
Abstract
Islet transplantation is emerging as an attractive option for the treatment of type 1 diabetes mellitus (T1DM). However, some major obstacles are needed to be overcome, including shortage of islet supply and excessive immunosuppressive therapy. Xenotransplantation of bioartificial pancreas (BAP) made of microencapsulated pig islets will effectively solve these problems. Before widespread application of this therapy, several important issues should be addressed to further improve pig islet viability and functionality, such as pig islet source, optimization of microcapsule preparation, cryopreservation of implant, selection of biocompatible material, and implant site, as well as prevention of xenoreaction and biosafety concern. It is hoped that improvements in these critical aspects will lead to wider human application of microencapsulation of pig islets.
Introduction
I
Pig is considered as a promising candidate for xenologous islets due to several advantages, including structural similarity of insulin between pig and human, lack of amyloid formation, resistance to recurrent autoimmunity, feasibility in genetic immunomodulation/engineering, and few ethical issues. 4 However, initiation of clinical application of pig islet still requires additional progress in two major hurdles: immune rejection due to xenogeneic incompatibility, and virus- or pathogen-based xenosis.5,6 Several strategies are developed to protect transplanted pig islet grafts from immune attacks of recipients. Nowadays, the mainstay of immunomodulatory therapy depends on the usage of conventional (e.g., steroid, tacrolimus, and cyclosporine) and/or relatively specific (e.g., costimulatory blocking agents) immunosuppressants to achieve sustained immunosuppressive state. These immunodepressors, while showing favorable efficacy in extending the functional survival of pig islet xenografts,7–12 have numerous severe side effects,13–15 such as opportunistic infection, malnutrition, neuritis, thrombogenesis, and islet toxicity. Therefore, to safely and efficiently promote experimental pig islet xenotransplantation into clinical trials, problems concerning life-long and heavy immunodepression must be solved first.
One alternative strategy for protecting the grafts against xenorejection is immunoisolation. Immunoisolation, that is, encapsulation of islets in a membrane that is selectively permeable for oxygen, nutrients, and insulin, but not for humoral and cellular components of the recipient's immune system (Fig. 1), enables successful pig islet xenotransplantation in the reduction or absence of immunosuppressive medication.16–20
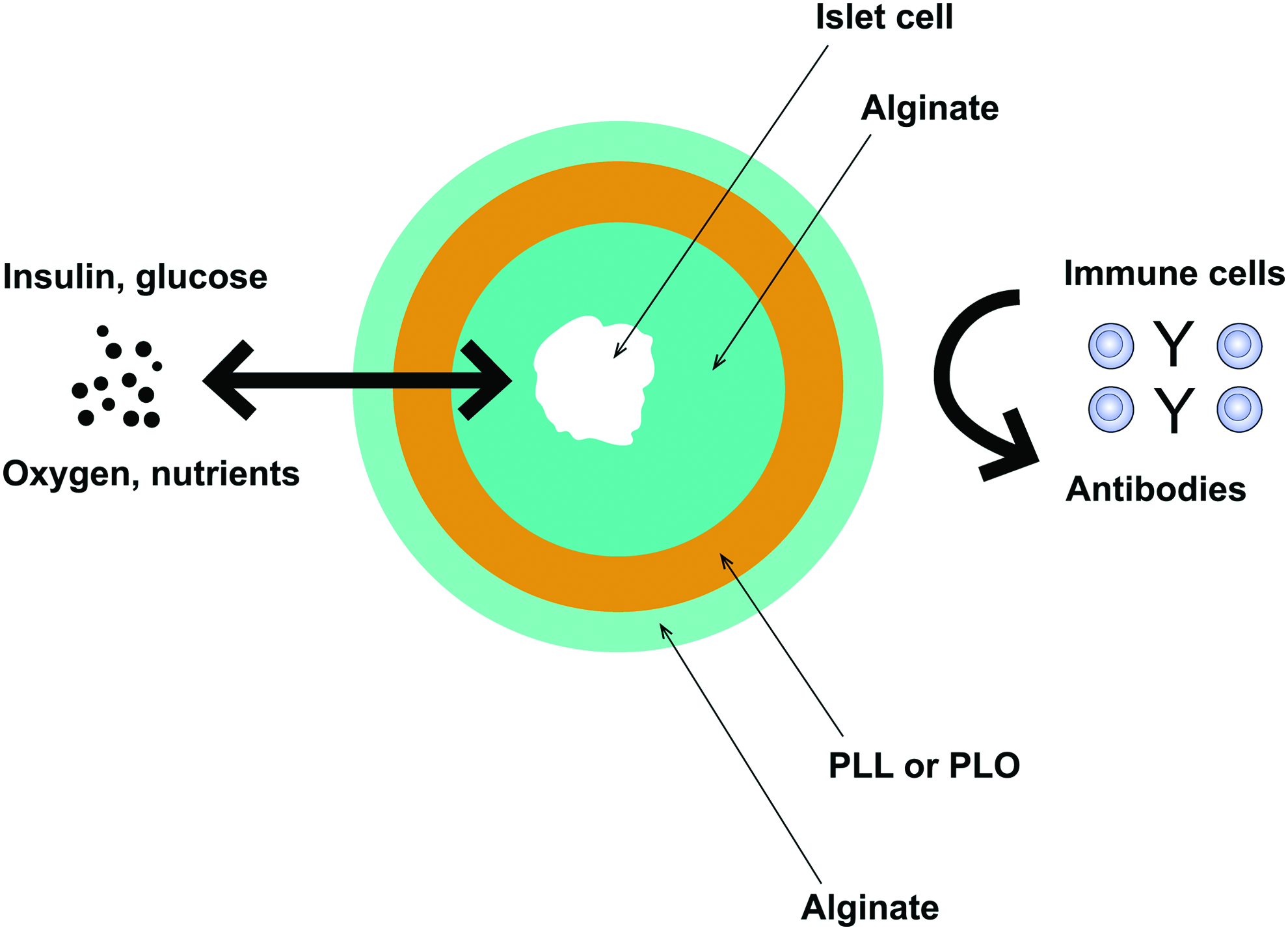
Illustration of the concept of islet microencapsulation and the principle of immunoisolation. The semipermeable membranes inhibit the entry of immune cells and antibodies, meanwhile, they allow the diffusion of insulin, glucose, oxygen, nutrients, and metabolites. Color images available online at www.liebertpub.com/teb
There are several distinct approaches for the transplantation of immunoisolated pig islets as a bioartificial pancreas (BAP). Intravascular devices (encapsulation of pig islets in a perfusion chamber which is anastomosed to the vascular system of the host) require high-risk vascular surgery and intense anticoagulation therapy,20,21 and therefore are unsuitable for clinical application currently. Extravascular approaches of immunoisolation are either macroencapsulation (encapsulation of a large mass of pig islets within a tubular diffusion chamber or planar chamber) or microencapsulation (encapsulation of individual or a small group of pig islets within a spherical chamber). Several considerations favor microcapsules over macrocapsules. Their spherical shape and low volume offers better diffusion profile due to higher surface-to-volume ratio. In addition, microcapsules require less complex manufacturing process, are mechanically durable, and can be simply injected without major surgery. A main drawback is the difficulty associated with the retrieval of transplanted capsules if necessary. However, fixation of pig islet microcapsules on a plasma-treated polydimethylsiloxane sheet, appears to be practicable for preventing the capsules from scattering in the body and perfectly retrieving them when required. 22 In the field of pig islet transplantation, there is a great deal more research and development with positive results for microdevices than for macrodevices,6,23–28 and some encouraging achievements have been made in preclinical/clinical xenotransplantation of microencapsulated pig islets without immunodepression (Table 1).
