
Abstract
Extracellular vesicles (EVs) are considered essential mediators of regenerative roles of autologous platelet- and extracellular vesicle-rich plasma (PVRP) and platelet- and extracellular vesicle-rich gel (PVRG). PVRP and PVRG are novel blood-derived products gaining attraction in regenerative medicine. However, despite their reported good efficacy, their preparation protocols are too time-consuming. Moreover, patient-tailored preparation protocols are desired to optimize platelet and EV count in PVRP and PVRG. This article presents the clinical implementation of one-step, patient-tailored erythrocyte sedimentation rate (ESR)-based, PVRP and PVRG preparation protocols through the presentation of three cases: (1) large chronic tympanic membrane (TM) perforation, (2) osteoradionecrosis of the lateral skull base, and (3) cerebrospinal fluid (CSF) leak in the sphenoid sinus. These were treated with PVRP and PVRG, prepared according to our preclinically constructed mathematical sedimentation model of cells and EVs based on the patient's ESR. (1) TM healed completely after the treatment with 3.6 mL of PVRP and PVRG (high platelet and EV protocol). The speech discrimination score and air conduction pure tone average improved from 75% to 95% and from 65 to 25 dB, respectively. (2) The osteoradionecrotic surface area decreased from 46 to 18 cm2, and infection was eradicated after six applications of 13–65 mL of PVRG (“half-volume” protocol). (3) No CSF leak recurrence was detected after surgical closure with 30 mL of PVRG postoperatively. Reproducible preparation protocols proved effective, safe, fast, and straightforward enough for the surgical staff to prepare PVRP and PVRG intraoperatively. To alleviate preparation, a calculator is provided. This pilot study presents a sound basis for further studies, which are needed to assess the therapeutic effect of PVRP and PVRG.
Impact statement
We introduce a clinical implementation of a patient-tailored, erythrocyte sedimentation rate-based platelet- and extracellular vesicle-rich plasma (PVRP) and gel (PVRG) preparation protocol based on a mathematical model. Products proved beneficial in wound healing and were, to our knowledge, used for the first time in the treatment of osteoradionecrosis of the lateral skull base. Furthermore, this reproducible preparation protocol is fast and straightforward to implement in clinical practice. A calculator is provided to alleviate PVRP and PVRG preparation for various clinical scenarios.
Introduction
Different names have appeared in the literature that describe blood-derived platelet-rich products, for example, platelet-rich plasma, platelet-rich fibrin (PRF) matrix, PRF, platelet-rich growth factors, platelet concentrate, and platelet gel. 1 Different observation methods, preparation protocols, and commercial intentions and industry drove to these terminological inconsistencies. 2 Nevertheless, platelet-rich preparations have been utilized in otorhinolaryngology—head and neck surgery (ORL-HNS), orthopedic trauma surgery, wound surgery, maxillofacial surgery, and dentistry. 3
On the other hand, the growing interest in research of nanotheranostics has led to the discovery of essential structures called extracellular vesicles (EVs). EVs are important mediators of intercellular communication due to their membranous structure and molecular signature, which enable them to be utilized in regenerative medicine and ORL-HNS. 4 International Society for Extracellular Vesicles defines EVs as particles that are naturally released from the cells, delimited by a lipid bilayer. EVs cannot replicate as they do not contain a functional nucleus. They are most commonly classified by their physical and biochemical composition and descriptions of conditions or cells of origin. 4 Furthermore, EVs are generally classified as exosomes and microvesicles. 5 Both have been recently recognized as advanced regenerative therapy products, especially platelet-derived EVs, due to induction of cellular differentiation and enhancement of musculoskeletal or neural regeneration. 6
Recently, significant concentrations of EVs have been measured and inspected in the autologous blood-derived platelet-rich product (in liquid form),7,8 which was named platelet- and extracellular vesicle-rich plasma (PVRP). PVRP is defined as a blood-derived product with concentrations of platelets and EVs higher than blood concentrations. For that reason, PVRP presents an upgrade in autologous regenerative therapeutics. 3 Later, autologous PVRP, prepared by a two-stepped plasma-based protocol, proved effective in treating chronic postoperative temporal bone cavity inflammation. 8 However, this time-consuming preparation protocol, which took an average of 80 min, resulted in an ∼10% yield of PVRP from withdrawn blood. 8 In addition, it has already been identified that PVRP composition is influenced by blood sample processing and a patient's blood characteristics.3,9
To overcome these obstacles, patient-tailored PVRP treatment has been proposed taking into account that the concentration of platelets and EVs in PVRP depends on the patient's erythrocyte sedimentation rate (ESR). 7
Meanwhile, PVRP has been successfully transformed to the semisolid (i.e., gelatinous) state in a preclinical in vitro pilot study and the product named platelet- and extracellular vesicle-rich gel (PVRG). 10
Since a clinical implementation of a patient-tailored ESR-based PVRP and PVRG preparation protocol is anticipated, the main aim of this pilot clinical study is to present the implementation of a reproducible novel, patient-tailored ESR-based autologous PVRP and PVRG preparation protocol by the presentation of three cases treated by ORL-HNS.
Materials and Methods
Patients' recruitment
In this prospective randomized clinical implementation pilot study, patients with different diseases were recruited between January and July 2021 at the Department of Otorhinolaryngology and Cervicofacial Surgery, University Medical Centre, Ljubljana, Slovenia, for the treatment with PVRP and PVRG. Each patient included in the study signed a written informed consent. The Medical Ethics Committee of the Republic of Slovenia approved the pilot study (No. 0120-146/2019/5, April 17th, 2019, and No. 0120-498/2020-3, January 13th, 2021). The study was conducted according to the guidelines of the Declaration of Helsinki.
Autologous PVRP and PVRG preparation protocol
This section provides step-by-step description of two patient-tailored protocols: (1) nondisease specific and (2) disease specific.
