
Abstract
Currently, surgical treatments for peripheral nerve injury are less than satisfactory. The gold standard of treatment for peripheral nerve gaps >5 mm is the autologous nerve graft; however, this treatment is associated with a variety of clinical complications, such as donor site morbidity, limited availability, nerve site mismatch, and the formation of neuromas. Despite many recent advances in the field, clinical studies implementing the use of artificial nerve guides have yielded results that are yet to surpass those of autografts. Thus, the development of a nerve guidance conduit, which could match the effectiveness of the autologous nerve graft, would be beneficial to the field of peripheral nerve surgery. Design strategies to improve surgical outcomes have included the development of biopolymers and synthetic polymers as primary scaffolds with tailored mechanical and physical properties, luminal “fillers” such as laminin and fibronectin as secondary internal scaffolds, surface micropatterning, stem cell inclusion, and controlled release of neurotrophic factors. The current article highlights approaches to peripheral nerve repair through a channel or conduit, implementing chemical and physical growth and guidance cues to direct that repair process.
Introduction
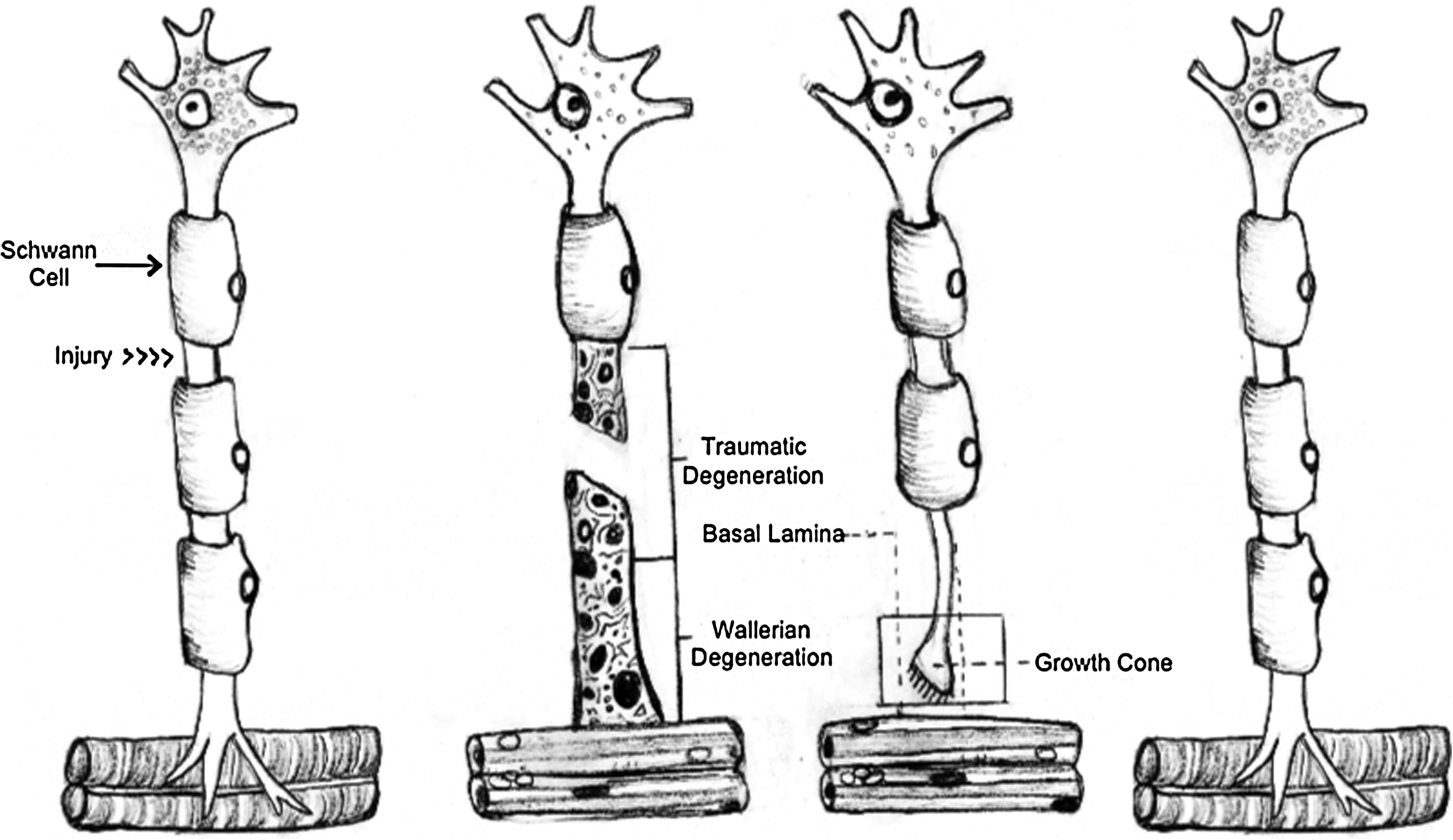
Natural regenerative processes in the mammalian peripheral nervous system. After axotomy, traumatic degeneration occurs in the proximal nerve segment (usually up to the closest proximal node of Ranvier) and the immediate distal portion of the nerve, and the connected muscle atrophies. Within 