
Abstract
The difficulty in the regeneration of cardiomyocytes after myocardial infarction is a major cause of heart failure. Together, the amniotic membrane and 15-deoxy-Δ12,14-prostaglandin J2 (15d-PGJ2) can help in the recovery of cardiomyocyte, as they present many growth factors and anti-inflammatory effect, respectively. The objective of this study is to compare the efficacy of Human Decellularized Amniotic Membrane Scaffold (AHAS) loaded with 15d-PGJ2 in improving ventricular function in a rat model of postinfarct ventricular dysfunction. Myocardial infarction was induced in 24 rats by left coronary occlusion. After a week, the animals were subjected to echocardiography for evaluation of left ventricle ejection fraction (LVEF), left ventricle end diastolic volume (LVEDV), and left ventricle end systolic volume (LVESV). Animals with ejection fraction <40% were included in the study and were randomized into three groups: control (n = 8), AHAS (n = 8) and AHAS +15d-PGJ2 (n = 8). In the AHAS group only the membrane was implanted, whereas in the AHAS +15d-PGJ2 the membrane +15d-PGJ2 was implanted on myocardial infarction. Echocardiographic evaluation was performed after 1 month. For histological analysis, heart tissue was stained with Gomori trichome, Sirius Red, the antibody against CD31 and connexin 43 (Cx43). There were no significant differences in the baseline LVEF, LVEDV, and LVESV in all groups. After 1 month, ejection fraction decreased in the control group but increased in the AHAS group and in the AHAS +15d-PGJ2 group in comparison with the control group. The LVEDV and LVESV in the AHAS and AHAS +15d-PGJ2 groups decreased compared with the control group, featuring a ventricular antiremodeling effect. Histopathology of the infarcted area identified the reduction of infarct size and collagen type 1 in the AHAS and AHAS +15d-PGJ2 groups. New blood vessels and cardiomyocytes have been identified in an infarcted area by CD31 and Cx43. AHAS +15d-PGJ2 provided an increase in the ejection fraction and prevented ventricular dilation in this postinfarction ventricular dysfunction model.
Impact Statement
Our study demonstrated reduction of myocardial fibrosis, proliferation of cardiomyocytes and increase in ejection fraction in rats after experimental acellular amniotic membrane scaffold (AHAS) carrying nanoparticles of 15d-PGJ2 scaffold engraftment in infarcted myocardium. AHAS grafts facilitated colonization of fibrotic myocardium regions with new contractile cells, in addition to preventing reduction of left ventricle wall thickness. This contribution is theoretically and practically relevant as current literature describes experimental studies performed on cardiac ischemic models which present conflicting results concerning cell types used in a research model.
Introduction
Cardiovascular disease (CVD) remains as the main cause of death worldwide. 1 Cardiac dysfunction has been associated with poor prognosis in patients after acute myocardial infarction (AMI). AMI is characterized by the loss of functional cardiomyocytes as a result of ischemic injury that leads to ventricular failure. 2
Therefore, the development of biomaterials is of great importance not only to stop the mechanisms underlying cardiac dysfunction but also to explore new therapies that can prevent the progression of the pathological process. 3
Some biomaterials such as bovine pericardial and the submucosa of the intestine have already been used as tissue repair in the heart despite the drawbacks of calcification and high immunogenicity.4,5 Human Decellularized Amniotic Membrane Scaffold (AHAS) has been used as a pericardial substitute, with interesting results. Owing to the low immunogenicity of the AHAS and the fact that it has many growth factors in its structure, it could help in the recovery of the infarcted myocardium.6,7
In contrast, the 15-deoxy-Δ12,14-prostaglandin J2 (15d-PGJ2) is implicated in the normalization of inflammatory processes and a previous study has demonstrated that 15d-PGJ2 causes a substantial reduction of myocardial infarct size in the rat.8–11
Synthetic or natural nanoparticle (NP) are defined as having diameters between 0.1 and 100 nm, and are composed of biocompatible materials able to incorporate lipophilic drugs avoiding drug degradation, decreasing toxicity, improving efficacy, and prolonging the pharmacological activity of the loaded active compounds. 12
The objective of this study is to compare the cardiac function improvement of AHAS with and without 15d-PGJ2 loaded NPs in a postinfarct ventricular dysfunction rat model.
Methods
The 15d-PGJ2-NC were prepared by the nanoprecipitation method, as described by Fessi et al. 12 The organic phase consisted of poly D,L-lactide-co-glycolid (PLGA) polymer (100 mg), acetone (30 mL), 15d-PGJ2 (100 μg; Sigma-Aldrich, St. Louis, MO), sorbitan monostearate (40 mg), and caprylic/capric acid triglyceride (200 mg). The aqueous phase was composed of polysorbate 80 (60 mg) and deionized water (30 mL). After the dissolution of the components in both phases, the organic phase was gradually added to the aqueous phase, and the suspension was maintained under agitation for 10 min. The solvent (acetone) was removed by evaporation, and the suspension was concentrated to a volume of 10 mL under low pressure, using a rotary evaporator, to obtain a suspension of 15d-PGJ2 with a final concentration of 10 μg/mL. After evaporation, no traces of acetone were observed in the formulation.
