
Abstract
The distraction osteogenesis (DO) technique has been used worldwide to treat many complex orthopedic and craniofacial conditions. One limitation of this technique is the long time of fixator needs to be left in place until the bone is completely consolidated. Various biophysical, mechanical, and biological methods have been investigated to accelerate bone regeneration during DO. Several growth factors (GFs) are known to enhance bone regeneration such as bone morphogenic proteins, transforming growth factor beta, fibroblast growth factor, insulin growth factor, vascular endothelial growth factor, and platelet-derived growth factor. These GFs are known to stimulate cellular growth, proliferation, migration, and differentiation. In this review, an extensive overview of these GFs development and applications on acceleration of bone regeneration in the context of DO is discussed. Current challenges and alternative tissue engineering techniques to address the delivery and sustain release of these factors are also discussed. Finally, we highlighted our view regarding the remaining questions and future research directions.
Introduction
Previous animal experiments have found successful distraction is based on the stability of the fixator, rate and rhythm of the gradual distraction, and degree of damage to local soft tissue.6–8 Although these studies have described the technical principles to achieve a successful outcome, the molecular mechanisms responsible for these processes were essentially undetermined until were primarily studied by Sato et al. and Rowe et al.9,10
Application of various growth factors (GFs) is one potential approach of other various modalities to enhance bone regeneration in DO models (Fig. 1).11–29
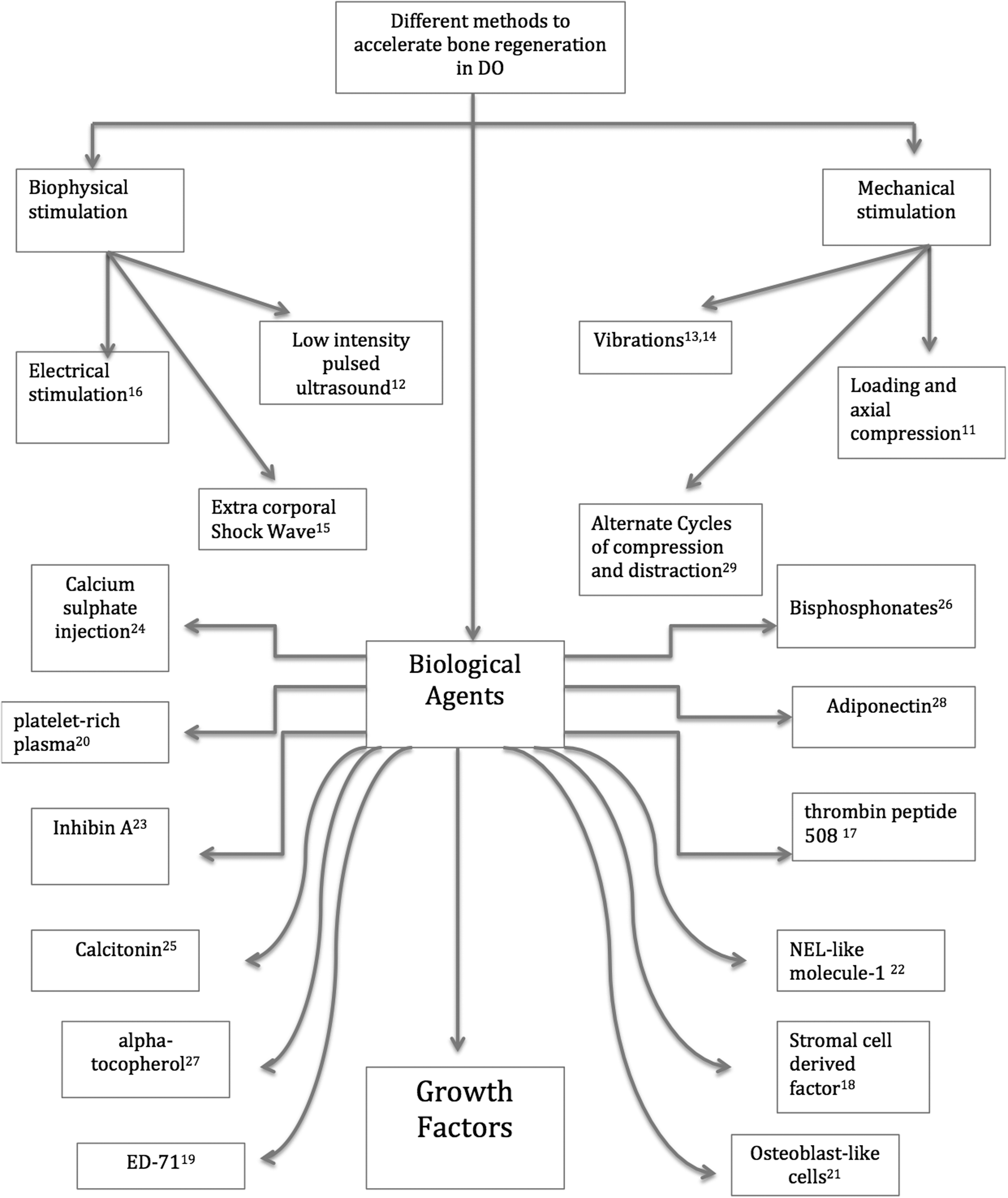
Illustrating different methods to accelerate bone regeneration during distraction osteogenesis. DO, distraction osteogenesis.