Blood withdrawal prerequisites
Before blood withdrawal, a patient should meet the following criteria:
□ Did not perform strenuous physical activity within 24 h of treatment. □ Is in a fasting state (i.e., no food or beverage intake, except water within 8 h of treatment). □ Did not have high-fat dietary intake or alcohol consumption 1 day before the treatment.
Blood withdrawal procedure
The blood is withdrawn through a peripheral venous catheter, from a peripherally inserted central catheter, a central venous catheter, or a peripheral artery according to the indications described in Table 1.
Inclusion and Exclusion Criteria of the Study
Metastatic malignant disease was classified as M1.
Residual malignant disease on the recipient site as R1 or R2 resection according to the Union for International Cancer Control, the TNM Classification of Malignant Tumours (TNM).
PVRG, platelet- and extracellular vesicle-rich gel; PVRP, platelet- and extracellular vesicle-rich plasma.
Nondisease-specific PVRP and PVRG preparation protocol
Citrated 4.5 mL evacuated blood tubes (9 NC sodium citrate 0.105 M, BD Vacutainer; Becton Dickinson, San Jose, CA, USA) stored at room temperature must be filled completely to provide appropriate blood to anticoagulant ratio. This blood is used for PVRP preparation. Tubes should be turned upside down three to four times immediately after sampling to achieve an adequate blood and sodium citrate mixture. The blood withdrawal volume is derived from expected blood yield and desired PVRP volume. According to previous findings, blood yield from a citrated blood specimen is ∼30–50% (i.e., from 10 mL of blood, 3–5 mL of PVRP will be produced). 7
After withdrawal, blood is stored and transported at room temperature (i.e., 22°C) to the centrifuge as soon as possible according to the platelet concentrate storage guidelines.
Blood centrifugation
Blood withdrawn in citrated tubes was centrifuged as described previously by Božič et al. 7 Before centrifugation, the blood tubes were again inverted three to four times to resuspend the samples. The blood was then centrifuged at the relative centrifugation force (i.e., RCF) of 300 g at 18°C. The centrifugation time (t) was calculated individually from the patient's ESR (i.e., ESR) according to the mathematical model proposed by Božič et al. 7
Two options were considered: (1) the “high platelet and EV” protocol aimed at yielding plasma with the highest possible platelet and EV concentration that can be obtained by a single spin preparation without pelleting platelets and EVs
7
and (2) a “half-volume” protocol where we calculated the time needed for the upper border of erythrocytes to arrive down to one half the length of the blood sample. The blood yield of “half-volume” protocol is 50% (Supplemental File 1),
xmax and xmin are the distances from the centrifuge rotor axis to the bottom and the level of the blood sample, respectively. ɛ is the adjustable constant, which was set to 0.13. By inserting the respective times of centrifugation into the expression for the concentration of platelets and EVs, the calculated platelet- and EV-enrichment factor in PVRP are higher than 2 (in the case of high platelet and EV protocol) or equal to 2 (in the case of “half-volume” protocol).
PVRP harvesting
After the centrifugation, blood divides into two distinctive fractions: red, which contains mainly erythrocytes, and yellow, which is PVRP. Sometimes an opaque whitish layer (i.e., buffy coat) is present between layers. PVRP is gently and slowly aspirated with a pipette (ref.: 225-1S; Termofisher Scientific, ZDA) above the red and white layer without disturbing them. PVRP extracts from all tubes are merged in another sterile plastic tube or container, and the total volume is measured.
PVRP is administered to the wound or activated to form a PVRG immediately or as soon as possible after PVRP harvesting.
PVRP activation (i.e., PVRG formation)
This step is skipped if the wound is treated with PVRP and PVRG is not required. PVRP, autologous serum (in the ratio of 1:5 to PVRP), and 1 M CaCl2 (in the ratio of 1:100 to PVRP) are mixed to transform PVRP to PVRG.
Additional blood is withdrawn in a 4 mL plastic blood tube without anticoagulant (e.g., Z Serum, Vacutube, LT Burnik, d.o.o., Slovenia) stored at room temperature. This blood is used to prepare serum, that is, activator, which transforms PVRP (i.e., liquid) into a gel (i.e., PVRG). After about 5–10 min, blood clot is formed within the tubes, and then the tubes are centrifuged for 10 min at 1260 g and 18°C. The supernatant above the red blood clot is a serum, which is gently aspirated without mixing layers and transferred by a sterile pipette into a sterile polypropylene tube.
The volume of autologous serum needed to prepare PVRG depends on the desired volume of PVRP that will be transformed to PVRG. A mixture in the ratio 1:5 with PVRP is needed (for activation of 5 mL of PVRP, 1 mL of serum is needed).
The blood yield for serum harvesting is calculated from the hematocrit. For instance, in 35% hematocrit, the serum presents 65% of blood volume.
To start the PVRP activation process (i.e., transformation of PVRP to PVRG), 1 M CaCl2 (14.7%, Pharmacy of University Medical Centre Ljubljana, stored at room temperature) in the ratio 1: 100 with PVRP (i.e., 1%; e.g., 170 μL to activate 17 mL of PVRP) is applied to the petri dish with the sterile pipette. Then, an autologous serum in the ratio 1:5 with PVRP (i.e., 20%; e.g., 4 mL to activate 20 mL of PVRP) is applied over the CaCl2. Finally, autologous PVRP is administered with the sterile pipette over the mixture of CaCl2 and autologous serum. At least 5 min should elapse for the activation process to occur and PVRG is formed. It is expected that some of the mixtures will not turn into a gel.
Disease-specific PVRP and PVRG preparation protocols
These preparation protocols are further optimized by disease characteristics (e.g., wound surface area).
Chronic tympanic membrane perforation
Chronic tympanic membrane (TM) perforations differ in size considerably from patient to patient. They can be very small or take up the whole area of the eardrum. Since the size of TM varies only slightly between people and its average surface area is 64.3 mm2, 11 the blood withdrawal volume and PVRG volume are relatively small. Due to these rationales, this preparation protocol is designed as if there is a total TM perforation (i.e., 100%) and the “high platelet and EV” centrifugation protocol [Equation (1)] is used. The protocol can be modified using a calculator in Supplemental File 1.
