
Abstract
Bone repair and regeneration is a dynamic process that involves a complex interplay between the (1) ground substance, (2) cells, and (3) milieu. While each constituent is integral to the final product, it is often helpful to consider each component individually. Therefore, we created a two-part review to examine scaffolds and cells' roles in bone tissue engineering. In Part I, we review the myriad of materials use for in vivo bone engineering. In Part II, we discuss the variety cell types (e.g., osteocytes, osteoblasts, osteoclasts, chondrocytes, mesenchymal stem cells, and vasculogenic cells) that are seeded upon or recruited to these scaffolds. In Part III, we discuss the optimization of the microenvironment. The biochemical processes and sequence of events that guide matrix production, cellular activation, and ossification are vital to developing successful bone tissue engineering strategies and are thus succinctly reviewed herein.
Introduction
Until recent years, the bone ECM was viewed as static, inert, and providing little more than mechanical support. 1 In reality, the bone ECM is a dynamic conductor of bone repair and regeneration. The ECM sequesters and preserves osteogenic and vasculogenic growth factors2,3 as well as provides a malleable scaffold upon which cells may migrate, adhere, proliferate, and differentiate. 4 It is now well known that many factors can impair successful bony reossification. For example, skull bone regeneration tends only to occur in infants younger than 2 years of age. 5 Since the ECM is so vital to native bone formation, scientists have used information gleaned from bone development and repair mechanisms to create artificial ECMs designed to overcome obstacles and guide bone regeneration. While many materials have been used clinically (e.g., autologous bone grafts, 6 allogeneic banked bone, 7 ceramic scaffolds composed of calcium phosphates, 8 demineralized matrix pastes, 9 and others), every month new investigational compounds and polymers are reported in the literature. 10 The multitude of techniques reflects both the inadequacy of each individual method as well as the enormous need to faithfully reconstruct the skeleton. To date, no ideal scaffolding material has been discovered and each existing ECM has limitations such as donor-site morbidity, an obligatory graft resorption phase, contour irregularities, insufficient autogenous resources, disease transmission, major histoincompatibility, graft-versus-host disease, immunosuppression, structural failure, stress shielding, and infection of foreign material. 11 Therefore, since the need for better bone scaffold materials is urgent; herein, we examine some of the successes as well as the failures of ECM replacement materials.
Bone Formation
