measure the width and depth of the tendon at the midportion of the repair site (Fig. 3B). Tendon thickness was measured using ImageJ. Assuming the cross section of the tendon was an ellipse, the cross sectional area was calculated by two perpendicular thickness axes (width = a and depth = b) as follows: cross sectional area = π ab/4. 16 Following the application of the preload, tendons were loaded to failure at 10 mm/min. Force and image data were synchronized and recorded at 10 Hz. The video was taken throughout testing with a model acA1600-20gm CCD camera (Basler, Inc., Exton, PA) fitted with a Zoom 7000 lens (Navitar, Inc., Rochester, NY) (Fig. 3A). Videos were imported into a custom MATLAB script (MathWorks, Natick, MA), which tracked position of each bead and calculated bead separation (gap formation) throughout each test. Outcome measurements were the maximum load to failure and stiffness. The maximum load to failure was defined as failure load or load at 2 mm gap formation (whichever came first). The stiffness was defined as the maximum slope of the load-displacement curve before 2 mm of gap formation.
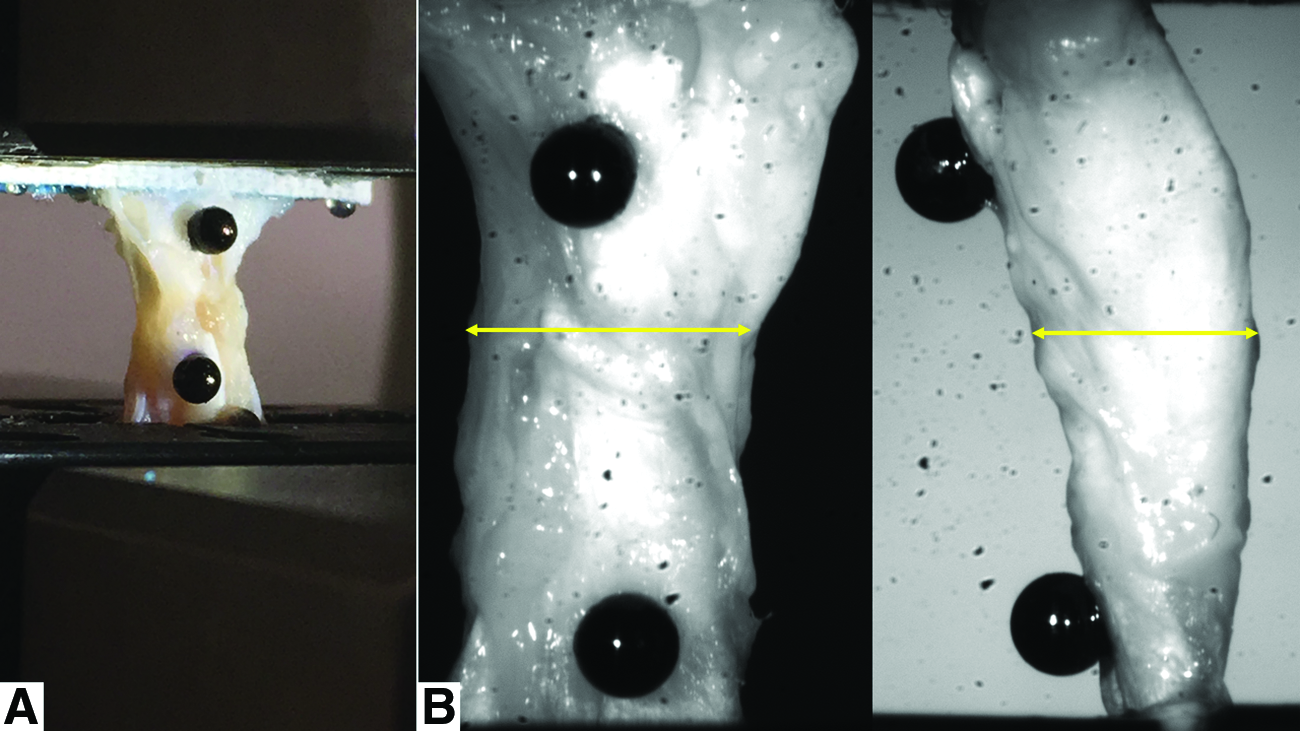
Mechanical testing setup
There were some tendons that ruptured before the preload (six tendons in the BMSC group and seven tendons in the Control groups at day 5, and one tendon in the BMSC group and three tendons in the Control groups at day 6). Paired tendons that ruptured before the preload were excluded from analysis: 11 of 20 paired tendons at day 5 and 3 of 12 paired tendons at day 6 were excluded. Overall, 9 paired tendons at day 5, 9 paired tendons at day 6, 10 paired tendons at day 7, 9 paired tendons at day 10, and 9 paired tendons at day 14 were used for gross measurements and biomechanical analysis.