The total blood withdrawal volume for the treatment of TM perforation is 12.5 mL:
□ Two citrated 4.5 mL blood tubes (for PVRP preparation).
□ One 4 mL plastic blood tube without anticoagulant (for autologous serum preparation.
One half of the prepared PVRP is used to prepare PVRG, and the other half is used to soak the sterile compressed sponge, as described later in the Treatment Regimen section.
Osteoradionecrosis of lateral skull base
A higher PVRG volume is required in this disease due to higher wound surface area. For that reason, a “half-volume” centrifugation protocol is used [Equation (2)]. Calculator for volume calculation is available in Supplemental File 2.
The required PVRG volume is calculated from the wound surface area:
where VPVRG is PVRG volume, S is wound surface area, and h is height.
In external wounds, as in this case, h = 1 cm is used for the calculation to cover the wound thoroughly. However, some of the mixture (PVRP, calcium chloride, and serum) remains untransformed (i.e., liquid), and PVRG height is expected to be less than 1 cm.
PVRG application can be repeated several times, depending on the healing process. The time between applications can vary from patient to patient from 1 to 14 days according to previous blood-derived product therapy regimens. 12 After applying PVRG, a glassy, water-resistant layer is formed over the wound. Wound healing (e.g., granulation tissue formation) can be observed through this layer. For that reason, we recommend at least a 14-day interval between each application.
The total blood volume (VT) needed for the PVRG preparation can be calculated as follows:
where VT is the total volume of withdrawn blood required to prepare the desired PVRG volume (VPVRG), Ht is the patient's hematocrit, and
The blood for serum and PVRP preparation must be withdrawn into different tubes (citrated 4.5 mL blood tubes for PVRP and 4 mL plastic blood tubes for serum). This is why an exact blood volume needed for PVRP (Vblood for PVRP) and serum (Vblood for SERUM) preparation must be known and calculated from Equations (5) and (6).
Cerebrospinal fluid leak in the sphenoid sinus
As in the previous case, also in this disease, the “half-volume” centrifugation protocol is used because a higher PVRG volume is needed for cerebrospinal fluid (CSF) leak closure [Equation (2)]. Calculator for volume calculation is available in Supplemental File 2.
The PVRG is applied once intraoperatively.13,14 If the procedure fails or the CSF leak persists, the procedure can be repeated, and PVRG applied as many times as needed until the CSF leak stops.
The area of the surface we want to cover with PVRG needs to be approximated with endoscopic instruments. The volume of needed PVRG is then calculated from Equation (3). In this case, we recommend a 0.5 cm is used for the height (h).
The total volume of withdrawn blood and its fractions for volume needed for PVRP and serum preparations are calculated from Equations (4) to (6) and Supplemental File 2.
Results
Three patients were recruited in this pilot clinical study between January and July 2021 at the Department of Otorhinolaryngology and Cervicofacial Surgery, University Medical Centre Ljubljana: (1) a patient with chronic TM perforation, (2) a patient with osteoradionecrosis of the lateral skull base, and (3) a patient with CSF leak in the sphenoid sinus.
They were treated with PVRP and/or PVRG prepared according to our previously proposed protocol, based on the mathematical sedimentation model of cells and EVs.
Chronic TM perforation
Patient profile and summary
A 35-year-old male smoker without chronic diseases was treated for 1 year, lasting left chronic TM perforation, which developed after an acute otitis media. The perforation encompassed 46% of the total TM area (Fig. 1A).
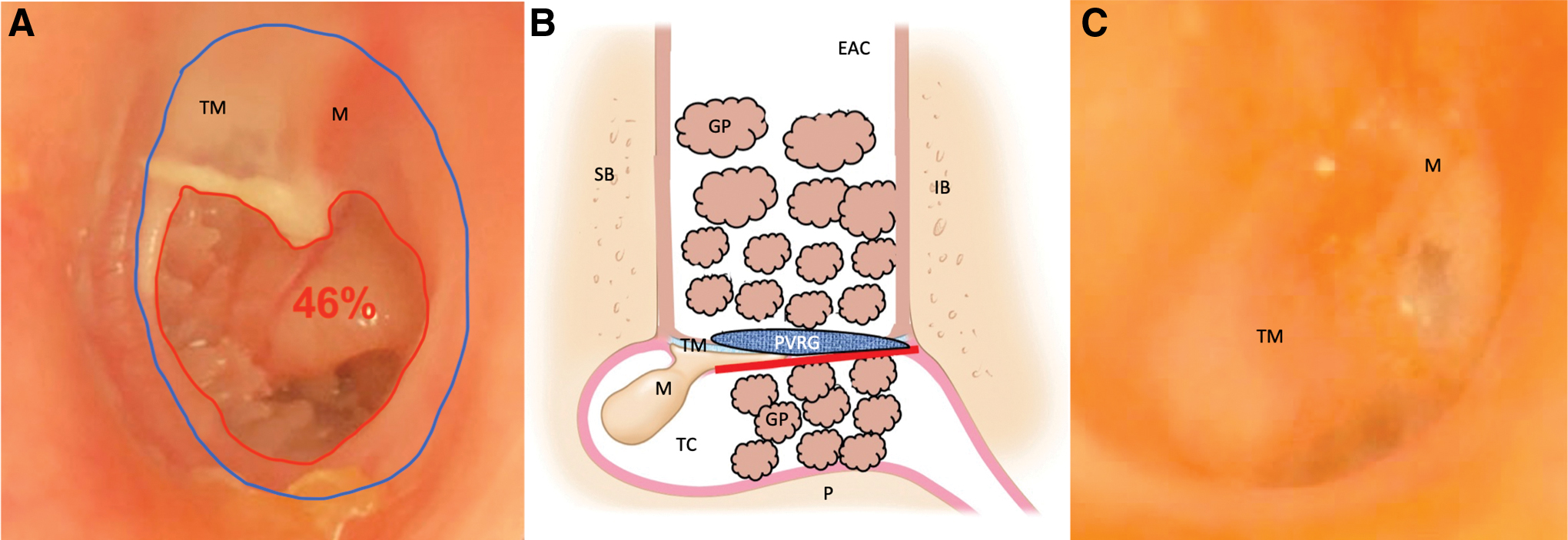
Photographs and treatment scheme of the patient with left chronic TM perforation, treated surgically (tympanoplasty) with PVRP, PVRG, and temporal muscle fascia.