Bone formation occurs by two distinct mechanisms: intramembranous and endochondral bone formation (Fig. 1). Briefly, intramembranous bone formation occurs by direct ossification of fibrous tissue while endochondral bone formation occurs through a cartilaginous intermediate that is replaced by nascent bone. Since intramembranous bone formation is thought to be mechanistically simpler, it has traditionally been the method of bone formation that scientists have targeted for BTE. However, recently investigators demonstrated that endochondral bone formation can be recapitulated using a bioceramic scaffold. (See section on Biphasic calcium phosphates)
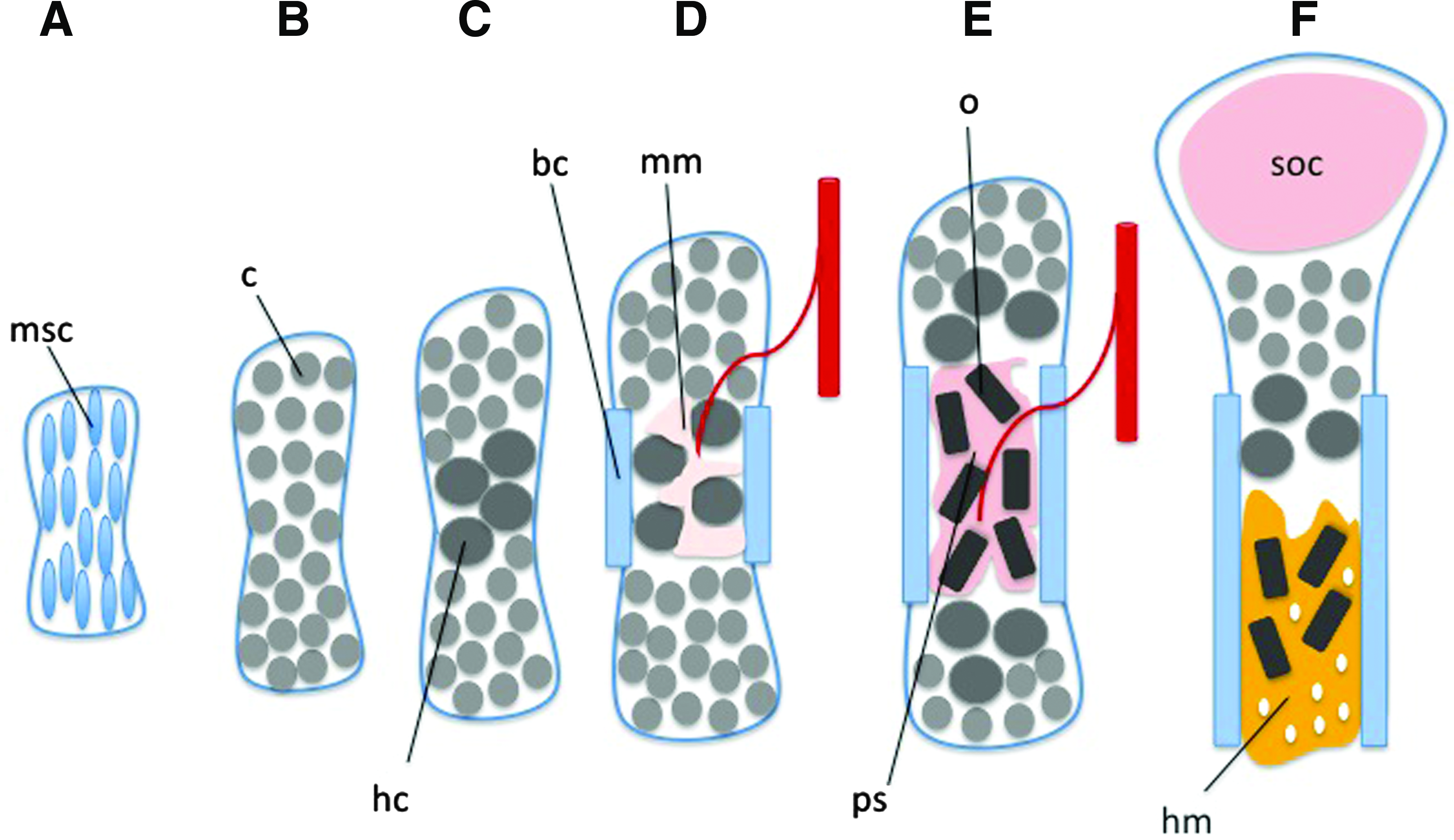
Bone growth: endochondral bone growth and intramembranous bone growth. Intramembranous bone formation occurs by the direct ossification of osteoprogenitor cells while endochondral bone formation is more complex requiring initial mobilization and hypertrophy of chondrocytes, followed by their death and replacement by osteoblasts.
Scaffold Materials
The number of novel scaffolds has skyrocketed in recent years due, in part, to the optimistic view that finding the right design and material will lead to bone regeneration in vivo. 12 Numerous investigators have worked hard to optimize BTE scaffold docking properties, biocompatibility, osteoinductivity, 13 osteoconductivity, 13 mechanical resilience, and functional resorption while minimizing inflammation and foreign body reaction (Table 1). While innumerable scaffolding materials have been tested, most empty scaffolds have largely failed to improve bone healing. 14 Therefore, investigators have the filled panoply of scaffolds with cells, growth factors, vasculogenic factors, and cellular signaling molecules.15–20 Herein, we examine the mainstay materials used to construct scaffolds and evaluate their efficacy as scaffolds as well as their drawbacks (Table 2).
Hydroxyapatite/tricalcium phosphate (HA/TCP) ratio dependent.
Calcium Phosphate Scaffolds
β-Tricalcium phosphates
β-Tricalcium phosphate (β-TCP) scaffold material was one of the first to be utilized as a platform for bone regeneration in vivo 21 due to its similar composition to mineral phase native bone22–24 [a molecular formula of Ca3(PO4)2 and a calcium-to-phosphate ratio of 1.5]. 25 In fact, as early as 1920 a study by Albee demonstrated that injection of β-TCP into a segmental defect of a canine radius aided in bone union. 26 β-TCP scaffolds are strongly osteoconductive and exert their effects via interaction with α2β1 integrins on osteogenic cells and subsequent downstream activation of MAPK/ERK signaling pathways in these cells. 27 Furthermore, β-TCP scaffolds have a compressive and tensile strength similar to native cancellous bone 28 and may thus be impregnated within a bony defect without the risk of compressive dissolution of the scaffold.
