
Abstract
Bisphosphonates (BPs) are a group of well-established drugs that are applied in the development of metabolic bone disorder-related therapies. There is increasing interest also in the application of BPs in the context of bone tissue engineering, which is the topic of this review, in which an extensive overview of published studies on the development and applications of BPs-based strategies for bone regeneration is provided with special focus on the rationale for the use of different BPs in three-dimensional (3D) bone tissue scaffolds. The different alternatives that are investigated to address the delivery and sustained release of these therapeutic drugs in the nearby tissues are comprehensively discussed, and the most significant published approaches on bisphosphonate-conjugated drugs in multifunctional 3D scaffolds as well as the role of BPs within coatings for the improved fixation of orthopedic implants are presented and critically evaluated. Finally, the authors' views regarding the remaining challenges in the fields and directions for future research efforts are highlighted.
Introduction
Bisphosphonates
BPs are a type of drugs that are considered stable analogs of pyrophosphate, a physiological regulator of calcification and bone resorption,8–10 in that the P-O-P bond of pyrophosphate is replaced by a P-C-P bond, which is resistant to chemical and enzymatic hydrolysis. Figure 1 shows the chemical structure of BPs in the inner circle. The R1 and R2 side chains attached to the carbon are responsible for the variation in activity observed among these drugs. 11 Substitutions in the side chains lead to the synthesis of a large number of compounds with different properties (Figure 1). It has been reported that R1 groups are responsible for the targeting and binding of BPs to bone, while R2 ones are responsible for their potency and their action on bone resorption. 12 Several studies have shown that BPs with–OH and–NH2 substitution in R1 increase their binding to bone mineral.13–15 BPs are classified into two groups: the Nitrogen-BPs (N-BPs), such as alendronate (ALN), residronate, ibandronate, pamidronate, and zoledronic acid, and the non-N-BPs, such as clodronate (CLO) and etidronate (Fig. 1). The classification of BPs into two groups is also according to their different mechanisms of action. The N-BPs act on the cholesterol pathway by inhibiting diphosphate synthase in the mevalonate pathway,16,17 while the non-N-BPs are metabolically transformed into cytotoxic ATP analogs that inhibit ATP-dependent intracellular enzymes. 18 Various BPs have already been used for the clinical treatment of Paget's disease, osteoporosis, hyperkalaemia of malignancy, osteogenesis imperfect, and inflammation-related bone loss, to promote fracture repair.5–7,19–24 The clinical pharmacology of BPs revealed that their affinity to bone mineral hydroxyapatite (HA) is the basis for their use as inhibitors of ectopic calcification and bone resorption. 10 Substantial literature regarding the pharmacodynamics of BPs also reporting on clinical results is available.25–28 All BPs are characterized by their low bioavailability via oral administration and their associated side effects as well as adverse reactions related with parenteral administration.10,30 Since 2003, many publications have reported an association between bisphosphonate therapy and osteonecrosis of the jaws.166–172 Most precisely, a correlation between the types of bisphosphonate, the period of the treatment, and the occurrence and gravity of osteonecrosis of the jaws has been proposed. 167 Most of the reported cases corresponded to intravenous therapy with high doses of amino-group-containing BPs such as zoledronic acid or pamidronate for malignant disease. In addition, a few cases of osteonecrosis of the jaws corresponded to long-term oral administration of nonaminogroup-containing BPs. 167 The mechanism behind this osteonecrosis of the jaws remains unclear. It can be speculated that with comparatively much lower doses of BP locally released—only in the required area and for a short period of time—none of the side effects just mentioned should be observed. BPs administration in situ, by mean of a drug delivery system, has the potential to obtain high specific bone response and optimal bioavailability, as bone targeting will concentrate the therapeutic agent at the desired site of activity. Nevertheless, it is important to highlight the importance of taking these effects into account during the evaluation of any new system of controlled local release of BP. During the last decade, several studies that are related to the development of delivery systems for the controlled release of BP have been published.7,29,31–41 Smart methods of local drug delivery systems could increase the drug activity and specificity by concentrating the release of BP to bone sites and could reduce side effects at extra-skeletal sites. For those interested in further reading, a recent review summarizes the latest advances in the application of BPs for in situ orthopedic medication and treatments. 29