At the initial presentation, the speech discrimination score (SDS) using Slovenian adaptation of the Freiburg monosyllabic word test was 75% 15 and pure tone average (PTA) calculated from air conduction hearing thresholds at 0.125, 0.25, 0.5, 1, 2, 4, 6, 8, 9, 10, 11.2, 12.5, 14, and 16 kHz was 65 dB. SDS and PTA were both measured on the ear with TM perforation. The tympanometry (Titan, Serial Nr. 421201; Interacoustics, Middelfart, Denmark) performed on the healthy ear showed an A curve, normal middle ear volume, and normal compliance.
Video head impulse test (vHIT) (EyeSeeCam vHIT 1.2.0 and Otoaccess 1.4.0; Interacoustics) and vestibular caloric test (Variotherm plus; ATMOS MedizinTechnik GmbH & Co. KG, Lenzkirch, Germany) results were normal.
Treatment regimen
According to the “high platelet and EV protocol” for chronic TM perforation (described in Chronic Tympanic Membrane Perforation section), 3.6 mL of PVRP was prepared from 9 mL of citrated blood withdrawn from the cubital vein after centrifugation for 4.15 min [ESR = 17 mm/h, inserted in Equation (1)] at 300 g and 18°C. Half of PVRP was used to soak the sterile compressed sponge (Gelfoam®; Pfizer, New York, USA) and the other half for PVRG preparation.
The patient was treated surgically under local anesthesia. Tympanoplasty was performed with an endaural microscopic approach. First, the edges of the TM perforation were refreshed, and the tympanomeatal flap was elevated. Then, a desiccated temporal muscle fascia, harvested from the incision site, was placed in an underlay manner to reconstruct the TM. Before that, Gelfoam soaked with PVRP was placed in the tympanic cavity to support the fascia (Fig. 1B).
The tympanomeatal flap was then repositioned, and PVRG was administered on the lateral side of the reconstructed TM. PVRG was prepared from 1.8 mL of PVRP, 0.36 mL of autologous serum (prepared from 4 mL of noncoagulated blood) and 18 μL of CaCl2. The external ear canal was packed with the remaining Gelfoam soaked with PVRP.
Treatment outcome
The patient had no postoperative complaint or complication in the 6-month follow-up. The TM healed completely. A healed TM was first observed on a checkup 6 weeks postoperatively when the external ear canal packing was removed (Fig. 1C). SDS improved to 95%, and air conduction PTA decreased to 25 dB postoperatively. vHIT and vestibular caloric testing remained normal postoperatively.
Osteoradionecrosis of lateral skull base
Patient profile and summary
An 84-year-old male with arterial hypertension, hyperlipidemia, aortic stenosis, and chronic atrial fibrillation on therapy with apixaban presented with a squamous cell cancer of the left auricle, classified as pT4pN0 according to TNM classification of Malignant Tumors. The patient was primarily treated with tumor resection, suprafacial parotidectomy and left-sided selective neck dissection of regions II and III. He received postoperative radiotherapy. One year postoperatively, he presented with a cancer recurrence in the left external ear canal and was treated surgically with complete microscopical cancer resection, including auricle amputation and subtotal petrosectomy. The tissue defect, which reached the superior part of the squama of the left temporal bone, could not be covered with a free flap due to the patient's age and vessel disease. Thus, the defect was entirely reconstructed with left extended musculocutaneous pectoralis major muscle flap, which included the region of rectus abdominis muscle.
A few days postoperatively, the patient tested positive for COVID-19, which compromised the patient's general condition. The flap started to necrotize, and osteitis of the lateral skull base developed. Corynebacterium striatum, Pseudomonas aeruginosa, Morganella morganii, and Peptostreptococcus magnus were isolated from the wound swab. Moreover, the epithelialization of exposed cortical bone was hampered due to osteoradionecrosis, and it was exposed in two areas of 0.4 and 1 cm2. The patient's general condition remained poor, but stable.
Treatment regimen
Due to the patient's general health care status, which posed a high risk of general anesthesia, surgical revision with flap reconstruction could not be performed. The patient was initially treated with intravenous antimicrobials and regular flap necrosis removal to prevent intracranial and systemic complications. Despite this treatment, the osteitis persisted, and epithelialization did not occur. Therefore, outpatient salvage treatment, including multiple PVRG administration and necrosis removal, was offered to the patient. The wound was treated with six applications of PVRG and debridement on day 0 (baseline), 8, 17, 35, 56, and 108 (Table 2). The number of PVRG applications is strictly patient specific and depends on the wound healing rate. It can be repeated as many times as needed until the wound reaches the desired degree of healing.
Blood Withdrawal Indications for Platelet- and Extracellular Vesicle-Rich Plasma and Platelet- and Extracellular Vesicle-Rich Gel Treatment
A, alternative option; PICC, peripherally inserted central catheter; CVC, central venous catheter: the same tubes are used in arterial blood withdrawal.
Blood was drawn from the radial artery in citrated tubes due to the requirement of large PVRG volume and unsuccessful peripheral vein cannulation (Table 1). Blood withdrawal volume was prepared with a “half-volume” centrifugation protocol as described in Osteoradionecrosis of Lateral Skull Base section. PVRG preparation started immediately for every treatment session according to the high-volume preparation protocol [Equation (2)]. Over the PVRG, a nonadhesive absorbent dressing, Mepilex® (Mölnlycke, Gothenborg, Sweden), was applied. Directed intravenous antimicrobial treatment for osteitis of 6-week duration was discontinued at the first PVRG application (Table 3).