Scaffolds composed of β-TCP have been utilized in animal models to help heal critical-size calvarial defects,29,30 mandibular defects,31–33 tibial 34 and femoral defects,35,36 radial defects,37,38 and others. The efficacy of β-TCP scaffolds has further been demonstrated in animals to be enhanced by coadministration with, or seeding of, recombinant human bone morphogenetic protein-2 (rhBMP-2) within the scaffold.39–42 Of particular importance for craniomaxillofacial and oral surgeons, a β-TCP scaffold seeded with rabbit mesenchymal stem cells (MSCs) transfected by an adenovirus carrying bmp-2 demonstrated complete regeneration of mature bone structure in an elevated maxillary sinus by 8 weeks. 43 Additionally, in human subjects β-TCP scaffolds have been utilized to fill segmental defects following resection of bone-related tumors. 44
Recently, investigation into β-TCP scaffolds seeded with adipose-derived stem cells (ASCs) has demonstrated that this material is capable of inducing stem cells to differentiate into osteoblastic cells.45,46 Specifically, a β-TCP scaffold seeded with ASCs completely healed a critical-size (15 mm) radial defect in a rabbit with bone composition similar to native bone. 47 It has further been demonstrated that this scaffold material seeded with the same ASCs is capable of markedly increasing angiogenesis in a rat prefabricated inferior epigastric artery flap. 48 Because angiogenesis and vasculogenesis are key events in bone healing and tissue regeneration, this is a significant finding. These studies, taken together, are important because much recent investigation has focused on ASCs as an abundant supply of MSCs for regenerative medicine. 49
Calcium phosphate scaffolds such as β-TCP are a promising avenue for bone regeneration because the normal process of mineral precipitation and ossification is dependent upon (i) the extracellular concentration of phosphate, and (ii) on the extracellular concentration of calcium (as demonstrated by a combination of in vitro and in vivo experiments by Murshed et al. 50 ). A major drawback to utilizing β-TCP scaffolds extensively in the clinical setting is the observation that in vivo bone resorption does not occur in a predictable 1:1 ratio 51 ; the resorption rate of the scaffold exceeds that of the production of native bone. Future research will determine whether or not β-TCP scaffolds have a significant future in BTE.
Hydroxyapatite
The inorganic element of the native bone ECM is composed of precipitated hydroxyapatite (HA) crystals. For this reason, HA scaffolds, which maybe designed with many different densities, porosities, sizes, and strengths, 52 have been advocated for use in BTE. HA scaffolds [Ca5(PO4)3OH] have a calcium-to-phosphate ratio of 1.67. 25 An important aspect of HA scaffolds that is medically relevant and must be considered is the fact that this material is strongly osteoconductive but minimally osteogenic. 53 By seeding the scaffold with osteogenic cells, however, the scaffold material can be made more osteogenic than on its own. 54 It has been reported in the literature that the porosity of the scaffold is important for proper cellular seeding and vascularization of the scaffold: a pore size of approximately 100 μm is ideal55,56 (human cortical bone, which is less porous than cancellous bone, has an average pore size of 100 μm within the Haversian canal sytem).56–58 As with β-TCP scaffolds, HA scaffolds have been cited numerous times in helping correct cranial,59–61 long bone,62–64 mandibular, 65 radial, 66 and other defects. Similar to the β-TCP scaffolds, HA scaffolds have been seeded with MSCs transfected with a bmp-7-carrying adenovirus and this construct was capable of inducing 55% new bone volume by 4 weeks postoperatively in a rabbit mandibular defect model compared with 33% for control animals. 67
In the recent literature, HA has been combined with other compounds such as collagen,68,69 poly D, L-lactic-co-glycolic acid [PLGA; a biodegradable nanocomposite of poly(lactide-coglycolide)], 70 and chitosan [a linear polysaccharide composed of randomly distributed β-(1-4)-linked D-glucosamine and N-acetyl-D-glucosamine], 71 and this combination approach has yielded scaffold materials that are more useful than HA. Specifically, these hybrid scaffolds are better promoters of osteoblast adhesion, proliferation, and differentiation than the pure HA scaffolds.
HA, when used alone, resorbs slowly, is quite brittle, and has a high melting temperature. 72 To address these issues, nanocomposite structures have been manufactured in many shapes and sizes so as to be able to fit any bony defect. They have been made with a mechanical integrity similar to that of spongy bone. 73 Another commonly recognized problem with HA scaffolds is their inability to maintain cells within the interior because of a lack of nutrient delivery to this area. To address this issue, Buckley and O'Kelly developed a scaffold that has two separate functional areas: one area for the seeding of cells, and a separate area for nutrient delivery. Between these two functionally distinct areas run unidirectional channels that maybe used to perfuse the cells from the area of nutrient delivery to the area of cell seeding (Fig. 2). The osteoblasts seeded within this scaffold design utilized oxygen more efficiently (0.91 fmol min−1 cell−1) when compared to a similar experiment by Guarino et al. who used a polysaccharide scaffold (0.80 fmol min−1 cell−1) and also demonstrated an overall 18-fold increase in permeability values.74,75 Certainly, future research into the best combinations of HA and other materials will yield important information on how we can utilize the native mineral-phase bone ECM to guide bone regeneration.
