
Abstract
With the expected rise in patients undergoing refractive lenticule extraction worldwide, the number of discarded corneal stromal lenticules will increase. Therefore, establishing a lenticule bank to collect, catalog, process, cryopreserve, and distribute the lenticules (for future therapeutic needs) could be advantageous. In this study, we validated the safety of lenticule banking that involved the collection of human lenticules from our eye clinic, transportation of the lenticules to a Singapore Ministry of Health-licensed lenticule bank, processing, and cryopreservation of the lenticules, which, after 3 months or, a longer term, 12 months, were retrieved and transported to our laboratory for implantation in rabbit corneas. The lenticule collection was approved by the SingHealth Centralised Institutional Review Board (CIRB). Both short-term and long-term cryopreserved lenticules, although not as transparent as fresh lenticules due to an altered collagen fibrillar packing, did not show any sign of rejection and cytotoxicity, and did not induce haze or neovascularization for 16 weeks even when antibiotic and steroidal administration were withdrawn after 8 weeks. The lenticular transparency progressively improved and was mostly clear after 4 weeks, the same period when we observed the stabilization of corneal hydration. We showed that the equalization of the collagen fibrillar packing of the lenticules with that of the host corneal stroma contributed to the lenticular haze clearance. Most importantly, no active wound healing and inflammatory reactions were seen after 16 weeks. Our study suggests that long-term lenticule banking is a feasible approach for the storage of stromal lenticules after refractive surgery.
Impact statement
Since 2011, close to 3 million refractive lenticule extraction procedures have been performed. The majority of the extracted lenticules are discarded. The lenticules could have been cryopreserved and retrieved at a later date for therapeutic or refractive applications. Therefore, establishing a lenticule bank to collect, catalog, process, cryopreserve, and distribute the lenticules could be advantageous. In this study, we simulated a lenticule banking service in a validated health authority-licensed facility and showed that long-term cryopreservation of the lenticules in the facility was safe and feasible in vivo.
Introduction
The advent of femtosecond lasers has revolutionized the field of ophthalmology, particularly in the field of refractive surgery. Since the first report of its clinical application to perform intrastromal incisions in 2003, 1 femtosecond lasers have been widely adopted in laser in situ keratomileusis (LASIK), cataract surgery, and corneal transplantation.2,3
Recent advancement in femtosecond laser technology has seen the emergence of small incision lenticule extraction (SMILE), in which the laser cuts a series of intrastromal incisions, to fashion a refractive lenticule. 4 The lenticule typically has a diameter between 6.00 and 7.00 mm with varying thickness depending on the attempted refractive correction and is extracted from 110 to 120 μm depth, from the epithelium. The refractive change results from the extraction of the lenticule, the geometry of which determines the lenticular refractive properties. This is in contrast to LASIK, which requires an excimer laser for photoablation, after 7.9-mm-diameter flap creation, to change the refractive profile of the cornea.
Close to 3 million SMILE procedures have been performed, mainly in Asia and Europe since 2011. 5 SMILE, which is a proprietary technology of Carl Zeiss Meditec (Jena, Germany), received the U.S. Food and Drug Administration (FDA) approval in 2016. 6 The procedure has been gaining acceptance as a safe and effective alternative to LASIK.7,8 More recently, other laser manufacturers, such as Ziemer Ophthalmic Systems (Port, Switzerland) with the Femto Leonardo Da Vinci (LDV) system and Schwind (Kleinostheim, Germany) with the ATOS system, have recently introduced software upgrades that are also capable of performing refractive lenticule extraction. With the increasing number of refractive lenticule extraction cases being performed worldwide, the pool of extracted lenticules that are disposed of after the procedure will also increase.
In 2012, we were the first to demonstrate the safety and viability of implanting stromal lenticules that were cryopreserved in a laboratory setup, to alter the refractive properties of the rabbit corneas. 9 Our study showed that rather than being disposed of, the refractive lenticules could be cryopreserved in an eye/lenticule bank and retrieved at a later date for implantation. 10 After our study, refractive lenticules, either fresh or after short-term cryopreservation, have been implanted in patients for the treatment of keratoconus,11,12 hyperopia,13,14 presbyopia, 15 and corneal perforation. 16 Others have also suggested the potential application of the lenticules as cell carriers for corneal tissue engineering.17–19
With the possible expanding indications of use of the lenticules and the expected increase in the refractive lenticule extraction cases worldwide, it would be beneficial to set up a validated licensed independent lenticule banking service. Intrastromal keratoplasty can be performed using fresh lenticule, but that would require coordination of two surgeries (refractive lenticule extraction and intrastromal keratoplasty) running in tandem, which may not occur regularly.20,21 It would be a more common occurrence to use a cryostored lenticule at the time required. Hence, the primary purpose of the lenticule banks would be to coordinate procurement, catalog, long-term cryopreservation, and processing and distribution of lenticules. They would also provide a quality control of all the processes to conform to the regulatory authority standards.