Treatment Regimen with Platelet- and Extracellular Vesicle-Rich Gel of the Osteoradionecrosis of the Lateral Skull Base
Blood withdrawal volumes were calculated from wound surface area and desired PVRG height with an automated calculator available in Supplementary Data S2. ESR, erythrocyte sedimentation rate (mm/h).
Treatment outcome
PVRG formed a protective biofilm over the wound after each application (Fig. 2C). The infection healed, that is, the antimicrobial swab was negative, and there was no discharge—fibrin and granulation tissue formed under the PVRG biofilm. Later epithelialization began from the wound edges and its central parts. However, the epithelialization did not cover the exposed cortical bone, not even after the cortical bone was drilled out and PVRG applied over the cancellous bone. One of the exposed areas of the bone surfaces was reduced from 1 to 0.4 cm2. The second one remained nonepithelialized (0.4 cm2).
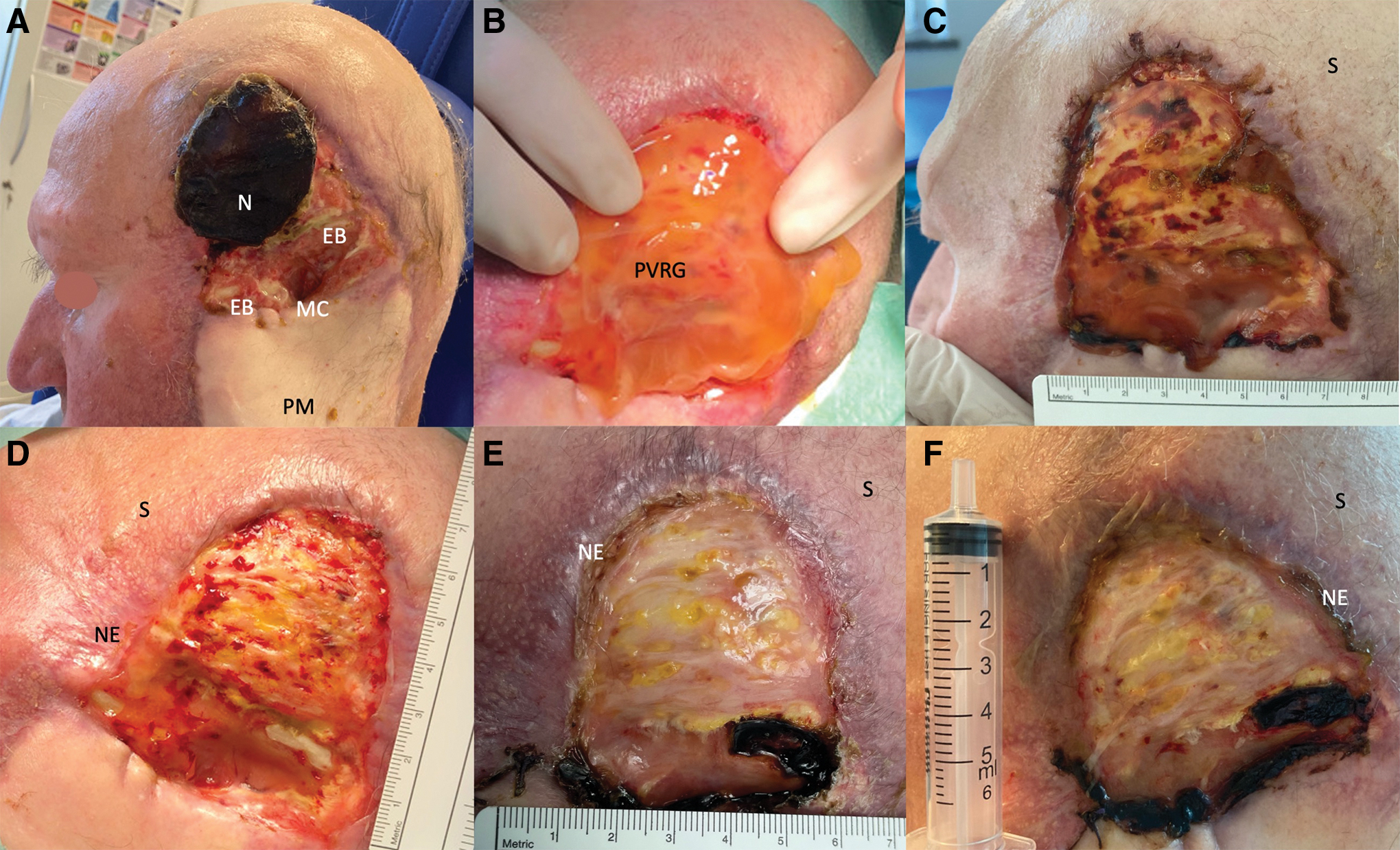
Photographs of a patient with an osteoradionecrosis and osteitis of left lateral skull base treated with six applications of PVRG.
CSF leak in the sphenoid sinus
Patient profile and summary
A 42-year-old female with persistent fever, headache, arterial hypertension, polycystic ovary syndrome, and prediabetes was admitted to treat the CSF leak in the sellar region of the sphenoid sinus, which occurred after transnasal transsphenoidal endoscopic extracapsular resection of pituitary adrenocorticotropic hormone-secreting adenoma. The patient presented with bilateral watery nasal discharge. The intraoperative dural defect has been reconstructed in a multilayer manner, with nasoseptal flap (NSF) and heterologous nonadhesive resorbable surgical adhesives. The patient developed an anterior watery nasal discharge on the seventh postoperative day, which was confirmed as a CSF leak. On the 10th postoperative day, lumbar drainage was inserted to lower the intracranial pressure. However, the CSF leak persisted.
