
Abstract
Cardiac and vascular diseases represent one of the most substantial medical areas for the applications of regenerative medicine. Despite advances in endovascular repair, surgical intervention, and disease management, atherosclerosis and heart failure continue to be prominent health problems. This report analyzes the regenerative medicine treatment opportunities in both cardiovascular and peripheral vascular repair, examining the treatment opportunities for tissue-engineered vascular grafts as well as cell-based therapies. U.S. hospital discharge data were used to generate a detailed estimate of the relative target populations for cardiac and vascular disease. Gap analyses were performed for vascular access, small caliber vascular grafts, and cell-based therapies for revascularization and heart failure. The analysis compared current alternatives, gaps in medical need, and what a tissue-engineered or regenerative alternative should achieve for optimum medical and commercial feasibility. Although the number of coronary bypass grafts vastly outnumbered peripheral grafts, a detailed consideration of re-grafts and the success of first grafts combined with gap analysis (GAP) leads us to conclude that peripheral vascular disease is the more commercially feasible and attractive target opportunity for engineered small caliber grafts for the foreseeable future. Cardiac bypass would need substantial long-term clinical experience, which could be a significant hurdle. Vascular access, often regarded as a first-in-man indication, is an excellent opportunity for an engineered graft as an alternative to arteriovenous fistula that could overcome complications associated with a prosthetic graft. The GAP also suggests that for heart failure, cellular therapies should link near-term changes in repair, such as improvement in cardiac output and reduced scarring with limiting progression of the disease, reducing the need for complex pharmacologic management, and reducing rates of hospitalization. Naturally, researchers must determine where their technology and know-how can be applied most effectively, but it is clear from our analysis that an astute strategy in the use of science and technology will be important to successful translation in this space.
Introduction
It has long been recognized that tissue engineering could play an important role in vascular disease. For example, for vascular grafts, the seminal work of Weinberg and Bell, 5 fabricating vascular grafts from cell-seeded resorbable scaffolds6,7 the innovation of cell-produced grafts by Auger and colleagues,8,9 employing biological matrices as acellular grafts remodeled in vitro pioneered by Badylak and coworkers,10,11 and many other efforts laid the foundation for the promising work of today. Regenerative medicine is currently at a point of designing and producing numerous first-generation products, many to treat cardiovascular and peripheral vascular disorders. For example, the ground breaking clinical work of Shinoka and colleagues 12 has contributed critical understanding of vascular graft remodeling in humans. 13 Innovation continues in biomaterial design (reviewed by Ravi and Chaikof 14 ) using bone marrow as a cell source (reviewed by Critser et al. 15 ) as well as finding better ways to deal with problems of graft integration, 16 stenosis 17 (reviewed by Duncan and Breuer 18 ), and fabrication.19,20 Commercial efforts have also progressed; McAllister and colleagues (Cytograft, Inc.) have advanced a cell-produced vascular graft to the clinic with promising results21,22 and Dahl and colleagues (Humacyte, Inc.) have devised an innovative commercial process for large-scale construction of cell-based vascular grafts starting with a resorbable scaffold. 4 There seems little doubt that the technology and innovative talent will develop to ultimately commercialize functional vascular conduits and grafts. However, now more than ever, medical, regulatory, and commercial considerations must be integrated into a translational strategy for one to succeed in delivering these advances to patients in a commercial product. Although most will be first in class, they must deliver the same clinical effectiveness and commercial feasibility of any drug or device. Also, heart and vascular disorders present a wide variety of translational challenges from fundamental science and engineering to practical aspects of production and delivery and, in some cases, demonstration of comparative value over more traditional alternatives. Added to that is the challenge of developing business models that balance the cost of development and future revenue potential.
Having previously examined the broad data on the treatment opportunities in the cardiac and peripheral vascular space, 3 we now performed a more detailed analysis of specific treatment opportunities to determine the strongest opportunities for regenerative therapies as well as the clinical and commercial challenges they may face. We analyzed the therapeutic need and commercial opportunity with a development perspective, the goal being to acquire, consolidate, and analyze data and information that could better enable astute choices by those developing or hoping to develop regenerative medicine therapies and devices in this clinical space.
Methods
Estimate of opportunity analysis
Medical information about patients includes diagnoses and procedures coded using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes. ICD-9-CM codes were reviewed down to a billable code in both diagnosis and procedure categories and culled of codes irrelevant to use of a regenerative therapy. Estimates of incidence for the remaining ICD-9-CM codes were made using the Center for Disease Control's National Center for Health Statistics database. Estimates of incidence were captured for first and second diagnoses and all diagnoses. The National Hospital Discharge Survey (NHDS) is a national probability survey designed to meet the need for information on characteristics of inpatients discharged from non-Federal short-stay hospitals in the United States. From 1988 to 2007, the NHDS collected data from a sample of ∼270,000 inpatient records acquired from a national sample of about 500 hospitals through 2006. Beginning in 2007, the sample size was reduced to 239 hospitals; so, we used data collected from 2004 to 2006 to give us a consistent, yet broad estimate of the relative opportunity between indications.
The methods employed in the NHDS are covered in detail in Dennison and Pokras. 23 In brief, the survey uses a three-stage probability design, including both manual and automated medical records. The stages are primary sampling units (PSUs), hospitals with PSUs, and discharges within hospitals, making sure that the largest PSUs and hospitals are included. The target sample size is 250 discharges from manual hospitals and 2000 discharges from automated system hospitals. The sampling of hospitals is based on a national probability sample of discharges from noninstitutional hospitals excluding government hospitals, located in all states and the District of Columbia. Only hospitals with an average length of stay of fewer than 30 days for all patients, general hospitals, or children's general hospitals are included in the NHDS. The NHDS estimates are prioritized based on national aggregation statistics, national trend statistics, and aggregate statistics for the four main Census regions of the U.S. SESUDAAN (a standard errors program for computing standardized rates from sample survey data) and SUDAAN (a program especially suited for survey data [RTI International]) are used to calculate variances. We recognize that we may not capture all relevant clinical settings by using the NHDS, but with 500 hospitals captured and the measures the National Center for Health Statistics has put in place to arrive at an accurate sampling, we feel that this is the best source of consistent data. Since our main interest is in comparing data for various procedures, we feel that this approach is acceptable. Naturally, if NHDS introduced bias during the down select, this would translate to some bias in our analysis, but we believe that they would have carefully avoided this at the time.
The design of the NHDS requires that the survey data be inflated or weighted to produce national estimates. There are three components to the final weight: inflation by reciprocals of the probabilities of sample selection, adjustment for nonresponse, and population weighting ratio adjustments. The size of the treatment opportunity was calculated for years 2004–2006 using the SAS Ver. 9.2 statistical programming package. The findings and conclusions derived from this data are those of the authors and do not necessarily represent the views of the Research Data Center, the National Center for Health Statistics, or the Centers for Disease Control and Prevention.
