
Abstract
The growing multidisciplinary field of tissue engineering aims at predictably regenerating, enhancing, or replacing damaged or missing tissues for a variety of conditions caused by trauma, disease, and old age. One area of research that has gained tremendous awareness in recent years is that of platelet-rich fibrin (PRF), which has been utilized across a wide variety of medical fields for the regeneration of soft tissues. This systematic review gathered all the currently available in vitro, in vivo, and clinical literature utilizing PRF for soft tissue regeneration, augmentation, and/or wound healing. In total, 164 publications met the original search criteria, with a total of 48 publications meeting inclusion criteria (kappa score = 94%). These studies were divided into 7 in vitro, 11 in vivo, and 31 clinical studies. In summary, 6 out of 7 (85.7%) and 11 out of 11 (100%) of the in vitro and in vivo studies, respectively, demonstrated a statistically significant advantage for combining PRF to their regenerative therapies. Out of the remaining 31 clinical studies, a total of 8 reported the effects of PRF in a randomized clinical trial, with 5 additional studies (13 total) reporting appropriate controls. In those clinical studies, 9 out of the 13 studies (69.2%) demonstrated a statistically relevant positive outcome for the primary endpoints measured. In total, 18 studies (58% of clinical studies) reported positive wound-healing events associated with the use of PRF, despite using controls. Furthermore, 27 of the 31 clinical studies (87%) supported the use of PRF for soft tissue regeneration and wound healing for a variety of procedures in medicine and dentistry. In conclusion, the results from the present systematic review highlight the positive effects of PRF on wound healing after regenerative therapy for the management of various soft tissue defects found in medicine and dentistry.
Introduction
T
Wound healing, which is defined as the natural restorative response to tissue injury, involves a cascade of complex, orderly, and elaborate events involving many cell types guided by the release of soluble mediators and signals that are capable of influencing the homing of circulating cells to damaged tissues. 6 Typically, wound-healing events are divided into four overlapping phases, including hemostasis, inflammation, proliferation, and remodeling.7–9 Platelets have been shown to be important cells regulating the hemostasis phase through vascular obliteration and facilitating fibrin clot formation. 6 Although debate has been ongoing as to whether platelets should be regarded as cell fragments or whole cells, 10 it is well known that they are responsible for the activation and release of important biomolecules, including platelet-specific proteins, growth factors including platelet-derived growth factor (PDGF), coagulation factors, adhesion molecules, cytokines/chemokines, and angiogenic factors that are capable of stimulating the proliferation and activation of cells involved in wound healing, including fibroblasts, neutrophils, macrophages, and mesenchymal stem cells (MSCs). 11 For these reasons, the use of platelet concentrates has been utilized in modern medicine for more than four decades due to their hypothesized impact on tissue regeneration by facilitating angiogenesis and various additional phases during wound healing, including cell recruitment, proliferation, remodeling, and differentiation. Later, we describe how tissue-engineering constructs have utilized various platelet concentrates to speed wound healing of either soft or hard tissues.
Platelet concentrates: from platelet-rich plasma to platelet-rich fibrin
Autologous platelet-rich plasma (PRP) was first developed in the early 1970s and was made popular in the 1980s.12,13 The first generation of PRP was introduced by mixing collected blood with thrombin and excess calcium, resulting in activated platelets trapped within a fibrin network. Since then, different platelet preparation protocols are now available and traditionally isolated by a dual-speed centrifugation process. The first spin separates red blood cells from plasma and buffy coat. Thereafter, the platelet plug is typically separated from the platelet-poor plasma in a second spin cycle generating PRP, a platelet concentrate with up to 6–8 times the concentration of growth factors when compared with whole blood. 14 These platelets have been shown to secrete high levels of bioactive substances that slowly diffuse to the surrounding micro-environment facilitating tissue regeneration.15–19 Much advancement has since been made in the medical field by various groups, who demonstrated that PRP could further enhance surgical wound healing of either soft or hard tissues.15,20,21 Despite its widespread use, one of the reported drawbacks was the use of anti-coagulation factors delaying normal wound-healing events.
Due to these reported limitations, further research was focused on developing a second-generation platelet concentrate without utilizing anti-coagulation factors. As such, a platelet concentrate lacking coagulation factors, later termed platelet-rich fibrin (PRF), was developed due to its anticipated properties in tissue regeneration and wound healing.22–25 PRF (also termed leukocyte-PRF), in addition, contains more white blood cells (WBCs), necessary cells that are important during the wound-healing process (Fig. 2).17,26–30 Furthermore, since WBCs, including neutrophils and macrophages, are one of the first cell types found in wounded sites, their role also includes to phagocytize debris, microbes, and necrotic tissue, thereby preventing infection. Macrophages are also key cells derived from the myeloid lineage and are considered one of the key cells implicated in growth factor secretion during wound healing, including transforming growth factor beta (TGF-beta), PDGF, and vascular endothelial growth factor (VEGF) (Fig. 2). These cells, together with neutrophils and platelets, are key players in wound healing and in combination with their secreted growth factors/cytokines are capable of facilitating tissue regeneration, new blood vessel formation (angiogenesis), and prevention of infection.22–25,28 To date, numerous studies have investigated the regenerative potential of PRF in various medical situations. The aim of this article was to systematically characterize the potential for PRF to influence soft tissue wound healing. A systematic search was carried out, including all in vitro, in vivo, and clinical studies performed on PRF to date dealing with soft tissue regeneration, wound healing, and/or angiogenesis after treatment with PRF.
