
Abstract
Tissue engineering is currently being actively investigated to ascertain if it can offer an alternative to prosthetic aortic heart valves that may overcome the current limitations of prosthetic aortic heart valves while at the same time conferring the advantages of a living autologous structure, such as biocompatibility, the capacity to grow, repair, and remodel. In vitro studies have shown tissue-engineered heart valves to have adequate structural and functional properties, indicating a promising future for heart valve tissue engineering. However, criteria are required to be able to evaluate autologous heart valves and to deem them satisfactory for clinical use. Preclinical animal studies are needed, as a precursor to long-term in vivo follow-up studies, to establish such criteria. The first challenge is to find appropriate techniques to evaluate the functionality of tissue-engineered heart valves in vivo without having to kill the animal. As such, the development of such noninvasive techniques that are able to assess the functionality of tissue-engineered heart valves is the next step in translational research. This review discusses methods of evaluating the functionality of autologous heart valves when translating from in vitro to in vivo studies and determines potential assessment criteria imperative to achieve clinical applicability of tissue-engineered heart valves in aortic valve replacement.
Introduction
Tissue engineering is currently being actively investigated to ascertain if it can offer an alternative to prosthetic aortic heart valves that may overcome the current limitations of prosthetic aortic heart valves while at the same time conferring the advantages of a living autologous structure, such as biocompatibility, the capacity to grow, repair, and remodel.6–9 Autologous heart valve tissue engineering begins with a (biodegradable synthetic or biological) preshaped carrier or scaffold in the form of a heart valve, which is then seeded with cells.10,11 In different approaches to scaffold development, either the valve leaflets 11 or a valved conduit resembling the aortic root can be formed. However, tissue-engineered valve leaflets lack sinus space formation, whereas tissue engineering of a valved conduit, mimicking the aortic root, poses serious challenges in terms of acquiring adequate mechanical properties and tissue quality. 12 This scaffold functions as a temporary matrix for cell support and anchorage preferably until the seeded cells have produced their own extracellular matrix (ECM) proteins. Potential cell types used for scaffold seeding are differentiated tissue-specific cells, such as endothelial and/or smooth muscle cells, and autologous or allogenic progenitor cells, such as umbilical cord–derived cells or mesenchymal stem cells.7,13–15 Second, an in vitro stage of tissue formation in a bioreactor follows. In heart valve tissue engineering, bioreactors aim to improve tissue formation, organization, and function by exposing the developing tissue to mechanical and biological stimuli, primarily through cyclical flow and pressure changes.16–19 The in vitro procedure takes approximately 3–4 weeks.7,10,11,19 Third, the heart valve construct can be implanted, succeeded by an in vivo stage of tissue remodeling and growth to recapitulate normal tissue architecture and function.8,20 A variance to this paradigm is to use decellularized xenograft or allograft valves as scaffolds instead.8,21,22
Currently, the research process has entered the phase of developing a means to translate the tissue-engineered products to clinical practice. Despite the demonstration of proof-of-concept and motivating results in animal models, translation of autologous tissue-engineered heart valves to humans using biodegradable scaffolds as cell carriers has not been accomplished.7,8,21–26 This is mainly due to the fact that the field suffers from the lack of established criteria and quality markers to determine when tissue-engineered heart valves can be qualified as satisfactory for long-term in vivo survival and thus application in patients. To establish such criteria, preclinical animal studies with long-term follow-up are required, based on which predictive models can be derived that can possibly be used for evaluating outcome of implanting tissue-engineered heart valves in humans. As such, it is preferable to apply methodologies that are desig] for valve assessment in humans, to animal models. Therefore, combined with computer models on tissue growth and remodeling, clinical epidemiology incorporating predictive models on late valve function should be used to monitor at least comparable valve function as observed by the use of prosthetic valves. 27
It is vital to find appropriate criteria to accurately assess the functionality and efficacy of tissue-engineered heart valves. Accurate functionality assessment is dependent on the evaluation of valve durability, biocompatibility, biomechanical properties, and the capability to grow, repair, and remodel in vivo. These properties need to be evaluated against a gold standard before and after implantation. With respect to autologous tissue-engineered heart valves, the aim must be for a design that mimics functionally, if not structurally, the performance of a healthy native heart valve in vivo or at least be of similar, and preferably better functional quality, as the heart valve replacements currently in use. Specifically, tissue-engineered heart valves are required to express adequate mechanical function, sustained durability, sufficient hemodynamic performance and not lead to immunogenic, thrombogenic, and/or inflammatory reactions, for example, due to breakdown/degradation products of the scaffold.28,29 It is also imperative, with respect to the role of tissue-engineered heart valves in treating congenital heart disease in pediatric patients or young adults, that the tissue-engineered heart valve shows the ability to grow and remodel.