Real-time polymerase chain reaction
Tissue samples at each time point (n = 5) were harvested from extra soft tissues at the lateral side of repaired tendon site and homogenized. RNA was extracted using the RNeasy RNA purification Mini Kit (Qiagen, Valencia, CA). The amount of RNA was quantified with the NanoDrop ND-1000 Spectrophotometer. One microgram of total RNA was reverse transcribed into complementary DNA (cDNA) using a High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems, Foster City, CA). The probes (Rn00574164_m1 tenomodulin [marker of tendon differentiation and maturity], 17 Rn01504576_m1 scleraxis [marker of neotendon formation], 18 and Rn01775763_g1 glyceraldehyde 3-phosphate dehydrogenase [GAPDH]) were utilized. Real-time polymerase chain reaction (RT-PCR) was performed using the TaqMan® Real-Time PCR Master Mixes on the ABI 7900HT Fast Real-Time PCR System (Applied Biosystems, Waltham, MA). Every sample was tested in triplicate for each gene. Relative gene expression levels were evaluated using the Pfaffl method (ΔΔCt method). 19
Histological analysis
After collecting the samples for RT-PCR, the tendons at each time point (n = 5 each) were fixed in 4% paraformaldehyde (pH 7.4), decalcified in 0.5M EDTA (pH 7.4), and embedded in paraffin. Five micrometer longitudinal sections parallel to the sagittal sections of the repair sites were obtained from the midline of the tendons and stained with hematoxylin and eosin (H&E). The images of the stained sections were observed under a fluorescence digital microscope (BZ-X 710 digital microscope; Keyence, Osaka, Japan). Each specimen was evaluated at the central part of the repair site according to the Bonar criteria, including the judgment of (1) tenocytes, (2) ground substance, (3) collagen fibers, and (4) vascularity.20,21 Each variable was evaluated on a four-point scoring system (0–3 points). Overall, the total score was summarized from these four variables (0–12 points; 0 points: normal tendon, 12 points: most severe abnormality detectable). The scores were determined by two blinded, independent investigators. If there was a mismatch in the judgment of any specimen between the two investigators, the specimen was examined together.
Statistical analysis
All data are expressed as mean ± standard deviation. The parametric data were assessed using paired t-tests, and Mann–Whitney U testing was used for nonparametric data. All statistical analyses were performed using GraphPad Prism 7.0 (GraphPad Software, La Jolla, CA). p < 0.05 was considered statistically significant.
Results
Cross sectional area was increased at days 5, 6, and 14
Photographs of the tendons and the cross sectional area at the repair site are shown in Figure 4. At days 5, 6, and 7, the repair sites were partially covered with soft tissue in both groups. The repair site was completely covered with soft tissue at 10 and 14 days in all specimens. The cross sectional area in the BMSC group was greater than the control group at day 5 (16.61 ± 3.29 mm2, 10.82 ± 3.10 mm2, p < 0.005), day 6 (17.67 ± 4.26 mm2, 12.85 ± 6.23 mm2, p < 0.05), and day 14 (18.67 ± 3.26 mm2, 13.73 ± 4.19 mm2, p < 0.05). There were no significant differences between the two groups at days 7 and 10.