On the 15th postoperative day, nasal endoscopy was performed in topical and local anesthesia. The origin of the CSF leak was identified, and the defect was plugged with a heterologous nonadhesive resorbable surgical adhesive. One week after the CSF leak closure, no CSF leak was detected, and the lumbar drainage was removed. Thirty-six days after the neurosurgical removal of pituitary adenoma, the CSF leak recurred, and the patient was admitted to our department. The antimicrobial therapy, which was prescribed on the day of the first surgery, was discontinued on the day of admission.
Treatment regimen
Three days after the patient was admitted to our ward, the closure of a high-flow CSF leak in the sellar region was performed under general anesthesia. First, the fibrin sealant patch TachoSil® (Baxter, Deerfield, IL, USA) was inserted as an inlay to plug the leak. Second, an NSF was put in an overlay manner. Thirty milliliters of PVRG was prepared intraoperatively after centrifugation by “high-volume” protocol as described in Cerebrospinal Fluid Leak in the Sphenoid Sinus section. The centrifugation of 57 mL peripheral venous blood was done for 2.05 min [calculated from ESR = 42 mm/h using Equation (2)] at 300 g and 18°C. PVRG was administered over the NSF.
In the end, everything was covered by layers of TachoSil, dissolvable nasal dressing—SINU-KNIT™ (Smith-Nephew, London, United Kingdom), and DuraSeal™ (Integra, Princeton, NJ, USA). The remaining PVRG was applied to exposed bone and damaged mucosa over the defect, which occurred after septectomy. At the end of the surgery, one Merocel® nasal pack (Medtronic®, Dublin, Ireland) was inserted in each nasal cavity to support the reconstruction and provide hemostasis. Perioperative antimicrobial prophylaxis was also administered. Postoperatively, the patient was admitted to the intensive care unit. Stool softeners, 30° head elevation, and measures against straining were taken. Two days later, nasal tampons were removed (Fig. 3).
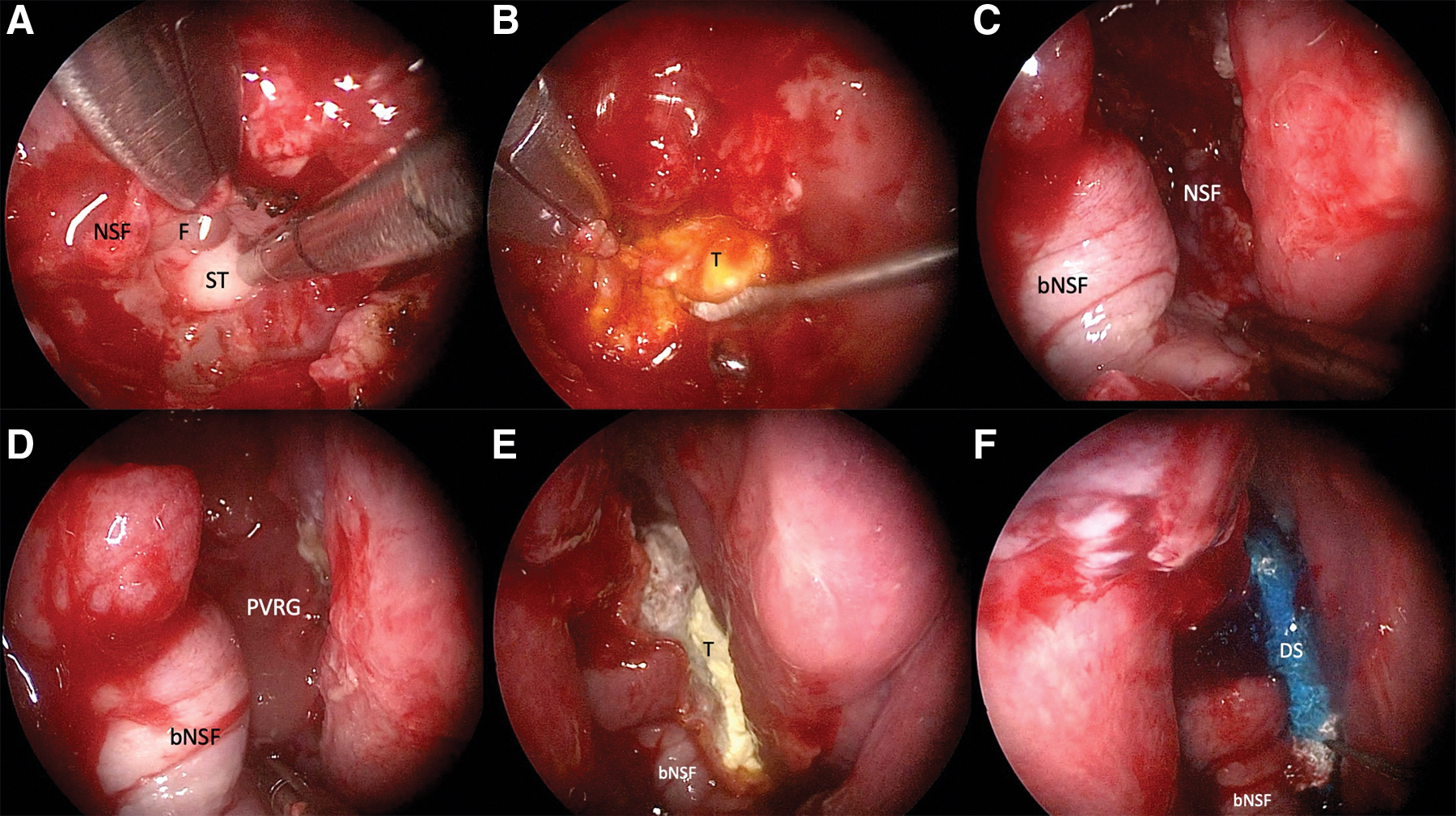
Intraoperative endoscopic photographs of a sphenoid sinus in patients with CSF fistula treated with multiple layers, including PVRG.
Treatment outcome
On the fifth day after the last surgical CSF leak closure, head computed tomography excluded significant pneumocephalus. The patient was discharged home 1 day later. At the checkup 2 months after discharge, the patient reported no watery discharge and headache. Nasal endoscopy showed no sign of CSF leak (Fig. 4).
