
Abstract
Bone loss in the oral and maxillofacial region caused by trauma, tumors, congenital disorders, or degenerative diseases is a health care problem worldwide. To restore (reconstruct) these bone defects, human or animal bone grafts or alloplastic (synthetic) materials have been used. However, several disadvantages are associated with bone graft transplantation, such as limited bone volume, donor-site morbidity, surgical and immune rejection risks, and lack of osseo-integration. Bone tissue engineering is emerging as a valid alternative to treat bone defects allowing the regeneration of lost bony tissue, thereby recovering its functionality. During the last decades, the increasing aged population worldwide has also raised the prevalence of maxillary atrophy. Maxillary sinus floor elevation (MSFE) has become a standard surgical procedure to overcome the reduced amount of bone, thus enabling the placement of dental implants. MSFE aims to increase the bone height in the posterior maxilla, by elevating the Schneiderian membrane and placing the graft material into the surgically created space in the maxillary sinus floor. Importantly, oral bone regeneration during MSFE offers a unique human clinical model in which new cell-based bone tissue engineering applications might be investigated, since biopsies can be taken after MSFE before a dental implant placement and analyzed at the cellular level. New approaches in oral bone regeneration are focusing on cells, growth factors, and biomaterials. Recently, adipose tissue has become interesting as an abundant source of mesenchymal stem cells, which might be applied immediately after isolation to the patient allowing a one-step surgical procedure, thereby avoiding expensive cell culture procedures and another surgical operation. In this new cell-based tissue engineering approach, stem cells are combined with an osteoconductive scaffold and growth factors, and applied immediately to the patient. In this review, MSFE is discussed as a valid model to test bone tissue engineering approaches, such as the one-step surgical procedure. This procedure might be applied in other regenerative medicine applications as well.
