
Abstract
Biomaterials are native or synthetic polymers that act as carriers for drug delivery or scaffolds for tissue regeneration. When implanted in vivo, biomaterials should be nontoxic and exert intended functions. For tooth regeneration, biomaterials have primarily served as a scaffold for (1) transplanted stem cells and/or (2) recruitment of endogenous stem cells. This article critically synthesizes our knowledge of biomaterial use in tooth regeneration, including the selection of native and/or synthetic polymers, three-dimensional scaffold fabrication, stem cell transplantation, and stem cell homing. A tooth is a complex biological organ. Tooth loss represents the most common organ failure. Tooth regeneration encompasses not only regrowth of an entire tooth as an organ, but also biological restoration of individual components of the tooth including enamel, dentin, cementum, or dental pulp. Regeneration of tooth root represents perhaps more near-term opportunities than the regeneration of the whole tooth. In the adult, a tooth owes its biological vitality, arguably more, to the root than the crown. Biomaterials are indispensible for the regeneration of tooth root, tooth crown, dental pulp, or an entire tooth.
Introduction
Tooth regeneration has long been the dental profession's aspiration. However, it was not until the recent past that experimental approaches for tooth regeneration have been made possible by advances in cell biology and bioengineering. Cells are the building blocks of multiple tissues in a tooth organ, including ameloblasts that form the enamel, odontoblasts that form dentin, cementoblasts that form the cementum, and cells of multiple lineages including mesenchymal, fibroblastic, vascular, and neural cells that form dental pulp. Collectively, enamel, dentin, cementum, and dental pulp form a tooth or tooth organ. Tooth regeneration encompasses not only regrowth of an entire tooth as an organ, but also biological restoration of individual components of the tooth including enamel, dentin, cementum, or dental pulp. However, a tooth cannot function unless it is connected to and supported by the periodontium that includes the periodontal ligament and alveolar bone. Biological scaffolds provide anatomic dimensions of temporary matrices in which cells synthesize tissues and, therefore, play important, if not indispensible, roles in tooth regeneration. Scaffolds provide biophysical support for cell recruitment, adhesion, proliferation, differentiation, and/or metabolism. The primary objective of this review is to synthesize existing literature in the design, fabrication, and application of biological scaffolds in tooth regeneration.
Regeneration of teeth can be divided into several specific areas as follows:
• Regeneration or de novo formation of an entire, anatomically correct tooth
6
; • Regeneration of the root
7
; • Regeneration of dentin that may either act as reparative dentin to seal off an exposed pulp chamber or as a replacement of current synthetic materials11–14
; • Regeneration of cementum as a part of periodontium regeneration or for loss of cementum and/or dentin resulting from orthodontic tooth movement15,16; • Regeneration of periodontium including cementum, periodontal ligament, and alveolar bone17–19
; • Regeneration or synthesis of enamel-like structures that may be used as biological substitute for enamel20–22
;
The native extracellular matrix of a tooth organ provides a scaffold for the recruitment, adhesion, proliferation, differentiation, and metabolism of a broad array of resident cells including odontoblasts, fibroblasts, vascular cells, and neural endings, in addition to stem/progenitor cells. In principle, biological scaffolds for the regeneration of tooth organ should allow the key functions of the native tooth organ. At a minimum, designed biological scaffolds for tooth regeneration should be biocompatible, nontoxic, and promote the regeneration of a single or multiple dental tissues.
Soft Biomaterials
Polymeric hydrogels can be native, synthetic, or hybrid.23–25 Native hydrogels are typically of biocompatibility, low immunogenicity, and with the ability to undergo biocompatible breakdown in vivo. A major drawback of native hydrogels is limited supply. Synthetic hydrogels have the advantage of virtually unlimited supply and can be tailored to possess a broad range of structural, mechanical, and chemical properties. Biologically safe degradation is usually intrinsic with native hydrogels, and frequently one of the desirable properties of synthetic polymers.
Fibrin
Fibrin hydrogel is polymerized from purified allogeneic fibrinogen by purified thrombin.
26
Fibrin has been widely used as scaffolds in the regeneration of cardiovascular tissue,
27
bone,
28
neural tissues,
29
cartilage,
30
and others. Fibrin hydrogel has several advantages such as controllable degradation rate, low immunogenicity, and allow relatively homogenous cell distribution on cell seeding and polymerization.
27
However, fibrin undergoes shrinkage and has low mechanical stiffness.27,31 Fixing agents such as poly-
Collagen
Collagen is a major macromolecule of the extracellular matrix and exists ubiquitously in diverse tissues such as bone, teeth, skin, cartilage, tendon, and ligament.35,36 Collagen type I is frequently extracted and used as a scaffold in tissue engineering.37–39 Allogeneic collagen, such as bovine collagen sponge or bovine collagen gel, has excellent biocompatibility and low immunogenicity in humans.37–39 A major drawback of collagen scaffold is its modest physical strength, 36 although it appears to be sufficient for dental pulp regeneration. 36 Chemical cross-linking by the addition of cross-linking agents such as glutaraldehyde or diphenylphosphoryl azide can enhance the mechanical stiffness of collagen scaffolds.40,41 However, cross-linking agents can compromise cell survival and biocompatibility. 36 Similar to fibrin, collagen's mechanical properties can be enhanced by forming hybrid scaffolds with β-TCP/polyethylene 42 and hydroxyapatite. 43
Collagen scaffolds loaded with a series of growth factors have been implanted in endodontically treated root canals. On in vivo implantation of endodontically treated human teeth in mouse dorsum for the tested 3 or 6 weeks, delivery of basic fibroblast growth factor (bFGF) and/or vascular endothelial growth factor (VEGF) yields re-cellularized and revascularized connective tissue that integrates to the native dentinal wall in root canals 9 (Fig. 1). Similarly, delivery of collagen scaffolds with dental pulp stem cells and dentin matrix protein-1 in tooth slices in mice leads to ectopic formation of dental pulp-like tissue. 10

Regeneration of dental-pulp-like tissues in human teeth.