APIs, adult pig islets; PLL, poly-l-lysine; Cyno, cynomologus monkey; i.p., intraperitoneal; HbA1c, glycated hemoglobin; C-P, C-peptide; RCs, retrieved capsules; PT, post transplantation; RPIs: retrieved pig islets; NPCCs, neonatal pig pancreatic cell clusters; PLO, poly-l-ornithine; IEQs, islet equivalents; PVT, porcine viral transmission; PR, peritoneal reaction; STZ, streptozotocin; DTZ, dithizone; T1DM, type 1 diabetes mellitus; PERV, porcine endogenous retrovirus; AEs, adverse events.
Consequently, xenotransplantation of microencapsulated pig islets may provide a promising option of applicable treatment for insulin-dependent diabetes mellitus (IDDM) patients with minimal risks from permanent immunosuppression or complicated operation. This article reviews advances and challenges for xenotransplantation of microencapsulated pig islets, and discusses demands to successfully promote this therapy into widely clinical application.
Pig Islet Source
The most important element of BAP is the islet cell mass encapsulated within the semipermeable membrane. Pig islet with high-quality contributes a lot to the efficacy and functional duration of the BAP. Compared with other variable factors of gender and body weight, the age of the pig donor plays a much more significant impact on islet size, yield, and functionality.4,29–31
Neonatal pig pancreatic cell clusters (NPCCs) offer additional advantages over adult pig islets (APIs), including apparent resistance to ischemia or inflammation, low sensitivity to collagenase variability, great ease of digestion and purification,32,33 and low level of T-cell response. 34 Usually, NPCCs obtained from piglets aged <5 days perform better viability and functionality than the older ones. 35 Additionally, culture of NPCCs (from piglets aged 1–3 days) for a long time (12 days) offers the best balance in vivo functionality, evidenced by better diabetes reversal, lower levels of tissue factor (TF) expression, and higher gene expression for insulin, glucagon, and antiapoptotic Bcl-2. 36 The NPCC represents an available and alternative source of islet grafts for human recipients,4,37 and immunoisolation can further enhance the metabolic response of these islet xenografts in vivo.38–40 In fact, microencapsulation process did not compromise the viability of NPCCs, and the encapsulated grafts could be held in culture for 5 weeks with maintenance of viability. 41 Also, a published study demonstrated that microencapsulation was able to maintain fine morphology/structure of cryopreserved NPCCs and effectively recover their endocrine function. 42 After in vivo implantation, the microencapsulated NPCCs showed considerable capacity for proliferation and further differentiation into β-cells, 40 thus displaying the ability to restore normoglycemia or significantly reduce insulin dosage in both experimental18,24,40 and clinical trials 16 (Table 1). Once the time lag between preparation and maturation of NPCCs was curtailed by preincubation with homologous Sertoli cells, the microencapsulated NPCCs could correct hyperglycemia more effectively in diabetic mice. 35 Currently, commercial product of microencapsulated NPCCs manufactured by Living Cell Technology (LCT) are undergoing late-stage clinical trials. 43
Taking into account the potential risk of zoonosis, islet xenografts should be derived from specific pathogen-free (SPF) or designated pathogen-free (DPF) pig herds. 44 Donor pigs fulfilling DPF status are usually raised and kept in biosecure barrier facilities where all activities and operations are in compliance with Standard Operating Procedures and current Good Manufacturing Practices. To guarantee and maintain the DPF status, pigs are transferred into such facilities through Cesarean section and the source pigs are raised as a closed herd. Compared with the wild-type or market pig herds, the SPF Chicago Medical School (CMS) miniature pig, 45 Wuzhishan (WZS) miniature pig, 46 New Zealand Auckland Island pig, 47 and the new conserved pig herd called XENO-1 48 may serve as more practicable and better islet sourcing for microencapsulation in clinical application.
