
Abstract
There is great clinical demand for synthetic vascular grafts with improved long-term efficacy. The ideal vascular conduit is easily implanted, nonthrombogenic, biocompatible, resists aneurysmal dilatation, and ultimately degrades or is assimilated as the patient remodels the graft into tissue resembling native vessel. The field of vascular tissue engineering offers an opportunity to design the ideal synthetic graft, and researchers have evaluated a variety of methods and materials for use in graft construction. Electrospinning is one method that has received considerable attention within tissue engineering for constructing so-called tissue scaffolds. Tissue scaffolds are temporary, porous structures which are commonly composed of bioresorbable polymers that promote native tissue ingrowth and have degradation kinetics compatible with a patient's rate of extracellular matrix production in order to successfully transit from synthetic conduits into neovessels. In this review, we summarize the history of tissue-engineered vascular grafts (TEVG), focusing on scaffolds generated by the electrospinning process, and discuss in vivo applications. We review the materials commonly employed in this approach and the preliminary results after implantation in animal models in order to gauge clinical viability of the electrospinning process for TEVG construction. Scientists have studied electrospinning technology for decades, but only recently has it been orthotopically evaluated in animal models such as TEVG. Advantages of electrospun TEVG include ease of construction, favorable cellular interactions, control of scaffold features such as fiber diameter and pore size, and the ability to choose from a variety of polymers possessing a range of mechanical and chemical properties and degradation kinetics. Given its advantages, electrospinning technology merits investigation for use in TEVG, but an emphasis on long-term in vivo evaluation is required before its role in clinical vascular tissue engineering can be realized.
Introduction
T
For most vascular bypass procedures, autologous vascular tissue is the surgeon's graft of choice. Autologous tissue is advantageous in that it has a living, nonthrombogenic endothelium, is biocompatible, and has favorable surgical handling characteristics. Examples of harvested vessels for vascular grafting include internal mammary artery, radial artery, and greater saphenous vein, and all are commonly used for coronary artery bypass surgery. Unfortunately, many patients lack suitable donor tissue due to either inherent disease or harvest during previous operations. In these instances, surgeons should employ synthetic vascular conduits such as expanded polytetrafluoroethylene (ePTFE, i.e., Gortex) or poly(ethylene terephthalate) (PET, i.e., Dacron®). 3 These two materials have been clinically used since 1956 and have been validated as successful conduits for large caliber arteries in which high flow and low resistance leads to low rates of thrombosis and excellent rates of long-term patency. 4
Despite the ready availability and clinical efficacy of Dacron and Gortex grafts in specific applications, there is much room for improvement. The results of synthetic vascular grafts for bypass of small-diameter (<6 mm) arteries have been uniformly poor with reported patency rates of 40% at 6 months and 25% at 3 years. 5 These smaller conduits are more vulnerable to failure secondary to thrombus formation or intimal hyperplasia and are, thus, precluded in coronary artery bypass and in distal lower extremity re-vascularization procedures. Given the burden of vascular disease, there is an obvious need for the development of a small-diameter vascular conduit with results that approach or exceed those of autologous vessel bypass procedures. Another important consideration in the use of these nondegradable synthetic grafts is their lack of capacity for growth, resulting in unacceptable or unproven long-term outcomes and a chronic risk of infection. This is of particular concern for pediatric patients, who often undergo vascular graft surgery at a young age. The inability of a synthetic graft to adapt to the patients' natural growth often necessitates reoperation with associated increases in morbidity and mortality. The ideal vascular conduit would eliminate these concerns by integrating with the patient's native tissue to restore physiologic function: the ability to grow, to remodel, to respond to vasoactive hormones, and to rebuild after injury. In addition, this conduit should be nonthrombogenic and resistant to aneurysmal dilatation or rupture. The ability to create such a graft on demand and tailored to an individual patient would eliminate the issue of supply that currently limits the use of autologous tissue. The field of tissue-engineered vascular grafts (TEVG) focuses on the development of a conduit with these goals in mind.
Tissue-Engineered Vascular Grafts
The definition of tissue engineering is the fabrication of substitute materials for defect or injury that restore biological function and become integrated into the living tissue of the patient. 6 In vascular tissue engineering, grafts are constructed or grown in vitro and subsequently surgically implanted. All TEVG can be described as either scaffold based or scaffold free, with the former relying on a temporary scaffold structure that is ultimately replaced by neotissue with characteristics similar to native vessels. Both approaches aim at restoring full biological vascular function, including the ability to grow and remodel throughout the course of the host's lifetime.
Scaffold-free systems make use of in vitro culture and tissue self-assembly to produce biological material akin to autologous tissue. Weinberg and Bell produced the first TEVG in vitro by incubating tubular collagen gels with smooth muscle cells (SMCs), fibroblasts, and an endothelial luminal layer. 7 Despite its significance in advancing the field, the TEVG was mechanically unstable and unfit for in vivo experimentation. L'Heureux et al. pioneered the in vitro culture of layered cell sheets composed of a functional endothelium, a medial layer of SMCs, and an adventitial layer of skin fibroblasts, which was then physically rolled to create a vascular conduit. 8 In 2004, McAllister and L'Heureux implanted a TEVG constructed from cultured fibroblasts and endothelial cells (ECs) as a graft for hemodialysis access.9,10 Their results on the first 10 arteriovenous graft implantations in humans showed 3 TEVG failures within 4 months due to thrombosis and aneurysm, all of which required explantation. 11 While the preliminary clinical outcomes have shown reasonable patency rates, the production process is complex and requires a venous biopsy and weeks of in vitro culture, resulting in increased costs and limited applications.
The use of scaffold-based systems has become the prevailing strategy with multiple technologies approaching or already in clinical use. With regard to tissue engineering, a scaffold is a biomaterial that temporarily supports three-dimensional (3D) cell culture during neotissue formation; the material degrades over time and is ultimately resorbed and eliminated through natural pathways. This class of materials is commonly referred to as bioresorbable. In 1982, Greisler implanted degradable polymer scaffolds as arterial grafts in rabbits and demonstrated cellular attachment and infiltration of the scaffold. 12 Twelve months after implantation, the polymer scaffold was fully degraded and resorbed, leaving only functional biological tissue resembling that of native artery.12,13 This seminal work proved that a highly porous, biocompatible, degradable vascular graft—acting as a temporary tissue scaffold—could harness the biologic regenerative capacity in vivo to remodel the synthetic construct into functional tissue in situ.