9
Root canals of endodontically treated human teeth were filled with collage sponges with or without delivery of bFGF and/or VEGF followed by 3-week in vivo implantation. Endodontically treated root canals with collagen sponge alone showed pale access opening
Hyaluronic acid
Hyaluronic acid (HA) is a primary extracellular component of connective tissue and plays an important role in wound healing. The HA is biocompatible and has low immunogenicity.44,45 The HA hydrogel has been exploited in the regeneration of bone, 46 cartilage, 47 vocal cord, 48 and brain. 49 A potential disadvantage of HA hydrogel is its poor mechanical strength and rapid in vivo degradation rate. 48 Accordingly, HA hydrogel can be chemically modified by the carboxylic acid groups such as esterification 50 or methacrylamide, 51 or the alcohol groups modified by divinyl sulfone, 52 diglycidyl ether, or poly(ethylene glycol) diglycidyl ether. 53 The HA hydrogel can also be crosslinked with dialdehyde, 54 dihydrazide, 55 or disulfide. 56 The attachment, spreading, and proliferation of cells in HA hydrogel can be enhanced with arginine-glycine-aspartic acid (RGD) peptides.57,58 The HA hydrogel can also be modified with biotin for probing HA-receptor interactions.57,58
The HA hydrogels have also been widely investigated for applications in tissue regeneration, but their application in dental pulp regeneration is limited. 59 An injectable hydrogel, over pre-shaped hydrogel (e.g., by molding), is often clinically preferable, because pulp chamber and root canal have irregular shape. The odontoblastic cell line (KN-3 cells) readily adheres to both HA or collagen sponges in vitro (Fig. 2). Expression of interleukin-6 and tumor necrosis factor-α by KN-3 cells seeded in a HA sponge is virtually the same as in collagen sponge. When HA and collagen sponges are implanted in amputated dental pulp of rat molars in vivo, the numbers of granulated leukocytes invaded into HA sponge from amputated dental pulp are significantly lower than those in collagen sponge, 59 suggesting that HA sponge has an appropriate structure, biocompatibility, and biodegradation for use as a scaffold for dental pulp regeneration. 59
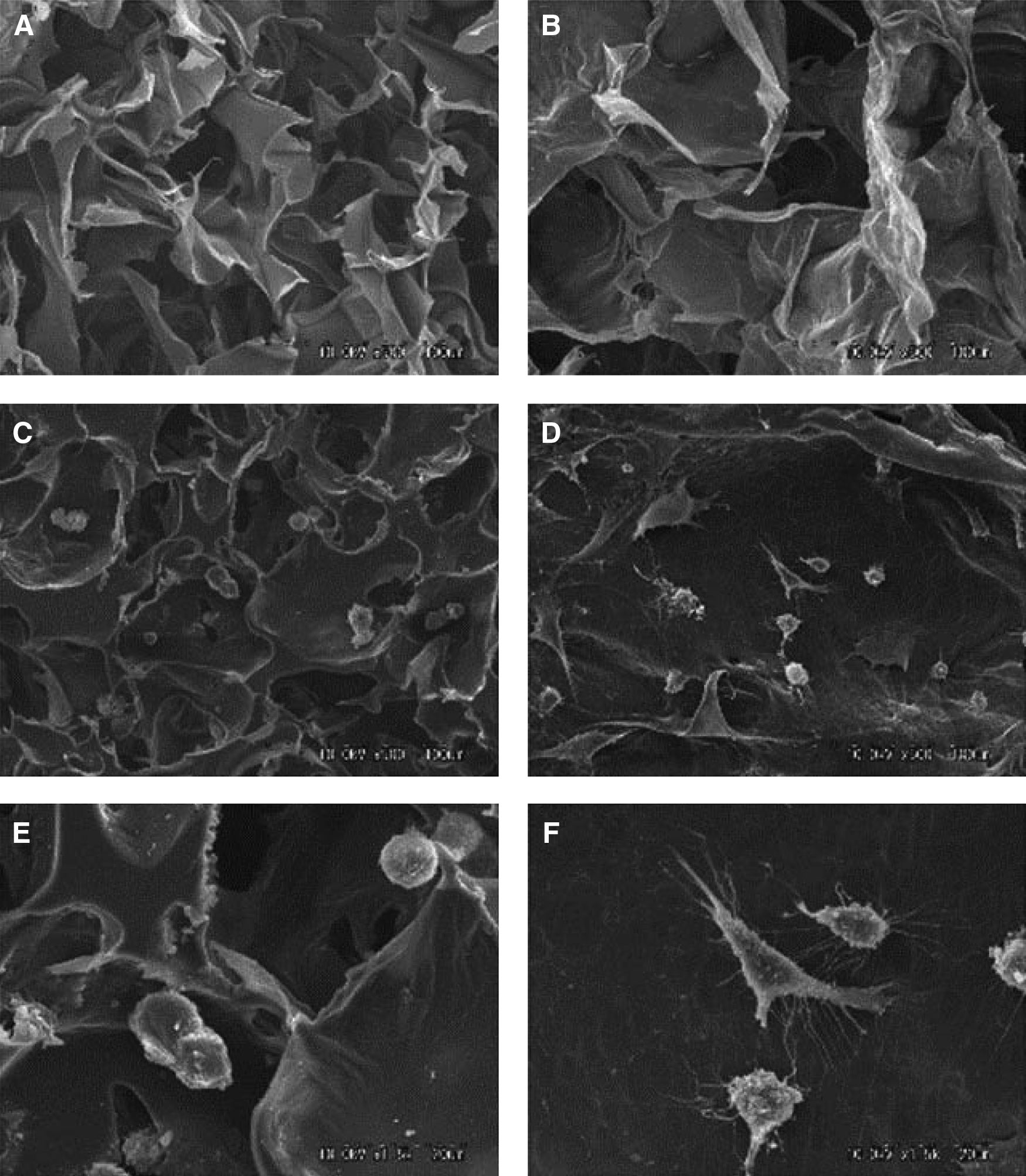
Scanning electron microphotographs of HA
Poly(ethylene glycol)-based hydrogel