Preparation of acellular human amniotic scaffold
The study was approved by Hospital Pequeno Príncipe Ethical Committee for the use of biological material for research purposes under the number 0948-11. All materials were used in compliance with ethical guidelines by the Brazilian National Health Council. Fresh human amniotic membrane (HAM) was obtained after cesarean deliveries. Maternal donors provided informed consent and were serologically negative for HIV, hepatitis B and C, and syphilis. In brief, blood clots were immediately cleaned off the placenta after surgery with phosphate buffered saline (PBS) solution containing 100 U/mL penicillin and 100 mg/mL streptomycin. The AHAS was prepared as described by Riau et al. 4 Part of the HAM was then deprived of amniotic epithelial cells to obtain AHAS by sodium dodecyl sulfate in PBS, and incubated with shaking rate of 100 rpm at 37°C for 24 h. Finally, the prepared AHAS was rewashed three times with PBS.
Culture and seeding of mesenchymal stem cells with 15d-PGJ2 nanoparticle
Mesenchymal stem cells (MSCs) were isolated through bone marrow aspiration of the posterosuperior iliac crest of Wistar rats. 11 MSCs were cultured for 7 days in Dulbecco's modified Eagle medium (Invitrogen) supplemented with 10% fetal bovine serum (Invitrogen) and 100 U/mL penicillin and 100 mg/mL streptomycin at 37°C with 5% CO2. The culture medium was changed every 2 days. 13 The MSCs were seeded on a plastic plate with 15d-PGJ2-NP in a concentration of 10 μg/mL. MSCs are not part of AHAS. They were placed together with the PLGA NPs for 24 h to incorporate the NPs to the AHAS.
Cell proliferation assay
The cells were incubated with NPs for 48 h, and the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) test was performed 24 h after treatment. Cell viability assays were performed using the MTT (Fisher Scientific) assay. Cells were plated at a density of 1 × 104 cells/cm2 into 96-well tissue culture plates to ensure that they would not be over confluent after 48 h post-treatment. After 24 h, they were treated with corresponding concentrations of dimethyl sulfoxide (DMSO), control, without 15d-PGJ2 and 15d-PGJ2 loaded PLGA NPs, for 1.5 h. After 1.5 h, the treatments were washed off with 1 × PBS, and 200 μL of fresh media was added to the wells. Cells were then incubated for 48 h at 37°C, >90% humidity, and 5% CO2 conditions. After the 48-h incubation period, the media was replaced with 100 μL of phenol red free media, and 10 μL of MTT was added to each well. Plates were incubated at 37°C, >90% humidity, and 5% CO2 conditions for 4 h, after which the media and MTT were removed, 100 μL of DMSO added, and incubated at 37°C for 10 min. The plates were then read using a Thermo Fisher Scientific Multi Scan GO. Cell viability data for each treatment group (control, without 15d-PGJ2 and 15d-PGJ2 loaded PLGA NPs) was normalized to their own vehicle control cell viabilities (DMSO and Blank NPs). The supernatant was used for analysis by spectrophotometry reader in 595. 14
Scanning electron microscope
The morphology and structure of the acellular human amniotic scaffold (AHAS) with 15d-PGJ2-NC (AHAS-NC) were examined in a JEOL 1200EX II microscope (JEOL Ltd., Akishima) operating at 80 kV. To perform the scanning electron microscope (SEM) analysis, the AHAS-NC was fixed on a top coverslip, dried, mounted on a stub for SEM, fixed in 2.5% (v/v) glutaraldehyde (Sigma-Aldrich) in PBS and postfixed with 1% (v/v) and 0.1 M sodium cacodylate trihydrate (Sigma-Aldrich).
Experimental profile
Myocardial infarction and echocardiographic analysis
All experiments were performed in the cell therapy laboratory of PUCPR according to the “Guidelines for the Care of Animals,” the guiding principles approved by the American Society of Physiology. Wistar rats weighing 250–300 g were intraperitoneally anesthetized using 50 mg/kg ketamine and 10 mg/kg xylazine. The animals were submitted to endotracheal intubation, without exposure of the trachea, and to mechanical ventilation at a frequency of 60 cycles/min and a volume of 2.5 mL (“683” Harvard® Apparatus, Inc.). All animals were submitted to left lateral thoracotomy and ligature of the left coronary artery with 7.0 polypropylene thread (Ethicon®, Inc., Somerville, NJ) for inducing myocardial infarction of the left ventricle anterolateral wall. The detailed operation procedure was previously described by Guo-Pan et al. 15 The mortality rate of the animals submitted to this procedure was 20%.