Niklason et al. grew arteries in vitro by culturing SMCs on a degradable scaffold of poly(glycolic acid) (PGA) fabric in a pulsatile bioreactor. 14 This technique is advantageous in that it is done in a controlled environment, mimics the physiologic milieu, encourages production of robust extracellular matrix (ECM), and offers the ability to manipulate culture conditions. Further, the TEVG can be decellularized and stored at 4°C, thereby offering a model for an off-the-shelf TEVG. Though cost and complexity of this approach remain high, a recent pilot study reported a patency of 88% for more than 6 months when evaluated as an arteriovenous graft in a baboon model. 3
In a similar manner, Kaushal et al. also utilized the process of decellularization to produce a scaffold onto which autologous cells could be seeded. In their study in the year 2001, decellularized porcine iliac vessels were seeded with autologous ovine ECs and then implanted into ovine carotid arteries. 15 The decellularized TEVG constructs with seeded endothelial surfaces remained patent whereas the unseeded control group occluded within 15 days, demonstrating in this instance that decellularized vessels alone are unsatisfactory for use as vascular grafts without endothelialization or further modification. This conclusion tempered the enthusiasm for decellularized xenografts and homografts as viable TEVGs in small-diameter applications.
The use of scaffold-based systems reached a significant milestone in 2001 when Shin'oka et al. reported the first successful clinical implantation of a degradable vascular graft seeded with autologous bone marrow-derived mononuclear cells. In that study, TEVGs were implanted in 26 pediatric patients as an extracardiac total cavo-pulmonary connections in patients with single ventricle anomalies. 16 Long-term efficacy of these TEVGs showed no evidence of aneurysm formation, graft rupture, graft infection, or ectopic calcification.17,18 These cell-seeded degradable grafts supported a robust influx of host cells that deposited and remodeled an ECM which was capable of replacing the biomechanical properties of the degrading scaffold. Ultimately, the cell-seeded scaffolds transformed into polymer-free neovessels that were capable of growth and remodeling with histologic similarity to native vessels. This clinical application demonstrated two important points in tissue engineering: that degradable polymer scaffolds seeded with autologous cells can facilitate human vascular regeneration in vivo and that a scaffold polymer construct can undergo complete degradation without compromising the mechanical properties of the vessel.
Following the success of Shin'oka et al., there has been renewed interest in TEVGs employing degradable polymer scaffolds. Importantly, Shin'oka's study was performed in the venous system, where pressures of 5–20 mmHg are significantly lower than those in the arterial circulation. Accordingly, translating successes in the venous circulation to a tissue-engineered arterial graft will require investigation of novel scaffolds that can withstand systemic arterial pressures while simultaneously promoting robust neotissue formation.
An ideal degradable polymer scaffold should be nonimmunogenic, highly porous, and receptive to cellular attachment, infiltration, and growth; however, this is an area of ongoing research and debate. 19 Methods for creating degradable polymer tissue scaffolds have included gas foaming, salt leaching, phase separation, freeze drying, 3D printing, and fiber processing, all of which are reviewed elsewhere.20,21 Among them, a few technologies have received as much attention as the electrostatic spinning (electrospinning) technique due to its accessibility for bench-top fabrication, versatile control over process parameters, and the ability to efficiently generate nanoscale fabrics of many polymeric materials that provide a favorable surface for cellular interaction. 22 Despite many encouraging preliminary results, there are no published reports to date of a purely electrospun scaffold implanted in the arterial circulation which demonstrated complete scaffold degradation and development of adequate neotissue. However, various electrospun scaffolds for TEVG have been investigated in vivo and here, we review the electrospinning process and all available studies that investigate surgical implantation of electrospun TEVG.