Poly(ethylene glycol) (PEG) is a nontoxic, water soluble, and biocompatible polymer. PEG has low immunogenicity and can undergo in vivo degradation. PEG is generally resistant to cell and protein adsorption, and has been widely explored as a drug delivery carrier. 60 Recently, PEG hydrogel has been explored as a scaffold material for tissue regeneration,61,62 including de novo formation of a structure in the shape of a temporomandibular joint regeneration.61,62 Compared with native hydrogels, PEG has several advantages such as the ability for photopolymerization, easy control of scaffold structure, and chemical composites. Poly(ethylene glycol) diacrylate (PEGDA), a chemical modification of PEG, is formed by the substitute of terminal hydroxyl groups with acrylates. 63 PEGDA can be crosslinked by a variety of methods. 64 The mechanical strength of PEG hydrogel depends on the molecular weight, cross-linking, and concentration. The elastic modulus can be enhanced by reducing the molecular weight or increasing polymer concentration.65–67 The permeability and mesh size of PEGDA are determined by molecular weight and concentration. 68
Vascularization is pivotal for tissue regeneration. In an in vivo investigation, biophysical and/or biochemical approaches are combined to induce neovascularization in PEGDA hydrogel. 69 Hydrogel cylinders are fabricated from PEGDA in four configurations: PEG alone, PEG with bFGF, microchanneled PEG alone, or both bFGF-adsorbed and microchanneled PEG (Fig. 3A–C). In vivo implantation reveals no neovascularization in unmodified PEG, but substantial angiogenesis in bFGF-adsorbed and/or microchanneled PEG. Strikingly, substantial angiogenesis is also present in microchanneled PEG without bFGF incorporation. The striking difference of neovascularization between unmodified PEG and microchanneled PEG suggests that microchannels provide a conduit for angiogenesis. Especially, engineered microchannels may provide a generic approach for modifying existing scaffolds by providing conduits for vascularization and/or cell metabolism. The separate or combined approaches to induce vascularization may be of relevance to dental pulp regeneration.
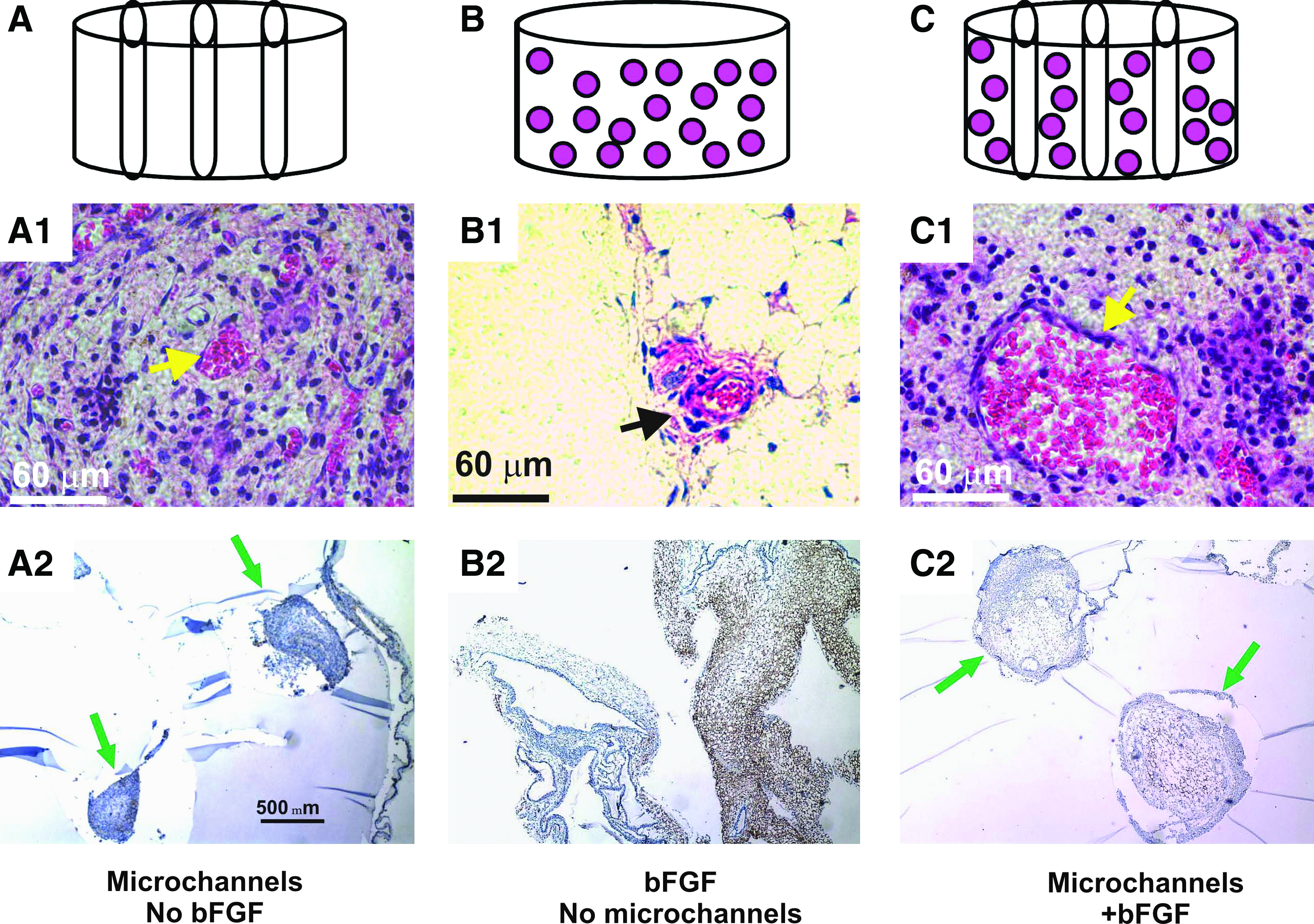
Induction of cellular ingrowth and angiogenesis in PEG hydrogel. After in vivo subcutaneous implantation in the dorsum of immunodeficient mice, the harvested PEG hydrogel samples showed distinct histological features.
