
Abstract
Recent advances in the fields of artificial organs and regenerative medicine are now joining forces in the areas of organ transplantation and bioengineering to solve continued challenges for patients with end-stage renal disease. The waiting lists for those needing a transplant continue to exceed demand. Dialysis, while effective, brings different challenges, including quality of life and susceptibility to infection. Unfortunately, the majority of research outputs are far from delivering satisfactory solutions. Current efforts are focused on providing a self-standing device able to recapitulate kidney function. In this review, we focus on two remarkable innovations that may offer significant clinical impact in the field of renal replacement therapy: the implantable artificial renal assist device (RAD) and the transplantable bioengineered kidney. The artificial RAD strategy utilizes micromachining techniques to fabricate a biohybrid system able to mimic renal morphology and function. The current trend in kidney bioengineering exploits the structure of the native organ to produce a kidney that is ready to be transplanted. Although these two systems stem from different technological approaches, they are both designed to be implantable, long lasting, and free standing to allow patients with kidney failure to be autonomous. However, for both of them, there are relevant issues that must be addressed before translation into clinical use and these are discussed in this review.
Introduction
K
According to the Organ Procurement and Transplant Network, 17,108 kidney transplants were performed in 2014, leaving more than 101,000 patients on waiting lists. 3 Dialyzed patients with ESRD still face major medical, social, and economic complications that strikingly jeopardize the quality of life. 4 The gap between donor pool and organs needed is driven in large part to several complex issues that include, but are not limited to, more rigorous graft evaluation. The increase in diabetes, atherosclerosis, and an ever-increasing older population, all contribute to compromised kidneys and ESRD. The National Institute of Diabetes, Digestive and Kidney Diseases reports that the 5-year survival rate for patients with ESRD is 35.8% for dialyzed patients versus 85.5% for transplanted patients. 5 The reason being that kidneys play a crucial role in the regulation of cardiovascular tone, hematopoiesis, and electrolyte and endocrine equilibrium. 6 Thus a successful renal replacement therapy (RRT) requires replication of all renal function by complementing the capabilities of the inanimate dialysis membranes with the innate biological functions of renal tubular epithelial cells. 7 This review focus on the latest frontier of RRT, the implantable artificial kidney produced by micromachining techniques and the bioengineered kidney based on biological templates seeded with suitable cell lines.8,9 These two systems offer different technological approaches and both are designed to be implantable, long lasting, and free standing so as to give patients with kidney failure autonomy. Figure 1 depicts the proposed connection between these two therapeutic options.
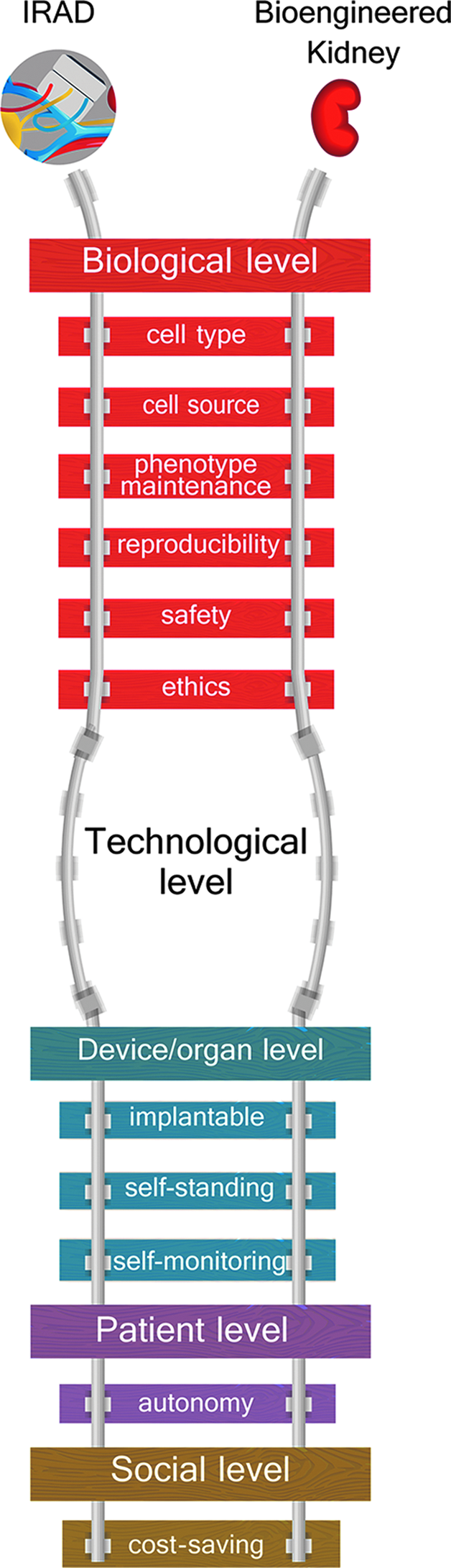
Implantable renal assist device (iRAD) and the bioengineered kidney. Proposed schematic that depicts commonality and potential interrelationships. The iRAD and the bioengineered kidney based on biological templates are currently the most promising alternatives in the field of renal replacement therapy (RRT). Although based on different technologies, they are the only two in-development systems designed to recapitulate the whole kidney function in patients with end-stage renal disease. This figure reports these two approaches and what they have in common, including basic biological concepts and device/organ general features, as well as clinical and social aspects. Color images available online at www.liebertpub.com/teb