This figure shows the chemical structure of bisphosphonates (BPs) (centre), the classification of BPs, and the mechanism of action depending on the classification group (sides), their physiological (top) and physicochemical (bottom, right) effects in bone tissue, as well as BPs' therapeutic applications (bottom, left).10,16–18,48–50,57–59 Color images available online at www.liebertonline.com/teb
BPs role in bone tissue
The bone is an essential tissue that provides protection, support, and storage of calcium and other trace inorganics ions as well as a site for production of white blood cells for the body. This mineralized tissue contains cell types of osteoblasts (bone matrix-producing cells), osteocytes (mature osteoblasts that are embedded in the mineralized matrix), osteoclasts (bone matrix-degrading cells), and osteoprogenitors (immature cells that are capable of differentiating into osteoblasts which are found in the bone marrow and periosteum). Trabecular bone (or cancelous bone) constitutes 20% of the total adult bone tissue and has a spongy branch-like structure of trabeculae, with a porosity of 50%–90%.42–44 Cortical (or compact) bone comprises the final 80% of adult bone tissue; it is denser than trabecular bone with only 10% porosity, this makes it much more resistant to mechanical forces. The bone is a specialized connective tissue that is made up of fibrous (collagen I) and solid components (HA crystals), making it a truly composite material with a highly hierarchical structured matrix.45,46 Collagen and HA combined in the nanoscale contribute to both the compressive strength and toughness of bone. Bone is not a static material but is constantly undergoing a state of remodeling. It secretes signaling molecules that are embedded in the matrix; when the matrix is degraded or stressed, these biomolecules are released, for example, bone morphogenic factors, which guide the remodeling process. 38 BPs are selectively taken up by osteoclasts in bone matrix containing HA and have various direct effects at the cellular level. 47 For example, BPs inhibit the recruitment and differentiation of osteoclasts precursors 48 and the resorptive activity of mature osteoclasts. 49 In addition, BPs induce apoptosis of macrophages and mature osteoclasts. 50 Furthermore, osteoclasts intercalated with BPs show morphological changes, such as a lack of the ruffled border 51 and disruption of the actin ring. 52 In addition, investigations of the molecular mechanism of the direct action of BPs on osteoclasts have shown that they are involved in inhibition of the mevalonate pathway. 53 It was reported that BPs reduce cell viability at concentrations in the range of 10−4 M.54,55 In addition, evidence has accumulated, showing that the effects of BPs on osteoclasts are indirectly mediated via osteoblasts. 56 These indirect effects on osteoclasts are likely to alter the secretion from osteoblasts of factors, such as interleukin-6, that regulate the differentiation or activation of osteoclasts.57,58 Furthermore, BPs have been shown to enhance the proliferation, differentiation, and bone-forming activity of osteoblasts directly. 59 Therefore, these studies suggest that BPs affect bone metabolism via both osteoclasts and osteoblasts.8–10,60 In bone remodeling, osteoclasts and osteoblasts work closely together, also in a spatial sense, at defined remodeling sites. Their activities are coupled: A decrease in bone resorption due to BPs leads to a reduction in bone formation to a similar degree. Thus, it was long thought that BPs would only slow down bone repair. 61 However, in bone repair, osteoblasts can work independently. A reduction in osteoclast activity can, therefore, be expected to shift the balance between formation and resorption toward increased net bone formation. During bone repair, BPs have an anti-catabolic or a net anabolic effect.24,61,62 The use of BPs delivery systems, given the cellular effects of BPs discussed in this section, opens new fields and attractive possibilities for BTE.