Alginate
Alginate is a naturally derived polysaccharide and has been widely used as a scaffolding material in tissue regeneration. Alginate is nontoxic, biocompatible, and permeable to small molecular-weight proteins. 70 However, alginate has several drawbacks including low mechanical stiffness and difficulty to control in vivo degradation rate. Alginate prepared with ionic cross-linking has weak mechanical stiffness, 71 although its mechanical strength can be improved by increasing calcium content and cross-linking density. 72 Compared with ionic crosslinking, stable covalent cross-linked alginate hydrogels have greater mechanical strength and swelling ratio. 73 γ-irradiation is a reliable and straightforward approach for the generation of a stable alginate hydrogels. 74 To address the issue of nonspecific cellular interactive property, the RGD modified alginate hydrogel promotes cell adhesion, spreading, proliferation, and differentiation.75,76
Alginate hydrogel has been loaded with exogenous transforming growth factor TGFβ1 for the regeneration of the dentin-pulp complex. 77 Both TGFβ1-containing and acid-treated alginate hydrogels, but not untreated alginate hydrogel, promote dentin matrix secretion and odontoblast-like cell differentiation with subsequent secretion of tubular dentin matrix (Fig. 4).
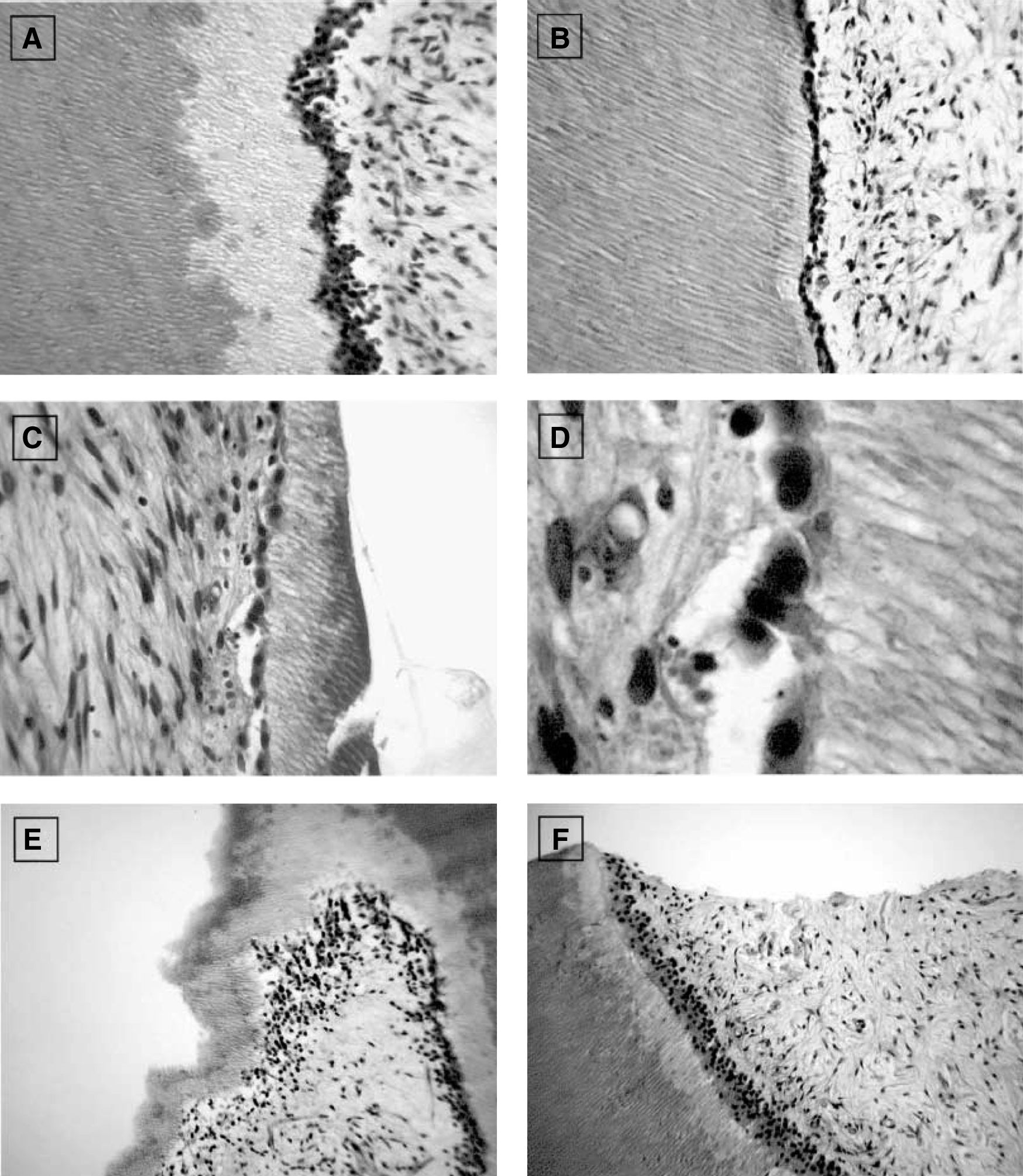
In vitro dentin repair model.
Agarose
Agarose derives from seaweed and forms thermally reversible gels. 36 Agarose has been exploited for drug delivery due to advantages such as easy-gelling, thermo-reversibility, and injectability.78–80 Agarose lacks native ligands in mammalian cells. 81 Incorporation of CDPGYIGSR peptides in agarose allows neurite outgrowth from dorsal root ganglion.82,83 Agarose hydrogels accommodate three-dimensional (3D) neurite extension from primary sensory ganglia in vitro. 82 The rate of neurite extension is inversely correlated to the mechanical stiffness of agarose gels in the range of 0.75%–2.00% (wt/vol) gel concentrations.
Stiff Biomaterials
Mechanically stiff biomaterials can provide mechanical and structural substitutes in tooth regeneration and accommodate cellular functions. Cells are typically seeded and adhere to the porous surface of mechanically stiff scaffolds. In comparison, cells are typically seeded in the aqueous phase of soft biomaterials, followed by polymerization for encapsulation.