Introduction
Since the reconstruction of (large) bone defects in the oral and maxillofacial region is a common challenge, bone tissue engineering has become a promising alternative for bone reconstruction. However, the application of bone tissue engineering approaches in the clinic is hampered by the fact that there is not a good human model available to study these concepts. MSFE could represent an excellent human model to study new bone tissue engineering modalities, such as the one-step surgical procedure, avoiding the use of autologous bone (Fig. 1). In this one-step surgical procedure, adipose tissue is harvested and processed to obtain the stromal vascular fraction (SVF), which contains adipose stem cells or adipose stromal cells (ASCs). These stem cells can be seeded on off-the-shelf scaffolds, to be applied immediately to the patient in an intraoperative concept.4,5
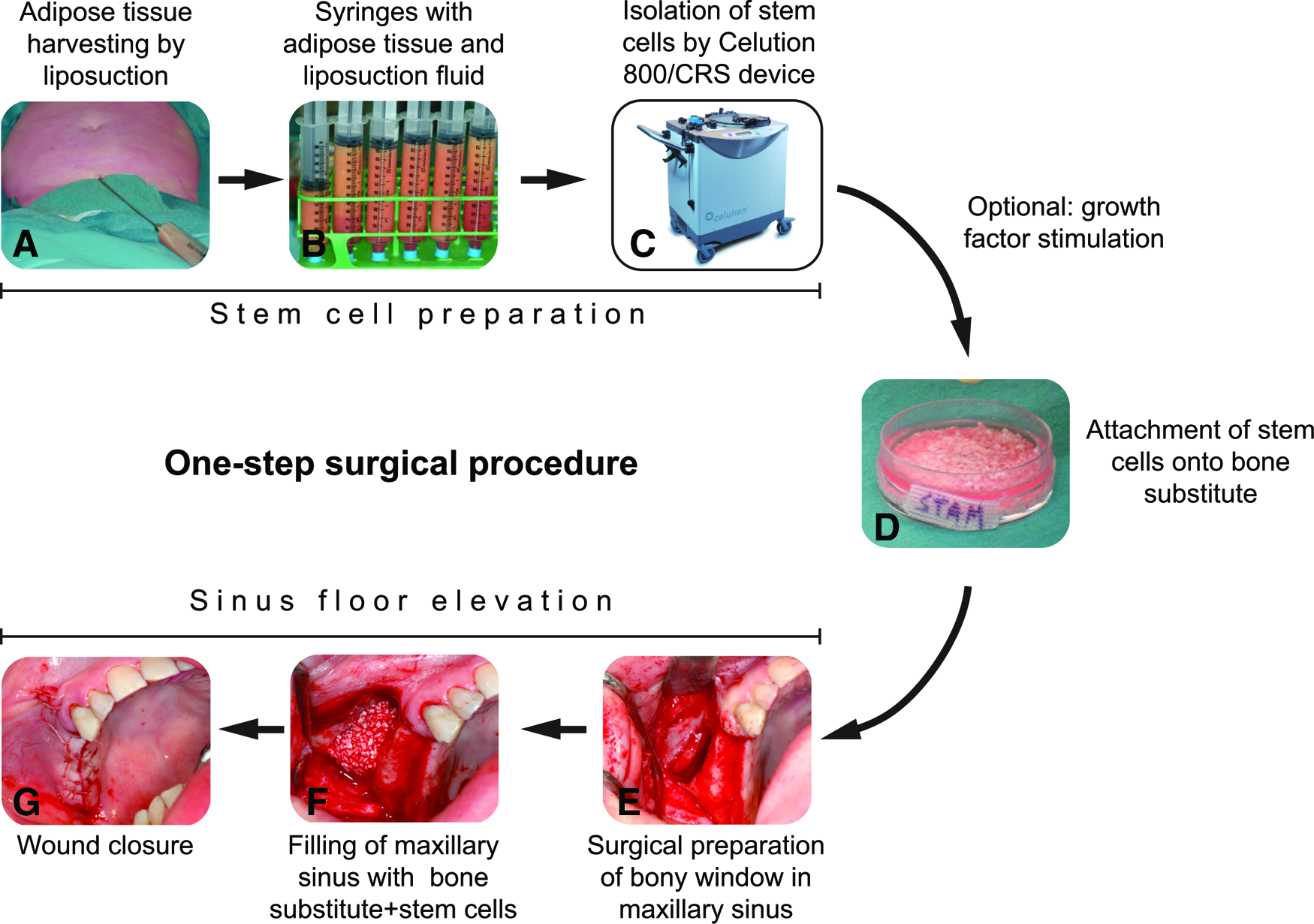
Concept of a maxillary sinus floor elevation (MSFE) with freshly isolated adipose-derived stem cells in a one-step surgical procedure.
Maxillary sinus floor elevation
The surgical procedure of MSFE was first performed by Tatum 6 and published by Boyne. 7 In the procedure described, a window in the lateral wall of the maxillary sinus is made, followed by elevation of the maxillary sinus membrane (Schneiderian membrane) to create a cavity in which a bone graft can be placed (Fig. 2). Nowadays, MSFE has become a standard surgical procedure to increase the bone height in the posterior maxilla.2,8 This procedure provides sufficient alveolar bone height for placement of dental implants after the appropriate healing time of the graft, and increases implant success.
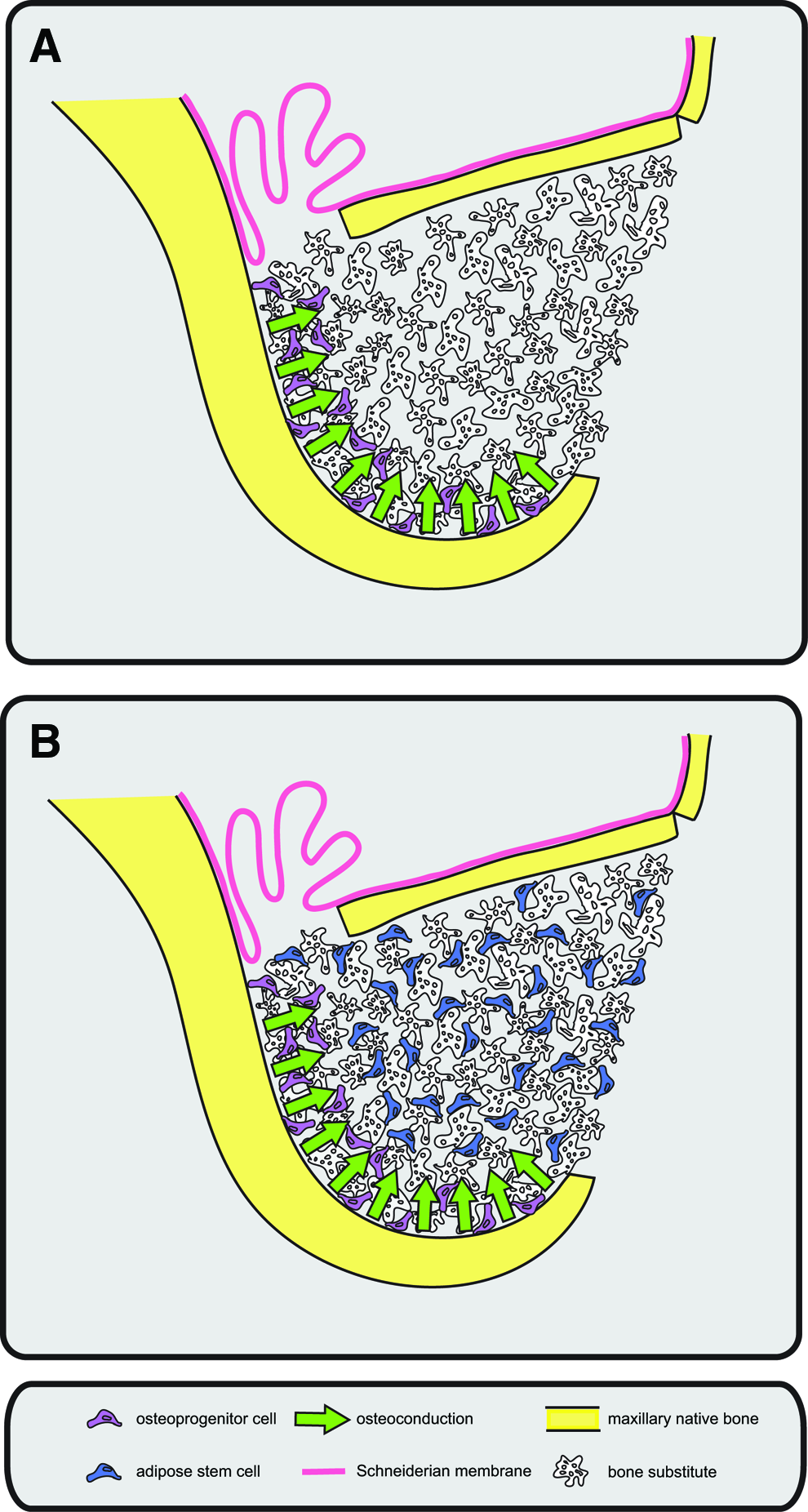
Schematic figure of the MSFE procedure.
