
Abstract
Loss of skeletal tissue as a consequence of trauma, injury, or disease is a significant cause of morbidity with often wide-ranging socioeconomic impacts. Current approaches to replace or restore significant quantities of lost bone come with substantial limitations and inherent disadvantages that may in themselves cause further disability. In addition, the spontaneous repair capacity of articular cartilage is limited; thus, investigation into new cartilage replacement and regeneration techniques are warranted. Along with the challenges of an increasingly aging demographic, changing clinical scenarios and rising functional expectations provide the imperative for new, more reliable skeletal regeneration strategies. The science of tissue engineering has expanded dramatically in recent years, notably in orthopedic applications, and it is clear that new approaches for de novo skeletal tissue formation offer exciting opportunities to improve the quality of life for many, particularly in the face of increasing patient expectations. However, significant scientific, financial, industrial, and regulatory challenges should be overcome before the successful development of an emergent tissue engineering strategy can be realized. We outline current practice for replacement of lost skeletal tissue and the innovative approaches in tissue regeneration that have so far been translated to clinical use, along with a discussion of the significant hurdles that are presented in the process of translating research strategies to the clinic.
Introduction: Clinical Need and Scale of the Problem
A total of 208,600 primary hip replacements were performed in the United States in 2005, and the demand is expected to grow by 174% to over 570,000 in 2030. 7 Further, the number of revision hip procedures is expected to double over this time. The acetabulum remains the “weak link” in total hip arthroplasty, whether cemented or uncemented, with aseptic loosening and polyethylene wear being the most frequent indications for revision. 8 In addition, knee arthroplasty is now performed more often than hip arthroplasty; thus, the true scale of the problem of inadequate bone stock in revising total knee replacements will only emerge in the coming years in an increasing aging population.
The high incidence of damage to other skeletal tissues is becoming increasingly recognized, with studies noting focal cartilage defects in up to 63% of patients undergoing knee arthroscopy and a fivefold increased risk of patients with such cartilage lesions progressing to osteoarthritis. 9 In addition, over 30 million tendon and ligament injuries occur worldwide each year, and since healing of these tissues occurs by the formation of a fibrotic scar, traditional treatments rarely have satisfactory results. 10 As a consequence, recent clinical attempts have been made to restore cartilage and tendon. These have had to adopt new strategies to overcome additional challenges of reduced local vascularity and the lack of inherent repair mechanisms. 11 The successful transplantation of a composite tissue-engineered airway, which contained stem-cell-derived chondrocytes, provides several potential strategies that may be readily transferred to the field of skeletal regeneration. 12 In particular, techniques of coculturing viable chondrocytes and epithelial cells on either side of a structural matrix could be adapted to skeletal tissue engineering strategies to create composite tissue constructs such as those at the osteochondral, bone-tendon, or bone-ligament junction.
The science of tissue engineering has expanded dramatically in recent years, notably in orthopedic applications, and it is clear that new approaches for de novo skeletal tissue formation offer exciting opportunities to improve the quality of life for many, particularly in the face of increasing patient expectations. 13 We, therefore, outline next current practice for replacement of lost skeletal tissue and the innovative approaches in tissue regeneration that have so far been translated to clinical use, along with a discussion of the significant hurdles that are presented in the process of translating research strategies to the clinic.
Current Reconstructive Strategies and Their Limitations
Procedures to reconstruct bone defects have developed from experience in varied clinical scenarios.14–22 Trauma accounts for many such situations: nonunion may follow any fracture, although the likelihood is increased after major injury with significant bony comminution, devascularization, or frank bone loss. Experience in this field has also been provided by the need to treat surgically induced defects. These may be caused by excision of tumors, debridement of osteomyelitis, osteoarthritis, and inflammatory arthritis, and in the treatment of congenital defects, particularly in maxillofacial surgery. However, only recently has the loss of bone stock around prosthetic implants become an additional factor driving the mandate to develop better reconstructive techniques (Fig. 1).23–25

Anteroposterior and lateral radiographs of a patient's left knee, showing a revision total knee replacement with significant loss of bone stock. Such scenarios are becoming increasingly common in clinical practice.
Reconstructive solutions currently include distraction osteogenesis (DO) and bone grafting using autologous bone, allograft, or synthetic biomaterials. DO was first described by Codivilla in 1905 to allow for gradual lengthening of soft tissues alongside correction of severe bone deformities. 26 Ilizarov refined the technique and apparatus, demonstrating successful healing of established fracture nonunions. 27 Patients are now routinely treated by this osteotomy-distraction technique to regenerate bone lost through surgical debridement, fracture non- and mal-union, congenital deformity, for limb lengthening in dwarfism, and for some skeletal sequelae of poliomyelitis. 16 Ring external fixators stabilize the affected area and are distracted at a rate of about 1 mm per day, generating healing and ossification by microfractures. 28 This technique makes use of bone's inherent regeneration potential, avoiding any requirement for bone graft and allowing large skeletal defects to be healed with some excellent functional outcomes. 29 However, the healing index is just 2–3 months per centimeter of bone lengthened, so patients often require treatment for many months. Further, successful outcomes of DO are dependent on intensive patient education and co-operation, high levels of specialist support, frequent hospital visits, and often multiple procedures including further soft-tissue releases as pins are distracted. Complications are frequent, with pin tract infection in up to 95% of patients as well as cellulitis, osteomyelitis, non- and mal-union, and psychological consequences. 16 In addition, failure to deal with pain from distraction of surrounding soft tissues can affect patient compliance. 30
Autologous bone graft, either vascularized or free, represents the current clinical gold standard for treating bone defects. 31 It provides an osteoconductive three-dimensional scaffold with osteoinductive properties through growth factors and vascularization, while retaining native cells with osteogenic potential. 32 It can be harvested from various sites and implanted during the same operation, and since no new material is introduced, it provokes no immunogenic reaction at the recipient site. However, it is only considered osteogenic if implanted immediately 32 and associated donor site morbidity and pain limit its use to smaller defects. 33 The development of free vascularized bone grafts has facilitated autograft use in larger defects, particularly where structural support is also required, for example, in limb salvage and reconstruction. 34 Autologous vascularized fibula, scapula, iliac crest, and rib transplants have been used to repair major discontinuity defects of over 5 cm, such as those that exist after ablative tumor surgery. 35 The proximal fibula is a particularly good candidate for such interventions, as it functions mainly as an attachment for muscles, and removal leads to minimal donor site morbidity. 36 In a series of 30 patients with surgically induced long-bone segmental defects after tumor resection, treatment with vascularized fibular grafts produced primary union in 23 patients within a mean of 6 months. However, over half of these had complications, and 40% required re-operation for nonunion, graft fracture, or infection. 22 The technique has been refined by placing the fibular autograft within the intramedullary space of a cortical allograft shell to provide initial structural support and promote the biology and regeneration of host bone. However, the technical difficulty and high complication rates of such procedures, and the additional problems inherent in using both autograft and allograft, remain.37,38 For these reasons, allograft alone is generally favored for the treatment of expansive defects despite significant biological, economic, and practical disadvantages to its use. 39
Allograft has been shown to initiate a healing response, inducing cells from surrounding soft tissue to produce new bone at the host-graft interface, which then progresses into the graft material. 32 However, this requires a contiguous vascular supply and adequate mechanical stability to allow vessel in-growth and eventual bone remodeling.40,41 These conditions are often absent, particularly in traumatic defects, where surrounding soft tissue disruption and instability are expected.