In collaboration with Cordlife Singapore, an American Association of Blood Banks (AABB) and Foundation for the Accrediation of Cellular Therapy (FACT)-accredited and Ministry of Health (MOH)-licensed cord blood bank in Singapore, we performed a simulation of lenticule banking service, starting from the collection of the stromal lenticules from our eye clinic for short-term (3 months) and long-term (12 months) cryopreservation, retrieval from the cryopreservation facility, and finally to the implantation in rabbits in our research institute. In this study, we report the effects of the short-term and long-term cryopreservation on the transparency, lenticular cells, and collagen fibrillar packing of the lenticules. We subsequently showed the safety of the implantation of both lenticules in the rabbit corneas for 4 months, of which steroidal and antibiotic prophylaxis were withdrawn for the past 2 months (Fig. 1). This study also served to validate the in vivo safety and feasibility of a lenticule banking service.

Experimental timeline for the simulation of lenticule banking service. Corneal stromal lenticules were collected from the eye clinic, SNEC, at time 0 and cryopreserved for either 3 months (short term) or 12 months (long term) at the lenticule bank in Cordlife Singapore. At the predetermined time points, the lenticules were retrieved from the cryostorage facility and transported to SERI. At SERI, the central 3 mm of the lenticules was trephined, which was later implanted in the rabbit corneas. The lenticules were implanted for 4 months, of which antibiotic and steroidal prophylaxis were withdrawn for the last 2 months. The remaining lenticules were subjected to TUNEL assay and TEM. SERI, Singapore Eye Research Institute; SNEC, Singapore National Eye Centre; TEM, transmission electron microscopy; TUNEL, terminal deoxynucleotidyl transferase dUTP nick end labeling.
Materials and Methods
Extraction and collection of corneal stromal lenticules
A total of 15 stromal lenticules were collected from nine patients who underwent SMILE for myopia correction at the Singapore National Eye Centre. Informed consent was obtained from the patients before the procedure. Three lenticules each were used for the short-term and long-term cryopreservation study arms. Three fresh lenticules were collected to serve a baseline for assessing the transparency and collagen fibrillar arrangement changes after cryopreservation. The mean patient age, gender, spherical error correction, and lenticular thickness are tabulated in Table 1. Correction of myopia was performed using a VisuMax femtosecond laser system (Carl Zeiss Meditec). All SMILE parameters and lenticule extraction were as described in our previous study. 8 In brief, the following laser parameters 120 μm cap thickness, 7.5 mm cap diameter, 6.5 mm optical zone with a transition zone of 0.1 mm, and 145 nJ of power with side cut angle of 90° were used to fashion the stromal lenticule. A lamellar dissector (Asico, Westmont, IL) was then used to separate the anterior and posterior lamellae of the lenticule, followed by extraction from a single incision with a circumferential length of 2.1 mm. A collection kit, containing labeled sterile containers, two individually packaged sterile saline solution (Opto-Pharm, Singapore), and a biohazard ziplock bag, was provided to the eye clinic for the collection of the corneal lenticule. After the extraction procedure, the lenticules were placed in their designated sterile containers, filled with saline solution, and secured tightly. The containers were sealed in a biohazard bag and transported at room temperature to the Cordlife Singapore facility.
Patient Demographics and Treatment Details
SE, spherical error correction.
Processing, cryopreservation, and thawing of lenticules
Containers were received at the storage facility and immediately transferred into a Class II biosafety cabinet that had been disinfected with 70% isopropanol. The lenticules were recovered by pouring the contents into a six-well plate (Corning, New York). Thereafter, the lenticules were disinfected by first immersing and rinsing for 10 min in wash solution, composed of Dulbecco's phosphate buffered saline (Biological Industries, Beith HaEmek, Israel) supplemented with 1% (v/v) penicillin–streptomycin–amphotericin B solution (Biological Industries), followed by second rinsing in fresh wash solution for another 10 min. After disinfection, the lenticules were immersed and equilibrated for 10 min in a well, containing cryopreservation medium composed of Dulbecco's modified Eagle's medium, high glucose formulation (Biological Industries), supplemented with 10% (v/v) dimethyl sulfoxide (DMSO; WAK-Chemie, Steinbach, Germany). The equilibrated lenticules were then transferred to labeled sterile cryovials and immersed in the cryopreservation medium. All lenticules were subjected to prestorage sterility testing by inoculating the cryopreservation medium from the equilibration step into the BacT/ALERT BPN and BPA culture bottles and incubated in the BacT/ALERT microbial detection system (BioMérieux, Marcy-l'Étoile, France). Any positive detection of microbial contaminations was further tested by a microbiology laboratory for microbial species identification. After that, the lenticules were subjected to controlled rate freezing of −1°C/min until −40°C was reached, whereupon the temperature was rapidly reduced to −90°C at −10°C/min. Subsequently, they were stored at −196°C in vapor-phased liquid nitrogen tanks for short-term cryopreservation of 3 months (n = 6) or long-term cryopreservation of 12 months (n = 6). The lenticule processing from the receipt to controlled rate freezing was completed between 24 and 96 h.
At the predetermined time points (month 3 or 12), the lenticules were retrieved from the liquid nitrogen tanks and thawed at 37°C for 1 min in a water bath. The thawed contents were first poured into a six-well plate. Subsequently, the lenticules were rinsed using a freshly prepared wash solution for 10 min, followed by a second rinse for another 10 min. All lenticules underwent post-thaw sterility testing by inoculating the post-thawed cryopreservation medium. The lenticules were then transferred to sterile containers containing sterile wash solution and secured tightly before transportation to the Singapore Eye Research Institute (SERI) for further experiments. At SERI, the lenticules were first tested for optical transparency, followed by trephination to 3-mm buttons, for subsequent in vivo implantation (n = 6). The other six lenticules were divided into two halves. One half was subjected to transmission electron microscopy (TEM) and the other half was subjected to histology and terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) assay.