Bone graft materials in MSFE
Tatum 6 introduced the use of allograft or bone from another individual of the same species, and alloplast or synthetic material, besides autograft to fill the space created when elevating the Schneiderian membrane, thereby eliminating the need for a second surgery to obtain an autologous bone graft, and thus also reducing potential complications from an additional surgery. 9 The lateral window MSFE technique is commonly used nowadays, and still the best results are achieved using autologous bone.3,10 Bone grafting material, such as demineralized bone matrix is also commonly used. It induces bone formation in the human maxillary sinus by providing an osteoconductive matrix that allows migration of precursor cells from the host and differentiation into bone matrix-producing cells 8 (Fig. 2).
A variety of bone grafts are used for MSFE with different degrees of success (Table 1). The bone graft materials applied in MSFE are (1) autologous bone graft, mostly from the iliac crest or mandibular bone, (2) allograft, (3) xenograft, from bovine or porcine origin, and (4) alloplast materials, such as β-tricalcium phosphate (β-TCP), hydroxyapatite (HA), mixtures of HA/β-TCP (biphasic calcium phosphate [BCP]), polymers, and bioactive glasses. Autologous bone graft is still considered as the gold standard, since it contains osteoblasts and osteoprogenitor cells, and is not only osteoconductive by allowing the migration of progenitor cells, but also osteogenic.11–13 Since these grafts are from the same individual, the tissue is recognized as self, and the immune system is not triggered with an immunological response. 14
Calvarial defects were critical-sized.
ABB, anorganic bovine bone; DBM, demineralized bone matrix; FN, fibronectin; CaP, calcium phosphate; HA, hydroxyapatite; β-TCP, β-Tricalcium phosphate; BCP, biphasic calcium phosphate (%HA/%β-TCP); PLA, polylactic acid; PLGA, polylactic-coglycolide copolymers; SVF, stromal vascular fraction; ASCs, adipose stem cells; BM-MSCs, bone marrow-derived mesenchymal stem cells; BMP-2, bone morphogenetic protein-2; PRP, platelet-rich plasma; MSFE, maxillary sinus floor elevation; GBR, guided bone regeneration; n.a., not available.
Although it is generally accepted that autologous bone is the gold standard for the MSFE procedure, this may not always be the case. Abscesses, fistulas, dehiscences, and large numbers of bacteria can be found in particulated bone collected with suction devices, such as bone traps, 15 in addition to the disadvantage of limited bone availability and patient morbidity. 14 Alternative bone graft materials frequently used are allogeneic bone and bone substitutes. Allogeneic bone is mostly applied in the form of demineralized freeze-dried bone matrix. The bone morphogenetic proteins (BMPs) present in the matrix of bone allograft are exposed by decalcification leading to induction of osteogenic differentiation of progenitor cells. However, The Sinus Consensus Conference held in Wellesley, MA, USA, in 1996 concluded that demineralized freeze-dried bone is not an appropriate bone substitute, since it always carries the risk of disease transmission and might cause marked bone resorption. 11 Other disadvantages, such as lack of osteogenesis and osseointegration, and the risk of immune rejection at the implant site,16,17 lead to a search for alternative graft materials.