Allograft can be milled and impacted to provide a mechanically solid graft, and this has been used in hip arthroplasty surgery for over 30 years as a “void filler” to support the prosthesis in the context of poor bone stock. 42 Relatively small acetabular and femoral defects have been treated with favorable outcomes at 10 and 20 years (99% 23 and 87%, 24 respectively). However, such surgery can be technically demanding and operator dependent. Thus, poorer results are often reported outside specialist centers or in the treatment of larger defects, such as those encountered during revision total hip arthroplasty.43,44
Allograft bone may be obtained from cadavers or from live donors, for example, patients undergoing procedures such as hip replacement surgery, where the femoral head would routinely be removed and discarded. However, given the concerns of potential pathogen transmission, regional “bone banks,” strictly regulated in the United States by the American Association of Tissue Banks, have been introduced to screen and store freeze-dried, fresh-frozen, or irradiated allograft for future use. 45 This system has the advantage of providing a ready supply of screened and quarantined bone; however, the mechanical, biological, and immunological properties of allograft may be affected differently by each storage process. 46 Although it can act as an osteoconductive scaffold, the requirement to process allograft for safe storage and to reduce its immunogenic reactivity removes much of its inherent osteoinductive properties. Nevertheless, despite stringent processing and donor screening, there remains the possibility of carriage of bacteria, viruses, and prions, some of which may not yet have been discovered. Studies have reported bacterial infection rates of 0%–12%, the incidence varying with donor selection criteria, processing technique, and quarantine protocol.46–49 The risk of Human Immunodeficiency Virus transmission from screened donors has been estimated at just 1 in 1.6 million procedures, 50 with no new reported cases since 1985,46,51 although the risk of hepatitis C virus (HCV) transmission is probably much greater. Four cases of HCV infection were attributed to transplanted skeletal tissue harvested from a single antibody-negative donor in 2000. 52
To minimize the risks of infection transmission, the U.S. Food and Drug Administration implemented new Good Tissue Practices legislation in 2005. 45 Such legislations ensure traceability of allograft and provide a framework to co-ordinate recalls of potentially infected allograft. 53 However, these regulations complicate the logistics of acquisition, transport, and storage of allograft, increasing its cost and reducing availability, and as requirements increase, supply will soon be outstripped by demand. 32
Commercial allograft composites (such as Osteocel and Trinity) containing allogeneic skeletal stem cells (SSCs) have recently become available.54,55 They employ a combination of immunodepleted cellular cortical allograft with particulate demineralized bone matrix, which have been cryopreserved to retain cell viability and multipotency, thus demonstrating osteoinduction, osteoconduction, and osteogenesis. 55 Encouraging case series confirm therapeutic utility of these products in maxillofacial reconstruction 55 and revision foot and ankle surgery 56 as an alternative to autogenous bone, although the caveats of using allogeneic material remain.
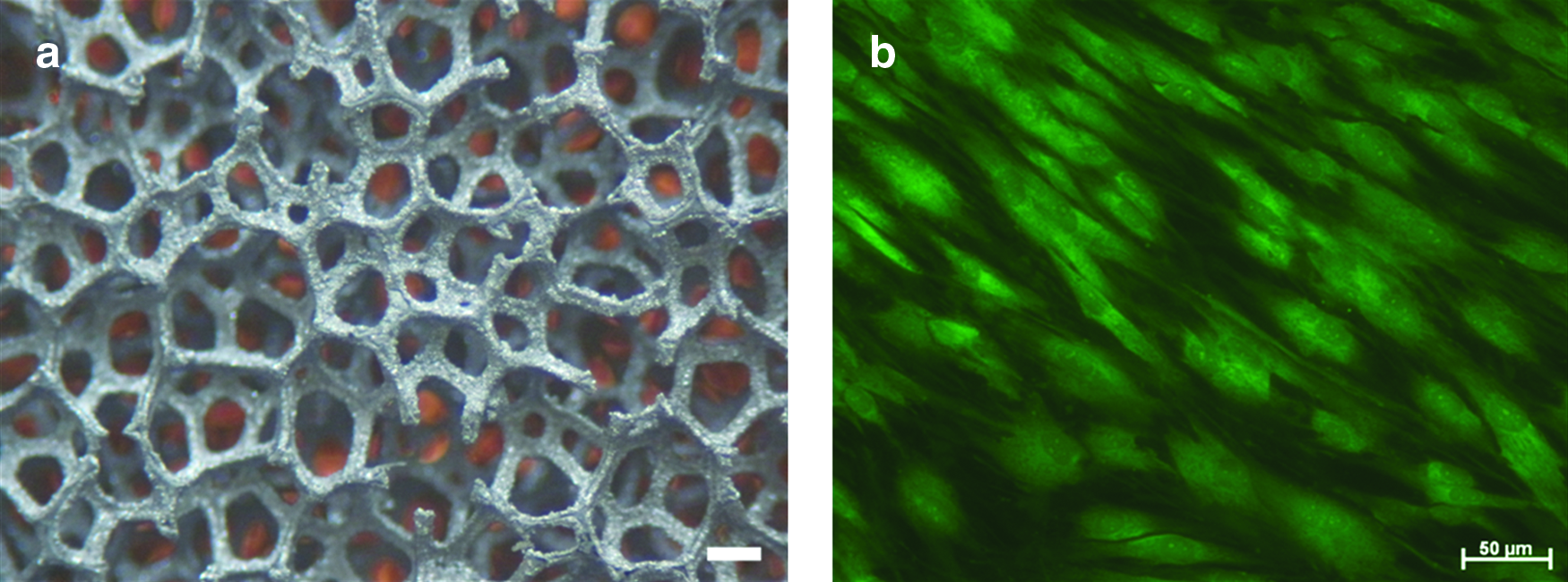
As a consequence of the disadvantages of using autograft and allograft, there has been a significant drive for the development of bioresorbable synthetic scaffold materials that aim at mimicking the beneficial characteristics of biological material while avoiding their drawbacks. Hydrogels and collagen are particularly favored as scaffold materials, because they occur naturally, although other promising candidates include polylactic acid, a synthetic polymer, and the minerals hydroxyapatite (HA) and beta-tricalcium phosphate. 57 These scaffolds can be fabricated to possess desirable osteoconductive properties, and the constituent materials are readily available subject to manufacturing processes. Work is ongoing to improve their structural and osteoinductive properties and to ensure their degradation within the body is safe, predictable, and complete. Interest has also grown in the use of osteoconductive metals, particularly with HA coatings and porous trabecular conformations (Fig. 2a), for the management of lost bone stock. 58 HA-coated implants are used in revision hip surgery 59 and for reconstruction after tumor resection, 60 to reduce the rate of aseptic loosening. The osteoconductive properties of tantalum trabecular metal are already exploited in several orthopedic applications, such as hip and knee arthroplasty, spinal fusion, for the treatment of avascular necrosis, and for reconstruction after skeletal tumor excision. 61 In a recent series to evaluate trabecular tantalum for the management of severe acetabular bone defects in revision hip arthroplasty, mechanical integrity was maintained in all 23 patients at 35 months follow-up. 62 The treatment of femoral head avascular necrosis using trabecular tantalum rods represents a pragmatic alternative to vascularized fibular grafting and has potential advantages of immediate construct stability, expediting safe weight-bearing, and return to function. The procedure can be performed using a minimally invasive technique and without the disadvantage of donor site morbidity; however, in cases where subchondral bone collapse does occur, the implant can become prominent, causing pain and acetabular degeneration. In addition, on eventual removal of the metal implant to allow joint reconstruction, the result is a sizeable defect that ultimately requires further grafting.