Several GFs are known to enhance bone regeneration such as the transforming growth factor beta (TGF-b1), fibroblast growth factor (FGF), insulin growth factor (IGF), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and bone morphogenic proteins (BMPs). These GFs are known to stimulate cellular growth, proliferation, migration, and differentiation. 30 They are released from the extracellular matrix after injury to contribute in the bone regeneration process. The interaction between various GFs and surface receptors on the target cells (adult mesenchymal stem cells, osteoblasts, fibroblasts, endothelial cells, and epidermal cells) activates production of proteins needed for the regenerative processes such as cellular proliferation, matrix formation, osteoid production, and collagen synthesis. 31
While the basic biological functions of certain GFs and their endogenic roles in tissue development and regenerative process have relatively been well studied, the use of GFs in a tissue-engineering regime has recently gained significant interest. Interference with any of these GF pathways will determine whether or not to accelerate the bone regenerative process.
In this article, we will discuss the aforementioned GFs that play an important role on acceleration of the bone regeneration process in the DO model, current challenges, and the future research directions.
Bone Morphogenic Proteins
In 1965, Dr. Marshall Urtist has introduced the term of bone morphogeinc proteins. He demonstrated that certain substances (BMPs) in the demineralized bone matrix could induce ectopic bone formation when implanted in extraskeletal sites in rodents. 32 Since then, more than 20 BMPs have been described in the literature. 33 It belongs to the TGF-B superfamily and has a critical role in stimulating bone regeneration leading to osteogenesis, chondrogensis, angiogenesis, and upregulation of other GFs, cytokines, and synthesis of the extracellular matrix. 34 They are also responsible for matrix formation and osteoblast formation and it is the only osteoconductive ones that play a role in the early differentiation process of undifferentiated mesenchymal cells. 35 Interestingly, Lou et al. have documented the ability of BMP-2 to stimulate mesenchymal cell proliferation in vitro under adenovirus-mediated BMP gene transfer. 36
BMP receptors (BMPRs) functioned as mediators for BMP signaling. These signals are transmitted by Smad proteins. 35 The action of BMPs is tempered by extracellular BMP-binding proteins such as noggin, chordin, dan family and twisted gastrulation, transmembrane BMP pseudoreceptors (Bambi), intracellular BMP antagonists (Smad 6/7), and intranuclear substance (c-SKI and Smurf1/2).37,38 In addition, BMP-3 has been also identified as a BMPR antagonist that blocks the BMP activity. 39 Furthermore, other GFs can also interact with the BMP action. For instance, the hepatocyte growth factor (HGF) was found to inhibit the BMP-2 action via activation of ERK1/2, which subsequently suppresses the BMP-2 Smad axis. 40 In contrast, the epidermal growth factor (EGF) enhanced significantly the action of BMP-2 and BMP-7 in vitro and, therefore, promoted the osteoblast growth. 41
BMPs are available in two forms, either heterodimers or homodimers. Previous reports have shown that heterodimer forms (BMP 2/7 and BMP 2/6) have a better effect on bone regeneration by 20 folds in vitro and 5 to 10 folds in vivo when compared to homodimers. 42 Of 20 BMPs, BMP-2, −4, −6, −7, and −9 have the greatest osteoinductive potentials in vitro.43,44
BMP expression and immunohistochemical localization of protein-signaling Smads have been investigated in the DO model. Sato et al. found high expression of BMP-2 and BMP-4 during the distraction phase in a DO rat model. 9 In our laboratory, we have investigated the temporal and spatial expression of BMP 2, 4, and 7 proteins during DO of tibiae in a rabbit model using immunohistochemistry, and interestingly found intense staining for these BMPs in the latency period and it was maintained during the entire distraction phase and once the distraction has stopped, BMP (2, 4, and 7) expression gradually disappears. 45 Similar results were found when we investigated the mandibular DO in rabbits except that the expression of BMP 7 was limited during the distraction phase. 46 Furthermore, delayed bone regeneration in the DO model was observed in BMP-2 knocked out mice when compared to the control group. 47 This confirmed the critical role of endogenous BMPs in the DO bone regenerative process. We also investigated the expression of receptor-regulated Smad 1, 5, and 8, which showed a significant increase mainly in the distraction phase, while Smad 6 and 7 showed high expression in the consolidation phase. 48
