
Abstract
Metal implants and polymeric devices for the application in the clinical treatment of orthopedic tissue injuries are increasingly coated with bioactive biomaterials derived from natural substances to induce desirable biological effects. Many metals and polymers used in biomaterials research show high affinity for endotoxins, which are abundant in the environment. Endotoxin contamination is indicated in the pathology of periodontitis and aseptic implant loosening, but may also affect the evaluation of a biomaterial's bioactivity by inducing strong inflammatory reactions. In this review, we discuss the high affinity of three commonly used implant biomaterials for endotoxins and how the contamination can affect the outcome of the orthopedic fixation. The chemical nature of bacterial endotoxins and some of the clinical health implications are described, as this knowledge is critically important to tackle the issues associated with the measurement and removal of endotoxins from medical devices. Commonly used methods for endotoxin testing and removal from natural substances are examined and the lack of standard guidelines for the in vitro evaluation of biomaterials is discussed.
Introduction
Endotoxins are abundant in the environment, can strongly interact with most metals and polymers used in biomaterials research, and represent one of the main issues in an already very complex research field. 3 The effect of endotoxin contamination on biomaterial performance in vitro should not be underestimated, as even minute amounts of endotoxins can elicit strong inflammatory reactions that might overrule any biological effect of the biomaterial itself.4,5 The problems accompanying the removal and measurement of endotoxins from medical devices require the knowledge of the chemical nature of bacterial endotoxins. 6
Here, we review the chemical nature of bacterial endotoxins and some of the clinical health implications associated with their presence in the human body. We also describe the affinity of three commonly used implant biomaterials for interactions with lipopolysaccharides (LPS) and the effect of contamination on the outcome of the orthopedic fixation. Finally, we examine the commonly used methods for endotoxin testing and how endotoxins can be efficiently removed from natural substances for the successful application in biomaterials research.
Endotoxins
During the 18th century, the search for the inducers of fever and sepsis in unhygienic conditions yielded a substance that was termed endotoxins. 7 An integral part of the outer membrane of gram-negative bacteria was found to consist of LPS associated with proteins and other cell membrane-related components.6,7 LPS is only secreted in minute amounts during cell division and the normal life-cycle of the bacteria, however, substantial amounts can be released during the destruction of the bacterial cell wall either by antibiotics or the actions of the host immune system.7,8
LPS is built of three main parts; a lipid moiety, called Lipid A, linked to an oligosaccharide, the core oligosaccharide, which in turn is attached to a sequence of repetitive subunits, named O-specific antigen. 9 The Lipid A moiety is characterized by a disaccharide backbone with two negatively charged phosphate groups and can carry as much as six acyl chains with 14–16 carbon atoms (Fig. 1). 10 The amphiphilic nature of Lipid A, having both hydrophobic and hydrophilic features, causes aggregation in aqueous solutions to form three-dimensional supramolecular structures, called micelles.10,11 The O-specific antigen is used to classify the bacterial serotype and assists the bacteria in evading the attack of serum complements from the host immune system.12,13 Although LPS is commonly regarded as prevalent endotoxin, other bacterial products, that is, peptidoglycan in the bacterial cell wall, as well as lipoteichoic acid and teichoic acid derived from gram-positive bacteria, may induce immune reactions in the host comparable to LPS. Consequently, the expression endotoxin, as used in this review, is intended to include both LPS and other bacterial substances that initiate similar biological actions.8,9