Osteoconductive metals possess some important disadvantages that limit their use in skeletal tissue engineering: metals in isolation lack osteoinductive capacity and as such may not be appropriate for use in large unsupported defects. In a goat femoral diaphyseal defect model for example, the use of trabecular tantalum cylinders required the preservation of native periosteum to achieve bony union. 63 This indicates potential limitations in the application of tantalum to reconstruction after trauma, infection, or tumor excision, because periosteum is often deficient in such scenarios. Further, metals are not biodegradable, and removal can cause considerable collateral damage to surrounding bone should subsequent revision be required.
The inherent disadvantages of metal implants, autograft, and allograft, combined with the aging population and a continuing increase in musculoskeletal pathology and patient expectations, highlight a pressing need to augment or replace current strategies with osteoregenerative techniques. However, these strategies will need to act as a functionally and physiologically appropriate surrogate for a patient's lost or damaged skeleton. In addition to the need to reconstruct bone defects, much orthopedic morbidity is derived from cartilage disease and tendon pathology.11,64 It is envisaged that novel technologies to address bone defects will also be readily transferrable to these applications.
Clinical Translation of Novel Therapies
Emerging strategies strive toward the ultimate therapeutic objective: to replace damaged skeletal tissues with appropriate autogenous components that have been harvested without significant morbidity. Research activity has, therefore, been centered on approaches that couple material science with autogenous SSCs as true tissue engineering constructs. SSCs appear particularly suitable as targets for tissue engineering in general, as they are responsible for the unique capacity of normal bone to regenerate without scarring. 65 The relative accessibility of an autologous osteoprogenitor population, which is able to replenish the osteoblasts to form mineralized bone matrix, has resulted in significant translational steps toward clinical application. 66 Research into novel, effective bone regeneration strategies has remained predominantly in the realm of laboratory-based in vitro experimentation and in vivo animal modeling, although more recently a number of research centers have bridged the translational gap from bench to clinic (Table 1).35,40,67–82
The tissue-engineering paradigm has recently been applied to DO to improve the healing index and clinical outcomes, whereby supplementation of the defect with concentrated autologous platelet-rich plasma (PRP) and SSCs from the iliac crest accelerates bone formation. 78 In the study comparing 24 femora and tibiae treated with concentrated PRP and SSCs with 32 control osteotomies (i.e., without additional cell therapy), the healing index dropped from 36.2 to just 27.1 days/cm. The considerable complication rates in DO correlate with the total treatment time; so, reducing the latter will have significant beneficial effects. 83
There is intense interest in augmenting the potential of SSCs by combining them with growth factors and biomimetic scaffolds as a self-contained implantable unit. 84 Several growth factors within bone are expressed during the process of fracture healing, suggesting a role in osteochondral development and in fracture repair. Bone morphogenetic proteins (BMPs), in particular, are critical to the recruitment, commitment, and differentiation of osteoprogenitor cells. Given these osteoinductive properties, BMPs are already in clinical use to enhance bone union, although widespread application has been limited by their high cost. 85 Extracellular matrix proteins have also been demonstrated to encourage osteogenesis.86,87 Type I collagen, precoated onto allograft, has been shown to enhance osteogenic differentiation of SSCs in basal culture, augmenting the mechanical properties of the allograft. 75 The most promising strategy for skeletal tissue regeneration is, therefore, likely to lie in the combination of such growth factors with enriched autologous SSCs added to a suitable synthetic or composite scaffold.
The ideal scaffold would be biocompatible and have structural integrity, yet bioresorbable, thus acting as a temporary framework until new bone is generated. 88 Research behind scaffolds and cell-based tissue engineering has culminated in their application to a number of human cases, summarized in Table 1. After successful ovine trials, 89 autologous bone-marrow stromal cells from three patients were culture-expanded ex vivo and seeded onto HA scaffolds to treat extensive segmental long-bone defects (between 4 and 7 cm). Radiological osseointegration and surrounding callus were observed after just 2 months, with subsequent functional recovery 68 and ongoing clinical success at 6–7 year follow-up. 69 However, the radiographic signs of bone healing presented in this study should be interpreted with caution: the layer of new bone surrounding each of the scaffolds remains limited, even at several years' follow-up, and additional evidence of bone formation and integration within the pores of the scaffold would be required for clinical confidence. The presence of such ossification within the implant is difficult to assess, even from the computed tomography (CT) sections presented, not least because the implanted porous HA scaffold is radio-opaque and nonabsorbable, and no immediate postoperative comparative CT scans are presented. Nevertheless, despite these limitations, these were clearly challenging cases, and it is important to note that the patients reached good clinical outcomes with no subsequent fractures reported to date.