Analysis of the vascular access opportunity required outpatient data. Outpatient data on the incidence and prevalence of vascular access were obtained from the Fistula First Breakthrough Initiative, which is a network of vascular access experts and stakeholders. The organization has collected monthly data on vascular access procedures from a network of thousands of outpatient facilities across the U.S. since 2003. Monthly data from 2004 to 2010 on the incidence and prevalence of vascular access procedures were used to estimate the opportunity for this indication. The data were downloaded in Microsoft Excel from the FistulaFirst.org website.
Gap analysis
Gap analyses were performed using data collected through PubMed literature search as well as Google internet search. We relied on multiple reviews in areas, where a broad assessment of practice or science was needed. Professional medical practice guidelines served as standards for current state of the art, where available. Each gap analysis (GAP) was done by indication by first defining the likely patient population based on current medical practice. The opportunities were then assessed based on treatment objectives for current standing, present deficiencies, and remaining or unfulfilled medical need.
Results
From both a technology and therapeutic target perspective, cardiovascular and peripheral vascular indications are closely related. Several biological processes, such as inflammation, vascularization, and regenerative signaling, intersect24–27 among these disease contexts. For this reason, we analyzed the therapeutic opportunities in cardiac and peripheral vascular medicine as a combined group referred to as “cardio/vascular.” It was clear that there were two categories of technology opportunity within the cardio/vascular disease space, (1) materials and grafts for vascular repair or bypass and (2) regenerative therapies for revascularization or regeneration. The first step was to understand the medical need and treatment incidence in each target indication.
General prevalence
Statistics from the American Heart Association estimate that over 81 million people in the U.S. have some form of cardiovascular disease. 1 The prevalence of coronary artery disease is estimated as 17 million and there are ∼10.2 million patients who suffer from angina. There are 8.5 million myocardial infarcts and 5.8 million patients with heart failure. A surprising 650,000 individuals have some form of congenital cardiovascular defect (Fig. 1).
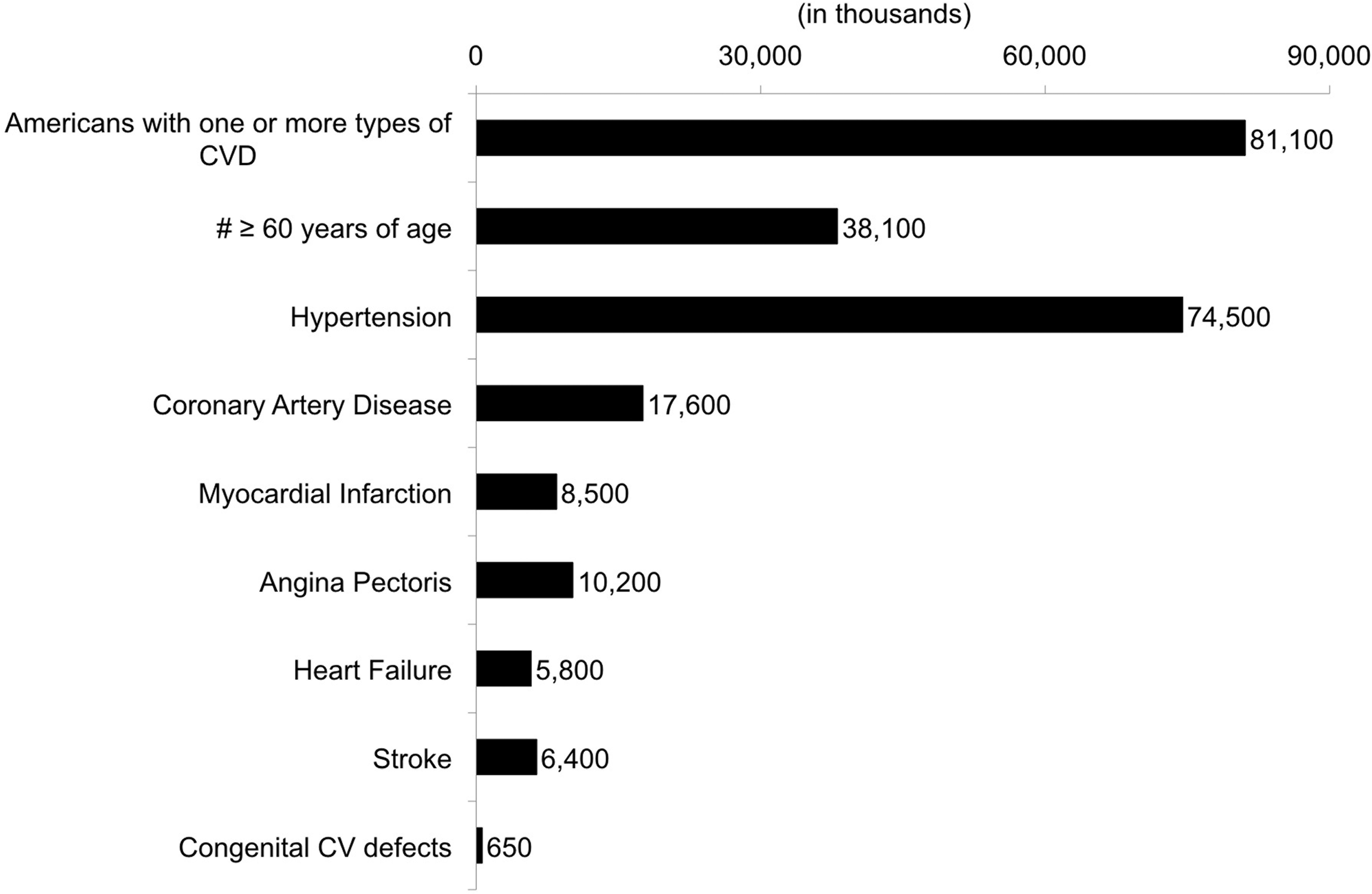
Prevalence of cardiovascular disease in the U.S. (2006). Prevalence is an estimate of how many people have a disease at a particular point in time. Data on the prevalence of cardiovascular disease in the U.S. was based on 2010 update of the Heart Disease and Stroke Statistics of the American Heart Association. 1 The data is based on the National Health and Nutrition Examination Survey and includes data collected from 2003 to 2006 against 2006 census population estimates.
U.S. prevalence of peripheral vascular disease is 5.7 million for patients older than 40 years of age representing 4.5% of the population (Table 1). This prevalence rises to 14.5% in patients older than 70 years of age; therefore, the prevalence of peripheral vascular disease might be expected to increase with the current aging of the U.S. population.
Data: Selvin and Erlinger (2004). 59
Data: Annual estimates of the resident population by sex and five-year age groups for the United States: April 1, 2000 to July 1, 2009 (NC-EST2009-01) U.S. Census Bureau Population Division, Release Date, June 2010.
ABI, ankle brachial index (The ratio of blood pressure in the lower leg over blood pressure in the arm); CI, confidence interval; PAD, peripheral vascular (arterial) disease.
The hospital discharge data from our database were used to examine the cardiovascular therapeutic targets more closely, looking at treatment incidence in hospitalized patients from 2004 to 2006. A top-level analysis comparing cardiovascular and peripheral vascular targets, as noted previously, 3 indicated that the incidence of treatments for cardiovascular disease heavily outweighed peripheral vascular targets, accounting for 96% of the regenerative therapy opportunity within the cardio/vascular space. Herein we further dissected the opportunity to understand the incidence of individual treatment targets within each major category as they relate to the different types of regenerative technologies.