Optical transmittance measurement
The optical transmittance of lenticules was determined using an Infinite 200 UV-Vis spectrophotometer (Tecan, Männedorf, Switzerland) with visible light wavelength ranged from 380 to 780 nm. The lenticules were placed on polystyrene coverslips (Thermo Fisher Scientific, Waltham, MA) and inserted into the spectrophotometer chamber for transmittance measurement. Data were collected at 10 nm wavelength increments. Fresh lenticules were used as the noncryopreserved or untreated control.
Transmission electron microscopy
The lenticules and one half of rabbit corneas were fixed sequentially with 3% glutaraldehyde (Electron Microscopy Sciences, Hatfield, PA), 1% tannic acid (Sigma-Aldrich, St. Louis, MO), and finally 1% osmium tetroxide (Electron Microscopy Sciences), and processed for epon-araldite resin embedding as previously described. 22 Ultrathin sections of 90–100 nm in thickness were cut using a Leica UC7 ultramicrotome (Leica Microsystems, Wetzlar, Germany). After staining with 3% uranyl acetate (Electron Microscopy Sciences) and lead citrate (Sigma-Aldrich), the sections were imaged with a JEM-2100 microscope (JEOL, Tokyo, Japan). Cross-sectional view of stromal lamellae was imaged in three random fields from each lenticule. Estimation of collagen fibrillar density was conducted by counting the number of fibers within a randomly selected window of fixed size (0.5 × 0.5 μm). Collagen fibrillar radial distribution pattern was obtained by first marking a randomly selected fiber as the center of the measurement. Six fibers, directly adjacent to the center fiber, which fit within ±6° of six different angles of orientation (0°, 60°, 120°, 180°, 240°, and 300°), were then marked and their interfibrillar distances were measured from the center fiber (Supplementary Fig. S1). These six marked fibers formed “layer 1 (red pseudohexagon)” of the radial distribution. The marking and interfibrillar distance measurement were repeated for the next six fibers, which were directly adjacent to the “layer 1” fibers, forming “layer 2 (green pseudohexagon)” of the radial distribution. This was repeated for another two layers of fibers. Three randomly selected center fibers were used to measure the fibrillar radial distribution from each TEM image.
Implantation of stromal lenticules in vivo
The in vivo experiment followed protocol 2015/SHS/1034, which was approved by the Institutional Animal Care and Use Committee of SingHealth, Singapore. All animals were treated according to guidelines of the Association for Research in Vision and Ophthalmology Statement for the Use of Animals in Ophthalmic and Vision Research. Six New Zealand White rabbits (9–12 weeks old) were obtained from In Vivos, Singapore. The rabbits were sedated with an intramuscular injection of ketamine hydrochloride (50 mg/kg; Parnell Laboratories, Alexandria, Australia) and xylazine hydrochloride (5 mg/kg; Troy Laboratories, Glendenning, Australia). Each rabbit received lenticule implantation in the right eye only. Three rabbits were implanted with short-term cryopreserved lenticules, and the other three were implanted with long-term cryopreserved lenticules. Before intrastromal lenticule insertion, a corneal pocket was first created. The corneas underwent incomplete flap creation (flocket) using a VisuMax femtosecond laser system (Carl Zeiss Meditec), 23 which was performed by one surgeon (J.S.M.). The laser parameters were set as follows: 120 μm flap thickness, 7.9 mm flap diameter, and 170 nJ power. The laser firing sequence was manually stopped with 3 s left to avoid a complete flap creation, leaving only a complete sidecut of ∼2 mm in circumferential length. A lamellar dissector (Asico) was then tunneled through the sidecut, and onto the flap bed. A stromal pocket was created once the lamellar adhesions of the flap were released. After irrigation of the flocket with a balanced salt solution, the 3-mm lenticule button was inserted into the center of the flocket and the opening was closed by an interrupted 10–0 nylon suture (Johnson & Jonhson, New Brunswick, NJ). The suture was removed after 1 week. The rabbit eyes were instilled with Tobradex (tobramycin and dexamethasone) eye drops (Alcon, Geneva, Switzerland) four times a day for 2 months. The rabbits were euthanized after 4 months. The corneas were harvested and divided into two. One half was subjected to TEM and the other half was subjected to immunohistochemistry.
Postoperative examinations
Postoperative examinations were performed on weeks 1, 2, 4, 8, 10, 12, and 16 after lenticule implantation. First, slit lamp photography (BM900, Haag-Streit AG) was performed to examine the gross appearance of the rabbit corneas. Corneal inlay haze was scored by two graders based on the scoring system by Fenner et al., 24 where no haze was graded as 0, mild peripheral edge haze was graded as 1, prominent peripheral haze was graded as 2, and central haze was graded as 3. Anterior segment-optical coherence tomography (AS-OCT; RTVue; Optovue, Fremont, CA) was performed next to examine the cross sections and thickness of the corneas. From the AS-OCT images, corneal clarity or densitometry was analyzed by measuring the integrated density of the corneas using the ImageJ software (National Institute of Health, Bethesda, MD).