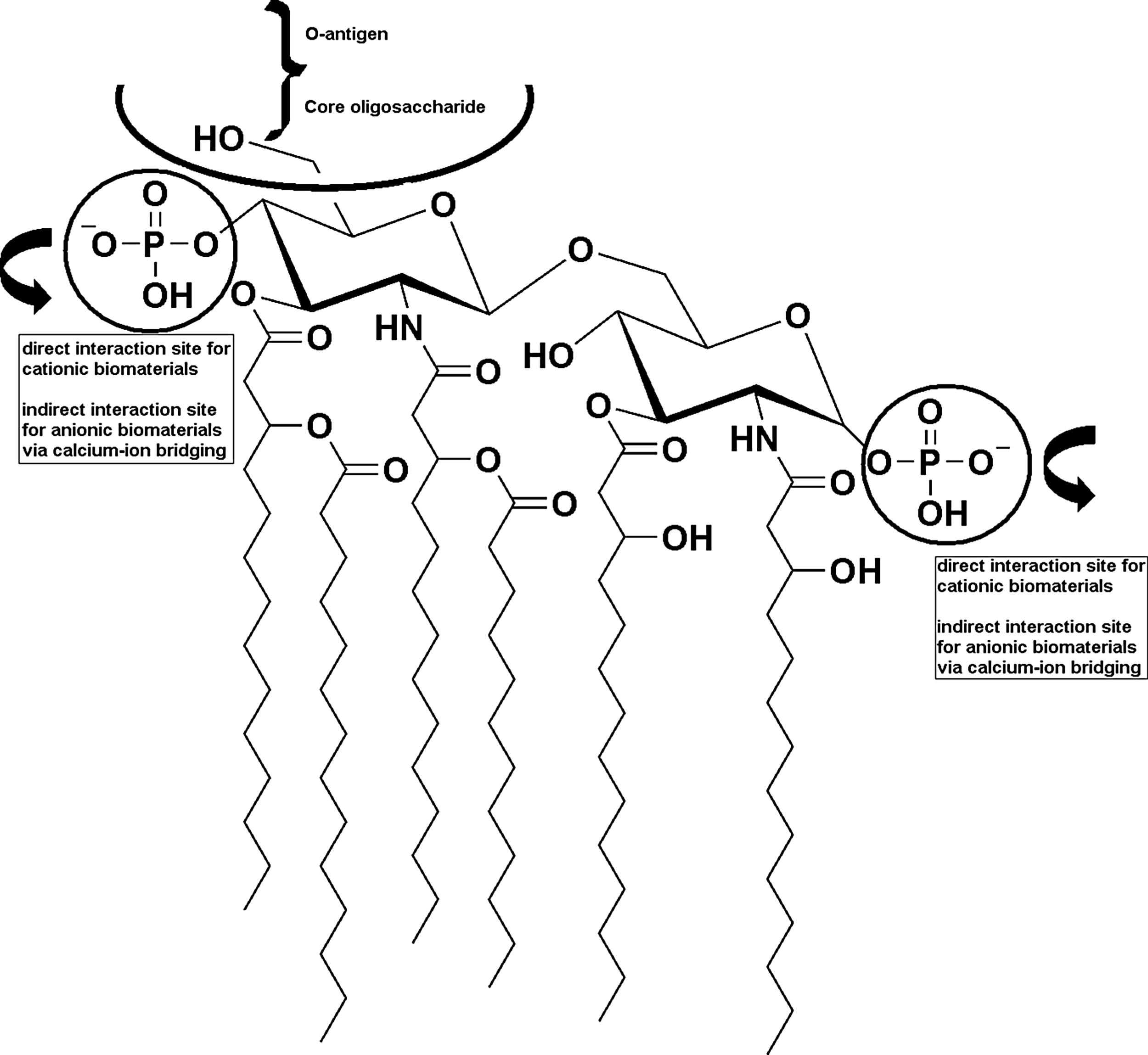
Structure of Escherichia coli Lipid A. The direct and indirect interaction sites with biomaterials are shown with a circle and an arrow. Positively charged biomaterials can directly interact with the negatively charged phosphate groups in the Lipid A moiety. Negatively charged biomaterials can bind Ca2+ ions, forming a bridge between the Lipid A phosphate groups and the interaction site of the biomaterial. On the top half of the structure, the connection to the core oligosaccharide and the O-antigen of the complete endotoxin structure is indicated.
The general properties of endotoxins include that they are negatively charged in solutions, thermally stable up to 180°C, and UV-resistant.3,14 Endotoxins are not soluble in methanol or ethanol, and range in their molecular weight from 10 kDa to 1000 kDa, depending on the presence of single molecules or aggregated micelles.14,15
Health implications of endotoxins
The immune system is able to detect and react to LPS at levels of less than 1 ng/mL. 16 Even without signs of bacterial infection, LPS can be found in human tissues. High concentrations are known to induce high fever, hypotension, and septic shock, whereas low levels of LPS might contribute to the development of several chronic diseases.7,17,18 Multiorgan failure, adult respiratory distress syndrome, and disseminated intravascular coagulation are further consequences of increased endotoxin levels in the blood.7,18
Sepsis and endotoxemia
The term sepsis describes a medical condition, in which an overwhelming bacterial infection can promote an inflammatory state of the whole body, accompanied by fever, increased heart, and respiratory rate. 19 The diagnostic test for severe sepsis includes the measurement of endotoxins in blood and other bodily fluids. 20 Severe sepsis with high levels of LPS is associated with worse prognosis and longer stays in the intensive care unit. 20 Multiorgan failure is common and the occurrence of acute liver damage is believed to be correlated to the presence of endotoxins.21,22 Antibiotics, one of the most common treatments for sepsis, can deteriorate the disease by destroying the bacterial cell wall and releasing large amounts of endotoxins into the blood stream. 23 Highly sensitive bioassays are needed to determine the presence of LPS in human plasma, since the compound has a very short serum half-life, is poorly immunogenic, and exhibits extreme potency. 19
Periodontitis
Endotoxins are believed to play a role in the development of chronic periodontitis, where the presence of LPS could result in delayed healing, inflammation, and reduced cell proliferation.24–26 Bacteria associated with periodontitis around teeth are also believed to contribute to failing implants in the jaw. 27 The process of implant loosening does not necessarily reflect the course of the inflammatory response to periodontitis, however, the induction of bone resorption might nevertheless be partly correlated to the presence of gram-negative bacteria and LPS. 28
Aseptic implant loosening
The role of endotoxins in the clinical setting of aseptic implant loosening is controversial, but increasing evidence indicates endotoxins as at least partially responsible for osteolysis and the loosening of the medical device.5,29–33 LPS was detected in the tissue surrounding the implant in patients diagnosed with aseptic implant loosening, who did not show any signs of microbial infection. 34 Additionally, the prophylactic use of antibiotics, systemically or as part of the implant, resulted in a 50% reduction in the incidence of aseptic loosening. 35