From Renal Assist Device to Implantable Renal Assist Device: Challenges of the Implantable Artificial Kidney
To date in the field of RRT, the only device approved for clinical trials by the food and drug administration (FDA) is the renal assist device (RAD) developed by (Fig. 2) Humes. 10 The RAD is a hollow-fiber standard hemofilter seeded with tubule renal cells. It was employed for up to 72 h in addition to conventional continuous RRT (CRRT) to treat 40 patients with acute kidney injury. After 6 months, a significantly higher survival rate was reported for these patients in comparison with those treated with only conventional CRRT. 11
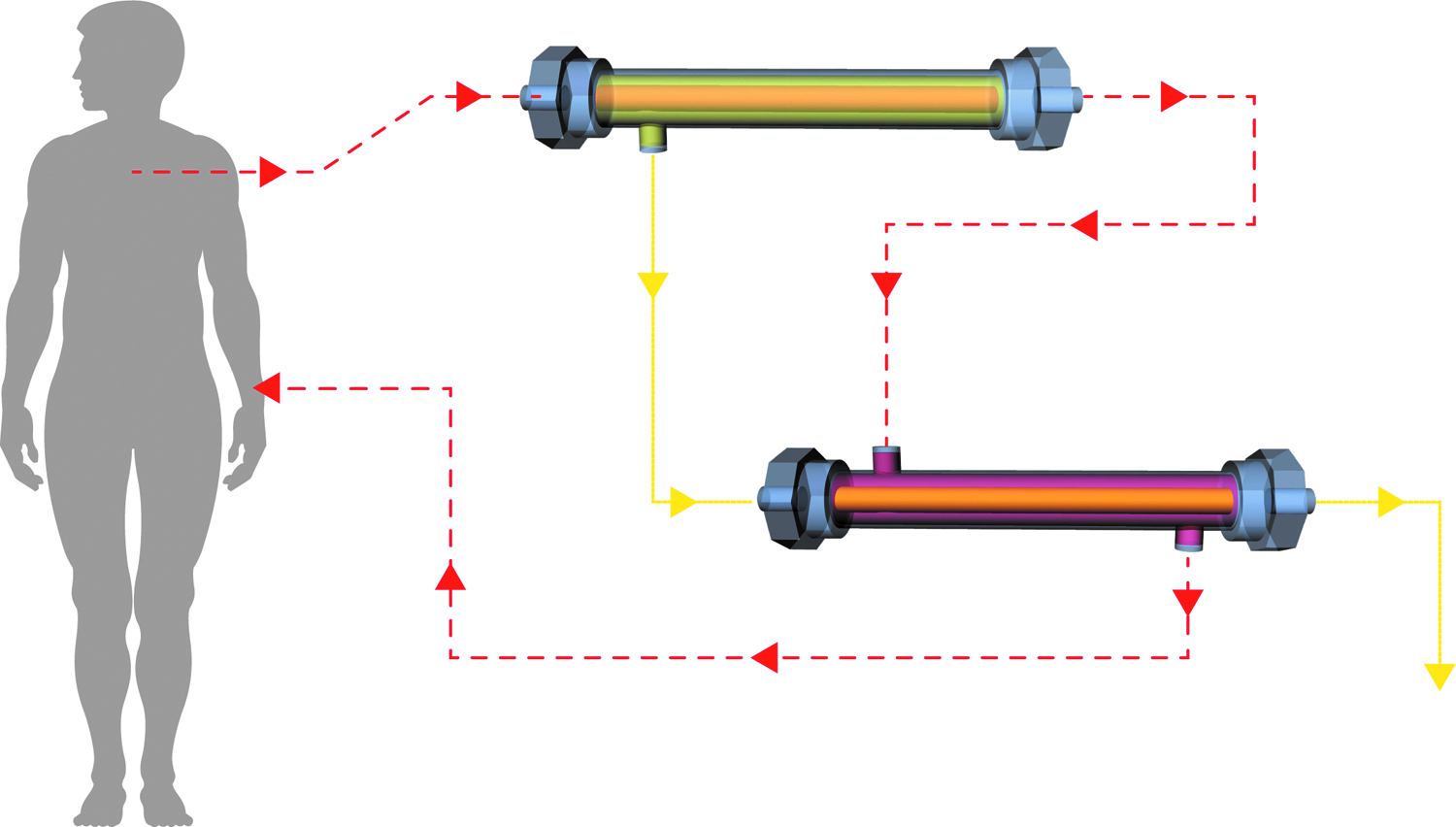
The RAD circuit. This circuit is made of two components, a standard hemofilter and a bioreactor (RAD), containing living tubule renal cells. The ultrafiltrate (continuous arrows) produced by the hemofilter enters the RAD lumen where it is processed and then discarded. In contrast, the blood (dashed arrows) that exits the hemofilter is delivered to the extracapillary space of the RAD and then returned to the patient. Color images available online at www.liebertpub.com/teb
Regrettably, a follow-up phase IIb study was discontinued after an interim analysis revealed an unpredicted high survival rate in patients treated with sham RAD without cells. 11 Notwithstanding its historic significance, this trial highlighted the need to complement RAD treatment with conventional systems, together with crucial limitations related to clinical protocol and device manufacturing. 11 In this context, Roy 12 and Fissell pioneered a breakthrough that encompassed the development of an implantable RAD (iRAD) that is reportedly entering clinical trials soon. 13
The iRAD will have a package size of 0.1 m2 and comprise two chambers, both containing silicon nanopore membranes (SNMs). The first chamber will act as a hemofilter, removing toxins, excess water, and salts, while the second unit will be a bioreactor and include SNMs seeded with renal proximal tubule cells. These cells will selectively reabsorb water and salts, also allowing the excretion of toxins through the bladder.8,14 A study focused on the interaction between SNMs and human cortical epithelial cells revealed that cells, when cultured for 10 days on these membranes, formed a confluent monolayer displaying tight junctions. In addition, transepithelial resistance, measured as a marker of cell polarization and differentiation, was comparable to that of polyester membranes commonly used for cell culture. However, only 50% of the cells were shown to have central cilia, suggesting that a longer culture time may be required for phenotypical maturation. 15 Within the iRAD, the SNMs play several crucial roles, including: (i) serving as a scaffold for the cells, (ii) providing immunoisolation, and (iii) allowing high ultrafiltration performance. The latter will enable the iRAD to function by relying exclusively on blood pressure. The candidate site for the iRAD implantation is the pelvis, where it will be connected to rather delicate anatomical sites, such as iliac vessels and the bladder (Fig. 3). In addition, the device is expected to be permanent and enable easy replacement of damaged components.