En face images of the rabbit corneas were scanned using a Heidelberg Engineering HRT3 in vivo confocal microscope (IVCM) equipped with Rostock corneal module (Heidelberg, Germany). Corneal scans were taken through the full thickness of the central cornea (through the center of the lenticule) and of the midperiphery cornea (to capture the lenticular edge). From the central corneal scans, the number of basal epithelial cells, keratocytes in the anterior (100 μm depth), within the lenticule and posterior stroma (200 μm posterior of the lenticular posterior interface), and endothelial cells within a 100 × 100 μm field of view were counted manually using the ImageJ cell counter feature (National Institute of Health).
Immunohistochemistry and TUNEL assay
After animal euthanization, the corneas were harvested and fixed with 4% paraformaldehyde (Sigma-Aldrich) overnight. The corneas were then embedded in the OCT cryocompound (Leica Microsystems). Serial cryosections (8 μm in thickness) of the corneas were cut with a Microm HM525 cryostat (Thermo Fisher Scientific). Sections on the slides were first washed in 0.01 M phosphate-buffered saline (PBS; 1st Base, Singapore), permeabilized with 0.15% Triton X-100 (Sigma-Aldrich) for 30 min, blocked with 2% bovine serum albumin (Sigma-Aldrich) and 5% normal goat serum (Thermo Fisher Scientific) for 1 h, and incubated with mouse monoclonal antibodies against cellular fibronectin (Sigma-Aldrich), tenascin-C (Abcam, Cambridge, MA), CD18 (Novus Biologicals, Littleton, CO), α-smooth muscle actin (α-SMA; Dako, Santa Clara, CA), and Thy-1 (Santa Cruz Biotechnology, Dallas, TX) at 4°C overnight. The antibodies were diluted in the blocking serum. After washing with 0.01 M PBS, the sections were incubated with goat antimouse Alexa Fluor 488 secondary antibody (Thermo Fisher Scientific) at room temperature for 1 h. Slides were then washed and mounted with UltraCruz Mounting Medium containing 4′,6-diamidino-2-phenylindole (DAPI) (Santa Cruz Biotechnology). Sections were observed and imaged with an AxioImager Z1 microscope (Carl Zeiss, Oberkochen, Germany).
A fluorescence-based TUNEL assay kit (Roche Applied Science, Indianapolis, IN) was used according to the manufacturer's instructions to detect the presence of apoptotic cells in the center 3 mm of the lenticules and rabbit corneas. The sections were viewed with an AxioImager Z1 microscope (Carl Zeiss) after counterstaining with DAPI. TUNEL-positive cells were manually counted in six random sections of each lenticule or rabbit cornea. The mean ratio to nonapoptotic (DAPI stained) cells was then calculated.
Statistical analysis
Data are expressed as mean ± standard deviation. Statistical comparisons of corneal densitometry and number of epithelial, stromal, and endothelial cells between preoperative and postoperative rabbit corneas were performed using paired Student's t-tests (Microsoft Excel 2010; Microsoft, Redmond, WA). Statistical comparisons between experimental groups were performed using Welch analysis of variance with post hoc Games–Howell test (SPSS version 17.0; IBM, Armonk, NY). The degree of agreement between two implant haze graders was determined by intraclass correlation coefficient (ICC) analysis (SPSS).
Results
Sterility and effects of cryopreservation
We did not encounter bacterial contamination in the cryopreservation medium before and after freezing of the six lenticules. Similar to previously reported, 25 we noted that cryopreservation affected the optical transparency of the lenticules. The lenticules had lower transparency after both short-term and long-term cryopreservation, in comparison with the fresh noncryopreserved lenticules (Fig. 2A). The average transparency to the visible light wavelength of the fresh lenticules was 94.8% ± 2.9%, which was significantly higher than that of the short-term stored lenticules (p = 0.014) and long-term stored lenticules (p = 0.001; Fig. 2B). There was no significant difference in the transparency between the short-term and long-term cryopreserved lenticules (p = 0.401).

Changes in visible light transmittance and collagen fibrillar arrangement after short-term (3 months) and long-term (12 months) cryopreservation.
The reduced transparency was due to the alterations in the collagen fibrillar packing of the lenticular stroma. From the collagen fiber radial distribution charts, we noticed, although the fibrillar spacings appeared regular (relatively undistorted hexagonal patterns), the interfibrillar distance was significantly reduced after cryopreservation (Fig. 2C). The average interfibrillar distance of fresh lenticular stroma was 70.3 ± 4.9 nm, which was substantially higher than that of short-term stored lenticules (p = 6.20 × 10−9) and long-term stored lenticules (p = 5.10 × 10−9; Fig. 2D). Interestingly, we observed more tightly packed collagen fibers after prolonged cryopreservation. The interfibrillar distance was reduced from 56.8 ± 6.5 nm after 3 months cryopreservation to 50.6 ± 4.4 nm after 12 months cryopreservation (p = 1.29 × 10−4; Fig. 2C, D). As expected, an inverse relationship between the interfibrillar distance and fibrillary density of the lenticules was observed, where the fibrillar density increased as the interfibrillar distance decreased (Fig. 2E). Similar to the interfibrillar distance, we found a significant difference in the fibrillary density between the fresh and cryopreserved lenticules (p = 8.21 × 10−9 vs. 3-month stored lenticules and p = 5.58 × 10−9 vs. 12-month stored lenticules).