2–4 days of axotomy, Wallerian degeneration occurs in the distal segment of the axon and lasts for 1–2 weeks. During this process, myelin clearance is performed by infiltrating macrophages and Schwann cells. Proliferating Schwann cells then begin to form bands of Büngner within the nerve basal lamina. Ultimately, the regenerating fibers track along these bands and migrate toward their original motor output. Within 2 weeks of the initiation of regeneration, the process of remyelination begins (as in development), by having Schwann cells wrapped around the regenerating axons. Once the axons reach their appropriate target site of innervation, axon diameter increases up to the original dimensions. Figure adapted from Bahr and Bonhoeffer 2 and Seckel 3 .
Current nerve guides
The first generation of artificial nerve conduits used in the clinic were nonresorbable silicone tubes, which were plagued by compression syndrome and often required secondary surgeries for removal. 13 Since then, there have been a variety of different biomaterials approved for clinical use, such as type I collagen, polyglycolic acid (PGA), poly-DL-lactide-co-caprolactone (PLCL), and polyvinyl alcohol (PVA). There currently are five FDA-approved nerve conduits, four of which—Neurotube (PGA), Neurolac (PLCL), NeuraGen (type I collagen), and NeuroMatrixNeuroflex (type I collagen)—are bioresorbable (with degradation rates on the order of 3 months to 4 years), and one that is nonresorbable—SaluBridge (PVA hydrogel). 14 Only clinical studies for NeuraGen, Neurotube, and Neurolac have results published in peer-reviewed journals.