Bone substitutes are interesting alternatives because they are available in unlimited quantity and may be used as off-the-shelf products. However, bone substitutes are cell-free and require more time for bone healing than autologous bone grafts. 18 It has been shown that maxillary sinus grafting with alloplast materials, such as bioactive glass, HA, or β-TCP, does not result in increased bone volume compared with autologous bone graft.10,12 Several attempts have been made to apply a cell-based approach using stem cells combined with an osteoconductive biomaterial or scaffold, which is known as cell-based bone tissue engineering.19–23
Bone Tissue Engineering in MSFE: A Potential Model to Be Used in Other Surgical Disciplines
For cell-based bone tissue engineering, the choice of osteoprogenitor cells and biomaterials is crucial, as well as the type of growth factor(s) that stimulate osteogenesis and improve osteogenic differentiation of the progenitor cells. Bone regeneration in the oral and maxillofacial region can be used to investigate tissue engineering approaches for later use in other surgical disciplines. Bone biopsies from patients can be taken after an MSFE procedure and before dental implant placement. These bone biopsies can then be analyzed by micro-CT, histomorphometry, and histology24–27 and are highly valuable for evaluating new approaches for oral and maxillofacial bone tissue engineering, such as the use of different progenitor cells, growth factors, and biomaterials. Furthermore, the treatment of patients requiring an MFSE procedure at both sites of the maxilla enables the use of a bilateral split-mouth design model, allowing to study simultaneously different conditions in the same patient. Therefore, the MSFE procedure is proposed as a human model for bone regeneration to be used in a so-called one-step surgical procedure. The maxillary sinus represents an excellent model as an osteogenic chamber for bone regeneration. 28
The lack of quantitative or histomorphometric data becomes an important drawback in studies comparing different bone grafts for MSFE. 29 Clinically, it is difficult and time-consuming to analyze a large number of samples, 13 and therefore it is desirable to generate a variety of studies with similar approaches, and to combine and compare these results in a meta-analysis.
A cell-based approach that uses stem cells combined with an osteoconductive scaffold may become an interesting alternative to conventional procedures, avoiding the major problems associated with bone graft transplantation. However, the paradigm of tissue engineering is to find a suitable human model to investigate the appropriate combination of scaffold and source of osteoprogenitor cells.
A limitation for successful application of bone tissue engineering in MSFE is the relative absense of mechanical loading, which is a critical issue for bone regeneration. It has been shown that mechanical loading favors proliferation and osteogenic differentiation of progenitor cells, while inhibiting adipogenic differentiation, 30 and this should be taken into account to decide the appropriate time for implant loading.
Sources of Stem/Progenitor Cells for Clinical Application
In the late 60s, Friedenstein showed that the mesenchymal stroma from human bone marrow contains a population of cells that proliferate when cultured on plastic, and differentiate to cell lineages derived from the mesoderm, such as chondrocytes and osteoblasts. 31 Later, these precursor spindle-shaped cells were referred to as mesenchymal stem cells (MSCs) 32 and shown to differentiate into several lineages in vitro 33 and in vivo,34,35 making them promising candidates for regenerative medicine applications. MSCs grow when adhered to plastic and express specific surface antigens. They also possess multipotent differentiation potential and low immunogenic potential, according to the minimal criteria to define MSCs, proposed in 2006 by the International Society for Cellular Therapy. 36 Their immunosupressive properties and differentiation potential make MSCs interesting for regenerative medicine clinical applications. The main sources of MSCs for clinical studies in bone tissue engineering are bone marrow and adipose tissue.
Bone marrow-derived MSCs
Bone marrow-derived MSCs (BM-MSCs) are widely used in bone regeneration, since they are relatively easy to harvest and show multipotent differentiation potential.33–35,37 MSCs secrete growth factors and cytokines that inhibit apoptosis and fibrosis or scarring at the site of injury. They also stimulate angiogenesis and proliferation of progenitor cells, and exert an immunomodulatory effect in the organism. These effects, known as “the trophic activity,” 38 make them interesting candidates to improve bone regeneration in the MSFE procedure (Table 2). Addition of BM-MSCs to bone derivative/substitute materials, such as BCP particles, enhances bone formation in the maxillary sinus area, with 41% mean percentage of newly formed bone observed at 3 months postsurgery. 23 Another study using BCP without cells showed 27% average of bone volume at 6 months postsurgery. 25 BM-MSCs applied to calcium phosphate scaffolds for MSFE promote faster bone formation and mineralization in animal models.39–42 One study in rabbits found an increase in bone formation when BM-MSCs were applied to a calcium phosphate scaffold in comparison with scaffold without cells. 43 These results suggest that BM-MSCs may improve new bone regeneration in the maxillary sinus.
Calvarial defects were critical-sized.
MCBA, mineralized cancellous bone allograft; CaCO3, calcium carbonate; CaSO4, calcium sulfate; VEGF, vascular endothelial growth factor; BMP-7, bone morphogenetic protein-7; GDF-5, growth and differentiation factor-5.