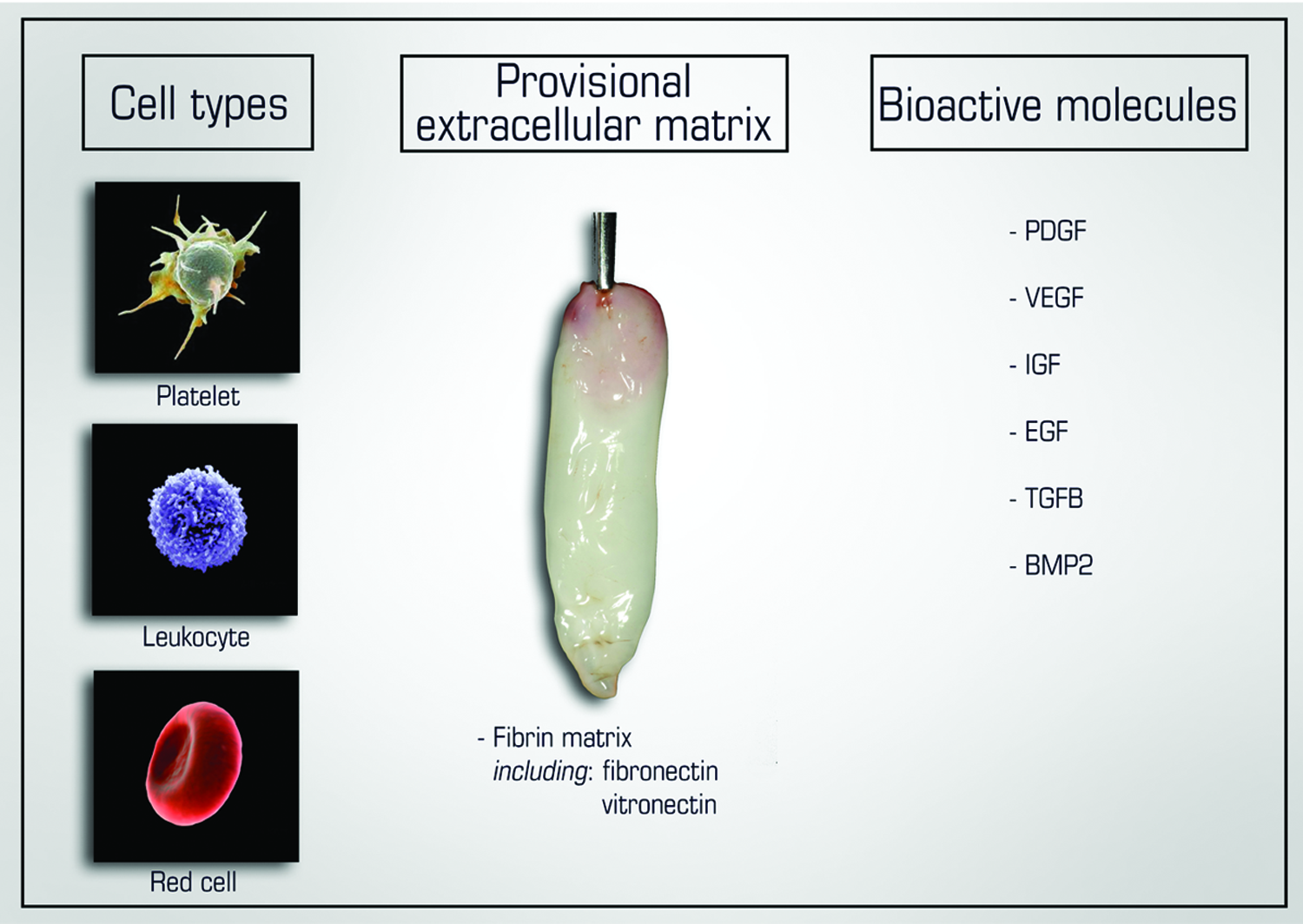
Representative diagram of the cell types, extracellular matrix components, and bioactive molecules found in PRF. PRF, platelet-rich fibrin. Color images available online at www.liebertpub.com/teb
Methods
Development of a protocol
A protocol including all aspects of a systematic review methodology was developed before commencing the review. This included a definition of the focused question; a defined search strategy; study inclusion criteria; determination of outcome measures; screening methods, data extraction, and analysis; and data synthesis.
Defining the focused question
The following focused question was defined: ‘‘Does platelet rich fibrin (PRF) affect/induce soft tissue regeneration and/or soft tissue wound healing?’’
Search strategy
Using the MEDLINE database, the literature was searched for articles published up to and including April 7th, 2016 (Figure 1). Combinations of several search terms were applied to identify appropriate studies (Table 1). Reference lists of review articles and of the included articles in the present review were screened.