Estimate of opportunity and GAP analyses by medical indication
Detailed market evaluations are often performed by analysts and potential partners when evaluating a product in the clinic; however, we contend that this information may also be vital much earlier in the translational process and should guide decisions from research goals to resource allocation and be an integral part of a company's early clinical strategy and business model development.
Vascular repair
Patch grafts and vessel replacement
Patch graft angioplasty is used to prevent stenosis and thrombosis at the site of an arteriotomy, a cut or opening in the arterial wall. A lesion that reduces the remaining arterial circumference is major indication for a patch graft. Patch grafts are currently fashioned from an autogenous vein, pericardium, or synthetics. Vascular surgeons prefer autogenous vein patches for small to medium caliber vessels, while synthetic material is used for large caliber vessels like the aorta or iliac arteries. Our estimate of opportunity analysis (EOA) analysis of patch graft procedures estimated the incidence of tissue grafts and synthetic grafts to be very similar (Fig. 2A). Clinically, there seem to be only small differences in performance between synthetic and vein grafts in carotid patch angioplasty. 28 In addition, vascular replacements, using the autogenous vein for small-caliber applications and synthetics for large caliber added another 15,000 procedures for repair of both small- and large-caliber vessels 2005–2006 (Fig. 2B). This suggests that there is a comparable need for both large- and medium- to small-caliber vessels or conduits for vascular repair.

The incidence of vascular repair. The graphs show the incidence of vascular repair in U.S. short-term stay discharged patients.
Endocardial repair
Biomaterials prostheses and conduits are also used in endocardial repair, the largest and most well-known application being valve replacement. Discussed elsewhere, 3 the EOA analysis suggests a large opportunity for valve replacement of over 50,000 procedures per year (Fig. 3A). Yet, as noted in the initial report in this series, 3 the opportunity for a substantially novel tissue valve is likely to be limited in the adult due to the clinical performance of current tissue valve alternatives. However, in pediatric applications, long-term function and growth of valve leaflets would be a distinct advantage over present alternatives. 29 Tissue grafts used for partial repair or replacement numbered close to 70,000 by 2006 (Fig. 3B).
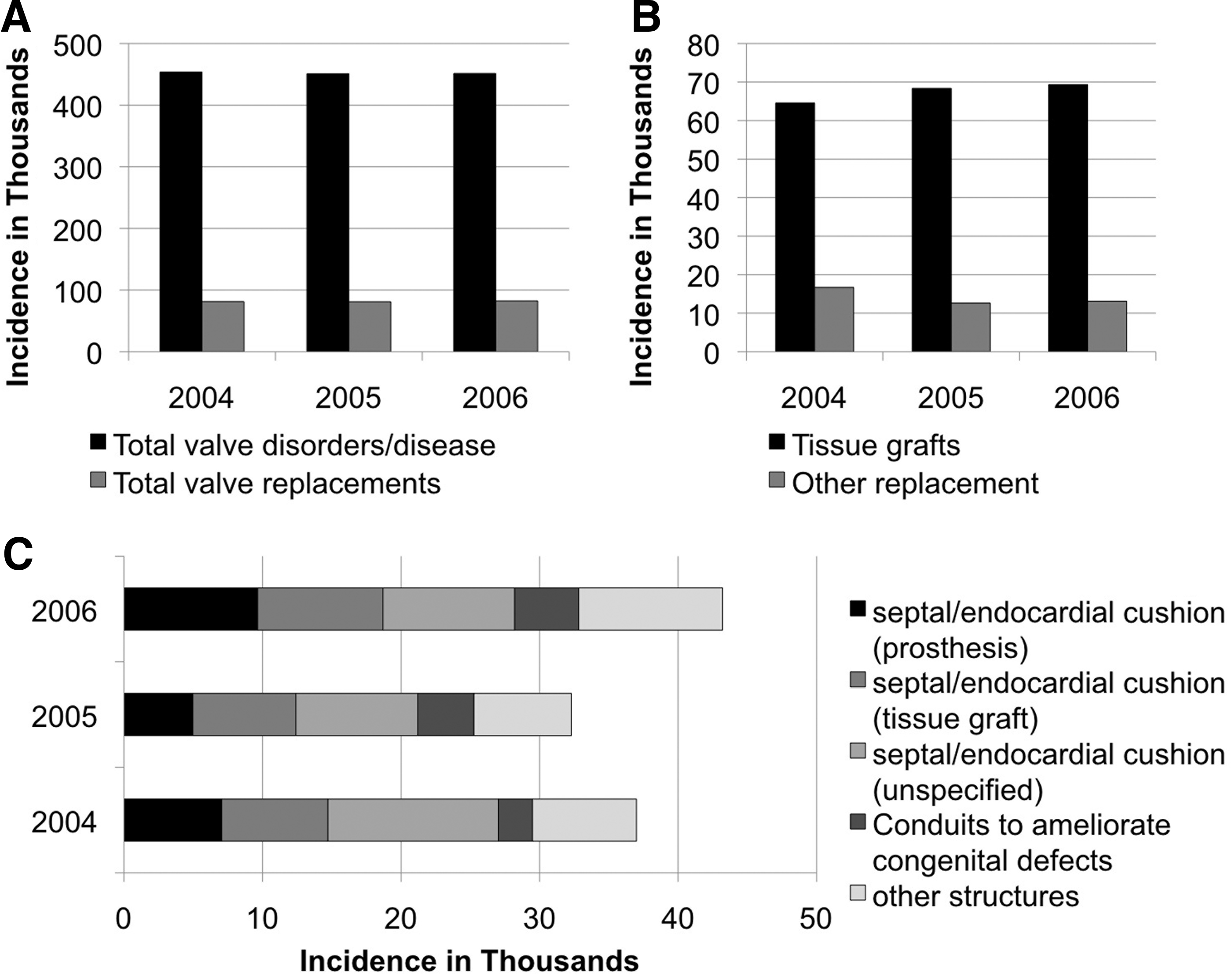
Incidence of endocardial disorders and procedures.
Additional endocardial applications, many to treat congenital defects, had a combined incidence of over 40,000 in 2006 (Fig. 3C). The use of prosthetics appears to be nearly equal to the use of tissue grafts; although the type of material is unspecified in a large number of reported septal and endocardial repairs.
Aortic aneurysm
EOA: The World Health Organization statistical data calculate death from aortic aneurysms in the U.S. to be just over 53 per 1 million people accounting for over 15,000 deaths. 30 AAA account for 9000 of these deaths. The EOA data estimate that aortic aneurysms without rupture represent a possible regenerative treatment target numbering ∼50,000 discharges per year based on primary and secondary diagnoses (Fig. 4A). In spite of the potential market, the repair of aortic aneurysms had undergone drastic transitions toward an endovascular repair that use a covered stent, these numbered just over 23,000 by 2006 (Fig. 4B). There is a large difference between the incidence and repair of aortic aneurysms. This is largely due to the threshold for repair when the benefit exceeds the risk of the aneurysm repair. For this reason, most patients are observed until the aneurysm attains a size of 5.5 cm, when rupture risk gains significance.