A porous HA scaffold, inoculated with autologous culture-expanded cells derived from periosteum, has also been used to re-create a human distal phalanx after traumatic amputation. 67 Although the resultant construct was limited in function with significant dorsal subluxation and no active range of movement at the interphalangeal joint, the resultant thumb was sufficiently functional for the patient to return to work within 3 months, and the case may be regarded as “proof of concept” to create new bone using, in essence, tissue-engineering principles.
The treatment of benign bone tumors using tissue-engineered implants has also recently been successful. Morishita et al. seeded ex vivo osteogenic culture-expanded SSCs derived from iliac crest aspirates onto a HA scaffold in three patients with benign long-bone tumors (aneurysmal bone cyst of the proximal tibia, giant cell tumor of the proximal tibia, and fibrous dysplasia of the proximal femur). 76 Weight bearing was commenced in all cases within 2–3 weeks with no adverse clinical or radiological sequelae, demonstrating excellent early mechanical strength. The same group successfully applied a tissue-engineering approach to ankle arthroplasty in three patients with osteoarthritis in an attempt to reduce the rate of aseptic loosening associated with these prostheses. 72 They culture-expanded SSCs from iliac crest aspirate in osteogenic conditions, then applied these to the ceramic bone-contacting surfaces of the prosthesis, culturing ex vivo for a further 2 weeks before implanting the construct (Fig. 2b). The authors emphasize several drawbacks of the study, including lack of a control group, a small cohort with short patient follow-up, and the need for an additional procedure to harvest the bone marrow. Nevertheless, this highlights an exciting new technique to enhance the integration at the prosthesis-bone interface.
PRP has received considerable interest in orthopedic approaches to enhance fracture union 78 and spinal fusion,81,90 although the first clinical studies to use PRP in bone reconstruction therapy were in maxillofacial surgery for reconstruction of mandibular and periodontal defects. 91 The effects of PRP are mediated through growth factors that are released from the α-granules of platelets on activation during clotting and are known to contribute to tissue healing. 92 They include vascular endothelial growth factor, transforming growth factor beta (TGF-β), insulin-like growth factor, epidermal growth factor, and platelet-derived growth factor. The combination of PRP with induced autologous SSCs derived from the iliac crest in a 9-year-old girl was successfully applied with a titanium mesh scaffold as an alveolar cleft osteoplasty. 77 A further study to evaluate the combination of autologous SSCs, PRP, and HA as grafting materials for maxillary sinus floor augmentation, or “onlay plasty,” was successful in 20 patients. 82 However, despite some good clinical outcome data, controversy remains over the therapeutic effects of PRP, as the growth factors within it only have a brief duration of action and many of the preclinical studies to date are inconclusive. 92 Further, clinical analyses are generally confined to case studies or small series, and many strategies also involve concurrent osteoprogenitor therapy, thus confounding the attributable cause of any benefit seen. 93