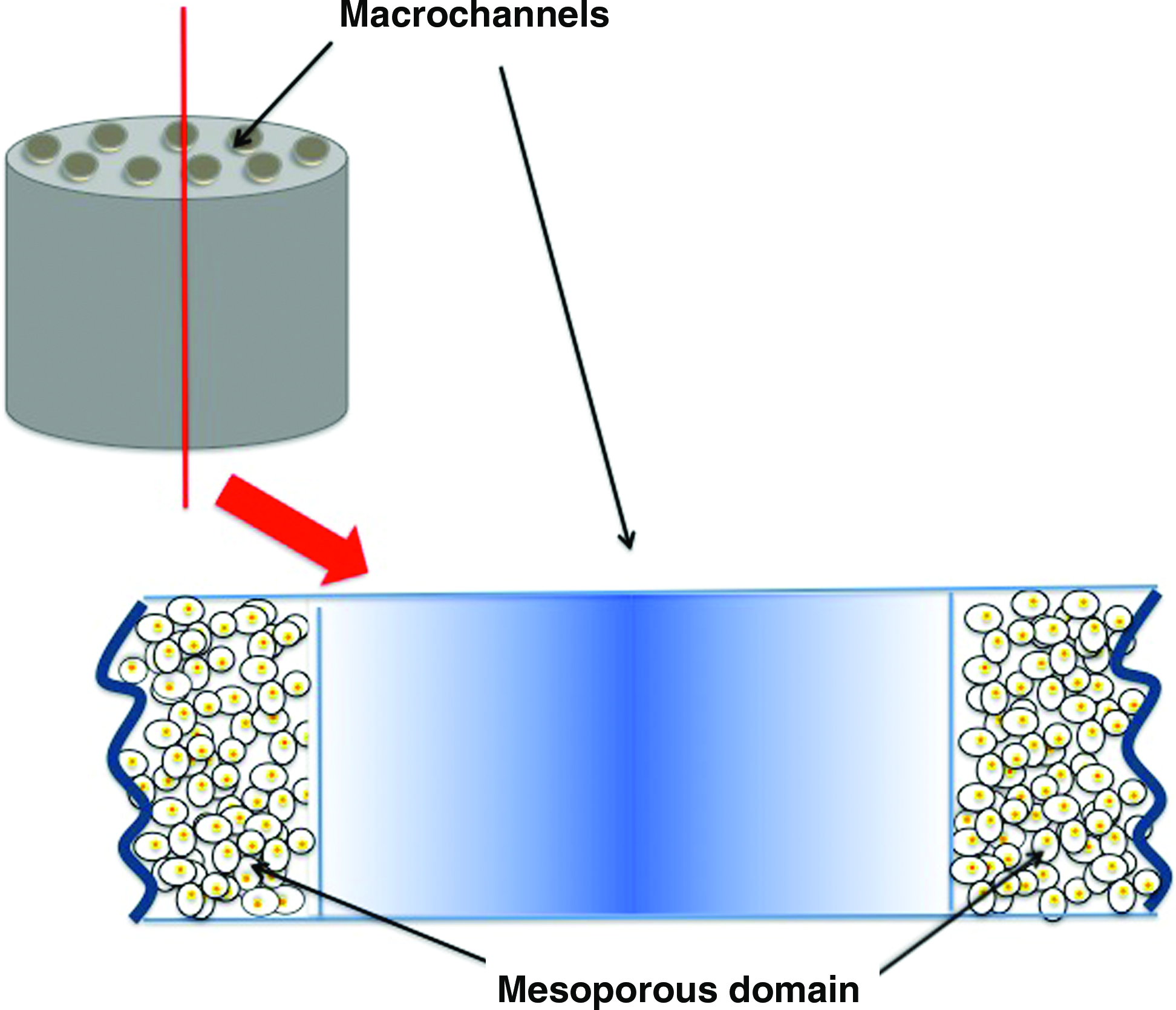
Buckley and O'Kelly “double” scaffold.74 This scaffold has two separate functional areas: one area for the seeding of cells, and a separate area for nutrient delivery. Between these two functionally distinct areas run unidirectional channels (macrochannels) that maybe used to perfuse the cells from the area of nutrient delivery to the area of cell seeding. Color images available online at www.liebertonline.com/teb
Because HA and β-TCP scaffolds have disadvantages that are largely in opposition to one another, people have tried scaffolds composed of combinations of these two compounds in order to reduce the independent drawbacks of each material. It is to this combination scaffold material that we now turn our attention.