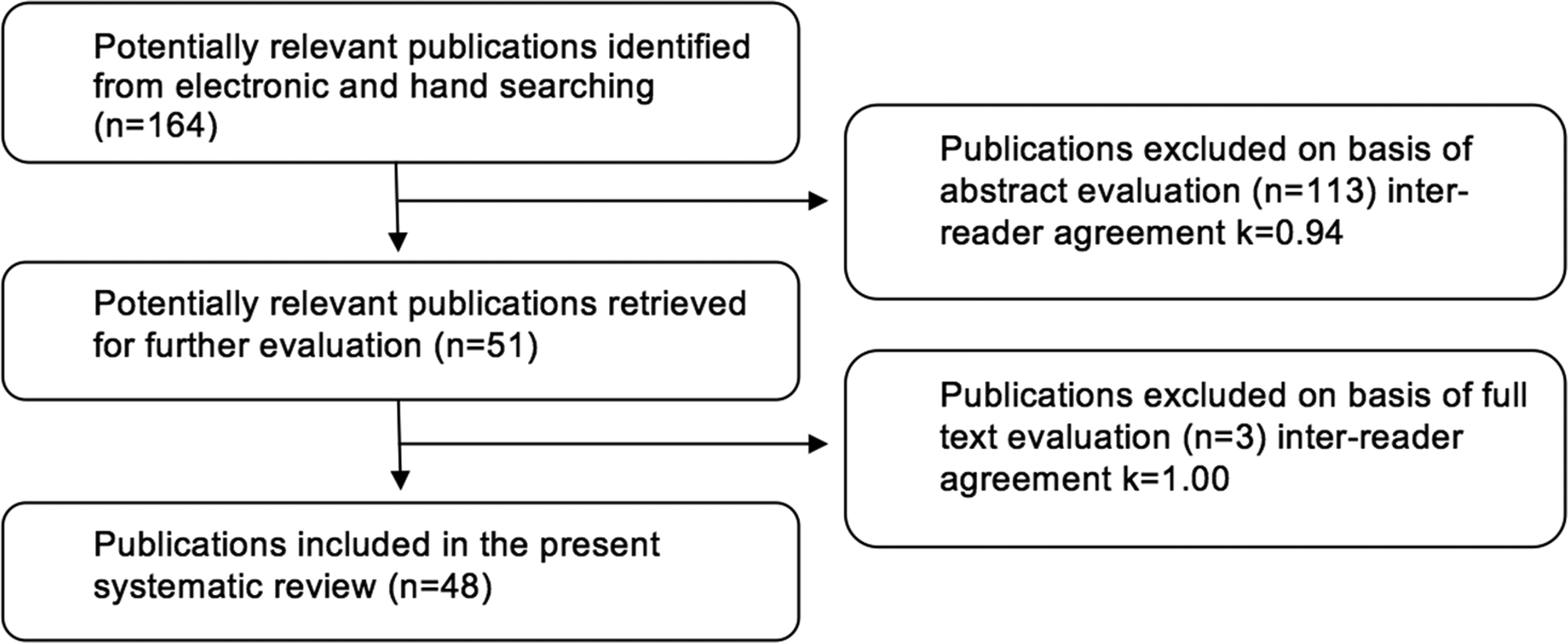
Flow chart of the screened relevant publications.
Criteria for study selection and inclusion
Study selection considered only articles published in English, describing in vitro, in vivo, and human clinical studies evaluating the effect of PRF on soft tissue wound healing. All in vitro studies were included on fibroblasts, endothelial cells, keratinocytes, and/or periodontal ligament fibroblasts. All in vivo data specifically characterizing the effects of PRF on soft tissue wound healing were included. All human studies reporting the effects of PRF were also included. Human studies were not limited to randomized clinical trials.
Outcome measure determination
The primary outcome of interest was to determine the effect in percentage increases that PRF is capable of inducing soft tissue regeneration and wound-healing events. The outcome measures were separated into (1) in vitro studies, (2) animal studies, and (3) clinical studies. Since large variability in the outcomes measured was performed by the various groups working across several fields of medicine, a meta-analysis was not considered. Outcomes were summarized in Tables 2–4 for the various in vitro, in vivo, and clinical studies according to the specific effect of PRF on soft tissue wound healing.
PRF, platelet-rich fibrin; PDGF, platelet-derived growth factor; A-PRF, advanced-PRF; PRGF, plasma rich in growth factors.
TGF-β, transforming growth factor beta; VEGF, vascular endothelial growth factor; MSC, mesenchymal stem cell; LV, left ventricular; FTSG, full-thickness skin graft; STSG, split-thickness skin graft.
“Bold” signifies a total of eight studies that have reported the effects of PRF in a randomized clinical trial.
VLU, venous leg ulcers; CTG, connective tissue graft; DFU, diabetic foot ulcers; OFD, open-flap debridement; PAOO, periodontally accelerated osteogenic orthodontics; PRP, platelet-rich plasma.
Screening method
Titles and abstracts of the selected studies were independently screened by two reviewers (R.J.M. and M.F.-K.) on April 7th, 2016. The screening was based on the question: “What effect does platelet rich fibrin (PRF) have on soft tissue regeneration and/or wound healing?” Full text articles were obtained if the response to the screening question was “yes” or “uncertain”. The level of agreement between reviewers was determined by kappa scores according to company software instructions (GraphPad Software, Inc., La Jolla, CA, http://graphpad.com/quickcalcs/kappa1.cfm). Disagreement regarding inclusion was resolved by discussion between authors. For necessary missing data, the authors of the studies were contacted. Articles referring strictly to use in tendons, and orthopedic/bone uses were excluded if soft tissue wound-healing events were not investigated/discussed. Furthermore, review articles and clinical cases with no measurable endpoint were excluded.
Data extraction and analysis
The following data were extracted: general characteristics (authors, year of publication), PRF centrifugation characteristics/protocols, evaluation characteristics (amount of PRF utilized, volume, period, outcome measures), methodological characteristics (study design, methodological quality), and conclusions. Because of the heterogeneity of the included studies (study design, in vitro vs. animal vs. clinical studies, investigated parameters, materials used, evaluation methods, outcome measures, observation periods), no mean differences could be calculated, and consequently, no quantitative data synthesis and meta-analysis could be performed. Instead, the data are reported in a systematic fashion characterizing all available literature to date. Therefore, data were extracted from the reviewed articles and summarized in separate tables based on the various in vitro, in vivo, and clinical studies and outcome measures employed.