In addition, genetically modified pigs are considered as alternative donor sources with potentially major benefits of reducing the early graft loss and protecting islets against immune rejection.4,49 For example, humoral rejection can be fully suppressed by the crossbreeding of Gal gene knockout (GT-KO) pigs with transgenic pigs expressing human complement regulators such as CD46, CD59, and human decay-accelerating factor (hDAF, CD55)50–53 ; transgenic expression of human heme oxygenase-1 (HO-1) and/or soluble human TNFRI-Fc (shTNFRI-Fc) can protect pig islets from oxidative and inflammatory injury54,55; knockout of TF and overexpressing of human antithrombotic gene (CD39/thrombomodulin), may prevent the occurrence of instant blood-mediated inflammatory reaction (IBMIR) and coagulation dysfunction.56–58 Also, genetic engineering of pigs (deletion of Gal epitope and/or knockin of human genes) results in few abnormalities in hematologic, biochemical, or coagulation parameters, and seems to modify these indicators closer to human values. 59 More importantly, the genetic alterations do not display an overtly detrimental effect on islet function. 60 Although significant variations exist between wild-type and transgenic pigs in terms of baseline metabolic data (e.g., insulin, blood glucose, C-peptide, glucagon levels) and responses to glucose and arginine, acceptable glucose metabolism can be achieved.60,61
Materials for Microencapsulation
Polymers applied for microcapsules should satisfy the following requirements, including negative influence on viability and functional survival of encapsulated cells, be pliable, soft and mechanically stable, free exchange of molecules of interest (e.g., nutrients, oxygen, glucose, and insulin), and high biocompatibility with minor host response. 62
Over the past two decades, a wide range of polymers, such as agarose,63,64 polyethyleneglycol (PEG),65,66 and sodium cellulose sulfate, 67 have been used for microencapsulation of pig islets. Most of them have not been adequately and comprehensively studied in terms of biocompatibility with longevity with the enveloped islets and the recipients, and therefore do not qualify as safe and valid for human application for the moment.
To date, the most widely used and more preferred biomaterial for pig islet microencapsulation is alginate (Table 1),17,19,40,68–73 an unbranched anionic polysaccharide (comprised of β-D-mannuronic acid and α-L-guluronic acids) extracted from brown algae (Phaeophyta), whose physicochemical and gelling properties make it more efficient and promising in sequestering pig islets from the immune system with a long-term stability and no alteration of graft function. In general, islet-containing alginate solution is dropped through a nozzle into a divalent cation solution, either barium chloride or calcium chloride, to generate a rigid and durable microbead incorporating an individual or few islet grafts (Fig. 2). As alginate is a polysaccharide, it will be subject to a gradual enzymatic and hydrolytic degradation under physiological conditions, let alone inflammatory conditions. Undesired quick biodegradation of alginate inherently influences the physicomechanical properties of capsules owing to structural changes, resulting in poor stability and impaired semipermeability/immunoprotection and therefore failing to achieve a sustained viability/functionality of encapsulated islets after transplantation. Basically, higher molecular weight (MW) of alginate reduces the number of reactive positions available for hydrolysis degradation, which further promotes a slower degradation rate. By changing the concentration of the alginate, it is possible to control the rate of capsule degrading or breakdown over various periods of time (ranging 3 months [≤0.5–0.75% alginate] to 1 year [≥1.5% alginate]), which correspond to the functional longevity of encapsulated pig islets. 74

The principle, technologies, and apparatus for the production of alginate-based microbead. Nozzle modes: a. simple dripping mode; b. air flow driven mode; c. electrostatic mode; d. vibration-controlled mode. Color images available online at www.liebertpub.com/teb
In general, barium crosslinkage provides alginate gels with higher dimensional stability/strength, better biocompatibility, and weaker reaction than those found with calcium75–78 ; however, the leakage of barium from alginate microcapsule and high risk of barium accumulation (chronic toxicity) largely limits its application in clinic. 79 Using low concentrations of barium ions and intensive rinsing of barium beads may be useful strategies to eliminate the safety concerns.79,80 Although different chemical formulations of alginates (e.g., high mannuronate or guluronate, high or low viscosity, with or without coupled peptide sequence) are selected for pig islet encapsulation; high mannuronic (≥50%) and high viscosity (≥100 mPa·s) alginate is considered as the most appropriate encapsulating material that possesses ideal biocompatible properties, with benefits including impermeability to natural/elicited antibodies (e.g., Ig G, 150 kDa), sufficient diffusion of nutrients/metabolites/insulin, suitable implant stability, low macrophage/lymphocyte recruitment and infiltration, as well as promotion of neoangiogenesis, and sufficient pO2 delivery (approximately 40 mmHg). 81 The favorable stability referred to slight implant degradation (−27% of initial graft weight) and inapparent fibrosis/inflammatory process. By contrast, most of the other alginates degraded at 12 weeks as evidenced by ≤50% of initial implant. The rapid degradation seems to be associated with the strong inflammatory response. In a pig-to-primate model, this type of simple alginate microcapsule could significantly prolong API survival into monkeys for up to 6 months even in the presence of antibody response. 82 No graft fibrosis or cellular overgrowth was observed, and after explantation, the residual pig islets in capsules showed the capacity to secrete insulin after glucose exposure.