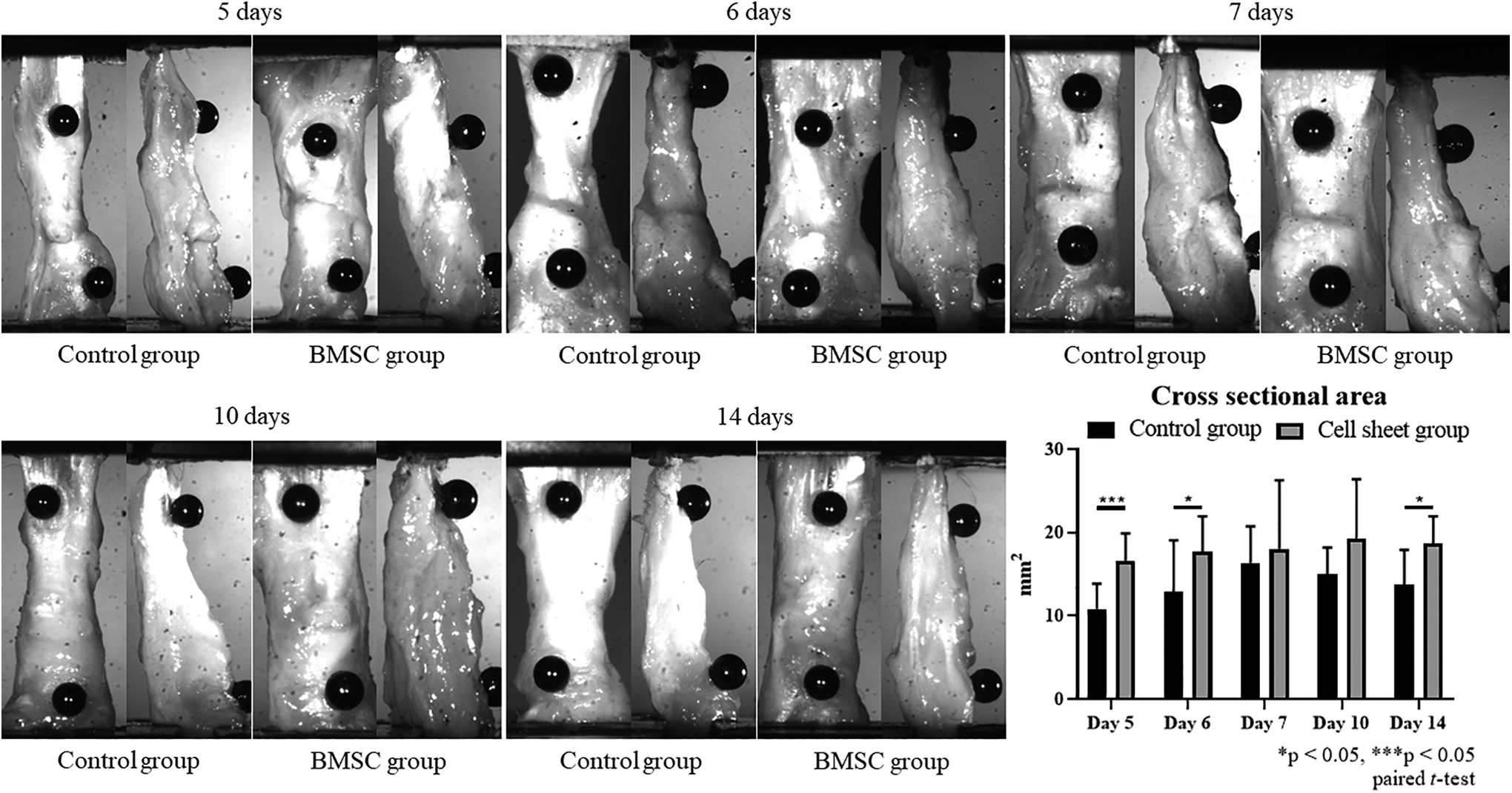
Photos of Achilles tendons and the cross sectional area at the tendon repair site. In both groups, the repair sites were partially covered with soft tissue at 5, 6, and 7 days. The repair site was completely covered with soft tissue at 10 and 14 days in all specimens. The cross sectional area of the BMSC group was greater than the control group at 5 days (16.61 ± 3.29 mm2, 10.82 ± 3.10 mm2, p < 0.005), 6 days (17.67 ± 4.26 mm2, 12.85 ± 6.23 mm2, p < 0.05), and day 14 (18.67 ± 3.26 mm2, 13.73 ± 4.19 mm2, p < 0.05). There were no significant differences between the two groups at 7 and 10 days.