Poly(lactide-co-glycolide)
Poly(lactide-co-glycolide) (PLGA) is broadly used in drug delivery due to its general biocompatibiltiy and low toxicity.84,85 However, PLGA can be hydrophobic and may yield acidic degradation products.
86
PLGA micro/nanoparticles are associated with harsh fabrication processes.
86
Accordingly, a variety of thermogelling block copolymers have been synthesized including diblock, triblock, and multiblock. Also, a block copolymer of PLGA and PEG is created as degradable thermo-sensitive hydrogels.
87
PEG-PLGA copolymer hydrogel has a number of advantages including injectability and minimal immune response as a drug delivery carrier with controlled release rate, as well as gene delivery.84,88,89 PLGA-PEG-PLGA triblock copolymer enhances gene transfection efficacy and promotes wound healing.90,91 Figure 5 shows an injectable composite consisting of poly(
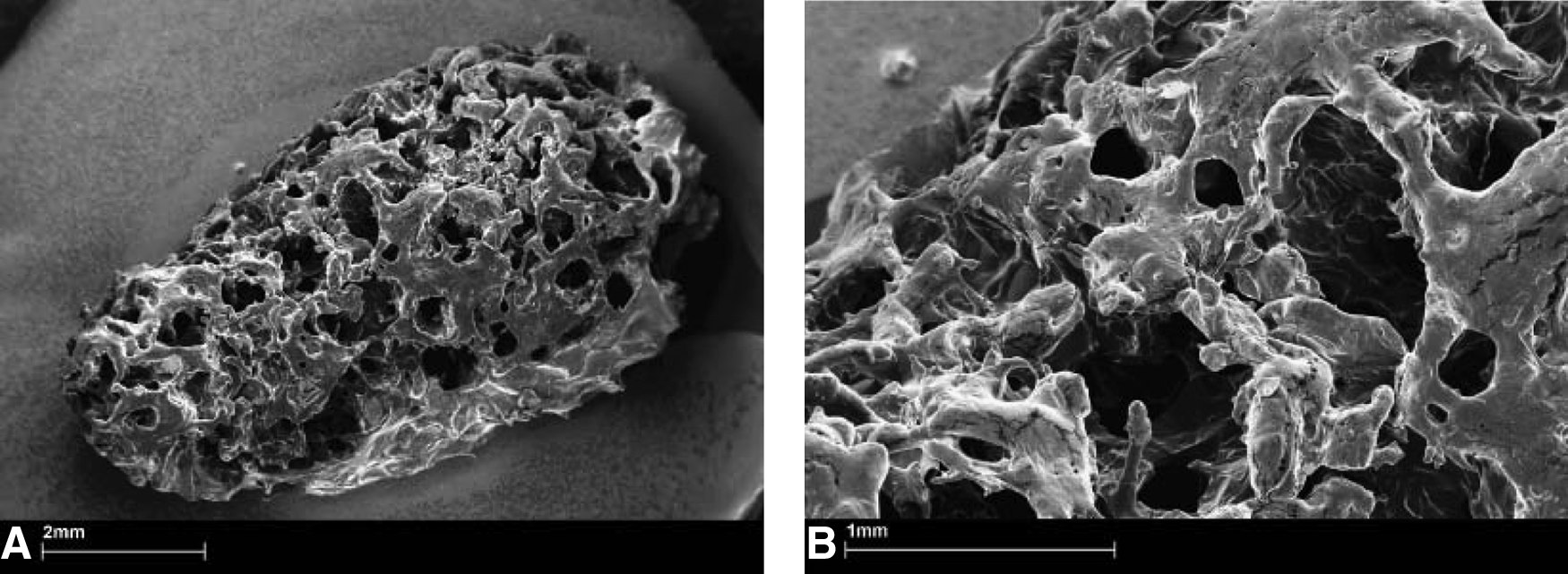
Scanning electron microscopy photomicrographs of the macroporous PLGA composite after a 2-h incubation at 37°C in phosphate-buffered saline and drying. The injectable composite consists of poly(
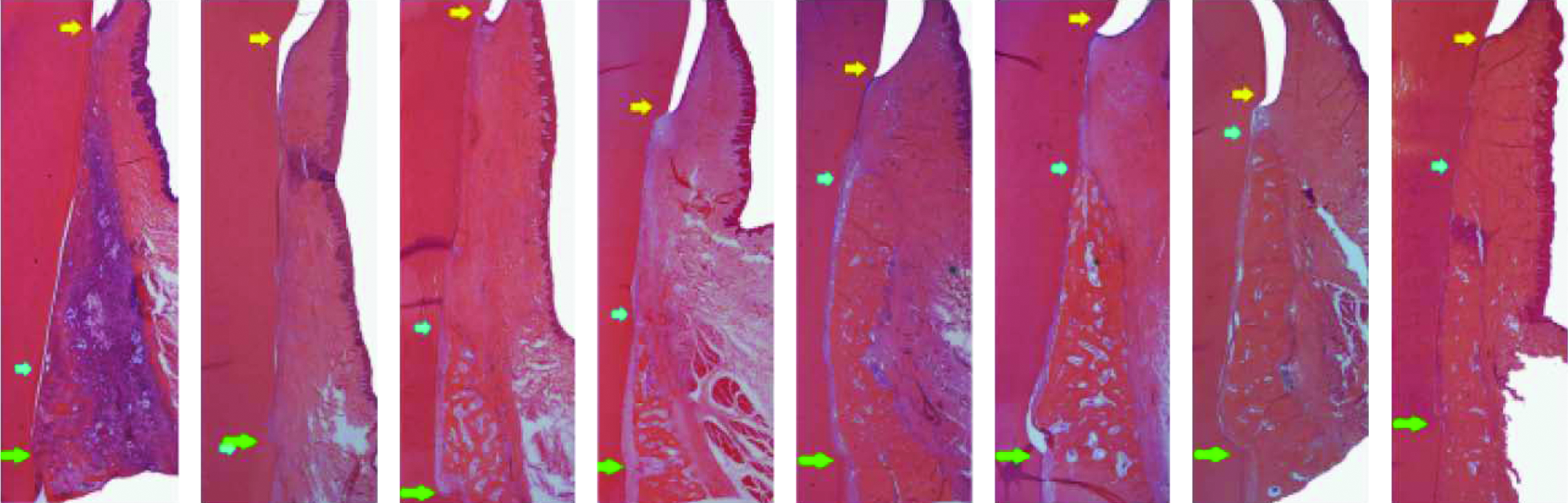
Representative photomicrographs of experimental pre-molar sites implanted with rhGDF-5/PLGA construct or serving as sham-surgery control at 2 (left), 4 (left centre), 6 (right centre), and 8 (right) weeks postsurgery. The left photomicrograph in each pair represents the rhGDF-5/PLGA construct. An inflammatory reaction likely assorted with biodegradation of the rhGDF-5/PLGA construct can be seen at 2 weeks. Generally, there are no other appreciable differences between the premolar site pairs. Green arrows represent the apical extension of the defects, blue arrows represent the coronal extension of newly formed alveolar bone, and the yellow arrows represent the location of the cemento-enamel junction. Color images available online at www.liebertonline.com/teb
Polycaprolactone
Polycaprolactone (PCL) is a versatile synthetic polymer and has been used as a scaffold in tissue engineering.94,95 PCL is approved as a suture material and a drug delivery device by the United States Food and Drug Administration. PCL has limited bioactivity and may be susceptible to bacterial-mediated degradation. 96 Surface properties of PCL can be modified, for example, by coating with hydroxyapatite to promote the adhesion and proliferation of endothelial cells, as hydroxyapatite increases surface wettability and roughness. 97 PCL coated with gelatin and calcium phosphate promotes osteoblast adhesion, spreading, and proliferation. 98 Composite scaffold of PCL and TCP nanoparticles has specific properties such as mechanical properties, wettability, porosity, and biodegradation rate distribution. 99 Moreover, PCL nanofiber scaffold modified with collagen type I and III not only influences cell attachment, migration, and proliferation, but it also provides mechanical integrity for 3D vessel formation in vitro. 100
Hydroxyapatite