Results
In vitro studies evaluating the effects of PRF on cell behavior
The evaluation of PRF on the cells found during soft tissue regeneration and/or wound healing has been investigated in seven in vitro studies to date (Table 2). The effects of PRF have been investigated on (1) cell behavior of fibroblasts involved in soft tissue wound healing, (2) endothelial cells, and (3) growth factor release from various PRF formulations.
Effects of PRF on fibroblast cell behavior in vitro
In 2008, Lundquist was one of the first to evaluate the effects of PRF on human dermal fibroblasts. 31 It was found that the proliferative effect of PRF on dermal fibroblasts was significantly greater than fibrin sealant and recombinant PDGF-BB. Furthermore, PRF induced rapid release of collagen 1 and sustained release and protection against proteolytic degradation of endogenous fibrogenic factors that are important for wound healing. 31 In a second in vitro study conducted by Lundquist et al. in 2013, PRF induced the mitogenic and migratory effect on cultured human dermal fibroblasts and they further showed that fibrocytes (a cell type important for acute wound healing) could be grown from within PRF patches, further favoring wound healing and soft tissue regeneration. 32 Thereafter, Clipet et al. found that PRF induced fibroblast and keratinocyte cell survival and proliferation. 33 In 2015, Vahabi et al. also confirmed that PRF induced gingival fibroblast proliferation at 24 h; however, they found that gingival fibroblast proliferation was significantly higher in the plasma rich in the growth factors group at 48 and 72 h. 34 In summary, it may, therefore, be concluded that PRF is able to induce the proliferation of dermal fibroblasts, gingival fibroblasts, and keratinocytes, as well as it participates in their production of extracellular matrix collagen 1 synthesis.
Effects of PRF on endothelial cell behavior
In the only in vitro report investigating the effects of PRF on angiogenesis in vitro, Roy et al. investigated the effects of PRF on endothelial cells. It was found that PRF induced endothelial cell mitogenesis via the extracellular signal-regulated protein kinase activation pathway. 35 A slow and steady release of growth factors from their PRF matrix was observed to be releasing VEGF, a known growth factor responsible for endothelial mitogenic response. These authors provide some evidence of probable mechanisms of action of PRF matrix in healing of chronic wound ulcers. 35
Effect of PRF on growth factor release
It has long been observed that PRF releases an array of growth factors to the surrounding micro-environment that contributes to soft tissue wound healing. 24 Interestingly, in 2014, a new protocol for PRF was introduced (termed Advanced-PRF or A-PRF) whereby centrifugal forces were decreased and total spin times were increased. 36 By decreasing the rpm while increasing the centrifugation time in the A-PRF group, an enhanced presence of neutrophilic granulocytes in the distal part of the clot was found to be contributing to monocyte differentiation to macrophages, 36 a cell responsible for inducing new bone formation.37,38 Therefore, this article concludes with the importance of centrifugation g-force on growth factor to the surrounding environment, which may be optimized by centrifugation time and speeds.
In a study investigating growth factors released from various PRF components, Kobayashi et al. quantified by enzyme-linked immunosorbent assay growth factors including PDGF-AA, PDGF-AB, PDGF-BB, TGF-beta, VEGF, and insulin-like growth factor (IGF). 39 Each of these growth factors has a specific role in tissue regeneration.
Platelet-derived growth factor
PDGFs are essential regulators for the migration, proliferation, and survival of mesenchymal cell lineages. 40 According to the distribution of mesenchymal-cell specific receptors, they are able to induce stimulation in mesenchymal cells. 40 For this reason, PDGFs play a critical role in physiologic wound healing and have been FDA approved for the regeneration of various defects in medicine and dentistry.41,42 Interestingly, PDGF is naturally found in PRF clots and is produced over time by leukocytes; therefore, it is considered one of the important released bioactive growth factors secreted over time from PRF.
Transforming growth factor-beta
TGF-beta is a vast superfamily of more than 30 members known as fibrosis agents, with TGF-beta1 being the most well described in the literature.43,44 It is a known stimulator of proliferation of various mesenchymal cell types, including osteoblasts, 45 constituting the most powerful fibrosis agent among all cytokines. 44 It plays a prominent role in matrix molecule synthesis such as collagen1 and fibronectin, whether by osteoblasts or fibroblasts. Although its regulatory mechanisms are particularly complex, TGF-beta1 plays an active role in wound healing.43,44
Vascular endothelial growth factor
VEGF is the most potent growth factor responsible for angiogenesis of tissues. 46 It has potent effects on tissue remodeling and the incorporation of VEGF alone into various bone biomaterials has demonstrated increases in new bone formation, thereby pointing to the fast and potent effects of VEGF.46,47
Insulin-like growth factor
IGF is a positive regulator of proliferation and differentiation for most mesenchymal cell types, which also act as cell-protective agents. 48 Although these cytokines are cell proliferative mediators, they also constitute the major axis of programmed cell death (apoptosis) regulation, by inducing survival signals protecting cells from many apoptotic stimuli. 48
Although many known growth factors are present within PRF clots, it remains interesting to note that further molecules are being investigated from PRF for their various roles in tissue wound healing. For example, Bayer et al. investigated for the first time the properties that are contained within PRF that may contribute to its anti-inflammatory/anti-microbial activities. 49 It was discovered that in human keratinocytes, PRF induced the expression of hBD-2, an anti-microbial agent necessary in the treatment of chronic and infected wounds. 49 Further in vitro research is necessary to characterize the potential anti-inflammatory/anti-microbial activity in PRF.