Furthermore, endotoxins were associated with inflammation in response to wear particles, accelerating the foreign body reaction, proinflammatory cytokine release, and macrophage activation.33,36,37 This theory is based on the notion that macrophages at the bone–biomaterial interface express endotoxin receptors, markedly Toll-like receptors, which are highly sensitive to even minute amounts of endotoxins and could be responsible for the induction of cytokine secretion, impairing osseointegration, and, finally, the failing of the implant.5,30,38,39 However, the removal of endotoxins was shown to have a greater impact on in vitro cell culture studies than it does on the in vivo setting. 33
There are a number of potential sources for endotoxins found in the periprosthetic tissue, including the bacterial biofilm on the surface of the implant, endotoxin contamination during the implant manufacture, and endotoxins derived from wear particles that can absorb LPS from systemic infections or the intestinal flora. 40 This notion reinforces the call for strict monitoring of endotoxin contamination during the evaluation of wear debris in in vitro models. 41
Endotoxin induced signaling pathways in vitro
The human body is unusually responsive to the biological effects of LPS as compared to other species and it is the response to LPS rather than the biological efficacy itself that causes the severe inflammatory reaction. 19 This also includes that the recognition of LPS and the downstream activated cell machinery does vary between human cells and, for example, mice cells, which greatly affects the comparability of studies on the biological effect of endotoxins. 42
One of the earliest events in sensing invading microbial pathogens is the activation of the Toll-like receptor (TLR) family and their interaction with comodulators. 43 These receptors play an important role in innate immunity and interaction with their respective ligands induces signaling cascades that lead to the secretion of various cytokines and chemokines.43,44 The possible development and course of sepsis is dependent on the activation of the innate immune system and the subsequently induced cellular machinery. 45 In the human body, TLR 4 was identified as the primary receptor for bacterial LPS. 46
The correct presentation of LPS to its receptor is mediated by two proteins.11,16,47 The LPS binding protein (LBP), an acute-phase plasma protein derived from the liver, binds LPS aggregates and delivers them in the form of monomers to a second protein, CD14.48,49 The biological activity of LPS is based on the interaction in the form of aggregates, since the encounter with monomer structures of LPS does not induce cytokine production in vivo. 11 Furthermore, LBP acts in a concentration-dependent manner, with low concentrations enhancing the activation of downstream receptors and high concentrations inhibiting stimulation.50,51 The glycoprotein CD14, expressed by myelomonocytic cells, transfers the LPS monomers to the extracellular adaptor protein MD-2, and can be present either in a soluble state or membrane bound as a glycosylphosphatidylinositol-anchored molecule.11,52 The resulting LPS-MD-2 complex then interacts with the cell surface-bound TLR 4 by forming dimeric structures. 19
Activation of TLR 4 results in the induction of two distinctive signaling pathways, the MyD88 and the TRIF pathway, subsequently causing the translocation of NF-κBeta to the nucleus. 46 This translocation is crucial to the activation of LPS responsive genes, that is, cytokines, chemokines, and acute-phase proteins. 19
To prevent the full induction of the biological response to endotoxins in the body, susceptibility can be reduced by the LPS interaction with innate antagonists in the blood stream. 42 These antagonists include the bactericidal/permeability increasing protein (BPI), which can neutralize LPS; apolipoproteins that reduce the production of proinflammatory cytokines; and Lactoferrin, which inhibits the binding of LPS to CD14 through competitive interaction.42,53