In most cases, several polycations are applied as positively charged coating on the simple alginate microbead to confer better permselectivity and mechanical stability. However, selection of optimal coating material remains controversial. Ponce et al. 83 suggested that poly-l-lysine (PLL) was the best option available and that utilization of poly-l-ornithine (PLO) and poly-d-lysine (PDL) should be avoided due to ongoing inflammatory responses and high rates of capsular overgrowth. By contrast, Darrabie et al. 84 demonstrated that PLO-coated alginate microcapsule (containing pig islets) was mechanically stronger and offered better permselectivity than PLL coating, suggesting that PLO is an alternative to PLL. Others preferred PEG-PLL diblock copolymers for preventing potential protein adsorption and improving biocompatible protection on the surface of capsules.85,86 The commercial microcapsule containing pig islets, which is being tested in clinical trials, is composed of an alginate core coated with a layer of PLO and an outer coat of alginate.87,88 But degradation of the outer layer of alginate will leave the underlying layer of PLO exposed, which eventually results in decreased biocompatibility in vivo. To address the problem, chemical crosslinking/modification of PLO layer using genipin, which has the properties of neutralizing immunogenic effect of PLO and reducing protein adsorption, offers a viable solution to improve the antidegradative, biocompatible, and hydrophilic properties of alginate/PLO/alginate capsules without any adverse effects on pig islets.87,89 Lately, Hillberg el al. 90 have shown that alginate microbead coating with glycol chitosan provides improved mechanical stability and biocompatibility over conventional alginate/PLO/alginate microcapsule. Within the novel microcapsule, comparable pig islet viability (>90%) and insulin release could be maintained over a month in vitro culture.
Methods for Fabrication of Microcapsule
In general, microcapsules used for immunoisolation of pig islets are generally fabricated by the following main steps (Fig. 3)40,82,91–94: (1) Islet preparation. Adequate supply of pig islets with high viability/functionality is a prerequisite for obtaining high-grade microencapsulated islets. (2) Blending. Pig islets are suspended in the polymer solution (commonly alginate) which makes up the microbeads. (3) Droplet generation. This process disperses the mixture of polymer (alginate) and pig islets into small droplets containing few cells by different methods such as extrusion or emulsification. During this procedure, several main factors should be considered when choosing the droplet generation technique, including capability of maintaining high islet viability/functionality, good control of capsular size and shape, as well as size distribution/uniformity, and viscosity of polymer solution.95,96 (4) Stabilization. The formed droplets are then further solidified and modified to improve the strength, permselectivity, and biocompatibility of microcapsules. All these procedures are also available for microencapsulation of islets isolated from other species, including rodents and humans.97,98
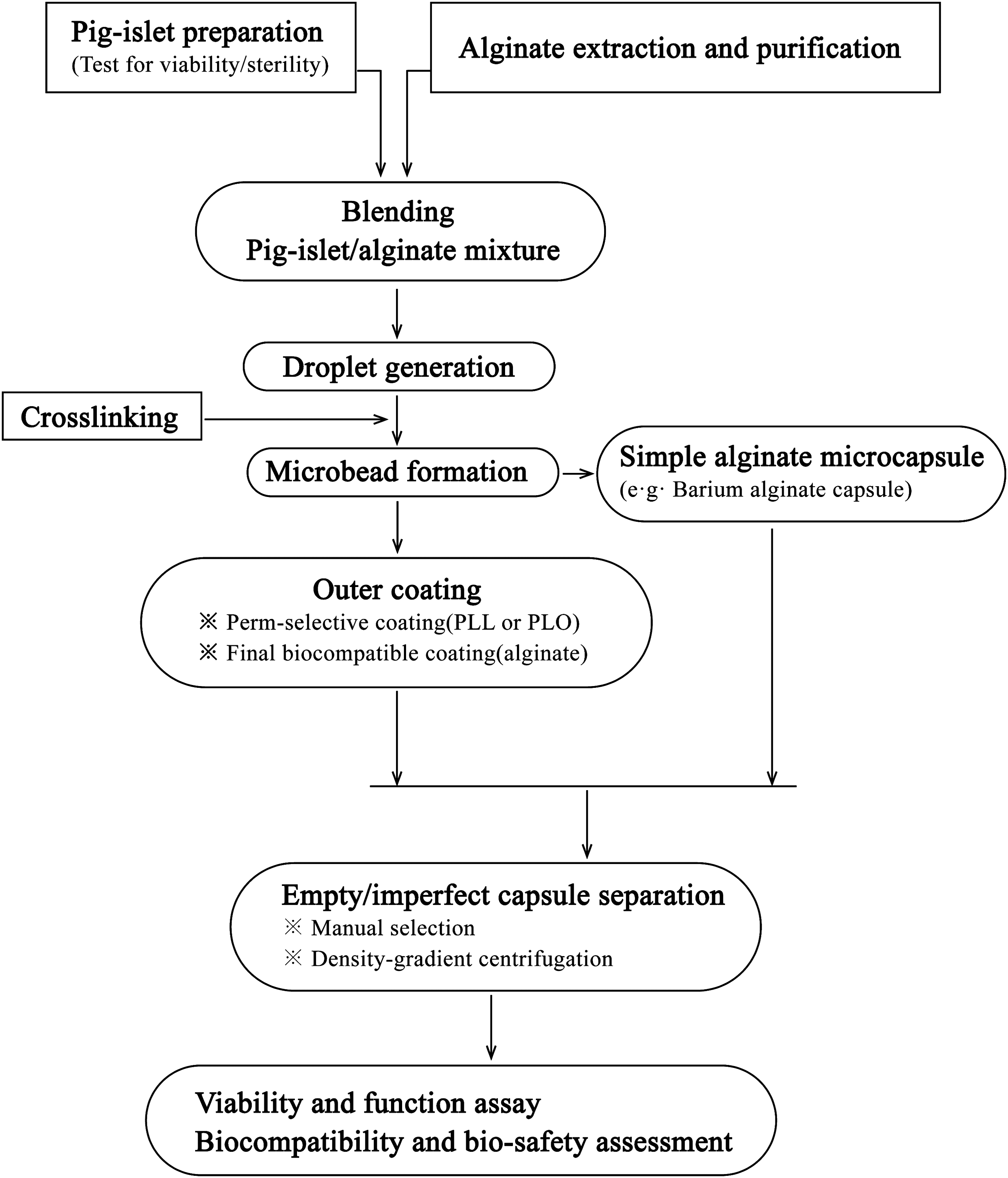
Flow chart for the fabrication of microencapsulated pig islets.