Electrospinning TEVG
The electrospinning apparatus consists of a voltage generator, syringe pump, and grounded collection target (Fig. 1). First reported by Zeleny in 1914, and later improved and patented by Formhals in 1934, the electrospinning process has changed little in the past 100 years.23,24 Briefly, a polymer solution is forced through an electrified capillary toward a grounded target via a syringe pump. As the charged polymer solution enters this large electric field (typically 10–30 kV), electrostatic repulsion exceeds the surface tension of the polymer solution, creating a jet of entangled polymer chains. This unstable jet accelerates in the electric field, creating a whipping effect and drawing ultrafine polymer filaments toward the grounded target while simultaneously evaporating the solvent.25,26
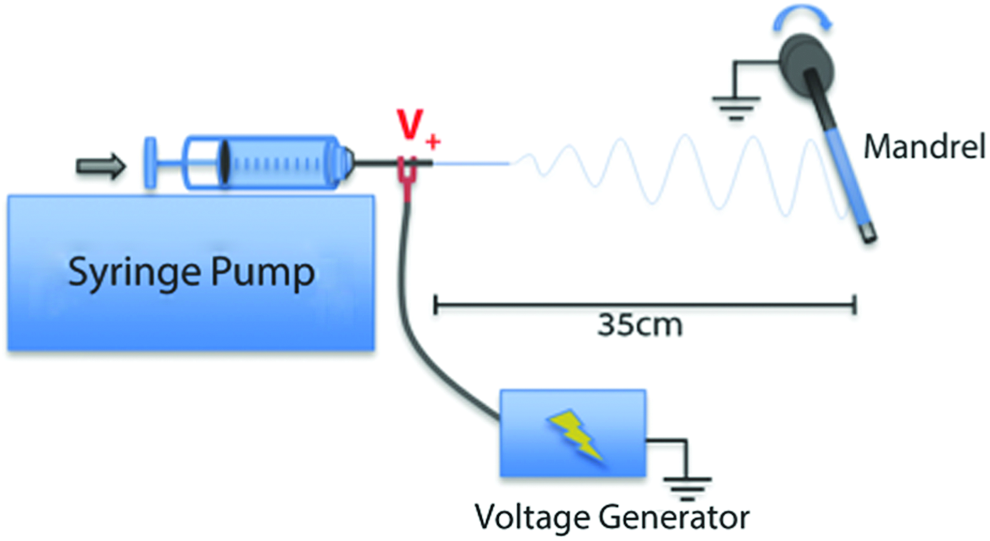
Representative electrospinning apparatus for constructing tissue-engineered vascular grafts (TEVG) around rotating mandrel. Color images available online at www.liebertpub.com/teb
Pertinent parameters in the electrospinning process include polymer type and molecular weight; solvent and solution concentration/viscosity; flow rate; applied voltage; distance between syringe and collector; collector design; and environmental factors such as humidity, temperature, and air velocity. 27 Optimization of the process parameters yields a fabric of fine, dry, nonwoven polymer fibers ranging in diameter from 50 nm to 20 μm, smaller than most other available fiber spinning techniques. A large decrease in fiber diameter can substantially improve an electrospun fabric's mechanical properties, and provide a unique scale for cellular interaction (Fig. 2A–C). 28 The topographies of these nanofiber fabrics not only have an immense surface area to volume ratio, but also resemble the structural components of native arterial wall ECM: collagen type I and type III fibrils that range in diameter from 20 to 100 nm.29–31 The ability to readily mimic the scale and architecture of natural ECM improves conditions for cellular attachment and proliferation, and has resulted in great interest in electrospun applications for TEVG.32–34 Many homopolymers, copolymers, and polymer blends have been electrospun and characterized, illustrating versatile control over properties such as fiber diameter, pore size (void space between fibers), mechanical strength, and degradation rate.35–37 Many modifications have been made to the traditional electrospinning apparatus in order to produce a variety of fiber alignments and topographic morphologies; for TEVG construction, fibers can be collected around a rotating mandrel of any diameter, forming a seamless, tubular scaffold in one step. 38
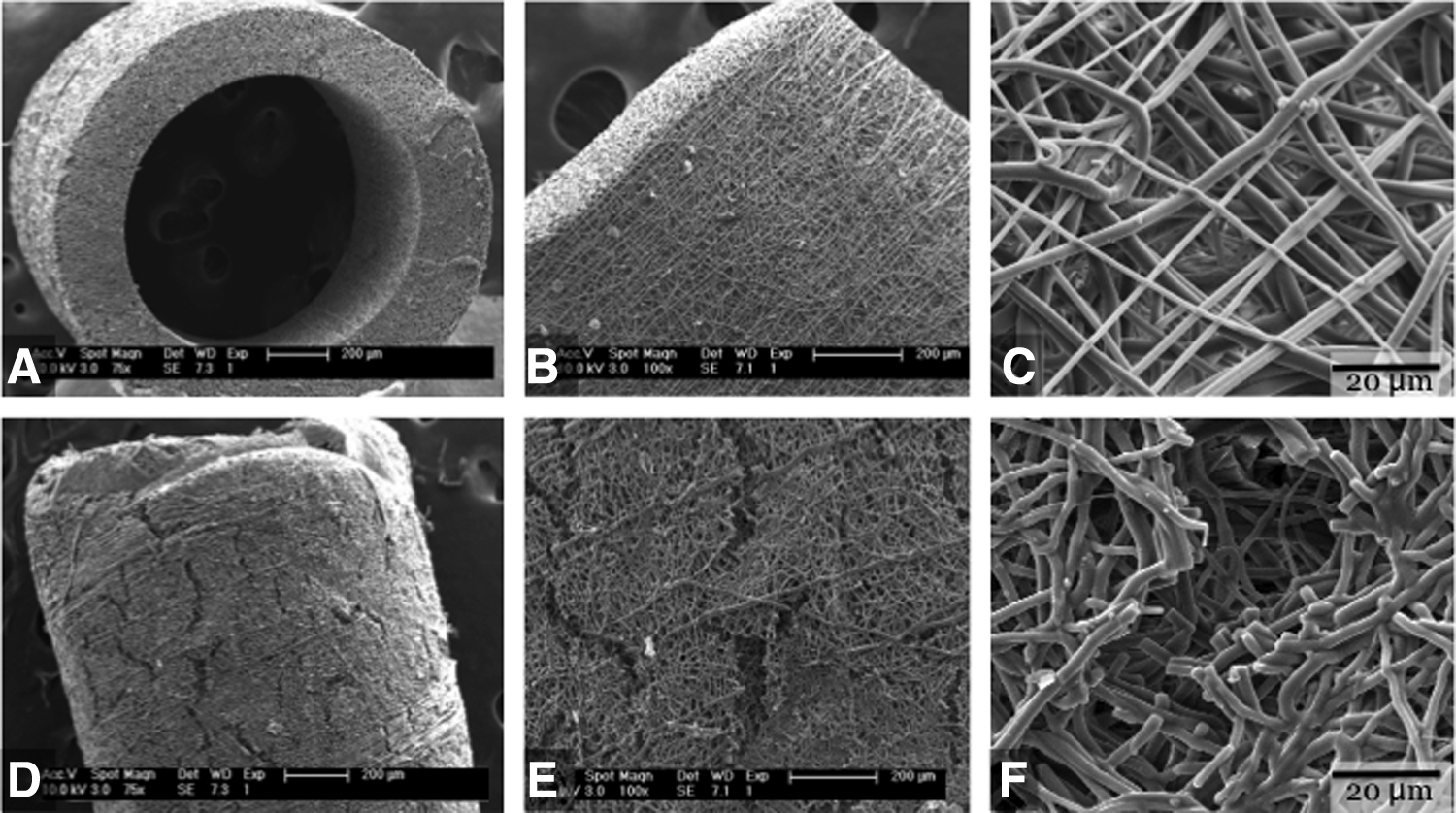
Scanning electron micrograph of electrospun PCLA TEVG
Materials
Despite tremendous interest in electrospinning vascular grafts, there have been relatively few published reports of surgically implanted electrospun TEVGs. Our literature review identified 27 publications featuring the development of an electrospun vascular graft that was also implanted as a bypass or interposition arterial conduit (Table 1). Orthotopic implantation is the gold standard for evaluating the complexity of TEVG viability, including patency rate, presence of endothelium, development of neotissue or a neolayer, graft degradation, and lastly, neovessel remodeling. It also marks a significant step in terms of assessing the utility of a given scaffold, with the ultimate goal of clinical utility. While many natural and synthetic polymers have been electrospun and characterized in vitro, relatively few have been used for TEVG scaffold construction and investigation in vivo. 25 To date, mostly all vascular implantations of electrospun polymers have been constructed of polyesters or polyurethanes and are, therefore, discussed here.