Biological effect of endotoxins
The chemical structure of the Lipid A moiety and the final concentration of LPS directly affect the interaction with its receptor TLR 4 and influence the biological efficacy.54–56 High concentrations of LPS induce toxic effects in the body, including irreversible shock and pyrogenicity, whereas low concentrations can act as stimulants for the immune system to withstand general bacterial and viral infections.56–58
In the body, LPS can increase cell proliferation, stimulate the secretion of cytokines and chemokines, along with causing a delay in wound healing.59–61 The secretion of bioactive mediators can be altered and endotoxins were shown to directly inhibit collagen production in osteoblasts.59–61 The primary biological effect of endotoxins includes the activation of immune cells, but subsequently also destabilizes bone homeostasis and disturbs the performance of biomaterials in vivo.44,59,60,62
Osteoclasts are derived from the hematopoietic system and can be influenced in their activity and survival by cytokines and other factors secreted from immune cells. 63 Bone resorption is known to be mediated by proinflammatory cytokines, such as interleukin (IL)-1, IL-6, and tumor necrosis factor-α (TNFα), and in vitro several of these cytokines were shown to similarly promote osteoblast functions.64–66 Osteoclast survival is prolonged in the presence of LPS, but the increase in cytokine secretion seems to be limited to macrophages, not terminally differentiated osteoclasts.67,68 In the presence of high numbers of titanium particles, macrophages additionally produce prostaglandin E2 (PGE2), an inflammatory mediator that can directly promote osteoclast differentiation. 69 Several regulatory mechanisms and pathways are shared between the immune and the musculoskeletal system, including the MyD88 signaling pathway induced by the activation of the TLRs, which was shown to influence osteoblast function and bone formation.70,71
Biomaterials
General aspects of biomaterial–endotoxin interaction
The interaction of endotoxins with biomaterials can be related to certain surface properties and material characteristics based on the chemical structure of LPS. Due to the negative charge of the phosphate groups and the hydrophobicity of the LPS molecule, endotoxins will readily interact with cationic or hydrophobic materials (Fig. 1). 72 Furthermore, LPS origin, pH of the environment, and the surface energy of the biomaterial can greatly affect the affinity for endotoxins.25,26
After implantation, the biological environment strongly influences the interaction of the biomaterial with bacterial endotoxins, as surface properties are quickly modified by the unspecific adsorption of matrix proteins. 73 Bacterial adhesion can be effectively averted by the combined action of the host defense system and the viable tissue, if the implant is rapidly colonized by tissue-derived cells. 73 The successful attachment of host cells is likewise dependent on the material properties. 74
The presence of endotoxins at the bone–implant interface can strongly affect the performance and the in vivo evaluation of a biomaterial. 75 Macrophages at the implantation site can prolong the inflammatory response by switching the set of secreted cytokines. 75 In addition, the foreign-body reaction to the biomaterial itself may be delayed in favor of the clearance of endotoxins from the implantation site. 75
Titanium, titanium alloys, and titanium wear debris