This article will discuss methods of evaluating the functionality of autologous tissue-engineered aortic heart valves when translating from in vitro to in vivo studies, by first, briefly describing the native aortic heart valve structure and function, and second, reviewing methods to evaluate structural integrity, endothelial function, the capacity to grow and remodel, and biomechanical functionality and hemodynamic stability of autologous tissue-engineered heart valves. In addition, we will highlight the challenges and shortcomings of techniques that may hamper in vivo follow-up primarily in animals and eventually in patients, and as such determine potential assessment criteria crucial to achieve clinical applicability of tissue-engineered heart valves in aortic valve replacement. Further, we will highlight the importance of obtaining evidence in animal models for predictive models on long-term efficacy.
Aortic Heart Valve Tissue Structure
Aortic heart valves are composed of supporting structures in the aortic root, a fibrous ring, and three cusps that seem to open when exposed to forward flow and then rapidly and completely close under minimal reverse pressure. However, it has been shown that the opening of the valve precedes the forward movement of blood from the ventricle, rather than in response to it.30,31 This illustrates the complex function of the valve and is one of the reasons as to why one should consider movements of the whole root, form the level of the annulus to the sinotubular junction when attempting to recapitulate the workings of the native valve. 32 Aortic heart valves maintain unidirectional blood flow during the cardiac cycle due to mechanical forces exerted by the surrounding blood and heart. The dynamic structure of aortic heart valves enables them to avoid excess stress concentration on the cusps and supporting tissues and allows them to withstand wear and tear of repetitive deformations over many years. 33 This function is dependent on the integrity and coordinated movements of the cuspal attachments and dynamics of the aortic root structures. 34
The native healthy aortic heart valve consists of two types of cells: valvular interstitial cells (VICs) that permeate the entire valve tissue and endothelial cells, which cover the surface. VICs are responsible for the synthesis of the ECM and express matrix degrading enzymes (matrix metalloproteinases [e.g., MMP-1, MMP-2, MMP-9, and MMP-13] and cathepsins [e.g., cathepsin S, K, and B], and tissue inhibitors [e.g., tissue inhibitors of metalloproteinases (TIMP) 1–4]), which mediate matrix remodeling. 29 VICs in the healthy aortic valve mainly have quiescent fibroblast-like properties but can change to an activated phenotype during valvular remodeling, response to injury, or pathology. The endothelial cells covering the native heart valve regulate immune and inflammation responses and provide the native heart valve with its nonthrombogenic properties. 35
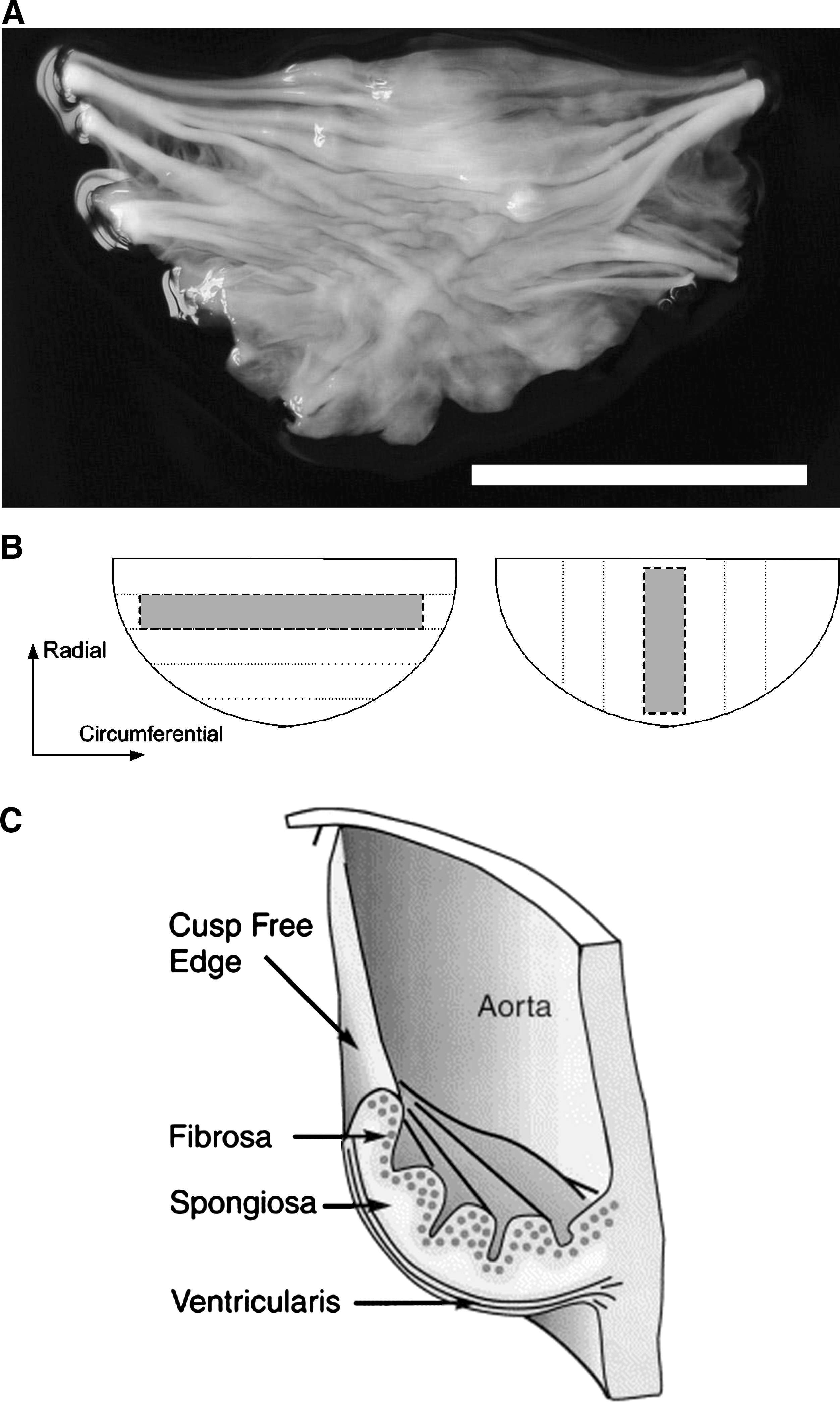