The implantable artificial kidney: MEMS technology applied to RRT. Schematic representation of the complex processes underlying the fabrication of the implantable artificial kidney and the final application of the device.
iRAD: technical aspects
iRAD is based on “microelectromechanical systems” (MEMS), a toolkit borrowed from the semiconductor industry. MEMS allow the production of miniaturized, streamlined, and cost-effective SNMs that embody a technological revolution of sorts in the field of RRT. In brief, the main technological steps leading to the fabrication of SNMs are depicted in Figure 3 and include the following: (i) deposition of a polysilicon thin film on top of a semiconductor substrate (usually crystalline silicon), (ii) the patterning of the polysilicon surface by photolithographic techniques, and (iii) the controlled growth of “sacrificial” silicon oxide. 16 The combination of the two latter steps plays a crucial role in the production of SNMs with uniform shape and size. Notably, this technique allows the fabrication of membranes with pores as small as 5 nm. 15 In particular, these membranes exhibit slit-shaped pores that enable them to closely resemble a significant feature of the glomerular filtration barrier. The glomerular filter is a size and charge selective barrier comprising three interacting layers: a fenestrated endothelium, the glomerular basement membrane (GBM), and a specialized epithelium. The endothelium contains pores of 70–100 nm and together with its glycocalyx form the endothelial surface layer.17,18 The GBM comprised a unique extracellular matrix composed of several proteins. Among them, laminin and type IV collagen are critical for membrane organization and function.19,20 The distal layer of the filtration barrier is composed of highly differentiated epithelial cells called podocytes, which feature interdigitating foot processes. 21 These extensions are linked by unique intercellular junctions generating the glomerular slit diaphragm, which is a key component of the filtration barrier.22,23 Although the integrity of these layers and complex interactions are essential to guarantee the physiological permselectivity of the glomerular filter, the slit diaphragm seems to be particularly significant in size-based plasma protein retention.24–26 It is unclear, however, whether the functional performance of the slit diaphragm produced by MEMS can replicate the characteristics of those in the native kidney.
Intriguing data about the impact of pore geometry on the ultrafiltration ability of SNMs were provided by Kanani et al. who compared the performance of polyethylene glycol (PEG)-coated membranes containing slit-shaped pores to those with cylindrical ones. 27 This study showed that ultrafiltration efficiency, in terms of selectivity/permeability balance, is greatly enhanced by uniformly sized slit-shaped pores. This feature enables a more accurate reproduction of the kidney filter compared to other membranes produced to date. 28 In addition, coupling silicon with polymers enhances biocompatibility, which is a key issue necessary to prevent device failure. Nanoporous silicon, indeed, tends to trigger the coagulation cascade in a blood-contacting milieu. 29 To address this, silicon membranes coated with PEG, a widely recognized antifouling polymer, were tested in the preclinical setting. 30 In particular, they showed good biocompatibility in a model of intravascular implantation. 31
In contrast, in case of exposure to oxygen and transition metal ions, PEG autoxidation may occur implying a reduction of its antifouling properties. 32 In view of this, Li et al. coated the membranes with a thin film of poly(sulfobetaine methacrylate) (polySBMA), a zwitterionic polymer used as an antifouling agent. They evaluated hemocompatibility based on the degree of fibrinogen adsorption when the polySBMA-coated silicon membrane was exposed to a fibrinogen solution and human plasma. Compared to a PEG-coated silicon substrate, the polySBMA-coated silicon membrane exhibited similar or higher fibrinogen repelling properties. In addition, following coating, both membrane permeability and chemical stability were maintained. Collectively, these findings support using polySBMA as an antifouling coating of silicon membranes for implantable devices.
iRAD: biological aspects
The combination of living cells and artificial devices has raised some critical issues related to cell source, type, and expansion, but also to phenotype modifications over time, safety, and reproducibility. In dealing with the cell source, pig kidneys have always been considered a natural choice, due to the recognized similarities between porcine and human tissues. In addition, a reliable protocol for cell isolation and expansion from pig kidneys has already been established.33,34 However, this option was abandoned because of the potential risk for patients to become infected by porcine endogenous retroviruses.35,36 Therefore, the focus was moved to the use of human cells. In this light, Humes et al. assessed the performance of human renal proximal tubule cells isolated from discarded kidneys. 37 These cells were harvested and seeded into the RAD and tested in an animal model of uremia. The cells within the device remained highly viable and functional for 24 h.