The use of BM-MSCs also has disadvantages, such as pain associated with the harvest procedure and low cell numbers upon harvest, especially in elderly patients. 44 Only one MSC per 105 adherent mononuclear cells is obtained upon harvest, 33 necessitating an ex vivo expansion step to obtain therapeutic cell numbers, which is time-consuming, expensive, and carries the risk of contamination. Long cell culture is associated with loss of differentiation potential and risk of cell transformation.45,46 The number and concentration of progenitor cells with an angiogenic potential in a scaffold are also important for successful bone formation in vivo, since the vascular network is crucial to ensure cell survival. 47 These considerations associated with BM-MSCs have led to a search for other sources of progenitor cells for clinical application.
Adipose stem cells
Adipose tissue has gained interest as it contains a population of stem cells with MSC characteristics. 48 Adipose tissue, as bone marrow, is derived from adult mesodermal tissue, and after tissue disgregation, collagenase digestion, and cell centrifugation, a pellet is obtained, which contains a heterogeneous cell population composed of preadipocytes, mast cells, endothelial cells, pericytes, smooth muscle cells, fibroblasts, and multipotent progenitor cells with similar characteristics to BM-MSCs, as well as hematopoietic stem cells. 48 This mixture of cells is known as the SVF.
When the pellet is cultured, an adherent cell population is obtained that can be expanded and used in a variety of assays. A wide nomenclature is used to identify this cell population, including adipocyte precursor cells, preadipocytes, adipose-derived adult stem cells, adipose-derived stromal cells, adipose-derived adherent stromal cells, processed lipoaspirate cells, and adipose-derived stem cells. 49 At the Second Annual International Fat Applied Technology Society meeting (October 3–5, 2004, Pittsburgh, PA), consensus was reached to use the term SVF for the freshly isolated SVF, and to refer to the stem cell-like cells within this fraction as ASCs. Passaged cells (cells cultured to homogeneity) are also referred to as ASCs. These ASCs can differentiate into multiple mesenchymal tissue cell types, such as osteoblasts, chondrocytes, adipocytes, and myocytes. 50
ASCs become an interesting alternative to BM-MSCs, since adipose tissue is easy to access, and its harvesting results in minimal patient discomfort. Furthermore, adipose tissue contains a 100 to 1000-fold higher number of stem cells than bone marrow, and ASCs proliferate faster than BM-MSCs.4,33,50,51 ASCs also secrete growth factors with angiogenic and antiapoptotic potential, which makes them interesting candidates for bone tissue engineering, where blood supply is needed.51–53 These angiogenic properties allow them to survive in low oxygen environments, and make them good candidates for cell-based therapies, such as maxillary reconstruction. 22 ASCs also abundantly express CD34, 54 in contrast with MSCs, which lack CD34 expression.36,55 Cultured ASCs show decreased CD34 expression, which is totally lost after long-term culture.49,54 The marker CD34, which is also expressed in hematopoietic and endothelial stem cells, is related to angiogenesis and could have important implications in bone tissue engineering, where angiogenesis is crucial.52,56
Since the amount of bone formed depends at least, in part, on the number of cells that survive, it is crucial to provide a high number of osteoprogenitor cells per given volume of tissue, to ensure adequate bone formation. A dose-dependent effect on bone formation has been reported for cultured ASCs applied to a calvarium rabbit bone defect. 57 ASCs promote healing of critical-sized cranial defects in mice and rabbits,57–60 and have been successfully used in animal models for vertical bone regeneration, 57 as well as in MSFE using the SVF containing the ASCs 61 (Table 2). ASCs have been used successfully in humans to reconstruct major maxillary defects 22 and traumatic calvarial defects. 62 Calvarial bone is embryologically, morphologically, and physiologically similar to bone in the oral and maxillofacial region. Its high flat surface eases the fixation of titanium osteosynthesis 57 making it an interesting model to study oral bone regeneration. Adipose tissue may be an interesting source of progenitor cells for oral and maxillofacial applications, where high cell numbers may be needed for successful bone regeneration. To select the appropriate scaffold for combination with these cells is another critical issue in bone regeneration.