Hernigou et al. used concentrated autologous bone-marrow stromal cells in the treatment of femoral head avascular necrosis. 80 In a large series, the authors demonstrated enduring bone architecture after treatment, particularly in the earlier stages of the disease. In addition, this technique was applied to the treatment of tibial nonunion, achieving sound bone healing in 53 of 60 cases after treatment with concentrated bone-marrow cells. 71 Further, all seven cases that failed to unite were implanted with significantly lower initial SSC concentrations than those cases that united soundly, suggesting a requirement for delivery of a critical concentration of progenitor cells (significantly in excess of 1000 progenitors/mL) to the defect site. This concentration exceeds numbers of stem cells in iliac crest aspirate and emphasizes a requirement for cell-enrichment approaches. 71
Further to this work, there has been significant interest in the addition of osteoprogenitor cells to impaction bone grafting (IBG) constructs (Fig. 3). Recent studies have demonstrated SSC survival after the impaction process and enhancement in the shear strength of the graft 73 (Fig. 4). These findings have been confirmed after clinical translation for the treatment of bone defects. 74 Further studies demonstrate a correlation between cell seeding density and the shear strength of the construct, reaching a significant difference at 2×105 cells/mL, with a 16% increase in shear strength over allograft alone. 75 The IBG technique has been used in the treatment of patients with early femoral head avascular necrosis (Ficat stages 1 and 2) with encouraging clinical results at 3-year follow-up. 94 The procedure involves initial removal of necrotic bone by drilling and curettage from the avascular region, followed by impaction of allograft seeded with concentrated autologous SSCs (Fig. 5). The approach aims at augmenting mechanical support to the overlying cartilage and also improves angiogenesis and new bone formation through enhanced biology.
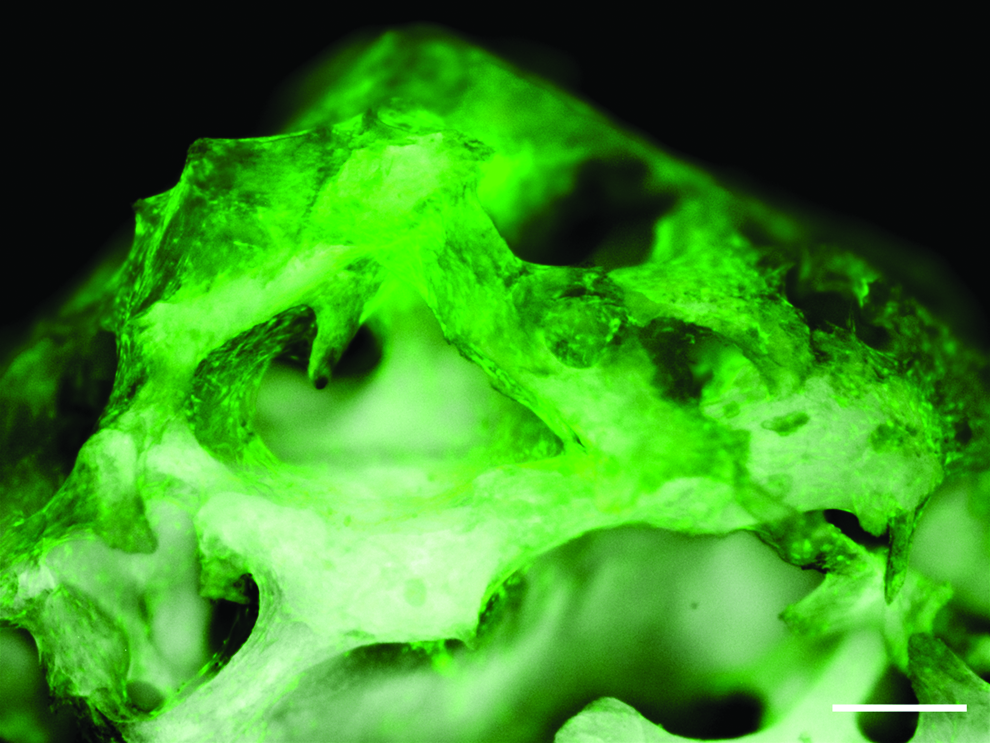
In vitro culture of human bone-marrow stem cells seeded onto allograft, stained with CellTracker™ Green after 7 days culture (scale bar=200 μm). Color images available online at www.liebertonline.com/teb
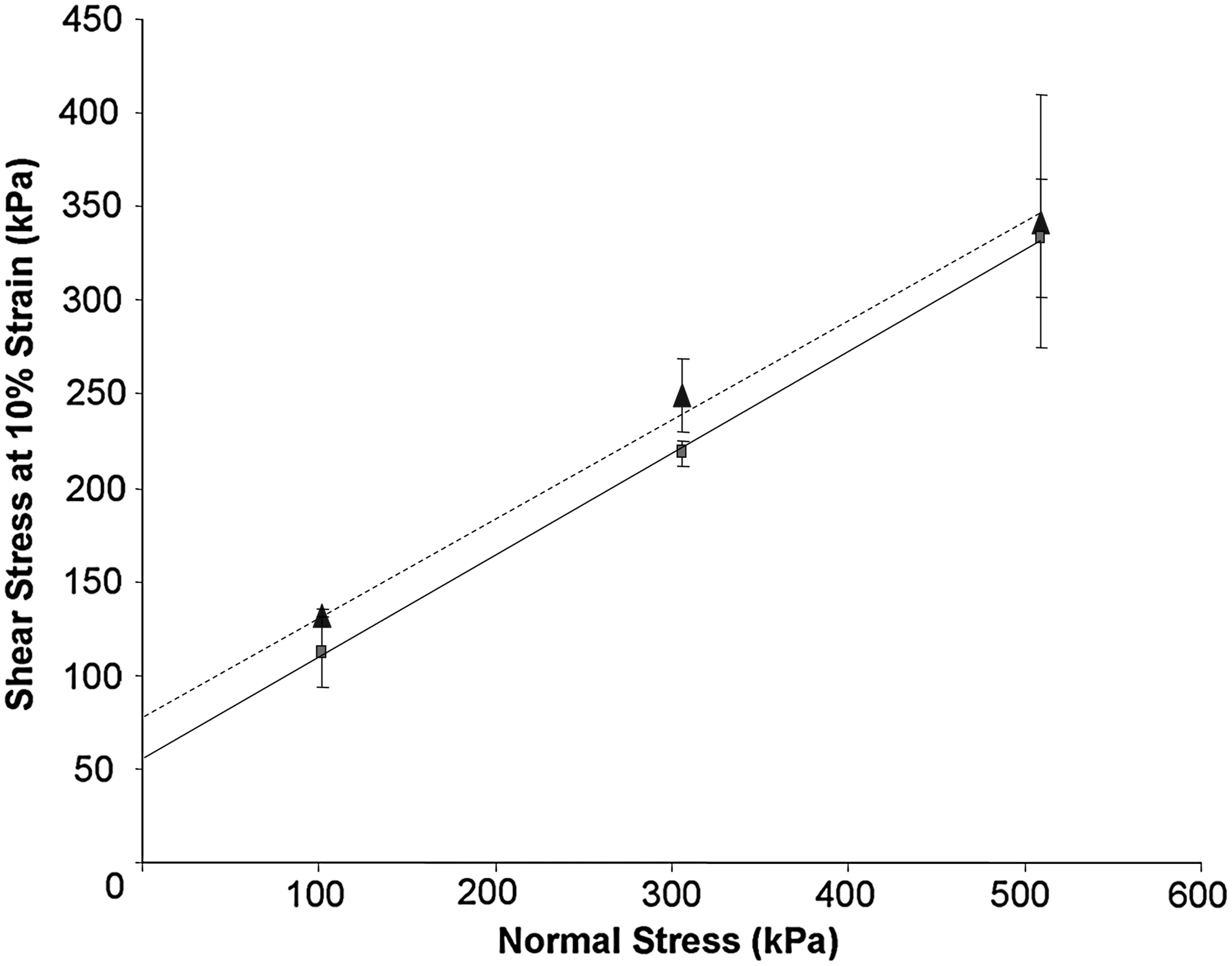
Mohr Coulomb failure graph demonstrating improved shear characteristics of allograft when incubated with skeletal stem cells (broken line) compared with plain allograft (unbroken line) at various levels of stress.
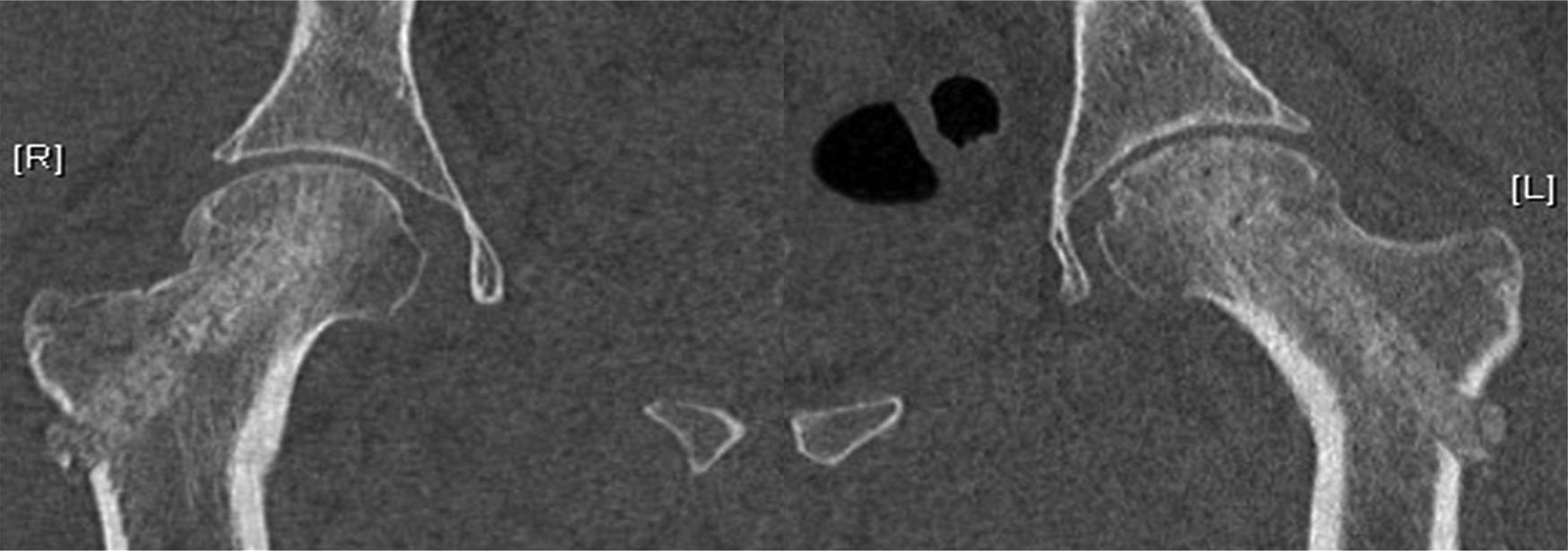
Coronal image of the pelvis and hips from a computed tomography scan. The patient was treated for bilateral femoral head osteonecrosis using an impaction bone-grafting technique with allograft and autogenous concentrated bone-marrow cells. The channels of regenerated bone are seen running diagonally up the femoral neck and into the previously osteonecrotic femoral head on both sides, demonstrating preservation of normal architecture.