Each of these conduits has yielded some variable clinical data. The Neurolac conduit initially showed some promising results, performing comparably with the positive control, with regard to sensory recovery; however, more recent data have accumulated (in clinical and animal studies), raising issues of biocompatibility, swelling, degradation rate, and automutilation.15,16 Rigidity and patient complications were also issues reported, leading one surgeon to discontinue clinical use of the Neurolac conduits. 17 The NeuraGen conduit has reported excellent clinical success for the surgical repair of brachial plexus birth injuries 18 ; however, recently, in a rat sciatic nerve model, processed nerve allografts (comparable to AxoGen's Avance allograft) performed significantly better than the NeuraGen conduit in critically sized defects. 19 For the Neurotube, a positive trend in clinical data for short gaps has been obtained. For digital nerve defects less than or equal to 3 cm, the conduit offered a higher percentage of patients with “excellent recovery,” though the data were not statistically significant. 20 More recent case studies reported positive results with sufficient recovery of sensorimotor function after median nerve reconstruction and with regeneration of cranial motor nerves.21,22
Processed (decellularized) allografts are another effective technique that has been clinically adopted for peripheral nerve regeneration applications. Decellularized nerve allografts carry the benefit of preserving the basal lamina/extracellular matrix (ECM) of the nerve, potentially leading to mechanical guidance of regenerating axons. The AxoGen Avance decellularized allograft, which uses a proprietary decllularization protocol involving detergents and chondroitinases, has been used in the clinic for repair of facial nerve defects, 23 and successful results were observed for hand nerve defects up to 3 cm in length. 24 Nerve allografts can also be decellularized by using simpler detergent-processing and cold-preserving methods. Although decellularized nerve allografts may provide another potential technology to bridge critically sized defects, no large-scale clinical studies testing their efficacy have been published to date. However, a recent study comparing different acellular allografts in a 14 mm rat sciatic nerve defect found superior performance in detergent-treated allografts, as compared with AxoGen-treated and cold-preserved allografts. 25
None of the approved conduits just mentioned nor any currently in clinical use have incorporated adhesive ECM protein or neurotrophic factors. Additionally, the degradation profiles of these conduits, with the exception of the polylactic acid (PLA)-poly(caprolactone) (PCL) conduit, cannot be tailored to the regeneration rate of different peripheral nerves. Further, swelling and biocompatibility issues have plagued the clinically available conduits. It appears that the most successful material implanted in humans, however, has been PGA (the synthetic polymer used in Neurotube). A compilation of nine studies ranging from 1990 to 2005 has yielded positive results (75% of patients presented with “good” or “very good” recovery). 14 Of the clinically available materials, PGA has the most rapid degradation rate (3 months for Neurotube). The current generation of conduits provides mainly physical guidance cues via conduit morphology to help direct damaged nerve to its target sensory and motor outputs. The next generation of conduits will seek to augment nervous system function by using topographical and protein cues that interact with nervous tissue at the cellular level. Additionally, these cues should be tailored to the nerve and function of interest.
Tissue engineering offers clinical potential for peripheral nerve repair, through the development of biocompatible, anisotropic NGCs. The next generation of clinically used artificial conduits should be able to incorporate the use of neurotrophic factors, ECM proteins, surface micropatterning, and favorable physical and mechanical properties. Incorporation of cells into conduits will likely be a part of the third generation of clinically available conduits, and this is discussed elsewhere. 26 The current article highlights current progress in tissue engineering research for the development of a comprehensive nerve conduit.
Current Materials
A wide variety of biomaterials are being used to promote functional recovery of injured nerves. Although autologous nerve grafts remain the gold standard, many material options are emerging. From biopolymers and synthetic polymers to blends, there are numerous options to capitalize on different properties of each material, such as mechanical strength, biocompatibility, degradation profile, and the ability to encapsulate different growth factors and proteins. The next section offers a selection of those materials currently available and being used for in vivo studies, which have clinical potential. This section is divided threefold: autologous tissues, primarily protein- and polysaccharide-based biopolymers, and synthetic polymers, the most common of which are displayed in Table 2a and b.
Recovery according to Sakellarides scale. 50
PGA, polyglycolic acid; PLCL, poly-DL-lactide-co-caprolactone.
GDNF, glial cell line-derived neurotrophic factor; NGF, nerve growth factor; PCL, poly(caprolactone); PHB, polyhydroxybutyrate; PLGA, poly(lactic-co-glycolic) acid.