Most of the recombinant BMP-2 and −7 applications in DO models have shown promising results from the animal data49–54 (Table 1). However, the clinical use of systemic and local BMPs is limited. When injected systemically, the half-life of BMPs is short and rapidly metabolized by the liver,55–57 while when injected locally its limitations could be explained by the short resident time in tissues and probably insufficient numbers of responding cells.58,59 Therefore, large doses are required to reach an optimal biological response. This is associated with unknown side effects and huge costs. 60 Other limitations for using BMPs in humans include possible neoplastic risk, potential teratologic sequences, osteoclastic activation, and unknown consequences on skeletally immature patients.61–63
BMP, bone morphogenic protein; DO, distraction osteogenesis.
We can overcome these challenges by finding an alternative strategy such as intrinsically stimulate BMP expression or developing an appropriate delivery system will allow local sustained release of BMPs in low doses.
In addition, administration of more than one exogenous BMP with respect to its spatiotemporal expression might accelerate the bone regeneration process during DO. Up to date, various tissue-engineering techniques have been utilized to enhance BMP action during DO, including gene therapy, coadministration of the bioactive factor, and protein therapy64–71 (Table 2).
ACS, absorbable type I collagen sponge; Adbmp-2, adenovirus containing the gene for BMP; TCP/HA, tri-calcium phosphate/hydroxyapatite; MSCs, mesenchymal stem cells; Nell-1, NEL-like molecule-1.
Several reports have emphasized the role of inhibiting the BMP antagonist in bone repair as a potential method to accelerate bone formation72–78 (Table 3). In the context of DO, we have previously reported that BMP antagonists such as of BMP-3, chordin, inhibin, and noggin showed significant expression during DO. 79 However, the role of inhibiting the BMP antagonist has not been investigated yet in the DO model.
OAZ, smad-interacting transcription cofactor; ROS, rate osteosarcoma.
Transforming Growth Factor-B
TGF-Bs are 25-kDa proteins. Three isoforms have been found (TGF-b1, b2, and b3). TGF-Bs are potent osteoblast chemoattractants, have mitogenic effects on osteoblast precursors produced by osteoblasts in culture, and are expressed by osteoblasts and osteoblast precursors during endochondral ossification. 80 TGF-Bs play an integral part of collagen production and upregulate the expression of noncollagenous ECM proteins implicated in the regulation of bone turnover and mineralization. 81 The most abundant GF of the bone matrix is TGF-b1, which has a wide range of cellular activities, including control of proliferation and expression of the differentiated phenotype of several cell types specific to bone, among them, mesenchymal precursor cells, chondrocytes, osteoblasts, and osteoclasts. 81
The spatial and temporal expression of TGF-b1 were investigated in mandibular DO in the rat model, and demonstrated an increase of TGF-b1 expression at the end of the latency period and shortly after the initiation of distraction and remain elevated until 4 weeks of the consolidation period when compared to sham-operated animals. 80 Yeung et al. have also found strong expression of TGF-b1 at the osteoblast and osteocyte in the newly formed callus and remained elevated throughout the distraction phase. 82
The effect of TGF-b1 application has shown promising results in fracture healing and bone repair in various animal experiments.83–86 However, few studies have reported the role of exogenous TGF-b1 in the DO model.87,88 In our laboratory, TGF-b1 treatment had no detectable effect on the bone mineral density or histologically determined bone volume in the distraction gap. In addition, load to failure in uniaxial tension was lower in TGF-b1-treated rabbits. 87 In contrary, Ozakan et al. found that locally applied TGF-b1 improves the mineral density of the distraction gap and the load to failure, but no histomorphometric difference was detected between the treatment and control groups. 88 They have also noted downregulation of the TGF-b1 type 2 receptors in the TGF-b1-injected group. The authors have justified this discrepancy by the lack of a specific stain to the type 1 receptor in their experiment, which likely will show upregulation secondary to the exogenous TGF-B1 administration. However, further experiments are needed to draw a clear conclusion regarding the use of exogenous TGF-b1 in the DO models.