Multiple keratocytes could be seen from the DAPI staining in fresh and both cryopreserved lenticules (Fig. 3A). Consistent with our previous study, 26 TUNEL assay revealed the presence of only a few apoptotic cells in the center 3 mm of the fresh lenticules (Fig. 3A). We focused the analysis on the center of the lenticule, instead of the whole lenticule, because it was more representative of the lenticular portion that was implanted in the rabbit cornea. We observed even fewer apoptotic cells in the lenticules after cryopreservation (Fig. 3A). The ratio of apoptotic cells to nonapoptotic cells was 7.0% ± 4.3% in the fresh lenticules, which was marginally higher than in the short-term stored (3.2% ± 1.1%; p = 0.447) and long-term stored lenticules (2.8% ± 1.0%; p = 0.386; Fig. 3B). No significant difference was found between the short-term and long-term groups either (p = 0.854). This marginal discrepancy was likely due to the sloughing off of some cells after cryopreservation. The average number of cells (DAPI-positive cells) reduced from 20 ± 6 in the fresh lenticules to 13 ± 3 (p = 0.330) and 16 ± 2 (p = 0.590) in the short-term and long-term stored lenticules, respectively (Fig. 3B).

Apoptosis in lenticules after short-term and long-term cryopreservation.
In vivo tissue responses after cryopreserved lenticule implantation
The in vivo corneal tissue responses were examined with a combination of slit-lamp photography, AS-OCT, and IVCM. On slit-lamp photography, the rabbit corneas appeared clear over 4 months of lenticule implantation (Fig. 4A). We did not observe haze or neovascularization in the host corneas that were either implanted with short-term stored or long-term stored lenticules. The withdrawal of antibiotic and steroidal prophylaxis after week 8 did not appear to cause any adverse reaction. We assigned two graders to score the implant haze. The graders had an excellent agreement in the grading of the haze in the short-term (ICC = 0.846; p = 7.03 × 10−5) and long-term (ICC = 0.839; p = 9.05 × 10−5) groups. We noticed a mild haze (median score 0.5) in the peripheral edge of both short-term and long-term cryopreserved lenticules at postoperative week 1 (Fig. 4A, B). The haze appeared to intensify at week 2 (median score 1) but was subsided after postoperative week 8 in the short-term cryopreserved implants and after week 4 in the long-term cryopreserved implants. Both lenticules were difficult to identify on the slit-lamp at 16 weeks postoperatively. Quantitatively, the corneal haze intensity increased after implantation of both lenticules, reaching the peak at week 4, where the densitometry in both the short-term (p = 0.045) and long-term (p = 0.009) groups was significantly higher than that of the preoperative corneas (Fig. 4C). In the following weeks, the haze intensity appeared to reduce up to week 10 but it rose again up to week 12. Nevertheless, the corneal clarity improved and returned to close to the preoperative state at week 16. Statistically, at no other follow-up time points did the haze become significantly more intense than that in the preoperative corneas. Also, we did not find significant differences at any time points between the short-term and long-term groups.