Seven days after myocardium infarction, the animals were again submitted to anesthesia using 50 mg/kg ketamine and 10 mg/kg xylazine intraperitoneally. Also, a bidimensional transthoracic echocardiographic evaluation was made using a Hewlett Packard Sonos model 5500, with S12 sectorial (5–12 MHz) and 15L6 linear (7–15 MHz) transducers developed for the ultrasonographic study of small animals, allowing an analysis up to 160 Hz. The transducer was placed in the left anterolateral portion of the thorax, and the heart was imaged as a bidimensional axial view of the left ventricle with the mitral and aortic valves and the apex in the same image. The digital conversion of the image was obtained by a delimitation of the interventricular septum and the left ventricle posterior wall. Subsequently, the following measurements were taken: final systolic and diastolic surfaces, final diastolic and systolic lengths of the left ventricle and heart rate to calculate the final systolic volumes (left ventricle end systolic volume [LVESV], mL), left ventricle end diastolic volumes (LVEDV, mL), and the left ventricle ejection fraction (LVEF %) using Simpson's method. All the dimensions were blindly measured three times by the same echocardiologist, after which the mean of each parameter was calculated.
Only animals with LVEFs of <40% were included in this study and were randomized into three groups consisting of eight animals each: control, AHAS, and AHAS +15d-PGJ2. The scaffold alone was implanted on the AHAS group, and the AHAS +15d-PGJ2 NPs were implanted on the scaffold +15d-PGJ2 group, both on the anterolateral wall of the infarcted left ventricle (Fig. 1). Control rats underwent sham operations using the same method, but without the implantation of the amniotic membrane. All rats received perioperative analgesia after surgery and a new echocardiographic evaluation was performed 1 month after scaffold implantation.
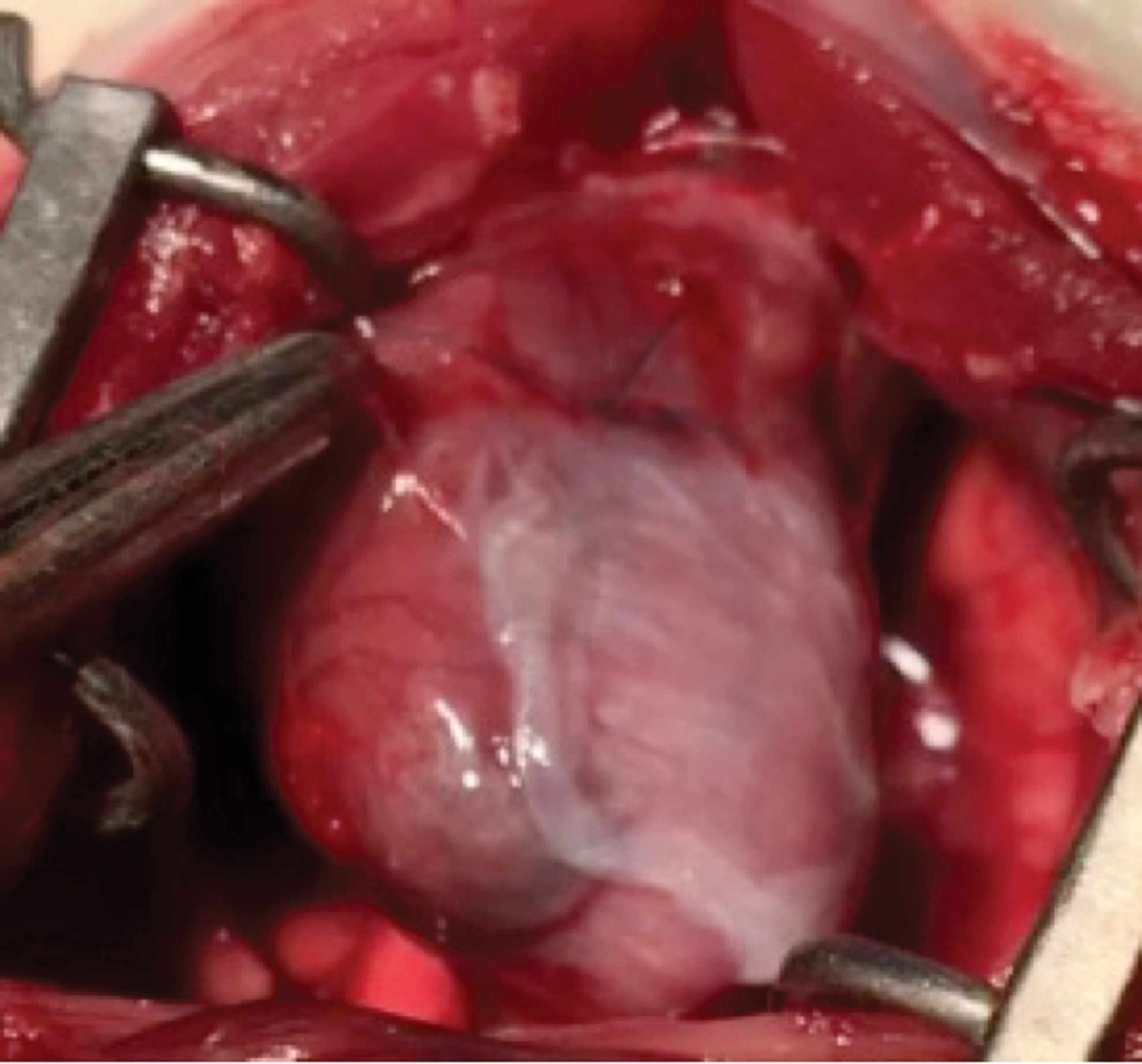
Intraoperative view of the mouse heart through sternotomy. The LAD has been ligated with a 7.0 prolene suture, which has also been used to attach the AHAS +15dPGJ patch. AHAS, Human Decellularized Amniotic Membrane Scaffold. Color images are available online.