Insulin Growth Factor-I
The IGF plays an integral role in the cellular growth, metabolism, differentiation, and cell cycle progression. 89 The IGF-I is also a potent chemotactic factor for osteoblasts. Interestingly, when a mouse IGF-I was neutralized, delayed osteoblast monolayer wound healing and cellular polarizations were observed, but this effect reversed when the human IGF-I was added. 90 In addition, when a conditional deletion of the IGF-I was performed in mice, a significant decrease in the femoral size and bone formation was noted. 91 Furthermore, osteoblast-specific knockout mice have also shown a decrease in cancellous bone volume, connectivity, and trabecular number, and an increase in trabecular spacing. 92 These studies have established the critical role of the IGF-I in bone regeneration.
Schumacher et al. have investigated IGF-I expression in tibiae DO in rabbits and found that periosteal IGF-I increased after 2 weeks of distraction and ceased gradually when the distraction stopped. 93 Eingartner et al. have also found strong expression of the IGF-I in the distraction callus of 3 patients. 94 Furthermore, the administration of IGF-1 during mandibular DO in rabbits showed a significant increase in the osteoblastic activity in both rapid and slow distraction rates. 95 Bernstein et al. have investigated the local application of enriched polylactide membranes (IGF-I and TGF-b1) in tibiae DO in a sheep model, although no statistical significance was found, a higher relative bone area was observed when compared to groups treated with an uncoated membrane or packing of the osteotomy defect with cancellous bone. 96 Although these results are encouraging, further experiments are required to determine when and how the IGF-I should be given during DO procedures.
Fibroblast Growth Factor
It is known to compromise 22 members. FGFs have multiple roles, including cell proliferation, migration, differentiation, and angiogenesis. These have been used for the regeneration of damaged tissues, including skin, blood vessel, muscle, adipose, tendon, ligament, cartilage, bone, tooth, and nerve. It functions through binding into the FGF receptors, which mainly stimulated through the RAS/MAP kinase pathway. 97 The FGF2 (bFGF) is recognized as a potent mitogen for a variety of mesenchymal cells. 98 The impact of locally applied bFGF injection under physiological conditions and osteoporotic-induced rabbits was investigated, the best results in terms of enhancing bone formation were found when a 400 mg or greater was given.99,100 Kato et al. also found that bFGF injection will increase the volume and mineral content of newly formed bone in long bone defect in rabbits in a dose-depended manner with significant results seen at 100 mg or greater. 101 Interestingly, the FGF-2 use in the fracture healing has been translated to the clinic. In a prospective randomized double-blind placebo-controlled multicenter trial that included 71 patients, local application of rhFGF2 hydrogel has proven to be effective in terms of accelerating fresh fracture healing. 102
The basic FGF plays an important role in neovascularization during DO and its expression found to be strongest from 0 to 7 days after the end of distraction in mandibular DO in a goat model, 103 while bFGF expression in long bone DO in the goat model was highest during the distraction phase. 104 Local applications of the bFGF in tibiae DO in rabbits showed significant enhancement in bone formation as early as 2 weeks after bFGF injection when compared with the control group. 105 Furthermore, the use of combined rhFGF-2 and b-tricalcium phosphate (b-TCP) have reduced the treatment period for DO and accelerated bone formation. 106 The basic FGF seems to be a promising agent. However, further experiments are required to establish the optimal time, dose, and delivery system of the bFGF during DO procedures.