Hydroxyapatite has been widely used in bone regeneration, owing to its biocompatibility, immune tolerance, and osteoconductivity. Hydroxyapatite is typically fabricated as a dense material. Porous hydroxyapatite is useful for bone regeneration, because it can be fabricated with 3D architecture similar to the trabecular bone. 101 The performance of the porous hydroxyapatite scaffold is dictated by internal architecture including pore size, porosity, and interconnections. 102 Internal architecture of hydroxyapatite can be created by several approaches including freeze casting, 103 gel casting technique, 104 and polymer sponge method. 105 One of the major drawbacks of hydroxyapatite is its brittleness that limits its applications as a replacement of highly load-bearing bone.
Bioceramics
Bioceramics refers to a group of bioactive glasses and calcium phosphate ceramics. Bioceramics are biocompatible and have been widely used in reconstructive, orthopedic, maxillofacial, and craniofacial applications. Bioceramics can be fabricated via several approaches including phase-mixing, 106 gas foaming, 107 soluble or volatile poragen processing,108,109 template casting, 110 and solid freeform fabrication. 111 Bioceramics can be fabricated with specific internal architecture and surface properties that accommodate cell distribution, adhesion, proliferation, and differentiation due to its porosity.112–114 Bioceramics have been loaded with osteogenic factors such as recombinant human bone morphogenetic protein-2 (rhBMP-2) to induce bone formation. 115 As with other materials such as PCL and HA, increases in porosity and pore size may compromise mechanical stiffness, and vice versa.116–119
In order to evaluate soft and hard tissue reactions to two different hydroxyapatites and compared with bioglass, hydroxyapatite (synthetic hydroxyapatite and natural hydroxyapatite) and bioactive glass are implanted into tooth extraction sockets. 120 The first and third upper and lower premolars, on both sides, are extracted in six female dogs. The extraction sockets are randomly assigned to four groups: Group 1: control (unfilled); Group 2: filled with synthetic hydroxyapatite; Group 3: filled with bovine bone mineral (natural hydroxyapatite); and Group 4: filled with bioactive glass. The animals are euthanized at 4, 8, and 28 weeks after extraction. Most particles of synthetic hydroxyapatite have bone formation on their surface, although some particles show a layer of fibrous connective tissue. The bovine bone mineral group shows particles partially replaced with bone formation. The bioactive glass group shows particles with a thin layer of calcified tissue, suggesting complete resorption (Fig. 7). 120
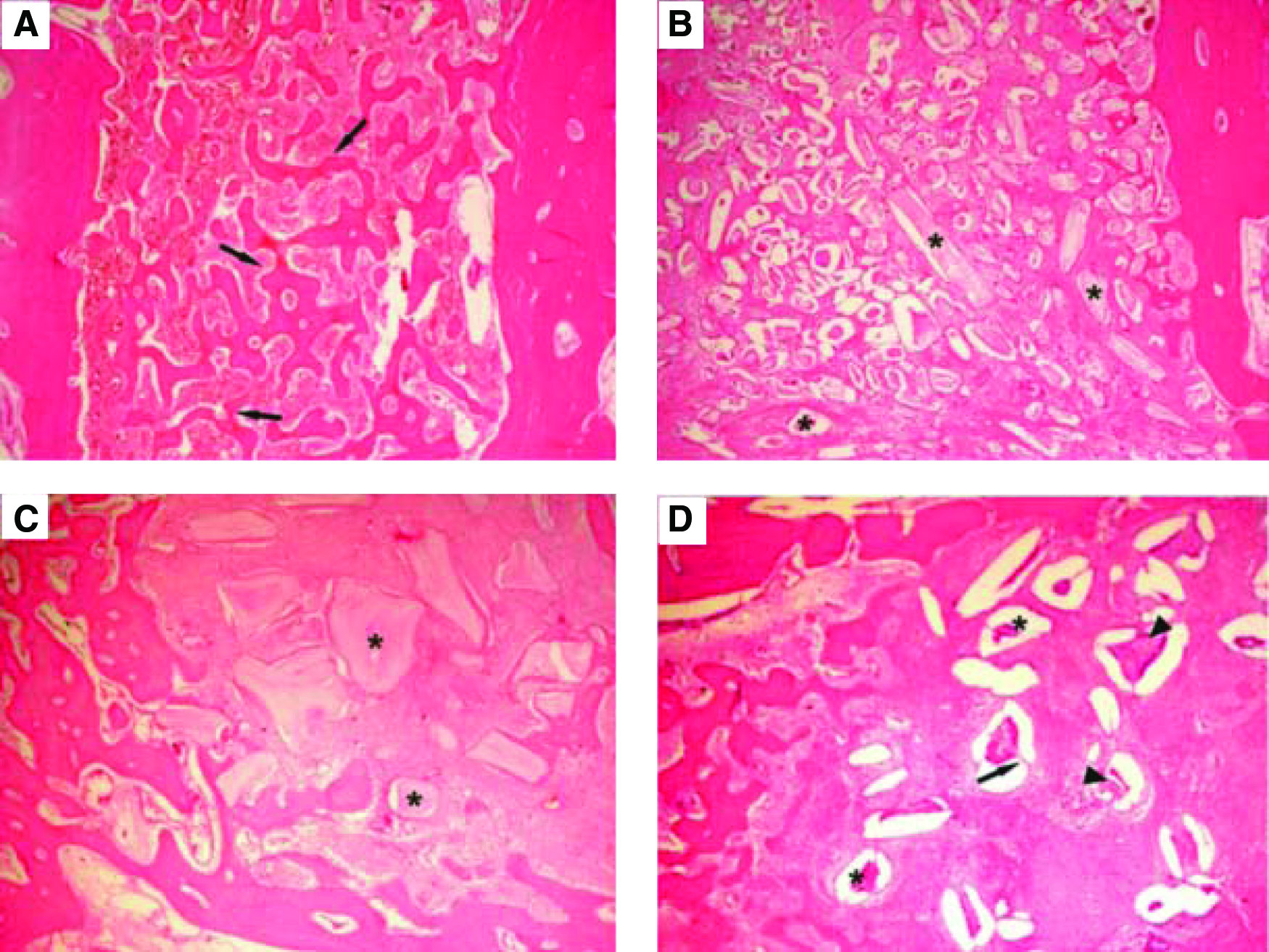
Photomicrographs at 4 weeks:
Tooth Regeneration: Cell Transplantation Versus by Cell Homing