Tissue-engineering principles are particularly suited to the field of maxillofacial surgery, given the region's high vascularity and because there is limited intra-oral bone suitable for grafting as an alternative. 95 In cases of deficient maxillary alveolus bone, maxillary sinus floor augmentation is required to ensure stability before dental implant insertion. This clinical necessity has provided further novel strategies for skeletal regeneration with some larger-scale studies. Schimming and Schmelzeisen demonstrated successful maxillary sinus floor augmentation at 3 months in 18 of 27 patients using a polymer fleece with impregnated culture-expanded mandibular periosteal cells. 96 Twelve of these patients underwent a one-stage procedure, and although one patient from this group sustained an early postoperative infection, and the graft was removed, good bone formation was demonstrated in all the other patients from this group. Fifteen patients underwent a two-stage procedure, where the dental prosthesis was implanted 3 months after augmentation. In eight of these patients, the engineered matrix underwent resorption and replacement with connective tissue, and they required supplementary augmentation with autologous bone. One reason cited by the authors for the poorer results in the two-stage procedures is the lack of adequate oxygen and nutrient supply to cells deep within these larger constructs. Current work to improve the induction of vascularization in such constructs will enhance their application to long-bone defects, where the extra-osseous blood supply is often significantly impaired. 97
Other cited examples of maxillofacial tissue-engineering approaches are small in vivo case-based studies; however, they do demonstrate proof of concept and provide a valuable platform from which to progress. In 2004, Warnke et al. used autologous bone-marrow cells seeded onto BMP-7-coated HA blocks to grow a patient's mandible de novo. 35 The construct was supported within a titanium mesh scaffold and grown in the patient's latissimus dorsi muscle before final implantation. Despite complications including infection, heterotopic ossification, and mesh fracture, a second patient has subsequently undergone the same procedure. 70 Transference of this technique to more load-bearing bones in an orthopedic context may prove even more difficult, as the authors provided no direct evidence that a normal mandibular structure or integration with surrounding tissue had been established. 98
In 2006, Heliotis et al. extended this paradigm by demonstrating that BMP-7 with HA induces osteogenesis in extra-skeletal sites, without the requirement for additional bone graft, osteoprogenitor cells, or bone precursor. 99 As a reconstructive strategy for a mandibular defect after resection of squamous cell carcinoma, they placed a HA/BMP-7 implant into a patient's pectoralis major muscle for 3 months. The construct was then raised as a pedicled “myo-osseo-HA” flap and secured to the existing mandibular stump. Unfortunately, despite good initial clinical results, the graft became infected and had to be removed after 5 months. More recently, von Wilmowsky et al. reconstructed mandibular defects in four pigs using autoclaved autogenous mandibular grafts loaded with collagen matrix and autogenous bone-marrow cells harvested from the pigs' tibiae. 100 Additional clinical applications for this technique include bone tumor surgery (the affected bone can be re-introduced after destruction of tumor cells by autoclaving, with a low incidence rate of local tumor recurrence) or after open fractures (as steam sterilization of the bone segment removes microbiological load, but preserves the bone morphology and osteoconductivity).
In addition to bone reconstruction, tissue engineering offers a host of potential solutions for cartilage loss. Osteochondral defects are focal lesions that involve full-thickness loss of cartilage. They have multiple causes, but present most commonly in adults as a consequence of trauma, and in children from either trauma or microvascular pathology such as osteochondritis dissecans.101,102 If symptoms warrant surgical intervention, options currently include arthroscopic debridement, microfracture treatment, mosaicplasty, and cartilage transplants. 103
Microfracture involves the creation of multiple perforations (microfractures) in the subchondral bone in areas that are cartilage deficient. This stimulates a healing response through the release of endogenous factors, but is unfortunately mostly manifested as fibrocartilage, which is mechanically inferior to hyaline cartilage native to synovial joints. Despite improved function and reduced pain in the short and mid term, substantial scope still remains for improvements in the longer term, and tissue engineering offers real potential to effect a cure. 104
A recent equine study has combined the microfracture technique with stem cell technology. 105 Twelve horses had full-thickness cartilage defects created in the lateral femoral trochlea, which were then either treated with microfracture alone or microfracture augmented with a concentrated fraction of bone-marrow aspirate. Subsequent analysis showed improved hyaline cartilage production in the group treated with the additional aspirate both in terms of amount, integration with surrounding native cartilage, and quality (as judged by glycosaminoglycan and type II collagen content). Clinical trials are likely to follow, to confirm the efficacy observed.
Mosaicplasty is an alternative to microfracture, and it is often used for larger defects of up to 2 cm in size. Several circular (4–8 mm) autogenous grafts are harvested from non weight-bearing regions (such as the superolateral trochlea) of the knee, which are then transplanted in a mosaic conformation to fill the osteochondral defect. This has yielded good results, but with the drawback of donor site morbidity. 106 Cartilage transplantation involves a smaller biopsy of a non weight-bearing area of cartilage, so it is less invasive than mosaicplasty and causes less donor-site morbidity. Chondrocytes are then isolated and cultured ex vivo before re-implantation during a subsequent operation either directly into subchondral bone or onto a matrix, which is implanted into the bone (matrix induced autologous chondrocyte implantation). However, these procedures are expensive; they require two operations to the injured joint, and the results are limited in comparison to those of mosaicplasty, both in terms of symptomatic relief and quality of cartilage regeneration. 107
As an alternative to autogenous cartilage transplantation, allogeneic articular cartilage may be obtained from a cadaveric donor, most commonly as an osteochondral allograft. 108 The intact cartilage with underlying subchondral bone can be implanted en bloc into a defect with the advantage of immediate viable cartilage restoration and no donor-site morbidity to the recipient. 109 Given that cartilage is avascular and, thus, relatively immunoprivileged, transmission of viral disease has not been reported after cartilage transplantation alone 50 ; however, the risks of bacterial infection and transmission from the osseous portion of grafts remain, particularly as the use of screened fresh osteochondral grafts is routine to avoid chondrocyte damage by storage and processing techniques. 108 Immunological incompatibility is also an issue, and bone is thoroughly washed with pulsatile lavage before implantation to reduce its antigenic load. 109 Despite these shortcomings, several large trials have reported successful medium-term outcomes of osteochondral allograft transplantation in 72%–88% of patients with corresponding radiological incorporation.108–110 However, this technique is expensive, and the procedure requires significant skill and logistical support. Further, the procedure is dependent on a reliable supply of screened cadaveric material with the inherent risks of disease transmission therein.