The ECM of the aortic heart valve is organized into three layers: (i) the zona ventricularis, closest to the left ventricle chamber and largely composed of elastin, which is able to extend in diastole and recoil in systole to minimize cusp area, (ii) the zona fibrosa, closest to the outflow surface, rich in densely packed collagen organized in radial and circumferential direction, which provides the strength and stiffness of the cusps and is mainly responsible for bearing diastolic stress, and (iii) the centrally located zona spongiosa, which mainly consists of glycosaminoglycans (GAGs), responsible for accommodation of shear forces of the cuspal layers and functions as a shock absorber during the valve cycle.3,8,29,36
This organization of the aortic native heart valve allows for certain unique qualities (Fig. 1). First, there are accordion-like folds present in the valve cusps, called corrugations, which allow for the cuspal shape and dimensions to vary with the cardiac cycle. Second, to allow lengthening of the valve at minimal stress, microscopic collagen folding, also known as crimp, exists. Additionally, the cusp tissue displays, anisotropy, the quality conferred by collagen architecture that permits differences in radial and circumferential extensibility. Finally, the macroscopic collagen alignment enables forces from the cusps to transfer to the aortic wall. 37 By employing these properties, the native heart valve avoids excess stress concentration on the cusps and supporting tissues and allows it to withstand biomechanical loads caused by repetitive deformations. In addition, biomechanical stress may induce remodeling and repair of connective tissue. 33 In particular, when stimulated by mechanical loading, VICs become activated and mediate connective tissue remodeling to restore a normal stress profile in the tissue. 38 Mechanical forces acting on the valve are translated into biological responses at the tissue level, which in turn lead to a VIC response at cellular level. Intracellular signaling leads to changes such as increased VIC stiffness and increased ECM biosynthesis. Concurrently, the higher valvular pressure gradients on the left side of the heart lead to larger local tissue stress on the VICs which that leads to higher VIC stiffness and collagen biosynthesis in the left-sided valves. 39
(
Structural Assessment
The ECM, consisting of collagen, elastin, and GAGs and with its unique organization, plays an essential role in the structural integrity of the native heart valve. It is the fundamental requirement for the long-term performance of a native aortic heart valve. Collagen is mainly responsible for structural integrity and biomechanical strength, predominantly tensile strength or tissue stiffness,40,41 whereas elastin provides tissue resilience, and GAGs enable valve tissue to withstand compressive forces. It is therefore necessary to assess the components of the ECM qualitatively and quantitatively in the tissue-engineered valve and compare it to the structural appearance of the native heart valve ECM, which can be viewed as the gold standard.