Vascular Endothelial Growth Factor
The VEGF represents a critical rate-limiting step in the physiological angiogenesis. 107 The family of VEGF-related molecules includes seven mammalian members: VEGF-A, placenta growth factor, and VEGF-B, -C, -D, -E, and -F. The biological functions of VEGF are mediated by at least three corresponding receptors: VEGFR-1/Flt-1, VEGFR-2/Flk-1, VEGFR-3/Flt-4 and 2 coreceptors of neuropilin and heparan sulfate proteoglycans. 108 VEGF-A is most predominately involved in the bone regenerative process and several studies have demonstrated its role in the regulation of chondrocyte activities, chondroblast/osteoclast activities, and osteoblast activities. 108 Several ways have been described to be involved in VEGF-A upregulation and gene expression such as BMPs, hypoxia-induced factor (HIF), TGF-B1, tumor necrosis factor alpha, and hormones. 108
Local application of VEGF in severe soft tissue trauma with fracture and bone segment defects in rabbits has shown promising results in terms of enhancing bone regeneration.109,110
VEGF mRNA expression has been investigated in femur DO in rats and found to be maximal during the active distraction phase. 111 However, in mandibular DO in goats, VEGF expression was highest from 0 to 7 days after the end of distraction. 103 Warren et al. have also found VEGF expression remains elevated throughout both distraction and consolidation phase in mandibular DO in rats. 112
There is no doubt that VEGF-A plays a central role of angiogenesis during DO. 113 Ohashi et al. have shown that better preservation of blood vessels during DO will lead to a better mineralization of the distracted callus. 114 It has been also shown that the rapid distraction rate can lead to a decrease in the VEGF and other angiogenic GFs; thus, administration of these factors might improve bone healing at these rapid distraction rates. 115 Surprisingly, Eckardt et al. did not find a significant difference in the bone mineral content, torsional stiffness, and histomorphometric parameters after local application of the VEGF in tibiae DO in rabbits. 116 The authors have suggested that high endogenous VEGF concentrations are expected during DO; thus, additional delivery of the exogenous VEGF would have no effect due to optimal endogenous DO signaling. Wan et al. have demonstrated that activation of the HIF-1 alpha pathway stimulates bone regeneration in DO; they also emphasize the importance of the HIF-1 alpha pathway in angiogenesis and its critical role in VEGF stimulation. 117 The authors suggested that the VEGF alone might be not sufficient to stimulate bone formation because HIFs are upstream of the entire angiogenic cascade and they would be expected to induce additional factors that are required for forming a new intact vascular network in the injured bone.
Platelet-Derived Growth Factor
The family of PDGF polypeptide GFs includes PDGF-A, B, C, and D, encoded by four genes located on different chromosomes. The PDGF has stimulatory effects as a potent mitogen and chemoattractant for various mesenchymal cells, including osteogenic cells. 118 The PDGFs signal through two cell-surface receptors, PDGF-R alpha and PDGF-R beta, which are capable of forming homodimers and heterodimers. 119 PDGF-BB is considered the universal PDGF isoform because of its ability to bind to all known PDGF receptor isotypes. The PDGF can modulate the bone regenerative process through other GFs, in which, it increases VEGF expression, enhances IGF-I signaling, and increases expression of some BMP antagonists. 118
Local application of PDGF-BB was investigated in the context of fracture healing and has shown its ability to stimulate the bone regenerative process.120,121 Moore et al. have investigated the role of PDGF-BB injections in femora DO in rats and found significant new bone formation in a dose-dependent manner at midconsolidation phase as well as union rate when compared to the control group. 122 Numerous preclinical and clinical studies have proven the safety of recombinant human platelet-derived growth factor-BB applications. 123 One drawback is that the PDGF has a short half-life of ∼30 min when circulating in the blood; thus, it is crucial to be combined with an appropriate delivery system. 118 However, although there is a paucity of data for using the PDGF in the DO context, it seems to be a promising candidate for future DO research and applications.
Platelet-Rich Plasma
Since the identification of platelet-secreted GFs, the use and development of platelet-rich plasma (PRP) gained significant interest.124,125 PRP is an autologous source of various GFs such as PDGF, TGFb1-b2, FGF, VEGF, IGF, HGF, EGF, and platelet-activating factor-4.126,127 These GFs are secreted secondary to the degranulation of alpha granules in the platelets. PRP also contain cell adhesion molecules (fibrin, fibronectin, and vitronectin), which act as a scaffold for osteoconduction. 128 In addition to that, PRP contain leukocytes, which provide an additional source of GFs. 124 The one major advantage of PRP is the autologous preparation, therefore, no risks about the transmission of diseases or immunogenic reactions.
PRP has been utilized in various domains, including skin ulcers, osteoporosis, bone regeneration tissue, and soft tissue healing.129–132 The efficacy of PRP in bone healing has been debated. Robert Marx has argued that some studies did not show the efficacy of the PRP likely because they had either small sample size, used damaged platelet, and may have not activated the platelets. 128
The application of PRP has been studied in animal DO models. Kawasumi et al. have shown that cellular proliferation was enhanced in all PRP groups when cultured with bone marrow cells in a dose-dependent manner in the rat DO model. 133 Choi et al. have found that the proliferation of alveolar bone cells can be suppressed or stimulated by PRP. 134 Recently, Kitoh et al. have observed a shorter bone healing time when the expanded bone marrow cells and PRP were injected into the callus bone in 11 patients during limb lengthening. 135 Furthermore, Latalski et al. have echoed the same findings when the PRP was applied from autogenous sources alone to enhance bone healing during DO procedures. 136 Although these are promising results, future studies are required for dose optimization, methods, and rhythm of administration.