Isolation and purification of pig islets have been elaborated in published reviews.5,33,99,100 Briefly, due to the lack of exocrine tissues and concomitant relative abundance of endocrine tissues, the immature pig islets, both fetal pig islet-like cell clusters (FPICCs) and NPCCs are easy to be obtained by simple enzymatic digestion and following pretransplantation culture (4–9 days). By contrast, it is relatively difficult to obtain APIs from adult pigs, despite many experiences in this field. Achieving successful API isolation needs complete blood exsanguination, extensive flushing of pancreas, reduced warm ischemia time (WIT, within 10 min), and appropriate cold ischemia time (CIT, within 2 h). Before storage of harvested pancreas in cold preservation solution (two-layer cold storage and controlled perfusion are advisable), morphological screening and rapid assessment of pancreas should be conducted, and only IEQs/cm2 of splenic lobe biopsy is a reliable predictor of islet yield. In the subsequent digestion and purification processes, to improve pig islet yield and viability, Good Manufacturing Practices Grade Liberase MTF C/T with low endotoxin content (≤10 EU/mg) and iodixanol solution is recommended for pancreas digestion (usually in a digestion/filtration chamber) and islet purification (usually on COBE 2991 cell separator), respectively. Postisolation, in vitro culture of APIs (for 7 days, at 37°C) is also recommended for improving islet viability/secretory capacity (e.g., by increasing ATP content and oxygen consumption rate) and possibly reducing the immunogenicity, as well as stress-associated damage and cell apoptosis (e.g., by upregulating prosurvival JNK-3 expression and downregulating proapoptotic signaling of JNK1/2/c-fos).101–103 In the process of bleeding, pig islets with high quality/purity and alginate with high purity are proposed for improving the biocompatibility and longevity of the subsequently formed capsulated grafts.17,82,104,105 The alginate/pig islet proportion (commonly used concentration range of ∼3000–10, 000 islet equivalents [IEQs]/mL alginate)17,25,40,82,91,105–107 should be properly adjusted so that one capsule will contain one or few islets, with fewer empty capsules.
For dispersion, with emulsion method, the aqueous solution (containing islet cells) is mixed and dispersed in an organic solvent (e.g., oil). When the dispersion reaches equilibrium, gel formation is triggered by cooling or by the addition of a gelling agent. Although this technique can be easily scaled-up, the shear stress during the procedure may induce islet injury and the process itself can result in heterogeneous dispersion. 95 Compared with the less popular method of emulsification, extrusion is a much more practical and promising process to generate droplets by forcing the homogeneous suspension through a needle using either vibration, or coaxial airflow (called air-driven droplet generator), or electrostatic potential (called electrostatic droplet generator) (Fig. 2). Generally, greater mechanical strength and better diffusion efficiency of microcapsules are directly associated with smaller size. The vibrating nozzle technique can generate uniform-shaped microbeads with small diameter at a high production rate, but this method is limited to a relatively low viscosity of alginate (≤0.2 Pa/s). 108 Mazzitelli et al. 109 further discovered that the optimized parameters of vibrational encapsulation to obtain NPCCs containing monodisperse droplets were, 150 Hz of vibrational frequency, 1 mm of vibrational amplitude, 8.6 mL/min of alginate pumping rate, and 140 mm of distance between nozzle and surface of gelling bath, with no alternation of morphological and functional properties of the enveloped pig islets. Although electrostatic pulse system can produce smaller (250–350 μm vs. 400–880 μm in diameter) and more uniform microcapsules in comparison with air-jet technique,17,107,110,111 the high electrostatic voltage used probably interferes with pig islet viability. At present, coaxial airflow is the most commonly utilized method in producing droplets containing islet grafts, 93 and smaller capsules (≤300 μm) with narrow size distribution can also be produced by a novel micro-airflow nozzle. 112 Also, this method seems to be less sensitive for alginate with high viscosity.108,113 To reduce the occurrence of fragmented droplets, the rate of air flow or polymer solution flow should be controlled within a certain range. 114 Koo et al. 25 established an optimal condition for microencapsulation of pig islets using alginate and air-driven droplet generator. For alginate at different concentrations of 2% (wt/vol), 2.5%, and 3%, the appropriate CO2 flow rate and alginate inflow rate were (2.0 L/min, 10 mL/h), (3.0 L/min, 20 mL/h), and (4.0 L/min, 40 mL/h), respectively. Park et al. 115 successfully laminated NPCCs within small microcapsules (<200 μm in diameter, also known as conformal encapsulation) using the air-driven encapsulator under the condition of alginate (2%) flow rate of 135 mL/h, and air pressure of 0.10 bar. With several advantages over large microcapsule (600–700 μm), including reduced capsular thickness, minimal dead space, and favorable metabolite transfer (e.g., oxygen and nutrients), the small capsule can acquire better selective permeability, tolerance, relatively low oxygen tensions without massive graft loss, result in a reasonable graft volume for implantation, and significantly enhance islet viability and insulin secretory response.116–118
In the subsequent stabilization step, alginate-based droplets are converted into rigid microbeads by gelification in a divalent cation solution, mostly Ca2+. Ordinarily, the microbeads are then coated with a second layer (e.g., PLL, PLO, or PEG) and another outer layer of alginate (Fig. 1). This step may be the key tache for ensuring the mechanical stability, permeability, biocompatibility, and longevity of islet microcapsules. Also, the associated principles and some considerations have been described previously.