Presently, the most commonly used assessment method for ECM formation in tissue-engineered heart valves is to explant the tissue-engineered constructs, thereby killing the animals at different time intervals, and comparing tissue structure to the native heart valve using histology or immunohistochemistry. Hematoxylin and eosin staining is used for general tissue morphology, and trichrome Masson's and Movat's pentachrome methods are examples of methods used to asses matrix composition.7,11,42 It has been shown that tissue-engineered constructs directly after the bioreactor phase have comparable ECM components and composition as native neonatal heart valve leaflets.10,42 Animal studies in which tissue-engineered heart valves are explanted after different time intervals have demonstrated that tissue-engineered heart valves remodel in time into three tissue layers.7,26,43 However, the degree of anisotropy in the tissue-engineered leaflets is lower when compared with adult native leaflets. This results in mechanical behavior in the circumferential direction which is inconsistent with the adult native heart valve. 11 Despite these findings, it is hypothesized that the valve leaflets are able to remodel in vivo once implanted and will adapt to a higher degree of anisotropy. Additionally, Aikawa et al. demonstrated that collagen adapts to the prevailing hemodynamic environment in human heart valves, which results in maturing of the collagen through increased fiber thickness and alignment. 38
Elastin ensures optimal valve closure. Immunohistochemical evaluation by monoclonal antibodies for elastin, and van Geison and Movat's pentachrome methods are the preferred assessment tools. Notably, studies have shown insufficient in vitro and in vivo elastin synthesis in present tissue-engineered heart valves. 11
Quantitative assessment of tissue formation and growth is generally done by evaluating DNA content, as an indicator of cell number and collagen, elastin, and GAG content. By normalizing collagen, elastin, and GAG content for the amount of DNA, a measure for the amount of these matrix components produced per cell can be obtained and compared to the normalized content of a native heart valve.26,42 As such, tissue proliferation and maturation can be assessed.
Conventional imaging techniques are limited to in vitro studies and require the invasive removal of tissue samples, the slicing by microtomes, embedding, fixation and staining procedures, or antibody labeling, preventing the investigation of dynamic progression of engineered tissues. Multiphoton fluorescence excitation, based on the simultaneous absorption of two or more near infrared photons, enables the nondestructive high-resolution deep tissue imaging of endogenous fluorophores. 44 Konig et al. used this novel technique to probe the ECM of tissue-engineered heart valves under different culture conditions. 45 The quality of the resulting images allowed the exact differentiation of collagenous structures and elastin fibers. However, this technique is limited by the fact that polymer scaffolds often have fluorescent properties that interfere with collagen examination. Additionally, the depth of multiphoton fluorescence is restricted. 46 Promising developments in the field of needle-like multiphoton endoscopes based on microsystem technology will hopefully allow in situ intrabody tissue imaging in the near future. 47
The evaluation of structural integrity in vivo remains a challenge, but is, however, necessary to establish functionality criteria of the autologous tissue-engineered heart valve. Additionally, it is crucial to develop noninvasive methods to monitor matrix development over time, without killing animals.38,48 This should eventually lead to long-term functionality assessment studies in animal models and clinical studies. Magnetic resonance imaging (MRI) holds great promise in terms of examining matrix development of an autologous tissue-engineered heart valve in vivo. In two studies the collagen fibril formation and remodeling process were elucidated by real-time imaging of the local three-dimensional collagen organization.41,49 Krahn et al. have recently developed a collagen-specific fluorescent probe, which examines collagen organization in vitro in great detail. 49 The probe also allows for real-time monitoring of collagen synthesis in cell culture, which means that the active change in collagen organization can be studied. Currently, an MRI-compatible version of the probe is under development which may lead to noninvasive assessment of structural integrity, by means of matrix observation of tissue-engineered heart valves in vivo.