Biphasic calcium phosphates
Biphasic calcium phosphate (BCP) scaffolds are made of variable amounts of β-TCP and HA76–78 and thus any given scaffold may have more or less capacity to release calcium and phosphate ions into the bony microenvironment. 79 As one increases the percentage of β-TCP, more ions are released, and as one increases the percentage of HA, the mechanical integrity of the scaffold is increased. 80 Moreover, their compressive strength is more influenced by the phase composition and the macroporosity then the pore geometry. This highlights the endless possibilities for personalization of scaffolds by modifying the pore size and phase composition in order to adjust strength values. 81 Polak et al. also showed that bone formation on BCP scaffolds can be significantly improved by two factors: microporosity (<20 μm) and the addition of rhBMP-2. Their study showed that bony healing of porcine mandibular defects could be accelerated up to 4-fold. 82 BCP scaffolds have been utilized for bone regeneration in canine mandibular defects and femoral head osteonecrosis cases83,84 and iliac wing defects in goats 85 : BCP scaffolds have, in fact, been demonstrated to be superior in guiding bone regeneration when compared with both HA scaffolds 86 and even native bone mineral. 87 Additionally, BCP scaffolds have excellent cellular biocompatibility. 88
While bone formation can occur by two different mechanisms (endochondral and intramembranous), intramembranous bone formation has traditionally been the method that investigators have attempted to mimic for BTE. However, it was recently demonstrated that endochondral bone could be created using a BCP scaffold. Investigators seeded chick embryonic tibia-derived chondrocytes onto macroporous BCP scaffold particles and treated them with retinoic acid in order to induce chondrocyte maturation and ECM deposition. 89
The thickness of the chondrocyte and ECM layer increased in the presence of the retinoid. Furthermore, extended retinoic acid treatment increased alkaline phosphatase (ALP) activity and expression, proteoglycan synthesis, and cbfa1 and type I collagen mRNA levels resulting in endochondral bone formation. This is a significant finding because the majority of the appendicular skeleton develops embryologically through endochondral bone formation. Moreover, native bone healing occurs through an endochondral repair mechanism. Although the literature is not devoid of studies utilizing BCP scaffolds, it is not affluent either. While BCP scaffolds have composite HA:β-TCP flexibility, it is unclear whether future research will uncover an optimal ratio to enable this scaffold material to solve large clinical problems.
Octacalcium phosphate
Octacalcium phosphate (OCP) scaffolds for guided bone regeneration were introduced within the last decade. The scientific rationale for using this material as a scaffold is that it is a biological precursor of apatite crystals (similar to HA) 90 and strongly induces MSC osteoblastic differentiation.91–93 Additionally, OCP scaffolds are more strongly osteogenic and direct more bone regeneration than both HA and β-TCP scaffolds.94,95 In addition to this, they have better surface microarchitecture for the attachment of osteoblasts and their precursors than both HA and β-TCP scaffolds. 96 As with many other scaffold materials, OCP scaffolds have been proven efficacious in seeding rhBMP-2 and promoting improved bone regeneration in vivo. Specifically, Kamakura et al. found that an OCP scaffold seeded with rhBMP-2 was capable of inducing 70% more functional bone by 8 weeks postoperatively in a rat cranial defect model. 97
OCP scaffolds have been commonly combined with collagen in an attempt to reproduce an ECM material that is similar to native bone. In a study by Kamakura et al., it was discovered that an OCP/collagen composite scaffold had the capacity to act synergistically and enhanced bone regeneration, nucleation, and cellular infiltration. 98 These composite scaffolds demonstrate improved bone regeneration and osteogenic cell attachment as the ratio of OCP:collagen is increased.95,99 Additionally, during the preparation of an OCP:collagen composite scaffold, dehydrothermal treatment of the collagen fibers strongly improves their capacity to guide new bone regeneration. This is because dehydrothermal treatment increases collagen crosslinking and slows its degradation; this increases the capacity for osteogenic cells to adhere to and proliferate upon the scaffold. 100 Unfortunately, the literature is currently bereft of extensive studies using this material. The few studies that do exist demonstrate OCP to be superior to both HA and β-TCP and thus more investigation into the usefulness of this scaffold material is pertinent.