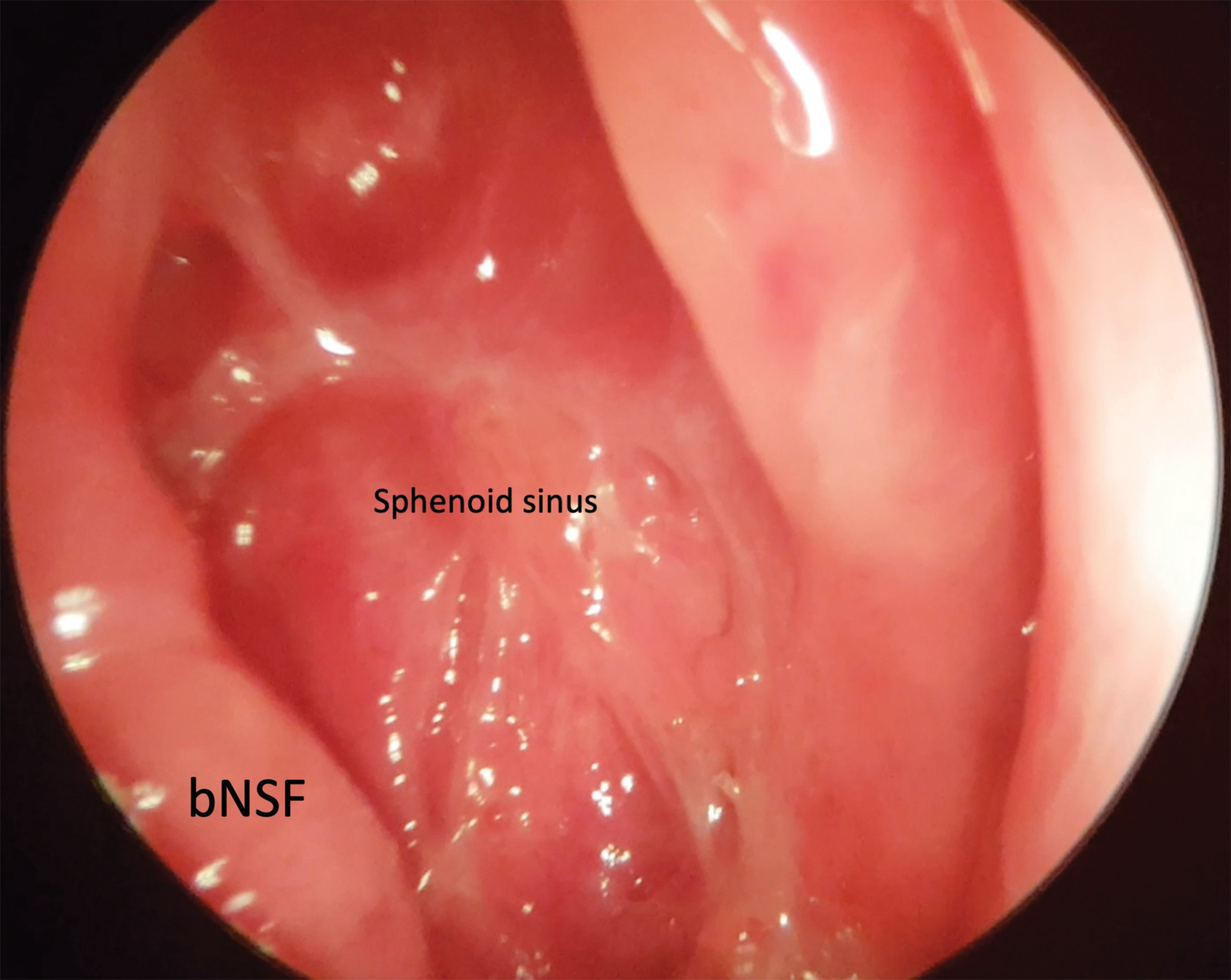
Postoperative endoscopic photograph of a sphenoid sinus after treatment of CSF fistula with multiple layers, including PVRG. No CSF leak was visible during the endoscopy at the checkup. Color images are available online.
Discussion
This pilot study presents the clinical implementation of a novel, patient-tailored ESR-based PVRP and PVRG preparation protocol by confirming PVRP's and PVRG's regenerative roles in managing three distinct therapeutically challenging diseases covered by ORL-HNS: (1) chronic TM perforation, (2) osteoradionecrosis of lateral skull base, and (3) CSF leak in the sphenoid sinus. Moreover, this article is an attempt to provide a manual for PVRP and PVRG preparation for these diseases.
Patient-tailored, disease-specific PVRP and PVRG preparation protocols
The preparation protocol was chosen according to the size and location of the target tissue and the patient's ESR. Two protocols designed in our previous research are also described in this study. 7 High platelet and EV protocol [Equation (1)] yields higher platelet and EV concentrations in PVRP at the expense of lower PVRP volume. 7 That is why this protocol was used to treat chronic TM perforation where the target tissue surface is small (Fig. 1). “Half-volume” protocol [Equation (2)] yields higher PVRP volume at the expense of lower platelet and EV concentrations in PVRP. However, these concentrations are still above the baseline blood level. 7 This protocol was used to treat osteoradionecrosis of lateral skull base and CSF leak in sphenoid sinus due to the large volume of PVRG needed to cover the target tissue.
Chronic TM perforation
The success rate of conventional tympanoplasty (defined as permanent TM closure) in our patient with chronic TM perforation was estimated at 86% according to MERI 3. 16 Moreover, a lower (75%) overall success rate of tympanoplasty was indicated in the large-scale study by van Stekelenburg and Aarts. 17 Since platelet-rich products are safe and their use improves the success rate in tympanoplasty,18,19 our upgraded product, based on a high concentration of platelets and EVs, was used as an adjunct autologous reconstruction material.