Endothelial Function
Successful application of tissue engineering to clinical practice is dependent on the ability of tissue-engineered constructs to control the foreign body reaction of the native immune system and cooperate with the directed remodeling process. 50 The endothelial layer, covering the surface of the native heart valve, provides anti-thrombotic properties and plays an important role in this remodeling process. Compared with grafts that are repopulated with endothelial cells, decellullarized allografts show increased thrombogenicity and an elevated risk for structural deterioration.22,51 Therefore, a functional endothelial layer on a prosthetic heart valve is crucial for thromboembolic event-free survival in heart valve recipients. Moreover, it is believed that the valvular endothelium regulates valve tissue remodeling by a feedback mechanism between the endothelial cells and VICs. Cytokines have been shown to cause changes in interstitial cell structure and function. However, at present no direct junctions have been observed between the valvular endothelium and VICs.29,35,52
These elements of biocompatibility are fundamental to create functional heart valve tissue. 50 Lichtenberg et al. demonstrated that in vitro reendothelialization of detergent-decellularized valves with autologous endothelial cells under simulated physiological conditions significantly improved the endothelial cell coverage of the matrix and prevented thrombotic formations within 3 months after implantation in a large animal model. 53 The endothelium of tissue-engineered heart valves has been characterized by surface expression of CD31, von Willebrand factor, and vascular endothelial growth factor receptor FLK-1. 22 Nitric oxide expression is used as a measure of endothelial functionality and can be evaluated by analyzing endothelial nitric oxide synthase, which produces nitric oxide. Endothelial nitric oxide synthase can be observed with immunohistochemistry by applying primary antibodies. 54 However, all the above investigations require explantation of the tissue-engineered heart valve and thus euthanization of animals.
Recently, an in vivo method was described to demonstrate endothelial cell activation in mice.48,55,56 Vascular cell adhesion molecule-1 (VCAM-1) expression was seen using a peptide derivatized VCAM-1–targeted magnetofluorescent nanoparticle. The nanoparticle triggers cellular internalization, which amplifies a biological signal detectable by MRI. Additionally, contrast-enhanced ultrasound imaging of VCAM-1–targeted microbubbles has been used to examine endothelial cell changes. 57 However, VCAM-1 molecular imaging has mainly been the focus of visualizing the inflammatory process of aortic valve disease, as this molecule is not detected in normal endothelium. 48 VCAM-1 mediates adhesion of leukocytes to endothelial cells and is mainly expressed as an inflammatory response 58 or as a response to endothelial cell activation/injury. 48 Applying VCAM-1–targeted molecular imaging agents could be used to evaluate tissue-engineered heart valve endothelial function in vivo, since VCAM-1 has shown to be associated with valvular tissue remodeling in fetal valve development and disease progression.38,48 Despite these findings, successful in vivo observation of VCAM-1 expression of autologous tissue-engineered heart valves, particularly monitoring the endothelial cell activation in large animal models or humans, remains warranted.
Growth, Repair, and Remodeling
A vital function of the native heart valve is the ability to remodel and regenerate potential structural deteriorations caused by excessive repetitive biomechanical stress. Growth and remodeling of tissue-engineered heart valves are evaluated by assessing change in structure and volume, of native ECM, mirrored by the change in its synthesis and degradation, which in turn is reflected by distribution of active VIC phenotypes. The exact mechanism of modeling the three-layer structural organization specific for native aortic heart valves is unclear. However, change in mechanical forces is associated with phenotypic changes of VIC. 38 More specifically, environmentally activated VIC are myofibroblast-like cells that synthesize ECM components and express MMPs and TIMPs. Remodeling and development primarily consists of degradation of ECM by MMPs and synthesis of new ECM by VIC. As such, MMP expression and TIMPs are important indicators for tissue remodeling.