Aortic aneurysm diagnoses and procedures. Aortic aneurysm repair is an opportunity for device intervention, but a traditional medical device employing a biomaterial is likely to remain the method of choice.
Of importance, repair of AAA less than 5.5 cm in diameter has not led to improvements in mortality compared to a waiting surveillance program. 31
GAP: Currently, the most advanced technology for repair is a minimally invasive procedure using an endovascular stent graft that is composed of a deployed stent with a polytetrafluoroethylene (PTFE) or Dacron lining introduced through the femoral artery (e.g., Medtronic AneuRx®, or Gore). Endovascular procedures for AAA intervention offer several near-term advantages, such as lower operative mortality (1.8% vs. 4.3%), shorter hospital stays, and decreased short-term patient morbidity. However, a large randomized trial conducted in the United Kingdom compared open versus endovascular repair and found no long-term differences in total and aneurysm-related mortality. 2 Endovascular repair resulted in three to four times higher rates of graft-related complications and re-interventions compared to open repair even after 4 years. This translated to a higher overall cost associated with use of the endovascular prosthesis with a mean cost of aneurysm-related admissions totaling over $4,568 more (total costs $23,153 compared to $18,586) during an 8-year follow-up period with costs of primary and later graft-related admissions contributing almost equally to this difference. A systematic review by Jonk et al. concluded that endovascular repair of AAA was not cost-effective regardless of the health status of the patient. 32 This suggests that next-generation prosthesis should be endovascular and ideally reduce the incidence of complications and re-intervention over time.
Apart from simply competing as an alternative conduit, what could a regenerative alternative offer over PTFE and Dacron? Because a biological graft would remodel, better integration of aorta and graft might be a possibility, but given the older target patient population, it also means that reliance on tissue remodeling in this patient population may be challenging, and the durability compared to synthetics may be questioned. Because most complications involve the patient anatomy (proximity to vessels of the bowel and kidneys, for example), a biological graft would not offer an advantage over synthetics with respect to prevention of complications or degeneration of the adjacent aorta. Since reoperation is fraught with high risk, safety, reliability, and durability would be paramount. For these reasons, we conclude that in aortic aneurysm repair, there is no prominent medical need that a regenerative implant could reasonably address and although a theoretical target for regenerative therapy, it is unlikely to be a feasible medical or commercial target.
Vascular access
EOA: Vascular access is a means of achieving a high-volume blood flow for the purpose of hemodialysis in patients with renal failure. This high flow needs to be easily accessed by a dialysis nurse with a needle stick, provide high flow to operate the dialysis unit, and yet, minimize infection risk. While a long-term catheter provides a degree of convenience, these devices are plagued by risks of infection, occlusion, and long-term damage to vessels within the chest. For this reason, catheters are actively discouraged in favor of surgical vascular access. The gold standard for surgical vascular access is an arteriovenous (AV) fistula created with connection of an artery and a vein.
AV fistula procedures and associated repairs represented only 14% of the large hospitalized hemodialysis patient population between 2004 and 2006 (data not shown). The majority of the vascular access procedures are performed on an outpatient basis. For this reason, the analysis was performed using data tracked from a large network of U.S. institutions and reported on a monthly basis by FistulaFirst.org. 33 While there is a high incidence of venous catheterization (not shown), catheterization extending to 90 days and beyond is discouraged and infrequent (Fig. 5A) and patients with chronic kidney disease will require vascular access beyond catheterization. The creation of an AV fistula is the first medical choice.34,35 AV fistulas are the preferred methods of hemodialysis access mandated by the Centers for Medicare and Medicaid services 34 and recommended by the KDOQI 36 guidelines for care of the dialysis patient. Despite these guidelines, a large number of patients do not have adequate vein for successful creation of a mature fistula necessary for hemodialysis. An appropriately designed biologic alternative may reduce the complications associated with prosthetic grafts currently used when adequate vein is not available.

Prevalence and incidence of U.S. vascular access procedures. Data on vascular access procedures were obtained from Fistula First.org,
14
which tracks vascular access procedures from a large U.S. network of institutions on a monthly basis.
While the use of AV fistulas is steadily increasing, the creation of fistulas at nearly twice that frequency highlights the failure of many fistulas to reach a state where they can be used clinically (Fig. 5B). There is a smaller, but persistent use of AV grafts (Fig. 5). The changes in prevalence year-to-year between AV fistulas and grafts appear to mirror each other suggesting that AV grafts and AV fistulas continue to compete in a certain segment of the patient population (Fig. 5A). The data suggests that there is an opportunity for a regenerative alternative both in the current AV fistula population and would otherwise receive an AV graft.
While peripheral bypass grafting is attractive from a market standpoint, the complications from potential graft failure are substantial and the margin to exceed performance of currently used autogenous vein is narrow. In contrast, an AV fistula presents advantages both from a production standpoint as the graft lengths are shorter, but also may present less immediate complications to the patient in the event of graft failure.
Our EOA and gap analyses suggest that a biological conduit or graft would compete with expanded PTFE (ePTFE) in an initial patient population of just over 50,000 individuals per year if one includes revisions and replacements.
GAP: Currently, when adequate vein is not available, the need for AV grafts is met with synthetic grafts like ePTFE (normally 6–8 mm in diameter) or the lesser used biological alternative, which is, processed bovine conduits. Both ePTFE and bovine grafts have high short-term patency rates even though endothelialization extends only 1–2 cm beyond the anastomoses and there is little transluminal endothelialization observed in humans. 37 This feature may explain, in part, the poor long-term patency of ePTFE and bovine grafts. Both grafts suffer from structural integrity issues, PTFE develops mechanical failure with development of pseudoaneurysm at sites of repeated puncture, while biologic grafts have been noted with frequent formation of aneurysm formation. PTFE also carries lifelong risks for infection, a feature that is far less common among biologic alternatives, such as vein. Professional and hospital services are estimated at $11,477 for AV graft surgery 38 and a total of $20,792 for all inpatient services. 39 In 2006, yearly patient costs were $71,616 for patients with grafts versus $59,347 for AV fistulas. Hemodialysis access costs were highest for grafts at $7,377 compared to only $3,284 for AV fistulas. In summary, prosthetic AV graft materials carry a higher complication rate and annual cost compared to vein; thus, for patients in whom vein is not available, there is a niche for regenerative conduits that may overcome some of these obstacles. A problem common to all forms of dialysis access is the development of scar tissue at the junction with the host vessel, known as intimal hyperplasia. The compliance mismatch of PTFE, in particular, is believed to accelerate this process. This disease is so problematic, in fact, that an average vascular access has an average longevity of under 18 months, obligating many of these patients to repeat procedures.