Histological analysis
The hearts were removed and fixed in 10% phosphate-buffered formaldehyde. Specimens were embedded in paraffin blocks, sectioned at 5 μm-thick slices (four sections per sample), subjected to Gomori trichrome staining, and examined under a light microscope. Digital images for epicardial and endocardial circumferences, areas, LV free wall, and infarct size were captured by Zeiss Axiovert S100 TV microscope (Zeiss, Jena, Germany) and Image Tool 2.0 (UTHSCSA, San Antonio, TX). The infarct size in each heart was calculated as the percentage of infarct scar relative to the outer circumference of the LV free wall with collagen Sirius Red-positive. The fixed tissues were sectioned and stained with primary mouse antibodies against CD31 (ab64543, 1:100; Abcam) to facilitate the quantification of vascular density in the border zone, with secondary antibodies of antirabbit Rhodamine (31665, 1/1:200; Thermo Fisher Scientific) and Connexin 43 (Cx43). The rabbit polyclonal anti-Cx43 antibody (Zymed Lab., Inc., Lot. No. 30476831) utilized to quantify the connexons was used at dilutions of 1:200 as the primary antibody and goat antirabbit IgG (Molecular PROBE, Alexa Fluor 488, Lot. No. 35068A). Finally, sections were incubated with 4′,6-diamidino-2-phenylindole (DAPI) mounting medium to provide nuclear staining (5 mL/section, DAPI H-1200, Vectashield). Negative controls were obtained from sections stained with secondary antibody only. Two blinded observers counted the number of vessels per high-power field, in five fields per slide, and the mean of vessels/field was used for subsequent analysis. The collagen fibers concentration was measured by the polarization colors in Picro Sirius Red-stained tissue sections.
Statistical analysis
The statistical analysis was performed by commercially available software (Prism 6.0; GraphPad Software, Inc., La Jolla, CA). All results were expressed as the mean ± standard deviation or standard error of the mean (Figs. 2 and 4–6), and differences were statistically analyzed by one-way or two-way analysis of variance followed by post hoc Bonferroni's multiple comparison tests. Values of p < 0.05 were considered significant.