Existing literature on tooth regeneration has taken two distinctive approaches: cell transplantation and cell homing. Cell transplantation has been the predominant approach in tooth regeneration. Disassociated cells of porcine or rat tooth buds in biomaterials yielded putative dentin and enamel organ.121,122 Tooth bud cells and bone marrow osteoprogenitor cells in collagen, PLGA, or silk-protein scaffolds induced putative tooth-like tissues, alveolar bone, and periodontal ligament.123–125 Embryonic oral epithelium and adult mesenchyme together up-regulate odontogenesis genes on mutual induction and yielded dental structures on transplantation into adult renal capsules or jaw bone. 126 Similarly, implantation of E14.5 rat molar rudiments into adult mouse maxilla produced tooth-like structures with surrounding bone.127,128 Multipotent cells of the tooth apical papilla in TCP in swine incisor extraction sockets generated soft and mineralized tissues resembling the periodontal ligament. 129 E14.5 oral epithelium and dental mesenchyme were reconstituted in collagen gels and cultured ex vivo, 130 and when implanted into the maxillary molar extraction sockets in 5-week-old mice, tooth morphogenesis took place and was followed by eruption into occlusion. 131 Several studies have begun to tackle an obligatory task of scale up toward human tooth size.132,133
Tooth regeneration by cell transplantation is a meritorious approach. However, there are hurdles in the translation of cell-delivery-based tooth regeneration into therapeutics. Autologous embryonic tooth germ cells are inaccessible for human applications.128,130,131 Xenogenic embryonic tooth germ cells (from non-human species) may elicit immunorejection and tooth dysmorphogenesis. Autologous postnatal tooth germ cells (e.g., third molars) or autologous dental pulp stem cells are of limited availability. Regardless of cell source, cell delivery for tooth regeneration, similar to cell-based therapies for other tissues, encounters translational barriers. 134 Excessive cost of commercialization and difficulties in regulatory approval have not precluded, to date, any significant clinical translation of tooth regeneration.
The dimensions of the permanent mandibular first molar are fabricated via 3D layer-by-layer apposition.61,135 The composite consists of PCL and hydroxyapatite. A blended cocktail of SDF1 and BMP7 is loaded in collagen gel and infused in scaffold's microchannels. On in vivo implantation, multiple tissues are formed de novo with structures reminiscent of the periodontal ligament and alveolar bone. Mineralized tissues were formed in microchannels of human molar-shaped scaffolds. Quantitatively, significantly more cells are recruited into the microchannels of the human molar scaffolds on combined SDF1 and BMP7 delivery than without growth-factor delivery. 6 Angiogenesis has taken place in microchannels with growth-factor delivery. Combined SDF1 and BMP7 delivery elaborates significantly more blood vessels than without growth-factor delivery. 6 Scaffolds in the shape of the rat mandibular incisor integrated with surrounding tissue, thus showing tissue ingrowth into the scaffolds' microchannels. New bone formation takes place on combined SDF1 and BMP7 delivery that integrates the scaffold and existing alveolar bone (Fig. 8). Angiogenesis takes place in the scaffolds' microchannels with growth-factor delivery. Quantitatively, combined SDF1 and BMP7 delivery elaborates significantly more blood vessels than the growth-factor-free group (Fig. 8). 6

Orthotopic regeneration of tooth-like structures in vivo.