Conclusions from in vitro research
In total, six of seven (85.6%) reported studies demonstrate a positive effect of PRF on soft tissue cell behavior in vitro. In all studies, appropriate controls were utilized. It was found that PRF was able to increase cell proliferation in a number of cells implicated in soft tissue repair, induced the mitogenic activity of endothelial cells important for angiogenesis, released an array of growth factors to the surrounding micro-environment, and possessed properties leading to its anti-inflammatory and anti-microbial activity.
In vivo studies evaluating the effects of PRF on soft tissue regeneration and/or wound healing
In total, 11 studies have evaluated the effects of PRF on soft tissue wound healing and regeneration (Table 3). These studies may be classified under the following four subheadings, including the effects of PRF on (1) wound healing and angiogenesis, (2) plastic and reconstructive purposes in the ear's auricular, (3) urethral repair, and (4) myocardial ischemia and ventricular remodeling.
Effects of PRF on wound healing and angiogenesis in vivo
The effects of PRF have most notably been investigated on soft tissue wound healing and angiogenesis in various animal models. In the first study, Roy et al. evaluated PRF after 14 days in a porcine ischemic excision wound model, where 8-mm skin biopsies were created and filled with PRF versus control. 35 It was found that PRF significantly improved angiogenesis in chronic wounds and collagen matrix deposition (Fig. 3). 35 Suzuki et al. further showed that PRF induced faster wound healing and angiogenesis in the dorsal tissues of rats after 14 days. 50 In another subcutaneous implantation model performed in mice, PRF readily integrated with surrounding tissues and was partially replaced with collagen fibers 2 weeks after implantation. 51 Furthermore, Horii et al. concluded that PRF significantly spread soft tissue healing of oral mucosititis in rats after a 14 day healing period (Fig. 4). 52 Tunali et al. found that PRF centrifuged in titanium vials improved soft tissue wound healing in a mucoperiosteal flap defect model in rabbits 30 days after implantation. 53 In a model designed to regenerate the parotid gland after their irradiation in minipigs, both adipose-derived stem cells and PRF significantly sped the repair of defects in maxillofacial soft tissue in irradiated minipigs, and their combined use was more effective after a 6-month healing period. 54 In 2014, it was found that PRF increased type 1 collagen formation in full- and split-thickness flaps and improved skin graft take in a skin graft model performed in porcine animals. 55 The totality of these studies show convincingly that PRF is able to increase soft tissue wound healing in various animal models, and reports document that this is primarily due to the increase in angiogenesis to defect sites.

Treatment of porcine ischemic wound with PRFM. Representative digital images of excisional wounds treated or not with PRFM on days 0 and 4 postwounding. Adapted with permission from Roy et al. 35 PRFM, PRF matrix. Color images available online at www.liebertpub.com/teb
Macroscopic aspects of the cheek pouches of hamsters injected with 5-fluorouracil. The control group
Effect of PRF for plastic and reconstructive purposes in the ear's auricular in vivo