Autologous tissues
The autologous nerve graft remains the gold standard in the field of peripheral nerve surgery. This is mostly a product of its structural and biological composition, which is closely matched to the nerve being repaired. 51 In the past due to lack of availability of autologous nervous tissue, surgeons have relied on other tissues. A common biological matrix used has been the vein autograft, which has yielded mixed results.27,32,52,53 The autogenous vein grafts are equally as effective as NGCs for nerve defects ≤3 cm, when applied to nonessential sensory nerves; however, the use of the graft for defects >3 cm has yielded poor outcomes. 31 Additionally, the vein constructs lack the physical robustness required for excellent clinical outcomes, as they are known to kink and collapse on themselves. 54
An alternative solution proposed to maintain the structural integrity of the vein graft and to provide a basement membrane for axonal outgrowth is to introduce a muscle graft filler. Early studies have shown that both the presence and alignment of the muscle basal lamina have a significant impact on peripheral nerve repair.55,56 The muscle grafts most likely serve two positive roles in peripheral nerve repair: (1) the anisotropic distribution of muscle fibers, coaxially aligned with the regenerating nerve, allowing for proper target innervation, and (2) the basement membrane of the muscle tissue offers adhesive, ECM proteins for the regenerating axons. A recent clinical investigation evaluating the impact of muscle-filled vein grafts with regard to nerve defects on the order of 0.5–6 cm yielded positive results in 85% of cases 28 ; however, the majority of these positive results came from sensory nerves with defects of 2 cm or less. The treatments for mixed nerves (containing both efferent and afferent projections) yielded a lower proportion of “good” and “very good” outcomes (“very good” being the best possible outcome) as compared with the sensory nerve group. Other findings in the literature27,57 have also reported that the best outcomes with venous and muscle-vein grafts are in the cases of shorter sensory nerve defects with mixed nerves yielding mixed results.
Biopolymers
Biopolymers are a source of biocompatible polymers, which often have tailored mechanical properties and degradation profiles engineered to be complementary to those of the regenerating nerve. Additionally, biopolymers have the potential to encapsulate and present growth factors and ECM proteins to the proximal nerve cable. Some biopolymers, such as keratin, have recurring integrin-binding domains (the RGD motif), which have yielded positive results in a short mouse defect model. 40 As previously mentioned, there are currently two FDA-approved biopolymer conduits (composed of type I collagen), and, hopefully, many of the following materials will add to clinical options in the next few years.
Recent studies have assessed nerve conduit efficacy in different models, with gaps generally spanning from 4 mm up to 30+ mm. In intermediate gaps (∼10–13 mm), fibrin and silk have been used with some degree of success. In one study using silk, the physical and functional recovery was close to that of nerve autografts. 42 The fibrin study did not assess electrophysiological properties of the regenerated nerve, but successful outcomes were reported based on histology when compared with the gold standard. With regard to critically sized defects, in the order of 20 mm in rodent and rabbit species, and ∼30 mm in larger animals such as dogs, biopolymer conduits have required internal fillers composed of either growth factor gradients or aligned mats/filaments. In one study, laminin-1 and nerve growth factor (NGF)-coupled gradients in agarose were used and led to significant axonal regeneration through a 20 mm gap in rats. 35 Other studies, using chitosan and collagen (with internal aligned filaments), were able to bridge 30 mm gaps in dogs, with functional recovery and at least partial physical repair and continuity of the nerve cable.36,37
Synthetic materials
Synthetic polymers, though often less biocompatible relative to biopolymers, offer opportunities for tailored degradation, and control of mechanical strength, porosity, and microstructure properties. Common chemical modifications of these polymers include the addition of adhesive proteins and growth factors. One strategy is the controlled release of neurotrophic factors by embedding microspheres into the conduit wall. A study using PCL conduits with embedded glial cell line-derived neurotrophic factor (GDNF)-eluting microspheres (made of a poly(lactic-co-glycolic) acid [PLGA]/poly-