Biomechanical strength was increased at days 5 and 6
The results of mechanical testing are shown in Figure 5. The maximum load to failure in the BMSC group was significantly higher than in the control group at day 5 day (4.8 ± 1.5 N vs. 3.9 ± 2.3 N, p < 0.05) and day 6 (7.3 ± 2.0 N vs. 5.0 ± 2.0 N, p < 0.05). In addition, the stiffness in the BMSC group was significantly higher than in the control group at day 5 (4.8 ± 1.4 N/mm vs. 2.9 ± 0.8 N/mm, p < 0.05) and day 6 (8.1 ± 5.2 N/mm vs. 5.4 ± 2.5 N/mm, p < 0.05). There was no significant difference in maximum load to failure and stiffness between the two groups at days 7, 10, and 14.
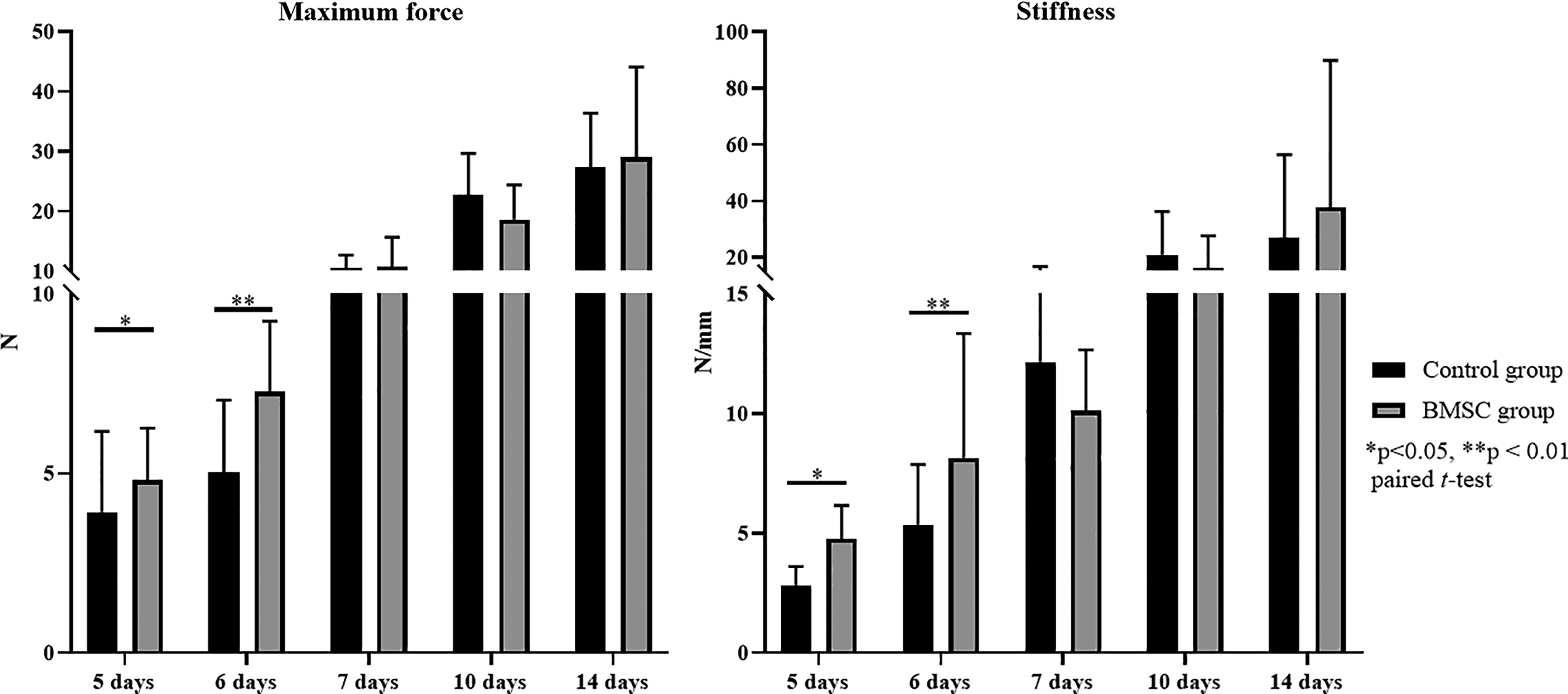
Results of mechanical testing. The maximum load to failure in the BMSC group was significantly higher than the control group at 5 days (4.8 ± 1.5 N vs. 3.9 ± 2.3 N, p < 0.05) and at 6 days (7.3 ± 2.0 N vs. 5.0 ± 2.0 N, p < 0.05). There were no significant differences between the two groups at 7, 10, and 14 days. The stiffness in the BMSC group was significantly higher than the control group at 5 days (4.8 ± 1.4 N/mm vs. 2.9 ± 0.8 N/mm, p < 0.05) and 6 days (8.1 ± 5.2 N/mm vs. 5.4 ± 2.5 N/mm, p < 0.05). There were no significant differences between the two groups at 7, 10, and 14 days.