Calcium Sulfate Scaffolds
Calcium sulfate (CS), also known as Plaster of Paris, has been utilized as a synthetic bone graft material for over 100 years 101 and is still widely used for bone repair as a bone graft binder and expander. 102 In addition to acting as a bone “glue” in orthopedic surgery, it is also thought to act as an osteoconductive substrate 103 and serve as a platform for the recruitment and invasion of blood vessels and osteoblasts when placed in contact with viable endosteum or periosteum. 104 Importantly, CS scaffolds have a nanoscale architecture that promotes osteoblast adhesion 105 and simultaneously produces no appreciable inflammation. 106
Because CS is such a simple compound, it has been combined with many other materials in an attempt to create a scaffold that promotes bone growth through a multitude of mechanisms. Gao et al. demonstrated that a CS/poly-L-lactic acid (CS/PLLA) scaffold was capable of promoting osteoblast adherence and spreading by altering the surface architecture of the scaffold. The PLLA slowed the conversion of calcium sulfate hemihydrate (CSH) to calcium sulfate dihydrate (CSD) and this changed the crystal structure of the scaffold so that its resorption time was increased; this decreased rate of absorption leads to increased time for cellular attachment and proliferation of osteogenic cells. 107 This same group has shown that CS maybe combined with gelatin and this combination also slows the conversion of CSH to CSD and therefore improves osteoblast adhesion to the scaffold. 108 CS has further been used as a coating on HA scaffolds in an attempt to improve the mechanical integrity and bioactivity of the scaffolds. CS-coated HA scaffolds demonstrated a significant improvement in mechanical and biological properties when compared with pure HA scaffolds. 109 As previously noted, CS has been used in bone repair for many years and perhaps this experience with the material will one day yield a scaffold compound that maybe utilized regularly in BTE applications.
Electrospun Nanoscaffolds
New methodologies for creating bone scaffold materials have emerged through improvements in nanotechnology and advances in polymer chemistry. These new scaffolds are teleologically designed to mimic natural ECMs.110,111 The wealth of different scaffold materials recently produced is in large part thanks to our increasing knowledge of the bone microenvironment and our ability to recapitulate it through technological advancements. It is now relatively simple to design a scaffold with the exact biochemical and biomechanical properties that one wishes to obtain. 112 In fact, scaffolds are now designed with nanoscale specificities and properties that are ingenious and are composed of nanofibers of varying calibers with varying adherence properties. 113 The process of electrospinning nanofibers, in which polymeric fibers are formed by subjecting a fluid jet to a high-power electric field, 114 is a widely used technique for generating bone scaffolds.
Nanofibrous scaffolds have been designed that function to activate enzymes that lead to improved bone regeneration and growth. An important enzyme for promoting bone regeneration is ALP. 115 Electrospun fibrin nanofibers have been demonstrated to immobilize enzymatically active ALP and therefore promote bone regeneration by increasing the local concentration of biologically available inorganic phosphate. 116 Additionally, electrospun scaffolds have been demonstrated to increase the level of ALP. As a reminder, ALP is a marker of osteoblast activity and thus, indirectly, of bone formation. These electrospun nanofibers have been composed of various materials (e.g., polycaprolactone (PCL), 117 PLLA/gelatin/HA, 118 and PLLA/TCP) 119 but they all have shown the capacity to increase osteoblastic ALP. In addition to increasing the activity of important osteogenic enzymes, electrospun nanofibrous scaffolds have been designed with specific molecular characteristics that may bind cells and or proteins ex vivo prior to implantation.
Since there are three important elements to consider when engineering bone, (the scaffold, the cells seeded on the scaffold, and the environment within which the scaffold sits), investigators have designed new scaffold technologies with the capacity to bind and sequester cells and growth factors120,121 in order to induce bone formation in vivo. McCullen et al. designed a multilayered, electrospun scaffold held together by type 1 collagen glue that was seeded with human ASCs. These scaffolds were subsequently laser ablated in order to form pores within the scaffolds. The ablated scaffolds, when compared with nonablated scaffolds, were found to have enhanced cell proliferation (500 ngDNA/construct vs. 300 ngDNA/construct) and mineral deposition (233 μgCa2+/construct vs. 188 μgCa2+/construct). 46 Similarly, Srouji et al. developed a multilayered PCL/collagen scaffold seeded with bone marrow–derived hematopoietic stem cells that was capable of inducing massive cellular proliferation and viability. 122 Interestingly, Ma et al. successfully designed an electrospun nanofiber scaffold composed of poly(dl-lactide-co-glycolide)/collagen type 1 that captured bone marrow–derived hematopoietic stem cells, which promote osteoblastic function. 123
In addition to cells, growth factors were loaded onto nanofiber scaffolds. β-FGF embedded within electrospun PLGA scaffolds 16 and rhBMP-2–embedded silk fibroin nanofiber scaffolds 124 have demonstrated the capacity to increase bone-specific transcription factors within MSCs and thus promote their differentiation into osteogenic cells (It is important to mention that cells may have varying degrees of osteogenic potential and, therefore, varying degrees of osteogenic responsiveness to nanofibers. Please see Part II of this article series). Yoon et al. also demonstrated that an electrospun PCL scaffold maybe used as a functional drug delivery system. 125 All of these different measures are being tested with an end goal in mind: to create mineral deposition and new bone formation within a bony defect.