Despite the many advantages of using synthetic materials, some of these materials can also elicit inflammatory responses. To reduce inflammatory responses, one strategy has been to combine or “blend” synthetic materials with other more biocompatible materials. A recent study used a chitosan-PLA blend, thus taking advantage of the natural biocompatibility of chitosan and the mechanical properties of PLA. 60 A polyurethane-collagen bilayer was also used to present a soft inner substrate and a harder shell, which maintained the conduit's structural integrity during regeneration; this design also enabled the diffusion of nutrients, while limiting fibrous tissue infiltration based on internal and external pore distribution. Asymmetric porosity is an excellent strategy for maximizing nutrient diffusion and minimizing scar tissue infiltration. This technique is most easily accomplished with synthetic materials, as demonstrated in numerous studies using a PLGA/poloxamer blend, which yielded internal nanosize pores and external microsize pores. This conduit outperformed silicone and plain PLGA in a 10 mm rat sciatic defect model. 48 A follow-up study was able to improve on these results by adding ultrasound stimulation to the wound site. 61 Additionally, PLGA has been shown to perform on par with the clinically approved Neurolac conduit in a 10 mm rat sciatic nerve defect. 62
Biomaterials that have exhibited positive qualities include biopolymers such as chitosan, collagen, synthetic polymers PCL, PGA, and polylactides (in blends). Collagen, PGA, and a specific polylactide/PCL blend are clinically available as NGCs. Chitosan is biocompatible and has been extensively studied in vivo, with different synthetic polymer blends, successfully bridging critical defects.63,64 There exist numerous strategies for selection of materials to generate a successful nerve conduit. Primary conduit requirements are biocompatibility, biodegradability, and porosity. It is also common to maximize mechanical properties and surface chemistries for cellular adhesion, tailored degradation, and directionality in neurite outgrowth. The next section will discuss how these parameters are generally selected and assessed with regard to the contribution of each modification to the comprehensive nerve conduit.
Materials Considerations
As previously mentioned, materials choice is essential for a successful nerve guide. The primary considerations required are mechanical/physical properties and surface chemistry/morphology. The proper mechanical and physical properties will generate a conduit that has a degree of similarity to native nervous tissue in terms of degradation profile, tensile modulus, and size. Careful selection of surface modifications is also essential in assuring (1) cellular adhesion, viability, and compatibility, and (2) directed tissue growth, which will be discussed in greater detail later. The next section briefly outlines primary considerations in conduit design, after the selection of a given material.
Mechanical/physical properties
For optimal nerve regeneration, a comprehensive conduit should match the mechanical and physical properties of native nerve, while maintaining biocompatibility. Factors to be considered in the mechanical design of nerve conduits are tensile strength, suturability, physical fit, degradation profile, and swelling due to degradation/fluid absorption. One popular strategy has been the use of synthetic/biopolymer blends as described earlier to take advantage of a given material's advantageous mechanical properties and excellent biocompatibility, respectively.
Stress–strain properties play an important role in materials choice. Unfortunately, many regenerating nerve cables are simply overmatched by synthetic polymers and biopolymers. For example, PLLA has a tensile strength reported in the range of 64.3–69.8 MPa, whereas a peripheral nerve in situ has a tensile strength of only ∼11.7 MPa.65,66 To approach the appropriate mechanical properties, one strategy has been to form polymer composites with biopolymers such as chitosan, 60 which have been established as “softer” and biocompatible. Many other strategies exist to obtain a reasonable compromise between biocompatibility and mechanical properties with a balance between the two design criteria required. It is worth noting that the role of mechanical compliance in directing cell fate and function has emerged as a critical issue in materials design.67–69 However, the impact of such factors on nerve cell regeneration has been less studied to date. Additionally, the conduit should be physically robust enough to accommodate the incorporation of sutures to tether to proximal and distal nerve segments.
Another physical property considered in conduit design is the rate of degradation. Degradation profiles of the conduits should accommodate the rate of nerve regeneration; the conduit should be fully resorbed by the body at the time of complete physical nerve repair. For a 10 mm nerve gap, the axonal phase occurs around the third week of regeneration (after the fluid, matrix, and cellular phases). 4 After this, axonal growth proceeds at a growth rate of ∼1 mm/day. 70 Thus, the conduit would ideally be significantly degrading after the axonal phase. This would mitigate entrapment-like symptoms and abolish the need for secondary surgeries for removal of the conduit, which are often required of the nonbiodegradable conduits discussed in the introduction.