Some years later, Fissell et al. focused on the interaction between SNMs and human cortical epithelial cells. The study revealed that cells, when cultured for 10 days on these membranes, formed a confluent monolayer displaying tight junctions. In addition, transepithelial resistance, measured as a marker of cell polarization and differentiation, was comparable to that of polyester membranes commonly used for cell culture. However, only 50% of the cells were shown to have central cilia suggesting that a longer culture time may be required for phenotypical maturation. 15 Nevertheless, the use of human primary tubular cells also raises important issues. First, there is a limited source of these cells, with a relatively low reproducibility of cell performance due to high interdonor variability, 38 as well as the tendency of the cells to dedifferentiate during in vitro culturing.39,40 These preliminary results emphasized the need for an unlimited source of human cells. In this perspective, either stem cells or cells expressing a stem-like phenotype were considered a good choice because of their potential to evolve into diverse renal cell lineages. 41 One important consideration is that cells have to be reasonably differentiated so as to enable seeding into an artificial device. 42
These ideas and hurdles encouraged the development of reliable protocols for guiding in vitro differentiation of stem cells into different renal cell types. 42 In particular, renal proximal tubular cells (PTCs) drew huge interest because of their ability to recapitulate the majority of kidney functions. 43 In this context, Narayanan et al. reported noteworthy results about the possibility to direct differentiation of human embryonic stem cells (hESCs) into renal PTCs in a reproducible manner. These PTCs were able to recapitulate some of the tubular structures both in vitro and in immunodeficient mice. 41 In addition, they were able to maintain a differentiated phenotype when cultured into a bioreactor, an essential requirement for cells when seeded into a bioartificial device.42,44
The protocol described by Narayanan et al. cannot be considered a concrete option yet, however. First, the valuable information regarding morphological and functional characterizations is only partially characterized and needs to be further assessed. 41 Second, the use of hESCs presently suffers from bioethical limitations. The FDA does not yet approve these cells for clinical use. 45 In this framework, a novel strategy has been proposed to address the issues of cell source, type, and expansion, based on a safe and reproducible protocol. This novel approach involves the use of adult human renal epithelial progenitor cells (hRECs) with enhanced propagation (EP) ability that would make organs that are unsuitable for transplantation a real source of nonautologous cells.46,47 Westover et al. developed the EP method to gain a sufficient biomass for cell-based therapies by promoting the expansion of resident kidney precursor cells from tissue samples. The EP protocol has been shown to guarantee a cell yield increase of 10.3 ± 1.4 doublings over standard methods. 46 Noteworthy, the study that showed the efficacy of the protocol in improving cell yield used kidneys from donors with a suboptimal health profile, revealing the potential of this procedure in extending the donor pool. In addition, this technique when applied to a kidney biopsy taken from the patient may provide a precious source of autologous cells. On the other hand, the high isolation yield gained by the EP method entails the cryopreservation of a large amount of cells for clinical use, which brings its own set of challenges.
Westover and colleagues improved the protocol to cryopreserve hRECs isolated by the EP method in accordance with FDA guidelines. 48 Retention of therapeutic potential after thawing was evaluated by measuring the γGT activity and Interleukin eight levels after lipopolysaccharide stimulation. These two parameters indicate cell response to inflammation and oxidative stress, mechanisms that are generally altered in ESRD. 46 Based on these results, the EP protocol applied to hRECs seems to hold great potential in relation to iRAD. It is now mandatory to test the interaction of both fresh and thawed cells with SNMs, as well as assess cell behavior under both conditions when the cellularized membranes are included in the device.
Challenges and future directions
Important milestones have been achieved in the development of the iRAD, however, the majority of reported studies primarily concern technological features related to device miniaturization and SNM engineering.14,27,32 The reported advances are unquestionably important, however, they do not yet provide an understanding of what extent the iRAD would be able to replace renal function. In particular, there is a significant informational gap regarding device testing in preclinical models, except in the case of single components that have been tested, but so far only in rodents. 31 These concerns not only involve the interactions within the device components and the entire device with the host but also the functional performance of iRAD in preclinical models of kidney damage. This gap makes it difficult to understand the real efficiency of the device in the host to replace native kidney function. These studies are ongoing and only time will tell how they will perform in clinical trials.
Biological Templates and Kidney Bioengineering: A Novel Approach to Organ Transplantation
Over the last decade, significant progress has been made in the field of organ engineering, mostly related to the replacement of hollow tissue structures, that is, trachea, urinary bladder, and blood vessels.49–51 A valuable technology for parenchymal organs has been developed to produce “organ-shaped” scaffolds with preserved extracellular matrices (ECM) and vascular networks. This strategy is based on perfusing the organ with specific detergents under pressure-controlled conditions and is aimed to create decellularized templates ready to be seeded with suitable cell lines (Fig. 4). This technique was first applied to the kidney by Ross et al. who produced an acellular scaffold from a rat kidney, then repopulated with pluripotent murine ESCs. 52 These methodologies require multistep processes toward creating a functional bioengineered kidney, which is discussed below.