These features suggest that a superior engineered graft will be one that can seamlessly integrate with the host vessels permitting repair, while limiting the hyperplastic reaction at the anastomoses. An ideal engineered graft would also be one with a more favorable compliance mismatch than currently available prosthetic grafts. It will also maintain a durable artery-like vessel that can endure repeated access without primary wall degeneration. It is conceivable that physical or pharmacologic design features may someday limit the intimal hyperplasia. The lengths needed for vascular access range from ≥20 to 40 cm; therefore, production issues for vascular access become more manageable than for long peripheral artery bypass grafts. It should be noted that current hemodialysis access costs for a graft is currently under $8,000. The GAP for vascular access is summarized in Table 2.
AV, arteriovenous.
Peripheral vascular disease
Surgical intervention
EOA: Peripheral vascular (arterial) disease (PAD) is due to atherosclerosis of the peripheral vessels. While several biologics and stem cell therapies have been advocated to stimulate a more robust microvascular network, these are unlikely to achieve clinical goals of limb salvage when macrovascular disease is present. In those instances, a long peripheral bypass will still be required. There are two primary categories of arterial insufficiency that merit discussion as they have an impact on clinical need for regenerative products. Patients with mild to moderate arterial insufficiency who have pain after walking certain distances carry a diagnosis of claudication. The mainstay of therapy includes lifestyle modification, such as smoking cessation and an exercise program. With this approach, most patients achieve their lifestyle goals without any intervention. In fact, the risk of amputation among these patients is quite low, under 5% at 5 years. It is for this reason that the perioperative risk (myocardial infarction, graft failure, infection, and wound complications) has widely discouraged invasive intervention among these patients. It remains unlikely that these patients will represent a meaningful population for engineered grafts, although biologic and stem cell therapies potentially would have a more favorable risk to benefit profile in this population. In contrast, patients with critical limb ischemia (CLI) have a far more advanced, often multilevel, arterial disease. These patients have rest pain symptoms that are constant and unremitting or may have nonhealing wounds or gangrene. The risk of limb loss is high among these patients. The long length of vein necessary for bypass and the likelihood that these patients may have had a previous harvest of vein for a cardiac bypass or bypass of the other lower extremity is high. The use of prosthetic bypass grafts for long leg bypass has dismal outcomes and for these reasons, patients with CLI represent a broad niche for an engineered bypass.
Importantly, not all CLI patients are candidates for bypass due to unavailability of outflow in the form of small vessels in the foot required to keep a bypass open. Therapies that would increase microvascularization of the tissue are considered to have theoretical potential for this patient population. 40 While endovascular options may present an alternative for many patients with PAD, there continues to be an ongoing need for open bypass due to superior durability and utility for extensive disease compared to most endovascular options.
Hospitalizations with a diagnosis of PAD with gangrene numbered nearly 50,000 patients per year suggesting that a significant medical need exists for more aggressive intervention to limit progression of CLI to this stage. The autogenous saphenous vein is the gold standard for peripheral bypass; however, about 30% of patients needing a below the knee revascularization procedure have inadequate saphenous vein for grafting. This number increases to 50% for those undergoing secondary procedures, 40 a population, where an engineered biological graft would be especially valuable. CLI symptoms of rest pain, ulceration, and gangrene combined for a total of up to 83,000 primary and secondary diagnoses in a single year (Fig. 6A). Of those, two-thirds or just over 55,000 CLI patients may be candidates for vascular surgery and nearly 28,000 nonsurgical candidates might be helped by cell therapy. Peripheral vascular grafts and bypass grafts numbered from over 66,000 in 2004 to just over 54,000 in 2006 confirming our estimates based on diagnosis (Fig. 6B). The decrease in grafts and bypass grafts from 2004 to 2006 were offset by an increase in the use of peripheral artery stents. PAD represents a substantial opportunity for both cell-based regeneration of the microvasculature and vascular grafting in different, but overlapping patient populations. The autogenous saphenous vein is the current gold standard in peripheral bypass grafting although there is opportunity for a regenerative graft to improve on saphenous vein in availability, reduced morbidity, and importantly, toward limiting intimal hyperplasia, one of the most troublesome causes of failure among vascular bypasses.
Dissection of the cardiac bypass medical need and opportunity.
GAP: Synthetic grafts are used in CLI when there is no alternative option, including other autogenous vessels. First generation PTFE grafts had inferior long-term patency compared to the saphenous vein, particularly below the knee; 37 new heparin-bonded prosthetic grafts are debatable with regard to improved patency, if any. We conclude from the GAP that a biological bypass graft should ideally narrow that performance gap in below the knee procedures. It would ideally be off-the-shelf as patients with CLI have the highest risk of amputation, and delay in prompt treatment can rapidly lead to infection, gangrene, and limb loss. Market penetration will also be challenged by increased use of endovascular procedures and improvements in the drug-eluting stent and balloon technologies, 41 although the use of such stents is limited and relatively undefined in many cases of CLI. The GAP for a peripheral bypass graft is summarized in Table 3.
Therapeutic angiogenesis
GAP: Cell therapies for tissue ischemia can act in two ways: (1) through proangiogenic signaling that acts in a paracrine manner to promote or prolong an angiogenic response in the host and (2) by directly contributing to the advance and/or stabilization of the microvascular network through the addition of endothelial cell precursors or supporting pericytes, for example. Angiogenesis is essentially regeneration of the microvasculature.
A growth factor or cell-based therapy could, in theory, increase the microvascular network and collateral circulation. Such technologies may have greatest utility in some chronic wounds, where the macrovascular system is functional, but the local microvascular supply may be impaired. In the context of claudication, symptoms of intermittent pain without ulcers or gangrene, lifestyle modification, such as exercise and smoking cessation will remain centerpieces of treatment. While bypass carries a higher risk to benefit profile and is considered inappropriate for the vast majority of claudication patients, injected or cell-based therapy may offer symptom relief, while presenting minimal risk to the patient. In the treatment of CLI, the critical nature of the disease and the lack of surgical options for a third or more of the patient population create a greater need for a regenerative therapy to augment nonsurgical options. A cell therapy will likely be used in conjunction with therapies, such as bypass rather than as an alternative in CLI. The GAP for regenerative therapy for PAD is summarized in Table 3.