Success with nerve regeneration outcomes is also correlated with how well the conduit physically fits around the nerve. Past research has shown that there exists a close relationship between the formation of neuromas in regenerated tissues and the thickness of the conduit tube wall; with reduced wall-thickness, this issue was alleviated. 71 Recently, tube wall thicknesses greater than 0.81 mm significantly attenuated axon growth. 72 The wall-thickness problem is most likely an issue of nutrient diffusion and wall porosity, which were also shown to play important roles in axonal regeneration. Recently, Kokai et al. demonstrated that a wall thickness of 0.6 mm, a porosity of 80%, and a pore size range of ∼10–40 μm are optimal for peripheral nerve repair. 73 Conduit “fit” is also a dynamic process, and swelling may be detrimental to recovery. In conclusion, it is essential to choose a material that will avoid swelling and not elicit an inflammatory response during degradation. Such a conduit will be able to encourage appropriate nerve cable repair, given the proper presentation of neurotrophic cues discussed next.
Surface chemistry, morphology, and modifications
Earlier studies investigating neurite outgrowth and adhesion involved micropatterned laminin- and fibronectin-coated substrata and their effect on sensory neurons from chick dorsal root ganglia. 74 Laminin is a protein commonly used for surface modification for nerve regeneration due to its positive influence on neurite outgrowth and growth cone chemotaxis.75,76 The role of laminin in neural development is understood. Neurite outgrowth has also been augmented through the use of electrically conducting polymers. In one study, coupling electrical stimulation to the electrically conducting polymer oxidized polypyrrole, neurite outgrowth response was significant, yielding neurites on average almost double in length. 58 Another investigation improved nerve and glial cell attachment and differentiation on positively charged hydrogels, in addition to augmented neurite outgrowth. 77 Alterations in surface chemistry are an effective strategy in promoting neurite adhesion and outgrowth.
In addition to chemical modifications, physical alterations, such as morphology, have been investigated for their role in cellular adhesion and survival. Effective strategies to promote neurite outgrowth based on micro- and nanopatterning (discussed next) have been reported; however, surface roughness can have deleterious effects on neural cells. A recent study investigating nanorough surfaces showed high sensitivity and apoptotic/necrotic response of neuronally differentiated SH-SY5Y cells to gold surfaces. 78 On exposure to the rough surfaces, a loss of neuronal polarity was observed. These results suggest that surface roughness and micro- and nanotopography need to be evaluated in vitro for their physiological impact before use in regenerative applications. Primary neuron cultures and neuron-differentiated cell lines are effective modules for analyzing the efficacy and/or neurotoxicity of various surface chemistries and morphologies.
Cues Inside of the Conduit
Nerve conduits have inconsistently performed in bridging rat defects greater than 10 mm. 79 An emerging concept is that of luminal fillers, which serve as secondary scaffolds within the nerve conduits. These internal scaffolds hypothetically allow for increased neurite and Schwann cell outgrowth/proliferation based on the proteins and growth factors that are presented within the conduit. Additionally, it is often advantageous to present these proteins in an anisotropic fashion, as this has proved effective in promoting growth cone chemotaxis. Conduit “cues” can be divided into three categories, based on their role inside the conduit: neurotrophic factors, protein cues, and anisotropy.
Neurotrophic factors
Controlled release of neurotrophic factors is a desirable property of a conduit. Neurotrophic factors offer outgrowth and survival cues to the nerve cable that are often essential for full regeneration of critical defects. For each type of nerve (whether motor or sensory or both) and desired outcome (outgrowth and/or survival), there is a subset of neurotrophic factors recommended. Most in vivo models are currently concerned with mixed nerves, containing efferent and afferent neurons, such as the sciatic nerve. For peripheral nerve regeneration, the principal neurotrophic factors used are NGF, GDNF, brain-derived neurotrophic factor (BDNF), neurotrophin-3,4/5 (NT-3,4/5), and ciliary neurotrophic factor (CNTF). An overview of the neurotrophic factors used in nerve repair is provided in Table 3a and b. Future considerations for neurotrophic factors will include investigations into controlled release and perhaps gradient delivery. Numerous mechanisms are currently in use for the delivery of neurotrophic factors such as matrices, microspheres, and hydrogels. Different release mechanisms and profiles may have different effects in vivo.