Implants made from titanium and titanium alloys have been the gold standard in orthopedic joint replacement for many years, based on their favorable mechanical and biological properties. 76 Friction at the bone–implant interface or between parts of the metal implant itself can lead to the generation of wear particles, which can decrease the quality and the life-time of the fixation. Particles derived from commercially pure titanium (cpTi) were shown to decrease collagen gene expression in osteoblasts depending on the size of the debris.77,78 A reduction in mineralization and extracellular matrix production was observed, and particles seemed to interfere with the cytoskeletal organization, ultimately preventing the successful differentiation of precursor cells into functional osteoblasts. 79 The suppression of the osteoblastic phenotype in combination with the activation of osteoclasts could explain the reduced bone formation in the presence of implant-derived wear particles.77,80 In addition, cell viability can be reduced with high particle numbers, but the contribution of titanium ions to the observed outcome could be excluded.69,77
The biological effect of wear particles shares many similarities to the response of cellular functions to endotoxins, including the induction of cytokine secretion and the attraction of osteoclast precursor cells. 5 Based on this resemblance, a number of studies compared the effect of endotoxin-contaminated and endotoxin-free particles, reaching uniform conclusions: endotoxin-contaminated wear particles induce greater cytokine secretion, increase osteoclast differentiation, and reduce osseointegration of the implant (Fig. 2).29,40,69,81,82
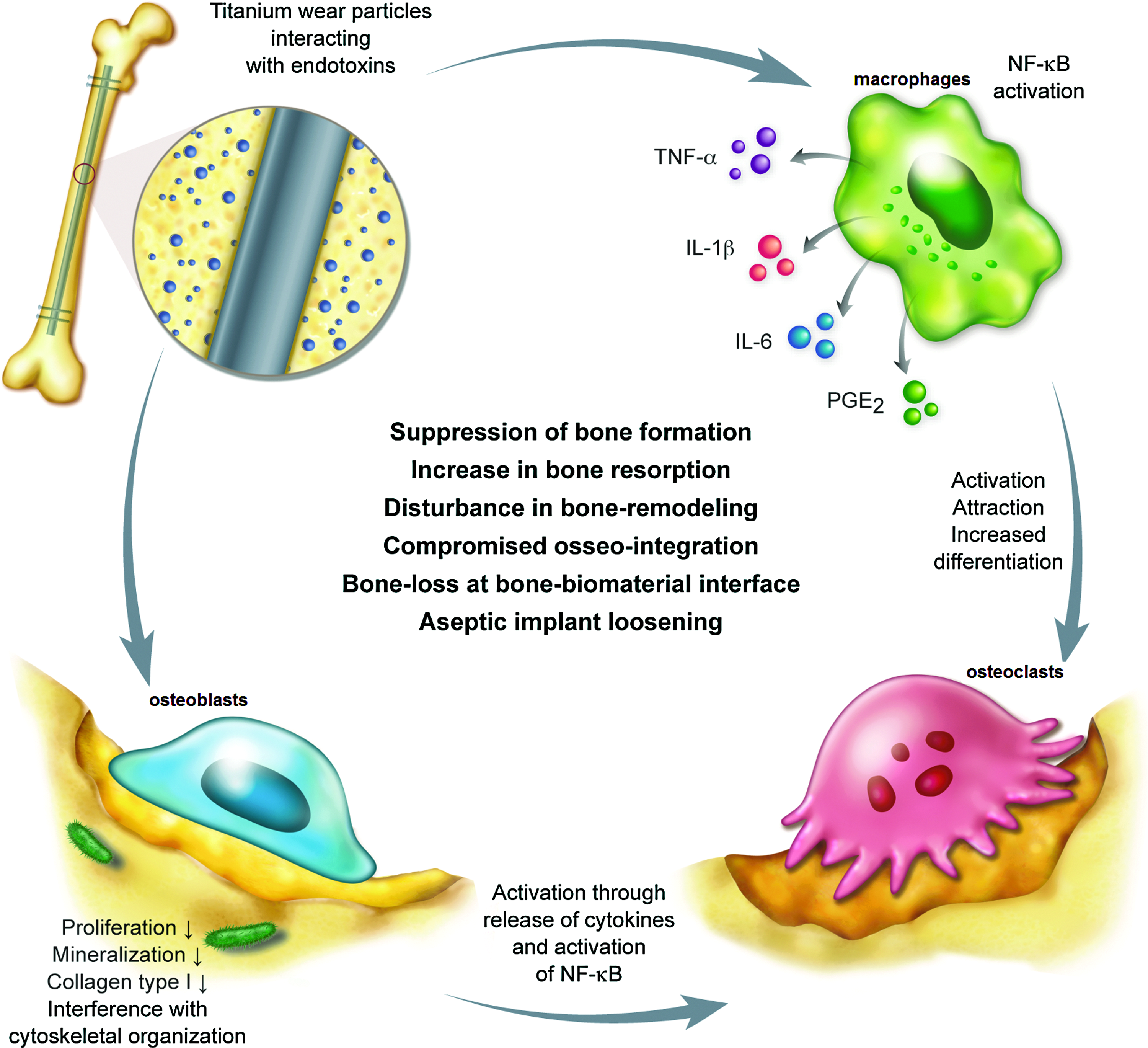
Biological effect of endotoxin-contaminated titanium wear particles on the bone environment. Titanium wear particles show high affinity for endotoxins, derived from the manufacturing process, the intestinal flora, dental procedures, or systemic bacterial infections. Endotoxins adherent to titanium surfaces are hardly cleared and display prolonged stimulatory effects. Macrophages located at the bone–biomaterial interface release cytokines, including tumor necrosis factor (TNF)-α, interleukin (IL)-1β, IL-6, and prostaglandin E2 (PGE2). These cytokines can activate, attract, and increase differentiation of osteoclast precursor cells. On the other hand, endotoxins affect osteoblastic cells by downregulating proliferation, mineralization, and matrix deposition. A disturbance in the osteoblast cytoskeletal organization can be observed. Osteoblasts in turn activate osteoclasts by secreting cytokines and activation of NF-κBeta. This circle of activation can ultimately result in the failure of the implant directly resulting from (1) suppression of new bone formation, (2) increase in bone resorption, (3) disturbance of the bone-remodeling process, (4) compromised osseointegration, (5) bone-loss at the bone–biomaterial interface, and (6) aseptic implant loosening. Color images available online at www.liebertpub.com/teb
In addition, titanium and titanium wear particles show high affinity for endotoxins that can adhere in substantial amounts to the surface.5,33,40,41,69,83,84 Systemic endotoxins originating from the intestinal flora, dental procedures, or bacterial infections are attracted to previously endotoxin-free implants and cpTi particles originating from them.29,40,85,86 The clearance of the pathogen, when absorbed to the titanium surface, is greatly reduced as compared to free endotoxins in the blood stream and might prolong the stimulatory effect. 69
The strong adherence of endotoxins to titanium and titanium alloys is based on bridging calcium ions, which may cause the induction of cytokine secretion in macrophages located at the bone–biomaterial interface, ultimately resulting in the failure of the implant. 83 The net concentration of endotoxin in the periprosthetic tissue may not be high enough to induce extensive cell activation per se, but could likely act in aggravating the negative biological effects attributed to wear particles. 41
Polyethylene particles