N, PGS graft completely degraded but evidence of PCL sheathing remained.
AA, abdominal artery interposition; AIB, aortoiliac bypass; CCA, common carotid artery interposition; CCAB, common carotid artery bypass; ECs, endothelial cells; ES, electrospun; FA, femoral artery interposition; IEV, inferior epigastric vein interposition; MDSCs, muscle-derived stem cells; MSCs, mesenchymal stem cells; ND, nondegradable; OECs, outgrowth endothelial cells; PCL, poly-ɛ-caprolactone; PCLA, poly(ɛ-caprolactone-co-
Polyesters
Polyester materials have been clinically used as arterial substitutes in Dacron grafts for more than 50 years. All polyesters feature an ester bond that is capable of hydrogen bonding, which makes this class of materials less hydrophobic than other synthetic graft materials such as Gortex. 39 Importantly, some types of polyesters feature an ester bond that is susceptible to hydrolysis, dividing the class into degradable and nondegradable polyesters. Dacron grafts are composed of a nondegradable polyester, PET, that is first spun into filaments and then either woven or knitted to generate a vascular graft which meets the essential requirements of strength, durability, and functionality. 4 Just as is true of clothing, the manufacturing process has a significant impact on the overall material properties; woven grafts typically have small pores and are stiff, whereas knitted grafts (typically velour) have large pores and are more compliant. 40 As a result of the larger pore size, knitted PET grafts have improved cellular infiltration that enables improved neotissue formation. However, the larger pore size also enables transmural bleeding, which necessitates preclotting with albumin, gelatin, blood, or fibrin glue before implantation.
Despite their utility in high flow, large-diameter applications, Dacron grafts have not been used in small-diameter applications due to exceedingly poor short-, medium-, and long-term patency rates. For example, only 50% of collagen-impregnated, knitted PET conduits with 6.0 mm inner diameter are patent at 5 years when used in femoro-popliteal bypass procedures. 41 Dacron polyester grafts are, in fact, contraindicated for replacing vessels<6.0 mm.
Dacron is considered a nondegradable polyester, whereas there are a number of clinically relevant degradable polyesters of the aliphatic family common to tissue engineering, such as poly(glycolic acid) (PGA), poly(lactic acid) (PLA), and poly-ɛ-caprolactone (PCL). These materials are commonly used for constructing TEVGs due to a wide range of material properties and a well-documented profile of in vivo degradation. They are also FDA approved for implantation and have been clinically used as Vicryl® and Monocryl® sutures for decades.42,43 These polymers degrade via hydrolytic cleavage at the ester bond, producing fragments of diminishing molecular weight. Macroscopically, bulk degradation of these materials is witnessed first as a loss of mechanical properties and later as a decrease in mass and volume (Fig. 2D–F).
39
In the final phase of in vivo degradation, low-molecular-weight polymer fragments are phagocytosed by macrophages and degraded into naturally occurring metabolites.
44
The final degradation product of poly(
PLLA
In 2007, Hashi et al. were the first group to report implantation of a degradable electrospun TEVG for arterial circulation in rat aortas. The scaffolds for this study were constructed from poly(
In later experiments, Hashi et al. constructed seamless PLA electrospun scaffolds via a rotating mandrel and a longitudinally moving spinneret, the most common and efficacious method used to date.46,47 The PLA surfaces of the grafts were then conjugated with hirudin, a polypeptide thrombin inhibitor, via a polyethylene glycol (PEG) linker and evaluated over 26 weeks in rat common carotid artery. 46 A bare PLA graft lacking the PEG/hirudin modification and a PLA graft with only the PEG linker present (PEGylated) were used as controls. Results demonstrated that the unmodified PLA nanofiber surface induced thrombotic occlusion in 50% of the cases, while the PEGylated surface and PEG/hirudin surface improved to 25% and 17%, respectively. Interestingly, the PEGylated linker significantly improved patency over the bare PLA surface, a finding that the authors attributed to hydrophilicity of the luminal surface secondary to PEGylation and its resultant behavior as a brush-like border. From these experiments, Hashi et al. concluded that unmodified PLA nanofiber grafts induce an unacceptably high thrombotic response in the arterial circulation whereas surface improvements such as cell seeding, PEGylation, and hirudin conjugation improve patency.46,47 Following on this success, Janairo et al. investigated the conjugation of electrospun PLLA with mucin, a negatively charged hydrophilic glycoprotein with a brush-shaped structure. 48 Using the modified PLLA-mucin scaffolds, they reported a suppression of platelet activation, improved patency, and improved cellular infiltration; however, PLLA did not degrade within the in vivo duration, so neovessel viability remains unanswered.