In one study, the effect of PRF has been combined with adipose tissue for fat pad grafting in the ear's auricular. Liu et al. found that after a 24 week healing period, fat grafting with PRF into the ear's auricula could be enhanced with PRF as a therapeutic adjuvant to these procedures. 56 Histological examinations showed that the implanted adipose granules were well engrafted in the group containing PRF, demonstrating a higher microvessel density 4 weeks postimplantation (p < 0.01). 56 At 24 weeks postimplantation, the resorption rates of implanted tissue in each group were also significantly different, with PRF demonstrating the least resorption after the study endpoints (p < 0.01). 56 The results from this study conclude that PRF can effectively be combined with adipose tissue as a therapeutic adjuvant offering a clinically translatable strategy for soft tissue augmentation and reconstruction of the ear.
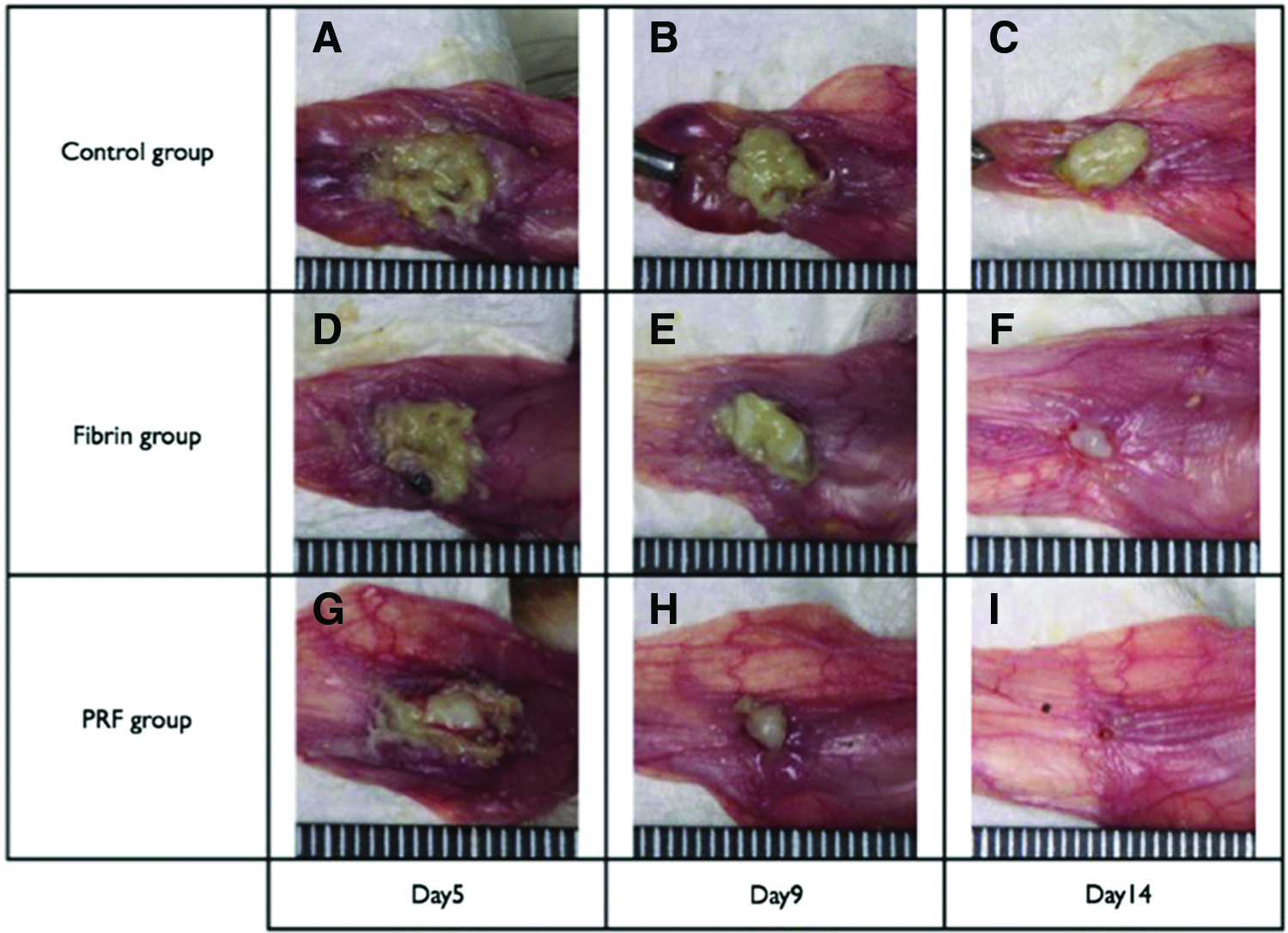
Effects of PRF on urethral repair in vivo
The effect of PRF was investigated on urethral repair in one animal study. Soyer et al. found in a 5 mm penile erethral defect model in 18 Wistar albino rats that treatment with PRF significantly increased TGF-beta and VEGF growth factor release after 24 h. 57 These authors conclude that the use of PRF after urethral repair increases TGF-β-receptor and VEGF expression in urethral tissue and may be considered an alternative measure to improve the success of urethral repair.
Effects of PRF on the repair of myocardial ischemia and ventricular remodeling in vivo
The effect of PRF on the repair of heart-related injuries has been investigated in two studies. Sun et al. first demonstrated that the combination of PRF with adipose derived MSCs improved the preservation of left ventricular (LV) function and attenuated LV remodeling in a rat model that induced regional myocardial ischemia by left coronary artery ligation. 58 Furthermore, in 2015, adipose-derived MSCs were embedded in PRF scaffolds to investigate its effect on angiogenesis in heart tissues. 59 It was found that the combination of PRF with adipose cells promoted angiogenesis, preserved heart function, and reduced LV remodeling in rat acute myocardial infarction when compared with controls (Fig. 5). 59 It may, therefore, be concluded that in both studies, the additional use of PRF led to improved heart function and angiogenesis; however, both research groups point to the fact that further study is necessary before these findings may be translated to clinical use.
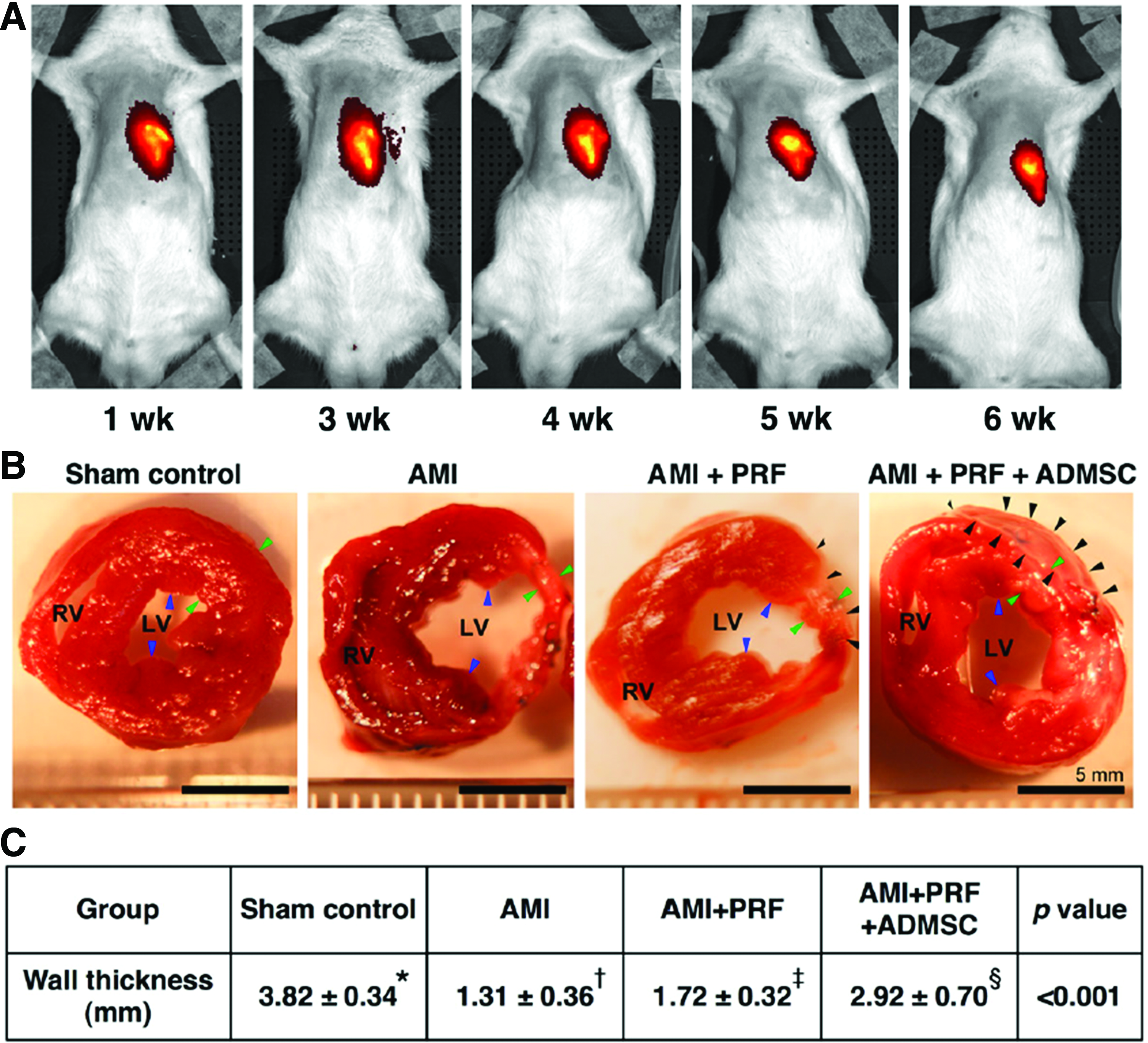
Illustration of IVIS study and anatomical and pathological findings on day 42 after AMI induction (n = 8).
Conclusions from in vivo research
In total, 11 studies found that PRF significantly improved soft tissue regeneration, wound healing, and/or angiogenesis in various animal models investigated. In all studies, appropriate controls were utilized. It was found that PRF was able to promote soft tissue wound healing in various wound-healing models by promoting local angiogenesis to defect sites, could be combined with adipose tissue/cells to further improve regeneration, could successfully be utilized for urethral repair, and led to improvements in myocardial ischemia and ventricular remodeling.