Cardiovascular
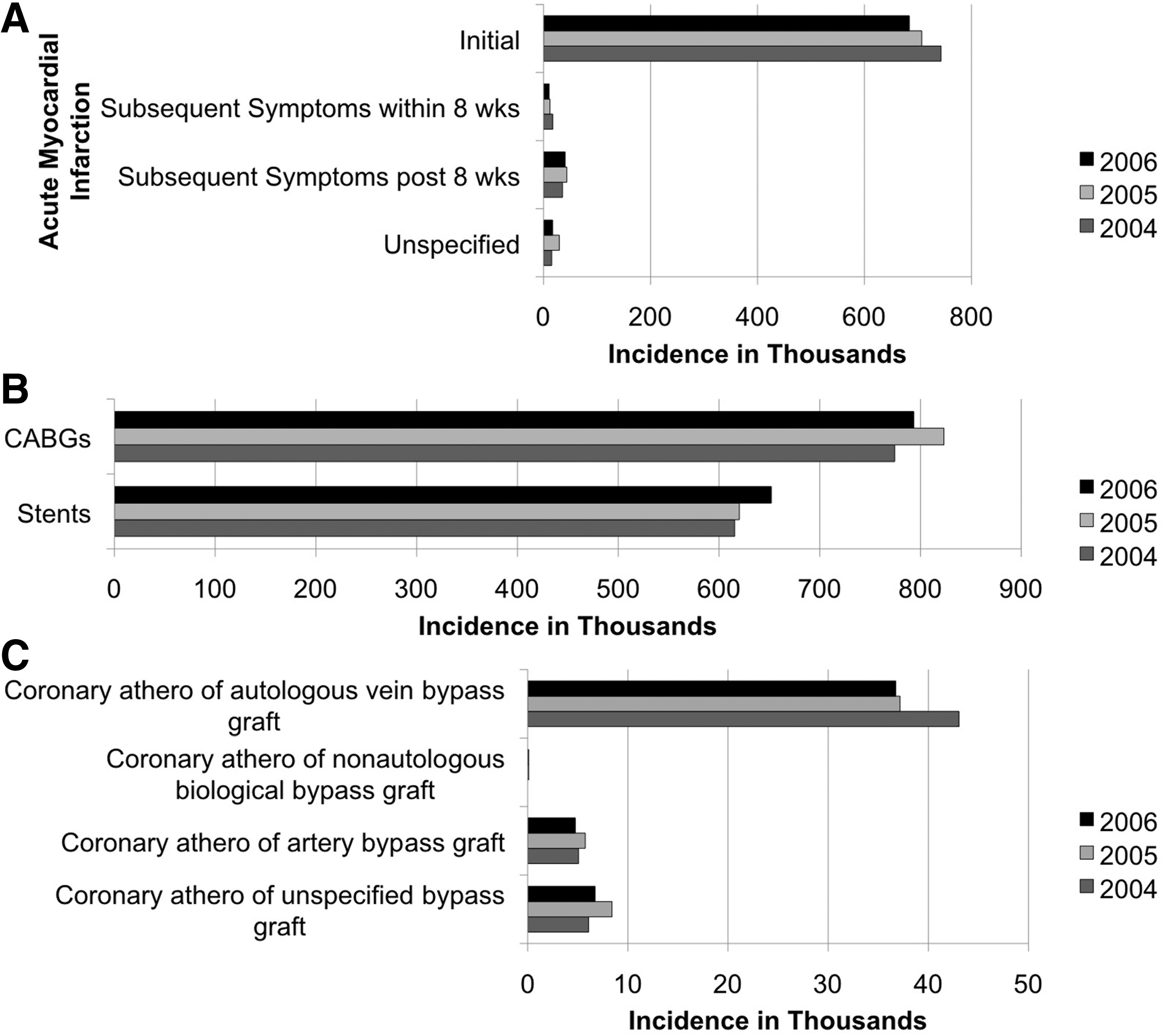
EOA: Coronary artery bypass is the first indication that comes to mind for vascular grafting. AMI, for which coronary bypass grafts (CABG) is primarily used for, had a high initial incidence of 684,000–743,000 discharges from 2004 to 2006 based on primary and secondary diagnoses (Fig. 7A). Looking at the type of procedures used to treat AMI, CABG still outnumbered the use of stents between 2004 and 2006 reaching a high of ≥823,278 grafts in 2005* (Fig. 7B). Of particular interest to regenerative medicine, is the incidence of recurrent atherosclerosis in the CABG, which could necessitate regrafting (Fig. 7C). It is estimated that 33% of patients undergoing coronary bypass will require one or more regrafts. 42 The incidence of coronary atherosclerosis of autogenous veins outweighed the incidence of atherosclerosis in artery bypass grafts. How much of this is due to the predominant use of autogenous vein in CABG was not discernable from the EOA data. However, the incidence data mirror clinical findings that 10-year patency rates for saphenous vein grafts are 61% versus 85% for internal mammary artery grafts, 43 although not all artery grafts may perform equally well. A recent clinical study found no difference in patency rates between saphenous vein grafts and radial artery grafts harvested from the arm at 1 year with the radial artery grafts having a higher associated morbidity and cost of harvest. 44

The medical need in peripheral artery disease.
GAP: AMI is the second most prevalent cardiovascular disorder after congestive heart failure (Fig. 8). Four hundred forty-eight thousand inpatient bypass procedures were performed in 2006. 1 Using data from the EOA analysis, it was clear that treatment of acute AMI has a high success rate (Fig. 9) with 97% of all hospitalized cardiovascular disease patients discharged alive, 70% to home. Pooled Framingham Heart Study, Atherosclerosis Risk in Communities Study, and Cardiovascular Health Study data from the National Heart, Lung and Blood Institute estimate that within 5 years after first myocardial infarction, 33% of men and 43% of women ≥40 years of age will die, 16% of men and 22% of women aged 40–69 will suffer a recurrent myocardial infarction or fatal coronary heart disease, and 7% of men and 12% of women will develop heart failure within 5 years. 1 The incidence of atherosclerosis in a bypass graft was ∼51,000 per year between 2004 and 2006 (Fig. 7). By excluding patients treated with bypass, we calculate that ∼150,000 AMI patients (25% of AMI patients) were treated with stents rather than bypass. Assuming that the frequency of endovascular intervention will be similar to interventions for the initial AMI, this leaves 38,250 of patients with atherosclerosis of their bypass grafts as candidates for re-graft. As stents continue to improve, this proportion may decrease further. A review of the literature reveals that autogenous arteries and veins will still be the first choice for re-graft whenever possible and that autogenous vessels can be harvested even for patients undergoing their third CABG procedure, 42 likely due to the short length needed for these procedures. Given the track record of bypass procedures and the morbidity associated with vessel harvest, the barrier to adoption of an engineered vessel is likely to still be high. Unlike CLI, failure of a CABG graft can have immediate life-threatening impact 45 and the extensive experience with successful CABG grafting 43 will make it hard to justify the use of an alternative unless absolutely necessary. Furthermore, the patient population who may need engineered conduit alternatives will be limited to a percentage of regraft patients lacking available autogenous artery and vein options. Over time, advantages in lower patient morbidity from avoiding vessel harvest will be an advantage, but we believe it is unlikely to be a key driver in the decision to use an autogenous alternative without substantial long-term data and clinical experience. Supporting data could come from use of a regenerative graft in peripheral bypass contexts, although there remain key differences in the requirements of and techniques used by peripheral vascular and cardiac surgeons. For these reasons, while the market is potentially large, there may be several initial barriers to adoption of engineered alternatives to CABG. The comparison of the vascular graft opportunities with findings of the GAP factored in is summarized in Table 4.