PCL
Walpoth and Moeller have produced a series of publications while making use of an optimized electrospun poly-ɛ-caprolactone (PCL) scaffold (graft inner diameter 2.0 mm, fiber diameter 1.9–2.2 μm) that was evaluated in vivo in an abdominal aorta rat model for durations of 12, 24, and 78 weeks.49–52 All of the surgeries were performed without the use of anticoagulation or anti-platelet drugs. Despite this, graft patency remained at 100% for the duration of the studies with no evidence of graft thrombosis. Importantly, the researchers included analysis of polymeric degradation using gel permeation chromatography to assess the degree of change in molecular weight of the scaffolds. Their PCL constructs lost 20% of the initial 80 kDa molecular weight after 3 months, 51.5% at 12 months, and 78.1% at 18 months. It is unknown whether the graft would remain mechanically stable on 100% degradation, because the slow degradation time of PCL cannot be fully assessed in a rodent model with a lifespan of 2 years. The authors also reported a decrease in cellular infiltration at time points after 1 year, as well as instances of chrondroid metaplasia that contributed to a gradual calcification of the grafts. These findings at late time points illustrate the importance of long-term in vivo experimentation.
Electrospinning blends of PCL with collagen or synthetic elastin biopolymers have also been investigated with the hypothesis that inclusion of natural ECM biopolymers would make a more biomimetic graft while retaining the strength and processing advantages of PCL. Tillman et al. electrospun grafts of PCL/collagen type I blends (1:1 ratio), and Wise et al. reported a bilayered electrospun graft of PCL/recombinant human tropoelastin blend that was modified to reflect the mechanical properties of native internal mammary artery.53,54 Both research groups reported improved biocompatibility, reduced platelet attachment, and 100% patency during pilot in vivo experiments over 4 weeks. Other groups have investigated and implanted electrospun PCL blends with chitosan, a polysaccharide derived from crustaceans, to improve biocompatibility, degradation, and mechanical properties.55,56
PCLA
Copolymers of poly(
Polyurethanes
Polyurethanes are copolymers that contain a urethane linkage which is typically formed by polymerizing two or more monomers, one containing multiple hydroxyl groups and the other containing isocyanate groups to form a copolymer of urethane linkages. Different isocyanate- and hydroxyl-containing components can be combined to form segmented polyurethanes that offer a wide range of material properties for the various components. Under the right conditions, the immiscible polymeric components can be arranged into a microphase separation of hard and soft domains within the material. The hard domain is hydrogen bonded and often semi-crystalline, contributing strength and a high tensile modulus. However, hard domains are dispersed within an amorphous and elastic soft domain, giving the overall material strength and elasticity. Examples of these polyurethanes include poly(ester urethane), poly(ether urethane) (PEU), and carbonate-based polyurethanes. These composite materials offer strength, flexibility, durability, and can be manipulated by controlling components and composition.61,62
Nondegradable polyurethanes
In the early 1960s, DuPont developed a segmented poly(ether-urethane urea) named Lycra® (commercially known as Spandex) that had the processability of thermoplastics and the behavior of elastomers, namely the capacity for repetitive stretch (e.g., rubber). 63 This elastic material was both durable and resistant to hydrolytic degradation, resulting in its quick adaptation for biomedical investigation. Ethicon produced a modified version of the material termed Biomer®, which featured a 4,4′-diphenylmethane diisocyanate (MDI)/ethylenediamine (ED) hard domain and a poly(tetramethylene oxide) soft domain. In 1967, Boretos and Pierce pioneered Biomer vascular grafts and implanted them in canine carotid arteries. 64 In 1978, Annis et al. first investigated the electrospinning of Biomer to fabricate vascular grafts and later implanted the grafts as interpositional carotid conduits in a canine model using intraoperative heparin and pre and postoperative antiplatelet agents.65,66 These experiments showed that 17 out of 26 (65%) of the grafts remained patent over 2 years, with five acute failures and four long-term failures occurring between the 59th and 301st day postimplantation. 67 More recently, Bergmeister et al. investigated grafts constructed of electrospun Pellethane®, a PEU similar to Biomer. 68 When implanted as rat abdominal aortic prostheses, an overall patency of 95% was reported after 26 weeks in vivo with no signs of graft degradation.
These polyurethanes were investigated with the ultimate purpose of their being implanted as permanent synthetic arterial prostheses. However, it has been shown that ester segments of poly(ester urethanes) are susceptible to hydrolytic degradation and ether segments of PEUs are susceptible to “environmental stress cracking” caused, in part, by reactive oxygen species from activated macrophages and foreign body giant cells, thus leading to unpredictable changes in graft mechanical properties.61,69 The discovery of in vivo degradation mechanisms presumably shifted interest away from these polyurethanes as permanent synthetic vascular grafts and toward their usage as TEVGs that can be tailored with a more controlled degradation profile.
Degradable polyurethanes
Utilizing degradable polyurethanes to construct a temporary tissue scaffold, Vorp and Wagner have published a series of reports investigating implanted electrospun poly(ester urethane)urea (PEUU) grafts in a rat abdominal aorta model. They reported electrospun PEUU grafts to be 40% patent at 8 weeks with cases of graft occlusion attributed to thrombosis.70,71 To improve the thrombogenic nature of PEUU, they blended or coated electrospun PEUU with copolymers featuring 2-methacryloyloxyethyl phosphorylcholine (MPC), a material known to reduce platelet adhesion.70,71 Hong et al. investigated PEUU grafts blended with an MPC-containing copolymer poly(2-methacryloyloxyethyl phosphorylcholine-co-methacryloyloxyethyl butylurethane) (PMBU), and reported a greater patency of PMBU-PEUU blended grafts at 8 weeks in rat abdominal aortas than the PEUU group (67% vs. 40% at 8 weeks). 70 Soletti et al. electrospun PEUU grafts and then covalently bonded an MPC-methylacrylic acid copolymer (PMA) to the surface of the scaffold. Patency was greatly improved with the PMA surface treatment (92% vs. 40% at 8 weeks), and the most common mode of graft failure was acute thrombosis (90% of the obstructed grafts). 71 These studies suggest that degradable polyurethanes are a viable class of polymers for TEVG construction. However, PEUU constructs warrant antithrombogenic surface treatment before surgical implantation. To fully assess the clinical viability of electrospun polyurethane or polyester TEVGs, long-term studies, including quantitative assessment of total polymer degradation, are needed.