Because electrospun nanofiber scaffolds are generally brittle, newer electrospun scaffolds have been designed to increase and improve mineralization of the scaffold once osteogenic cells adhere to it and thus improve its mechanical stability and integrity. Many different materials and techniques have been utilized to promote rapid mineralization of electrospun scaffolds. Andric et al. used a PLLA scaffold pretreated with 0.1 M NaOH and subsequently immersed in simulated body fluid and placed in a vacuum. This technique improved mineralization of the scaffold and increased its yield stress and elastic modulus each by 2–3 times. 126 Chen et al. similarly used a PLLA scaffold in NaOH and found an increased capacity for mineralization of the scaffold. 127 Many other scaffold materials have also been used that promote mineralization including electrospun chitosan-based/HA nanofibers, 128 electrospun polydioxanone/HA nanofibers, 129 electrospun PCL scaffolds, 130 electrospun HA/collagen nanofibers,131,132 electrospun PCL/HA/gelatin nanofibers, 133 electrospun PLLA/HA/collagen nanofibers, 134 electrospun poly[(R)-3-hydroxylbutrate]/poly(ethyleneglycol) nanofibers, 135 and others.
The recent advent of electrospun nanofiber technology has led to an explosion of new polymers and scaffold materials. Certainly, as time progresses more and more scaffolds will be utilized and designed.
Other Advanced Polymers
Lu et al. tested the use of collagen to create scaffolds interestingly designed to promote a more even cell distribution. These collagen-based scaffolds were designed in a funnel shape but, when tested, were found to be lacking in strength. However, when combined with PLGA, they were found to be stronger and more resilient and were, in addition, found to have more homogenous cell distribution. 136
Since hyperthermia and local drug delivery have been proposed as potential therapeutic approaches for bone defects resulting from malignant bone tumors, Wu et al. (Shanghai Institute of Ceramics) worked on a formulation of mesoporous bioactive glass (MBG) with magnetic and drug delivery properties to potentially meet this goal. 137 They successfully prepared magnetic MBG scaffolds and investigated what effects the incorporated iron could have on the mesopore structure, physiochemistry, magnetism, drug delivery, and biological properties. Incorporating iron into mesoporous MBG glass scaffolds made them magnetic, as expected, but also, interestingly, significantly improved the cell mitochondrial activity of and bone-related gene expression by the seeded BMSCs. The Fe-MBG scaffolds were biodegradable, bioactive, magnetic, and, at the same time, capable of sustained drug delivery. Moreover, the authors suggested that the multifunctionality of Fe-MBG scaffolds could be used for the therapy of malignant bone disease by a combination of hyperthermia and local drug delivery, and for the regeneration of bone defects by virtue of the excellent osteoconductivity of the material. 137 This still needs to be proven but is certainly a very interesting approach to cancer-related bone loss.
Another group (the Lawrence Berkley Laboratory in Berkeley California) has also been successfully using bioactive glass, referred to here as F-127. When assessed prior to submersion in simulated body fluid, this sintered glass was demonstrating an increased compressive strength of 136 MPa. And even after it had been immersed in simulated body fluid for 3 weeks, it was retaining a compressive strength of 77 MPa. Compared to cortical bone, which is known to withstand between 100 and 150 MPa, this demonstrates impressive strength; strength that is often required when weight bearing is concerned. 138
One of the many limitations of scaffold-based tissue engineering is the inability to create densely populated constructs thicker than a few 100 μm. At the University of Utah, they found that by creating channels in polyurethane sheets, and then perfusing them in an even-flow bioreactor, they were able to achieve greater cell density, as well as more homogenous cell distribution within the scaffolds. 139
When Tantalum (chemical element #73) scaffolds were evaluated by Jonitz et al., they found that under critical oxygen and nutrient supply, osteoblasts were shown to migrate more evenly. Since in the past it has been assumed that lack of migration of osteocytes was due to inadequate nutrient and oxygen in the middle of the scaffold, their experiments were done such that after 24 h, there was a deficit of nutrients in the normally uninhabited regions of the scaffold. What they found was that in spite of lower oxygen and nutrient levels, and slight acidification, there was, nonetheless, osteoblast migration. At least for Tantalum scaffolds, there seems to be evidence for reasons other than nutrient and oxygen content for the lack of migration seen in synthetic scaffolds. 140
Lastly, Psycharakas et al. investigated the use of a new polymer. 141 They used a combination of silicon-zirconium and silicon-titanium that supplied both the inorganic structural integrity and the organic, “cell friendly” environment that is necessary for successful osteocytic migration. These scaffolds were treated with a two-photon polymerization laser technology that was able to create micrometer-sized pores that was shown to lead to more effective cell distribution. 141 The purpose of this work was to analyze the effect of the organic/inorganic composition of the materials on cell behavior and the establishment of a “cell-culture friendly” environment and further experiments are still needed to validate its use.