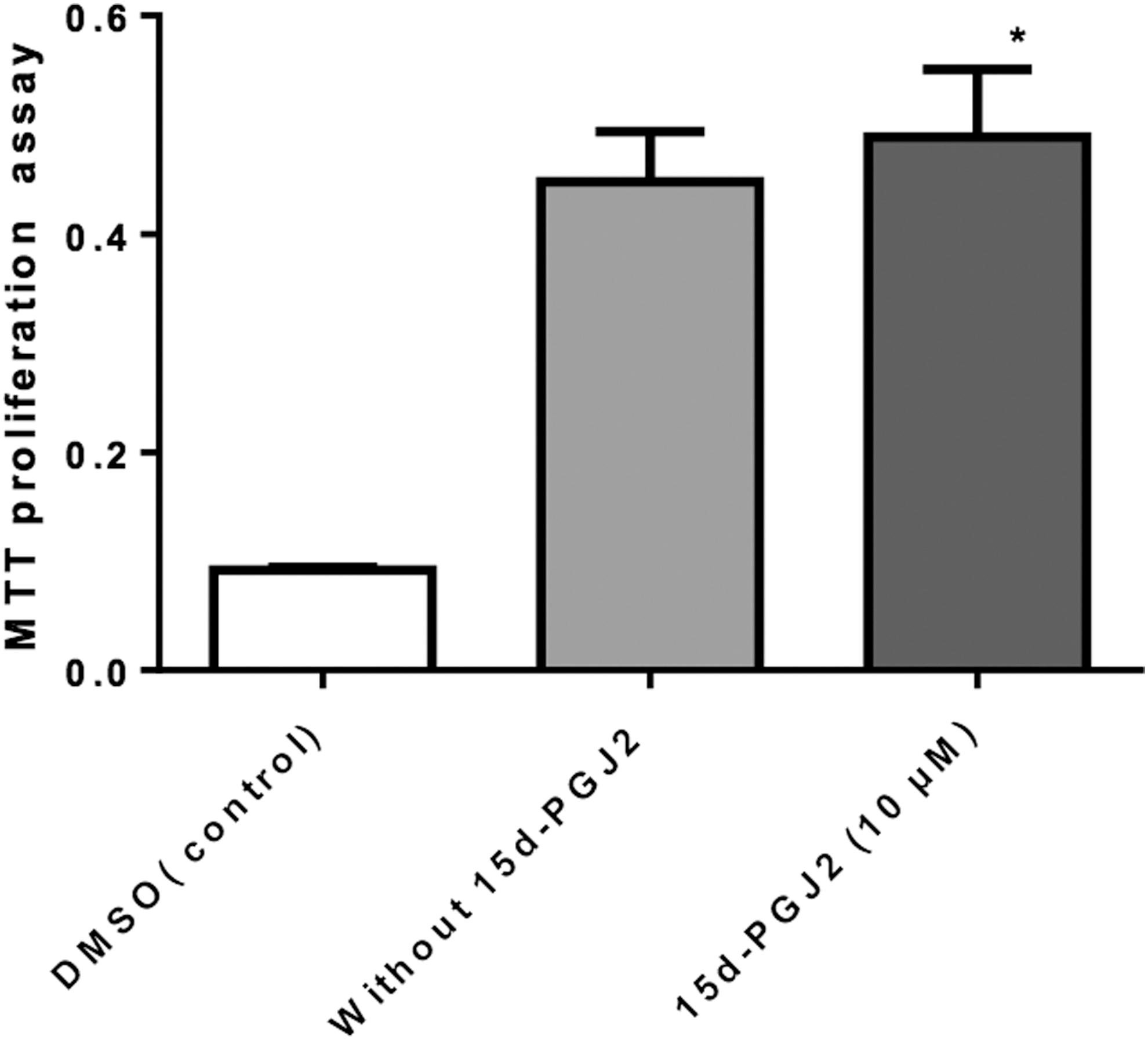
Effect of 15d-PGJ2 on the viability of mesenchymal cells. Mesenchymal cells were treated with DMSO at a concentration of 10 μM of 15d-PGJ2 for 24 h and the survival rate was analyzed using an MTT test. ANOVA p < 0.001. MTT index. Data are expressed as the mean ± standard error of the mean; ANOVA p < 0.001; post hoc comparison tests: *p < 0.001 versus control. 15d-PGJ2, 15-deoxy-Δ12,14-prostaglandin J2; ANOVA, analysis of variance; DMSO, dimethyl sulfoxide; MTT, 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide.

Phase contrast images of the acellular amniotic membrane

Intragroup comparison of the echocardiography. AHAS (acellular HAM scaffold), AHAS +15d-PGJ2 (acellular HAM scaffold +15d-PGJ2), LVEDV, LVESV, LVEF. HAM, human amniotic membrane; LVEDV, left ventricle end diastolic volume; LVEF, left ventricle ejection fraction; LVESV, left ventricle end systolic volume.

Comparison of echocardiographic measurements among groups at baseline and at 1 month.