Scaffolds for Oral and Maxillofacial Bone Tissue Engineering
Not only the appropriate source of progenitor cells, but also the use of the right type of carrier scaffold with adequate pore size, porosity, and composition, is a key issue in bone tissue engineering. The ideal scaffold has a high porosity and interconnected pore network, which is large enough to facilitate vascular invasion and bone development. 26 Large pore sizes (>300 μm) promote neovascularization and favor mineralized bone ingrowth, whereas smaller pore sizes (90–120 μm) promote endochondral bone formation. 63 For tissue engineering, the ideal scaffold should be biocompatible with the right porosity and pore size to facilitate neovascularization, and an adequate surface allowing cell adhesion, proliferation, and differentiation. Furthermore, the scaffold should be osteoinductive, releasing growth factors that modulate osteoblastic cell functions and enhance bone formation, and the mechanical properties should match those of living bone. Finally, the scaffold degradation rate should be tuned with the growth rate of the de novo bone formation, id est the scaffold is totally degraded by the time the injury site is fully regenerated.3,64 The size of the scaffold is also important for adequate bone regeneration. Particles with a size ranging from 250–500 μm have been shown to increase the volume of mineralized tissue in MSFE showing the presence of lamellar and woven bone. 8
Absorbable scaffolds used in bone tissue engineering are divided in biodegradable polymers of synthetic origin, such as polylactic acid, polyyglicolic acid, polylactic-coglycolide copolymers, and poly(ɛ-caprolactone),65–68 natural polymers, such as collagen, hyaluronic acid, fibrin, and silk fibroin,64,69–72 bioactive glasses with a silica-based osteoinductive surface, 73 inorganic materials containing calcium phosphate (ceramics), and finally composite materials, which combine, for example, calcium phosphate ceramics with polymers. 64
Various grafts or combinations of graft materials have been used successfully in the oral and maxillofacial region (Table 2). Inorganic materials or ceramics from natural origin, such as calcium carbonate, calcium phosphate, calcium sulfate, bovine-derived, or coralline HA, and from synthetic origin, such as synthetic HA or β-TCP, have been widely used in MSFE due to their good biocompatibility and osteoconductivity,10,26,74–79 besides bone grafts,13,16,17,26,29,74,77,78 polymers,28,78,80–86 and bioactive glass.78,87,88
Synthetic Calcium Phosphate Scaffolds for Oral and Maxillofacial Bone Tissue Engineering
HA and β-TCP have been successfully used for MSFE procedures because of their good biocompatibility and chemical composition, which resembles the composition of natural bone matrix.10,25,89,90 Advantages of using ceramics, such as β-TCP, is that they support cell in-growth and promote osteogenic differentiation of osteoprogenitor cells.90,91 However, unlike HA, β-TCP reabsorbs rapidly, but concurrent bone formation does not occur in a 1:1 ratio, and often less bone is produced as compared with the volume of β-TCP absorbed. 10 BCP combines the bioactive properties of HA with the good bioresorbability of β-TCP. Due to its high surface area and three-dimensional hierarchical porosity, it supports attachment, proliferation, and osteogenic differentiation of progenitor cells.92,93 BCP contains a mixture of 60% HA and 40% β-TCP and has been used successfully for MSFE,25–27,94 with an implant survival >98%27,89 and bone formation similar to allograft and xenograft.16,26 The macroporosity (pore diameter 300 to 600 μm) of BCP scaffold allows colonization by osteogenic cells. Osteoclasts attach to the BCP surface to resorb biomaterial, stimulating osteoblast differentiation and activity through signaling molecules, while no osteoclast resorption is found on the β-TCP material, which is resorbed mainly by chemical dissolution.90,95 This suggests that the BCP material may be promising for use as a scaffold for bone tissue engineering. The favorable clinical results obtained with BCP are similar as those obtained with xenografts, such as an organic bovine bone,13,16 or other alloplastic materials, such as HA. 26 However, significantly, less bone formation is observed when compared with autologous bone grafts, indicating that autologous bone grafts still remain the gold standard, showing increased bone formation compared to alloplast material and xenografts.13,24,27,77,78,87
In certain augmentation cases, such as maxillary sinus grafting, complete resorption of the bone substitute to be replaced by new bone is not preferable. A long-lasting active osteoconductive guiding scaffold is required to support osseointegrated dental implants without destabilization of bone. 74 Therefore, the stability of the graft material in the maxillary sinus and height changes of the graft material over time are important issues for successful bone regeneration in MSFE. Calcium phosphate ceramics have also drawbacks, such as lack of osteogenic properties, brittleness, and low mechanical stability observed when using β-TCP, which makes them unsuitable for reconstruction of large bone defects.65,96 Therefore, addition of osteoprogenitor cells might be required to improve the osteogenic properties of the graft, since the ideal bone graft should provide osteogenic cells as well as osteoinductive factors for bone regeneration 64 (Table 1). For clinical application of bone tissue engineering, the appropriate source of stem cells, together with the adequate scaffold, and the use of growth factors that speed up tissue regeneration are crucial issues for successful clinical application.97,98
Growth Factors for Oral and Maxillofacial Bone Tissue Engineering
Angiogenesis is extremely important in bone regeneration, since blood vessels carry nutrients, which are crucial to ensure the survival of transplanted progenitor cells, 99 and vascular development needs to be induced before osteogenesis.77,100 To establish the vascular network, growth factors, such as platelet-derived growth factor, transforming growth factor-β (TGF-β), vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and those factors present in platelet-rich plasma (PRP), a platelet concentrate obtained from the patient's own blood, are needed to induce and speed up angiogenesis in the regenerating tissue, and may be used in oral and maxillofacial applications to reduce the healing time and enhance bone formation53,84,101–105 (Table 3). These growth factors can be added to all grafting materials. There is a controversy in the literature related to the use of PRP in MSFE procedures. Although some studies found an effect of PRP on bone formation in combination with bone substitutes 104 and bone grafts, 106 other studies did not find such an effect when PRP was combined with a xenograft, 29 an autologous bone graft, 12 or a synthetic bone substitute. 87 Ex vivo seeded ASCs onto a scaffold secrete a high variety of angiogenic growth factors, such as VEGF and FGF-2, which makes them interesting candidates for inducing bone tissue formation.51,107
Calvarial defects were critical-sized.