In addition, after microencapsulation, especially conformal encapsulation, separation of empty capsules appears to be essential since production of empty capsules results in enlargement of implant volume, as well as interference of nutrients and insulin transfer. In comparison with traditionally manual selection, the density gradient (e.g., Ficoll or Percoll)-based centrifugation is much more adaptable for large-scale processing to discard poorly encapsulated islets and generate sufficient uniformly sized encapsulated islets without any adverse effects on viability.23,119
Cryopreservation of Microencapsulated Pig islet
Considering the effective protection of fragile islet from freezing-induced damage by microencapsulation,42,107,120,121 as well as advanced microcapsule design/fabrication technology and successful preclinical transplantation studies, a banking system (by cryopreservation) that allows for effective and long-term storage of the BAP, represents a critical prerequisite for facilitating donor pooling and promoting transplantation of microencapsulated islets as available cell-based medicine since graft demand is unpredictable and just-in-time processing of encapsulated islets is impossible.
Many improvements have been made to optimize cryopreservation technology for maintaining islet viability and functionality, as well as the biointegrity of microcapsule.107,122 Zhou et al. 107 reported acceptable cryopreservation of alginate-based microencapsulated pig islets by slow-cooling protocols. The freezing process neither induced morphological change and fragmentation of pig islet nor altered surface property of the microcapsule. After rapid thawing, the encapsulated pig islets preserved in liquid nitrogen could restore normoglycemia in diabetic mice for the duration of the study (90 days). It is notable that a tightly controlled freezing rate is essential in dealing with the delicate and sensitive pig islets. Moreover, the use of nucleation (ice seeding) seems to play an important role in preserving the physiological competence of the cryopreserved islet grafts. The major challenge of slow freezing is the relatively high risk of islet injury due to ice formation.
Another approach of cryopreservation is vitrification, which is less complicated and time-consuming than the slow-freezing method. Recently, Agudelo et al. 122 developed a novel vitrification solution KYO-1 for cryopreserving encapsulated islets, which showed more superior ability to maintain morphological integrity and mechanical/physicochemical property of the agarose microcapsules in comparison with dimethylsulfoxide-based conventional freezing solution. Subsequently, in a xenogeneic transplantation model, the cryopreserved agarose-encapsulated hamster islets (storage for at least 2 weeks) could reverse hyperglycemia in diabetic mice for a long period, up to 56 days. 123 The feasibility studies serve as solid foundations for conducting available and practicable cryopreservation of microencapsulated pig islets.
As a note, the polymers (e.g., alginate, agarose) utilized for islet microencapsulation appear to be not very stable in the frozen–thaw cycle. The cryoprotectant (e.g., ethylene glycol) can directly influence the volume of alginate-based microcapsules during cryopreservation. 124 Also, the cryopreservation process probably cause changes of network structures of agarose gel as evidenced by differences in diffusion coefficients for substances with intermediate MWs before and after freezing. 125 Thus, more suitable protocol for cryopreservation needs to be developed in terms of achieving prolonged storage of encapsulated islets without any adverse effects on islet viability/functionality and capsular stability.
Other Factors Influencing Survivability and Functionality of Microencapsulated Pig islets
Xenoreaction and inflammation
Although microencapsulation suppresses direct interaction of enveloped islets and host immune system, leakage of small xenoantigens (e.g., porcine macrophage inflammatory protein-1 alpha, interleukin-8, high mobility group B1, chaperone heat shock protein 90, and non-Gal antigen) from the encapsulated pig islets may attract immunologic cell and initiate immune and/or inflammatory reaction, resulting in pericapsular fibrotic overgrowth (PFO) and xenograft failure.71,126,127 CD4+ T cells and macrophages are the primary immune effector cells recruited to the surface of microencapsulated islets and implicated in xenogeneic rejection.71,91,111,126,128
It is possible that CD4+ T cells trigger the rejection through an interferon-γ (secreted by activated CD4+ T cells)-dependent activation/accumulation of macrophages, and the macrophages are regarded as the direct effectors of xenogeneic response to encapsulated pig islets leading to rapid graft destruction.71,126,129,130 Although the encapsulation can effectively protect against large molecules such as T cells and antibodies, proinflammatory cytokines (e.g., tumor necrosis factor-α and nitric oxide) and other inflammatory molecules (e.g., interferon-γ, monocyte chemotactic protein-1, and macrophage inflammatory protein-1) secreted by these activated immune cells, as well as complements can freely diffuse through the microcapsule membrane and are responsible for the formation of cellular overgrowth and graft damage/failure.71,128,131–134 Theoretically, preventing the passage of small molecules is necessary for the adequate immunoprotection of microcapsules, but reducing the pore size of capsular membrane will also cause the inadequate diffusion of nutrients/insulin and subsequently impair islet viability/functionality. At present, a membrane's molecular weight cutoff (MWCO) of 100 kDa should at least be granted to avoid intracapsular ingress of immune cells and immunoglobulins (e.g., IgG, about 150 kDa). 135
Notably, strategies, such as macrophage depletion by clodronate liposomes, 136 inhibition of cellular immune response by short-term/low-dose traditional immunosuppressants (e.g., cyclosporine) 66 or by targeted T-cell costimulation blockade regimens (e.g., cytotoxic T lymphocyte antigen 4-immunoglobulin [CTLA4Ig], anti-CD154 antibody, and antilymphocyte function-associated antigen-1 monoclonal antibody),111,128,137,138 and induction of localized immunomodulation using syngeneic Sertoli cell, 139 have effectually delayed the sensitization of host and led to prolonged survival/improved functionality of encapsulated pig islets. Recent study involving encapsulated pig islets in alginate microcapsules incorporating anti-inflammatory chemokine CXCL12, which could repel effector T cells and selectively recruit suppressive regulatory T cell (Tregs), dramatically resulted in delayed xenogeneic rejection and diminished cellular infiltration (macrophage and fibroblast) around the capsules, and consequently led to long-term xenoislet survival/function without systemic immune suppression. 140 In the future, studies exploring the (1) more exact mechanism and procedure of xenogeneic immune response to encapsulated xenoislets, especially in primate or humanized models, (2) highly biocompatible membrane with a critical pore size, which offers adequate immunoprotection without compromising islet viability and function, (3) optimized combination of microencapsulation and more specific immunosuppressive treatment, and (4) encapsulation of genetically modified islets54,55,141–144 (e.g., Gal and N-glycolylneuraminic acid gene knockout pig islets, TF knockdown pig islets, CTLA4Ig transgenic pig islets, human HO-1 transgenic pig islets, transgenic islets that are resistant to the deleterious effects of inflammatory cytokines, and multitransgenic pig islets) will advance the possibility of utilizing microencapsulated pig islets as a treatment for IDDM patients.