These findings are described in detail in 6 and represent the first report of regeneration of anatomically shaped tooth-like structures in vivo, and by cell homing without cell delivery. The potency of cell homing is substantiated not only by cell recruitment into scaffold's microchannels, but also by regeneration of a putative periodontal ligament and newly formed alveolar bone. 6 Tooth regeneration requires condensation of sufficient cells of multiple lineages.128,136 The observed putative periodontal ligament and newly formed alveolar bone suggest SDF1's and/or BMP7's ability to recruit multiple cell lineages. The SDF1 is chemotactic for bone marrow stem/progenitor cells and endothelial cells, both of which are critical for angiogenesis.137–139 The SDF1 binds to CXCR4, a chemokine receptor for endothelial cells and bone marrow stem/progenitor cells.137,140 Here, SDF1 likely has homed mesenchymal and endothelial stem/progenitor cells in native alveolar bone into porous tooth scaffolds in rat jaw bone, and connective tissue progenitor cells in dorsal subcutaneous tissue into human molar scaffold.141–143 BMP7 plays important roles in osteoblast differentiation and phosphorylation via SMAD pathways, which induces transcription of multiple osteogenic/odontogenic genes.144,145 Here, BMP7 likely is responsible for newly formed, mineralized alveolar bone in rat extraction socket and ectopic mineralization in human tooth scaffold implanted in the dorsum. Our ongoing work has identified additional growth factors that may constitute an optimal conglomerate for tooth regeneration. Cell homing is an under-recognized approach in tissue regeneration, 146 and it offers an alternative to cell-delivery-based tooth regeneration. Omission of cell isolation and ex vivo cell manipulation may accelerate regulatory, commercialization, and clinical processes. The cost for tooth regeneration by cell homing is not anticipated to be nearly as excessive as for cell delivery. In this work, 6 regeneration of a putative periodontal ligament and new bone that integrates with the native alveolar bone appears to provide the ground for a clinically translatable approach. The present work does not preclude parallel studies of tooth regeneration by cell transplantation. Our recent work continues to explore regeneration of multiple tissues by cell delivery.147,148 One of the pivotal issues in tooth regeneration is to devise economically viable approaches that are not cost-prohibitive and can translate into therapies for patients who cannot afford or are counter-indicated for dental implants. Cell-homing-based tooth regeneration may provide a tangible pathway toward clinical translation.
In another study, the effect of scaffolds on in vivo tooth regeneration is evaluated. 149 Collagen and fibrin are selected based on the biocompatibility to dental papilla-derived cells, compared with those of polyglycolic acid (PGA) fiber and β-TCP porous block. Isolated porcine tooth germ-derived cells are seeded and implanted to the back of nude mice. Tooth bud-like structures are observed more frequently in collagen and fibrin gels than in PGA or β-TCP scaffolds, but the amount of hard tissue formation is less (Fig. 9). Thus, collagen and fibrin gel supports the initial regeneration process of tooth buds possibly by promoting functions of epithelial and mesenchymal cells. However, maturation of tooth buds is difficult in fibrin and collagen gels. 149

Graph showing the percentages of epithelial cell area
Biomaterial Selection for Tooth Regeneration
Biomaterials are likely indispensible for tooth regeneration. Soft biomaterials may serve as cell-encapsulating scaffolds, whereas mechanically stiff biomaterials scaffolds may serve as structural substitutes. Soft and mechanically stiff materials may be used together to complement each other's properties. When a kidney is bioengineered to function in humans, it probably does not matter what shape the tissue-engineered kidney is, as long as it functions similarly to a native kidney. However, a tooth should assume anatomic shape and dimensions in order to function in occlusion and in the dentition. The following are the general requirements of biomaterial scaffolds in tooth regeneration:
• Biocompatible, nontoxic, and ideally undergo biologically safe degradation. • Provide encapsulation of cells or surface adhesion for cells that regenerate singular or multiple dental tissues. • Allow functionality of at least some of the multiple cell types including ameloblasts, odontoblasts, cementoblasts, fibroblasts, vascular cells, and/or neural endings. • Either native or synthetic polymers, or a hybrid, are valid choices as scaffolding materials for tooth regeneration, but multiple polymeric layers may be preferred in view of the diversity of tooth organs in structures and functions. • Clinically applicable and offer a turn-key approach for clinicians. It can be readily sterilized, stored in a clinical setting, and has reasonable shelf life.
Tissue engineering was initiated with a concept of functional restoration of tissue or organ defects by the triad of cells, growth factors, and biomaterial scaffolds.150–152 The doctrine of cells, biomaterial scaffolds, and biological signals has been the guiding principle for tissue engineering. However, bioactive scaffolds may include those with embedded bioactive molecules and/or cells. The bioprinting approach as described above can “print” cells and/or molecules in 3D bioscaffolds. 146 Both cell transplantation and cell homing are valid scientific approaches in tooth regeneration. Transplanted cells or delivered biomolecules and/or bioscaffolds can be infused in vivo to create a new environment that promote tooth regeneration. Biomolecules can be chemical compounds, peptides, proteins, or DNA/RNA. What is delivered in vivo is the means, whereas the best possible outcome of tooth regeneration is the end. Importantly, the cost of tooth regeneration therapy cannot be excessive for broad applications. Costly regenerative therapies are unlikely to be clinically viable. High-cost regenerative therapies for a patient with paralysis resulting from spinal cord injuries or stroke are likely justified and clinically applicable. However, expensive regenerative therapies for tooth regeneration, which do not treat life-threatening diseases, are not clinically viable. Costs for dental implant procedures are not modest and not affordable by numerous individuals in developing countries in which tooth loss is widespread. One of the challenges in front of us is to develop regenerative therapies that are less costly than dental implants and yet regenerate tooth components or an entire tooth. Biomaterials offer great potential for reduction in the cost of regenerative tooth therapies.
Footnotes
Acknowledgments
The authors thank F. Guo and K. Hua for technical and administrative assistance. This work was supported by the NIH Grant 5RC2DE020767 from the National Institute of Dental and Craniofacial Research (NIDCR).
Disclosure Statement
No competing financial interests exist.