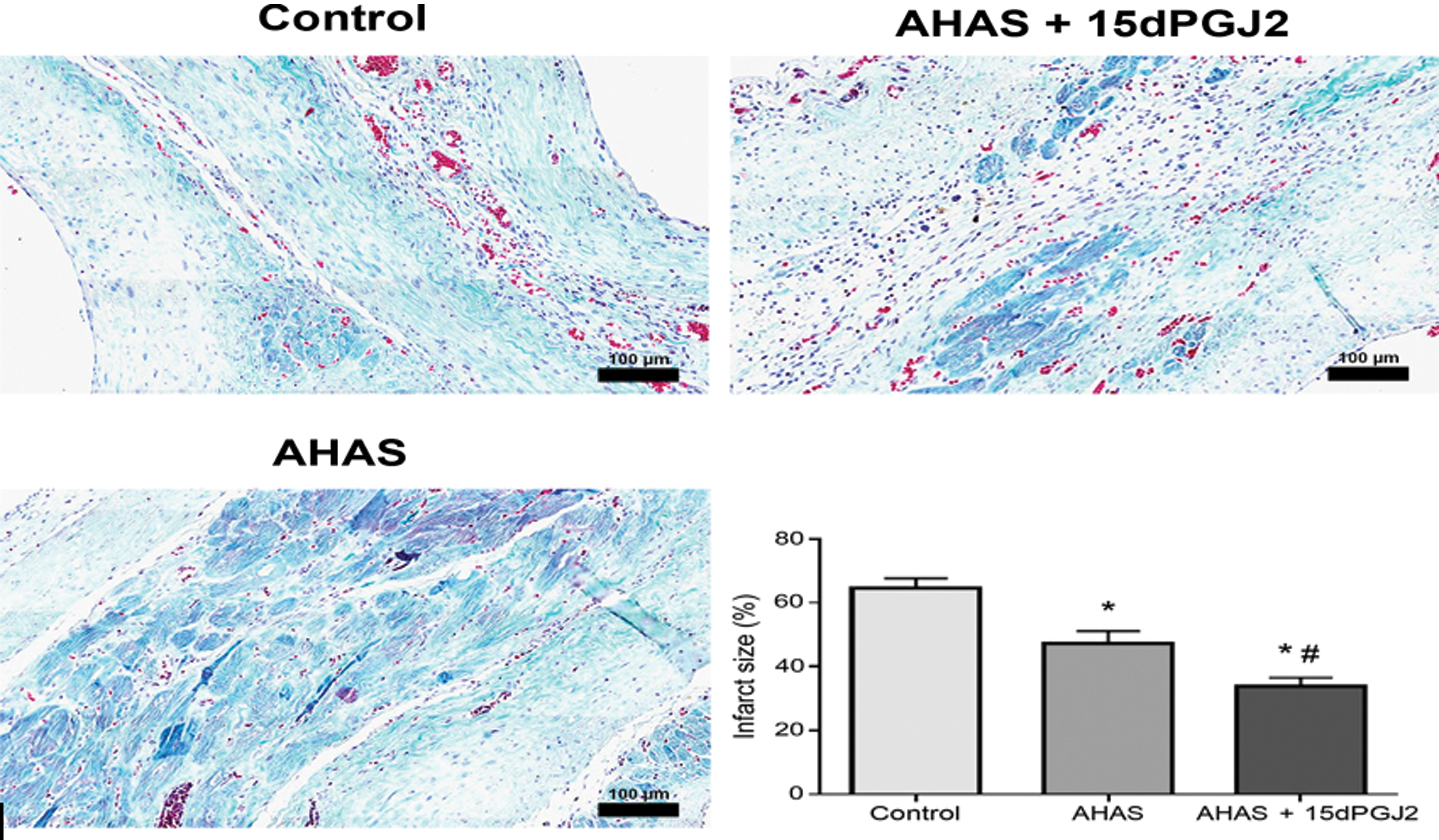
Representative Gomori trichrome stained heart sections obtained from hearts 1 month after surgery. Scar tissue is identified by blue. Quantitative analysis of infarct size. Data are expressed as the mean ± standard error of the mean; ANOVA p < 0.001; post hoc comparison tests: *p < 0.001 versus control, #p < 0.01 versus AHAS. Color images are available online.
Results
Evaluation of cytotoxicity—MTT assay
The cytotoxicity of NPs with and without 15d-PGJ2 was quantitatively evaluated on MSCs by MTT assay (Fig. 2). Results clearly demonstrate that at the concentration of 10 μM, with 15d-PGJ2, NPs showed 53.20% cell viability, whereas without 15d-PGJ2 the cell viability decreased to 46.60%.
Acellular human amniotic scaffold analysis (in vitro)
Phase contrast images of decellularized HAM scaffolds (Fig. 3A). Morphological rearrangement of cells after 24 h incubation with 15d-PGJ2 NPs (Fig. 3B).
SEM examination of decellularized human amniotic scaffolds showing migration and ingrowth of seeded mesenchymal cells and homogeneous spherical aggregates after 24 h of cell culture (Fig. 3C, D).
Echocardiographic analysis
Separate analysis for each group
There was no statistical difference in LVEF, LVESV, and LVEDV parameters in all animals studied when compared with the baseline values. In this way, the groups were considered homogeneous. One month after scaffold implantation, the LVEF decreased significantly in the control group from 33.13% ± 2.75% to 28.13% ± 3.8% (p = 0.008), increased in the AHAS group from 35.38% ± 2.67% to 38.88% ± 4.29% (p = 0.082) and increased significantly in the AHAS +15d-PGJ2 group from 33.5% ± 5.07% to 38.88% ± 3.14% (p = 0.004). The LVESV, over the same time interval, increased in the control group from 0.305 ± 0.178 mL to 0.380 ± 0.182 mL (p = 0.854), and decreased in the AHAS group from 0.168 ± 0.039 mL to 0.161 ± 0.052 mL (p > 0.9999) and in the AHAS +15d-PGJ2 group from 0.290 ± 0.143 mL to 0.179 ± 0.063 mL (p = 0.356). The LVEDV, over the same time interval, showed significant increases in the control group from 0.350 ± 0.362 mL to 0.569 ± 0.274 mL (p = 0.007), stabilized in the AHAS group from 0.260 ± 0.058 mL to 0.262 ± 0.074 mL; p > 0.9999, and decreased in the AHAS +15d-PGJ2 group from 0.418 ± 0.19 mL to 0.292 ± 0.094 mL (p = 0.185) (Fig. 4).