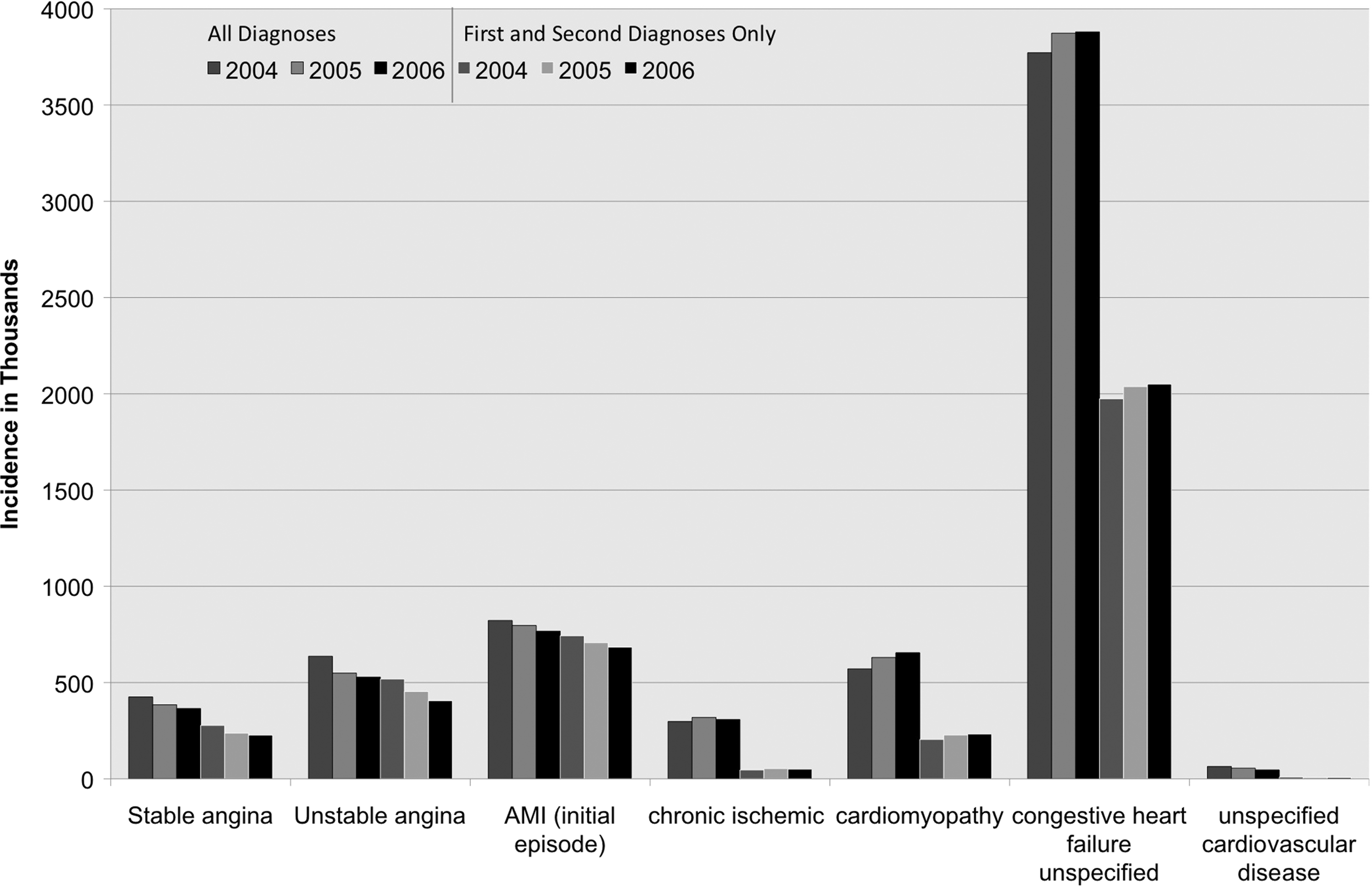
The medical need in cardiovascular disease (all diagnoses vs. primary and secondary diagnoses). Comparison of primary and secondary reported incidence versus all reporting estimates, both the current and unmet need in hospitalized patients with cardiovascular disorders over a 3-year period. Congestive heart failure substantially outweighed all other cardiovascular disorders in the hospitalized patient population.
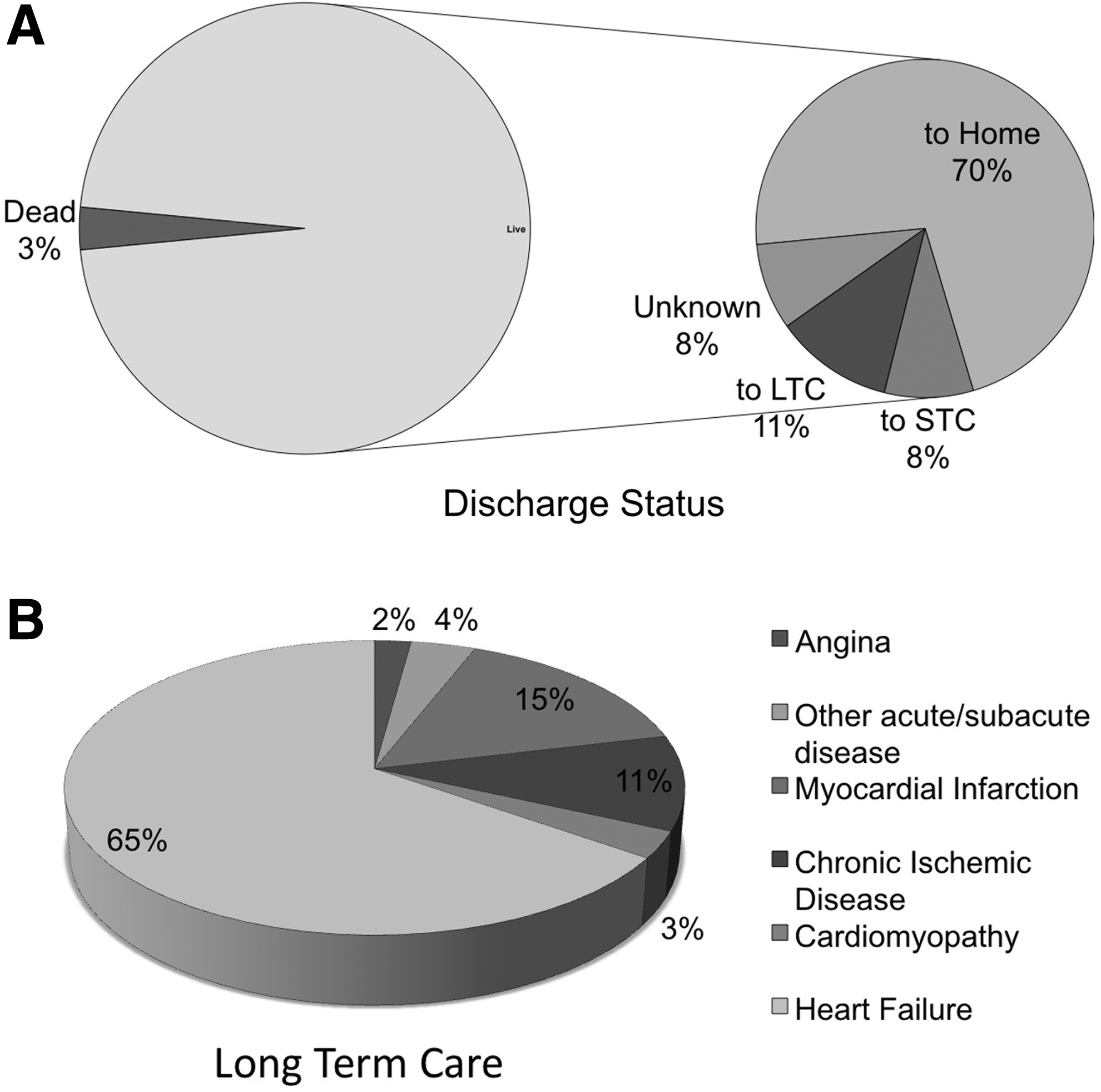
Medical need in cardiovascular disease discharge status in all cardiac disease.