Clinical studies evaluating the effects of PRF on soft tissue regeneration and/or wound healing
In total, 31 studies investigated the effects of PRF on soft tissue wound healing/regeneration in various clinical scenarios. Table 4 presents a summary of each of the outcomes found in each of the clinical studies, with italicization denoting randomized clinical studies with appropriate controls. The use of PRF has been utilized for 20 different clinical procedures; 7 of which come from the oral and maxillofacial region (Table 4). In the dental field, the most commonly utilized use of PRF was for the treatment of extraction sockets,60–63 gingival recessions,64–66 and palatal wound closure67–69 with PRF being additionally utilized for the repair of potentially malignant lesions, 70 regeneration of periodontal defects, 71 hyperplastic gingival tissues, 72 and in addition to periodontally accelerated osteogenic orthodontics. 73 In other medical procedures, the use of PRF has been mostly combined for the successful management of hard-to-heal leg ulcers, including diabetic foot ulcers, venous leg ulcers, and chronic leg ulcers.74–78 Furthermore, PRF has been investigated for the management of hand ulcers, 79 facial soft tissue defects, 80 laparoscopic cholecystectomy, 81 in plastic surgery for the treatment of deep nasolabial folds, volume-depleted midface regions, facial defects, superficial rhytids and acne scars, 82 induction of dermal collagenesis, 83 vaginal prolapse repair, 84 urethracutaneous fistula repair,85,86 during lipostructure surgical procedures, 87 chronic rotator cuff tears, 88 and acute traumatic ear drum perforations. 89 A total of eight studies have reported the effects of PRF in a randomized clinical trial (Table 4, bolded). Five nonrandomized studies reported appropriately selected controls, whereas 18 studies (58% of the total listed clinical studies) reported no controls in their investigation and instead focused on the technical utilization/aspects of combining PRF during their various medical procedures. In total, 9 of the 13 studies utilizing appropriate controls reported a significant positive influence combining PRF to their surgical protocols during soft tissue wound healing (Table 4). In total, 27 of the 31 studies (87%) reported having beneficial effects for the utilization of PRF during soft tissue regeneration and/or soft tissue wound healing and angiogenesis in human applications. Noteworthy, 18 of 31 studies (58%) did not use appropriate controls in their clinical studies.
Discussion and Future Perspectives
Platelet concentrates, including PRP and PRF, have been used for regenerative procedures in various fields of medicine, including dentistry, reconstructive surgery, plastic surgery, and dermatology, to deliver supernatural concentrations of autologous growth factors directly to host tissues. These growth factors have been shown to be chemotactic for various cell types, including monocytes, fibroblasts, endothelial cells, stem cells, and fibroblasts, creating tissue micro-environments and directly influencing the proliferation and differentiation of progenitor cells. 90 Furthermore, platelet concentrates are safe, reliable, and cost-effective means to accelerate tissue healing and for improving the efficiency of tissue repair after injury.