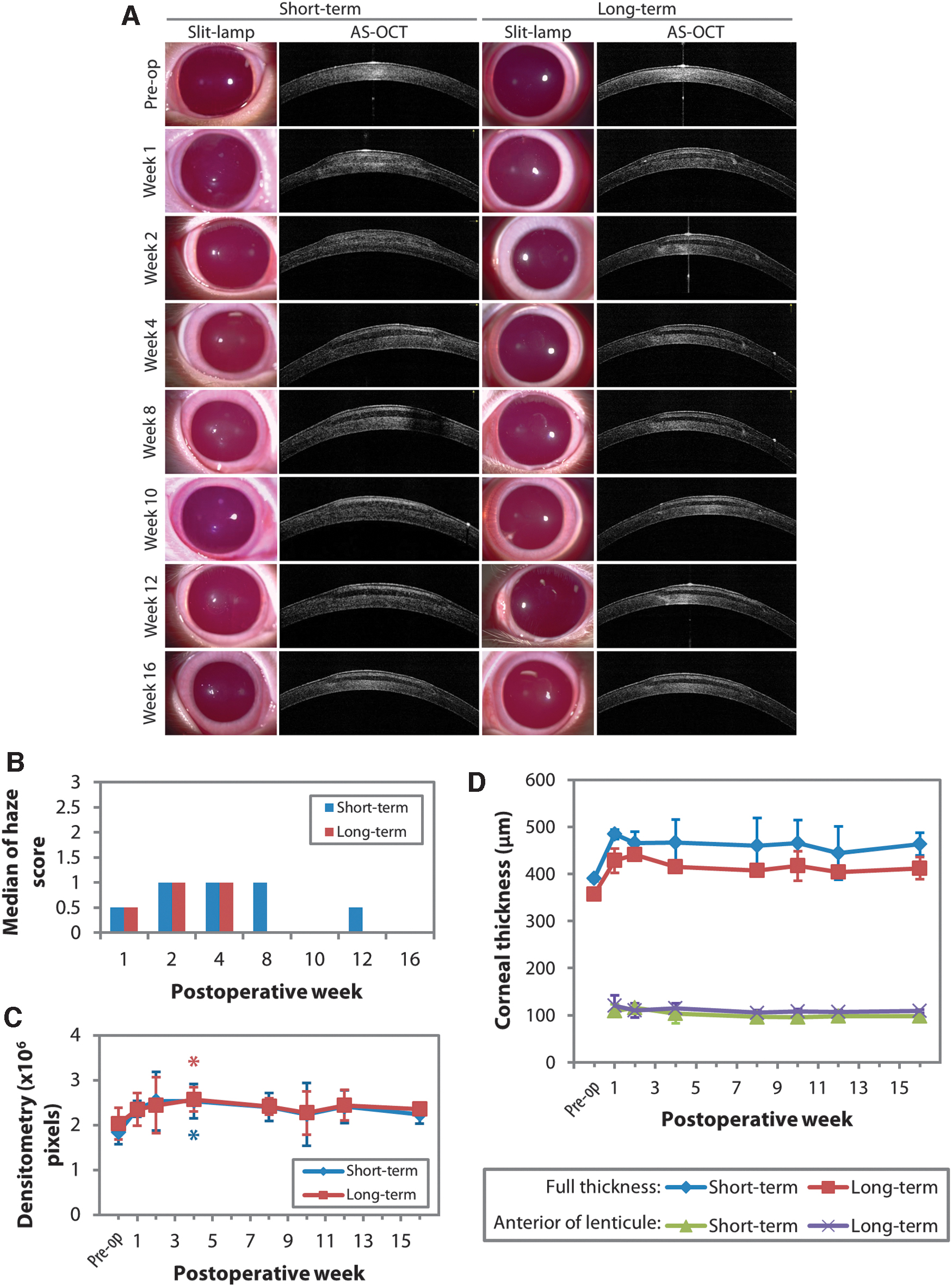
Gross appearance and cross-sectional view of the corneas implanted with cryopreserved lenticules.
On AS-OCT, the lenticules could be differentiated from the host corneal stroma (Fig. 4A). The lamellae of the lenticules appeared less light reflective compared with the host corneal stromal lamellae. This contrasting appearance was maintained throughout the 4-month follow-up period. Mild edema, indicated by central corneal thickness (CCT) increase, occurred at postoperative week 2 in corneas implanted with either short-term or long-term cryopreserved lenticules (Fig. 4D). The edema resolved in the subsequent follow-up periods, shown by the stabilization of the CCT after postoperative week 4. It should be noted that the significantly thicker corneas, in comparison with the preoperative corneas, after the CCT stabilization were due to the lenticule addition. The rabbit CCT changes were consistent with the thickness of the implanted lenticules (−1D correction was equivalent to ∼13 μm-thick lenticule). 27 Anterior stromal thinning, which often occurs in the corneas that are implanted with synthetic inlays due to the impedance of nutrient flow, 28 was not seen in both of the cases here (Fig. 4D). The corneal thickness anterior to the lenticules did not significantly change at any follow-up time point.
On IVCM, we found that the implantation of either short-term or long-term cryopreserved lenticules did not induce cytotoxicity to the host epithelial cells, keratocytes both in the anterior and posterior stroma, and endothelial cells over 16 weeks (Fig. 5 and Supplementary Fig. S2). Quantitation of the host basal epithelial cells (Fig. 6A), keratocytes (Fig. 6B), and endothelial cells (Fig. 6D) from the IVCM images did not yield any significant differences compared with the number of cells before the lenticule implantation. The cellular morphology appeared unchanged in comparison with that in the preoperative corneas, even after the withdrawal of the antibiotic and steroidal administration after week 8. The corneal basal epithelial cells maintained their cobblestone morphology. The stromal cell bodies appeared elongated with similar reflectivity as the preoperative cells, which was characteristic of corneal stromal keratocytes. The endothelial cells maintained their hexagonality throughout the follow-up periods. The stroma of the implants had few cells and remained the same over 16 weeks (Figs. 5 and 6C). Intense light reflectivity or haze was seen at both short-term and long-term cryopreserved implant periphery at postoperative week 4, consistent with the slit-lamp observation. The haze intensity appeared to reduce over time and returned to the preoperative state at week 16.

En face images of rabbit corneas implanted with cryopreserved lenticules. No sign of cytotoxicity was observed in the corneas up to 16 weeks. The stroma of the implants had little to no cells and remained in the same condition throughout the follow-up periods. Intense light reflectivity or haze was noted at both short-term and long-term cryopreserved implant periphery at postoperative week 4. The haze intensity appeared to reduce over time and returned to the preoperative state at week 16. Scale bars = 100 μm.