AMI, acute myocardial infarction; CABG, coronary bypass grafts.
Heart failure
EOA: The data suggest that current management does well in saving the lives of patients with AMI due to ischemia, but the longer term impact of cardiac damage appears to be another matter. Heart failure is the largest opportunity within the cardio/vascular space (Fig. 8). Of the cardiac patients discharged to long-term care, 65% of them have heart failure (Fig. 9). Since heart failure is simply managed medically for many patients, we compared primary and secondary diagnoses to all listed diagnoses to get a sense of how many individuals hospitalized each year had heart failure. EOA analysis comparing primary and secondary diagnoses versus all diagnoses revealed that a large number of heart failure patients are hospitalized each year (Fig. 8). Early-stage treatment post AMI represents a population of about 70,000 to just over 80,000 hospitalized patients per year. In comparison, diagnoses of congestive heart failure reach ∼2 million discharges based on primary and secondary diagnoses and expand to nearly 4 million patients if one takes into account all hospitalized patients with a diagnosis of congestive heart failure (Fig. 8). It is clear from the incidence data that early regenerative treatments to improve cardiac perfusion and/or function should ideally tackle the primary unmet medical need by intervening to limit the progression to heart failure and/or by restoring cardiac function.
Cardiac ischemia
GAP: It is reasonable to anticipate that treatment of microvascular cardiac ischemia will be mechanistically similar to the treatment of PAD. A cell therapy might be introduced in a transvascular procedure, injection into the circulation or injection into the myocardium at the time of a cardiac catheterization or endovascular procedure to treat angina symptoms. Post AMI, cell therapy may be introduced into the site of infarct to promote optimal healing of the cardiac wall. Animal and human studies to date suggest that cell therapy can exert a positive effect on left ventricular function and limit the extent of scarring although reviews of the clinical data to date46–49 have confirmed that the results are variable and improvements modest though the procedures are safe. Other procedures exist and, for example, treatment to promote transmyocardial and other revascularization procedures approached 5000 procedures in 2006. 3 Of note is that while medical therapy can reduce the risk of heart failure in asymptomatic patients with left ventricular dysfunction, only a small difference is observed in mortality between patients managed in a preventative versus a therapeutic approach for heart failure. 50 For these reasons, more aggressive interventions may be warranted.
The majority of clinical studies to date have examined the infusion of bone marrow stem cells into the heart as an approach to restoring lost function. The durability of the differences in healing and function is unclear and the mechanism of action is also unclear 51 although promotion of angiogenesis, limiting inflammation, and promoting the regenerative phase are all possibilities. Further evidence of the mechanism of action for these therapies is still needed. The GAP for regenerative therapy for cardiac ischemia is summarized in Table 4.
Cardiomyopathy
GAP: AMI is not the only cause of heart failure and, in fact, can be caused by viral infection, hypertension, valve dysfunction, and renal failure. 52 Similar to the use of cell therapy to improve microvascularization, the primary gap at present is in determining and optimizing the mechanism of action and delivery approach for these therapies. Defining cell sourcing and integration of injected cells into cardiac tissues will be other considerations. The GAP for regenerative therapy to reverse heart failure is summarized in Table 5. An effective therapy for heart failure is a clear medical need with limited alternative treatments.53,54 Currently, a multi-disciplinary approach to management of heart failure appears to be most effective.53,55–57 Early intervention may present advantages by prevention of clinical heart failure, both to the patient and the resources of the medical system in general. Again, much work remains to define the best cells or factors to achieve this goal. To date, the absence of scientific data on mechanism(s) of action is still a significant gap standing in the way of a regenerative therapy to halt progression to heart failure.49,58 Cells from different source may not be equally effective at all stages, 25 the same will be true for regenerative factors. Although these therapies remain in their infancy, the market size and medical need justify the continued effort and investment. It seems inevitable at this point that regenerative products will become as important to cardiac patients as currently used angioplasty, medical therapy, and surgery.
LVEF, left ventricular ejection fraction.
Summary
Although generalized projections may identify high-yield areas for clinical products, more detailed information of the potential barriers to clinical adoption of new technologies is necessary. The results of our analysis dispel some long-held assumptions regarding paths to the marketplace and confirm the translational importance of performing a GAP that incorporates a realistic EOA for each application of a technology. To summarize our findings:
(1) The opportunity for biological patch grafts and vessel replacements is modest at around 15,000 procedures per year. The gap in medical need is small compared to other cardio/vascular indications. (2) AAA repair represents ∼20,000 procedures per year. However, the long track record of current technologies and competing endovascular technologies make this area an unlikely commercial target for regenerative technologies. (3) Vascular access offers one of the best opportunities for a tissue-engineered vascular graft. At minimum, such a graft would serve as an alternative to current AV grafts (over 30,000 per year), if a regenerative conduit could compete competitively with the current gold standard of autogenous vein (also around 30,000 per year). (4) Extensive surgical experience make CABG a difficult indication of a tissue- engineered vascular graft. Despite a large initial CABG population, regraft procedures will likely face increasing competition from endovascular innovations in a patient population of just over 30,000 per year. The CABG indication will likely require supporting data from other vascular indications to be approachable clinically and commercially. (5) PAD (nonaortic) represents over 60,000 procedures per year now treated using a graft, bypass, or endovascular procedures. PAD patients with intermittent claudication (over 35,000 in 2006) represent an opportunity for cellular therapy, but not likely surgical grafts. Critical limb ischemia (CLI) represented over 90,000 primary and secondary diagnoses. Subpopulations of CLI patients are candidates for both cellular therapy and vascular bypass grafting. An engineered vascular graft could offer several clinical benefits over native vessels in availability, consistency, reduced morbidity, and extent of intimal hyperplasia. Advances in endovascular approaches to PAD will reduce some of the potential in the area, but is unlikely to completely replace open surgical bypass among patient with extensive disease. (6) Heart failure is the single largest treatment opportunity for regenerative medicine at ∼2 million discharges based on primary and secondary diagnoses and close to 4 million patients if one includes all patients hospitalized with a diagnosis of congestive heart failure. Cellular or biological therapy to treat ischemic heart disease should ideally impact the progression to heart failure and yield results superior to current standards of care.
We believe that this information will help guide new regenerative technologies to the areas of greatest clinical need.
Footnotes
Disclosure Statement
No competing financial interests exist.
*
CABG procedures involving more than four bypass grafts are coded the same as quadruple bypass.