Bone Tissue Engineering
Multifunctional 3D scaffold: dual role as matrices and drug delivery systems
Under normal conditions, bone tissue has the capacity to regenerate itself. However, critical-size bone defects require a bone substitute that fills the defect and regenerates the damaged tissue. Even though biocompatible and resorbable 3D matrices (scaffolds) have shown capabilities to direct and promote host bone cells proliferation, the incorporation of bioactive molecules such as growth factors, cytokines and hormones, and/or therapeutic drugs can substantially improve the osteogenic potential of the scaffolds for the stimulation of bone regeneration and repair.3,46,63,64 Therefore, the challenge for tissue engineers is to design and develop temporary bone scaffolds with suitable mechanical properties and the capability to be resorbed in concert with the ongoing bone formation, which should be also able to incorporate bioactive molecules and/or therapeutic drugs and to deliver them to the repairing site in a controlled manner; thus, extending the scaffold's biological functionality. A variety of materials have been employed in the elaboration of 3D scaffolds for BTE, most commonly bioactive and resorbable inorganics biomaterials, including calcium phosphates (CaP) (such as HA and tricalcium phosphate), mesoporous silica, 65 bioactive glasses,46,66–72 and biodegradable polymers, both natural (e.g., collagen, chitosan, alginate) and synthetic, such as poly (D,L-lactide), poly(D,L-lactide-co-glycolide) (PLGA), and polylactide-co-glycolide copolymers.73–75 Generally, the rationale of using polymers as drug delivery vehicles is based on the hydrolytically reactive unions in their backbone, which allow the tuning of their biodegradation rate; thus, encapsulated drugs can be released as the polymer degrades. Further, composites of inorganic biomaterials and polymers are being developed in order to improve the mechanical and biological properties of scaffolds, exploiting the flexibility of the polymers and the bioactivity of bioactive glasses or CaP.69,76–92 It is expected that multifunctional scaffolds will be able to maximize the access of bioactive molecules and/or therapeutic drugs to the surrounding tissues, and to control the release of drugs or growth factors in order to sustain the desired concentration level in their specific sites for the necessary period of time to stimulate bone formation. 93 In this context, the effect of drug incorporation on the physicochemical and mechanical properties of scaffolds and the capability of releasing drugs from scaffolds in predictable and reproducible kinetics are issues to be taken into account for the design of advanced functional scaffolds. In general, changes in the mechanical properties can be caused by some chemical interaction between the constituents of the scaffold and the loaded drug (e.g., chelation), which can also modify the kinetics of the dissolution reaction of the scaffold. On the other hand, it is well known that the release of drugs from a matrix depends on several factors, such as the type of union between drug and matrix as well as the microstructure of the matrix and its mechanism of degradation. Generally speaking, the release kinetic of drugs within 3D scaffolds for tissue engineering is linked to the degradation kinetic of the scaffold (a biodegradable matrix by definition). However, most multifunctional scaffolds studied as a matrix for drug release have been shown to have rates of degradation much lower than the required rate of drug release.40,94–96 Thus, it is important to recognize that the drug release from a scaffold can be mainly controlled by the process of diffusion through it, at least during the first stages of the process. In addition, during the degradation of the scaffold, the dissolution of bioinorganic components is followed in most cases by the formation of an apatite surface layer and precipitation of HA, which will also affect the drug release kinetics. In the case of scaffolds elaborated from bioinorganic materials, it is possible to modulate the rate of scaffold degradation by varying the chemical composition, microstructure, and percentage of crystallinity.34,35,40,66 Further, it is important to highlight that the development of these complex systems for the delivery of BPs should involve first the characterization of the drug release kinetics in vitro. Subsequently, in vivo studies should assess the effectiveness of the 3D scaffold that acts as a matrix for in situ administration and controlled release of loaded BP, the conservation of scaffold bioactivity, the BP distribution zone, and the occurrence of possible undesirable effects, for example, if migration of the drug out of the region of interest occurs. Finally, clinical assays should evaluate the performance of the system. An important issue to be taken into account is the way to quantify the release of BPs from those delivery systems. Due to the lack of chromophore groups, BPs are complex molecules that are analyzed by simple techniques of quantifications, and, in many cases, a sample pretreatment is required, most commonly, derivatization as a previous step for high-performance liquid chromatography quantification. 97 Different methods that quantify BPs in biological or pharmaceuticals samples were reported in the last years, and a summary of the most common ones is presented in Table 1.
HPLC, high-performance liquid chromatography; LOD, limit of detection; LOQ, limit of quantification; RP, reverse phase; ICP, inductively coupled plasma; ELSD, evaporative light-scattering detector; CZE, capillary zone electrophoresis; GC, gas chromatography; PAM, photoacoustic microscopy; PCL, poly(ε-caprolactone).