From acellular bioscaffolds to bioengineered kidneys. The creation of a bioengineered kidney is based on three main steps: organ decellularization (
Toward the ideal ECM scaffold
The preparation of acellular ECM scaffolds with preserved structure and biochemical cues is the first critical step toward creation of a functional bioengineered kidney. In the aforementioned seminal work, Ross et al. optimized a protocol to create kidney acellular scaffolds with preserved architecture and matrix signals necessary to support stem cell proliferation and differentiation. 52 The choice of using ESCs was inspired by the cellular complexity of the kidney, where nearly 30 cell types function in harmony.
The orchestration of this heterogeneous population is highly challenging. In contrast, ESCs are potentially able to differentiate into numerous renal cell types.53,54 In addition, the persistence of matrix signals may limit the risk of teratoma formation, which is a major concern related to the use of ESCs. However, this aspect is still hypothetical and has not been specifically defined. The decellularization procedure, applied to a rat kidney, was based on the use of nonionic (Triton X-100) and ionic sodium dodecyl sulfate (SDS) detergents that, together with the enzyme deoxyribonuclease 1, allowed the removal of cellular contents, degradation of nuclear membranes and constituents, as well as elimination of cellular debris. Next, murine pluripotent ESCs were seeded onto the remaining matrix by antegrade or retrograde infusion performed through the renal artery or through the ureter, respectively. The seeded scaffold was then cultured under dynamic conditions, to mimic in vivo hemodynamic and mechanical cues and to enhance nutrient delivery and waste removal. The feasibility and proof of principle were confirmed using the immunohistochemical markers Ki-67 for cell proliferation and Pax-2, Ksp-cadherin, and pan-cytokeratin for cellular differentiation. Regarding the seeding route, arterial infusion resulted in cell retention of >95% at the vascular and glomerular levels. Infusion made through the ureter was >50% in cell retention. In both cases, cells remained confined to the specific compartment, vascular or tubular, where the infusion was performed. These results were undeniably significant considering that this study was the first in a long series and, as such, a very early stage toward the development of mature tissue. Certainly, the improvements in the culture conditions of the seeded scaffold, including perfusion systems and the modulation of mechanical stimuli, are essential to establishing a more in vivo-like milieu. Likewise the addition of specific growth factors may encourage tubule differentiation and vasculature endothelialization. However, as has been shown in more recent studies, there is a critical role for site-specific engraftment dictated by the recellularization strategy.55–57
The essential role of an intact ECM in guiding cellular behavior and organ maturation was described by Caralt et al. who established a useful scoring system to assess the preservation of both the microarchitecture and the vascular network. This system also evaluates the degree of decellularization and ability of the matrix to retain key growth factors. Applying this criterion to rat kidneys, the use of Triton/SDS for the organ perfusion was more effective than Triton alone or a trypsin–ethylene glycol tetraacetic acid mixture. Indeed, when implanted in rats for 3 h, Triton/SDS-decellularized scaffolds supported systemic blood flow properly. To investigate the ability of the ECM in guiding cell behavior, the scaffold was seeded through the renal artery by low-pressure injection of human endothelial cells (ECs) and by high-pressure infusion of human epithelial cells. ECs repopulated the vascular tree, as expected, while epithelial cells infused at high pressure were able to migrate to the parenchyma and peritubular spaces, showing a 50% recellularization of the entire organ. 58
The optimized decellularization protocol and the seeding strategy based on the infusion of epithelial cells at high pressure are valuable, however, the results reported are partial and most likely different from what can be obtained in human-sized organs. On the other hand, the architecture of rat kidney papillae probably does not favor homogeneous cell dispersion and is something that may be improved in kidneys from pigs or other species. 52 In contrast, the criteria underlying the scoring method can be easily translated to evaluate the potential of acellular scaffolds in the clinical setting. It could be particularly useful in the case of human discarded kidneys where protocol standardization and scaffold evaluation can be complicated by the presence of scar tissue and interdonor variability. 59
Bonandrini et al. using a protocol based exclusively on SDS proposed a further improved decellularization procedure. 61 They produced rat ECM scaffolds with a highly preserved extracellular matrix in a relatively short time. Decellularization was completed after 17 h of perfusion and this was a clear improvement compared to the 5 day protocol applied to the same species. However, these results showed no difference when compared to more recent protocols that have been developed.52,55,60 Although the data describing the use of SDS alone are interesting, the preservation of elastin, collagen IV, and laminin and the integrity of GBM were demonstrated in studies that included the use of Tryton during decellularization.55,58,60
Important findings were revealed when low-pressure arterial infusion of mouse ESCs was performed into the decellularized scaffold in combination with 24 and 72 h of cell medium recirculation. After 24 h, cells appeared homogeneously engrafted into the vascular structures up to glomerular capillaries but also, in some cases, at the peritubular level. In addition, proliferation and differentiation toward endothelial and epithelial lineages occurred over 72 h, as revealed by immunostaining for the endothelial markers, CD-31 and Tie 2, and the neuronal cell adhesion molecule. 61 Interestingly, the data involving cell engraftment following arterial infusion reported in this study are similar to those shown in the case of seeding made through both the artery and the ureter. This suggests that the use of a double route is not sufficient to guarantee a homogeneous engraftment. 55 On the other hand, the issue of an effective seeding strategy is the focus of several current and ongoing studies.56,57 Furthermore, the SDS-based decellularization and improved scaffold repopulation findings with dynamic perfusion would be much more advanced by proving protocol scalability to human or large animal kidneys.