Success Criteria for Electrospun Scaffolds
In Vivo
and Rational Design Considerations
In order to achieve successful in vivo application, a TEVG should first resist a thrombotic response on implantation. Failure to resist thrombosis can result in acute graft occlusion or thromboembolism. Next, the TEVG should permit cellular infiltration within the graft and achieve adequate neotissue formation. Lastly, the polymer scaffold should degrade and resorb entirely, transferring mechanical responsibility from the polymer to the neovessel and permitting vascular remodeling without inducing aneurysmal dilatation. 72 Analyzing and understanding the reported in vivo studies to date offers a better understanding of the benefits and challenges of electrospun TEVG and offers a framework for creating a rationally designed TEVG.
Prevention of thrombosis and stenosis
A primary cause of TEVG failure in active circulation is occlusion due to thrombosis or stenosis. Graft thrombosis is most commonly due to turbulent blood flow or a thrombogenic luminal surface. Graft stenosis is a more chronic problem and is most commonly due to either recurrent episodes of partial graft thrombosis leading to luminal narrowing or neointimal hyperplasia. Neointimal hyperplasia itself has a variety of causes, including compliance mismatch between the graft and native vessel and prolonged states of inflammation.49,50 The primary aim of a rationally designed TEVG is, therefore, to reduce the incidence of graft occlusion by either thrombosis or stenosis in order to enable adequate distal perfusion and development of neovessels. Strategies for minimizing graft thrombosis include the use of experimentally determined thromboresistant scaffold materials, anti-coagulant or anti-platelet drug eluting polymers, chemical modification of the TEVG luminal surface, and expediting the development of a confluent endothelial layer.
Hashi et al. investigated the antithrombogenic properties of mononuclear stem cells seeded onto electrospun PLLA grafts. 46 In a 60-day study, unseeded PLLA grafts showed significant intimal thickening compared with seeded grafts, suggesting that mononuclear cell seeding resisted not only a thrombotic response but also intimal hyperplasia. The same group investigated chemical surface modification with an antithrombogenic PEG-hirudin-conjugated PLLA scaffold. 47 The PEG-hirudin grafts exhibited 75% patency after 1 month as carotid artery interposition grafts, whereas untreated grafts were 50% patent at the same time point, thus demonstrating the utility of luminal surface chemical modification on reducing rates of graft thrombosis.
Walpoth and Moeller explored the antithrombogenic properties of grafts loaded with paclitaxel, an anti-proliferative drug aimed at reducing neointimal formation. 73 The drug eluted over the course of 4 weeks and was successful in reducing neointimal formation; however, it also appeared to inhibit cellular ingrowth and delayed EC layer formation, which are two critical processes for in situ vessel regeneration. Ye et al. and Lu et al. investigated PCL conjugated with heparin, and while both studies had acceptable patency rates, detailed information about endothelialization or neovessel formation was limited.74,75
As previously discussed, electrospun PCL surfaces resist thrombosis and have been shown to generate a confluent EC layer within the first 6 to 12 weeks after implantation, faster than that seen in ePTFE grafts.49,50 However, most other materials that have been implanted featured modifications to the material or luminal surface such as cell seeding, conjugation of the luminal surface with heparin or a thrombin inhibitor, or incorporating antithrombogenic polymers (collagen, synthetic elastin, or MPC-containing polymers) into the scaffold.46,47,53,54,70,71,74,75 Ideally, the TEVG should resist thrombosis until cells from adjacent vascular tissue can migrate and form a confluent luminal layer. 72
Indeed, the presence of an intact EC monolayer provides the most effective and long-term strategy for thromboresistance, and, therefore, any TEVG construct should ideally encourage rapid development of an EC layer. One significant advantage of electrospun TEVG is that the nanofibers mimic the structure of fibrillar collagen in native ECM and therefore promote rapid EC migration and proliferation while maintaining a cellular phenotype.77,78 In an attempt to expedite endothelialization, Kuwabara et al. fabricated electrospun PCL grafts (0.7 mm inner diameter) containing the peptide CAG (cysteine-alanine-glycine) and reported a significant increase in the rate of endothelialization and levels of endothelial nitric oxide synthase compared with control grafts.79,80 Zheng et al. investigated coating electrospun PCL with an arginine-glycine-aspartic acid (RGD)-containing molecule and found it increased the amount of endothelialization and cellular infiltration while also improving patency. 81 The best way to ensure endothelialization of a TEVG is via ex vivo EC seeding and subsequent in vitro culture. Such a process has been validated, but it adds considerable complexity to TEVG construction and diminishes off-the-shelf value. 15
Cellular infiltration and neovessel formation
For a TEVG polymer construct to develop into a neovessel in situ, a robust cellular influx, proliferation, and remodeling should occur to ultimately form a confluent luminal endothelial layer and medial SMC layer. Further, these cells should deposit an ECM composed of collagen, elastin, and laminin that promotes cellular functioning and gradually assumes responsibility for the mechanical properties of the neovessel. 82 Thus, the ideal scaffold material should have adequate porosity to enable inflammatory cell influx and adherence to the graft, thereby allowing these cells to induce a more robust cellular influx via paracrine signaling to circulating cells and adjacent vascular cells. Our group has previously reported the importance of inflammatory cell influx and paracrine signaling for TEVG remodeling, as grafts transition from cell-seeded scaffolds to neovessels in a murine model using a highly porous TEVG. 83 When TEVG are implanted, there is an initial inflammatory cell influx in response to increased levels of monocyte chemoattractant protein-1 (MCP-1) secreted by the seeded bone marrow-derived mononuclear cells. After influx into the TEVG, these inflammatory cells secrete more MCP-1, in addition to multiple other growth factors and cytokines that are critical for angiogenesis, including vascular endothelial growth factor. 83 This cytokine response triggers the recruitment of circulating endothelial progenitor cells to the scaffold and, more importantly, the migration of mature cells from the adjacent vessel wall, which ultimately comprise approximately 93% of the neotissue.72,83 (Fig. 3). A SMC layer and supporting ECM is crucial for replacing the loss of polymer strength as it degrades. The final neovessel is able to fully support physiologic loading and is also able to grow, repair, and remodel akin to native tissue. This entire process hinges on the ability of cells to localize to the graft surface and migrate within the graft wall, and, therefore, rests on the porosity of the scaffold and the availability of free space for cellular infiltration, proliferation, and tissue formation.