BTE using BPs
Different strategies for the delivery and sustained release of BPs in the nearby host tissue have been investigated. Figure 2a summarizes the different strategies that incorporate BPs in scaffolds for BTE. BPs loading in CaP scaffolds was first reported to be via chemical or physical sorption on the CaP surface, which resulted in limited drug loading content and burst release on administration.32,36,129–131 The use of these techniques may produce unspecified irregular shapes and sizes of the carriers and heterogeneous drug distribution within CaP, and, thus, the release kinetics would be without control. One of the strategies very often reported is based on the chelating capacity of BPs due to their two oxygen ions from bilateral phosphonate groups; most commonly, chelation between BPs and bioactive inorganic materials has been reported (Fig. 2a, items iii-iv). Although matrices for drug delivery are usually polymers, the bioactive inorganic materials that are usually employed in BTE scaffolds such as CaP and bioactive glasses with different solubilities and chemical compositions are attractive as drug carriers as well. Most commonly, the linkage of the drug to inorganic materials is made by soaking the inorganic scaffold in a BP solution, and recent examples of this method have been published in the last few years.32,34,36,37,40,132–135 In a relevant study, Boanini et al. (2008)
132
synthesized HA nanocrystals loaded with different ALN contents (3.9, 6.2, 7.1 wt%). The in vitro evaluation showed that the presence of the BP in the composite nanocrystals produced a reduction in the number of osteoclasts of approximately 30% and an increase in osteoblastic growth and differentiation.
132
In particular, osteoblasts cultured at 6.2 wt% and 7.11 wt% content of ALN displayed an increase in the synthesis of alkaline phosphatase, osteocalcin, and type I collagen.
132
Moreover, it was shown that the dissolution rate of CaP can be modulated by modifying the percentage of crystallinity of the CaP phase, which is stable in water, and, thus, the dissolution rate is reasonably slow.
136
Thus, the modulation of the dissolution rate of CaP may enable control of the release rate of incorporated BPs.136,137 A variety of this strategy includes the development of CaP-BPs coatings over polymer scaffolds (e.g., made of starch)
138
(Fig. 2a, item v). In addition, the chelation capability between BPs and bioinorganic materials such as CaP and bioactive glasses has been utilized to prepare BP-loaded microspheres. For example, bioactive glasses were used by Välimäki et al. (2006)
133
to develop microspheres containing Zoledronate (ZOL), and CaPs were utilized for elaboration of BPs-loaded CaP microspheres.32,33,36,40,129,130 Microspheres can be conveniently used for the elaboration of scaffolds for BTE (Fig. 2a, items ii and iii

Different strategies for incorporating BPs in scaffolds for bone tissue engineering
BP, bisphosphonates; RP, reverse phase; ALN, alendronate; HA, hydroxyapatite; PCL, poly(ε-caprolactone); CLO, clodronate; PLA, Poly (L-lactic acid); PEO, polyethylene oxide; ZOL, Zoledronate; CaP, calcium phosphates; UV, ultraviolet.
Bisphosphonate-conjugated drugs in multifunctional 3D scaffolds
The strong interactions between BPs and the inorganic components of bone has led to the exploration of the benefit of associating BPs to therapeutic drugs, including radioisotopes (such as samarium-153 complexed to tetraphosphonate), anti-inflammatory and anti-neoplastic drugs, as well as bioactive molecules such as cytokines and growth factors by conjugation through a specific linkage (Fig. 2c, items i and ii), 148 thus acting as an osteotropic drug delivery system.149,150 In this context, Pignatello et al. (2009) 151 proposed a nanocarrier developed from the PLGA-ALN conjugate. ALN was bound covalently to a free-end carboxylic group of PLGA. In a second step, nanoparticles with a mean size of 200–300 nm were obtained by a classical solvent-evaporation method. The authors demonstrated in vitro that nanoparticles do not affect osteoblast and endothelial cell viability. In addition, it was shown that PLGA–ALE nanoparticles were adsorbed onto HA to a higher extent than pure PLGA nanoparticles due to the presence of ALN. Even though the prepared conjugate represents a novel biomaterial, no drug was loaded into the system. A step further was proposed by Wang et al. (2011) 152 through the development of a drug delivery system by combining composite scaffolds made up of collagen and HA (Col/HA) with bisphosphonate (2-(3-mercaptopropylsulfanyl)-wthyl-1, 1-bisphosphonic acid)-derivatized liposomes. In this case, the affinity between HA and BPs was useful for the controlled release of the drugs from BP-liposomes in Col/HA scaffolds. The Col/HA material was prepared by a freeze-drying method that yields a porous scaffold. Three different model drugs, carboxyfluorescein, doxorubicin, and lysozyme, were entrapped in liposomes; no difference was observed in drug release between BP-derivatized liposomes and free liposomes in vitro. 152 Unencapsulated drugs and drugs encapsulated in non-derivatized liposomes were seen as displaying rapid release from the scaffolds, whereas the drugs entrapped in BP liposomes showed a slower release from the Col/HA scaffolds due to the BP high-binding affinity for calcium ions in the HA structure, which enhances the adsorption of BP-liposomes onto Col/HA scaffolds. 152 Wang et al. 2011 provided a potential drug release platform that is used in bone regeneration and repair. 152 However, it would be important to determine whether the rate of HA dissolution could modify the rate of liposome release in vivo.