In this perspective, Sullivan et al. scaled up the decellularization process to human-sized kidneys and developed a high-throughput system able to process up to 24 pig organs. First, they identified the most effective and reproducible decellularization protocol showing that the use of 0.5% SDS resulted in acellular scaffolds with high biocompatibility. The constructs produced using the high-throughput system maintained well-preserved architecture, vascular networks, and ECM. Furthermore, primary human cells after seeding on scaffold samples grew over 4 days showing an appropriate cytocompatibility. 62 The high-throughput system holds potential as a platform to produce organs suitable for transplantation. However, the final ECM characterization following decellularization is limited to glycosaminoglycans and collagens, so it is not sufficient to establish the ECM potential in influencing cell behavior after seeding. Additional information regarding growth factor retention would better characterize the outputs of the described system. Furthermore, it would be of high interest to investigate how the properties of the scaffolds produced by the high-throughput system impact cellular distribution after seeding and the ensuing tissue organization during bioreactor culturing.
Uzarski et al. developed a dual-purpose scalable perfusion bioreactor. This device enables monitoring of the dynamic changes occurring in the seeded scaffold during tissue maturation and thus improves repopulating strategies. In addition, it allowed seeding under vacuum to increase the efficacy of cell infusion through the ureter as previously reported. 54 The proposed methodology enhanced scaffold properties, recellularization efficiency, and cell performance through analysis of the physical and biochemical markers expressed in kidney ECM scaffolds. The authors produced acellular scaffolds from rat kidneys, then repopulated with human renal tubular epithelial cells. Hydrodynamic pressure drops across the vascular network was considered a marker of scaffold integrity. Furthermore, it was used in addition to histological data to monitor indirectly matrix degradation over time. The bioreactor was also designed to obtain a sterile in situ collection of the perfusate, enabling assessment of cell function during culturing. 63 This study provides a valuable tool to improve long-term bioreactor culture and highlights that culture is unquestionably a complex and delicate stage in the development of a bioengineered kidney. In addition, the majority of studies performed in the field focus on aspects other than construction of an optimal bioreactor. However, precisely because the study has a technical footprint and includes specific physical markers that correlate with scaffold features, its outputs are difficult to translate and are limited to rodent models. Of course, the use of human cells to repopulate the rat scaffold was aimed to investigate the interplay between ECM constituents and human cells in a pilot system. However, this modified version tailored to human-sized kidneys and the related testing panel should be appropriately assayed to maximize the methodology.
Understanding cell–matrix interactions
As reported above, several studies concerning decellularization and basic ECM characterization resulted in significant advances. However, the mechanisms by which ECM influences cellular response during renal ECM scaffold repopulation remain relatively unknown. In an interesting study on decellularized rat kidneys seeded with mouse pluripotent precursor cells, Ross et al. reported that, after 14 days in culture, cells tended to replace the original matrix and remodel the basement membrane of the scaffold leading to a kind of “murinization.” The finding that host–isolated precursor cells are able to initiate scaffold remodeling when seeded into donor matrix suggests new and exciting strategies for xenotransplantation. 64 Indeed, a gradual replacement of the scaffold's antigens with patient-derived components may potentially reduce the immunogenicity of the original matrix. Nevertheless, a longer term study would be required to investigate to what extent the donor's matrix is replaced. Regardless, these results remain a valuable proof of concept, necessary to begin to think about replacing rodent models with more clinically relevant ones to better understand what occurs in humans. It is in this perspective that Orlando et al. created acellular scaffolds from porcine and human kidneys deemed unsuitable for transplantation. In these studies, pig kidneys were completely decellularized after 36 h of arterial perfusion with detergents, while human organs required both antegrade and retrograde perfusion for 48 h.65,66 The longer perfusion time reported for human kidneys was probably due to fibrosis that often occurs in discarded organs.