Tissue-engineering principles offer good potential alternatives to these procedures, with the combination of autologous SSCs (obtained with minimal donor site morbidity) and novel carrier materials. Clinical trials have shown some success; for example, Haleem et al. used platelet-rich fibrin glue as a scaffold to carry culture-expanded SSCs, which were implanted into five patients with full-thickness cartilage lesions. 111 Beneficial results were observed in all patients, both in terms of symptomatic relief and actual cartilage regeneration, as measured by magnetic resonance imaging and arthroscopically.
A recent rabbit study has taken this concept a stage further, exploiting the potential for the contents and structure of the scaffold itself to manipulate the surrounding environment, hence stimulating and incorporating the host's own local SSCs and removing the need for ex vivo cell culture and scaffold seeding. 112 In the study, the articular surface of the proximal humerus of a group of rabbits was completely excised and replaced with an anatomically correct bioscaffold spatially infused with TGF-β3-adsorbed or TGF-β3-free collagen hydrogel. Four months after surgery, the articular surfaces of TGF-β3-adsorbed bioscaffolds were entirely covered with hyaline cartilage, whereas TGF-β3-free bioscaffolds supported only isolated cartilage growth. Further, there was no difference in shear and compressive characteristics of TGF-β3-mediated articular cartilage, compared with those of native articular cartilage, although these properties were significantly reduced in the group without TGF-β3. In addition, TGF-β3 delivery recruited approximately 130% more cells in the regenerated articular cartilage than in the group without TGF-β3. 112 Clearly, the reconstruction of a complex human joint is still some way off, but this study demonstrated proof of concept for development of novel scaffolds and carrier materials as potential treatments for advanced arthritis.
Initial translational efforts have centered on bone and cartilage reconstruction for several reasons, not least because the differentiation pathways for osteo- and chondrogenesis are almost completely established and can now be modulated. Attention is now turning to the therapeutic manipulation of the bone-marrow stem cell to generate other skeletal cells, such as tenocytes, for clinical use. 113 Although the pathway for tendon/ligament formation has recently been identified, little is currently known about methods to generate these cells in vitro. Neotendon formation has been demonstrated in the rat achilles tendon model using adenoviral modification of SSC differentiation by transfection of the biologically active Smad8 signaling molecule. 114 However, successful translation to heal ligamentous damage or tendon rupture in humans remains a real challenge.
Hurdles to Successful Clinical Translation
Despite some excellent recent advances in the field of tissue engineering and consistent high levels of government research funding, only a small proportion of the successful basic science research currently reaches in vivo analysis with a view to clinical translation. Critically, even fewer strategies are successfully scaled up for commercial manufacture and clinical use. 115 This translational gap often referred to in financial venture capital circles as the “Valley of Death” is highly relevant for the development of regenerative medicine. 116 There is no single cause for this disparity; rather, it is the result of a complex of practical, regulatory, logistical, and financial factors that serve to ensure only the most promising strategies ultimately succeed.
The successful development of an emergent tissue-engineering approach requires a series of tightly co-ordinated processes to take place within a limited timeframe and budget (Fig. 6). The initial concept should hold an accurate insight into the current clinical needs and a realistic vision of future potential. Progression to each subsequent stage in the development process requires close collaboration between multiple agencies with wide-ranging expertise and a high degree of discrimination to select the most promising cell, candidate material, and protocol. Informed allocation of adequate funding is required at each step, particularly after upscaling to preclinical studies, and although this has, to date, been available, there remains a disparity between early-stage funding and final clinical output.115,117 This contrast may reflect the sources of funding: late-stage projects are often funded for a specific product by industry or venture capital companies, where given the associated risk, potential losses can be high—this restricts funding, therefore, to only a few selected therapies or approaches. Economic modeling has been advocated as a solution to determine the likely cost-benefits of a putative tissue engineering construct before product development is considered, allowing stakeholders to assess convincing data on value and clinical efficacy before investing. 118 However, the tissue engineering “life-cycle” remains an exhaustive process, such that even for the successful strategies that progress to sustained production, there is often a significant lead-time to financial return.