Polyethylene is commonly used in combination with titanium in joint replacement implants, but the particles originating from the friction between the metal and the plastic compound have been indicated in the pathology of osteolysis.87,88 In vitro studies with commercial ultrahigh molecular weight polyethylene particles showed an increase in the proliferation rate of MG63 osteoblasts and downregulation of differentiation-related attributes, that is, matrix production, alkaline phosphatase activity, and mineralization.89,90 Furthermore, polyethylene particles demonstrated high affinity for LPS, both during manufacture and following implantation of originally endotoxin-free particles.40,80,84
The presence of polyethylene particles severely reduces osseointegration at the bone–biomaterial interface and disturbs the bone remodeling process, with aggravating outcomes through the adsorption of endotoxins. 80
When covered by a fibrous tissue capsule, the polyethylene particles can come into contact with extracellular fluids, which can disperse the supramolecular LPS structures and support adsorption mechanisms. 80 As a consequence, an inflammatory reaction is elicited, which negatively affects bone formation and remodeling. 80
Interestingly, it was shown that endotoxins are cleared from originally contaminated polyethylene particles upon implantation, whereas endotoxin-free particles can accumulate endotoxins from the area surrounding the implant, implicating that the in vivo scenario is more complicated than previously thought.40,91
Chitosan
Chitosan is derived from chitin by removing at least 50% of the N-acetyl groups and is under extensive investigation as bioactive coating material for orthopedic implants and as a scaffold in tissue engineering.92,93 The deacetylation process introduces a cationic charge to the polymer and favors interactions with the negatively charged phosphate groups in LPS.92,94,95 The affinity for endotoxins is, in fact, so strong that crosslinked chitosan microfiltration membranes are used for the removal of endotoxin contamination from medical preparations. 96
Other studies showed that chitosan polymers can reduce LPS toxicity in HEK-293 cells that were transfected with LPS receptor complexes. 97 This activity was attributed to the close interaction with the endotoxin and a possible shielding mechanism of chitosan that prevents the interaction of endotoxins with cellular receptors.94,97
The chemical basis for endotoxin binding to chitosan polymers includes the formation of electrostatic interactions and hydrogen bonds, involving hydroxyl and carbonyl groups of both partners. 98 The number of charged groups, reflecting the degree of deacetylation, and the chain length of the polymer represent the basis for this interaction. 98
Seemingly contradicting, we showed in our research of human mesenchymal stem cells that chitooligosaccharides (derived from chitosan) do not reduce cytokine secretion in the presence of LPS and may in fact increase osteogenic differentiation, feigning excellent bioactivity performance of the potential biomaterial. 99 The difference between our study and the former lies in the cell culture models used for bioactivity evaluation. HEK-293 cells and some cells of the immune system, that is, monocytes and macrophages, express soluble or membrane-bound CD14, whereas human mesenchymal stem cells per definition lack the expression of this receptor. 100 CD14 acts in the transfer of LPS monomers to the extracellular adaptor protein MD-2, which in turn forms a complex with the cell surface-bound TLR 4 receptor, the primary endotoxin receptor in the human body.11,19,46,52 Based on this difference, we suggest that the reduction of endotoxin toxicity in the presence of chitosan polymers is dependent on the expression of cellular receptors, which are known to interact with LPS.
Other biomaterials
Literature about the interaction of endotoxins with other commonly used biomaterials and metals apart from titanium, polyethylene, and chitosan, is scarce, adding to the notion that the threat of endotoxin contamination is rarely considered.