Groups comparison
One month after the scaffold implantation, statistical differences were identified in LVEF when comparing the control versus AHAS groups (p < 0.0001) and the control versus AHAS +15d-PGJ2 groups (p < 0.0001). No difference between the AHAS and AHAS +15d-PGJ2 groups was identified. Regarding the LVESV, statistical differences were identified among the control versus AHAS and control versus AHAS +15d-PGJ2 groups (p = 0.0072 and p = 0.0154, respectively). No difference between the AHAS and AHAS +15d-PGJ2 groups was identified.
In respect to the LVEDV, differences were identified among the control versus AHAS and the control versus AHAS +15d-PGJ2 groups (p = 0.0020 and p = 0.0056, respectively). No difference between the AHAS and AHAS +15d-PGJ2 groups was identified (Fig. 5)
Histology
The infarct size determined in the Gomori trichrome-stained sections was 64.59% ± 2.84% in the control group, 46.63% ± 10.42% in the AHAS group, and 34.04% ± 6.62% in the AHAS +15d-PGJ2 group, with p < 0.001 for all groups (Fig. 6). The collagen type determined in histological sections showed that the collagen type I (content index) was 166.8% ± 11.2% in the control group, 98.68% ± 7.4% in the AHAS group, and 32.7% ± 5.3% in the AHAS +15d-PGJ2 group with p < 0.001 for all groups (Fig. 7).

Images from Sirius Red staining were obtained with circularly polarized light. Collagen type I (red fibers) was more predominant in the scar from animals treated with AHAS +15dPGJ than with collagen type III (green fibers). Scale bars, 50 μm. Collagen type I content index. Data are expressed as the mean ± standard error of the mean; ANOVA p < 0.001; post hoc comparison tests: *p < 0.001 versus control, #p < 0.001 versus AHAS. Color images are available online.
CD 31 and Cx43
There was an increase in myocardial antibody CD31 (vessels) and Cx43 (gap junction) concentration in the AHAS and AHAS +15d-PGJ2 groups when compared with control (Fig. 8).

Control group negative for CD31 and Cx43. AHAS and AHAS +15dPGJ groups positive for CD31 antibody and Cx43 (expressed gap junction formation and DAPI-stained blue nuclei). The bar scale is 50 μm. The 15d-PGJ2 were characterized and the results showed a mean size distribution of 158 nm, polydispersion of 0.082 and zeta potential of −24.6 mV. The nanoformulation was also characterized by atomic force microscopy and transmission electron microscopy and the results showed that the nanocapsules presented a spherical shape without any aggregates. Cx43, connexin 43; DAPI, 4′,6-diamidino-2-phenylindole. Color images are available online.
Discussion
The treatment for the CVDs is one of the core targets of new regenerative medicine. Previous experimental studies performed on cardiac ischemic models have aimed to investigate the efficacy of cell therapy on cardiac repairment of different cell types, including bone marrow-derived cells,16,17 skeletal myoblasts,18,19 and fetal cardiomyocytes,18,13 However, results are still conflicting concerning the type of cell to be used and in each research model, especially when we seek the transmural fibrosis regeneration. Some studies with skeletal myoblasts suggest recolonization with new muscle fibers without integration with the native myocardium, 19 whereas bone marrow stem cells feature integration with the native myocardium, but with little ability to regenerate from the myocardial fibrosis. 16
The main goal of scaffold implantation in the infarcted myocardium is to stimulate the colonization of the fibrotic region with new contractile cells to recover the left ventricle function. The great advantages of AHAS are its low immunogenicity, a large number of growth factors and the fact that it is technically easy to use. It has recently been shown that transplantation of placental fetal membrane-derived cells into ischemic rat hearts results in a reduction of cardiac scar size as well as an improvement in cardiac contractile function, with less reduction of left ventricle wall thickness.18,21 It was demonstrated that AHAS is nontoxic for cardiomyocytes and can be incorporated into the heart tissue over time, what might be characterized by positive Cx43 identified in the myocardium infarcted. The acellular human membrane scaffold preserves growth factors and other proteins that maintain the alignment of collagen fibers and could release paracrine factors to promote vascular endothelial differentiation and prevent the apoptosis. 20 Another important consideration is that decellularized amniotic membrane has shown to possess the same elasticity and tensile strength in vitro.24,25 In this study, AHAS +15d-PGJ2 cultivated with cells was used as a biocompatible biomaterial model that preserves different intrinsic growth factors, promotes differentiation, and prevents apoptosis in the myocardium. A model of chronic myocardial infarction with pre-established fibrosis has demonstrated that AHAS +15d-PGJ2 provides cardioprotection by reducing cardiac dysfunction. The results showed that the ejection fraction in AHAS +15d-PGJ2 group increased satisfactorily followed by a ventricular antiremodeling effect that was also observed by Cargnoni et al. 21 and Fang et al. 22 In previous studies related to myocardial tissue regeneration, results of therapy using bone marrow cells, fetal cardiomyocytes and skeletal myoblasts in the same model of transmural myocardial fibrosis, failed to reduce the ventricular remodeling.16–18 Those results are very different from that revealed in this study, which demonstrates a preservation of ventricular dilatation. This finding can be justified by some considerations.