Quantitation of corneal epithelial cells, stromal cells, and endothelial cells in rabbit corneas implanted with cryopreserved lenticules. Basal epithelial cells
Active wound healing and inflammatory responses at the last postoperative time point
We performed immunohistochemical staining of fibronectin, tenascin-C, CD18, Thy-1 and α-SMA, and TUNEL assay after animal euthanization to assess the wound healing and inflammatory reactions that might still be active at the last follow-up time point. 29 As expected, these proteins were not expressed in the nonoperated corneas. In the corneas, either implanted with short-term or long-term cryopreserved lenticules, we did not find the expression of the aforementioned wound healing and inflammation-related proteins as well (Fig. 7). We also did not detect any apoptotic cell in the stroma of the rabbit corneas. To ascertain that the negative staining outcomes were not due to technical errors or inactive antibodies, we performed immunohistochemistry with the same antibodies on positive controls that were appropriate to show the expression of each marker of interest. Rabbit cornea 2 months post-surface ablation (phototherapeutic keratotomy) was used as a positive control for fibronectin, tenascin-C, Thy-1, and α-SMA.30,31 CD18, a neutrophil marker and binding partner of CD11b, 32 was shown to be positive in the rabbit corneas 1 day post-treatment with surface ablation. 33 Finally, to induce TUNEL-positive apoptotic cells, we treated rabbit corneas with DNase I. 34

Immunohistochemical staining of wound healing and inflammatory markers in nonoperated and lenticule-implanted corneas. No active wound healing and inflammatory reactions were seen in all corneas 16 weeks after lenticule implantation. Positive controls, such as corneas 1 day (1D SA) and 2 months (2M SA) post-treatment with surface ablation (phototherapeutic keratotomy) and corneas treated with DNase, were stained with the same antibodies, used to stain the lenticule-implanted corneas to ascertain that the nonstaining was not due to technical errors or inactive antibodies. *indicates the lenticules. Scale bars = 50 μm. 1D SA, 1 day post-surface ablation; 2M SA, 2 months post-surface ablation.
The corneal stroma of the lenticule-implanted rabbit corneas, which were subjected to TEM, showed regular fibrillar spacing (based on the fibrillar radial distribution chart; Fig. 8A). Interestingly, the collagen fibers in the stroma of the implanted lenticules showed a slight spatial distortion (stretched hexagons) although the mean interfibrillar distance was not that significantly different than the rabbit stroma (p = 0.944; Fig. 8A, B). This was consistent with a similar fibrillar density between the rabbit stroma (349 ± 10 fibers/mm2) and the stroma of implanted lenticules (354 ± 17 fibers/mm2; p = 0.519; Fig. 8C).

Collagen fibrillar arrangement of the implanted lenticules and rabbit corneal stroma.
Discussion
The idea of refractive lenticule cryopreservation and implantation (for refractive or therapeutic indications) was first suggested by Prof. Jose Ignacio Barraquer in the 1960s. 35 However, the precise and accurate fashioning of refractive lenticules and the creation of intrastromal pockets (for lenticule implantation) was challenging due to technological limitations. Since then, technologies, such as femtosecond lasers, have advanced significantly. The most recent software allows the creation of accurate and precise intrastromal incisions, which has enabled refractive lenticule extraction. 35 With the expected increment of refractive lenticule extraction cases worldwide, the number of available stromal lenticules will increase. Therefore, establishing a lenticule bank to collect, catalog, cryopreserve, and distribute the lenticules could be useful. In this study, we simulated a lenticule banking service, which was carried out by a local cord blood bank, an institution independent of our eye clinic/laboratory. We showed that short-term and long-term cryopreservation induced a number of apoptotic cells similar to fresh lenticules, which we reported in an earlier study. 26 The cryopreserved lenticules, however, had reduced optical transparencies in comparison with fresh lenticules, which we showed were due to reduced interfibrillar distances and fibrillar densities. Nevertheless, the implantation of the lenticules in the rabbit corneas did not result in adverse reactions over 16 weeks. Implant haze was noticed in the earlier time points but was largely subsided after 4 weeks, which we showed was most likely contributed by the lenticular collagen fibrillar remodeling and adaptation to the host corneal hydration. The withdrawal of steroidal and antibiotic prophylaxis after 8 weeks appeared to induce a transient haze redevelopment at week 12. The haze subsided in the following weeks and the corneal clarity returned close to the preoperative state at week 16. The fluctuations, however, did not result in significantly different light reflectance when compared with the preoperative state.
Corneal tissue cryopreservation in DMSO was first mentioned in the literature as early as 1965. 36 It was found to be safe when implanted in patients. 37 In our earlier study, in a laboratory setup, we utilized 20% (v/v) DMSO as the cryopreservative of human stromal lenticules. 26 After a 30-day cryopreservation period, we found an average of 13.3% apoptotic cells in the lenticular stroma centrally. After the same cryopreservation procedure, we showed that implantation of cryopreserved primate lenticules in primate corneas was safe over 16 weeks. 38 Ganesh et al. further showed the safety of DMSO cryopreservation by implanting cryostored allogeneic lenticules in seven patients. 39 The findings in those earlier studies formed the rationale behind the use of DMSO in this study. Improvements to the technique were made in that a clinical-grade slow-freezing device and validated storage were now employed. Together with the lowering of the concentration of the DMSO to 10% (v/v), we found they resulted in a lower number of apoptotic cells after both 3 months (3.2%) and 12 months (2.8%) of cryopreservation.