BDNF, brain-derived neurotrophic factor; CNTF, ciliary neurotrophic factor; CNTFR, ciliary neurotrophic factor receptor; NT, neurotrophin; PNS, peripheral nervous system.
Table adapted from Schmidt and Leach. 86
CNS, central nervous system; FGFs, fibroblast growth factors.
Secondary scaffolds/protein cues
To cross critically sized defects, there may be a need for secondary scaffolds within the NGC. Although nerve gaps can be physiologically repaired over short distances, via band of Büngner formation (fibrin/LN-1 cables with Schwann cells), larger defects eliminate this possibility. 79 To bridge these defects, one strategy has been to incorporate mesenchymal stem cells (MSCs), which are expected to have neurotrophic function, significantly upregulating growth factors BDNF, CNTF, and basic fibroblast growth factor relative to an empty conduit control. 87 MSCs can also be transdifferentiated into Schwann-like cells, which were shown to encourage nerve regeneration and remyelination in a 1 cm facial nerve defect in rabbits. 88 Additionally, favorable results were observed in an 8 mm rat facial nerve defect model supplemented with autologous adipose-derived stem cells. 89
Another strategy has been to incorporate a soft interior scaffold, which can provide the matrix for growth of Schwann cells and regenerating neurons and aid in more rapid band formation. Secondary scaffolds have yielded some positive in vivo results. The use of keratin-based hydrogels yielded axon diameters and densities greater than nerve autografts. 41 Recently, positive results have also been observed with keratin “fillers” in a subcritical 2 cm rabbit tibial defect. NeuraGen collagen nerve guides were supplemented with internal keratin hydrogel scaffolds, which significantly outperformed empty nerve guides with regard to electrophysiology and histolomorphometry. 90 Similarly successful conduits used fibrin, with neovascularization and early-stage formation of fibroblast- and macrophage-rich tissues 4 weeks postimplantation in a rat model. 91 Despite these findings, other studies found that only tandem gradients of laminin-1 (LN-1) and NGF were able to promote axonal regeneration of a critically sized defect (20 mm) in a rodent model. Isotropic distributions of these proteins were actually insufficient for regeneration. 35 These results are not surprising, as to bridge these critically sized defects, the regenerating cable needs a chemotactic signal to promote (1) cell survival via the presence of the ECM protein/growth factor, and (2) directionality via the ECM protein/growth factor gradient. Eloquent in vitro experiments have shown that gradients of growth factors such as NGF and adhesive proteins such as laminin (IKVAV peptide) are effective modulators of growth cone chemotaxis.75,92 The lack of these features in conduits could hinder neurite outgrowth in vivo. Over short gap defects in humans (≤3 cm in humans), chemotaxis from the distal nerve segment is most likely sufficient for recovery and guidance of the regenerating proximal segment; however, over longer distances, the lack of growth and chemotactic signals hinders the regenerative capacity of the nerve.
Although secondary scaffolds present an excellent platform for accelerated nerve regeneration, swelling has to be assessed before implantation. Hydrogels swell and deform during degradation, on occasion to the detriment of the nervous tissue. A recent study using poly(ethylene glycol) hydrogels as conduits showed that the gels swelled and deformed during degradation, leading to increased water uptake and decreased compressive modulus. 93 As discussed earlier, it is essential to confirm that swelling will not compress the nerve, which could possibly lead to entrapment-like syndromes causing pain and/or loss of function in the regenerated nerve.