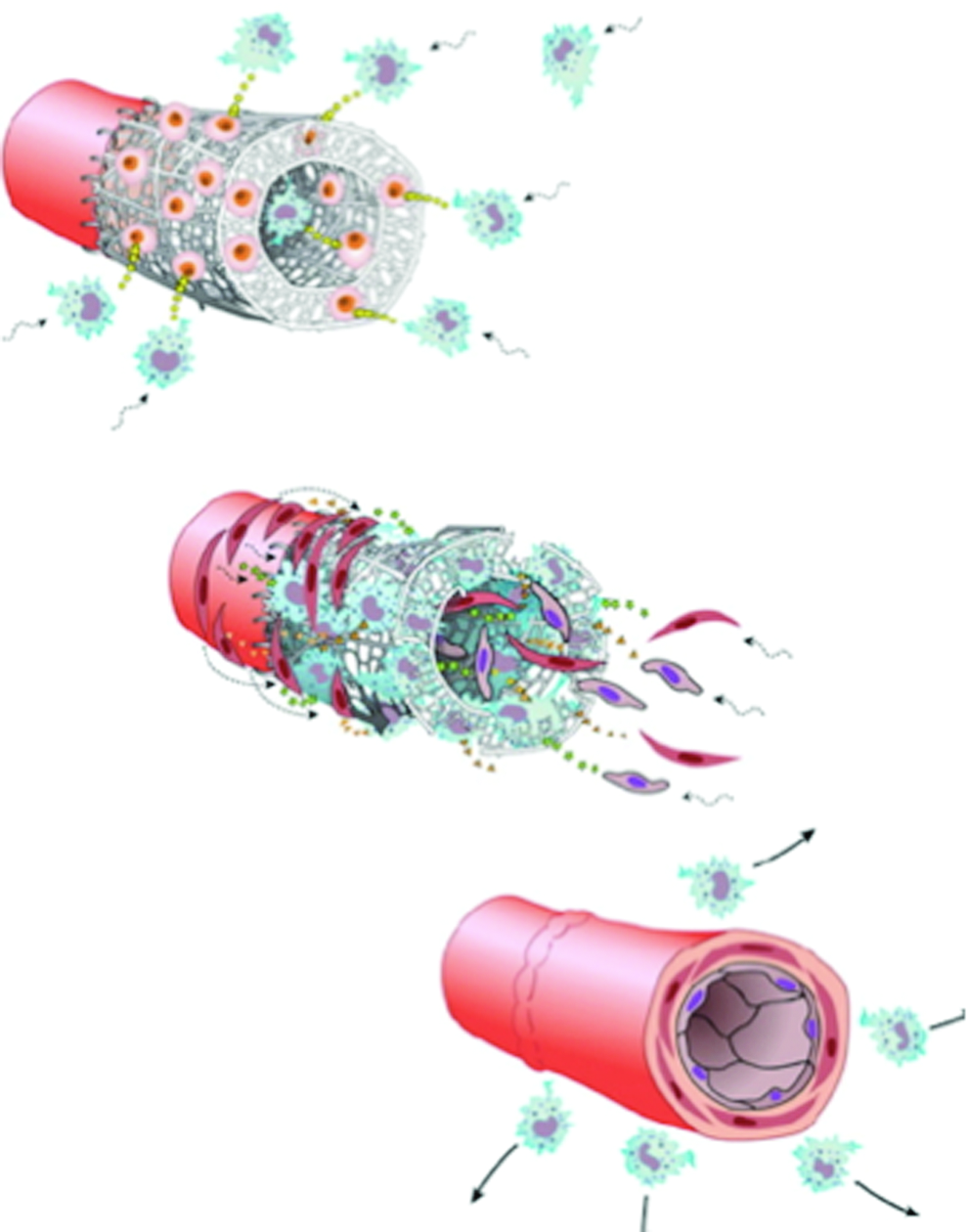
Process of neovessel formation is driven by inflammation-mediated cellular infiltration (top), extracellular matrix deposition (middle), and complete scaffold degradation and neovessel remodeling (bottom). Reprinted with permission from authors. 76 Color images available online at www.liebertpub.com/teb
For electrospun constructs, maintaining an adequate pore that enables cellular influx poses a challenge: The fabrics are relatively dense in three dimensions with pore sizes limited to the void spaces of overlapping nanofibers that can inhibit cellular infiltration and limit the quantity of deposited ECM. 84 Ju et al. demonstrated that electrospun fiber diameters of<1.0 μm inhibited infiltration of SMCs and necessitated the development of a bi-layered graft to provide adequate porosity. 85 In studying randomly oriented PCL electrospun fibers, Lowery et al. used mercury porosimetry to demonstrate that peak pore diameter scales linearly with fiber diameter by a factor of 3.44 (R 2 =0.97). 86 This implies that randomly aligned electrospun fibers of 1 μm diameter create a fabric having a peak pore diameter of 3.44 μm, smaller than the average rounded cell diameter of 5–20 μm.86,87 Table 1 displays the fiber diameters of electrospun materials implanted in vivo and whether cellular infiltration was reported. It is apparent from these studies that unmodified electrospun vascular grafts of fiber diameters<1.0 μm inhibit cellular infiltration in all cases except those reported by Bergmeister et al. and Zhou et al., though it is likely that a wide disparity in fiber diameters increases porosity.55,68
Walpoth and Moeller's unseeded electrospun PCL grafts with a nanofiber diameter of 1.9–2.2 μm (estimated peak pore size of 6.5–7.6 nm) were implanted in vivo and grafts were found to be fully patent, transmurally infiltrated by macrophages and fibroblasts, and completely endothelialized after 12 weeks. In addition, the electrospun PCL graft exhibited greater cellular infiltration and more rapid endothelial coverage (97% in 6 weeks) as compared with a conventional ePTFE graft, most likely due to increased cellular affinity for the electrospun materials. 49 Interestingly, this group also investigated bilayered electrospun PCL grafts featuring a less porous (fiber diameters of 0.83 μm) and more porous layer (fiber diameters of 2.21 μm). 52 After implantation, the group noted that cellular infiltration was diminished when the adventitial layer was less porous but neither construction affected the rate of endothelialization.