Histological studies have used immunohistochemical staining using monoclonal antibodies against MMPs to demonstrate MMP expression. Additionally, mRNA precursors for protein synthesis can be assessed by evaluating collagen I, III, and elastin gene expressions. 59 Further, tissue sections are stained for vimentin and α-smooth muscle actin, the indicators of myofibroblast-like cells, which represent activated VICs responsible for matrix remodeling.42,60 Thus, by comparing samples of valves harvested at the time of implantation and samples of valves explanted after a certain period of time, growth, and remodeling of tissue-engineered heart valves can be demonstrated on a histological level, by evaluating volume, matrix composition, or cell phenotype changes of the valve tissue. As such, research has demonstrated that native porcine aortic valve leaflets exposed to hypertensive cyclic pressure showed increased collagen and GAGs synthesis that varied in a magnitude and frequency-dependent manner. 61 Additionally, exposing native porcine aortic valve leaflets to isolated effects of flow, laminar steady shear stress, and constant static and cyclic pressure resulted in a reduced level of expression of α-smooth muscle actin. 62
The current challenge in tissue-engineered heart valve assessment is to noninvasively evaluate growth and remodeling potential in vivo. Growth potential of a vascular tissue-engineered graft has been demonstrated in vivo by Hoerstrup et al. 26 The authors evaluated functional performance by means of two-dimensional (2D) Doppler echocardiography and computed tomography (CT) angiography at different time intervals and concluded that the absence of thrombus, calcification, stenosis, suture dehiscence, or aneurysm formation underlines the functionality and the capacity to adapt to a changing environment. Growth potential of tissue-engineered heart valves might be studied by implanting the valves in young animals and monitor the diameter and function of the valves during growth of the animals. Increase in diameter of the valve without regurgitation can then be subscribed to growth, whereas increase in diameter with regurgitation is more likely to be caused by dilation. In addition, normal or expected growth can be determined from normal connection to the surrounding (and also growing) tissue, whereas dilated tissue will show a mismatch with the neighboring host tissue. To evaluate remodeling and repair potential of tissue-engineered heart valves in vivo, MMP and TIMP, collagen, elastin, and GAG expression pose interesting imaging targets. Indeed, recent molecular imaging studies used an activatable molecular imaging agents to examine proteolytic enzyme activity (e.g., MMP-2, MMP-9, cathepsin B, and cathepsin K) in early aortic valve disease and atherosclerosis.48,63,64 In addition, the collagen probe developed by Krahn et al. might be further developed to noninvasively view collagen synthesis as a structural integrity assessment.49,65 VCAM-1 expression observation also poses an interesting imaging target in terms of examining growth and remodeling potential in vivo in the tissue-engineered construct. The endothelial cell layer of heart valves works synergistically with VIC in the process of growth, repair, and remodeling. Therefore, VCAM-1, being a marker for an active endothelial cell layer, can also be viewed as a marker for valvular tissue remodeling. 38
Biomechanical and Hemodynamic Assessment
The unique structure and morphology of the native heart valve is responsible for its biomechanical properties and hemodynamic performance. Pressure gradients across cardiac valve prostheses have been identified as one of the most important performance measures in valve replacement surgery. Specifically in aortic valves, these gradients influence reduction of left ventricular hypertrophy and are postulated to influence long-term survival. 66
These functional characteristics are equally important in tissue-engineered heart valve assessment. When translating tissue-engineered constructs from in vitro to in vivo studies, it is important to validate mechanical and hemodynamic function and opening/closing motion before implantation. Generally, uniaxial or biaxial tension tests have been used to measure mechanical properties of tissue-engineered valve leaflets in vitro.10,11 Forces acting on the tissues as a response to elongation are represented in stress–strain curves, from which tissue strength, tissue extensibility, tissue stiffness, and even anisotropic properties can be derived. By comparing results from this method to data available from native healthy heart valve performance, the mechanical properties of a tissue-engineered heart valve can be assessed before implantation or after explantation. Recently, a valve performance tester has been developed, in which simulated physiological aortic flows can be generated to create an environment that mimics the systemic circulation. 11 This tester can be used to evaluate tissue-engineered heart valve function ex vivo from parameters such as transvalvular flow velocity, pressure gradients, and effective orifice area can be measured.
Accelerated mechanical testing, required for the assessment of mechanical heart valves, is less appropriate for the evaluation of engineered heart valves. The high, nonphysiologic, frequencies applied during these tests are not representative of the normal cellular and tissue environment and hence will provoke unknown and unrealistic responses of the living tissues. In addition, the long test period required for such tests bears the risk of contaminating the living tissue in due time.
After implantation, in vivo noninvasive techniques, such as echocardiography, CT, and MRI, have proven useful in determining mechanical function of prosthetic heart valves. Doppler and 2D echocardiography are imperative diagnostic tools, but have also proven to be essential in the postoperative follow-up of patients after heart valve replacement. By means of assessing postoperative graft geometry, and comparing these baseline data to subsequent follow-up measurements, clinicians are able to assess the functional development of prosthetic heart valves. 67 The following hemodynamic indices of prosthetic heart valves are measured by means of Doppler echocardiography: prosthesis size, peak velocity across the valve, mean and maximum pressure gradient, left ventricular outflow tract velocity, aortic valve area, and root dimensions. 68 From these measurements, the effective orifice area can be calculated which is a measure of the presence and severity of stenosis. The calculated effective orifice area and pressure gradients can be compared to the range of those reported for commonly accepted bioprostheses. 66 Two-dimensional echocardiography focuses more on measures of left ventricular wall thickness and leaflet motion. Although transesophageal echocardiography has proven to be superior to transthoracic echocardiography in evaluating prosthetic heart valves or diagnosing valvular disease,69,70 in clinical practice transesophageal echocardiography is used when transthoracic echocardiography is unable to delineate the cause of valve failure.