Role of BPs as coatings for improved fixation of orthopedic implants
Although not a “classical” tissue-engineering approach, relevant research on the use of BPs to improve the fixation of orthopedic implants is discussed in this section for completeness and for the relevance of this review to the topic. The fixation of orthopedic implants in bone relies strongly on the initial stability of the implant. When the initial stability is not achieved, then micromotions occur at the bone implant interface.153,154 Micromotions activate premature bone resorption and remodeling by osteoclasts, 155 which result in periprosthetic osteolysis and later implant migration and wear, limiting the implant longevity. 156 BPs incorporated into orthopedic implants can be used to reduce periprosthetic osteolysis at the implant/bone interface, allowing orthopedic implants to achieve a stronger primary fixation 157 by the inhibition of osteoclast action. 158 The materials that are most widely used to fabricate implants for bone therapy are Titanium (Ti) and Ti alloys.60,131,158–164 Several strategies have been developed to incorporate BPs onto the surface of titanium implants (Fig. 3). Surface modifications with CaPs were reported as being very attractive, because BPs have a marked affinity to these substances as explained in previous sections. 159 CaPs, most commonly HA, have been used to generate thin coatings on the surface of titanium implants.60,131,159,158,160,161,165 The most common strategy that produces the chemical association of BPs with the CaPs coating is by soaking the implants in a BPs solution (Fig. 3) 60,131,158–164 Other strategies that produce the chemical association of BPs with CaPs reported include bisphosphonate adsorption onto plasma-sprayed HA and simulated body fluid-grown HA coatings that are commonly used for orthopedic implants.131,158,164 Table 3 summarizes different methods for titanium surface modification that have been used for BPs fixation.
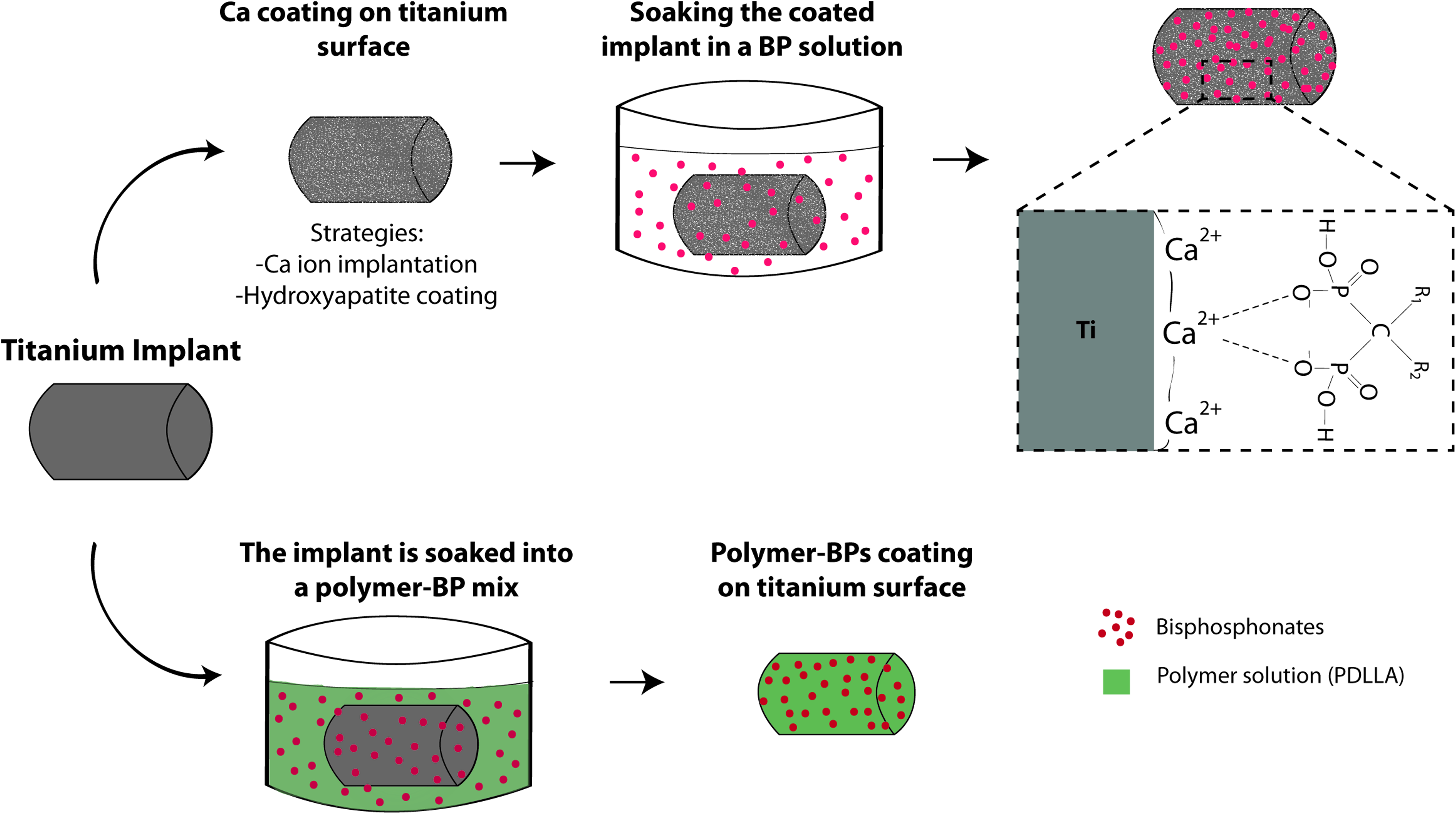
Different strategies employed for binding BPs to coated titanium.60,131,158–164 Color images available online at www.liebertonline.com/teb