Thus, there is a paradox in electrospinning TEVG as the advantages of nanoscaled fibers (less than a micron in diameter) are potentially offset by the accompanying decreased porosity that inhibits cellular infiltration and limits the available space for ECM production. To address this concern, methods for electrospinning grafts with increased pore size without increasing fiber diameter have been investigated and include the following: bilayers, salt leaching, sacrificial fibers, air-flow impedance, and cryogenic spinning.52,53,75,84,85,87–92 Importantly, only bi-layered constructs have been examined in vivo.52,53,75,91,92
Graft degradation and vessel remodeling
The premise of tissue engineering rests on the restoration of biological function. The final phases of transition from TEVG to neovessel are completion of graft degradation and vessel remodeling. 93 Despite the importance of scaffold degradation in vivo, a few studies have thoroughly investigated this process. More specifically, no studies to date have investigated in vivo data of electrospun TEVG that have progressed through complete polymeric degradation. In part, it is because many of these polymers, such as PCL, take years to fully degrade in vivo, exceeding the life span of many animal models.
Recently, the Walpoth and Moeller group published 18 month in vivo data from electrospun PCL grafts. 50 Interestingly, even as the graft degraded to 20% of original molecular weight at 18 months, it neither dilated nor had a significant increase in compliance. These data suggest that the neotissue and neo-ECM were providing adequate mechanical properties in the context of systemic arterial pressures as the polymeric tensile strength was lost. Unfortunately, 18 months represented the capacity of the lifespan of the animal and there was still polymer remaining at the end of the experiment.
Our group's murine model of PGA TEVG inferior vena cava (IVC) interposition grafts requires 6 weeks after surgical implantation for scaffold constructs to lose all mechanical properties, but tissue analysis has demonstrated continued remodeling over the next 6 months, four times the duration of the polymer degradation period (Fig. 4).94,95 It is imperative that a similar strategy be used to investigate arterial scaffolds, in which in vivo experiments exceed the duration necessary for complete polymer degradation, resorption, and remodeling. In order to facilitate this, either a faster degrading polymer should be used in small animal models or large animal models should be employed over a longer lifespan. Most importantly, a thorough and validated animal model should be developed to evaluate neotissue after complete polymer degradation before clinical evaluation and translation.

In vitro pressure-diameter responses from explanted TEVGs demonstrated a gradual increase in distensibility over the implantation period, and the response of the TEVGs became similar to the native vessel by 24 weeks. Specifically, at 2 weeks, the TEVG showed almost no response to an increase in pressure; at 6 and 12 weeks, durations at and beyond TEVG polymer degradation, the TEVGs became more responsive to applied pressure and distended approximately 10% at 20 mmHg. At 24 weeks, four times the duration of polymer degradation, the TEVGs were more distensible and began to closely match native inferior vena cava. This result clearly shows the transition from a stiff scaffold-dominated mechanical behavior to a more distensible, neotissue-dominated mechanical behavior. Values are mean±standard error of the mean. Reprinted with permission from authors. 94
In a promising development, Wu et al. constructed a TEVG using a bilayered approach featuring a highly porous elastomer and a reinforcing outer layer of electrospun PCL. 92 The inner elastomer, poly(glycerol sebacate), is a copolymer of glycerol and sebacic acid that not only enables 3D cross-linking to increase strength and stability but also includes an ester bond which degrades hydrolytically within 2 months in vivo.96,97 Unlike the aliphatic polyesters reviewed earlier, this copolymer degrades via surface erosion such that mass and strength are lost simultaneously, permitting a gradual polymer removal during neovessel formation.96,97 Importantly, when implanted in rat abdominal aorta, the unseeded grafts rapidly remodeled over the first few weeks and were reported to be nearly polymer-free neovessels after only 90 days with an overall patency of 80.9% (17 of 21). The remaining polymer in the constructs at 3 months was attributed to the PCL sheath, but the bulk of the graft had mostly transitioned into neovessels, unlike any other report to date (Table 1). 92 This study suggests that short duration arterial regeneration is viable and electrospinning technology may work best as a supplementary coating with other TEVG scaffold designs.
Conclusion
The use of synthetic vascular grafts, including Dacron and Goretex, has successfully been employed by surgeons for decades to bypass and reconstruct medium to large-diameter vessels. For small-diameter (<6 mm) clinical applications, autologous veins and arteries are preferred; however, these vessels are limited. With a steadily increasing incidence of cardiovascular disease, there is a growing need for TEVG that can resist thrombosis, withstand systemic arterial pressures without aneurysmal dilatation, and successfully transition into polymer-free neovessels. Electrospinning is a simple and versatile method for constructing polymeric TEVG scaffolds that has been shown to improve cellular infiltration and endothelialization over standard ePTFE grafts in vivo. 48 Despite promising early results of electrospun TEVG, there have been no reported in vivo studies to date that have investigated neotissue formation beyond complete polymer degradation. This is the most critical remaining challenge to effectively characterize the mechanical properties of the neotissue and its capacity for continued vascular remodeling. The transition of mechanical strength from the electrospun scaffold to viable neotissue is crucial for TEVG function, and this complete transformation process should be adequately characterized before clinical investigation. Therefore, further long-term studies should be performed to investigate the efficacy of different electrospun TEVG materials and porosities, the use of modifiers to inhibit thrombosis and promote neotissue formation, and the mechanical characterization of neotissue formation after complete polymer degradation in vivo. Such studies will help elucidate the true potential of bioresorbable electrospun vascular grafts and enable this commonly proposed tissue engineering technology to reach clinical investigation.
Footnotes
Disclosure Statement
The authors wish to disclose that C.K.B. receives grant support from the Pall Corporation.