FDA-Approved Scaffolds Used in Humans
Some scaffold combinations have been used successfully in craniomaxillofacial and orthopedic surgery. In orthopedic surgery, for example, two studies showed that bilateral treatment of the posterolateral spine with rhBMP-2 (in carrier consisting of 60% HA and 40% tricalcium phosphate granules) resulted in complete spinal fusion in 100% of patients receiving the treatment.142,143 Moreover, Dawson et al. compared the combination of an absorbable collagen sponge soaked with rhBMP-2 and ceramic granules to the classic iliac bone graft for an anterior lumbar interbody arthrodesis, they showed improved clinical outcomes and higher rates of fusion. 144 It is important to mention that in Europe, some kits are already commercially available. For example, rhBMP-2 is available for the treatment of acute open tibial fractures (InductOS implant kit; Medtronic Sofamor Danek and Wyeth Pharmaceuticals) as a lyophilized powder, dissolved in sterile water, and applied to an absorbable collagen matrix made of type 1 bovine collagen. A similar kit (InFuse bone graft; Medtronic Sofamor Danek) is also available in Europe and in the United States for the treatment of degenerative lumbar disc disease. 145 All these previously mentioned kits use rhBMP-2 but two additional kits using rhBMP-7 are also available on the market. OP-1 Implant (Olympus Biotech) is rhBMP-7 formulated with a purified type I collagen carrier indicated for the revision of posterolateral fusion and long-bone nonunion, when OSIGRAFT (Stryker), also made of rhBMP-7 in an osteoconductive bovine type 1 bone collagen matrix, is indicated for nonhealing tibial fracture. 146 Some complications with the use of rhBMP-2 have been reported; cases of exhuberant/ectopic bone formation,147,148 acute airway obstruction associated with their use in cervical spinal fusion, 149 and vertebral osteolysis 150 can be found in the literature.
Craniomaxillofacial surgeons commonly use autologous bone grafts to reconstruct dentoalveolar clefts. Recently, a number of investigators have begun comparing the volume and location as well as the height of neodentoalveolar bone formed at the cleft site in patients treated with rhBMP-2–loaded scaffolds versus iliac crest bone graft (current gold standard). For example, Dickinson et al., Fallucco et al., and Jung et al. reported more bone formation, a greater bone height, and successful osteointegration of dental implants.151–153
In both orthopedic and craniomaxillofacial surgery, initial scaffold-induced new bone formation results are promising. However, the success is limited to smaller defects (e.g., dentoaleolus) and long-term data are still needed.
Conclusions
After many years of BTE research and the development of an untold number of scaffolds, we still have not yet identified the ideal material or design; however, we have made significant progress. Working together, scientists, physicians, chemists, and engineers have learnt a tremendous amount from the successes and failures of natural, synthetic, inorganic, and organic/hybrid nanoscaffolds. While the disruptive breakthrough technology remains elusive, all agree that the ideal scaffold material will have excellent biocompatible, osteocompatible, osteoconduction, osteoinduction, and neovasculogenic profiles.
Although the scaffold material is important for bone regeneration, it is not the only important factor. In the next part of this two-part review, we will focus on the important cell types that may be used to help guided bone regeneration.
The research on BTE is both promising and rewarding. The past few decades have demonstrated a remarkable increase in the literature of BTE, but many questions still remain unanswered: Can newly formed bone be self-supporting and renew itself? Can scaffold-derived bone support hematopoiesis? How exactly the host organism reacts and its cells react to implants of any biomaterial? Should we use different types of scaffolds and modulate their mechanical strength for different uses (different bones)? Almost certainly in the next few years we will see an even greater increase in that knowledge and our capacity to help correct bony defects.
Footnotes
Disclosure Statement
The authors hereby certify that, to the best of our knowledge, no financial support or benefits have been received by any coauthor, by any member of our immediate family, or any individual or entity with whom or with which we have a significant relationship from any commercial source which is related directly or indirectly to the work that is reported in the article.