Calcium phosphate ceramics, for example, hydroxyapatite and tricalcium phosphate, are used as biodegradable bone substitutes and bioactive coatings for metal implants. 101 Human monocytes, closely related to bone-resorbing osteoclasts, can degrade calcium phosphate ceramics, with increased activity in the presence of low levels of LPS. 62 This population of monocytes, activated by endotoxins, could constitute the precursor of osteoclastic cells and play an important role during biomaterial degradation. 62
Nickel–chromium–beryllium and type III gold alloys, employed in dental prostheses, were shown to interact with LPS depending on the chemistry of their surface oxide layer and other surface characteristics. 26
Membranes prepared from polyether polymer alloys or polymethylmethacrylate are clinically used as endotoxin filters for dialysis applications. 102 Affinity for endotoxins is dependent on the water contact angle, with efficient adsorption only on the hydrophobic side of the membrane. 102 Nevertheless, the risk for a biological response is still present, since the filter membranes do not retain smaller structures originating from the fragmentation of endotoxin aggregates. 102
The use of extracellular matrix products, for example, collagen, as support matrices for the growth of different cell types and in scaffolds for tissue engineering, is extensive, but the risk for endotoxin contamination is rarely considered. 103 Commercial collagen products can contain substantial amounts of endotoxins and using these preparations for the coating of tissue culture plates in the growth of dendritic cells can induce maturation and increased stimulatory capacity, independent of the contribution of collagen. 103
The same issues can be observed in gelatin preparations, where the removal of endotoxins constitutes a major problem. 104 The common use of high temperature, distillation, reverse osmosis, or endotoxin absorbance membranes is counter-indicated for gelatin preparations, as these methods can alter quality, performance, and composition. 104
Cellulose is another natural substance currently used in the field of biomaterials research for the production of scaffolds in tissue engineering. 105 Polyethylenimine-modified cellulose and diethylaminoethyl-cellulose, commonly used for ion-exchange chromatography purposes, are strongly basic anion-exchangers that have high affinity for endotoxins.106,107 Endotoxins bind with such high affinity to these modified cellulose preparations that they can efficiently replace the use of activated charcoal as endotoxin removal agents. 106 When macroporous particle preparations are used, even common issues related to the presence of high protein concentrations can be resolved. 106
The concern for endotoxin contamination in hydrogels, used as scaffolds in tissue engineering, as drug delivery systems, and biosensors, is small. Even though bacterial attachment is lower on hydrogels than on solid surfaces, bacterial contamination can result in complete colonization of the hydrogel surface. 108
Alginates are under investigation for cell encapsulation and transplantation purposes, but the commercially available pharmaceutical grade alginate preparations vary in their composition and contain diverging amounts of contaminants, for example, polyphenols, proteins, and LPS.109–111 The removal of endotoxins from alginate preparations is difficult and most current purification methods are considered inefficient.109,111,112 One of the most effective cleansing procedures includes chemical extraction with acetic acid and sodium citrate, 109 but the effect on the chemical structure of alginate should be carefully evaluated to ensure comparability and reproducibility. 111
Biomaterial Endotoxin Testing
In clinical applications of medical devices and parenteral drugs, endotoxins constitute a major health threat.3,4,113 The Food and Drug Administration (FDA) has therefore established recommendations for endotoxin measurements and safety limits that describe the allowed amount of contamination depending on the application site of the medical device.3,4,113 The current protocols include the immersion of the medical device in endotoxin-free water for at least 1 h at room temperature, and then measuring the endotoxin content in the extract.3,113 Current test systems include the kinetic limulus amebocyte lysate (LAL) method, based on a lysate from the horseshoe crab to detect biologically active LPS, and the rabbit pyrogen test, evaluating the temperature rise in rabbits associated with endotoxins and other pyrogens.113,114 The FDA guidelines recommend endotoxin levels below 0.5 EU/mL (20 EU/device) for medical devices and levels below 0.06 EU/mL (2.15 EU/device) for devices in contact with the cerebrospinal fluid.3,4
The use of extracts raises concern over the accuracy of endotoxin levels determined with the LAL method.3–5,33,82,114,115 The amount of LPS that is released into solution during the immersion of a medical device is strongly dependent on the properties of the biomaterial, including surface properties, wettability, pH, and more.4,82,115 In addition, the elution of hydrophobic LPS into a polar solvent like water is small. 4
The difficulty in accurately measuring endotoxin levels exponentially increases with specimens that are not transparent or have complex shapes, making direct determination of endotoxin levels on medical devices troublesome. 4 This creates serious issues in the field of biomaterials research, because the biological response to the presence of endotoxins in vitro can overrule the actual effect of the biomaterial.4,5 In addition, further studies showed that the endpoint LAL assay can only be used for the determination of cutoff values within a narrow concentration range, whereas the kinetic version of the assay introduces high error rates and may be more susceptible to influences from surface properties. 4
Another possibility to determine the extent of endotoxin contamination is the use of gas chromatography mass spectrometry methods. 116 Both the amount of active and inactive forms of endotoxins can be assessed simultaneously, including the gathering of information about the environmental origin of the contaminant. 116 This method, however, requires expensive equipment and specially trained personnel.