Biocompatibility
The similar survival times in both encapsulated islet allo- and isografts 145 indicate that immune response alone may not be the cause of graft failure. Insufficient biocompatibility of encapsulation membrane still can induce a nonspecific foreign body reaction against the capsules, and contribute a lot to the process of PFO and subsequent graft failure. 146
It is very important that material selected for microencapsulation should be biocompatible, and some of these have been discussed in detail previously. Besides, the purity of the encapsulation material is another vital factor influencing the capsule's biocompatibility. Alginate is an originally crude product extracted from algae, contaminated with some inflammation-provoking impurities such as endotoxins/pyrogens, polyphenols, and heterologous proteins. Recent study further demonstrated that pathogen-associated molecular patterns (PAMPs) in alginate were potent immunostimulatory agents. 147 The varying degrees of purity may help to explain for the disputes in studies concerning the cause of bioincompatibility of alginate microbeads with or without outer coating. Thus, the commercially available alginate must undergo an unltrapurification procedure to obtain a clinical-grade alginate product with extremely high degree of purity and lack of PAMP/protein/heavy metal contents, which are essential to avoid activation of innate immune system of recipient, for improving capsular biocompatibility and reducing PFO, and for enhancing insulin secretory activity and islet survival.104,145,147–151 However, so far, these noninflammatory alginates with improved biocompatibility are only produced on a laboratory scale and are not yet commercially available.
Irregularities in microcapsule shape can also impair encapsulated pig islet biocompatibility and lead to PFO or capsular breakage. 82 To obtain a long-term biocompatibility of capsule, a high percentage (≥90%) of regular, spherical shape of capsule with smooth surface is needed as irregularity and roughness tend to allow for immune cell adhesion and activation. Furthermore, there is a close relationship between the capsule shape and the pig islet purity. The contamination of exocrine cells will disturb the laminar jet of encapsulation device and consequently result in decreased percentage of well-shaped capsules. Therefore, pig islets with high purity (≥90%) are preferred for microencapsulation.
Implant site
The implant site in which microencapsulated pig islets are in close contact with blood flow is a requisite for successful transplantation due to advantage of sufficient/rapid diffusion of nutrient/oxygen and prompt delivery of secreted insulin, which are important factors affecting functional performance and longevity of the capsulated pig islets.
Organs with a rich blood supply such as liver and spleen, which are the frequently used locations for free islet (approximately 100–150 μm in diameter) transplantation in diabetic patients152–153 or large animals155,156 with favorable outcomes, seem to be unable to accommodate the dramatically increased implant volumes after islet microencapsulation (600–800 μm in diameter), especially in transplantation into primate recipients. Thus, in most of the studies, transplantation of microencapsulated pig islets into primates is intraperitoneal (Table 1) since the peritoneal cavity is suitable for the implantation of large graft volumes and allows for physiological insulin delivery.16–18,69 Although the process is much more simple and convenient through injection or laparoscopic implantation, the peritoneum, a relatively avascular site, is less favorable for the engraftment of microencapsulated pig islets on account of more inflammatory cell (macrophage and lymphocyte) aggregation and limited oxygen/nutrient diffusion.106,129,157 By contrast, in nondiabetic rats, subcapsular kidney and subcutaneous space display weaker cellular reaction, better islet viability, and less broken capsules than peritoneum, 106 rendering these two sites interesting alternatives.19,82 Nevertheless, space is limited in the kidney capsule, precluding this location suitable for implantation of large volumes of grafts in diabetic large animals or humans. Furthermore, this implant site does not represent an oxygen-rich environment for islet engraftment. 158 Indeed, the subcapsular kidney currently appears to provide no marked benefit for clinical transplantation of encapsulated islet.
With advantages of a relatively large space, easy accessibility for graft placement/retrieval, and biopsy with minimal complications, subcutaneous space is considered as an attractive candidate site for implantation of encapsulated islets. Several studies demonstrated the successful xenotransplantation of encapsulated pig islets into the subcutaneous space.19,81,106,159,160 Notably, insufficient oxygenation can hamper the long-term survival/functionality of capsulated pig islets in sparsely vascularized implant site, particularly in subcutaneous tissue. However, prevascularization of subcutaneous site159,161 or preimplantation of empty subcutaneous devices,162,163 or the current coencapsulation of pig islets and mesenchymal stem cells160,164 offers very useful strategy to improve the implant oxygenation and neoangiogenesis, as well as to reduce the hypoxic stress of intragrafts and to minimize the number of islets needed to reverse diabetes.
In addition, due to the advantages of well vascularization and relatively easy access, striated muscle 165 and bone marrow 166 reported recently offer alternative locations for the implantation of microencapsulated islets. However, they are not yet fully and perfectly characterized regarding sustained islet viability and functionality.