Due to its practical, cost-effective, readily available, and noninvasive nature, echocardiography has been applied frequently in in vivo studies of prosthetic heart valve to evaluate the mechanical function and hemodynamic performance. However, due to an underestimation of parameters by echocardiography and interobserver variability, 71 other technologies have been pursued to evaluate biomechanical function of heart valves. Similar to using transesophageal echocardiography to evaluate heart valve function, multidetector row CT has proved to show a reliable high-qualitative observation of aortic heart valve function. Moreover, in contrast to echocardiography, multidetector row CT can quantify aortic valve calcification. 72 Additionally, MRI is useful in examining mechanical and hemodynamic performance of heart valves. T2-loaded MRI can demonstrate blood flow velocity, valve opening and closing motion, and valvular dysfunction. In addition, T2-loaded MRI is especially able to quantify regurgitation volumes.
In vivo follow-up should in addition to the aortic valve leaflets also include the assessment of the aortic root. Flow patterns in the aortic root might affect aortic valve function by allowing load and stress sharing between the valve leaflets and the aortic wall. 73 There is theoretic support for the concept that prompt and smooth closure of the valve might rely on the presence of normal aortic root flow. 74 Quantifying aortic root blood flow therefore poses interesting possibilities in evaluating the functional performance of a tissue-engineered heart valve in vivo. Aortic blood flow can be evaluated by MRI using three-dimensional time-resolved particle traces and velocity vector fields, which are reformatted onto 2D planes. 75 This technique examines aortic flow dynamics in patients undergoing aortic valve or root surgery, and thus poses an interesting assessment method of the aortic root functionality. The intrinsic sensitivity of MRI with respect to flow and motion offers the unique capability to acquire cardiac gated and spatially encoded functional information simultaneously with morphological data. 76 In addition, the opening and closing motion of the valve leaflets during the cardiac cycle is supported by vortex formation in the sinus of Valsalva. Experimental noninvasive techniques, such as laser Doppler anemometry and particle image velocimetry, are techniques that have been developed to gain insight into hemodynamic and functional-related aspects of heart valves. They have proven to perform velocity measurements and accurately evaluate fluid dynamical performance, which is of great interest for valve design. 77
Discussion
Autologous tissue-engineered heart valves have the potential to overcome the limitations of current prosthetic heart valve replacements in treatment of aortic valve disease. This technology aims to create living heart valve substitutes in vitro by seeding cultured autologous cells on heart valve–shaped biodegradable scaffolds. The tissue-engineered construct is then conditioned in a bioreactor before implantation into the (human) heart. However, challenges remain to successfully translate autologous tissue-engineered heart valves to clinical practice. Next to finding the optimal cell source, scaffold material, conditioning environment, and surgical handling, the need exists to find means to accurately evaluate the functionality of the tissue-engineered construct before implantation to establish quality criteria that characterize the tissue-engineered heart valve as “good enough” for clinical use.
A tissue-engineered heart valve can be viewed as cardiac valve prosthesis and/or as living tissue. For that reason, creating tissue-engineered heart valves is subject to the criteria for new cardiac valve prostheses as defined by the International Standard Organization (ISO), which outlines an approach for qualifying design and manufacture of a heart valve substitute through risk management. 78 However, considering the nature of tissue-engineered heart valves also to be living tissue, the ISO standard is not sufficient.
Long-term in vivo follow-up studies are the preferred approach to provide for data that can be used to establish accurate quality criteria as mentioned before. Especially the structure–function relationship should be the focus of active research. As has been previously demonstrated by others and outlined in this article that the functional properties of an aortic heart valve are correlated with its structure. Therefore, structural integrity, endothelial function, the ability to grow and remodel, and biomechanical and hemodynamic properties are the major parameters of autologous tissue-engineered heart valve functionality assessment. A possible study paradigm to evaluate the clinical performance of autologous tissue-engineered heart valves to establish such criteria is presented (Fig. 2).

Clinical performance evaluation of autologous tissue-engineered heart valves. Autologous heart valve tissue engineering paradigm; autologous cells are seeded on biodegradable on-demand scaffolds and inserted into a bioreactor that simulates physiological conditions to promote tissue growth, after which tissue-engineered valve is implanted into animal or human heart. Functionality assessment occurs (a) before implantation by means of in vitro testing and functionality tester and (b) during follow-up by means of echocardiography and biomedical imaging. Data acquired should be compared to native heart valves or bioprosthetic heart valves at similar time intervals. Implantation criteria can be established in vitro. Functional prediction models can be derived from in vivo follow-up.