Concerning biocompatibility, no deleterious effects were observed by seeding MS1 murine ECs onto porcine scaffold biopsies. Once implanted in pigs, the acellular porcine scaffold sustained physiological blood pressure for 2 weeks. Although nephron integrity was preserved in the explanted constructs, some inflammatory cells infiltrated the glomeruli and, more so, the pericapsular area. Furthermore, thrombi and clots occluded the entire vascular network, likely due to the lack of endothelium and the resulting exposure of the subendothelial basal membrane. 65
More recently, Peloso et al. provided for the first time an accurate characterization of both morphology and function of the renal vascular tree, including glomerular microvasculature, of a human renal ECM scaffold (hrECMs). 59 Resin casting techniques accurately displayed morphological features, while a high degree of compliance and resilience within the scaffold vessels was demonstrated by using a pulse wave. Lower glomerular size was found in hrECMs in comparison to the native kidney, probably because the scaffold vasculature lacked ECs that physiologically encourage regeneration of endothelium. In addition, the hrECMs were able to retain essential growth factors involved in the regulation of glomerular endothelial function and angiogenesis resulting in a favorable milieu for regeneration. This latter feature is of particular interest in view of the suboptimal conditions of discarded kidneys. Further experiments using seeded scaffolds will be crucial to understanding the impact of the preserved vascular tree and improving organ decellularization and scaffold repopulation. The same applies to the ability of the retained growth factors to control cell behavior. Work by Petrosyan et al. reported for the first time how the decellularized ECM is able to modulate the stem cell secretome profile. 67
In this study, human amniotic stem cells (hAFSC) were seeded on hrECM scaffold samples from discarded kidneys. Histology and immunohistochemistry revealed that matrix cellularization and cell viability peaked at day 14 gradually decreasing over time (at 28 and 35 days). Improved culture conditions, including addition of growth factors likely improved cell viability. Alternatively, ultrastructural analysis performed after 28 days of culture showed that cells were active and displayed a site-specific morphology at the glomerular, tubular, endothelial, and interstitial level. In addition, hAFSC produced essential mediators involved in matrix remodeling, inflammation, and angiogenesis, particularly during the first week of culture as revealed by secretome analysis. On the basis of these results, the biosystem composed of hAFSC and hrECM samples displays huge potential as an in vitro platform to study cell–matrix interactions.
A similar approach was proposed by Nakayama et al. who performed a series of studies in a nonhuman primate model. The authors first adapted the decellularization protocol to Rhesus Monkey kidney and characterized the resulting ECM scaffold. 68 Next, they explored the impact of age on both cell and scaffold performance and how the relationship between these two variables influenced cell migration. 69 Rhesus Monkey Kidney explants or fetal renal fractions were layered onto sections from acellular renal ECM from the same species. The experiments, which included fetal, juvenile, and adult cells and scaffolds, showed the highest degree of migration when using cells from younger donors, independent of the age of the scaffold donor. In a further study, hESCs were seeded onto an ECM scaffold from Rhesus Monkey kidney sections to test the ability of the matrix to guide differentiation of human cells. The authors performed an accurate analysis of the ECM components to assess the aptitude of the scaffold to be integrated into the host without inducing rejection. Proteomic analysis of the decellularized matrix showed the presence of growth factors and antimicrobial proteins, as well as complement fractions and stress-related and proapoptotic proteins. During 8 days in culture within the scaffold, hESCs expressed kidney-specific genes compared to baseline values and also exhibited a tubular-like organization. Collectively, these data have a translational value related to future human use, however, the use of sections and explants instead of the entire organ and isolated cells leads to significant limitations in data translation. In addition, decellularization of Rhesus Monkeys kidney sections required 7–14 days, which is considered a long time compared to the same procedure applied to the whole human kidney.66,69,70 Furthermore, data validation on entire kidneys would be of great interest and must be recognized that performing these experiments in nonhuman primates is complicated by the regulatory aspects related to the use of these species in research.
Improving scaffold repopulation
Scaffold recellularization is currently a major challenge toward obtaining a functional bioengineered kidney due to the complex architecture of the kidney vascular and tubular systems. Thus, the development of a functional tissue is strongly influenced by efficient cell delivery and site-specific engraftment, differentiation, and function. Adequate cell delivery involves a combination of multiple factors, including cell type, the route of seeding, modulation of specific infusion/injection parameters (pressure value, flow rate, and conditions), and the settings during bioreactor culture. Commonly, cell seeding is performed by perfusion of suspended cells through the renal artery,52,61,64 either enhanced or not by retrograde infusion through the ureter. 51 To date, these procedures have led to poor results. Alternative strategies have been tested in the past few years with interesting readouts.
Abolbashari et al. described a cell seeding method based on injection of primary renal cells directly into the cortex of porcine kidney scaffolds instead of infusion through the vasculature or the ureter as typically performed. Cells isolated from pig kidneys were expanded and characterized and the seeded scaffolds were cultured into a bioreactor. Histology revealed cell organization into renal tubular structures between culture days 7 and 21. Detailed immunohistochemical analysis of the repopulated scaffold showed that the majority of these structures resembled the proximal tubule and the descending limb of the Henle loop, as well as displaying a few distal tubules and collecting ducts. Functional assessment showed the activity of specific hydrolases involved in amino acid transport across the membranes of the PTCs similar to that observed in native kidneys. Conversely, erythropoietin production corresponded to almost 10% of the physiological blood value. These results have some relevance from a clinical perspective as they indicate concrete alternatives to address the issues of cell sources and seeding routes in human-sized organs. On the basis of these findings, further studies are justified and needed to optimize cell expansion protocols to concretely address the limitation of donor shortage. Furthermore, a precise characterization after isolation would be relevant in trying to assemble the composite array of renal cells, including ECs and podocytes, in adequate percentages that exist in native kidneys. In addition, it would be important to further refine the number of injection sites to understand whether or not seeding by injection would enable repopulation of the entire kidney cortex.