Conclusions
Research carried out in the past decade has put in evidence the great potential of incorporating BPs in multifunctional scaffolds for bone regeneration applications. Especially encouraging are the results obtained with composite 3D scaffolds for BTE. The technologies and strategies summarized and discussed here represent significant progress achieved toward the development of multifunctional scaffolds with the added value of the controlled release of BPs at the desire site, thus enhancing the scaffold potential performance in vivo. However, and despite several obstacles already overcome by the research, there is still a significant gap that should be bridged to meet the complex requirements for effective bone regeneration in vivo. Among the issues to be addressed, it is important to highlight the difficulties of achieving controlled release rates, avoiding initial burst release, and the important lessons to be learned from the need to improve drug loading on scaffolds, especially when the matrix is made of bioactive inorganic materials. In this context, it is essential to know how the BPs release kinetics is affected by the variable resorption rate of the scaffold and by the morphological changes caused during its degradation in vitro and in vivo, in particular, considering the in-situ formation of an HA layer on the surface of bioactive inorganic scaffolds. Other issues include the need to be certain about the specific amount of BP that is needed to be released from the system, also taking into account the physiological constant clearance of the drug from the microenvironment in in vivo situations and also the effect of new vascularization induced by the presence of the scaffold. In addition, for successful clinical and commercial development, considerations should also be given to the ability to cost effectively manufacture the delivery system and to obtain approval from the appropriate regulatory authorities. These last two important requirements are often overlooked.
Footnotes
Acknowledgment
This work was supported by ANCyT (grant PICT 0138).
Disclosure Statement
No competing financial interests exist.