PDGF, platelet-derived growth factor; FGF-2, fibroblast growth factor-2.
One substantial group of growth factors for bone tissue engineering is the BMPs. BMPs have been found in the demineralized bone matrix more than 40 years ago. They belong to the TGF-β superfamily and promote the differentiation of osteoprogenitor cells and induce osteogenesis. 108 An acute increase in the secretion of bone morphogenetic protein-2 (BMP-2) and bone morphogenetic protein-7 (BMP-7), together with bone morphogenetic protein-4 (BMP-4), has been shown when applying ASCs in critical-sized mouse defects, 58 which suggests a role of these growth factors in bone regeneration and remodeling.
The osteoinductive properties of BMPs make them interesting candidates to promote bone formation in rehabilitation of partially or completely edentulous patients with severe maxillary or mandibular atrophy. Favorable regenerative responses to the graft materials containing BMPs in MSFE procedures have been reported.11,15,22 BMP-2, BMP-7, and bone morphogenetic protein-14 (BMP-14, known as growth and differentiation factor-5) have been applied in MSFE procedures75,79,80,83,109 (Table 3). Only recombinant human bone morphogenetic protein-2 (rhBMP-2) and recombinant human bone morphogenetic protein-7 (rhBMP-7) are approved by the food and drug administration (FDA) as medical device. 108 Although FDA approval is limited to few orthopedic applications, other (off-label) applications are considered safe, and may warrant the use of rhBMP-2 and rhBMP-7 clinically in MSFE procedures.
Bone morphogenetic protein-7
There are contradictory reports concerning osteoinduction of osteoprogenitor cells by BMP-7. Some studies suggest that BMP-7 is osteoinductive,38,110 while others suggest that BMP-7 stimulates chondrogenesis. 5 This is in contrast to the stimulatory effect of BMP-2 on osteogenic differentiation of progenitor cells.5,85,111 BMP-7 applied in the MSFE procedure induces bone regeneration.80,112 However, the use of BMP-7 is associated with swelling and the presence of some granular tissue, which could indicate an inflammatory response. 80 This is likely due to the putty component of the BMP-7 preparation, which recruits multinucleated giant cells. 113
Bone morphogenetic protein-2
BMP-2 is a potent osteoinductive molecule that has been shown to increase and speed up osteogenic differentiation, and induce healing of intrabony periodontal defects as well as critical size defects in animals.82,86,105,114 BMP-2 applied to osteoprogenitor cells5,115,116 and/or to osteoconductive scaffolds22,43,76,81–86,105,114 stimulates osteogenic differentiation in vitro and accelerates bone healing and new bone formation in vivo (Table 3). Carriers combined with BMP-2 have also been shown to induce bone formation when applied in MSFE in sheep, 85 rabbit,43,76,84 and pig, 81 as well as in the healing of critical-sized calvarial defects in rats 86 and periodontal defects in dogs. 82 In an in vivo study in rats using a femoral osteotomy model, a 2-mm femoral gap stabilised by an external fixator device failed to heal within 6 weeks, whereas local application of rhBMP-2 within a blood clot showed proper bone healing with bony bridging. 117 This indicates that BMP-2 stimulates osteogenic differentiation of osteoprogenitor cells and might be beneficial for clinical application.