Other studies with cell therapy by directly cellular injection in the anterior wall of the left ventricle are different from the model used in this article because the AHAS was deployed on the anterolateral wall of the left ventricle, not injected, which may decrease the deleterious effects of cell injection, mainly the inflammatory reaction and the high rate of cell death. Another justification for interesting antiremodeling effect may be related to the delivery of stem cells. Owing to the great loss of cells at the time of the cell implant, the amniotic membrane will eventually settle for more time on the site allowing a cardioprotective effect in the ischemic heart, probably through paracrine mechanisms.
One of the ways to deliver the NPs drugs to the myocardium would be direct injection into the infarcted region; however, this method is known to have a high mortality rate due to the inflammatory reaction and the trauma of the injection itself. Thus, as the AHAS was placed on the infarcted region, (being adhered to the infarcted myocardium and the NPs of 15d-PGJ2 as well), so it is suggested that the NPs adhered to AHAS may have less inflammatory reaction and less trauma to delivery. Based on this context, it is believed that these two aspects may have contributed to the functional improvement of the treated animals.
In contrast, therapy with bone marrow cells and myoblasts cells in chronic myocardial infarction did not exert the antiremodeling effect, probably because of the ability of the stem cells to regenerate only blood vessels, and not cardiac myocytes, due to the lack of integration of myoblasts with myocardial native tissue. 23 It was also observed a decrease in the cardiac infarcted area, a reduction in the amount of collagen type I, and the presence of new cardiomyocytes and blood vessels in the myocardial fibrosis region of the AHAS +15d-PGJ2 treated group.
No difference in any of the echocardiographic parameters evaluated was identified between the AHAS and AHAS +15d-PGJ2 groups, except to LVEF after 1 month (28.13 ± 3.8 in control and 38.88 ± 3.14 in AHAS +15d-PGJ2, p = 0.004). These findings suggest that the anti-inflammatory effect of NPs may have contributed to the functional benefit in treated group. It has been reported that amniotic membrane is able to release cytokines that have potent anti-inflammatory effects (interleukin-10 and interleukin-6). 26 The 15d-PGJ2 loaded NPs act as local reservoirs of anti-inflammatory interleukin that, when administered in low doses, is able to recruit host endothelial cells and provides tissue regeneration. 27 In this study, the AHAS adhered well to the heart with electrical conductance of the gap junction, as can be observed with the increase of Cx43. In addition, the implanted NPs provide a base for the development of new vessels that connected the underlying myocardium and reverse remodeling, which has been verified as the general recovery of cardiac function in the AHAS and AHAS +15d-PGJ2 groups. The use of amniotic membrane as a treatment for myocardial fibrosis offers the advantages of having plentiful supply and applicable without the need for any cell isolation or culture process, which makes it a low-cost approach. Furthermore, amniotic membrane has good preservability 28 and is immunologically well tolerated. 29
Conclusion
This study reports the evaluation of a novel way to deliver NPs loaded with 15d-PGJ2 to prevent myocardial dysfunction using as acellular amniotic membrane scaffold. In summary, we evaluated the therapeutic effect of acellular membrane scaffold isolated and carrying NPs of 15d-PGJ2 on infarcted myocardium. We observed enhanced angiogenesis, reduced myocardial fibrosis, proliferation of cardiomyocytes and, as outcome, increase in the ejection fraction of the left ventricle with preservation of ventricular dilatation in both groups treated with acellular membrane scaffold, alone and in combination with NPs loaded with 15d-PGJ2.
Footnotes
Acknowledgment
We thank Pelé Pequeno Principe Institute for providing acellular human membrane scaffold.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financially supported by the Brazilian National Research Council (CNPq 09/2018).