Gene expression levels of scleraxis and/or tenomodulin were increased at all timepoints
The levels of scleraxis and tenomodulin expression are shown in Figure 6. Gene expression of scleraxis in the BMSC group at days 5, 6, 7, and 14 was significantly increased compared with the control group (p < 0.01). Similarly, gene expression of tenomodulin in the BMSC group was significantly increased at days 5, 6, 10, and 14 (p < 0.01).

Gene expression levels of scleraxis and tenomodulin. Gene expression levels of scleraxis in the BMSC group were significantly increased at 5, 6, 7, and 10 days (p < 0.05). Gene expression levels of tenomodulin in the BMSC group were significantly increased at 5, 6, 10, and 14 days (p < 0.05).
Histological evaluation at the repair sites revealed no differences
H&E staining of the specimens is shown in Figure 7. Some gapping at the surgical site was seen at days 5 and 6 in both groups. On the contrary, the gap was completely filled (“healed”) in both groups at days 7, 10, and 14. Bonar scores of the central part of the repair site revealed no significant differences at all timepoints.
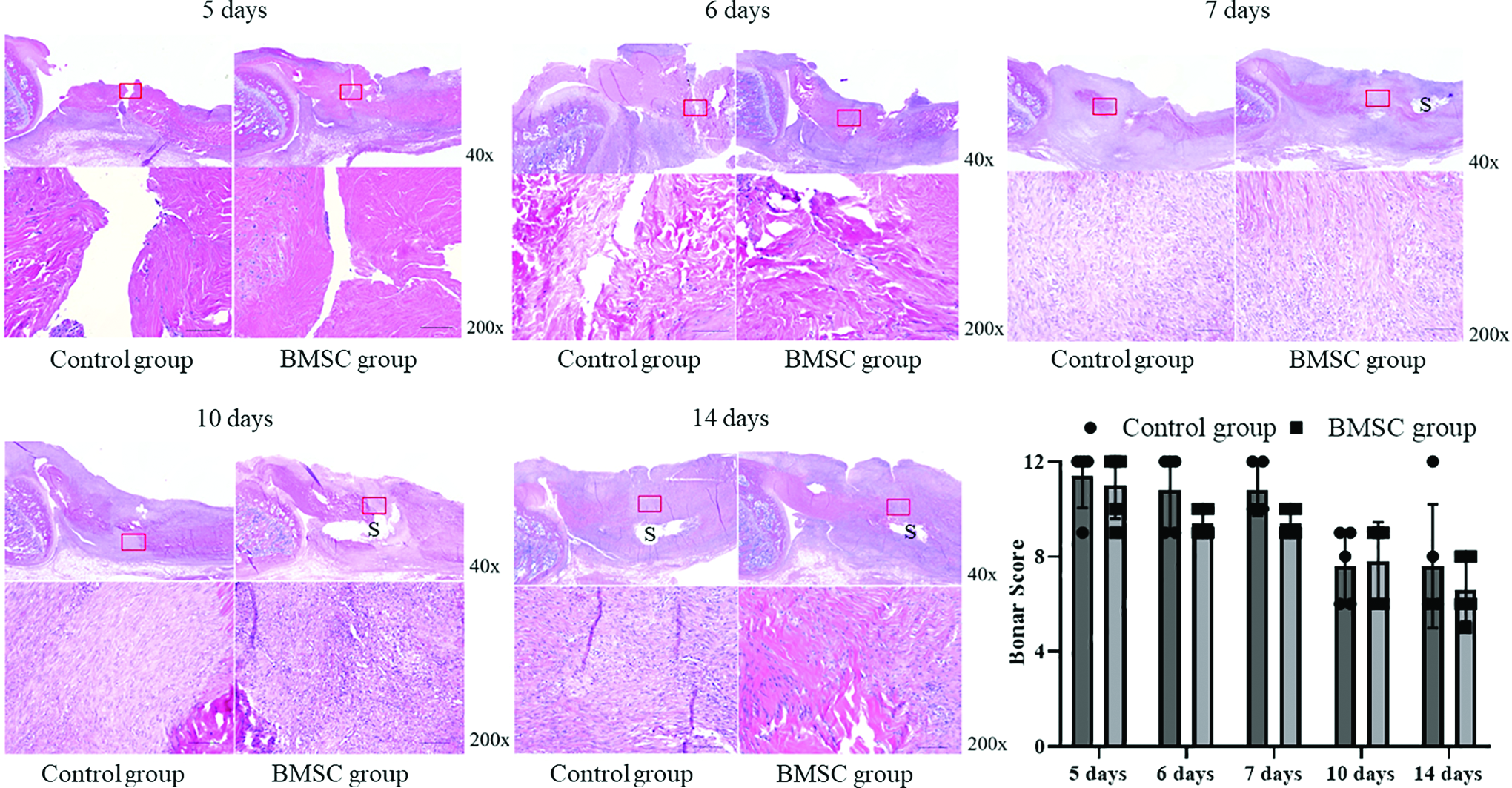
H&E staining. Slight gapping at the repair site is seen at days 5 and 6 in both groups. On the contrary, the gap is completely filled (“healed”) in both groups at days 7, 10, and 14. Bonar scores at the central part of the repair site revealed no significant differences at all timepoints. Bar: 100 μm, S: suture. H&E, hematoxylin and eosin. Color images are available online.
Discussion