In the present study, we investigated specifically the regenerative potential of soft tissue after use of PRF. To date, no systematic review has characterized the regenerative potential of PRF specifically for soft tissue wound-healing/regeneration, despite the great number of in vitro, in vivo, and clinical studies that have been reported on this topic to date. Although a large number of research to date has focused on the effects of PRP on various wound-healing events such as tendon regeneration,91–95 this systematic review article focused specifically on the regenerative potential of PRF for soft tissue management and excluded all studies where PRF was utilized for bone, cartilage, or tendon regeneration. In total, 48 studies met our inclusion criteria, with 31 studies being derived from human clinical studies (Table 4).
Although the effects of PRF were shown to enhance soft tissue regeneration in all but one in vitro and in vivo study (18 studies total), the results from the clinical studies need to be interpreted with caution. In total, 18 of the 31 clinical studies (58%) report a beneficial effect of PRF based on the investigators’ reported clinical experience; however, in these studies, no controls were utilized and the authors instead focused primary on their case reports/case series (Table 4). In contrast, all in vitro and in vivo studies utilized appropriate controls. It may, therefore, be concluded that this first wave of research provides the clinical evidence that PRF seems to promote soft tissue wound healing; however, it is clear that future human studies are needed to systematically compare the effects of PRF in a randomized, controlled fashion across a wide range of medical fields.
Similarly, it was recently reported in a systematic review that the effects of platelet concentrates showed similar findings on bone healing/formation of extraction sockets and intrabony defects (Fig. 6).96,97 Although the results of that meta-analysis are suggestive that platelet concentrates increase new bone formation in postextraction sockets, the authors report that due to the limited amount and quality of the available evidence, these results need to be cautiously interpreted. 96 It was reported that a standardization of the experimental design was necessary for a better understanding of the true effects of the use of platelet concentrates for enhancing postextraction socket healing. 96 Within the limits of our review article, we conclude similar findings that the effects of PRF enhance soft tissue regeneration; however, future studies on soft tissue regeneration after use of PRF need to be designed with appropriate controls and these findings need also to be interpreted with caution until further randomized clinical trials are gathered.

Clinical diagram of intrabony defect regeneration with PRF. Notice the initial lesions and soft tissue recessions that have successfully been regenerated after application with PRF. Adapted with permission from Anuroopa et al. 97 Color images available online at www.liebertpub.com/teb
One of the reported advantages of PRF was the ability for the fibrin network containing leukocytes to resist and fight infection. Chronic nonhealing wounds are a significant medical challenge and the pathogenesis of nonhealing wounds, therefore, requires new treatment options to improve clinical outcomes. One of the main factors to date hypothesized to further speed the wound-healing properties of PRF in comparison to PRP is the fact that it contains higher levels of WBCs that favor the continuous release of growth factors. Recently, we demonstrated that both PRF and the new formulation of PRF termed A-PRF were able to release significantly higher levels of growth factors when compared with PRP over a 10-day period. 39 Furthermore, macrophages have been shown to be key players during tissue regeneration, wound healing, and prevention of infection.28,37,38 Furthermore, they contain antimicrobial effects that are capable of reducing bacterial contamination after surgeries. 28 This finding was best exemplified in the healing of third molar extraction sockets. 61 It was reported that infection (osteomyelitis) is commonly reported in 9.5% of wisdom tooth removal and when a PRF plug was inserted after extraction, this was significantly reduced to 1% of cases. 61 Despite these reported findings, very little is yet known what the antibacterial properties of PRF are, as very little/few studies have investigated this phenomenon. 98
From a tissue-engineering standpoint, it remains interesting to note that no research to date has focused on the strength, stiffness, or toughness of PRF despite its clinical use for more than 15 years. Therefore, it remains of interest to better characterize its biomaterial properties and future research should focus on what factors might further improve its characteristics for various biomedical applications. For instance, it may be that for cartilage regeneration, versus ligament repair versus periodontal soft tissue management that variations of PRF may be further modified depending on the tensile demands and requirements of the defect. As currently only one centrifugation protocol of PRF is utilized for clinical use, it remains of interest to further study how modifications in centrifugation speeds and time might affect the biomechanical properties of PRF for various medical applications.
Furthermore, to date, very little is known regarding the effects of the fibrin architecture and leukocyte content from these products, as both these components are too often neglected as contributing factors in the tissue regenerative potential of PRF. The presence of leukocytes has a great impact on the biology of wound healing,17,30 not only due to their additional release of growth factors and their implications in antibacterial immune defense but also because they are key regulators controlling the wound-healing environment through local factor regulation. Future basic research should focus specifically on the contribution of these cells in specific cell knock-down/knock-in systems to determine the functional roles of each cell in the wound-healing process when PRF is utilized. For instance, it has been reported that addition of activated macrophage to wounds in aging mice and humans accelerated healing time. 28 Thus, in theory, the concept of developing newer modified protocols of PRF to further increase the number of WBCs would, in principle, increase wound repair. Nevertheless, a better understanding of the individual roles of the various cells found in PRF could prove to be an important finding for the development of these technologies, leading to modern changes to their protocols and further increasing their regenerative potential.
Conclusion
In summary, two main findings can be drawn from the present systematic review: (1) The currently available literature supports soft tissue regeneration after soft tissue regenerative procedures utilizing PRF; and (2) there is a lack of appropriate controls to the majority of studies drawing conclusive evidence that PRF is able to further, as most of the clinical studies to date thus far highlight the use of PRF in case series experiments or retrospective analysis without comparative results to appropriate controls. Therefore, it is imperative that the next wave of research utilizing PRF as an adjunct to soft tissue regenerative therapies designs appropriate studies with necessary controls to further evaluate the regenerative potential of PRF for soft tissue wound healing.
Footnotes
Disclosure Statement
No competing financial interest exist.