Considerations for Delivery Systems and Other Alternatives
There is no doubt that the mode of delivery will enhance the efficacy of using exogenous GFs.137,138 The ideal delivery system has to be biocompatible, has predictable biodegradability, low immunogenicity and antigenicity while preserving the GF bioactivity. It should also have the ability to control and meter/tailor protein release at an effective dose, for the appropriate period of time while considering the defect of anatomical site, size and vascularity, malleability, ease of manufacture, safety, stability, sterility, availability and cost-effectiveness. 139
Most osteogenic and endogenous GFs are expressed during the early stages of the bone regenerative process. Therefore, it is critical to be delivered in the appropriate time.
Extensive research has been performed investigating various BMP delivery systems, including the use of natural polymers, synthetic polymers, inorganic materials, and composites.140–144 However, each delivery system has limitations (Table 4).
Modified and adapted from Haidar et al. 140
CPC, calcium phosphate cements.
In the past decade, intensive research was performed for the use of nanoparticle formulation in anticancer drugs, as many advantages were found in nanoparticles such as small size, long shelf life, ability to interact with drugs, longer stay in the circulation, and ability to cross the epithelial membranes.145–147 These are attractable properties for tissue engineering, which can be utilized to develop a promising GF delivery system.148,149 Recently in our laboratory, we have developed a novel hybrid nanoparticle core shell release-controlled delivery system, the core is composed of charged large unilamellar liposomes and the shell is constructed through the L-b-L self-assembly of alternating layers of sodium alginate and chitosan. 150 This was proven to be safe and biocompatible and also has the capability of releasing a range of BMP-7 concentrations up to 45 days.151,152 Moreover, a single injection of nanoparticles loaded with low doses of BMP-7 have shown enhancement of bone regeneration in the DO model. 66
Gene therapy also is another attractable field to study. Although few studies have shown promising results when administrated adenovirus containing the gene of BMP-2 in the DO model,65,67 further experiments are required to examine its safety and efficacy.
Administration of multiple GFs is also a potential approach to enhance the bone regenerative process during DO. Several studies have demonstrated promising results when dual GFs were administrated. Coadministration of BMP-2 and Nell-1 have shown promising results in a long DO animal model. 71 Similarly, cotransfection with a combination of BMP-7 and IGF has promoted osteoblast cell differentiation in vitro. 153 However, Vanau et al. have reported decrease bone formation when BMP-2 and bFGF were coadministrated in a fracture-healing model. 154 Therefore, using this technique should consider mimicking the natural bone regeneration cascade to obtain the desired results. 155 It has been hypothesized that inserting a scaffold with a controllable multiple-gene delivery system can arrange the sequential expression of GFs, thus, manipulating cell proliferation, chemotactic properties, differentiation, and matrix synthesis. 156 The ultimate goal is to find what are the optimal GF combinations to accelerate bone regeneration during DO.
Moreover, several reports have proven the safety of administrating exogenous FGF-2 and PDGF-BB in human.102,123 This should encourage scientists to conduct further experiments to examine its efficacy with regard to dosing, timing, and delivery system in the context of DO.
Conclusion
Most of the current osteogenic GF applications in DO have relatively satisfactory outcomes in vivo studies. However, there are some limitations to its use secondary to the lack of an optimal delivery system, controversial reports about its efficacy (e.g., TGF-b1), safety concerns, and lack of data that provide the full map of how these factors interact with each other during DO. Future research can be directed to identify the cross talk between various GFs during DO, investigate the role of endogenous stimulation of the GFs (e.g., inhibiting BMP antagonists), carefully administrate multiple GFs (e.g., EGF/BMP-2 or 7) or multiple BMPs (e.g., 2/7) mimicking the natural spatiotemporal expressions during DO, and optimizing the delivery systems to determine the appropriate time and dose during DO procedures.
Footnotes
Disclosure Statement
None of the authors received payments or services, either directly or indirectly (i.e., via his institution), from a third party in support of any aspect of this work.