Biologic enhancement of flexor tendon repairs with the addition of MSCs is an attractive concept with some promising preliminary results.10,15,22,23 The optimal delivery method of MSCs to tendon repair sites is still unknown. Local intravenous MSC injection is one described method. However, a limited and variable number of MSCs is distributed via the circulating blood to the correct site and there is relocation of these cells to other sites. 24 Injectable tendon-derived extracellular matrix hydrogel25,26 and fibrin glue27–29 have also been used as a scaffold to carry MSCs to flexor tendon repairs. However, Xu et al. 30 demonstrated that a core suture repair with fibrin glue augmentation showed increased gliding resistance compared to a core suture repair with a running epitendinous suture in human cadavers. Thus, the efficacy of fibrin glue for repair augmentation is inconclusive due to concerns of causing adhesion formation. The poly(L-lactic-co-glycolic acid) (PLGA)-based scaffolds loaded with adipose-derived MSCs was also attempted in the treatment of flexor tendons. 31 However, the strength of the PLGA-based scaffold was not investigated. Therefore, we utilized a scaffold-free BMSC sheet to deliver BMSCs to the repair site.
Quirk et al. 32 investigated the biomechanical properties of rat Achilles tendons cryopreserved at −20°C or −80°C for later testing and showed that 1–2 freeze-thaw cycles did not affect the tensile strength of tendons for short periods of time (up to 3 months). In our study, the tendons were stored at −20°C and were processed for biomechanical testing within 1 month. The tendons underwent only one freeze-thaw cycle and thus, this delayed processing was assumed to have little effect on our biomechanical evaluations.