The dose of growth factor is also an important issue to take into account in clinical applications. It has been shown that incubation with only 10 ng/mL BMP-2 during 15 min is enough to stimulate osteogenic differentiation of goat-derived ASCs. 5 This dose of the growth factor is magnitudes lower than the concentration of BMP used in in vivo and clinical studies (0.2–2.5 mg/mL carrier), and may avoid side effects of using mg-range concentrations, such as swelling, ankylosis, and calcified seromas, as observed in some studies.80–83,114,118 It would also avoid the high costs of using high BMP-2 concentrations. BMP-2 supplementation at a low concentration (10 ng/mL) may help to maintain the viability of endothelial cells, 100 as well as ASCs (Overman and Farré-Guasch, submitted). Moreover, this rather low and short incubation with BMP-2 could easily fit within a one-step surgical procedure, where autologous stem cells are isolated, triggered with growth factors, and immediately used for bone regeneration within the same surgical procedure (Fig. 1).4,5
One-Step Surgical Procedure Approach for MSFE
The SVF, obtained after collagenase digestion and centrifugation of adipose tissue, has potential for bone tissue engineering, since it contains ASCs with osteogenic potential, among other cell populations.62,119,120 For clinical application, it would be advantageous to transplant the whole SVF, thereby avoiding expensive and time-consuming in vitro selection and/or expansion steps, loss of differentiation potential, and the risk of contamination. Additionally, the harvesting of human adipose tissue by liposuction is an easy and safe procedure, unlike the harvesting of human bone marrow, which is associated with donor-site morbidity. 44 Most studies have been performed on cultured ASCs, but before being used clinically, they must overcome prohibitively expensive good manufacturing practice production facilities. 55 In addition, FDA approval in the USA, or European Agency for the Evaluation of Medicinal Products approval in Europe, is required before use. These limitations hamper the use of cultured stem cells for clinical use. However, using uncultured ASCs in the form of SVF produced via CE-marked devices would overcome at least several of these restrictions.121–123
ASCs in SVF act in coordination with blood cells, such as endothelial cells and hematopoietic cells, regulating their undifferentiated state as occurs in the perivascular niche. 124 These cells secrete factors that increase proliferation of progenitor cells, such as ASCs, and enhance their osteogenic potencial. 125 When SVF was cotransplanted on calcium phosphate scaffolds subcutaneously in mice, the vascular number and diameter and ectopic mineralization were increased. Therefore, vasculogenesis and osteogenesis may be improved by a synergistic action of ASCs with (pre)vascular cells present in the SVF. 126 The synergistic actions of (pre)vascular cells and MSCs may provide an alternative approach for the regeneration of vascular tissues, such as bone, where an adequate vascularization is pivotal in effective cell-based bone tissue engineering.
For a one-step surgical procedure in MSFE, an appropriate amount of adipose tissue would be obtained from the patient. Most patients have an adequate supply of adipose tissue that can be obtained by liposuction using local anesthetics, and the SVF obtained from adipose tissue is a rich source of ASCs readily available for immediate clinical application. 121 The freshly isolated SVF can be shortly stimulated with growth factors, such as BMP-2, before seeding the stimulated cells onto a carrier material. 5 After a short attachment period, 127 the tissue-engineered construct is implanted immediately in the patient. 4 The feasibility of a one-step procedure relies on the ability of the ASC fraction within the SVF to attach to a scaffold material in sufficient quantities and within a short time frame, which was recently demonstrated to occur. Moreover, it was shown that the multidifferentiation potential was maintained, thus likely enhancing angiogenesis and osteogenesis and the final clinical outcome. 127
Summary and Future Directions
A cell-based bone tissue engineering approach using stem cells combined with an osteoconductive scaffold and growth factors that stimulate osteogenesis and angiogenesis may become an interesting alternative to the conventional MSFE procedure using autologous bone. Future directions in tissue engineering for MSFE should consider:
1. The need to find the appropriate scaffold for cell-based tissue engineering in MSFE. Calcium phosphate ceramic scaffolds have been widely used in MSFE and support attachment, proliferation, and promote differentiation of osteoprogenitor cells. 2. The appropriate source of stem cells as well as the cell dose to be used in MSFE and study scaffold–cell interactions. The SVF obtained from adipose tissue contains, among other cell types, a relatively large number of freshly isolated cells with angiogenic and osteogenic potential, required for vascularization and osteogenesis in the tissue-engineered construct. 3. The delivery method and the appropriate dose of growth factors, such as BMP-2, are critical issues to be considered to enhance bone formation in MSFE. A short (minutes) incubation with a low dose of BMP-2 of 10 ng/mL may avoid the side effects of higher concentrations seen in clinical studies, which are shown to be dose-dependent, and may be enough to stimulate an osteogenic response in ASCs. 4. New bone tissue engineering cellular therapeutic approaches have to be evaluated in phase I-IV clinical trials that meet the ATMP Regulation 1394/2007/EC and/or FDA regulations, as well as (local) rules and good clinical practice guidelines.
In summary, previous studies have shown the importance of scaffolds and growth factors, together with the appropriate source of stem cells, in bone tissue engineering, and have highlighted the need to find an appropriate model for clinical applications. Human MSFE may be a valid model to test bone tissue engineering approaches in a one-step surgical procedure for later use in other surgical disciplines. The comparison of a large number of patients treated with scaffolds differing in their properties, in combination, with different cell types and numbers, which are either or not stimulated with different doses of growth factors, will provide critical evidence for future meta-analysis evaluating the safety, efficacy, and outcome measures of clinical trials using new bone tissue engineering approaches.
Footnotes
Disclosure Statement
No competing financial interests exist.