Ko et al. presented a proof-of-concept study about an intriguing double strategy approach for efficient repopulation. 57 MS1 mouse ECs were seeded into a porcine acellular scaffold, whose vascular matrix had previously been conjugated with an antibody (Ab) against CD31, a surface protein normally found on ECs. In addition, seeding was made by both static and ramping the cell infusion into the scaffold vasculature. The “expendient” of Ab conjugation was meant to enhance EC attachment and retention during exposure to blood flow. The reendothelialized construct was implanted into a pig kidney, harvested after 4 h, and analyzed. Improved vascular patency was shown in the treated scaffold compared to control, highlighting the potential of this strategy in establishing a functional vascular network onto the ECM scaffold. Validation of these findings in more extensive experiments aimed to assess how long the construct is able to support the physiological blood flow would be worthwhile. The function of a kidney repopulated with both endothelial and epithelial cells using an improved seeding protocol was assayed in vivo by Song et al. in a rat model. 55 After decellularization, the scaffold was perfused with ECs from human umbilical vein and epithelial cells from rat neonatal kidney through the renal artery and ureter, respectively. To accomplish this, a 40 mmHg negative pressure was maintained outside the kidney during cell infusion to create a transrenal pressure gradient for improved cell delivery. The kidney was then maintained in a perfusion bioreactor for up to 12 days to encourage tissue maturation in a biomimetic manner. In vitro functional analysis displayed relative oliguria and higher vascular resistance of the bioengineered organ compared to cadaveric controls. Creatinine clearance was increased 10% and 23% compared to controls under an arterial perfusion pressure of 80 and 120 mmHg, respectively. Furthermore, albumin retention and glucose reabsorption in comparison to physiologic values were around 90% in cadaveric control kidneys, decreasing to about 47% in bioengineered ones, probably because of the immaturity of neonatal epithelial cells.
It must be considered that a quantity of fluids and creatinine is naturally filtered by both the glomeruli and tubuli of the acellular kidney and is unrelated to specific filtration/reabsorption functionality. 71 After orthotopic transplantation in immunodeficient rats, the bioengineered construct revealed the absence of adverse effects such as thrombi formation or bleeding. In contrast, compared to native kidneys, those that were bioengineered showed lower urine production and creatinine clearance in accordance with in vitro findings. This study provides the first preliminary data set describing the production of “basic” urine after transplantation, however, the duration of the in vivo test was not reported. Furthermore, the proposed seeding strategy should be reproduced in human or porcine scaffolds using more suitable cell lines.
Challenges and future directions
Ideally, the use of recellularized ECM in clinical practice may include various options. First, there is autotransplantation and in this case the scaffold would be derived from the patient's own kidney. After harvesting the organ, it will be decellularized, repopulated, cultured into a bioreactor, and implanted back into the patient without requiring immunosuppression. Throughout the process, the renal function of the patient would be aided by supportive therapies and, to a limited extent, by the contralateral kidney. In addition, once reimplanted, the bioengineered organ will be expected to interact with the host giving rise to an “in-host” maturation period. 72 However, this hypothesis is rather unrealistic due to the severity of kidney injury in patients with ESRD. In contrast, the use of discarded human kidneys destined to be repopulated with autologous or heterologous cells may represent a feasible choice.56,59,66,67,73 Unfortunately, although, this option will always be limited by donor shortage. Therefore, a further intriguing strategy is one designed as a semixenotransplantation.74,75 In this study, the implant of porcine ECM scaffolds that are recellularized with patient-derived cells brings a number of benefits. First, these scaffolds will be expected to be almost “antigen free” and thus patients would not need immunosuppression, and the risk of PERV transmission would be highly decreased. 76 In addition, organ supply would be almost unlimited and procedures reproducible.
Conclusions
Crucial advances in the field of RRT have been made over the past decade, however, the majority of research outputs are far from providing a self-standing product able to recapitulate whole kidney function without being integrated into a circuit or an undefined device.37,77–79 In contrast, the implantable RAD and the bioengineered kidney described in this review are both potentially perfect candidates to surmount the huge challenge of having patients with ESRD become free from dialysis and the transplant waiting lists, and also to enable autonomy. Furthermore, they are both ideally suited to be prepared with autologous cells and thus to potentially wean patients from immunosuppressive therapy and the associated heavy side effects. However, common to both technologies are the issues related to the introduction of live cells into a “device,” either iRAD or decellularized ECM scaffolds, which influences the pace of technological development and human testing.
Regarding economic aspects, the only certainty is that these two strategies will offer tremendous cost-saving advantages compared to the healthcare expenses related to patients with ESRD. Conversely, it is quite difficult at this stage to quantify the manufacturing costs of these products. The cost-effectiveness coupled with manufacturing, scale-up, and preparation time is still under development. In addition, data related to in vivo performance of both candidate strategies have to be corroborated by further studies. In the case of iRAD, the individual components, but not the entire device, have been tested in preclinical models, while in bioengineered kidneys, animal studies reveal a partial function of the transplanted construct, but no information regarding long-term function after transplantation. It is hard to predict which of these two promising kidney substitutes will be available first to be tested in a clinical trial. It is reported that iRAD may be ready in 2017, however, several crucial hurdles still have to be overcome. 13 Collectively, the results reported so far are astonishing and both approaches reviewed hold the potential to improve, in the near future, the quality of life for patients with ESRD.
Footnotes
Disclosure Statement
No competing financial interests exist.