In our study, the suture material and any adjacent tissue were removed to ensure that mechanical testing was only measuring the repair tissue. The rat Achilles tendons repaired with BMSC sheets had significantly higher maximum load to failure and stiffness at days 5 and 6 compared to the contralateral tendons repaired without BMSC sheets. Moreover, the tendons repaired with BMSC sheets showed significantly increased gene expression of scleraxis and/or tenomodulin at all timepoints. The reason for the discrepancy between our high expression of tenomodulin and scleraxis throughout all timepoints and the high biomechanical strength seen only at days 5 and 6 in our repaired tendons with the BMSC sheets is not fully known. It is evident that the cell sheets led to increased tenogenesis as evidenced by the increased gene expression at all time points. In fact, the BMSC sheets were not induced to tenogenic differentiation (without stretching or adding tenogenic growth factors) during cell culture. Thus, the high expression of scleraxis and tenomodulin clearly reflects improved tendon regeneration by the BMSC sheets compared with the normal healing tendons. However, based on our data, the aforementioned increased tenogenesis was only biomechanically relevant (leading to significantly increased strength) at days 5 and 6. These results suggest that although there is clearly augmented tenogenesis in the presence of cell sheets, this augmentation does not lead to significantly improved biomechanical strength over normal tendon healing at all timepoints, but rather only early in the healing process (days 5 and 6). This, in fact, supports our ultimate hypothesis that early tendon healing may be augmented with this cell-based augmentation. Therefore, these results suggest that the increased biomechanical strength afforded by BMSC sheet implantation into tendon repair sites may allow for the earlier onset of rehabilitation and improved clinical outcomes in flexor tendon surgery.
Although the cross sectional area of the tendons repaired with BMSC sheets was significantly larger at days 5, 6, and 14, H&E staining revealed that the Bonar score at the central part of the repair site showed no significant difference between groups. These results indicate that BMSC sheets may contribute to the increased amount of soft tissue around the repair site (extrinsic healing), but may have less effect on healing within the gap (intrinsic healing). Extrinsic healing has been related to tendon adhesions.2,33 The degree of tendon adhesion formation was not evaluated in this study. Thus, further study will be needed to find the optimal use of these MSC sheets in vivo.
There are some limitations in this study. First, the rat Achilles tendon repair model was utilized due to its relatively low cost. However, the hind limb in rats is anatomically different from humans. There may be different effects of MSCs treatment on Achilles tendons and flexor tendons due to the differences between extrasynovial and intrasynovial tendon healing. 34 Therefore, the findings in this model might not be directly translatable to the human hand.
Second, although the sciatic nerves were transected to avoid tendon ruptures, 14 of 190 repaired tendons (7%) were still ruptured. In our previous experience, cast immobilization was applied. However, in that series, 49% of the repaired tendons ruptured. 15 Thus, although transection of the sciatic nerve was performed to avoid tendon ruptures, nerve transection is never performed in the clinical setting of flexor tendon surgery.
Finally, tendon healing was only evaluated at the early phase of tendon healing (time points: 5, 6, 7, 10, and 14 days). These timepoints were chosen because in our previous rat model study, 15 the bioactive cell-coated sutures enhanced tendon repair strength at the early phases (7–10 days), but there were no significant effects at later stages (14–28 days). Tendon healing with scar formation is biomechanically inferior to a native tendon, and this can lead to tendon reruptures. This current study neither specifically evaluate the repaired tendon at later stages nor did it explore whether BMSC sheets could prevent scar formation. This will be the focus of our ongoing studies utilizing this concept. Currently, it is well accepted that the earlier onset of rehabilitation decreases adhesion formation and increases the biomechanical properties of the tendon during its healing process, resulting in the reduction of reruptures. 35 Therefore, we are most interested in the augmentation of the early phases of tendon healing as this is where clinically the most improvement may be made. The focus of this current study is to explore the possibility of optimizing the early phase of tendon healing. We believe that this biological optimization of healing will be critical for allowing the earlier onset of rehabilitation, resulting in the improvement of the prognosis following flexor tendon surgery.
In conclusion, BMSC sheets interposed into a rat Achilles tendon repair site biomechanically improved early healing. Gene expression of scleraxis and tenomodulin was also enhanced. Therefore, although further study is needed, BMSC sheet implantation into tendon repair sites may allow for accelerated healing and, furthermore, the earlier onset of rehabilitation and potentially improve clinical outcomes in flexor tendon repair.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this project was provided by Johnson Family Fund, Stanford University Department of Orthopaedic Surgery.