Removal of Biomaterial-Associated Endotoxins
Efficient methods for the removal of endotoxins from metallic implants often involve harsh conditions, for example, baking at 160°C for 24 h, or cycles of washing with alkali ethanol and 25% nitric acid for 18–20 h each.5,69 The sole use of nitric acid for titanium particles, as implemented by many manufacturers, was shown to be inefficient at removing adherent endotoxins from the implant surface. 5 It was suggested that the soaking of particles in 70% ethanol at room temperature for at least 48 h, followed by washes with PBS, is an efficient method to remove endotoxins from metal particles, 117 but based on the chemical structure of LPS, solubilization in ethanol or methanol seems unlikely.
A number of other methods are known for the removal of endotoxins118,119 and the most commonly used methods are summarized in Table 1. Ultrafiltration is effectively used for water decontamination, but is not recommended in the presence of proteins. 120 Anion exchangers can be applied to protein solutions, but negatively charged proteins may be lost in the process, whereas cationic proteins could interact with the endotoxin and reduce the removal capacity. 121 Membrane-based chromatography, another method for the removal of endotoxins from protein solutions, has its drawbacks in the limited binding capacity, but can remove trace levels of endotoxins and other contaminants. 119 Polymyxin B immobilized on Sepharose 4B is widely applied for protein solutions with improved results when nonionic detergents are used before separation.122,123 Dispersion by surfactants, that is, sodium dodecyl sulfate, or Triton X-100, is effective, but may require the subsequent removal of excess amounts of surfactant by dialysis.124,125 Washing medical devices and biomaterials with the neutral detergent Triton X-100 may potentially replace the use of alkali and acid, but the impact on the properties of the biomaterial needs further investigation. 80 Current research focuses on the application of two-phase micellar systems in the purification of biomaterials. 119 The method includes a water phase and a surfactant-rich phase, which attracts the endotoxins and following a phase-separation step, efficiently removes them from the biomaterial. 126 Several further methods for effective endotoxin removal from saline solutions and pharmaceuticals are available, for example, the use of activated charcoal, modified cellulose, and chitosan microfiltration membranes.96,127
LPS, lipopolysaccharides; S-LPS, smooth LPS; R-LPS, rough LPS; SDS-PAGE, sodium dodecyl sulfate polyacrylamide gel electrophoresis.
Most of these treatments, however, are not suitable for polymeric biomaterials, because the aggressive methods may damage polymer structures and alter surface properties, changing product performance, and reducing product life-span.4,80,128 Alternative milder treatments are required that ensure penetration of small pores and complex polymeric structures. 128 Ultimately, the development of specific methods for endotoxin removal in a particular biomaterial, to account for the chemical structure and surface properties, may become necessary.
Final Remarks
The biological effects of endotoxins on the human body are extensive and strict regulations are in place to reduce the risk of adverse health effects from medical devices.3,4,113 The safety limits recommended by the FDA and the United Service Organization (USO) take into account the different concentrations of endotoxins, eliciting biological effects depending on the implantation site.3–5,28,55,113 Despite the concern about the measurement of endotoxins in extracts of water-immersed biomaterials, based on the unknown amount of endotoxins that is released into the solution, the regulations have proven sufficient over the years for in vivo applications. 6
For the in vitro evaluation of biomaterials, however, these recommendations may be inadequate. 3 Depending on the cell type used, the amount of endotoxin that can be tolerated without biological response may be different and is insufficiently specified at the moment.59,60,112 Furthermore, there is a lack of standard guidelines for the in vitro evaluation of biomaterials, including the need for regular endotoxin testing and publication of all values along with biomaterial characteristics (Table 2). 3
FDA, Food and Drug Administration.
Footnotes
Acknowledgments
We like to acknowledge the Technology Development Fund and the Icelandic Research Fund, managed by the Icelandic Centre for Research and the Landspitali University Hospital research fund for funding.
Disclosure Statement
No competing financial interests exist.