Anisotropy
Scaffold anisotropy is a powerful strategy to control neuritogenesis and cellular alignment. 94 Indeed, in vitro cellular alignment is an excellent precursor to in vivo alignment and regeneration. 95 Consequently, many groups have devised strategies to achieve optimal cellular alignment, with techniques primarily based on micro- and nanopatterning and electrospinning. Numerous in vitro studies have successfully shown that topographical cues significantly influence neurite outgrowth/alignment, synaptic connections, and cellular differentiation,96,97 though fewer studies have used this strategy in vivo. However, these studies have found positive results. Recent in vivo studies bridging critically sized rat defects (≥14 mm) have found significant regeneration in treatment groups using highly aligned poly-acrylonitrile-co-methylacrylate thin films. Aligned films, alone within a conduit, were sufficient in bridging these critical defects.95,98 Scaffold anisotropy has been an effective technique in promoting nerve repair, and it will hopefully be concurrently implemented with other effective neurotrophic signals to generate successful, holistic conduits.
Cues from developmental biology-growth cone chemotaxis
There are multiple methods to guide axons through complex environments. To initiate robust growth cone chemotaxis, permissive substrates (such as laminin) are commonly used. 99 Additionally, guidance by contact inhibition is a prevalent mechanism of inhibiting neurite outgrowth and, thus, regeneration. Human neuroma expresses semaphorin 3A, which reduces neurite extension in vitro. 100 Future directions in peripheral nerve regeneration may include inhibiting such a class of molecules, in a similar fashion as is done with chondroitin sulfate proteoglycans in the central nervous system 101 and in the peripheral nervous system102,103 (as has been applied to decellularized nerve grafts). Additionally, regenerative outcomes are improved when mechanical guidance is provided by the original endoneurial tubes. 104 Use of technologies such as acellular nerve grafts, which precisely recapitulate the original nerve microarchitecture, could improve regenerative outcomes.
Conclusions
Nerve regeneration is a complex process that requires the presence of numerous factors, signaling cues, and design parameters to be successful (Table 4). The goal of peripheral nerve repair is to promote the robust regenerative response of the proximal nerve cable, so that it may eventually grow through its distal end, and recover functionality through synapsing with its original output. The purpose of this article is to elucidate some of the bioengineering strategies currently in use to address these challenges. There remains no biomaterial solution today than has been shown to outperform the autologous nerve graft, though there are many strategies that are encouraging. A useful nerve guide or conduit should contain some key design parameters: anisotropy to allow for directional outgrowth of the axons, controlled release/delivery of growth factors in tandem (as listed in Table 3)/adhesive molecules such as laminin and fibronectin, biocompatibility, biodegradability to complement the nerve regeneration rate, and conduit porosity to allow sufficient nutrient infusion while limiting fibrous tissue infiltration. A list of the current generation of clinically and experimentally available NGCs with various design criteria implemented can be found in Table 5. The next generation of conduits will incorporate all the factors just mentioned. Additionally, the importance of scaffold selection cannot be ignored. Both biopolymers and synthetic materials may contribute to the development of more successful solutions than nerve autografts, though they each have limitations. Although biopolymers offer the highest degree of biocompatibility and cellular affinity, synthetic materials often offer a higher degree of modifications. As scientists continue to investigate the mechanisms behind nerve injury and repair, engineers will be able to incorporate more complex designs and distributions of factors into conduits, to best mimic natural nerve regeneration. As we learn more about the mechanisms behind repair, strategies will continue to emerge toward more successful outcomes.
Bio, biocompatibility; Deg, degradation/porosity; Anis, anisotropy; Pro, protein modification/release, Phys, physical fit; Supp, support cells; Elec, electrically conducting.
Footnotes
Acknowledgments
The authors would like to thank Robyn Lindenberg for drawing ![]() . They thank the Tissue Engineering Resource Center (TERC) through the NIH (P41EB002520) from the National Institute of Biomedical Imaging and Bioengineering, and the Armed Forces Institute for Regenerative Medicine (AFIRM) for support toward this work.
. They thank the Tissue Engineering Resource Center (TERC) through the NIH (P41EB002520) from the National Institute of Biomedical Imaging and Bioengineering, and the Armed Forces Institute for Regenerative Medicine (AFIRM) for support toward this work.
Disclosure Statement
No competing financial interests exist.