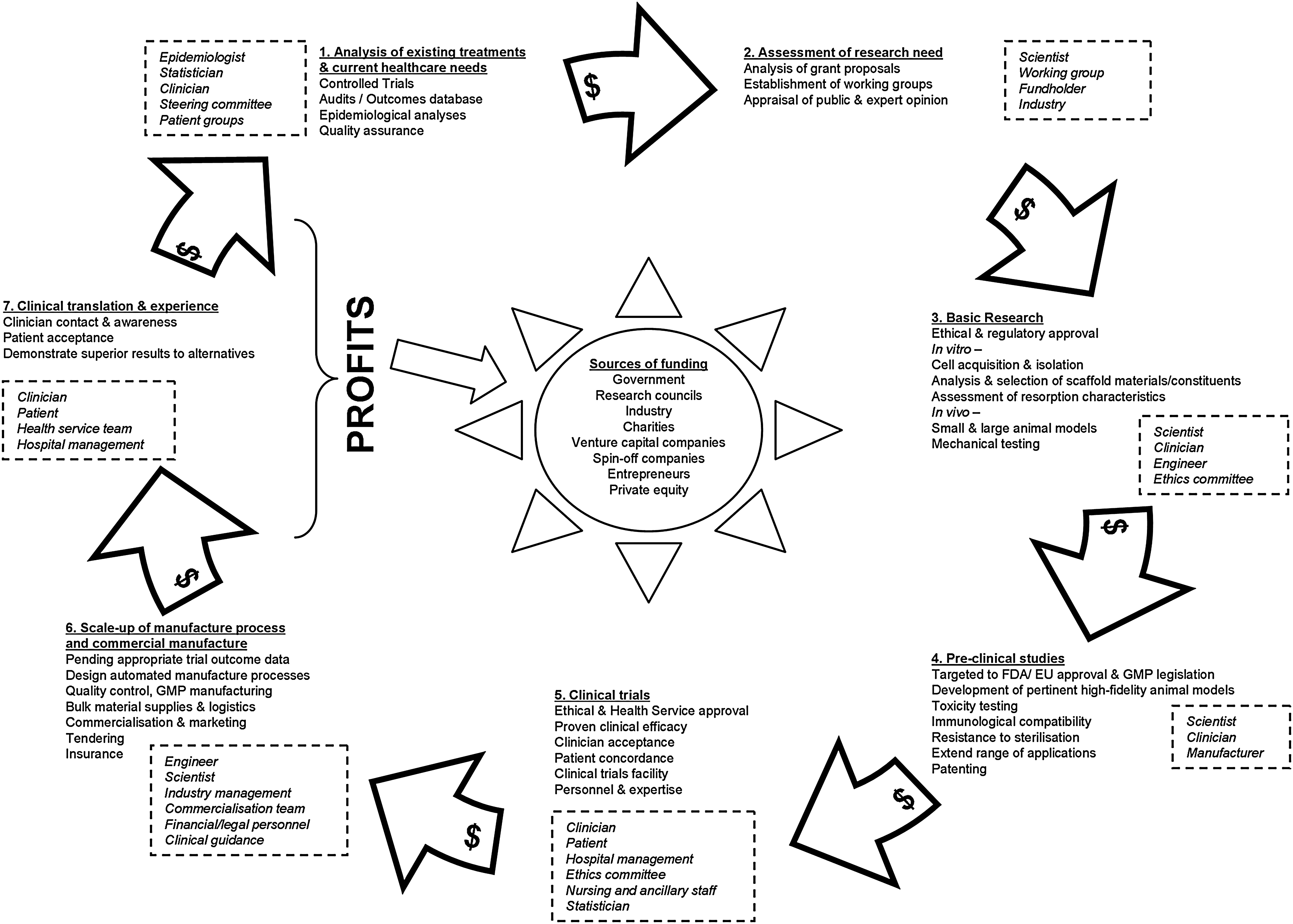
The collaborative tissue engineering “life-cycle.” The process is driven at all stages by informed allocation of funding (denoted by $). The speed of the cycle is not only dependent on the success of the scientific research and testing but also heavily relies on the collaboration of multiple agencies (dashed boxes).
Besides associated difficulties with funding, there are important regulatory hurdles that should be overcome, from in vivo work (including adherence to the principles of replacement, reduction and refinement 119 ) to preclinical and clinical therapeutic evaluation. In addition, the use of human cells in research and the conduct of any clinical trial requires previous scrutiny by the appropriate ethics committee, and before any biomaterial is used in the clinic, it should comply with stringent production and safety standards such as International Organization for Standardization, U.S. Food and Drug Administration, and Good Manufacturing Practice. 120
Practical obstacles to in vivo scale-up should also be addressed to reliably assess new strategies for skeletal tissue engineering before preclinical studies can take place. Challenges include the establishment of appropriate large animal models for the clinical scenarios to be modeled, the requirement to manufacture larger biomaterials, and the need to culture cells on a much greater scale than is routine in most research laboratories. 121 Although the bone composition of the dog, sheep, goat, and pig is similar to those of humans, the age and rate at which osteonal remodeling occurs varies between these groups. In addition, cost, local availability, temperament, and husbandry expertise are important factors. 122 For bone regeneration models, sheep and goats are particularly relevant, as their bodyweight is comparable to humans and the dimensions of their long bones allow for the use of human implants and fixation techniques.120,123 The equine knee is often the favored model for cartilage repair strategies, because it has thick hyaline cartilage that allows investigation of both partial and full-thickness defects. 124 Further, horses have large joints that permit arthroscopy, and they are more compliant with postoperative rehabilitation protocols compared with pigs and ruminants. 125
Once efficacy has been demonstrated in a large animal model and preclinical safety approval has been granted, the successful product can then undergo clinical trials before commercial manufacture. Clinical trials present further challenges including a requirement for significant clinician involvement, patient concordance, organization, and appropriate clinical facilities to undertake such studies. Further, the technicalities of large-scale manufacture should not be (but often are) neglected until a late stage in product development, when modification of manufacturing processes may be costly or require regulatory re-approval.
The difficulties associated with mass production of complex biocomposites or cell production processes may be overcome by incorporating commercial interests and production strategies in the initial research and development. This would provide a platform for progression in parallel with translation. 118
Summary
Current strategies for the treatment of lost bone stock have inherent disadvantages and in view of ever increasing demand, there is a pressing need for novel treatment modalities. The approaches outlined in this article provide a snapshot of future potential, but the scarcity of these cases in the literature and the absence of reliable controls prohibit the routine clinical use of many of these strategies until large-scale clinical trials have been performed. However, the application of these novel techniques has afforded the opportunity to push the boundaries of tissue-engineering strategies in clinical practice, where current treatment strategies are insufficient.
The therapeutic panacea would be the integration of a custom-sized immunomodulated package containing an absorbable synthetic scaffold and impregnated with sustained-release growth factors, with viable autogenous skeletal cells (in the first instance, followed by allogeneic skeletal populations) that have been stimulated to commit to appropriate differentiation pathways. This would have to be presented within a sustained environment that provides adequate nutrition and oxygenation and removes metabolic waste products. The development of such a construct clearly requires close co-ordination within a multidisciplinary framework, involving cell scientists, biomedical engineers, mathematicians, clinicians, and patients. 84 In addition, development and manufacture will require continued financial input, which may become harder to secure in the current fiscal climate until greater numbers of translated therapies reach the market. Thus, efforts should be made to ensure research developments are closely allied at an early stage to the processes involved in large-scale manufacture for clinical use. These include ethical and regulatory approval, good manufacturing practices, logistical planning, appropriate marketing, and financial commitment.
In the intervening years, it will be necessary to clarify and demonstrate the continuum of skeletal cell development and differentiation, as well as the interplay between cells, their local environment, and growth factors that govern their fate. Ultimately, the true gauge of clinical success will lie in the relevance of these strategies in vivo for an increasing aging population.
Footnotes
Acknowledgments
This work was funded by Biotechnology and Biological Sciences Research Council (BB/GO10579, G006971), Technology Strategy Board and Engineering, and Physical Sciences Research Council (TS/G001650/1)
Disclosure Statement
No competing financial interests exist