We believe that platelet-derived EVs carry fundamental regenerative roles of PVRP and PVRG when treating chronic TM perforation. It has been shown that they improve collagen synthesis and deposition, which promotes wound reduction, reepithelialization, and dermal angiogenesis. 20 PVRP and PVRG in the vicinity of the TM during tympanoplasty promote collagen formation and thus increase the chance of TM closure. TMs with more extensive perforations contain less collagen and, at the same time, need a higher amount of newly synthesized collagen to overcome this significant area of perforation. For that reason, we believe patients with large TM perforation could significantly benefit from PVRP and PVRG applications during tympanoplasty.
Despite our patient's 100% healing rate and hearing improvement (decrease in PTA and increase in SDS), a further large-scale study of PVRP and PVRG in tympanoplasty is obligatory. However, our high-platelet PVRP and PVRG preparation protocol can be proposed in future tympanoplasty research, especially for treating large and recurrent perforations, where the healing potential of the TM remnant is poor.
Lateral skull base osteoradionecrosis
Even more therapeutically challenging is lateral skull base osteonecrosis, which was a sequela of radiotherapy of external ear canal cancer and the patient's overall poor health status post-COVID-19. It is known that severe and fatal complications of osteonecrosis in this area can develop. Drastic changes to bone tissue result from postradiation DNA damage and cell death, 21 which cause disorganization of the extracellular matrix and prevent new vessel formation resulting in hypocellularity and tissue hypoxemia. 22 Irradiated bone becomes necrotic and exposed through the skin, and may become infected (i.e., osteitic). 23
Platelet-rich preparations have been mainly reported as a helpful adjunct in treating mandible osteoradionecrosis so far. 24 It is described that the main regenerative effects of platelet-rich products are conveyed by a high concentration of several growth factors and cytokines organized in a fibrin mesh within the product. 24 However, there are only 20 search results about osteoradionecrosis treated with platelet-rich products on Web of Science™ at this time when searching with a query: “platelet rich (Topic) and *radionecros* (Topic).” Moreover, there is no report of treating scalp or lateral skull base osteoradionecrosis with platelet-rich products.
For that reason, this study presents, to our best knowledge, the first patient treated with lateral scalp osteoradionecrosis in literature. Since the wound surface area decreased noticeably after multiple PVRG applications (from 46 to 18 cm2) and bacterial osteitis was treated successfully, PVRG could be considered a treatment modality for scalp osteoradionecrosis in further research. Furthermore, PVRG's antimicrobial roles could be explained by the effective treatment of osteitis with platelet-rich products elsewhere. 25
Since the main fundamental regenerative roles of PVRP and PVRG have been attributed to EVs in other clinical settings, we believe that they also exert essential effects in the treatment of osteoradionecrosis. Platelet-derived EVs contain different growth factors and cytokines, which stimulate tissue healing, increase endothelial permeability, 26 and exert antimicrobial functions. 27
CSF leak in the sphenoid sinus
As has already been reported, the role of platelet-rich products in CSF leak closure has not been clarified yet, and further studies are required.10,14 Based on the lack of a consensus on which surgical material should be used in this surgery, 28 PVRG could be considered a part of multilayered skull base closure. We have experienced a favorable tension resistance of PVRG, which enabled easy handling with endoscopic instruments. Since a CSF leak did not recur in our patient, PVRG prepared with our “half-volume” centrifugation protocol indicates an excellent clinical practice of intraoperative preparation of autologous surgical material, which can also be used by other surgeons.
We believe that PVRG's efficiency in CSF leak closure is attributed to its abovementioned stimulation of collagen synthesis and deposition, reepithelialization, angiogenesis, and antimicrobial functions exerted by EVs.20,27 Moreover, water-tight closure of CSF leak could be enhanced by the osteogenic capability of platelet-derived EVs, which results in new bone formation. 29
Although it is premature to predict PVRG's implementation in endoscopic skull base surgery, the future probably holds a development in autologous reconstruction materials. These reconstructive materials, for example, PVRP and PVRG, are safe, cost-effective, and easy to prepare.
Main strengths and limitations of the study
The main strength of this study is the novel, thoroughly described, repeatable PVRP and PVRG preparation protocols based on the patient's ESR in a clinical setting. Two options are available: “high platelet and EV” and “half-volume” protocol. They have been used in clinical practice for the first time in this pilot study. Furthermore, disease-specific protocols are provided in this study. This study provides sufficient details for the reproduction of PVRP and PVRG if instructions are followed and automated calculations are used by inserting variables (wound surface area, ESR, hematocrit, the desired volume of PVRG, and known or expected yield) in the calculator provided in the Supplemental File 2.
Despite the broad applicability of platelet-rich products in medicine, including ORL-HNS, there is a lack of randomized controlled clinical studies and meta-analyses due to poorly described, nonrepeatable, and diverse preparation protocols of platelet-rich products.3,30 Therefore, our thoroughly described, replicable preparation protocols provide a step-by-step guide and fill the research gap.
To our best knowledge, this is the first report of scalp osteoradionecrosis treatment with a platelet-rich preparation in literature.
Moreover, PVRP and PVRG have shown encouraging regenerative roles in this study, which could be attributed to platelets and EVs mediating growth factors and other bioactive substances.4,8,14,31 Nevertheless, this is only a pilot study based on three patients, which presents the main limitation of our study. However, in vitro studies on cell cultures would improve the understanding of PVRP's and PVRG's effect on the cellular level.
Conclusion
This novel patient-tailored, ESR-based PVRP and PVRG preparation protocol proved effective, safe, fast, and straightforward enough for the surgical staff to use intraoperatively. Our pilot study presents a sound basis for further studies that are needed to assess the therapeutic effect of PVRP and PVRG.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Slovenian Research Agency (Grant Nos. P3-0374, P3-0388, J3-3066, J2-8166, and J2-8169) and University Medical Centre Ljubljana (No. 20210092). The funders had no role in the study's design, in the collection, analyses, or interpretation of data; in the writing of the article; or in the decision to publish the results.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.