The next step in successfully translating heart valve tissue engineering to in vivo follow-up studies is the development of in vivo noninvasive techniques that are able to assess the functionality of tissue-engineered heart valves, without having to explant the tissue-engineered heart valve. This could potentially lead to important tools usable by physician. Biomedical imaging seems to provide successful means for long-term in vivo nondestructive monitoring of tissue-engineered heart valves. In particular, MRI and evolving molecular imaging approach have the ability to view ECM components and functional endothelium, and monitoring growth and remodeling in vivo.
It is questionable whether the assessment of these previously discussed parameters is of equal importance in terms of evaluating the performance of autologous tissue-engineered heart valves in vivo. The main function of heart valves is to provide for a unidirectional flow of blood without causing obstruction or regurgitation, trauma to blood elements, thromboembolism, or excessive mechanical stress in the cusps and leaflets. 29 Normal valve function is thus a result of structural integrity, coordinated interactions among supporting structures and leaflets, endothelial cell and VIC functions, and the capacity to grow and remodel. These properties are responsible for the biomechanical and hemodynamic performance of heart valves. Hence, one can argue that the evaluation of the biomechanical and hemodynamic performance of tissue-engineered heart valves in vivo is sufficient to the task of functional performance evaluation. This would entail using 2D and Doppler echocardiography, which also forms the backbone of postoperative management of patients with prosthetic heart valves according to the American College of Cardiology/American Heart Association guidelines. 68 Although CT and MRI techniques show added value in terms of intraobserver validity, sensitivity, and specificity, the advantages of functional assessment by means of echocardiography presently outweigh those of CT and MRI, mainly because of its experienced use in clinical practice, low user threshold, and low costs. It is nonetheless imperative to evaluate growth and remodeling, because this is the main advantage and difference with contemporary heart valve replacements. The main challenge of remodeling assessment is that it is not possible to make a comparison to a gold standard; however, alternatively, over time tissue-engineered heart valves can be compared to data from the tissue-engineered heart valve at implantation.
Before entering the clinical phase, new prosthetic heart valves need to be evaluated in a large animal model. Although the ISO standard does not hold a preference for any animal model and merely states that implant animals should be of the same species, the animal of choice for in vivo studies of tissue-engineered heart valves for the development of new assessment approaches is sheep. 79 The anatomic and hemodynamic properties are adequately equivalent to the human situation. In addition, sheep are viewed as “the worst case model,” due to increased calcium metabolism leading to degenerative processes in a relatively short period of time. 80 Most importantly, the juvenile sheep are full grown within 2 years, allowing for relatively fast evaluation of growth and development. As described before, functional development of prosthetic heart valves is estimated by comparing postoperative follow-up measurements to baseline data acquired immediately after implantation and to control valves comprising of mechanical and/or bioprosthetic valves. The observation period of functional performance assessment in the juvenile sheep model should be no less than 90 days. 78 Following animal experiments, clinical studies must evaluate the functionality of tissue-engineered heart valves. Assessing tissue-engineered heart valve performance in humans would require numerous patients to be studied, upon which evaluation times should at least be similar to the American College of Cardiology/American Heart Association guidelines for postoperative management of patients who have acquired prosthetic heart valves: 2–4 weeks after tissue-engineered heart valve implantation followed by the minimum of annual follow-up assessment. 68 However, pursuing clinical applicability in humans, species-specific differences between humans and sheep are relevant for the development of assessment criteria. Preclinical studies and assessment of the autologous tissue-engineered heart valves in animals do not guarantee success in humans.
In conclusion, autologous heart valve tissue engineering holds a promising future for surgical heart valve replacement; however, criteria are needed to evaluate autologous heart valve tissue engineering as good enough for clinical use. Long-term in vivo follow-up studies are needed to establish such criteria; however, the challenge remains to find appropriate means to evaluate the functionality of tissue-engineered heart valves in vivo. Biomedical imaging holds great promise in overcoming this hurdle and is the next step in translating heart valve tissue engineering from bench to bed.
Footnotes
Acknowledgments
The authors would like to thank Dr. E. Aikawa (Department of Pathology and Center of Molecular Imaging Research, Harvard Medical School, Massachusetts General Hospital, Boston, MA) and Dr. G. Strijkers (Eindhoven University of Technology) for their useful comments in preparing this manuscript.
Disclosure Statement
No competing financial interests exist.