Biosafety and Clinical Trials
Safety
The risk of transmission of porcine pathogens (e.g., bacteria, protozoa, fungi, and viruses) remains a key issue before large-scale clinical application of pig islet xenografts.167–170 Most microorganisms can be eliminated by rearing pig donors under qualified and SPF conditions, respectively. Nevertheless, this is not possible in the case of porcine endogenous retroviruses (PERVs), which are integrated into the pig genomes 171 and display the potential of cross-species transmission to human HK-293 cells in vitro 172 and to severe combined immunodeficiency (SCID) mice in vivo.173,174 Although PERV represents a continuing concern, most of the published studies suggested that no evidence of PERV or other porcine virus infections was observed in the recipients such as dogs,175–177 diabetic monkeys,18,178 and diabetic patients47,179–181 after transplantation of free or encapsulated pig islets. Although the pig islets contain PERV DNA and RNA, it seems unlikely that the PERVs can traverse the capsules used and then cause infections (Table 1).18,47,182
Most notably, the recent data further demonstrated the microbiological safety in the first clinical trial of pig islet (alginate-microencapsulated) transplantation in New Zealand.27,72 At all stages of rigorous safety assessment, no transmission of either PERVs or other potentially zoonotic pathogens, such as porcine circovirus (PCV), porcine lymphotropic herpes virus (PLHV), and porcine cytomegalovirus (PCMV), were detected by PCR and immunological methods. All these findings strongly indicate the biosafety of xenotransplantation of encapsulated pig islets. However, an important point to be stressed is that lack of evidence for transmission of porcine pathogens dose not exclude such a possibility in future clinical application. Therefore, at present, both source pig herd and recipient need to be extensively screened and monitored for cross-species infection by combining available and sensitive methods (e.g., cocultivation, microarray analysis, and RNA-Seq).183–185
Recently, RNA interference (RNAi) is a promising option for knocking down PERV expression in pig primary cells or donors,186–188 and a long-term (≥3 years) efficacy of inhibition of PERV expression has been confirmed in the transgenic pig expressing PERV-specific small hairpin RNA (shRNA). 189 It seems likely that this strategy may be helpful to improve the biosecurity of pig xenotransplants. In the near future, with the emergence and development of PERV and other pathogens (PCV, PLHV, and hepatitis E virus et al.) gene knockout pigs, as well as more specific and effective antiretroviral drugs and vaccines, the biosafety risk will be reduced significantly or even eliminated completely.
Clinical studies
The first long-term (≥9.5 years) viability and functionality of microencapsulated pig islet in clinical trials was reported by Elliott et al. 16 In May 1996, a 41-year-old male patient with T1DM for 18 years was intraperitoneally xenotransplanted with alginate-based microencapsulated NPCCs (15, 000 IEQs/kg) through laparoscopy. After implantation, his average daily insulin dose was reduced for the following 14 months by up to 30%, and the exogenous insulin requirement returned to the pretransplant level at week 49. Also, amelioration in glycemic control continued as evidenced by repeatedly lower glycated hemoglobin (HbA1c) levels (ranging from 7.6% to 8.2%, compared with the pretransplant value of 9.3%) during the 14-month follow-up period. More importantly, at laparoscopy 9.5 years posttransplantation (in March 2005), a number of microcapsules retrieved were intact and still contained viable and functional pig islets, which could secrete insulin in response to glucose stimulation. Additionally, neither peritoneal reaction/fibrosis nor porcine viral/retroviral infection was detected in the recipient. The single case first confirmed the therapeutic effect of microencapsulated pig islets in a diabetic patient without immunosuppressive medication, indicating the necessity to conduct large-scale clinical trials.
In 2007, a phase I/IIa clinical study of microencapsulated pig islets (also called DIABECELL) was conducted by the LCT Company.43,190 A total of eight patients with T1DM were transplanted with DIABECELL (5000–10, 000 IEQ/kg) intra-abdominally. Two patients were completely independent with insulin administration for up to 32 weeks, and six patients showed improved blood glucose control as reflected by reduced HbA1c levels and daily insulin requirement. Following the successful completion of this clinical trial in Russia, LCT launched another phase I/IIa trial under the current framework of regulations of xenotransplantation in New Zealand and recently released the obtained clinical outcomes. 72 From October 2009 to March 2011, alginate/PLO/alginate-encapsulated NPCCs (5000–20, 000 IEQ/kg) were intraperitoneally implanted into nonimmunosuppressed patients (n=14) with unstable T1DM. After transplantation, the numbers of unaware hypoglycemia events were significantly decreased in all patients. However, the efficacy of reducing HbA1c level and insulin dose was not marked. The relatively low efficacy in this trial may be due to insufficient implantation of islet grafts since it is assumed that adequate number (40, 000 IEQ/kg) of microencapsulated NPCCs is necessary to achieve insulin independence in a clinical setting. Currently, a Phase IIa Safety and Efficacy Study are under way in Argentina.
To be clear, all these clinical trials cannot be considered as true breakthroughs for the treatment of T1DM currently, since no exogenous insulin administration was interrupted and the metabolic control was not very excellent. Yet, the trials confirmed the security, biosafety, and therapeutic potential of transplantation of microencapsulated pig islets into humans. Therefore, further improvements are needed to improve the clinical outcomes and develop a consensus statement in the future.
Conclusions
The BAP comprised of microencapsulated pig islets may overcome the major obstacles to islet transplantation: shortage of donor supply and extensive use of immunosuppressants. Although pilot preclinical/clinical trials demonstrate the safety, practicability, efficacy, and promise of microencapsulated pig islet xenotransplantation, the currently available therapy is far away from the final possible cure of T1DM. Several major obstacles remain to be overcome: reinforced immune protection, enhanced oxygen/nutrients supply and transfer for capsulated islets, reduced activation of destructive host immune reaction, and improved survival and functionality of islet xenografts when implanted. It is expected that sufficient supplies of pig islets or renewable insulin-producing cells with high quality and low xenoantigenicity, coupled with optimization of capsule design/size/preparation, advances in biomimetic materials, and immunomodulatory strategies, as well as better selection and bioengineering of the capsules' site of implantation may potentially lead to a reliable and sustained glycemic control. Furthermore, the achievements made in successful xenotransplantation of microencapsulated pig islets will provide potential guidance for the application of other bioartificial organs.
Footnotes
Acknowledgment
The authors thank Dr. Ning Jing for the help in editing the article.
Disclosure Statement
No competing financial interests exist.