Interestingly, we found a significant reduction in optical transparency after the cryopreservation when compared with the fresh lenticules. On the TEM, it was clear that the reduction was due to the alterations in the stromal collagen fibrillar arrangement. Although the collagen fibers were regularly spaced, the interfibrillar distance was significantly reduced, resulting in an increased fibrillar density. This, in turn, increased the light scattering and lowered the light transmittance of the cryopreserved lenticules. Although optical transparency was not influenced, prolonging the cryopreservation appeared to decrease the interfibrillar distance further. Whether a longer period of cryopreservation would affect the collagen fibrillar spacing further remains to be seen. This phenomenon could be explained by the physiochemical stress on the proteoglycans induced by the cryopreservation process. 40 Because the interfibrillar spacing of the corneal stroma is regulated and maintained by the proteoglycans, 41 the breakdown in the proteoglycan aggregates caused the compaction of the lamellae and reduction of the interfibrillar spacing. 40
In vivo, the reduced lenticular transparency appeared as mild implant haze at postoperative weeks 1–4 on the slit-lamp. The transparency of the lenticules improved in the subsequent follow-up time points, which occurred in tandem with the stabilization of the corneal hydration (marked by the stabilization of the corneal thickness after week 4). TEM of the rabbit corneas revealed that the interfibrillar distance and fibrillar density of the implanted lenticules became similar to the host corneal stroma, although we observed a slight distortion in the fibrillar radial pattern of the lenticules. The fibrillar spatial distortion was an indication of the remodeling of the host stromal matrix around the collagenous implant, which typically involves rearrangement of collagen fibers through mechanical force generation. 42 The reshaping of the corneal stroma also permitted the equalization of the fibrillar density after the implanted lenticules had adapted to the long-term deturgescence cycles of the rabbit corneas. 43 This finding implicated that the changes in the fibrillar density induced by the cryopreservation may not be that critical to the patients' vision over the long-term due to the adaptability of the stromal lenticules to the host stromal microenvironment.
Other than the implant haze, which cleared at week 4, we did not observe significant adverse reactions in the host corneas. The morphology and number of epithelial cells, keratocytes, and endothelial cells did not change from the preoperative state. The host corneas were clear throughout the follow-up period. No neovascularization was seen at any time during the lenticule implantation. Our immunohistochemical staining of fibronectin, tenascin-C, Thy-1, α-SMA, and CD18 revealed the absence of these proteins, indicating no active wound healing and inflammatory response was occurring at postoperative week 16. We also did not detect any TUNEL-positive cells in the rabbit stroma and the stroma of the human lenticules. This suggests that the cells that appeared within the implant on the IVCM were viable human cells, although most of the cells had abnormal morphology and nonproliferative (the number of cells remained largely the same over 16 weeks), an observation that was consistent with that found in human subjects who underwent lenticule implantation procedures.44,45 Zhao et al. reported similar findings in nonhuman primates even after 2 years of lenticule implantation. 46 The inactive stromal cells, as well as the negligible immunogenicity in cryopreserved lenticules,25,47 may explain the low risk of graft rejection after the lenticule implantation, even in the xenografting cases we showed here. Nevertheless, decellularization of lenticules for allografting would be recommended to eliminate the graft rejection risk. 48
A limitation of this study is perhaps the exclusion of fresh human lenticule implantation in the rabbits. There are two reasons for this exclusion. First, the implantation of fresh lenticules has been performed in humans and its safety has been established.15,20,21,49 Xenogeneic lenticule implantation in rabbits and primates has also been previously conducted by our group and He et al. and was demonstrated to be safe with minimal induced wound healing and inflammatory reactions.50,51 In light of these studies, the IACUC deemed fresh lenticule implantation in rabbits redundant. Second, the context of this study was to show the feasibility and procedural pathway involved in lenticule banking, as well as the safety of the implantation of the banked lenticules. The study of short-term banking was to simulate, for example, a case wherein the patient developed ectasia after corneal refractive surgery and would need the lenticule to restore the corneal volume and tectonic strength. Whereas the investigation of the long-term banking was to simulate a scenario where the aging patient developed presbyopia and would need the lenticule as a refractive inlay.
To the best of our knowledge, Cordlife offers the first health authority-licensed lenticule banking service in the world. In this study, we validated the safety and feasibility of lenticule banking that involved the collection of refractive lenticules from our eye clinic, transportation of the lenticules to the ministry of health-licensed lenticule bank, processing, and cryopreservation of the lenticules, which after two different periods (3 and 12 months), were retrieved from the lenticule bank and transported to our laboratory for implantation in rabbit corneas. The aseptic technique in the handling of the lenticules was successful in preventing bacterial infections throughout the study, including the transportation and cryopreservation processes. The cryopreserved lenticules did not induce any haze or neovascularization to the host corneas. As time progressed and after collagen remodeling, the implant haze subsided and was not noticeable at the end of our study. Cordlife's lenticule banking service is currently offered for the cryopreservation of autologous lenticules. Allograft lenticule cryopreservation may be offered in the future by setting up a network of lenticule banking worldwide. This would increase the accessibility of lenticules with different refractive profiles to suit the patients' refractive or therapeutic requirements at the time of need.
Footnotes
Acknowledgment
The authors thank Dr. Nyein Chan Lwin for his assistance in the animal experiments.
Disclosure Statement
K.P.B., K.F.T., C.S.P., H.J.C., and Y.F.C are employees of Cordlife Group Limited. J.S.M. is a medical advisor for Cordlife Group Limited. The rest of the authors have no conflict of interest.
Funding Information
This study was supported by the NRF Translational and Clinical Research Programme (Grant No. NMRC/TCR/008-SERI/2013) and NMRC Clinician Scientist Award-Senior Category (Grant No. MOH-000197-00).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.